acute cyclosporine renal dysfunction reversed by dopamine infusion in healthy subjects
TRANSCRIPT

Kidney International, Vol. 36 (1989), pp. 1086—1092
Acute cyclosporine renal dysfunction reversed by dopamineinfusion in healthy subjects
GIUSEPPE CONTE, ANTONIO DAL CANTON, MAssIMo SABBATINI, PIETRO NAPODANO,LUCA DE NIc0LA, GIUSEPPE GIGLI0TTI, GI0RGI0 FuIAN0, ANGELO TESTA,
CIR0 EsposITo, DOMENICO Russo, and VITT0RI0 E. ANDREUCCI
Department of Nephrology, Faculty of Medicine of Caranzaro, University of Rep gb Calabria, and Department of Nephrology, SecondFaculty of Medicine, University of Naples, Naples Italy
Acute cyclosporine renal dysfunction reversed by dopamine infusion inhealthy subjects. Up to now, no studies have been performed in normalhumans to investigate the role of renal hemodynamic abnormalities inrelation to acute-cyclosporin A (CsA) renal dysfunction and to verifywhether the specific renal vasodilator, dopamine, can counteract theseabnormalities. Eight normal subjects were examined both (A) after oralCsA (12 mg/kg body wt) and (B) after oral CsA + dopamine infusion (2mg/kg body wt/min), under water diuresis. Both in protocols A and inB, four basal renal clearances were performed before CsA and everytwenty minutes for four hours after CsA administration. In protocol A,after CsA, inulin (GFR) and PAH clearance (RPF) fell by up to 27% andto 41%, respectively, so that filtration fraction (FF) increased (P <0.01). A slight (not significant) hypertension occurred while renalresistances were markedly raised (P < 0.001). Fractional urine and Naexcretion as well as CH,o decreased, while Uosm increased (P < 0.01).In protocol B, dopamirie was infused from 120 to 180 minutes after CsA(that is, when the maximal adverse effects of CsA on renal hemody.namics had been observed in A). Dopamine infusion could reversecompletely the effects of CsA on RPF, GFR, fractional urine output andCH2O; only U0,,, remained higher than normal in conjunction with anincreased fractional excretion of sodium (P < 0.01). No changes wereobserved in plasma renin activity, aldosterone and in urinary epineph-rine and norepinephrine excretion both in protocols A and B. Inconclusion, our data indicate that, in normal humans: (I) a single-dose ofCsA (12 mg/kg body wt per oz) causes marked renal vasoconstriction,impairment in GFR, increase in FF and proximal tubular overreabsorp-tion with fall of fractional urine and sodium excretion and, conse-quently, reduction in the renal ability to generate free-water (CH,O); (ii)the acute changes of glomerular and tubular function observed after oralCsA are accounted for by primary reversible alterations in renalhemodynamics; (iii) these effects are completely reversed by dopamineinfusion at low dosage.
Nephrotoxicity is the main limiting factor to a more extensiveuse of cyclosporin A (CsA) in the immunological managementof transplants and autoimmune diseases: sixty to ninety percentof patients treated with CsA develop impairment of renalfunction [1]. Its mechanism(s), however, is still unclear in spiteof several studies performed both in experimental animals andin humans [2—81. Whether the CsA-induced renal dysfunction is
Received for publication October 20, 1988and in revised form July 10, 1989Accepted for publication July 17, 1989
© 1989 by the International Society of Nephrology
due to a direct tubulo-interstitial toxic effect [5, 9—11] or to arenal vasoconstriction [4, 12—141 remains an unanswered ques-tion.
In experimental animals the acute hemodynamic effects oc-cur almost instantaneously after i.v. administration of CsAwhen renal blood flow is measured by electromagnetic flowprobe [15]. Therefore, the hemodynarnic changes might precedetubulo-interstial damage. The histopathological lesions, in fact,are detected after repeated administration of CsA and consistpredominantly of proximal tubular lesions [161. These morpho-logic changes are, however, nonspecific [161 and can be sec-ondary to the ischemia due to renal vasoconstriction [17].Hitherto, no studies on the acute effects of CsA on renalhemodynamics and tubular function have been carried out inrenal patients or in healthy subjects. Since it is not possible toexclude some renal dysfunction in patients with organ allograftor with autoimmune diseases [5, 6, 18], we decided to study thefunctional effects of CsA on the kidney of healthy subjects.
In laboratory animals, various attempts have been made toclarify the pathogenesis of acute CsA nephrotoxicity and toprevent renal functional impairment [3, 19—221 by vasodilatingagents, The results of these studies were not conclusive; inparticular, vasodilating drugs generally showed a partial revers-ibility of the reduced GFR. The efficacy of vasodilators inpreventing CsA nephrotoxicity in humans has been poorlyevaluated [23], and never by prospective studies. Dopamine atlow dosage is known to increase renal blood flow and GFR byacting on specific intrarenal receptors without causing systemicpressure effects; for this property, it has been used to evaluatethe renal functional reserve in normal subjects [24J. It has alsobeen used to ameliorate the clinical course of patients withorganic acute renal failure [25].
The present studies were, therefore, designed to investigatein normal humans the role of renal hemodynamic abnormalitiesin relation to acute glomerular and tubular dysfunction inducedby CsA and to test the possibility that the specific renalvasodilator, dopamine, can counteract these abnormalities. Asingle-dose CsA administration either alone or associated withdopamine infusion in healthy subjects appeared to be the mostsuitable model for assessing the functional effects of CsA in acondition in which histopathological damage could not occur[26].
1086

Conte et a!: GsA and dopamine in healthy patients 1087
Methods
SubjectsThe studies were performed in eight healthy male volunteers,
all physicians of our Unit aged 25 to 36 years (mean: 28).Informed written consent was obtained from each of them afterexplanation of the experimental protocol as well as CsA anddopamine side-effects. The subjects were taking no medicationsfor at least one month before the study; the use of alcohol,tobacco, tea, and coffee was prohibited for at least one daybefore the study. Beginning one week before and during thewhole study, all subjects received a controlled diet with con-stant intake of protein (1 g/kg of body wt), sodium (170 mmolper day), potassium (40 mmol per day) and calories (30 kCal/kgof body wt). A period of stabilization was allowed until themagnitude of changes in creatinine clearance, urinary sodiumand potassium excretion did not exceed 10% in three consecu-tive days.
Clearance methods
All subjects were studied by renal clearance methods duringmaximal water diuresis (induced by 20 ml of water/kg of bodywt per os in 20 mm and maintained by 20 mI/mm of 5% glucosei.v.). The increase in urine flow induced by water diuresis, infact, permits several clearance periods in a relatively shorttime. When a steady state of urine flow had been obtained (thatis, when the magnitude of changes in urine volume did notexceed 10% in three consecutive periods), renal clearanceswere performed. The subjects were allowed to stand duringvoiding, and to sit in the intervening period. A solution of inulinand PAR (6 g of inulin and 4 g of PAH in 500 ml of NaCI 0.9%)was infused i.v. at a rate of I mI/mm to maintain plasmaconcentrations of inulin at 15 to 20 mgldl and PAH at 1.5 to 2.0mg/dl. A 60-minute equilibration period was allowed after thestart of infusion for the achievement of steady plasma levels ofinulin and PAH.
Two different studies (A and B) were performed in the sameeight subjects.
Protocol A: Cyclosporin studyAfter a steady urine volume was achieved, four accurately-
timed urine collections of twenty minutes were obtained byspontaneous voiding before giving CsA orally at the dosage of12 mg/kg of body wt. Three clearance periods per hour werethen performed in the four hours following CsA administration.This time period of four hours was chosen on the basis ofprevious studies of CsA pharmacokinetics [27], in which asingle oral dose of CsA, administered in healthy subjects,determined a peak of blood CsA concentration from two to fourhours after drug administration. Blood samples were collectedat the beginning and the end of each clearance period fordetermination of plasma inulin, PAR, creatinine, urea, sodium,potassium, chloride, osmolality, aldosterone, renin activity,blood CsA levels and hematocrit. Urinary samples were ana-lyzed for determination of inulin, PAH, creatinine, urea, so-dium, potassium, chloride, osmolality and catecholamines (nor-epinephrine and epinephrine). Blood pressure and heart ratewere monitored every ten minutes throughout the study. Renalblood flow (RBF) was calculated from renal plasma flow (RPF,PAH clearance) and hematocrit. Mean arterial pressure was
calculated as the sum of the diastolic pressure plus 1/3 of thedifference between systolic and diastolic pressure. Renal vas-cular resistance (RVR) was calculated by dividing the meanarterial pressure by RBF.
Protocol B: Cyclosporin plus dopamine studyOn the basis of data of protocol A, a second study was
performed following the same protocol, but with the addition ofan i.v. infusion of dopamine (2 pg/kg of body wt/min) in 5% ofglucose for 60 mm, from the beginning of the third hour afterCsA administration. After the end of dopamine infusion, threefurther clearance periods (4th hour) were performed. Clearancemeasurements were identical as in protocol A.
Laboratory proceduresInulin and PAH concentrations were determined by tech-
niques that have been previously described [281. In all analyti-cal determinations the standard curves of inulin and PAH weredetermined by linear regression analysis; the correlation coef-ficient of these curves was always greater than r = 0.996.Sodium and potassium were measured by a flame photometer;chloride, creatinine and urea by a Technicon AutoAnalyzer;osmolality by an osmometer (Model 250 D, Fiske AssociatesInc., Uxbridge, Massachusetts, USA). Plasma renin activitywas measured by radioimmunoassay of angiotensin I and aldo-sterone by standard radioimmunoassay, as previously de-scribed [291; blood levels of CsA were measured by radioim-munoassay of polyclonal antibodies (Sandoz LTD, Basle,Switzerland). Urinary excretion of norepinephrine and epineph-rifle were determined by fluorometric assay on acidified urine asdescribed elsewhere [30]; urinary determination was chosen asa better estimate of adrenergic activity than plasma cathechola-mines levels, because of the very short half-life of thesehormones [31].
Statistical analysisAll the clearance data have been corrected for a body surface
area of 1.73 m2. Data are presented as means and standarderrors. Analysis of variance for repeated measures and linearregression analysis were used. P values less than 0.05 wereconsidered statistically significant.
Results
Since the four clearances for the determination of above-mentioned parameters before CsA were not different in thestudy A and in the study B, the means of these four clearanceperiods were used as basal values.
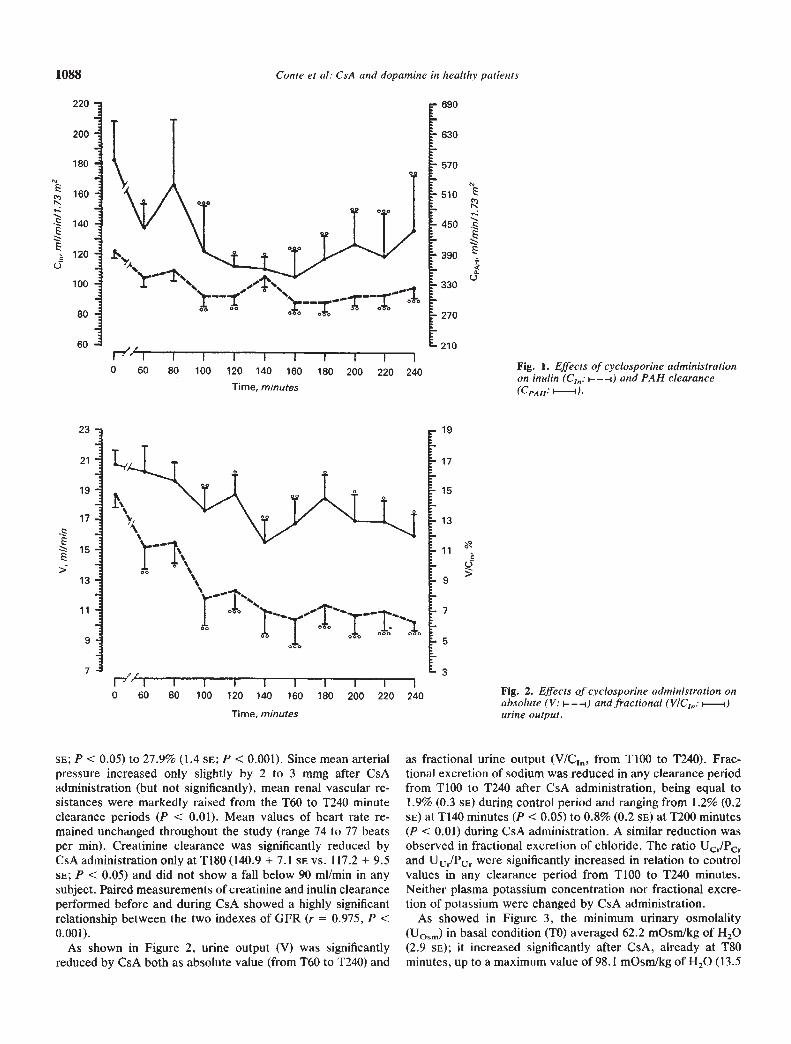
Protocol A: Cyclosporin studyAs shown in Figure 1, CsA caused a decrease of both inulin
(C1) and PAH (CPAH) clearances, which became significant atTl00 and at T60 minutes after CsA administration, respectively.C1,, in fact, fell significantly from a basal value of 121.9 (5.4 SE)mi/mm to 92.3 (7.5 SE; P < 0.01) at TlOO minutes and remaineddecreased thereafter; CPAH fell from 581.1 (73.5 SE) to 396.6(88.7 SE) mI/mm (P < 0.001) at T100 minutes and remained lowthereafter, The FF was significantly increased in any clearanceperiod from TlOO to 240 minutes after CsA administration:during the control period, FF was equal to 20.5% (1.6 SE) whileduring the period from T100 to T240 it ranged from 23.0% (2.4
1088 Conte et a!: CsA and dopamine in healthy patients
0 60
220 -
200 -
180
160-
140:
5120:100 -
80 -
60 -
23 -
21
19
17
11
9.
7.
I I I
80 100 120 140 160Time, minutes
180 200 220 240
"-——-I"
• 690
• 630
• 570
-sb
-450
390
0- 330
- 270
210
Fig. 1. Effects of cyctosporine administrationon maim (C1,,: i-—-i) and PAH clearance(CPAH: —i).
- 19
- 17
15
13
1°e>
H5
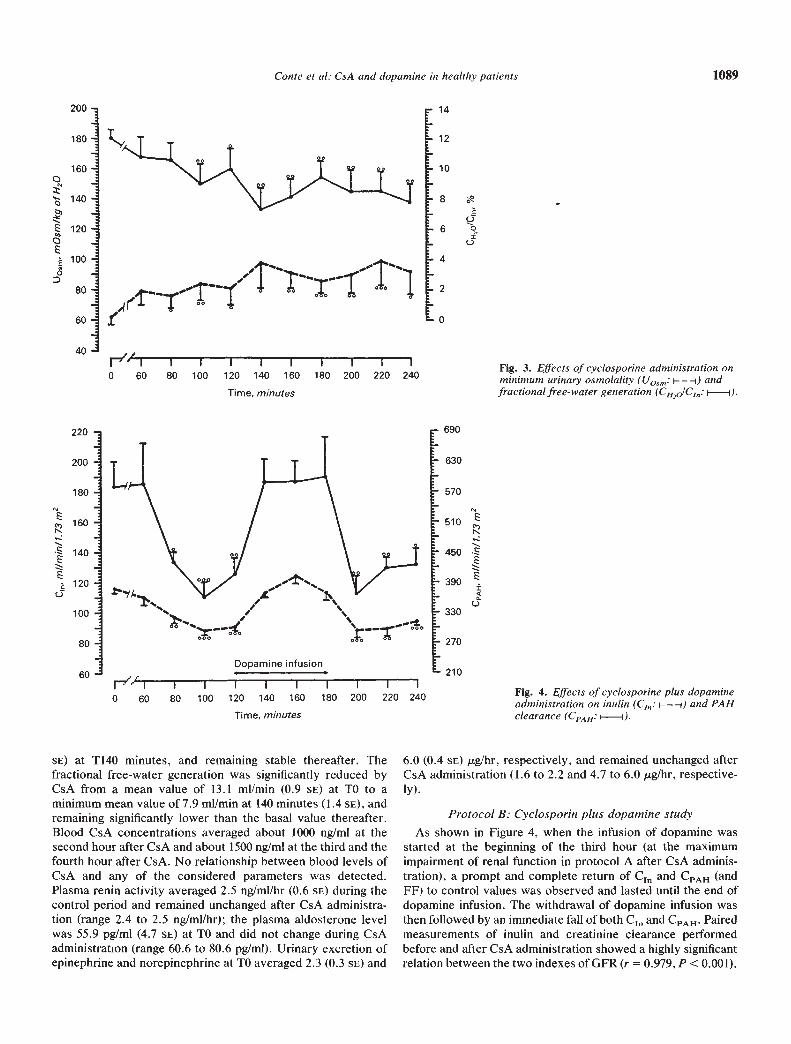
Fig. 2. Effects of cyclospormne administration onabsolute (V: I———l) and fractional (V/C,,,: i—i)urine output.
as fractional urine output (V/C1, from TlOO to T240). Frac-tional excretion of sodium was reduced in any clearance periodfrom Tl00 to T240 after CsA administration, being equal to1.9% (0.3 SE) during control period and ranging from 1.2% (0.2SE) at T140 minutes (P < 0.05) to 0.8% (0.2 s) at T200 minutes(P C 0.01) during CsA administration. A similar reduction wasobserved in fractional excretion of chloride. The ratio UcjPcrand UUjPU, were significantly increased in relation to controlvalues in any clearance period from TlOO to T240 minutes.Neither plasma potassium concentration nor fractional excre-tion of potassium were changed by CsA administration.
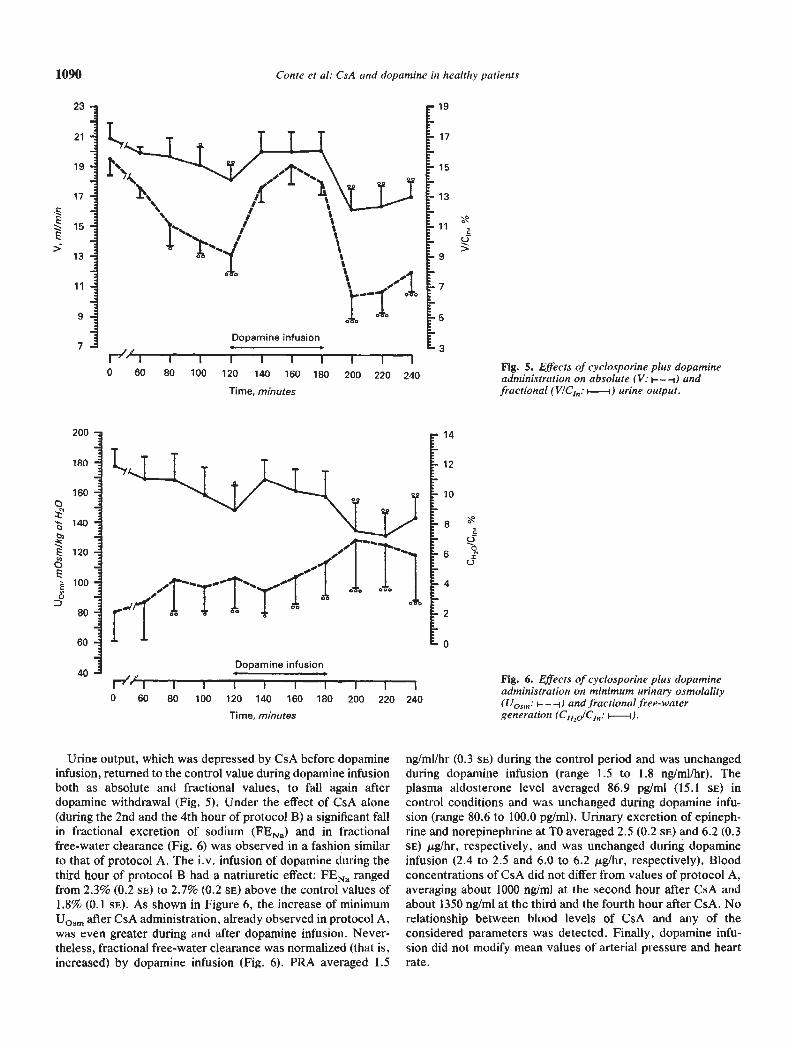
As showed in Figure 3, the minimum urinary osmolality(Uosm) in basal condition (TO) averaged 62.2 mOsm/kg of H20(2.9 se); it increased significantly after CsA, already at T80minutes, up to a maximum value of 98.1 mOsmlkg of H70 (13.5
I I I I I I I I I0 60 80 100 120 140 160 180 200 220 240
Time, minutes
SE; P C 0.05) to 27.9% (1.4 SE; P < 0.001). Since mean arterialpressure increased only slightly by 2 to 3 mmg after CsAadministration (but not significantly), mean renal vascular re-sistances were markedly raised from the T60 to T240 minuteclearance periods (P C 0.01). Mean values of heart rate re-mained unchanged throughout the study (range 74 to 77 beatsper mi. Creatinine clearance was significantly reduced byCsAadministrationonlyatTl8O(14O.9 + 7.1 srvs. 117.2 + 9.5sE; P C 0,05) and did not show a fall below 90 mI/mm in anysubject. Paired measurements of creatinine and inulin clearanceperformed before and during CsA showed a highly significantrelationship between the two indexes of GFR (r = 0.975, P C0.001).
As shown in Figure 2, urine output (V) was significantlyreduced by CsA both as absolute value (from T60 to T240) and
200 -
180
160 -0 -
140--
E 120--
100 -0 -
80 —
60 -
40 -
Conte et at: CsA and dopamine in healthy patients
690
- 630
- 570
:450
—390—
C-)330
270
L 210
1089
SE) at T140 minutes, and remaining stable thereafter. Thefractional free-water generation was significantly reduced byCsA from a mean value of 13.1 mI/mm (0.9 SE) at TO to aminimum mean value of 7.9 mI/mm at 140 minutes (1.4 SE),andremaining significantly lower than the basal value thereafter.Blood CsA concentrations averaged about 1000 ng/ml at thesecond hour after CsA and about 1500 ng/ml at the third and thefourth hour after CsA. No relationship between blood levels ofCsA and any of the considered parameters was detected.Plasma renin activity averaged 2.5 ng/ml/hr (0.6 SE) during thecontrol period and remained unchanged after CsA administra-tion (range 2.4 to 2.5 ng/ml/hr); the plasma aldosterone levelwas 55.9 pg/mI (4.7 SE) at TO and did not change during CsAadministration (range 60.6 to 80.6 pg/mI). Urinary excretion ofepinephrine and norepinephrine at TO averaged 2.3 (0.3 SE) and
6.0 (0.4 SE) pg/hr, respectively, and remained unchanged afterCsA administration (1.6 to 2.2 and 4.7 to 6.0 pg/hr, respective-ly).
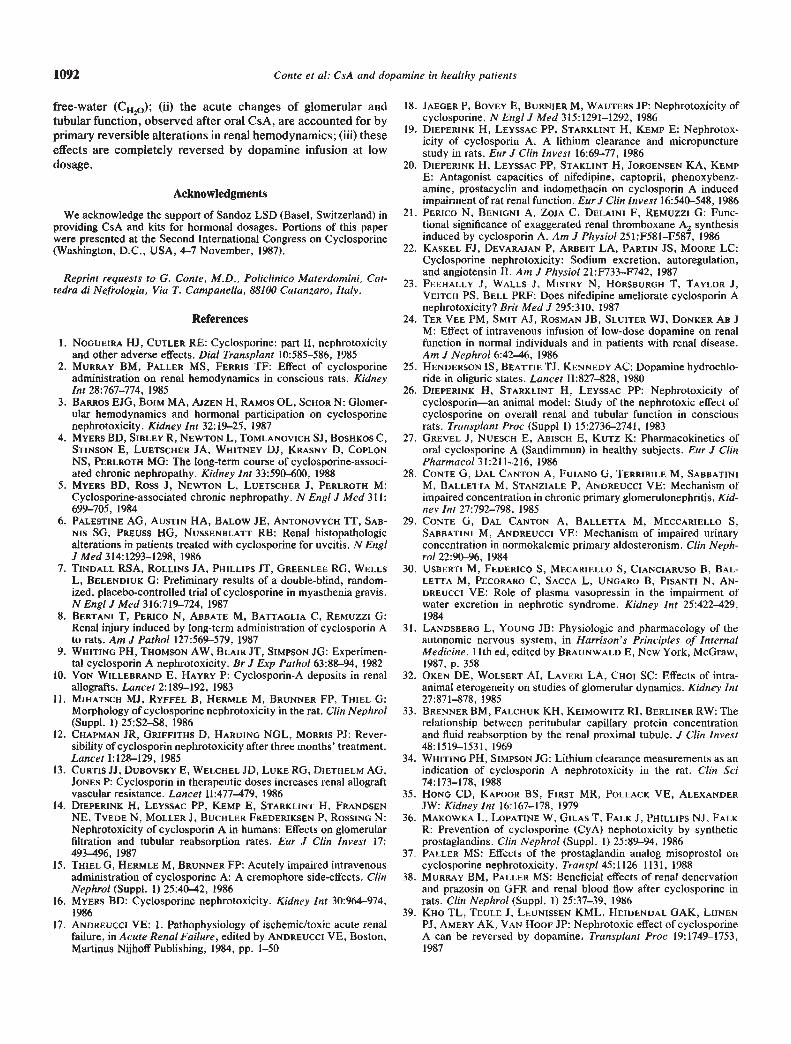
Protocol B: Cyclosporin plus dopamine studyAs shown in Figure 4, when the infusion of dopamine was
started at the beginning of the third hour (at the maximumimpairment of renal function in protocol A after CsA adminis-tration), a prompt and complete return of C1 and CPAH (andFF) to control values was observed and lasted until the end ofdopamine infusion. The withdrawal of dopamine infusion wasthen followed by an immediate fall of both C1, and CPAH. Pairedmeasurements of inulin and creatinine clearance performedbefore and after CsA administration showed a highly significantrelation between the two indexes of GFR (r = 0.979,P < 0.001).
• 14
- 12
- 10
-8
-6
-4
-2
-0
00I0
.f9,4
i-"i0 60 80
I I I100 120 140 160
Time, minutes
180 200 220 240
220
200
180 -
160
1140:a 120 -
0100 -
80 -
60 -
Fig. 3. Effects of cyclosporine administration onminimum urinary osmolality (Uo,,,: — — -i) andfractional free-water generation (CH2O/CJ,: F—I).
Fig. 4. Effects of cyclosporine plus dopamineadministration on inulin (C,,,: i— — —i) and PAHclearance (CPAH: —F).
rr0 60
Dopamine infusion
I I I I I I80 100 120 140 160 180
Time, minutes
—f_-I I200 220 240
1090
23 -
21 -
19
17 --
15-E> 13 -
11 —
9-
7-
Conte et a!: CsA and dopamine in healthy patients
Urine output, which was depressed by CsA before dopamineinfusion, returned to the control value during dopamine infusionboth as absolute and fractional values, to fall again afterdopamine withdrawal (Fig. 5). Under the effect of CsA alone(during the 2nd and the 4th hour of protocol B) a significant fallin fractional excretion of sodium (FENa) and in fractionalfree-water clearance (Fig. 6) was observed in a fashion similarto that of protocol A. The i.v. infusion of dopamine during thethird hour of protocol B had a natriuretic effect: FENa rangedfrom 2.3% (0.2 SE) to 2,7% (0.2 SE) above the control values of1.8% (0.1 SE). As shown in Figure 6, the increase of minimumUosm after CsA administration, already observed in protocol A,was even greater during and after dopamine infusion. Never-theless, fractional free-water clearance was normalized (that is,increased) by dopamine infusion (Fig. 6). PRA averaged 1.5
ng/ml/hr (0.3 SE) during the control period and was unchangedduring dopamine infusion (range 1.5 to 1.8 nglmllhr). Theplasma aldosterone level averaged 86.9 pg/ml (15.1 SE) incontrol conditions and was unchanged during dopamine infu-sion (range 80.6 to 100.0 pg!ml). Urinary excretion of epineph-rine and norepinephrine at TO averaged 2.5 (0.2 SE) and 6.2 (0.3SE) gIhr, respectively, and was unchanged during dopamineinfusion (2.4 to 2.5 and 6.0 to 6.2 gIhr, respectively). Bloodconcentrations of CsA did not differ from values of protocol A,averaging about 1000 ng/ml at the second hour after CsA andabout 1350 nglml at the third and the fourth hour after CsA. Norelationship between blood levels of CsA and any of theconsidered parameters was detected. Finally, dopamine infu-sion did not modify mean values of arterial pressure and heartrate.
1-7'AT-0 60
Dopamine infusion
1 I I80 100 120 140 160 180
Time, minutes
- 19
- 17
- 15
- 13
— 11
-9
—7
-5
—3
• 14
- 12
- 10
-6
.4
-2
•0
0>
00I0
200 -
180 -
160 -
140 --
E 120 --
1000
80T
60
40
I I IFig. 5. Effects of cyclosporine plus dopamine200 220 240 administration on absolute (V: i— — -i) andfractional (V/C1: —i) urine output.
,/1.1.
Fig. 6. Effects of cyclosporine plus dopaminel' I I I I I I I I I I administration on minimum urinary osmolality0 60 80 100 120 140 160 180 200 220 240 (Uosm: ——-i) and fractional free-water
generation (C1120/C1: —i).
Dopamine infusion
Time, minutes

Conte et at: GsA and dopamine in healthy patients 1091
Discussion
After a single oral administration of CsA in healthy subjects(12 mg/kg of body wt), in a dose similar to that proposed in theearly phase of organ allograft [16], we have observed a rapid,progressive impairment of renal function: C1, and CPAH, in fact,were already reduced after about one hour, reaching steadly thelowest values from the second hour on. The striking fall ofCPAH was associated with a moderate decrease of C1,,, so thatFF increased significantly. These changes of renal function areusually observed in laboratory animals and in humans duringprerenal acute failure [171. The nonproportional decrease ofCPAH and C1,, after CsA administration was likely due to adisequilibrium of glomerular pressures at the efferent end of theglomerular capillary network, as demonstrated in dogs andhypothesized in men [32], so that GFR is not plasma flowdependent. The resulting increase of filtration fraction, byraising the oncotic pressure in peritubular capillaries, is ex-pected to cause proximal overreabsorption of tubular fluid [33].This proximal overreabsorpticn did presumably occur in ournormal subjects after CsA administration, as suggested by thedecrease of urine output and free-water clearance. Other stud-ies, performed after short-term CsA administration both inexperimental animals and in humans, have demonstrated anincreased proximal fractional reabsorption [14, 18, 34]. Theevaluation of the diagnostic indexes commonly used for differ-entiating "prerenal" acute failure from acute tubular necrosis(FENa, Uosm, U/Pcr, U/Pur, etc.) indicates that the CsAinduced impairment of renal function "mimics" the conditionof functional renal insufficiency caused by renal hypoperfusion,suggesting an arteriolar vasoconstriction as the primary renaleffect of CsA when given acutely. These observations haverelevant clinical implications: our findings, observed duringacute CsA nephrotoxicity, are similar to those shown by otherauthors during the early stage of renal rejection [35].
Undoubtedly, measurement of renal plasma flow by CPAHwithout determination of PAH extraction has an importantdrawback in that CPAH does not represent effective renalplasma flow, neither in healthy subjects nor when renal functionis impaired by CsA [4]. After acute administration of CsA inrats, however, Dieperink et al [19] did not find any significantdifference between CPAH and effective renal plasma flow mea-sured by PAH extraction. In our acute study, CsA caused onlya moderate impairment of Ci,,. In agreement with other authors[13], it is reasonable to argue that in such a condition CPAH canbe considered a reliable index of renal plasma flow.
It is well known that dopamine interacts in the kidney withspecific dopaminergic receptors and reduces glomerular arteri-olar resistances, thereby improving renal cortical perfusion[24]. In our CsA + dopamine study, in spite of blood levels ofCsA similar to those obtained during CsA study, the infusion ofdopamine at dopaminergic dosage was able to completelyreverse the marked renal vasoconstriction, the impairment inGFR and the depressed fractional urine output. These modifi-cations occurred with no changes in blood pressure nor in heartrate. According to the worldwide literature, attempts to protectlaboratory animals from CsA by other agents, such as phenox-ibenzamine [20], tromboxane inhibitors [9], nifedipine [20],captopril [3, 20, 22], and prostaglandin [20, 36], have not led tocomplete correction of GFR impairment induced by CsA.
The reversibility of the renal effects of CsA by dopamineinfusion, the reappearance of renal CsA impairment immedi-ately after dopamine withdrawal and the rapidity by which thereversion and reappearance occurs strongly indicate that renalvasoconstriction is the primary effect of CsA acute dysfunction,and that dopamine counteracts this effect in humans. Recently,it has been demonstrated in experimental animals that bothrenal vasodilators, as misoprostol [371, and antivasoconstrictiveagents, as phenoxibenzamine [2], and renal denervation [38]can completely reverse the effects of CsA on renal plasma flow.These findings indicate that the beneficial vascular effects ofdopamine are not specific to this agent and its receptors.
In normal subjects, dopamine infusion is known to increasesodium chloride excretion by reducing proximal tubular reab-sorption [24]. Such an effect may have contributed (in additionto the normalized glomerular dynamics) to the increase offractional excretion of sodium observed in our study with CsAplus dopamine. The augmented delivery of sodium chlorideduring dopamine infusion restored the fractional generation offree-water (CH2O/CIfl) to normal, previously reduced by CsAalone. The increased osmolar load, however, did not allow theachievement of the minimal urinary osmolality obtained duringcontrol period.
Also, Kho et al [39] have studied the influence of dopamineinfusion on renal hemodynamics in CsA-treated renal transplantpatients. In this paper, however, the patients were examinedafter chronic treatment with CsA and had impairment of renalfunction. In such conditions, the infusion of dopamine slightlyincreased the "effective" renal plasma flow without changingGFR. But, the measurement of "effective" renal plasma flow,performed by Kho et a! [391, by using a radioisotope infusionmethod without venous catheterization is not adequate inconditions of renal failure; no information is given concerningradioisotope infusion method, renal clearances periods, statis-tical methods, cause of renal failure, etc.
Taken together, the findings of the protocols A and B inrelation to tubular function indicate that the tubular alterationsinduced by CsA may be explained by renal hemodynamicchanges rather than by direct effects of the drug on tubularepithelial cells, and than these dysfunctions can be overcomeby dopamine infusion, suggesting a vascular disturbance. Thesestatements must be restricted to the very short period of theinvestigation. Indeed, our study does not conclusively rule outthe possibility that direct tubular insults are occurring or willoccur in time and/or that the vascular effects might not takeplace after repeated doses of CsA over many days.
PRA, aldosterone plasma levels and urinary excretion ofepinephrine and norepinephrine were not affected by CsA, norby dopamine in our studies. Thus, neither the renin-angiotensinsystem nor the sympathetic nervous system appear to beinvolved in the changes of renal hemodynamics secondary toCsA and/or dopamine administration in humans. Undoubtedly,other hormonal factors, such as prostaglandins and trombox-ane, may play some role in CsA-induced nephrotoxicity buttheir involvement in humans has still to be defined.
In conclusion, our data indicate that: (i) a single oral dose ofCsA (12 mg/kg body wt) causes marked renal hypoperfusion,impairment in GFR, increase in FF and proximal tubularoverreabsorption with fall of fractional urine and sodium excre-tion and, consequently, reduction in the renal ability to generate
1092 Conte et a!: GSA and dopamine in healthy patients
free-water (CH2O); (ii) the acute changes of glomerular andtubular function, observed after oral CsA, are accounted for byprimary reversible alterations in renal hemodynamics; (iii) theseeffects are completely reversed by dopamine infusion at lowdosage.
Acknowledgments
We acknowledge the support of Sandoz LSD (Basel, Switzerland) inproviding CsA and kits for hormonal dosages. Portions of this paperwere presented at the Second International Congress on Cyclosporine(Washington, D.C., USA, 4—7 November, 1987).
Reprint requests to G. Conte, M.D., Policlinico Materdomini, Cat-tedra di Nefrologia, Via T. Campanella, 88100 Catanzaro, Italy.
References
1. Noauiii Hi, CUTLER RE: Cyclosporine: part II, nephrotoxicityand other adverse effects. Dial Transplant 10:585—586, 1985
2. MURRAY BM, PALLER MS, FERIUs TF: Effect of cyclosporineadministration on renal hemodynamics in conscious rats. Kidneymt 28:767—774, 1985
3. BARROS EJO, BOIM MA, AJZEN H, RAMOS OL, SCHOR N: Glomer-ular hemodynamics and hormonal participation on cyclosporinenephrotoxicity. Kidney mt 32:19—25, 1987
4. MYERS BD, SIBLEY R, NEWTON L, TOMLANOVICH Si, BOSHKOS C,STINSON E, LUETSCHER JA, WHITNEY Di, KRASNY D, COPLONNS, PERLROTH MG: The long-term course of cyclosporine-associ-ated chronic nephropathy. Kidney mt 33:590—600, 1988
5. MYERS BD, Ross J, NEWTON L, LUETSCHER J, PERLROTH M:Cyclosporine-associated chronic nephropathy. N Engl J Med 311:699—705, 1984
6. PALESTINE AG, AUSTIN HA, BALOW JE, ANTONOVYCH TT, SAB-NIS SG, PREUSS HG, NUSSENBLATT RB: Renal histopathologicalterations in patients treated with cyclosporine for uveitis, N EngiJ Med 314:1293—1298, 1986
7. TINDALL RSA, ROLLINS JA, PHILLIPS JT, GREENLEE RG, WELLSL, BELENDIUK G: Preliminary results of a double-blind, random-ized, placebo-controlled trial of cyclosporine in myasthenia gravis.N EngiJ Med 316:719—724, 1987
8. BERTANI T, PERICO N, ABBATE M, BATTAGLIA C, REMUZZI G:Renal injury induced by long-term administration of cyclosporin Ato rats. Am J Pathol 127:569—579, 1987
9. WHITING PH, THOMSON AW, BLAIR iT, SIMPSON JG: Experimen-tal cyclosporin A nephrotoxicity. Br J Exp Pathol63:88—94, 1982
10. VoN WILLEBRAND E, HAYRY P: Cyclosporin-A deposits in renalallografts. Lancet 2:189—192, 1983
11. MIHATSCH Mi, RYI'FEL B, HERMLE M, BRUNNER FP, THIEL G:Morphology of cyclosporine nephrotoxicity in the rat. Gun Nephrol(Suppl. 1) 25:S2—S8, 1986
12. CHAPMAN JR, GRIFFITHS D, HARDING NGL, MORRIS PJ: Rever-sibility of cyclosporin nephrotoxicity after three months' treatment.Lancet 1:128—129, 1985
13. CURTIS ii, DUBOVSKY E, WELCHEL iD, LUKE RG, DIETHELM AG,JONES P: Cyclosporin in therapeutic doses increases renal allograftvascular resistance. Lancet 11:477—479, 1986
14. DIEPERINK H, LEYSSAC PP, KEMP E, STARKLINT H, FRANDSENNE, TVEDE N, MOLLER .1, BUCHLER FREDERIKSEN P, ROSSING N:Nephrotoxicity of cyclosporin A in humans: Effects on glomerularfiltration and tubular reabsorption rates. Eur J Clin In vest 17:493—496, 1987
15. THIEL G, HERMLE M, BRUNNER FP: Acutely impaired intravenousadministration of cyclosporine A: A cremophore side-effects, GunNephrol (Suppl. 1) 25:40—42, 1986
16. MYERS BD: Cyclosporine nephrotoxicity. Kidney mt 30:964-974,1986
17. ANDREUCCI YE: 1. Pathophysiology of ischemic/toxic acute renalfailure, in Acute Renal Failure, edited by ANDREUCCI yE, Boston,Martinus Nijhoff Publishing, 1984, pp. 1—50
18. JAEGER P, BOVEY E, BURNIER M, WAUTERS JP: Nephrotoxicity ofcyclosporine. N Engi J Med 315:1291—1292, 1986
19. DIEPERINK H, LEYSSAC PP. STARKLINT H, KEMP E: Nephrotox-icity of cyclosporin A. A lithium clearance and micropuncturestudy in rats. Eur J Clin Invest 16:69—77, 1986
20. DIEPERINK H, LEYSSAC PP, STAKLINT H, JORGENSEN KA, KEMPE: Antagonist capacities of nifedipine, captopril, phenoxybenz-amine, prostacyclin and indomethacin on cyclosporin A inducedimpairment of rat renal function. EurJ Gun Invest 16:540—548, 1986
21. PERIc0 N, BENIGNI A, ZOJA C, DELAINI F, REMUZZI G: Func-tional significance of exaggerated renal thromboxane A2 synthesisinduced by cyclosporin A. Am J Physiol 25l;F58l—F587, 1986
22. KASKEL Fi, DEVARAJAN P, ARBEIT LA, PARTIN JS, MOORE LC:Cyclosporine nephrotoxicity: Sodium excretion, autoregulation,and angiotensin II. Am J Physiol 21 :F733—F742, 1987
23. FEEHALLY J, WALLS J, MISTRY N, HORSBURGH T, TAYLOR i,VEITCH PS, BELL PRF: Does nifedipine ameliorate cyclosporin Anephrotoxicity? Brit Med J 295:310, 1987
24. TER VEE PM, SMIT AJ, ROSMAN JB, SLUITER Wi, DONKER AB JM: Effect of intravenous infusion of low-dose dopamine on renalfunction in normal individuals and in patients with renal disease.Am J Nephrol 6:42—46, 1986
25. HENDERSON IS, BEATTIE TJ, KENNEDY AC: Dopamine hydrochlo-ride in oliguric states. Lancet 11:827—828, 1980
26. DIEPERINK H, STARKLINT H, LEYSSAC PP: Nephrotoxicity ofcyclosporin—an animal model: Study of the nephrotoxic effect ofcyclosporine on overall renal and tubular function in consciousrats. Transplant Proc (Suppl 1)15:2736—2741, 1983
27. GREVEL J, NUESCH E, ABISCH E, KUTZ K: Pharmacokinetics oforal cyclosporine A (Sandimmun) in healthy subjects, Eur J ClinPharmacol 31:211—216, 1986
28. CONTE G, DAL CANTON A, FUIANO G, TERRIBILE M, SABBATINIM, BALLETTA M, STANZIALE P, ANDREUCCI YE: Mechanism ofimpaired concentration in chronic primary glomerulonephritis. Kid-ney mt 27:792—798, 1985
29. CONTE U, DAL CANTON A, BALLETTA M, MECCARIELLO S,SABBATINI M, ANDREUCCI VE: Mechanism of impaired urinaryconcentration in normokalemic primary aldosteronism. Clin Neph-
rol 22:90—96, 198430. USBERTI M, FEDERICO S. MECARIELLO S, CIANCIARUSO B, BAL-
LETTA M, PECORARO C, SACCA L, UNGARO B, PISANTI N, AN-DREUCCI VE: Role of plasma vasopressin in the impairment ofwater excretion in nephrotic syndrome. Kidney mt 25:422—429,1984
31. LANDSBERG L, YOUNG JB: Physiologic and pharmacology of theautonomic nervous system, in Harrison's Principles of Internal
Medicine, 11th ed, edited by BRAUNWALD E, New York, McGraw,1987, p. 358
32. OKEN DE, WOLSERT Al, LAVERI LA, CH0! SC: Effects of intra-animal eterogeneity on studies of glomerular dynamics. Kidney mt27:871—878, 1985
33. BRENNER BM, FALCHUK KH, KEIMOwITZ RI, BERLINER RW: Therelationship between peritubular capillary protein concentrationand fluid reabsorption by the renal proximal tubule. J Clin invest
48:1519—1531, 196934. WHITING PH, SIMPSON JG: Lithium clearance measurements as an
indication of cyclosponn A nephrotoxicity in the rat. Gun Sci74:173—178, 1988
35. HONG CD, KAPOOR BS, FIRST MR, POLLACK yE, ALEXANDERJW: Kidney mt 16:167—178, 1979
36. MAKOWKA L, LOPATINE W, GILAS T, FALK J, PHILLIPS Ni, FALKR: Prevention of cyclosporine (CyA) nephotoxicity by syntheticprostaglandins. Cliii Nephrol (Suppl. I) 25:89—94, 1986
37. PALLER MS: Effects of the prostaglandin analog misoprostol oncyclosporine nephrotoxicity. Transpl 45:1126-1131, 1988
38. MURRAY BM, PALLER MS: Beneficial effects of renal denervationand prazosin on UFR and renal blood flow after cyclosporine inrats. C/in Nephrol (Suppl. 1) 25:37—39, 1986
39. Kio TL, TELJLE J, LEUNISSEN KML, HEIDENDAL GAK, LIJNENPJ, AMERYAK, VAN HooF iP: Nephrotoxic effect of cyclosporine
A can be reversed by dopamine Transplant Proc 19:1749-1753,1987