acupuncture cpd back & lower limb · extra lower limb points •ex-le 2 heding lower extremity...
TRANSCRIPT

31/07/2017
1
ACUPUNCTURE CPD Back & Lower Limb
Jonathan Hobbs MSc MCSP FHEA
AACP Chairman & Accredited Tutor
ACUPUNCTURE ASSOCIATION OF
CHARTERED PHYSIOTHERAPISTS
Aims
• Improve knowledge of BL, GB, ST, SP, LR, KI and GV meridians
• Review meridian point selection for msk conditions
• Review extra point location and usage for msk conditions
• Review additional techniques for the treatment of msk pain related to the back and lower limb

31/07/2017
2
Objectives
To be able to:
• Have a greater understanding of BL, GB, ST, SP, LR, KI and GV channels for the treatment of msk pain
• Treat back and lower limb msk pain and dysfunction with BL, GB, ST, SP, LR, KI and GV channels
• Treat back and lower limb msk pain and dysfunction with trigger points and off channel techniques
Overview
• Mechanisms and theories
• Layering technique
• Classic meridian points
• HTJJ
• Extra points
• Myofascial trigger points
• Paraspinal Needling
• Summary

31/07/2017
3
Acupuncture Trialists’ Collaboration
• Systematic review 29 (RCTs), n=17 922, acupuncture for chronic pain (back and neck pain, osteoarthritis, chronic headache, and shoulder pain).
Conclusion:
• Effective for the treatment of chronic pain - reasonable referral option
• Significant differences between true and sham acupuncture
• Indicates acupuncture is more than a placebo
• Relatively modest difference – additional effects to needling important to therapeutic effect
• Vickers et al, (2012)
Acupuncture Needle Painful Stimulus
Skin
Muscle
Spinal Cord
Mid Brain
Pituitary
Hypothalamus
Thalamus
Cortex
1
2
7
6
5
8 9 10 11
3
14 12
13
4
E
ALT
DLT
M
M
E
E E
E
STT
Legend
Nerve Cell
Excitatory Synapse
Inhibitory Synapse
Sensory Nerve
Blood Vessel
Direction of Impulse
Acupuncture needle
Sensory Receptor
Painful Stimulus
Hormone Release
ALT - Anterolateral
Tract
DLT – Dorsolateral
Tract
STT – Spinothalamic
Tract
M – Monoamines
E - Endorphins
Acupuncture Analgesia
(after Stux & Hammerschlag, 2001)

31/07/2017
4
Peripheral (local) effects
• Needle points close to injury
• Stimulate gently to maximise local effect.
• Superficial tissues –low-intensity to reduce sympathetic tone and aid circulation
31/07/2017
5
Segmental/spinal effects
• Local points anatomically near to damaged tissue
• Or points away from damaged tissue with same segmental innervation
• Same myotome, choose area with tender points
Supraspinal effects
• Extra-segmental points & “big points‟ of the extremities
• Strong stimulation to activate descending inhibitory systems from the hypothalamus, and DNIC
• Rx time 20-40minutes
31/07/2017
6
Central sympathetic effects
• Autonomic nervous system controlled by the hypothalamus; stimulated in same manner as analgesic supraspinal effects.
• Choose large points of extremities and stimulate strongly for 20 to 40minutes
Checklist – what do you want?
• Peripheral effects?
• Segmental/spinal effects?
• Supraspinal effects?
• Sympathetic outflow?
• Central sympathetic effects?
• Immune effects?
• Bradnam L . A proposed clinical reasoning model for Western acupuncture J of AACP Jan 2007:21-30

31/07/2017
7
Layering Technique
Location of points needled
• Points distal to elbows and knees:
• Have a larger peripheral nerve plexus – less stimulation, stronger central response?
• Have a greater sympathetic innervation – more efficient at modulating response?
• More superficial (hands and feet) – connective tissue and periosteum stimulated - greater sensory input into the CNS?
• Concept of „Big Points‟ Bradnam L. A pathway of progression for Western acupuncture: Using the power of the brain. J of AACP July 2003:27-33
Classic Meridians
Ordinary
• Bladder
• Gall Bladder
• Stomach
• Spleen
• Liver
• Kidney
Extraordinary
• Governor Vessel
Extra
• Huatuojiaji
• Extra Back
• Lower Extremity
31/07/2017
8
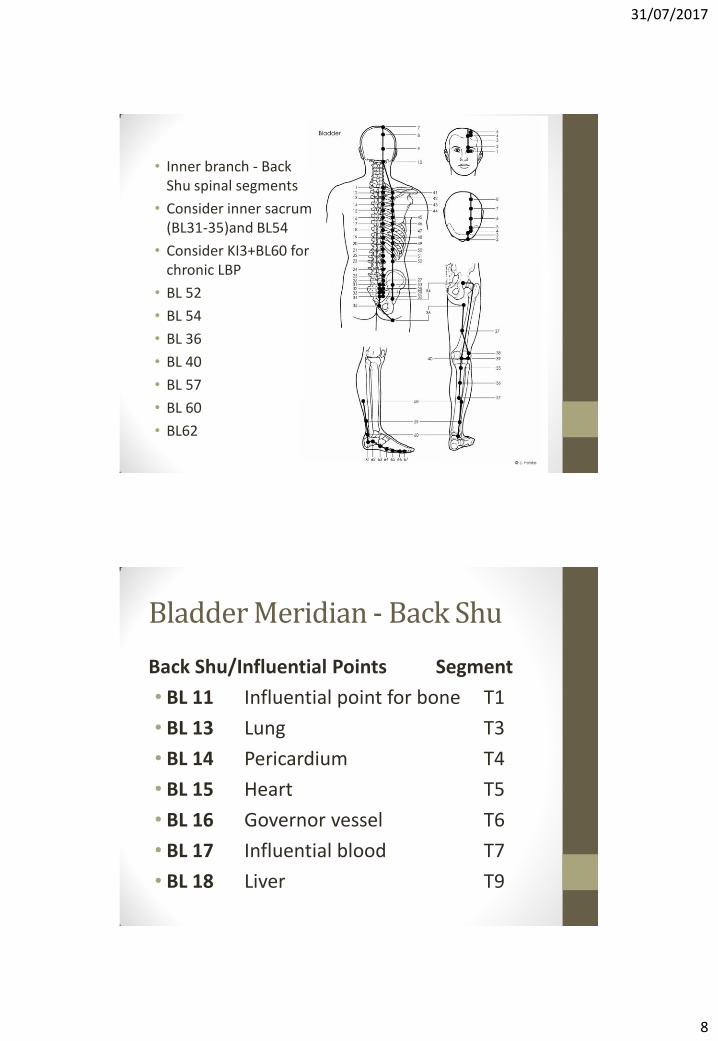
• Inner branch - Back Shu spinal segments
• Consider inner sacrum (BL31-35)and BL54
• Consider KI3+BL60 for chronic LBP
• BL 52
• BL 54
• BL 36
• BL 40
• BL 57
• BL 60
• BL62
Bladder Meridian - Back Shu
Back Shu/Influential Points Segment
• BL 11 Influential point for bone T1
• BL 13 Lung T3
• BL 14 Pericardium T4
• BL 15 Heart T5
• BL 16 Governor vessel T6
• BL 17 Influential blood T7
• BL 18 Liver T9
31/07/2017
9
• BL 19 Gallbladder T10 • BL 20 Spleen T11 • BL 21 Stomach T12 • BL 22 Triple Energizer L1 • BL 23 Kidney L2 • BL 24 Sea of Qi L3 • BL 25 Large Intestine L4 • BL 27 Small Intestine S1 • BL 28 Bladder S2
EX-B 2 Huatuojiaji 0.5 cun lateral to the lower border of the spinous processes T1-L5.
• T1-T3 HTJJ Points: disorders of the upper limbs.
• T4-T6 HTJJ Points: disorders of the HT.
• T7-T9 HTJJ Points: LV/GB issues.
• T10-T12 HTJJ Points: ST/SP issues.
• L1-L2 HTJJ Points: KD issues.
• L3-L5 HTJJ Points: UB, LI, SI, Uterine & Lower Limb issues.
• Consider C1-C7 options?
• Also EX-B 1 Dingchuan – “Stop Wheezing”
• 0.5 cun lateral to C7. Local point for neck, shoulder and upper back pain.

31/07/2017
10
• GV 3
• GV 4
• GB 29
• GB 30
• GB 31
• GB 33
• GB 34 as master point for connective tissues.
• GB 39
• GB 40
• GB 41
• GB 42

31/07/2017
11
• ST 30
• ST 32
• ST 34
• ST 35
• ST 36
• ST 41
• ST 42
• ST 44
• SP 3
• SP 4
• SP 5
• SP 6
• SP 9
• SP 10
31/07/2017
12
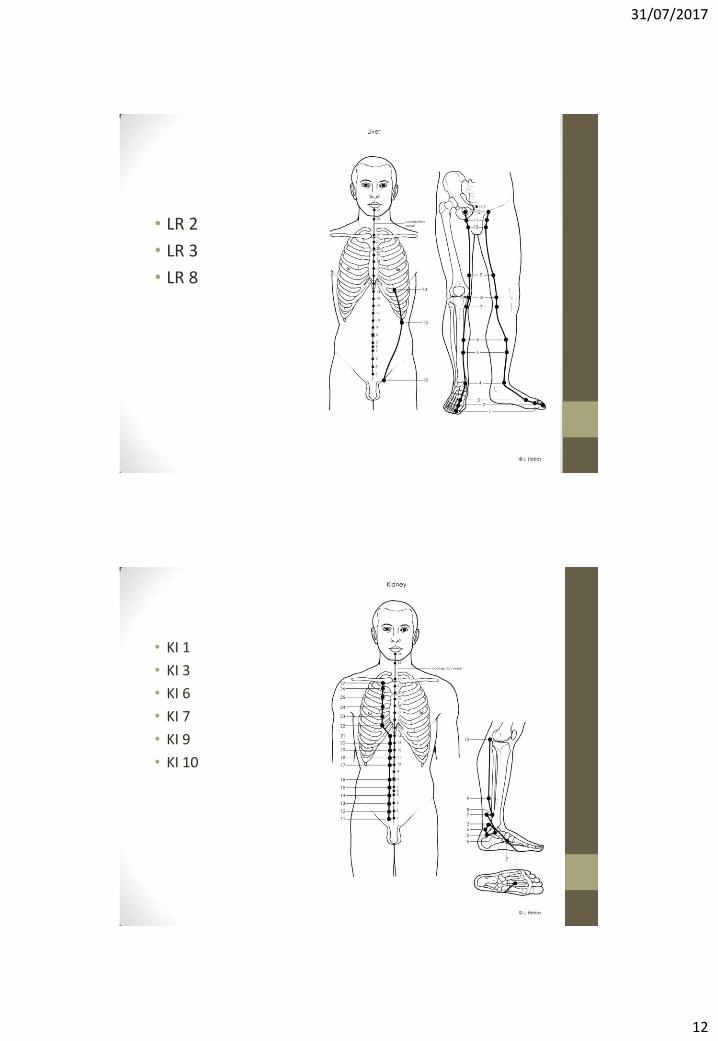
• LR 2
• LR 3
• LR 8
• KI 1
• KI 3
• KI 6
• KI 7
• KI 9
• KI 10

31/07/2017
13
Extra lower limb points
• EX-LE 2 Heding Lower extremity 2
• Location: Above the knee, in the depression of the midpoint of the superior patellar border. Needle perpendicularly 0.5 - 0.8 cun.
• Knee, leg and foot pain and weakness.
• EX-LE 4 Xiyan Lower extremity 4
• Location: Medial knee depression.
• Needle perpendicularly 0.7 – 1 cun.
• Knee pain and inflammation.
Extra lower limb points
• EX-LE 10 Bafeng Lower extremity 10
• Location: On the dorsum of the foot between the web and metatarsophalangeal joint (4 points on each foot). Needle obliquely and proximally 0.5 cun.
• Foot pain, swelling and numbness.
• LR 2, ST44, extra, GB 43

31/07/2017
14
Myofascial Trigger Points
• ‘‘a hyperirritable spot in skeletal muscle that is associated with a hypersensitive palpable nodule in a taut band’’ (Simons and Travell, 1999)
• 400 muscles all can develop MTrPs- referred pain and motor dysfunction (Simons et al, 1999).
• Active: Painful at rest, tender on palpation with referred pain pattern that replicates the patient’s pain
• Latent: do not cause obvious pain, may restrict movement or cause weakness or dysfunction
• Melzack (1977) reported a high degree (71%) of correspondence between MTrPs & acupuncture points.
• Referred pain distribution matching meridian?
• headaches - GB1-GB21
• All MTrPs may be Ah-Shi acupuncture points?
31/07/2017
15
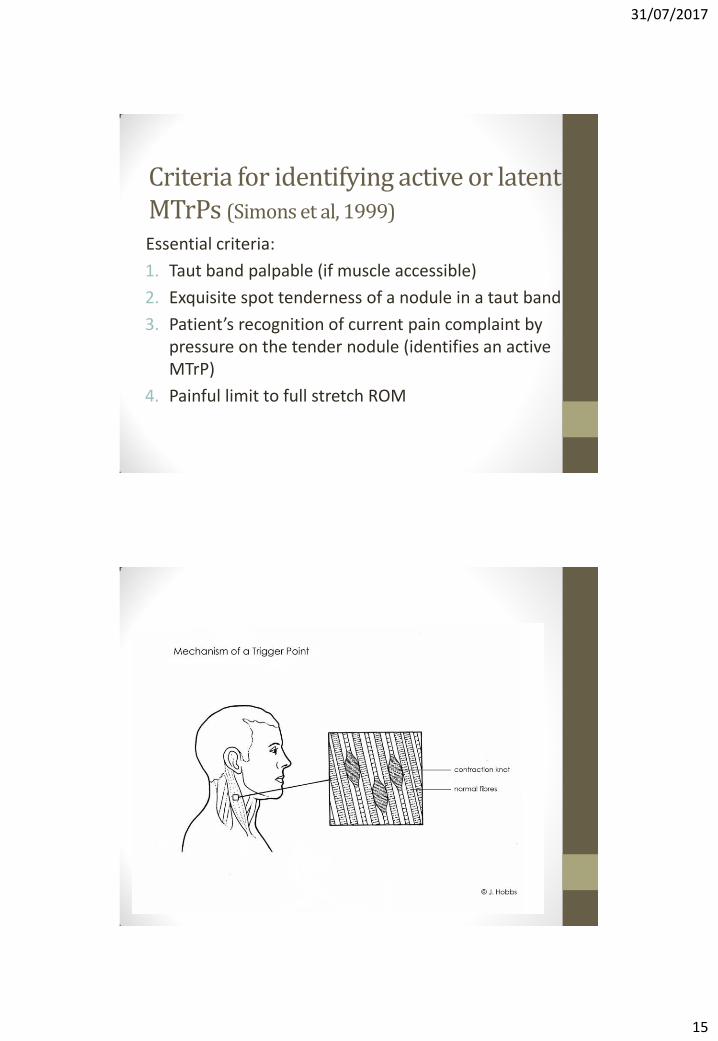
Criteria for identifying active or latent MTrPs (Simons et al, 1999)
Essential criteria:
1. Taut band palpable (if muscle accessible)
2. Exquisite spot tenderness of a nodule in a taut band
3. Patient’s recognition of current pain complaint by pressure on the tender nodule (identifies an active MTrP)
4. Painful limit to full stretch ROM
31/07/2017
16
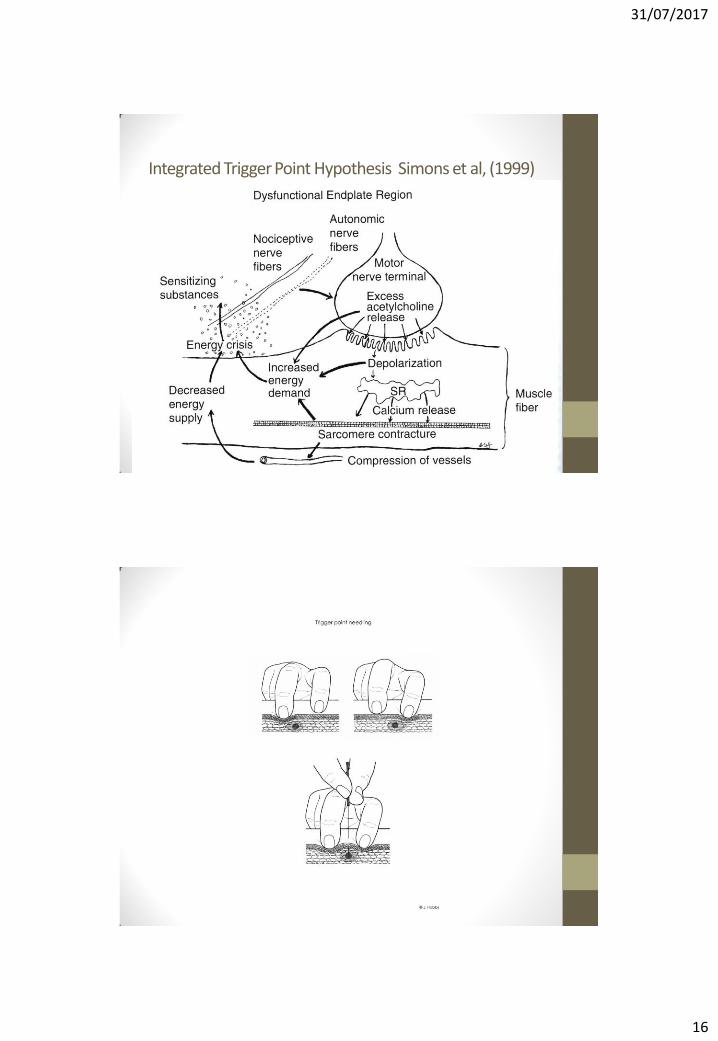
Integrated Trigger Point Hypothesis Simons et al, (1999)

31/07/2017
17
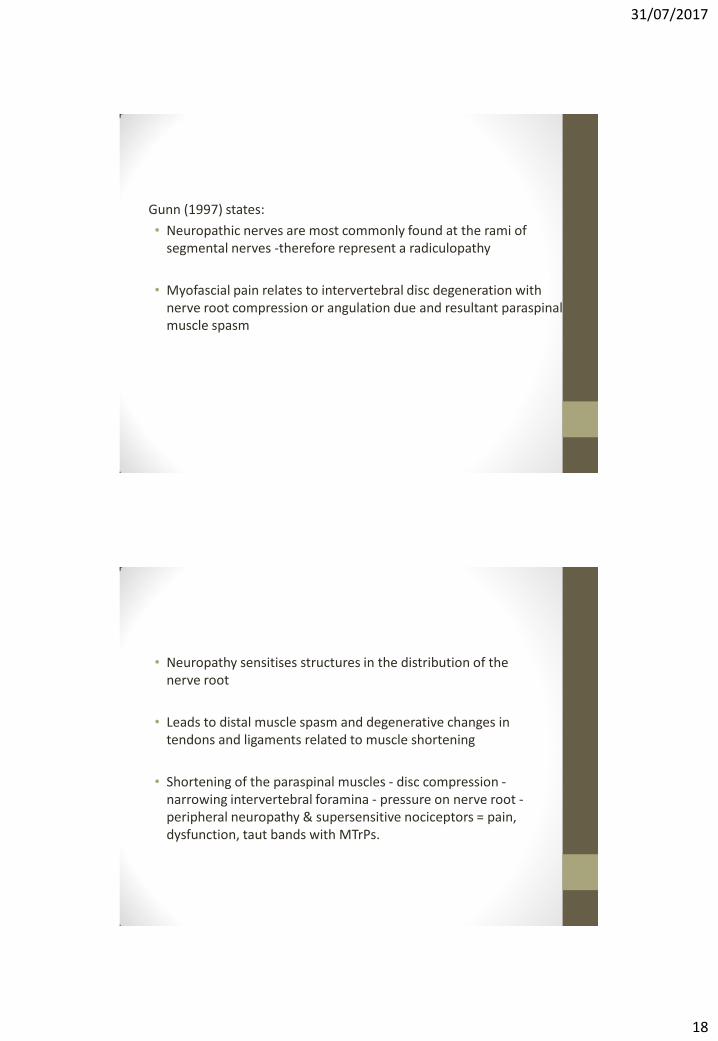
• Needle cause very small focal lesions (no risk of scar tissue formation)
• Needle diameter - 160-300μm (0.16mm-0.3mm)
• Muscle fibre diameter 10-100μm (Dommerholt et al., 2006).
• Muscle damaged - satellite cells are activated from other areas in the muscle to repair or replace damaged myofibres - muscle regeneration (Schultz et al, 1985).
• Process occurs 7-10 days (Schultz et al, 1985)
• Baldry (2005) recommends leaving the needle in situ for 30-60 seconds (may be up to 2-3 minutes?)
Radiculopathic Model for Muscular Pain • Gunn (1997) suggested a radiculopathic model for muscular pain
and states that;
“myofascial pain describes neuropathic pain that presents predominantly in the musculoskeletal system’
• Gunn (1997); Quintner and Cohen (1994) - proposes neurological cause as the primary stimulus and MTrPs as a secondary phenomenon
31/07/2017
18
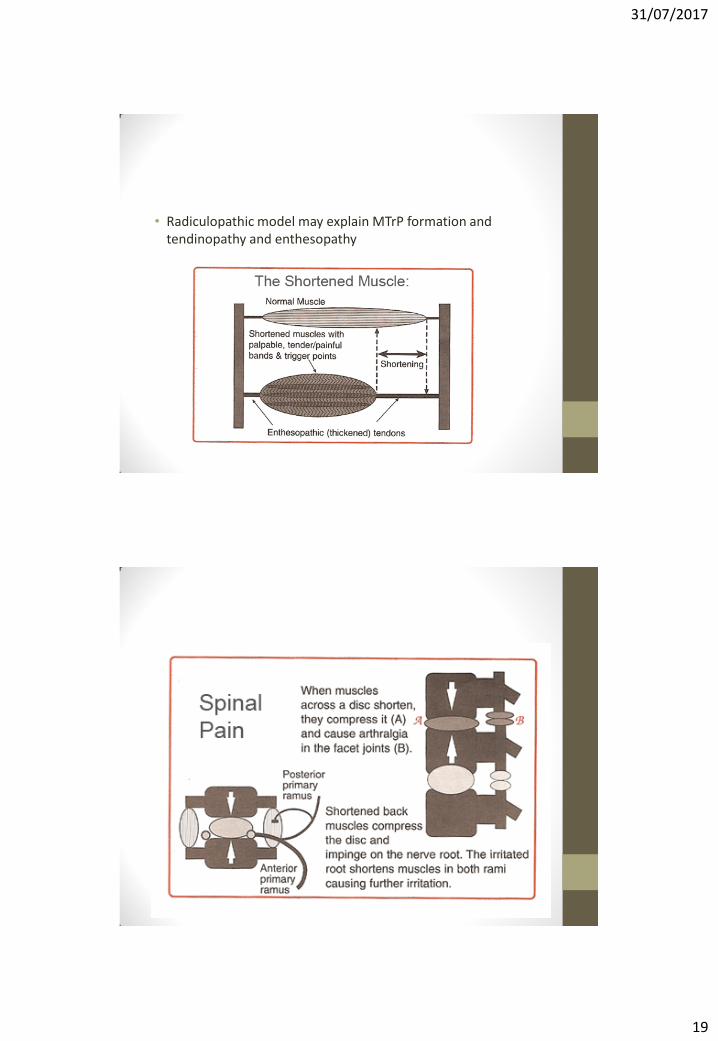
Gunn (1997) states:
• Neuropathic nerves are most commonly found at the rami of segmental nerves -therefore represent a radiculopathy
• Myofascial pain relates to intervertebral disc degeneration with nerve root compression or angulation due and resultant paraspinal muscle spasm
• Neuropathy sensitises structures in the distribution of the nerve root
• Leads to distal muscle spasm and degenerative changes in tendons and ligaments related to muscle shortening
• Shortening of the paraspinal muscles - disc compression - narrowing intervertebral foramina - pressure on nerve root - peripheral neuropathy & supersensitive nociceptors = pain, dysfunction, taut bands with MTrPs.
31/07/2017
19
• Radiculopathic model may explain MTrP formation and tendinopathy and enthesopathy

31/07/2017
20
• Long lasting pain relief requires needle treatment to the shortened paraspinal muscles to reduce nerve root compression & local trigger points (Gunn, 1997).
• Cannon and Rosenblueth’s Law of Denervation Supersensitivity states that “when a tissue is deprived of its nerve supply, it will develop hypersensitivity to its own neurotransmitter(s).”
• Cohen & Quintner (2008) suggest that with regards to trigger point theory;
“in the face of evidence of refutation’ we should ‘stop flogging a dead horse’ and reject the concept of MTrP pain as a clinical entity”
IMS concepts (paravertebral) Gunn
• Diagnostic tool
• Deep contractures beyond palpation
• Penetration of contracture: firm resistance, needle grasp, cramping/grabbing
• Fibrotic tissue: grating sensation (cutting a pear)
31/07/2017
21
Practice
Needle grasp:
• Provokes fasciculation and release quickly
• Shortened muscle grasps the needle.
• Grasp resists withdrawal.
• Leave in situ 10 to 30 minutes leads to release of persistent contracture.
• Failure (correctly placed needle) to induce needle-grasp - spasm is not present - not the cause of pain - not respond to this treatment.
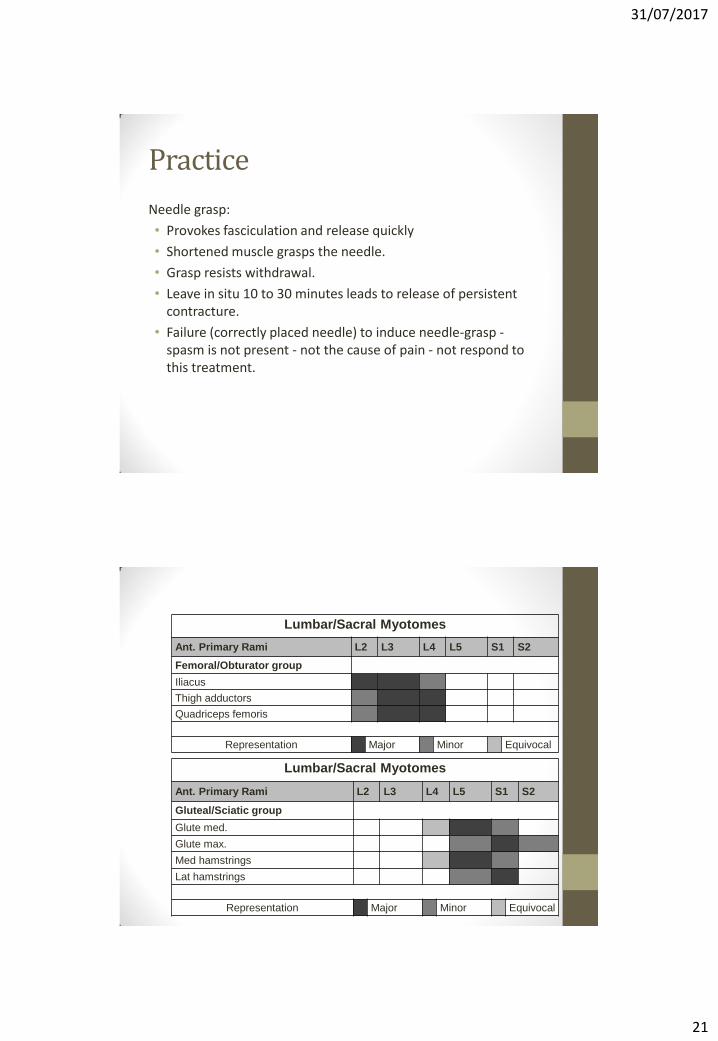
Lumbar/Sacral Myotomes
Ant. Primary Rami L2 L3 L4 L5 S1 S2
Femoral/Obturator group
Iliacus
Thigh adductors
Quadriceps femoris
Representation Major Minor Equivocal
Lumbar/Sacral Myotomes
Ant. Primary Rami L2 L3 L4 L5 S1 S2
Gluteal/Sciatic group
Glute med.
Glute max.
Med hamstrings
Lat hamstrings
Representation Major Minor Equivocal
31/07/2017
22
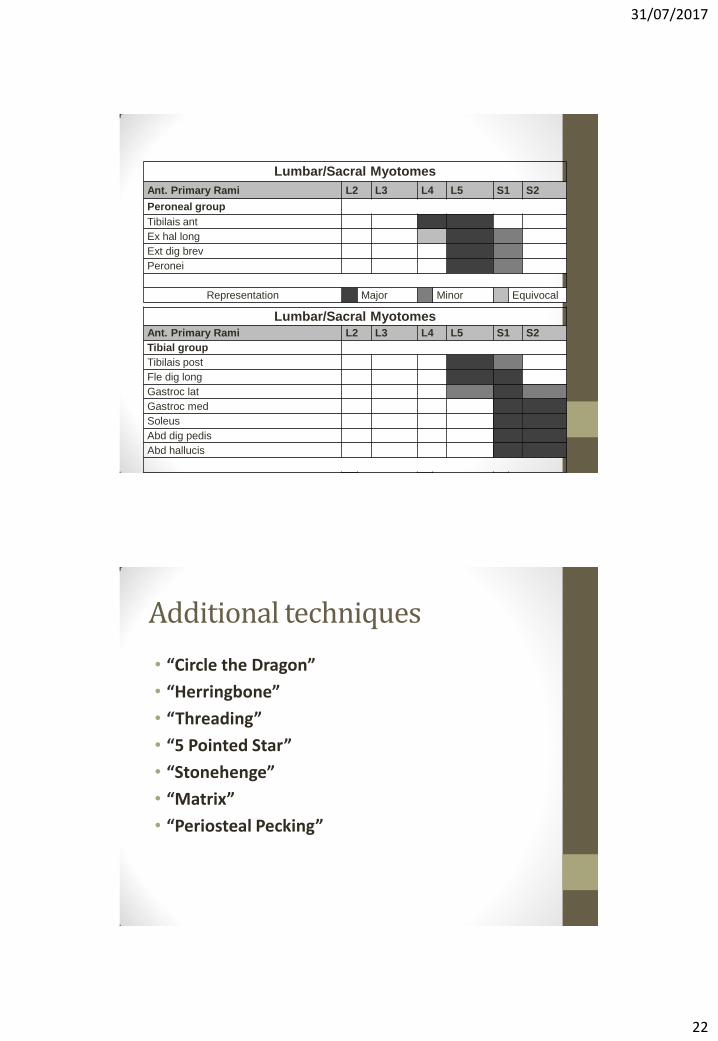
Lumbar/Sacral Myotomes
Ant. Primary Rami L2 L3 L4 L5 S1 S2
Peroneal group
Tibilais ant
Ex hal long
Ext dig brev
Peronei
Representation Major Minor Equivocal
Lumbar/Sacral Myotomes
Ant. Primary Rami L2 L3 L4 L5 S1 S2
Tibial group
Tibilais post
Fle dig long
Gastroc lat
Gastroc med
Soleus
Abd dig pedis
Abd hallucis
Representation Major Minor Equivocal
Additional techniques
• “Circle the Dragon”
• “Herringbone”
• “Threading”
• “5 Pointed Star”
• “Stonehenge”
• “Matrix”
• “Periosteal Pecking”

31/07/2017
23
Summary
• Layering
• Classic meridian points
• HTJJ- segments: local, visceral, referred, triggers
• Myofascial trigger points- local & spinal
• Consider Extra points & techniques
• Prescriptions/combinations
• Always: • Respect your client
• Respect the anatomy
• Respect the technique
References • Baldry P (2002) Management of myofascial trigger point pain. Acupuncture in
Medicine. 20(1), 2-10.
• Bradnam L (2003) A pathway of progression for Western acupuncture: Using the power of the brain. J of AACP July, 27-33
• Cohen M, Quintner J(2008) The horse is dead: let myofascial pain syndrome rest in peace. J. Pain Med. May Jun; 9(4): 464-5
• Dommerholt, J., Mayoral del Moral, P. T. and Grobli, C. (2006) Trigger Point Dry Needling. The Journal of Manual & Manipulative Therapy; 14(4): E70-E87.
• Gunn, C.,(1997) Radiculopathic pain: diagnosis and treatment of segmental irritation or sensitisation. Journal of Musculoskeletal Pain 5, 119–134.
• Keown, D (2013)What God forgot to tell surgeons: the science of acupuncture. Original Medical Publishing.
• Langevin, H. M., Churchill, D. L., Wu, J., Badger, G. J., Yandow, J. A., Fox, J. R. and Krag, M. H. (2002) Evidence of connective tissue involvement in acupuncture. Journal of the Federation of American Societies for Experimental Biology; 16: 872- 874.
31/07/2017
24
• Langevin, H (2008) Potential role of fascia in chronic musculoskeletal pain. In: Audette, J.F., Bailey, A. (Eds.), Integrative Pain Medicine: The Science and Practice of Complementary and Alternative Medicine in Pain Management. Human Press, Otowa, pp. 123–132.
• Ma, Y (2011) Biomedical acupuncture for Sports and Trauma Rehabilitation: Dry Needling Techniques. Churchill Livingstone. St Louis, Missouri.
• Melzack R, Stillwell DM, Fox EG (1977) Trigger points and acupuncture points for pain: correlations and implications. Pain 1977; 3: 3-23.
• Quintner, J., Cohen, M (1994) Referred pain of peripheral nerve origin: an alternative to the “myofascial pain” construct. The Clinical Journal of Pain 10, 243–251.
• Shang C (1989) Singular point, organizing center and acupuncture point. Am J Clin Med17:119–127.
• Shang C (1993) Bioelectrochemical oscillations in signal transduction and acupuncture: An emerging paradigm. Am J Clin Med ;21:91–101.
• Shang C (1995) Health indicators beyond the absence of disease. AMSA Task Force Quarterly, Fall, 22.
• Shang C (1999) Toward a unified theory of acupuncture and modern sciences. In: Handbook of Faculty Syllabus Materials for the 1999 Symposium. The American Academy of Medical Acupuncture, Los Angeles, 299–312.
• Shang, C (2001) The Journal of Alternative and Complementary Medicine. Volume 7, Number 1, pp. 83–91.
• Simons, D.G., Travell, J.G., Simons, L. (1999) Myofascial Pain and Dysfunction: The Trigger Point Manual. Williams & Wilkins, Baltimore.
• Vickers AJ, Cronin AM, Maschino AC, Lewith G, MacPherson H, Foster NE, Sherman KJ, Witt CM, Linde K, (2012) Acupuncture for Chronic Pain: Individual Patient Data Meta-analysis. Arch Intern Med Published Online September 10, 2012.
• Winfree AT (1984) A continuity principle for regeneration. In: Malacinski GM, ed. Pattern Formation. New York: Macmillan, 106–107.