access to health services − analyzing non-financial ... · ... planning, financing ... vietnam...
TRANSCRIPT

Access to health services − Analyzing non-financial barriers in Ghana, Rwanda, Bangladesh and Vietnam using household survey data A review of the literature
August 2013
Maternal, Newborn and Child Health
Working Paper
UNICEF Health Section, Program Division
unite for children

2
Access to health services − Analyzing non-financial barriers in Ghana, Rwanda, Bangladesh and
Vietnam using household survey data
A review of the literature
© United Nations Children’s Fund (UNICEF), New York, 2013
Knowledge Management and Implementation Research Unit, Health Section, Program Division
UNICEF
3 UN Plaza, New York, NY 10017
August 2013
This is a working document. It has been prepared to facilitate the exchange of knowledge and to
stimulate discussion. The findings, interpretations and conclusions expressed in this paper are
those of the authors and do not necessarily reflect the policies or views of UNICEF or of the United
Nations. The text has not been edited to official publication standards, and UNICEF accepts no
responsibility for errors.
The designations in this publication do not imply an opinion on legal status of any country or
territory, or of its authorities, or the delimitation of frontiers.
The editors of the series are Theresa Diaz and Alyssa Sharkey of UNICEF Program Division. For
more information on the series, or to submit a working paper, please contact [email protected] or
COVER PHOTO: Sirijganj, Bangladesh, © Juliet Bedford, Anthrologica

3
Access to health services – Analyzing non-financial
barriers in Ghana, Rwanda, Bangladesh and Vietnam
using household survey data
A review of the literature
Michael Thiede, Katharina C. Koltermann
Keywords: health system strengthening, district-level, district health system strengthening,
performance, planning, financing, performance-based financing, performance-based planning,
resource allocation, equity, universal health coverage, child health, health services, Ghana,
Bangladesh, Vietnam, Rwanda
Comments may be addressed by email to: Michael Thiede ([email protected])
cc: [email protected], [email protected]
MATERNAL, NEWBORN AND CHILD HEALTH
WORKING PAPER
August 2013

4
TABLE OF CONTENTS
ACKNOWLEDGEMENTS .......................................................................................................................... 5
EXECUTIVE SUMMARY ........................................................................................................................... 6
INTRODUCTION ...................................................................................................................................... 8
CONCEPTUAL FRAMEWORK................................................................................................................... 9
QUANTITATIVE APPROACHES .............................................................................................................. 11
QUANTIFYING NON-FINANCIAL BARRIERS TO ACCESS ......................................................................... 13
Information extracted from each article ....................................................................................... 15
Flowchart – Summary of literature screening ............................................................................... 15
FINDINGS .............................................................................................................................................. 16
Structuring the findings ................................................................................................................ 16
Bangladesh .................................................................................................................................... 16
Ghana ............................................................................................................................................ 32
Rwanda ......................................................................................................................................... 40
Vietnam ........................................................................................................................................ 42
DISCUSSION ......................................................................................................................................... 52
Barriers and survey data - limits of the data sources .................................................................... 53
Selected approaches - methodological constraints and pitfalls .................................................... 55
Policy implications of the findings ................................................................................................. 55
CONCLUSIONS AND RECOMMENDATIONS .......................................................................................... 55
REFERENCES ......................................................................................................................................... 57
APPENDIX ............................................................................................................................................. 61

5
ACKNOWLEDGEMENTS
The authors would like to thank Thomas O’Connell and Dr Martin Evans of UNICEF for their tireless guidance and support. The report benefited greatly from the exchange with Dr Juliet Bedford, team leader for the report “Access to health services: analyzing non-financial barriers in Ghana, Bangladesh, Vietnam and Rwanda using qualitative methods. A review of the literature”. Sincere thanks goes to Professor Di McIntyre, University of Cape Town, and Lara Brearley, Save the Children UK, for helpful comments and discussions. The authors would also like to express their thanks to Mary Kaltenberg, U.S. Fund for UNICEF, for her input into the literature search.

6
EXECUTIVE SUMMARY
This study forms part of a larger project designed to synthesize existing knowledge on the operationalization of equity as a central objective of universal health care (UHC). It aims to contribute to the development of an evidence-base for the formulation of equity goals, targets and indicators for children within UHC, and provides recommendations on embedding equity-focused indicators into multiple indicator cluster surveys (MICS). The findings of the study also serve to refine the diagnostic and monitoring and evaluation (M&E) components of UNICEF’s district health systems strengthening (DHSS) approach. The objectives of the structured literature review are to explore a) how non-financial barriers to the uptake of healthcare services in low-and middle-income countries are analyzed in studies applying primarily quantitative methods, b) which non-financial barriers to general and maternal and child health (MCH) services have been identified, and c) how access barriers have been contextualized. The study focuses on access barriers in four countries: Bangladesh, Ghana, Rwanda and Vietnam. A conceptual framework, building on the model by Frenz and Vega (2010), guides the presentation of findings and the deduction of policy recommendations. An access barrier is defined as a manifestation of a lack of fit between a potential health care need and the actual service designed to address that need. The relative significance of an access barrier depends on the socio-economic and socio-cultural position of the individual, household and community. The literature review is based on an online search using the databases PubMed, EconLit, PsycInfo, Sociological Abstracts and the International Bibliography of the Social Sciences (IBSS). A total of 1,188 articles were identified. After screening titles and abstracts, 83 publications remained for full text screening. After application of the exclusion criteria, 36 articles were carried forward for detailed review and the most important findings were extracted. All empirical research reviewed describes differences in health services utilization based on individual, household and community characteristics and emphasizes the demand-side of healthcare, rather than the supply-side. All studies focus on the uptake of services in the case of need and, therefore, only capture a proxy indicator of access. Study designs were guided by the variables captured in the household surveys and not explicitly designed to capture factors related to health services access. In this paper, factors or determinants are categorized into three groups: “predisposing”, “enabling” or “need" factors. The characteristics of the data sources, the methodological approaches of the quantitative studies and key findings are presented by country. The comprehensive structured overview sheds light on the nature of predisposing, enabling and need factors that shape access barriers. The findings clearly show that access barriers arise in particular contexts. Despite a lack of local data within the four countries, given the dominance of national level data sources, there is plenty of evidence demonstrating that local context matters. Rural-urban differences in MCH service utilization become most obvious in the Ghanaian studies. Beyond geographical differences, there are many local factors that give rise to access barriers, including those related to spatial and socio-cultural

7
differences. In Bangladesh and Vietnam the role of local context is clear as ethnicity and religious affiliation significantly influence health service uptake. The analysis of non-financial access barriers on the basis of national household surveys can only provide preliminary results to guide further quantitative or qualitative analysis at sub-national and sub-provincial levels. The literature review demonstrates that a) non-financial access barriers play an important role in explaining low service uptake; b) there are important predisposing, enabling and need factors that can be expected to vary widely according to local context; and c) factors interact in complex ways. This implies that targeted smaller scale surveys should routinely complement large scale surveys in order to identify access barriers and guide strategies to strengthen services at lower administrative levels. Many linkages between non-financial and financial barriers are apparent. There is a complex relationship between material circumstances, psychosocial conditions and behavioral factors. There are obvious limitations in the data sources underlying the reviewed studies; these are discussed. Furthermore, the quality of methodological approaches is variable, and there are considerable limitations to the use of quantitative tools exclusively in the analysis of access barriers. Within the same larger project, a parallel study with similar objectives, offers a review of qualitative research studies of non-financial barriers to access to health services. Wherever appropriate, this study refers to findings of the qualitative analysis. The qualitative research identified six analytical themes: perception of the condition; home management and local treatment; the influence of family and community; lack of autonomy and agency to act; physical accessibility; and health facility and biomedical deterrents. Conclusions and recommendations are largely based on the significance of local context. It is recommended that nationally standardized survey tools be systematically installed at the district level and implementation should initially focus on problematic geographic areas. Implementation should include routine monitoring and evaluation of the progress towards a reduction of access barriers and subsequent increases in service uptake; quick adaptations of strategies at the local level should be encouraged. The standardized toolkit should ideally employ a mixed methods approach. Standardization of the design and reporting of equity analyses using survey data should be developed in order to achieve comparability of findings, taking into account weaknesses in national-level household surveys, e.g. a shortage of economic variables. Furthermore, future operational research should be directed at the development of a comprehensive approach to analyzing financial and non-financial barriers simultaneously, taking into account the complex interrelationships within and between dimensions of access. The review emphasizes the importance of health information to empower individuals, and in particular, the need for context-specific communications to reduce access barriers and strengthen health services at the local level.

8
INTRODUCTION
The complex set of barriers to attaining universal health coverage (UHC) is poorly understood. This is particularly true for non-financial barriers not related to direct and indirect health service costs, and the complex relationships between financial and non-financial barriers. Unless approaches for identifying and understanding access barriers are used to inform and support equity-focused health services, UHC with equity can hardly be achieved. Different quantitative and qualitative approaches have been applied to study determinants of health service access and utilization. Strategies and policies that are based on the analysis of available data are limited due to the complexities of analyzing access barriers. A feasible and contextually appropriate approach to assessing access barriers included under national UHC policies requires a thorough qualitative and quantitative methodological framework and must rely on suitable data in terms of scope, currentness and representativity. This study forms part of a larger project designed to synthesize existing knowledge on the operationalization of equity as a central objective of universal health care (UHC). It aims to contribute to the development of an evidence-base for the formulation of equity goals, targets and indicators for children within UHC, and to the development of recommendations on how to embed equity-focused indicators into multiple indicator cluster surveys (MICS). The findings also serve to refine the diagnostic and M&E components of UNICEF’s DHSS approach. Within the same larger project, a parallel literature review study with similar objectives, examines non-financial barriers to access to health services based on qualitative research (Bedford et al. 2013). Wherever appropriate, this study refers to findings of the qualitative analysis. In December 2012, the UN General Assembly adopted a consensus on UHC and encouraged governments to pursue the transition towards universal access to affordable and quality health care services. Equity, which lies at the heart of UHC, is reflected in access to appropriate health services of sufficient quality. The provision of health services is considered inequitable if access to health care differs between people with different characteristics. Such characteristics include gender, age, socio-economic status, culture or place of residence within a country. Thus, access to health care is a phenomenon dependent on several dimensions and is frequently exacerbated by barriers or bottlenecks with particular relevance for certain population subgroups. In the past, the main focus has been on economic or financial barriers to health services utilization. Financial burdens associated with the uptake of health services are often causal for under-utilization, treatment delays, as well as for seeking the wrong treatment. Consequently, the World Health Organization (WHO) and others have emphasized the need to provide quality health services that do not create financial burdens. Health care affordability, as defined by the relationship between the actual costs of health care and the patient’s economic position, constitutes only one dimension of access. This dimension has been analyzed across countries in studies highlighting different components, such as user fees, that contribute to the financial burden of illness and health services utilization. Other components include transport costs to distant facilities and indirect costs. In terms of health services uptake,

9
the quantitative analysis of large-scale household surveys across the globe consistently illustrates the impact of socio-economic status and service costs. More recently, social determinants of health research has led to increased attention paid to access dimensions beyond economics. Non-financial barriers have been identified as significant constraints to equitable access of the full range of health services included under national UHC policies (O’Connell 2012). Such non-financial barriers include a broad set of conditions including lack of citizenship, ethnicity, gender, political affiliation, and other socio-cultural factors. Whilst awareness of the relevance of these factors has grown, their role and relative contribution have neither been systematically explored, nor monitored. In addition, methods for assessing non-financial access barriers are not well developed. Non-financial barriers often arise locally. If they can be identified and the underlying factors are monitored, the findings can be used to improve local policies, strengthen district health systems and inform national UHC policies to narrow access disparities. This work aims to synthesize and critique existing evidence on quantitative models of monetary and non-monetary barriers to the uptake of healthcare services, and the contribution of research to understanding how equitable progress towards UHC can be facilitated. It highlights critical points and lessons learnt that emerge from the literature. Different approaches to using quantitative data to assess non-financial barriers to health services utilization are discussed, taking into account both national and sub-national levels. Research strengths and weaknesses are evaluated and recommendations are provided on applying findings to strengthen district health services. The structured literature review focuses on four countries: Ghana, Rwanda, Bangladesh and Vietnam. These countries were previously studied in a UNICEF-Rockefeller Foundation project assessing national health insurance in Africa and Asia (O'Connell 2012), which included in-depth case studies. In addition, UNICEF and the Rockefeller Foundation have a strong presence in these four countries, enabling support where needed for this project. Both organizations are also working in these countries to develop an evidence base for equity goals, targets and indicators for children within UHC. The research analysis was dependent on the availability of adequate data. In the case of Rwanda, few relevant research studies exist although it is considered an important country in terms of its role in UHC research and its commitment to achieving UHC goals.
CONCEPTUAL FRAMEWORK
Advancing towards UHC implies reorienting services and structures within existing health systems to align them with strategies for achieving the goal. Equity in financing and in the delivery of services are important milestones in the establishment of UHC (Frenz and Vega 2010). Equal access to health services for people whose health care needs are similar can be regarded as an established principle of health equity (Oliver and Mossialos 2004). However, beyond this principle, the health equity debate has not succeeded in presenting a single operational definition of access

10
to health services. There is, nevertheless, a general understanding that any conceptualization of access needs to consider different dimensions. Tanahashi (1978) promoted a comprehensive view of health service coverage that includes the ability of a health service to interact with the target population. Tanahashi’s work constitutes a centerpiece for the conceptualization of equity and access in the context of UHC, as it elegantly links the different concepts. Tanahashi’s model, which has been integrated into a UHC framework of equity by Frenz and Vega (2010), distinguishes between service capacity or potential coverage and service output or actual coverage. The relationship between the two is defined by service utilization. The model assumes five successive stages towards a “desired health intervention” and defines measures of coverage: the availability of resources (manpower, facilities, drugs, etc.), coverage accessibility, coverage acceptability, contact coverage (people who have “contacted” the services as a share of the target population), and effectiveness coverage (indicating that the quality of the intervention was sufficient to achieve the desired outcome or impact). Whereas Tanahashi’s model leads the way towards the analysis of equity and health service coverage, the default order in which it regards the different stages or dimensions appears unnecessarily limiting. There is widespread agreement within the research community that the dimensions of access comprise the affordability, availability, accessibility and acceptability of services, even if these dimensions cannot always be clearly delineated. While such headings include different aspects, it is important to acknowledge that there are sets of factors which describe the relationship of the health system and the target groups and which determine access to effective health care. These factors can be grouped into “dimensions” with multiple underlying layers, characterized by interdependencies and grounded in root causes (McIntyre et al. 2009, Thiede et al. 2007). It is useful to distinguish access from utilization and regard access as the state of an individual’s empowerment to use health services following an informed decision (McIntyre et al. 2009, Thiede 2005). Equitable access can only be achieved if all dimensions of access are addressed, taking into account both the health care system and individual perspectives. In assessing what infringes on access, it is important to consider the relational and bidirectional nature of the dimensions of access (Thiede et al. 2007). Access dimensions can only be interpreted in relation to both the health system and its targeted users, e.g. affordability differs for a potential user from a high-income household as compared to a low-income user. And, acceptability of a service may change depending on the patient’s cultural background. In this project, a barrier is defined as a manifestation of a lack of fit between a potential healthcare need and the actual service to address that need. A barrier is not absolute or static, but is dynamic; and can manifest in multiple ways. The relative significance of an access barrier depends on the socio-economic and socio-cultural position of the individual, household, and community. In fact, the position itself can be regarded as a barrier. Barriers are located at the interface of the health delivery system and its target population. They can occur at any point in the relationship, i.e. towards the delivery system (e.g., an infrastructure issue) or closer to the target population (e.g., cultural characteristics of a subgroup). Service

11
quality and appropriateness are critical for equitable health outcomes. Removing barriers in a way that reduces inequities amongst various sub-populations is a policy challenge, yet a precondition of equitable UHC. This study takes a broad view in investigating barriers to access. As indicated above, there are interdependencies between access dimensions and barriers. The experience of specific barriers is circumstantial and subjective. As Joseph and Poyner (1982) point out, both consumer and facility attributes interact to produce different reactions from different persons. In health equity research and policy debates, attention has largely been focused on financial barriers. Research findings on affordability have greatly influenced health financing discussions and shaped the debate around user fees. Given the interdependencies of access dimensions, financial and non-financial barriers to access cannot be viewed in complete separation. As indicated in the framework applied by Frenz and Vega (2010), a population subgroup’s resources and capabilities are characterized by the interdependence of human, social and financial capital. Assessment of these resources requires new instruments and a challenge lies in developing a methodological framework to examine the interdependent spheres and related dimensions of access. This study identifies barriers reported in the literature that documents the analysis of household surveys. It places a particular focus on the interconnectedness of barriers in order to guide future analyses of household surveys, inform health policy, and strengthen health systems at the district level.
QUANTITATIVE APPROACHES
Over the past decade, quantitative approaches to measuring health equity and access to health services have developed rapidly and been widely applied. In a seminal volume summarizing quantitative techniques (O’Donnell et al. 2008), the authors cite reasons why (quantitative) health equity research has become an increasingly popular topic since the mid-1980s. In addition to the increased demand from policy makers, donors, and NGOs, they emphasize the availability of suitable household data sets, computing power and a growing number of analytic techniques to quantify health inequities.1 A key driver of this research stream has been the ECuity project, a multi-country, EU-funded research project focused on health care finance equity and delivery, as well as income-related health inequalities. The ECuity project has led the methodological debate and produced important comparative studies across OECD countries for 20 years.2 Their research toolkit has been refined
1 The World Bank has recently developed an easy-to-use software platform for applied economic analyses, ADePT (Automated
Development Economics [DEC] Poverty Tables) to simplify and streamline the analysis of survey data. The publicly available tool is
based on Stata statistical software. It allows the quick generation of summary statistics and charts as well as small-scale analyses of
equity issues both in health financing, e.g. progressivity analysis or the analysis of catastrophic expenditure, and in health
outcomes, e.g. benefit incidence analysis (Wagstaff et al. 2011). 2 The project is documented at http://www2.eur.nl/bmg/ecuity/.

12
and applied to low and middle-income contexts since the early 2000s. For example, a multi-country study in Asia assessed households’ ability-to-pay, health financing contributions and presented concentration indices across Asian countries. Results indicated that better-off households were characterized by higher health expenditure than poorer ones, and they consume significantly more health care (O’Donnell et al. 2008). A study from Bangladesh suggests the use of benefit incidence analysis and sequential sampling techniques for monitoring utilization of health services by the poor (Bhuiya et al. 2009). The analysis of quantitative health research (individual and household-level) to inform health policy in low and middle-income countries gained momentum with the introduction of the Demographic and Health Survey (DHS) program by the United States Agency for International Development (USAID) in 1984. DHS are nationally representative household surveys with a standardized core questionnaire allowing for cross-country comparisons of indicators. So far, approximately 260 DHSs have been conducted in over 90 countries. Analyses of DHS from different perspectives have informed public health and health systems research and informed policy choices. The focus of DHS is on health care use and health status of women of childbearing age (ages 15-49) and their children. The surveys collect information on health-related issues such as fertility, fertility rate, reproductive health, maternal health, child health, immunization and survival, HIV/AIDS, maternal mortality, child mortality, malaria, and nutrition among women and children. The women’s questionnaire is complemented by a household questionnaire. Due to the observation that health care utilization is considerably higher among wealthy groups, while need is higher among the poor, there has been a range of studies examining the affordability dimension of access across countries on the basis of DHS data over the past decade. Although the DHS focuses on health issues, and is not designed to capture a broad range of socioeconomic and sociocultural variables, the questionnaires include background characteristics useful to analyze socioeconomic determinants of service utilization and health. Household characteristics captured in the questionnaire, including the household’s water source, type of toilet facility, access to electricity, building materials, and asset ownership, have been used to develop an indicator of household wealth and socioeconomic status. Using principal component analysis (PCA), such an asset index can easily be generated to assign households to socioeconomic quantiles (Filmer and Pritchett 2001). This approach has expanded DHS data analysis to address economic access barriers. The household questionnaire captures general household characteristics, education, water and sanitation and may include modules related to particular health topics, such as malaria. The women’s questionnaire focuses on the woman’s background, access to media and a range of topics around maternal, newborn and child health and sexual behavior. UNICEF’s multiple indicator cluster surveys (MICS) have been developed to provide rigorous data on women’s and children’s health and have been conducted (or are scheduled to be conducted) in 112 countries since the mid 1990s. The survey has been subject to several rounds of revision, is comparable to the DHS, and typically consists of three components: a household questionnaire, a women’s questionnaire and a child (under 5 years) questionnaire. The under-five questionnaire examines birth registration, anthropometry, early childhood development, breastfeeding, health

13
care and illness, as well as immunization. Both the latest version of DHS and the MICS permit analysis of sub-national patterns of access in a number of countries, at least at the state or provincial level. WHO’s World Health Survey (WHS), developed in individual countries involving routine health information systems, collects baseline information on population health and evidence on inputs, functions and outcomes of health systems. A survey of adult individuals selected randomly from a nationally representative sample of households forms the core of the WHS. While the content of questionnaires varies across countries, in principle, it includes general household information, income and household expenditures (including health expenditures), health insurance status and individual variables covering health state valuations, risk factors and health system responsiveness. Country-specific WHSs have been widely used in public health research. Living Standards Measurement Study (LSMS) surveys, established by the World Bank as multi-topic surveys in the early 1980s, have also played a role in quantitative analyses of access to health care. Designed to allow analyses of living standards and poverty, the impact of policies and government programs on welfare, they contain a health module that captures health expenditure and utilization of health services. While the health section of the LSMS is not as specific as in the aforementioned surveys, it allows analyses of health-related behaviors in a socioeconomic context. Innovative studies on the interrelationship of socioeconomic status and health expenditure, i.e. the affordability dimension of access, have been conducted using data from LSMS surveys (e.g. Wagstaff and van Doorslaer 2003). As has been demonstrated in analyses comparing results from different survey types there is a need to further harmonize methods and standardize questions on health service uptake and household health expenditures across types of internationally conducted, large household surveys in order to achieve valid and reliable results (Lu et al. 2009; Xu et al. 2009) An important consideration in the context of this study is the scope and quality of available data sources. Health equity analysis requires health-related variables, as well as demographic and socioeconomic variables. Whereas wealth, income and expenditure data are easily definable and financial access barriers straightforwardly delimitable, non-financial barriers are not easily identified and measured. Research agendas may in turn be limited by the deficiencies of non-financial survey data.
QUANTIFYING NON-FINANCIAL BARRIERS TO ACCESS
This study uses a structured literature review to explore, a) how non-financial barriers to the uptake of healthcare services in low-and middle-income countries are analyzed in studies applying primarily quantitative methods, b) which non-financial barriers to general health and maternal and child health services have been identified by the studies, and c) how the identified access barriers have been contextualized. The literature search was conducted online, using the database PubMed, American Economic Association's electronic bibliography (EconLit), PsycInfo, Sociological Abstracts and the
14
International Bibliography of the Social Sciences (IBSS). Including databases focusing on different social sciences enabled a comprehensive collection of literature on this interdisciplinary topic. For the initial search the following inclusion criteria were defined:
Study language was English
Date of publication was between 1st January 2000 and 31st December 2012
Study was carried out in Bangladesh, Vietnam, Ghana or Rwanda
The publication reported quantitative data (derived from surveys or comparable sources)
The paper was published in a peer-reviewed academic journal, book, or publicly available report (e.g. available dissertations)
These criteria constituted the basis of the search strings used to browse the above-mentioned databases. Besides the focal regions and the defined time horizon, health service accessibility was included in the search strategy. Key words such as cross sectional or health care surveys were embedded in the search to better carve out the applicability of existing survey data within the context of the study question.3 The search strings were refined for each source depending on the database requirements. After searching the databases, a four-step screening method identified those publications deemed relevant and studies were excluded if, (i) a wrong study type was used (e.g. an epidemiological or predominantly qualitative study), (ii) the research focused exclusively on finance, financial access barriers or health insurance, (iii) if the main focus was not on a health service, or (iv) if not the correct geographical region. The inclusion/exclusion criteria were formulated to support the study objectives and go beyond the general discussion of affordability and financial barriers. The study selection process is described below, including a flow chart of the filtering process. Step 1 The results identified by the initial database searches were combined. In total, 1,188 articles were identified and 96 were duplicates and excluded. Step 2 Two researchers independently analyzed each of the 1,092 papers by title and abstract. The researchers graded every publication as strong inclusion, weak inclusion or exclusion and each were discussed in detail until consensus was achieved. A total of 1,009 articles were excluded because they failed to meet the inclusion criteria resulting in 83 articles. Step 3 The full text of the remaining 83 publications was reviewed for eligibility and inclusion agreed upon by consensus resulting in exclusion of 47 articles. Articles were removed because they were the wrong type of study, e.g. a predominately qualitative analysis (21 articles), focused on the wrong question, e.g. focused exclusively on finance, on financial access barriers or showed a
3
The refined search strings are presented in the Appendix.

15
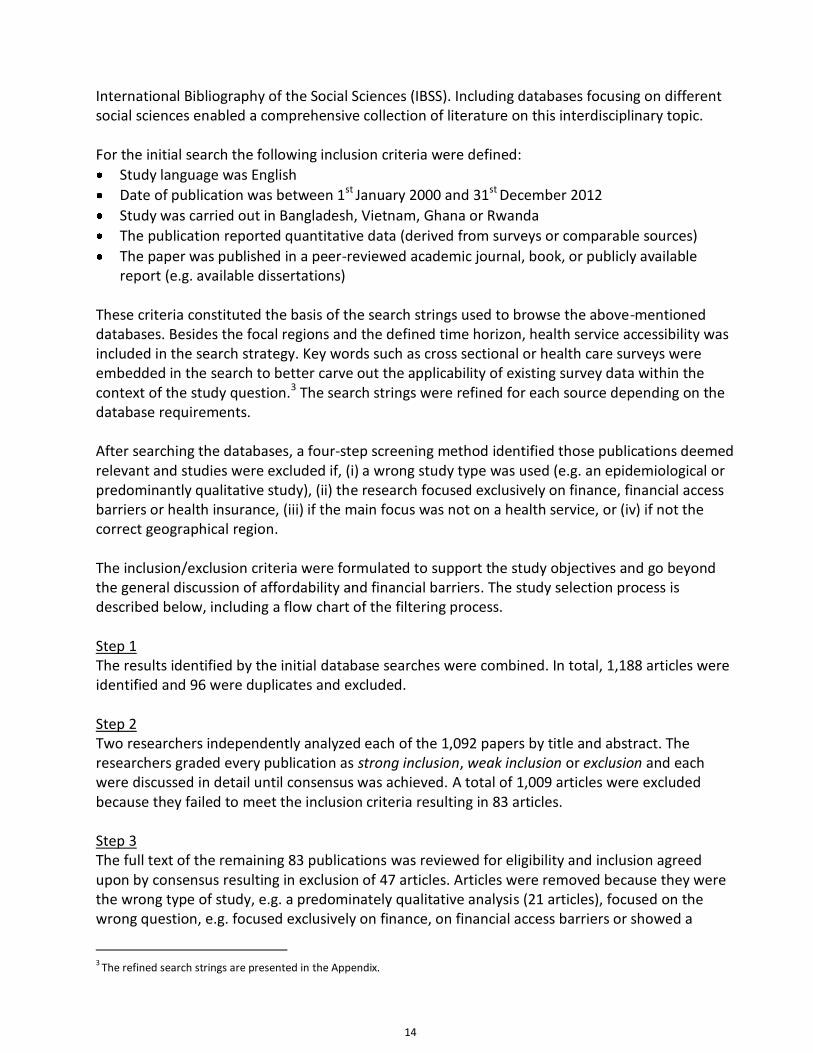
health insurance focus (25 articles) or full text was not available (1 article: a conference paper). In total, 36 articles were carried forward for detailed review and the most important findings were extracted. Snowballing and forward citation did not yield any additional studies. Step 4 The key findings relating to non-financial barriers and to methodological implications were extracted in the form of a tabular synopsis for each country (Tables 1-4). This study highlights maternal and child health (MCH) services. Since most publications identified in the search strategy addressed MCH services, it was not necessary apply additional filters, and the few non-MCH studies were included in the final analysis. Information extracted from each article The extraction of information from the eligible papers was guided by the research objectives. A tabular synopsis presents the most relevant information from the literature in a comprehensible and unified way. The synopsis tables include general information about each paper: author, year, type of health service in focus, target population and the main study question. Study design information includes the data and methodology used by each study, short description of the data source (type and name of survey, time of the survey, study population) and the specific econometric approach. While all studies included in the review have been properly conducted and well presented, the methodological approach was rated as either high quality (++) or acceptable quality (+), indicating both the appropriateness of the model, as well as the presentation. A high quality study is usually characterized by the presentation of a well-defined underlying model or conceptual framework and methodological rigor that acknowledges limitations and biases. A second table for each region includes the types of barriers identified or the different determinants of treatment seeking behavior reported by each study. Finally, the main results and conclusions are summarized.
Articles identified: 1,188 PubMed 643 EconLit 137 SocAbstr 55 IBSS 68 Psycinfo 285
Screened by title and abstract: 1,092
Duplicates removed: 96
Flowchart – Summary of literature screening
Screened by full text: 83
Articles included in final review: 36
Excluded articles: 1,009
Excluded articles: 47

16
FINDINGS
Structuring the findings The empirical research reviewed describes differences in health services utilization based on individual, household and community characteristics and emphasizing the demand-side, rather than the supply-side. All studies focus on the uptake of services in the case of need and, therefore, only capture a proxy indicator of access. Study designs were guided by the variables captured in the household surveys and not explicitly designed to capture factors related to health services access. Building on the conceptual work of Andersen and Newman (1973), factors or determinants are categorized into three groups: “predisposing”, “enabling” or “need" factors. However, in some cases, characterization of factors is not consistent in the literature. For example, education can be designated as either predisposing or enabling. In this report, education, place of residence and wealth are all considered enabling factors. Predisposing factors are individual characteristics and health beliefs that determine the likelihood of health service uptake and are demographic and socio-structural in nature. These types of factors are unlikely to be changed by social action and include age, gender, ethnicity and religion. Enabling factors are individual or household characteristics that play a role in empowering a person to make autonomous decisions about health services. Few studies analyze interactions between explanatory variables. One exception is the study by Young and colleagues (2006) who analyze the interactions between predisposing and enabling factors, but provide little interpretation of the results. Findings are presented separately for each country. Whilst the four countries exhibit many commonalities, in terms of the determinants of health services uptake and barriers perceived by vulnerable groups, there are peculiarities that warrant a country-specific separation of findings. In the first section of the analysis, studies are described for each country, indicating the data source, population, type of health care service, and type of data analysis. Additionally, any unique research approaches were described. The second section focuses on access barriers identified in each country and the findings are grouped into predisposing or enabling factors. Bangladesh For Bangladesh, nineteen articles were identified for detailed review (Table 1a). This was the largest number of eligible publications for any of the four countries. Of these articles, five studies assessed the general population, five focused on children, one on adolescents, two on adults, three on women and their children, and two articles exclusively on women. MCH services were the topic of fourteen studies and the utilization of general health services was assessed in three articles (Ahmed et al. 2001, Uddin et al. 2009, Young et al. 2006). One publication (Ahsan et al. 2004) addressed Tuberculosis (TB) treatment. The oldest study (Ahmed et al. 2001) analyzed data from 1988, and the most recent survey data was from 2007/2008 (Uddin et al. 2009). Six of the reviewed studies (Chowdhury et al. 2007, Kamal 2009, Rahman et al. 2012, Reynolds et al. 2006, Senarath & Guanawardena 2009, Story and Burgard 2012) used the Bangladesh Demographic Health Survey (BDHS) as data source (different years). Two studies (Alam et al. 2009, Young et al 2006) used the Matlab Health and Socioeconomic Survey (MHSS) 1996.

Tab
le 1
a:
Ban
glad
esh
- e
ligib
le p
ub
licat
ion
s an
d s
tud
y d
esig
ns
A
uth
or
Serv
ice
Targ
et
Stu
dy
Qu
esti
on
s D
ata
sou
rce
Po
pu
lati
on
Ti
me
An
alys
is &
Qu
alit
y
Ah
me
d
(20
01
) G
ener
al s
ervi
ces
(5
typ
es o
f p
rovi
der
s)
Gen
eral
p
op
ula
tio
n,
Ch
itta
gon
g H
ill
Trac
ts
Mo
rbid
ity
pre
vale
nce
, illn
ess
pro
file
s an
d h
ealt
h-
seek
ing
beh
avio
r o
f d
iffe
ren
t e
thn
ic
gro
up
s
BR
AC
su
rvey
o
f 5
eth
nic
gr
ou
ps
2.5
50
ho
use
ho
lds
inte
rvie
wed
, 5 s
elec
ted
et
hn
ic g
rou
ps
(min
. p
op
ula
tio
n o
f 2
0.0
00
)
19
98
B
ivar
iate
an
d
mu
ltiv
aria
te a
nal
ysis
(+
)
M
eas
ure
d o
utc
om
es:
Co
mm
on
ly o
ccu
rrin
g ill
nes
ses,
nu
trit
ion
of
6-5
9 m
on
ths
old
ch
ildre
n, a
vaila
ble
hea
lth
care
pro
vid
er, d
ista
nce
of
nea
rest
sta
tic
hea
lth
fac
ility
, hea
lth
-see
kin
g b
ehav
ior
(fir
st c
on
tact
)
Ah
san
et
al.
(20
04
) Tu
ber
culo
sis
trea
tmen
t A
du
lts
wit
h T
B
Gen
der
dif
fere
nce
s in
ep
idem
iolo
gica
l fa
cto
rs a
sso
ciat
ed
wit
h t
reat
men
t se
ekin
g b
ehav
iors
Cas
es f
rom
11
ru
ral u
pze
la
hea
lth
ce
nte
rs
(UZH
Cs)
an
d 1
co
mm
un
ity
(Dat
tap
ara)
in
Gaz
ipu
r d
istr
ict.
30
7 a
du
lts
No
t re
po
rted
M
ult
iple
logi
stic
re
gres
sio
n
(+)
M
eas
ure
d o
utc
om
es:
Tre
atm
ent
seek
ing
beh
avio
r
Ala
m e
t al
. (2
00
9)
Ch
ildh
oo
d a
nd
infa
nt
hea
lth
C
hild
ren
un
der
ag
e 1
5
Ass
oci
atio
n o
f so
cial
, ec
on
om
ic a
nd
oth
er
fact
ors
wit
h
per
ceiv
ed m
orb
idit
y an
d u
se o
f h
eal
th
serv
ices
by
rura
l ch
ildre
n.
Ban
glad
esh
: H
ealt
h a
nd
So
cio
eco
no
mic
Su
rvey
co
nd
uct
ed in
M
atla
b 1
99
6
(MH
SS)
3,7
98
ch
ildre
n
19
96
Lo
gist
ic r
egre
ssio
n
(+)
M
eas
ure
d o
utc
om
es:
Use
of
any
hea
lth
pro
vid
er, d
oct
ors
, par
amed
ics
or
ho
meo
pat
hs

1
8
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Ari
fee
n e
t al
. (2
00
8)
Ch
ildh
oo
d a
nd
in
fan
t h
ealt
h
Ch
ildre
n u
nd
er
age
5
Rat
es a
nd
d
iffe
ren
tial
s b
y se
x an
d s
oci
oec
on
om
ic
stat
us
for
3 a
spec
ts
of
child
hea
lth
m
orb
idit
y an
d
ho
spit
aliz
atio
ns,
in
clu
din
g se
veri
ty o
f ill
nes
s; c
are
-see
kin
g;
and
ho
me-
care
fo
r ill
nes
s.
Po
pu
lati
on
-b
ased
sam
ple
su
rvey
as
bas
elin
e fo
r th
e B
angl
ades
h
com
po
nen
t o
f th
e M
ult
i-co
un
try
Eval
uat
ion
of
the
Inte
grat
ed
Man
agem
ent
of
Ch
ildh
oo
d
Illn
ess
stra
tegy
2,2
89
ch
ildre
n in
ru
ral
Ban
glad
esh
: 2
00
0
Des
crip
tive
an
alys
is
(bas
ed o
n s
tan
dar
d
ind
icat
ors
of
the
M
CE
of
IMC
I Ef
fect
iven
ess,
Co
st
and
Imp
act
and
eq
uit
y an
alys
is
guid
elin
es a
dap
ted
fo
r u
se in
B
angl
ades
h)
(+)
M
eas
ure
d o
utc
om
es:
Mo
rbid
ity
and
ho
spit
aliz
atio
ns,
incl
ud
ing
seve
rity
of
illn
ess;
car
e-s
eeki
ng
for
child
illn
ess;
an
d h
om
e-c
are
for
illn
ess
B
ish
ai e
t al
. (2
00
2)
Vac
cin
es
Ch
ildre
n 9
-59
m
on
ths
for
mea
sles
va
ccin
atio
n a
nd
1
2-5
9 m
on
ths
for
DP
T va
ccin
atio
n
Co
mp
aris
on
of
the
effe
ct o
f p
aren
tal
sch
oo
ling
on
ch
ildh
oo
d v
acci
ne
rece
ipt
wit
h a
nd
w
ith
ou
t an
inte
nsi
ve
pu
blic
hea
lth
ca
mp
aign
(in
ten
sive
o
utr
each
vis
its
by
com
mu
nit
y h
ealt
h
wo
rker
s)
Ban
glad
esh
: kn
ow
led
ge,
atti
tud
es a
nd
p
ract
ice
(K
AP
) su
rvey
of
fam
ily
pla
nn
ing
and
ch
ild h
ealt
h
42
38
res
po
nd
ents
in
inte
rven
tio
n a
rea
that
re
ceiv
ed o
utr
eac
h
37
08
res
po
nd
ents
in
com
par
iso
n a
rea
(on
ly
limit
ed g
ove
rnm
enta
l se
rvic
es)
Jan
- J
ul
19
90
M
ult
ivar
iate
an
alys
is
wit
h in
tera
cted
m
od
els
(+)
M
eas
ure
d o
utc
om
es:
Pro
bab
ility
of
vacc
ine
rece
ipt
(me
asle
s an
d D
PT)

1
9
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Ch
akra
bo
rty
et
al. (
20
03
) M
ater
nal
hea
lth
W
om
en
15
-49
yea
rs
Iden
tifi
cati
on
of
ind
ivid
ual
fac
tors
th
at m
ay f
acili
tate
or
imp
ede
the
eff
ecti
ve
use
of
hea
lth
car
e se
rvic
es f
or
mat
ern
al
mo
rbid
ity.
Ban
glad
esh
: lo
ngi
tud
inal
d
ata
fro
m t
he
‘M
ater
nal
M
orb
idit
y P
rosp
ecti
ve
Stu
dy’
by
BIR
PER
HT
1,0
20
pre
gnan
t
wo
men
N
ov
19
92
-
Dec
1
99
3
Biv
aria
te a
nd
m
ult
ivar
iate
an
alys
is
(tri
cho
tom
ou
s lo
gist
ic r
egre
ssio
n)
(+)
M
eas
ure
d o
utc
om
es:
Fac
tors
ass
oci
ated
wit
h t
he
use
of
mat
ern
al h
ealt
h c
are
serv
ices
Ch
ow
dh
ury
e
t al
. (2
00
7)
Mat
ern
al h
ealt
h
Wo
men
1
5-4
9 y
ears
U
se o
f m
ater
nal
h
ealt
h s
ervi
ces
for
sele
cted
pre
gnan
cy-
rela
ted
co
mp
licat
ion
s (e
.g.
pro
lon
ged
lab
ou
r,
exce
ssiv
e b
leed
ing,
h
igh
fev
er/d
isch
arge
, co
nvu
lsio
ns)
Ban
glad
esh
D
emo
grap
hic
H
ealt
h S
urv
ey
10
,54
4 e
ver-
mar
ried
w
om
en a
ged
10
– 4
9
year
s
19
99
-2
00
0
Biv
aria
te,
mu
ltiv
aria
te a
nal
ysis
, m
ult
ino
mia
l lo
gist
ic
regr
essi
on
(+
)
M
eas
ure
d o
utc
om
es:
Hea
lth
care
-see
kin
g b
ehav
ior
for
dif
fere
nt
rep
ort
ed c
om
plic
atio
ns
H
ald
er e
t al
. (2
00
7)
Mat
ern
al h
ealt
h
Wo
men
1
5-4
9 y
ears
In
equ
alit
ies
and
im
plic
atio
ns
of
faci
lity-
bas
ed
mat
ern
ity
care
su
ch
as A
NC
, del
iver
y p
lace
an
d P
NC
BD
HS
5 4
16
wo
men
2
00
4
Biv
aria
te a
nd
m
ult
ivar
iate
an
alys
es
(+)
M
eas
ure
d o
utc
om
es:
Use
of
AN
C, b
irth
fac
ility
, PN
C

2
0
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Kam
al (
20
09
) P
erin
atal
hea
lth
M
arri
ed
ado
lesc
ents
P
reva
len
ce o
f an
d
fact
ors
ass
oci
ated
w
ith
mat
ern
al h
eal
th
serv
ice
uti
lizat
ion
Ban
glad
esh
D
emo
grap
hic
an
d H
eal
th
Surv
ey
(BD
HS)
17
28
wo
men
wh
o h
ad
give
n b
irth
in t
hei
r te
ens
in t
he
pas
t 5
ye
ars
20
04
B
ivar
iate
an
d
mu
ltiv
aria
te a
nal
ysis
(+
)
M
eas
ure
d o
utc
om
es:
Fac
tors
ass
oci
ated
wit
h m
ater
nal
he
alth
car
e s
ervi
ce u
tiliz
atio
n a
mo
ng
mar
ried
ad
ole
scen
ts
M
ash
reky
e
t al
. (2
01
0)
Ch
ildh
oo
d a
nd
in
fan
t h
ealt
h
Bu
rned
ch
ildre
n
un
der
age
18
H
ealt
h s
eek
ing
beh
avio
r o
f p
aren
ts
for
thei
r ch
ildre
n
wit
h b
urn
inju
ries
.
Ban
glad
esh
: p
op
ula
tio
n-
bas
ed c
ross
-se
ctio
nal
su
rvey
Fam
ilies
of
10
13
bu
rned
ch
ildre
n
20
03
M
ult
iple
logi
stic
re
gres
sio
n.
(+)
M
eas
ure
d o
utc
om
es:
Use
of
dif
fere
nt
typ
es o
f se
rvic
e p
rovi
der
s (q
ual
ifie
d a
nd
un
qu
alif
ied
) fo
r th
e tr
eatm
ent
of
bu
rn in
juri
es
N
ajn
in e
t al
. (2
01
1)
Ch
ildh
oo
d a
nd
infa
nt
hea
lth
C
hild
ren
un
der
ag
e 5
Fa
cto
rs a
sso
ciat
ed
wit
h u
pta
ke o
f se
rvic
es f
rom
tra
ined
h
ealt
hca
re p
rovi
der
s fo
r u
nd
er-5
ch
ildre
n
wit
h r
epo
rted
feb
rile
ill
nes
s
Ban
glad
esh
: cr
oss
-se
ctio
nal
su
rvey
in t
he
catc
hm
ent
area
s o
f 2
te
rtia
ry-l
evel
p
aed
iatr
ic
ho
spit
als
in
Dh
aka
Fam
ilies
of
12
90
b
urn
ed c
hild
ren
A
ug
- O
ct
20
07
Pri
nci
pal
co
mp
on
ent
anal
ysis
, mu
ltip
le
logi
stic
reg
ress
ion
s (+
)
M
eas
ure
d o
utc
om
es:
Up
take
of
trai
ned
hea
lth
ser
vice
s fo
r ch
ildre
n u
nd
er a
ge 5
wit
h f
ever

2
1
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Rab
ban
i &
Ale
xan
der
(2
00
9)
Ch
ildh
oo
d a
nd
in
fan
t h
ealt
h
Ru
ral p
op
ula
tio
n
in a
reas
imp
acte
d
by
flo
od
ing
Fact
ors
ass
oci
ated
w
ith
rep
ort
s o
f ill
nes
s an
d d
eman
d
for
do
cto
rs in
h
ou
seh
old
s w
ith
ch
ildre
n le
ss t
han
10
ye
ars
of
age
Inte
rnat
ion
al
Foo
d P
olic
y R
esea
rch
In
stit
ute
’s
Foo
d
Man
agem
ent
and
Su
pp
ort
P
roje
ct
75
7 h
ou
seh
old
s in
se
ven
th
anas
3
su
rvey
ro
un
ds,
N
ov
19
98
&
Dec
1
99
9
Des
crip
tive
an
alys
es a
nd
logi
t m
od
els
(+)
M
eas
ure
d o
utc
om
es:
Fac
tors
infl
uen
cin
g h
ealt
h-c
are
seek
ing
beh
avio
r fo
r si
ck c
hild
ren
un
der
age
10
Rah
man
et
al.
(20
08
) P
erin
atal
hea
lth
W
om
en
15
-49
yea
rs
Soci
oec
on
om
ic
dif
fere
nti
als
of
mat
ern
ity
care
se
ekin
g, a
nd
w
het
her
acc
essi
bili
ty
of
serv
ices
red
uce
s d
iffe
ren
tial
s in
m
ater
nit
y ca
re
seek
ing
Lon
gitu
din
al
dat
a fr
om
th
e
Mat
ern
al
Mo
rbid
ity
Pro
spec
tive
St
ud
y b
y B
IRP
ERH
T
19
19
wo
men
1
99
3 -
1
99
4
Mu
lti-
leve
l lo
gist
ic
regr
essi
on
(+
+)
M
eas
ure
d o
utc
om
es:
Det
erm
inan
ts o
f an
ten
atal
car
e s
eeki
ng
and
bir
thin
g as
sist
ance
Rah
man
et
al.
(20
12
) P
erin
atal
hea
lth
G
ener
al
po
pu
lati
on
A
sso
ciat
ion
bet
wee
n
mat
ern
al
exp
erie
nce
s o
f p
hys
ical
an
d s
exu
al
IPV
an
d u
se o
f A
NC
se
rvic
es a
nd
del
iver
y as
sist
ance
BD
HS
20
01
cu
rren
tly
mar
ried
w
om
en a
ged
15
- 4
9
wit
h a
t le
ast
on
e ch
ild
un
der
age
5
20
07
M
ult
ivar
iate
an
alys
is
(+)
M
eas
ure
d o
utc
om
es:
Ass
oci
atio
ns
bet
wee
n IP
V a
nd
use
of
rep
rod
uct
ive
hea
lth
ser
vice
s: S
uff
icie
nt
AN
C, t
ype
of
AN
C p
rovi
der
, del
iver
y as
sist
ance
, use
of
rep
rod
uct
ive
hea
lth
ser
vice
s an
d o
ther
co
vari
ates

2
2
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Re
yno
lds
e
t al
. (2
00
6)
Per
inat
al h
ealt
h
Wo
men
age
d
15
-23
wit
h
child
ren
Ass
oci
atio
ns
bet
we
en h
eal
th
ou
tco
me
& e
arly
ch
ildb
eari
ng,
ad
ole
scen
t m
oth
ers'
u
se o
f m
ate
rnal
an
d
child
hea
lth
ser
vice
. U
se o
f an
ten
atal
ca
re, d
eliv
ery
care
&
infa
nt
imm
un
izat
ion
se
rvic
es r
elat
ive
to
that
of
old
er w
om
en,
taki
ng
into
acc
ou
nt
fact
ors
th
at m
ay
med
iate
th
e
rela
tio
nsh
ip b
etw
een
ag
e an
d u
se o
f se
rvic
es
BD
HS
and
D
HS
fro
m
14
oth
er
cou
ntr
ies’
Wo
men
an
d t
hei
r p
regn
anci
es a
nd
bir
ths
(lim
ited
to
ch
ildre
n
bo
rn t
o e
ver-
mar
ried
w
om
en)
- sa
mp
le s
ize
no
t gi
ven
DH
S af
ter
19
92
Mu
ltiv
aria
ble
an
alys
es w
ith
su
rvey
-bas
ed lo
gist
ic
regr
essi
on
mo
del
s (+
)
M
eas
ure
d o
utc
om
es:
Use
of
skill
ed m
ater
nal
hea
lth
car
e
Se
nar
ath
&
Gu
naw
ard
en
a (2
00
9)
Fem
ale
hea
lth
W
om
en a
ged
1
5-4
9 a
nd
th
eir
pre
sch
oo
l age
d
child
ren
Det
erm
inan
ts o
f w
om
en’s
au
ton
om
y in
hea
lth
car
e
dec
isio
n m
akin
g
Nep
al
Dem
ogr
aph
ic
and
He
alth
Su
rvey
20
01
, B
DH
S 2
00
4,
and
th
e
Nat
ion
al
Fam
ily H
ealt
h
Surv
ey In
dia
1
99
8-1
99
9
Nep
al (
8,7
26
),
Ban
glad
esh
(1
0,5
82)
, In
dia
(8
9,1
99
)
19
98
-
20
04
D
escr
ipti
ve s
tati
stic
s (+
)
M
eas
ure
d o
utc
om
es:
Fac
tors
ass
oci
ated
wit
h w
om
en’s
par
tici
pat
ion
reg
ard
ing
thei
r o
wn
hea
lth

2
3
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Sto
ry &
B
urg
ard
(2
01
2)
Mat
ern
al h
ealt
h
Mar
ried
co
up
les
U
sin
g m
atch
ed
hu
sban
d a
nd
wif
e re
po
rts
abo
ut
wh
o
mak
es c
om
mo
n
ho
use
ho
ld d
ecis
ion
s to
pre
dic
t u
se o
f an
ten
atal
an
d s
kille
d
del
iver
y ca
re
BD
HS
1,6
23
mar
ried
co
up
les
wit
h a
ch
ild u
nd
er f
ive
year
s o
ld
20
07
B
ivar
iate
an
d
mu
ltiv
aria
te a
nal
ysis
(+
)
M
eas
ure
d o
utc
om
es:
At
leas
t o
ne
an
ten
atal
car
e v
isit
an
d la
st b
irth
was
ass
iste
d b
y a
skill
ed h
ealt
h p
rofe
ssio
nal
su
ch a
s a
do
cto
r, n
urs
e, o
r m
idw
ife
U
dd
in e
t al
. (2
00
9)
Bas
ic h
ealt
h
Ho
mel
ess
in
Dh
aka
aged
1
5-4
9
Exte
nt
to w
hic
h t
he
n
eed
fo
r p
rim
ary
hea
lth
car
e s
ervi
ces
amo
ng
stre
et-
dw
elle
rs is
met
th
rou
gh e
xist
ing
faci
litie
s.
Ban
glad
esh
: co
mm
un
ity-
bas
ed c
ross
-se
ctio
nal
st
ud
y
89
6 h
om
eles
s p
eop
le
Jun
2
00
7 -
M
ay
20
08
Biv
aria
te a
nd
m
ult
ivar
iate
an
alys
is
(+)
M
eas
ure
d o
utc
om
es:
Use
of
gen
eral
hea
lth
ser
vice
s as
wel
l as
ante
nat
al c
are
(AN
C)
and
po
stn
atal
car
e (
PN
C)
Yo
un
g e
t al
. (2
00
6)
Bas
ic h
ealt
h
Gen
eral
p
op
ula
tio
n
Del
inea
te a
ge, s
ex
and
oth
er f
acto
rs
asso
ciat
ed w
ith
ac
cess
ing
hea
lth
care
Ban
glad
esh
: M
atla
b H
ealt
h
and
So
cio
eco
no
mic
Su
rvey
.
11
,15
1 a
du
lts
ove
r ag
e 1
5
19
96
-
19
97
W
eigh
ted
logi
stic
re
gres
sio
n, h
ealt
h
beh
avio
r m
od
el
(++)
M
eas
ure
d o
utc
om
es:
Use
of
the
he
alth
care
sys
tem
(vi
sits
in t
hre
e m
on
ths
pri
or
to s
urv
ey)
*Qu
alit
y: h
igh
(++
), a
ccep
tab
le (
+)

Access barriers: Predisposing factors The findings on determinants and barriers to health service utilization in Bangladesh are summarized in Table 1b. A person’s age has a strong impact on the decision whether to use professional health services, less appropriate services or even no services. The higher the age of a woman giving birth, the more likely she uses professional delivery services (Rahman et al. 2012, Reynolds et al. 2006, Chowdhury et al. 2007). Further, the age of a woman at marriage is associated with the use of maternal health care services. Chakraborty and colleagues (2003) show that women who married at an age younger than 15 years were less likely to use maternal health care services than those who married later. In the case of child health services, the age of the affected child matters. Najnin and colleagues (2011) demonstrates a higher uptake of trained health services for children less than 2 years as compared with those between 2 and 5 years. Another study confirms that the likelihood of children being taken to a health provider for illness (across different acute morbidity symptoms) decreases with increasing age (Alam et al. 2009). The impact of gender on the use of health services differs depending on the type of service required. In the case of general health services, Ahsan and colleagues (2004) show that male TB cases are less likely to obtain TB care in a study that specifically highlights gender differences. In contrast, in a study across different ethnic groups in the Chittagong Hill Tracts, Ahmed (2001) found women were significantly less likely than men to secure any type of health care service (including traditional and modern forms of self-treatment or consultations, or allopathic care). In yet another study looking at sex differentials in health care use, women were less likely to utilize healthcare services than men; elderly rural women were less likely than younger urban; and never-married women less likely than women that were married or had been married (Young et al. 2006). According to the authors, in rural households women may be less valued and thus fewer household resources are spent on women’s health. When it comes to child health services, the child’s gender influences a mother’s decision on whether to seek health care, request professional help, or to be satisfied with traditional or untrained help. Rabbani and Alexander (2009) show that girls are far less likely to be taken to a doctor. Family income and mother’s education influence service uptake for boys; the analysis does not produce any comparable significant influence for girls. Similar results hold in relation to vaccinations (Bishai et al. 2002). Boys are vaccinated more consistently than girls. The same form of gender inequity was not identified in a similar study conducted in Vietnam (Thang et al. 2007). A higher likelihood for boys to benefit from health services in cases of illness is confirmed by two further studies (Alam et al. 2009, Najnin et al. 2011). In Bangladesh, significant differences in health service utilization between religious groups were apparent in two studies (Rahman et al. 2012, Young et al. 2006). In one study, obtaining health care was positively related to being a Muslim man and negatively related to being a Hindu. Male Hindus at every age used services less than Muslims (Young et al. 2006). A different study

25
indicated a negative association between Muslim faith and the use of reproductive health services in the context of intimate partner violence (Rahman et al. 2012). Ethnicity is an important predictor of treatment seeking. Ahmed (2001) presents a study that focuses on health and health-seeking behavior of ethnic minorities in the Chittagong Hill Tracts in southeast Bangladesh. The survey distinguishes five ethnic groups (Bangali, Chakma, Marma, Mro and Tripura) residing in mostly ethnically homogeneous villages. The probability of an ill person of non-Bangali ethnicity seeking health care is significantly lower than that for a member of a Bangali group. The impact of ethnicity on health seeking behavior is more pronounced than that of gender or distance to a facility. Access barriers: Enabling factors The studies offer rich information on enabling factors and important insight into access issues can be derived from an analysis of individual and household characteristics. Apart from the household’s economic status, captured either by household wealth (sometimes elements thereof, such as land-holding) or income, the information status of the household plays a critical role. Lack of information about health and the availability of health services constitute a major access barrier. Conversely, information is a crucial enabler of health services uptake. Several studies illustrate contextual examples of the role of health knowledge as an enabling factor. Bishai reports (2002) that health service users gain experience as they access care and when parents know the local health facility well, they are more likely to have their child vaccinated. Husbands who understand the risk of pregnancy complications will support their wife’s use of appropriate services (Chowdhury et al. 2007). Mass media exposure (that ideally conveys some rudimentary information on health and health care) positively affects the use of reproductive health services among women in Bangladesh in the context of intimate partner violence (Rahman et al. 2012). Information status depends on several characteristics of the household and its members and information may be gained from mass media (Rahman et al. 2012) or prior utilization of health services (Chakraborty et al. 2003). Not surprisingly, a positive relationship exists between the information status of an individual or household and education level. Education facilitates the processing of information or “information effectiveness” (Thiede 2005). The surveys underlying the reviewed studies, without exception, capture the respondent’s education level. One study limited analysis to the mothers’ and household head’s literacy (Mashreky et al. 2010) and defined literacy as a binominal variable: A person who attended school at least 1 year was designated literate. The Demographic and Health Surveys utilize the following categories: no school education, completed primary, completed secondary and completed higher education. Most studies include different education levels as explanatory variables in their regression models. All studies show a positive relationship between education level and utilization of qualified health services. Not only is the prospective health service client’s education a factor, but also, the household head’s education is a significant predictor of care-seeking behavior, as indicated by Ahmed (2001). Even in the context of seeking care for children, the father’s education has a positive effect on care-seeking decisions (Najnin et al. 2011).

26
Quantitative analysis of the surveys conducted in Bangladesh provides little insight into the interplay of factors at the household level. Whereas a general awareness of different patterns of household decision-making is reflected in the literature, quantitative studies do not explicitly address the interactions. Quantitative studies also provide no clarity as to the underlying socio-cultural and socio-economic patterns that promote the role of the household head in decision-making or the role of education of both the household head and the spouse or mother. And yet, this information could improve targeting health communications, both geographically and structurally. When a mother’s education level has been analyzed, separately from that of the father or household head, in the context of MCH services, findings shed light on the woman’s level of autonomy. Moreover, in the context of Bangladesh – and in most of the included studies – the mother’s characteristics cannot be regarded independent of household characteristics. Chakraborty and colleagues (2003) demonstrate a positive association between a mother’s education level and health care utilization. Education level not only impacts access to care by means of its link to information effectiveness, but also, co-determines the opportunities to earn and secure the household’s living. The Bangladesh studies indicate that non-financial and financial access barriers are inextricably linked. Indicators for “enablers” within the access dimension “affordability”, include household socioeconomic status or wealth, e.g., as a household asset index (Arifeen et al. 2008; Bhuiya et al. 2009; Chowdhury et al. 2007; Kamal 2009; Najnin et al. 2011), family income (Mashreky et al. 2010; Rabbani and Alexander 2009), household average monthly expenditure (Rahman et al. 2008) or land-holding status (Ahmed 2001). Gainful employment or occupation is also and indicator of a household’s ability to pay. However, in some cases, occupation may hinder access given that some occupations require absence from the household and limit availability to attend health services or facilitate service uptake by family members. As indicated, individual and household characteristics that enable individuals to seek treatment are not always separable. Apart from common food consumption and intermingling of income, the household is an entity ruled by particular decision-making patterns, the determinants of which are manifold and can hardly be captured by a household survey. Some characteristics may be subsumed under household rather than individual characteristics. Decision-making patterns are rarely explicitly addressed in analysis of household surveys. An exception is the illuminating study of Senarath and Gunawardena (2009) that examines women’s autonomy regarding health care decisions. Their results indicate autonomy increases with age, level of education, employment (for cash) and with the number of living children. Further, a high socioeconomic status and urban residence promote women’s autonomy in health care decision-making.

Tab
le 1
b:
Ban
glad
esh
– F
ind
ings
A
uth
or
Bar
rie
rs a
nd
de
term
inan
ts id
enti
fied
P
osi
tive
Co
rre
lati
on
N
ega
tive
Co
rre
lati
on
Ah
me
d (
20
01
) Fi
nan
cial
an
d n
on
-fin
anci
al d
ete
rmin
ants
of
trea
tmen
t se
ekin
g b
ehav
ior
for
hea
lth
pro
vid
ers,
in
par
ticu
lar
for
allo
pat
hic
tre
atm
ents
.
Lan
d-h
old
ing
stat
us,
h
ou
seh
old
hea
d's
ed
uca
tio
n.
Bei
ng
fem
ale,
em
plo
ymen
t, n
ot
Ben
gali
eth
nic
ity,
dis
tan
ce f
rom
sta
tic
allo
pat
hic
hea
lth
car
e fa
cilit
y.
R
esu
lts
/ co
ncl
usi
on
s: S
ex, t
ypes
of
illn
ess,
eth
nic
ity,
ho
use
ho
ld h
ead
’s e
du
cati
on
an
d h
ou
seh
old
’s la
nd
ho
ldin
g w
ere
sign
ific
ant
pre
dic
tors
of
seek
ing
trea
tmen
t, a
nd
allo
pat
hic
tre
atm
ent
in p
arti
cula
r.
Ah
san
et
al.
(20
04
) B
arri
ers
to u
pta
ke o
f TB
ser
vice
s, g
end
er in
equ
alit
y.
Sati
sfac
tio
n w
ith
pro
vid
er's
b
ehav
ior,
dru
g in
take
su
per
visi
on
.
Bei
ng
mal
e, p
oo
r h
eal
th c
ou
nse
ling,
u
nfr
ien
dly
tre
atm
ent.
R
esu
lts
/ co
ncl
usi
on
s: S
ign
ific
ant
gen
der
dif
fere
nce
s in
tre
atm
ent
seek
ing
beh
avio
rs a
sso
ciat
ed w
ith
so
cio
-cu
ltu
ral b
arri
ers,
p
arti
cula
rly
amo
ng
fem
ales
in t
hei
r ac
cess
to
TB
car
e. F
emal
e TB
cas
es f
ace
mo
re s
oci
o-c
ult
ura
l bar
rier
s th
an m
ales
in a
cces
s to
TB
ca
re.
Ala
m e
t al
. (2
00
9)
Det
erm
inan
ts o
f se
ekin
g b
ehav
ior
for
any
he
alth
p
rovi
der
. C
hild
age
bel
ow
5,
illn
ess
du
rati
on
, h
ou
seh
old
less
th
an 2
p/p
er r
oo
m,
no
n-g
ove
rnm
enta
l hea
lth
ser
vice
in
the
area
, mo
ther
's e
du
cati
on
, m
oth
er h
as s
oci
al n
etw
ork
.
Feve
r sy
mp
tom
s, c
hild
is f
emal
e.
R
esu
lts
/ co
ncl
usi
on
s: M
oth
er’s
ed
uca
tio
n w
as t
he
mo
st im
po
rtan
t fa
cto
r, f
ollo
wed
by
nu
mb
er o
f p
erso
ns
livin
g p
er r
oo
m a
nd
so
cial
net
wo
rks.
Th
e ef
fect
s o
f o
ther
var
iab
les
such
as
ind
icat
ors
of
wo
men
’s s
oci
al a
nd
eco
no
mic
sta
tus
was
oft
en in
th
e p
red
icte
d
dir
ecti
on
, bu
t n
ot
stat
isti
cally
sig
nif
ican
t. R
elat
ion
ship
s o
f h
ou
seh
old
eco
no
mic
an
d s
anit
atio
n v
aria
ble
s, w
ith
use
of
ph
ysic
ian
s w
ere
in
gen
eral
str
on
ger
than
fo
r u
se o
f p
aram
edic
s an
d h
om
eop
ath
s, a
nd
sta
tist
ical
ly s
ign
ific
ant
wit
h r
esp
ect
to t
hes
e tw
o in
dic
ato
rs.
Thu
s, im
ple
men
tati
on
of
soci
al a
nd
eco
no
mic
dev
elo
pm
ent
pro
gram
mes
an
d p
rogr
amm
es t
o in
cre
ase
the
wo
men
’s p
osi
tio
n in
ru
ral B
angl
ades
h, s
ho
uld
lead
to
mo
re f
req
ue
nt
use
of
mo
de
rn m
edic
al c
are
by
child
ren
bel
ow
15
.
Ari
fee
n e
t al
. (2
00
8)
Rat
es a
nd
dif
fere
nti
als
by
sex
and
so
cio
eco
no
mic
st
atu
s fo
r 3
asp
ects
of
rura
l ch
ild h
ealt
h: m
orb
idit
y an
d h
osp
ital
izat
ion
s, in
clu
din
g ill
nes
s se
veri
ty; c
are-
seek
ing;
an
d h
om
e-ca
re f
or
illn
ess
Wea
lth
, per
ceiv
ed s
ever
ity
of
illn
ess,
dan
ger
sign
s.
Per
ceiv
ed lo
w q
ual
ity
of
care
.
R
esu
lts
/ co
ncl
usi
on
s: T
her
e w
ere
no
sig
nif
ican
t d
iffe
ren
ces
in t
he
pre
vale
nce
of
illn
ess,
eit
her
by
sex
or
soci
oec
on
om
ic s
tatu
s.
Ch
ild h
ealt
h p
lan
ner
s an
d r
esea
rch
ers
sho
uld
ad
dre
ss t
he
app
aren
t p
op
ula
tio
n p
refe
ren
ce f
or
un
trai
ned
an
d t
rad
itio
nal
pro
vid
ers.
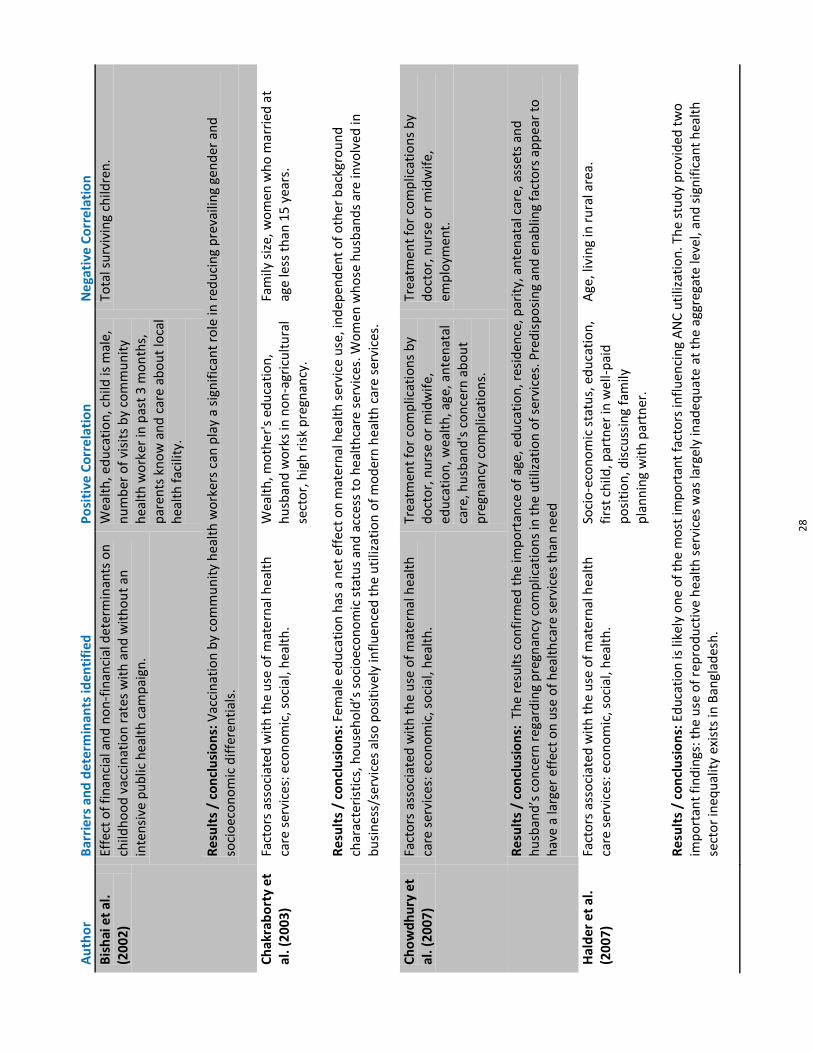
2
8
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Bis
hai
et
al.
(20
02
) Ef
fect
of
fin
anci
al a
nd
no
n-f
inan
cial
det
erm
inan
ts o
n
child
ho
od
vac
cin
atio
n r
ates
wit
h a
nd
wit
ho
ut
an
inte
nsi
ve p
ub
lic h
ealt
h c
amp
aign
.
Wea
lth
, ed
uca
tio
n, c
hild
is m
ale,
n
um
ber
of
visi
ts b
y co
mm
un
ity
hea
lth
wo
rker
in p
ast
3 m
on
ths,
p
aren
ts k
no
w a
nd
car
e a
bo
ut
loca
l h
ealt
h f
acili
ty.
Tota
l su
rviv
ing
child
ren
.
R
esu
lts
/ co
ncl
usi
on
s: V
acci
nat
ion
by
com
mu
nit
y h
ealt
h w
ork
ers
can
pla
y a
sign
ific
ant
role
in r
edu
cin
g p
reva
ilin
g ge
nd
er a
nd
so
cio
eco
no
mic
dif
fere
nti
als.
Ch
akra
bo
rty
et
al. (
20
03
) Fa
cto
rs a
sso
ciat
ed w
ith
th
e u
se o
f m
ate
rnal
hea
lth
ca
re s
ervi
ces:
eco
no
mic
, so
cial
, hea
lth
. W
ealt
h, m
oth
er'
s ed
uca
tio
n,
hu
sban
d w
ork
s in
no
n-a
gric
ult
ura
l se
cto
r, h
igh
ris
k p
regn
ancy
.
Fam
ily s
ize,
wo
men
wh
o m
arri
ed a
t ag
e le
ss t
han
15
yea
rs.
R
esu
lts
/ co
ncl
usi
on
s: F
emal
e ed
uca
tio
n h
as a
net
eff
ect
on
mat
ern
al h
eal
th s
ervi
ce u
se, i
nd
epen
den
t o
f o
the
r b
ackg
rou
nd
ch
arac
teri
stic
s, h
ou
seh
old
’s s
oci
oec
on
om
ic s
tatu
s an
d a
cces
s to
hea
lth
care
ser
vice
s. W
om
en w
ho
se h
usb
and
s ar
e in
volv
ed in
b
usi
nes
s/se
rvic
es a
lso
po
siti
vely
infl
uen
ced
th
e u
tiliz
atio
n o
f m
od
ern
hea
lth
car
e s
ervi
ces.
Ch
ow
dh
ury
et
al. (
20
07
) Fa
cto
rs a
sso
ciat
ed w
ith
th
e u
se o
f m
ate
rnal
hea
lth
ca
re s
ervi
ces:
eco
no
mic
, so
cial
, hea
lth
. Tr
eatm
ent
for
com
plic
atio
ns
by
do
cto
r, n
urs
e o
r m
idw
ife
, ed
uca
tio
n, w
ealt
h, a
ge, a
nte
nat
al
care
, hu
sban
d's
co
nce
rn a
bo
ut
pre
gnan
cy c
om
plic
atio
ns.
Trea
tmen
t fo
r co
mp
licat
ion
s b
y d
oct
or,
nu
rse
or
mid
wif
e,
emp
loym
ent.
R
esu
lts
/ co
ncl
usi
on
s: T
he
resu
lts
con
firm
ed t
he
imp
ort
ance
of
age,
ed
uca
tio
n, r
esid
ence
, par
ity,
an
ten
atal
car
e, a
sset
s an
d
hu
sban
d’s
co
nce
rn r
egar
din
g p
regn
ancy
co
mp
licat
ion
s in
th
e u
tiliz
atio
n o
f se
rvic
es. P
red
isp
osi
ng
and
en
ablin
g fa
cto
rs a
pp
ear
to
h
ave
a la
rger
eff
ect
on
use
of
hea
lth
care
ser
vice
s th
an n
eed
Hal
der
et
al.
(20
07
) Fa
cto
rs a
sso
ciat
ed w
ith
th
e u
se o
f m
ate
rnal
hea
lth
ca
re s
ervi
ces:
eco
no
mic
, so
cial
, hea
lth
. So
cio
-eco
no
mic
sta
tus,
ed
uca
tio
n,
firs
t ch
ild, p
artn
er in
wel
l-p
aid
p
osi
tio
n, d
iscu
ssin
g fa
mily
p
lan
nin
g w
ith
par
tner
.
Age
, liv
ing
in r
ura
l are
a.
R
esu
lts
/ co
ncl
usi
on
s: E
du
cati
on
is li
kely
on
e o
f th
e m
ost
imp
ort
ant
fact
ors
infl
uen
cin
g A
NC
uti
lizat
ion
. Th
e st
ud
y p
rovi
ded
tw
o
imp
ort
ant
fin
din
gs: t
he
use
of
rep
rod
uct
ive
hea
lth
ser
vice
s w
as la
rgel
y in
adeq
uat
e a
t th
e a
ggre
gate
leve
l, an
d s
ign
ific
ant
hea
lth
se
cto
r in
equ
alit
y ex
ists
in B
angl
ades
h.

2
9
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Kam
al (
20
09
) Fa
cto
rs a
sso
ciat
ed w
ith
th
e u
se b
y ad
ole
scen
ts o
f m
ater
nal
hea
lth
car
e se
rvic
es: e
con
om
ic, s
oci
al,
hea
lth
.
Wea
lth
, hu
sban
d w
ork
s in
no
n-
agri
cult
ura
l sec
tor,
ed
uca
tio
n.
Wo
man
is w
ork
ing,
livi
ng
in r
ura
l ar
ea.
R
esu
lts
/ co
ncl
usi
on
s: S
tro
ng
dif
fere
nce
s in
up
take
of
ante
nat
al a
nd
bir
th h
elp
be
twe
en r
egi
on
s. W
ealt
h, e
du
cati
on
, res
iden
ce a
nd
b
irth
ord
er a
re m
ost
imp
ort
ant
det
erm
inan
ts.
M
ash
reky
et
al. (
20
10
) D
eter
min
ants
fo
r th
e h
ealt
h s
eeki
ng
beh
avio
r o
f p
aren
ts f
or
thei
r ch
ildre
n d
uri
ng
bu
rn in
juri
es.
Fam
ily in
com
e, li
tera
cy o
f ei
the
r p
aren
t.
Fam
ily s
ize,
livi
ng
in r
ura
l are
a, b
irth
o
rder
of
affe
cted
ch
ild.
R
esu
lts
/ co
ncl
usi
on
s: A
bo
ut
two
-th
ird
s o
f ch
ildh
oo
d b
urn
vic
tim
s w
ere
tre
ated
by
un
qu
alif
ied
ser
vice
pro
vid
ers
du
e to
par
ents
’ ch
oic
e. P
refe
ren
ce o
f se
ekin
g h
ealt
h c
are
fro
m u
nq
ual
ifie
d s
ervi
ce p
rovi
der
s w
as h
igh
er a
mo
ng
po
or,
illit
erat
e an
d r
ura
l peo
ple
.
Naj
nin
et
al.
(20
11
) Fa
cto
rs a
sso
ciat
ed w
ith
th
e u
se o
f p
aed
iatr
ic h
ealt
h
care
ser
vice
s: e
con
om
ic, s
oci
al, h
ealt
h.
Fam
ily w
ealt
h, m
ale
child
, fat
her
's
edu
cati
on
, ch
ild a
ge u
nd
er 2
, ch
ild h
as
dec
reas
ed le
vel o
f co
nsc
iou
snes
s.
R
esu
lts
/ co
ncl
usi
on
s: D
esp
ite
livin
g in
th
e ca
tch
men
t ar
eas
of
two
wel
l-fu
nct
ion
ing
pae
dia
tric
ho
spit
als
wit
h o
utp
atie
nt
faci
litie
s,
ove
r 1
/3 d
id n
ot
avai
l th
emse
lves
of
qu
alif
ied
car
e, il
lust
rati
ng
that
ph
ysic
al a
vaila
bili
ty o
f se
rvic
es a
lon
e d
oes
no
t en
sure
use
by
all.
R
abb
ani &
A
lexa
nd
er
(20
09
)
Fact
ors
ass
oci
ated
wit
h t
he
use
of
hea
lth
care
se
rvic
es f
or
child
ren
un
der
10
yea
rs.
Mo
ther
's e
du
cati
on
if m
ale
ch
ild,
inco
me
if m
ale
child
, ch
ild is
mal
e.
R
esu
lts
/ co
ncl
usi
on
s: G
irls
are
far
less
like
ly t
o b
e ta
ken
to
a d
oct
or.
Mo
ther
's e
du
cati
on
infl
uen
ces
up
take
on
ly f
or
bo
ys, t
her
e is
n
o in
flu
ence
on
up
take
fo
r gi
rls.
Rah
man
et
al.
(20
08
) So
cio
eco
no
mic
fac
tors
infl
uen
cin
g h
ealt
h c
are
up
take
W
ealt
h, s
ervi
ce a
cces
sib
ility
(cl
inic
n
earb
y), w
om
an c
on
sid
ers
hea
lth
to
be
imp
ort
ant,
acc
essi
bili
ty o
f ce
ntr
e f
or
ante
nat
al c
are.
R
esu
lts
/ co
ncl
usi
on
s: In
are
as w
her
e se
rvic
es
are
acce
ssib
le, t
he
dif
fere
nce
in d
eliv
ery
care
see
kin
g b
etw
een
wo
men
wit
h h
igh
er
ho
use
ho
ld r
eso
urc
es a
nd
th
ose
wit
h lo
we
r re
sou
rces
is s
ign
ific
antl
y d
imin
ish
ed. T
his
is a
lso
th
e c
ase
wit
h s
ervi
ce a
cces
sib
ility
an
d
wo
men
’s g
ain
ful e
mp
loym
ent.
Th
e u
pta
ke o
f an
ten
atal
car
e is
no
t re
late
d t
o t
he
acc
essi
bili
ty o
f su
ch c
are
(n
earb
y an
d f
ree)
.
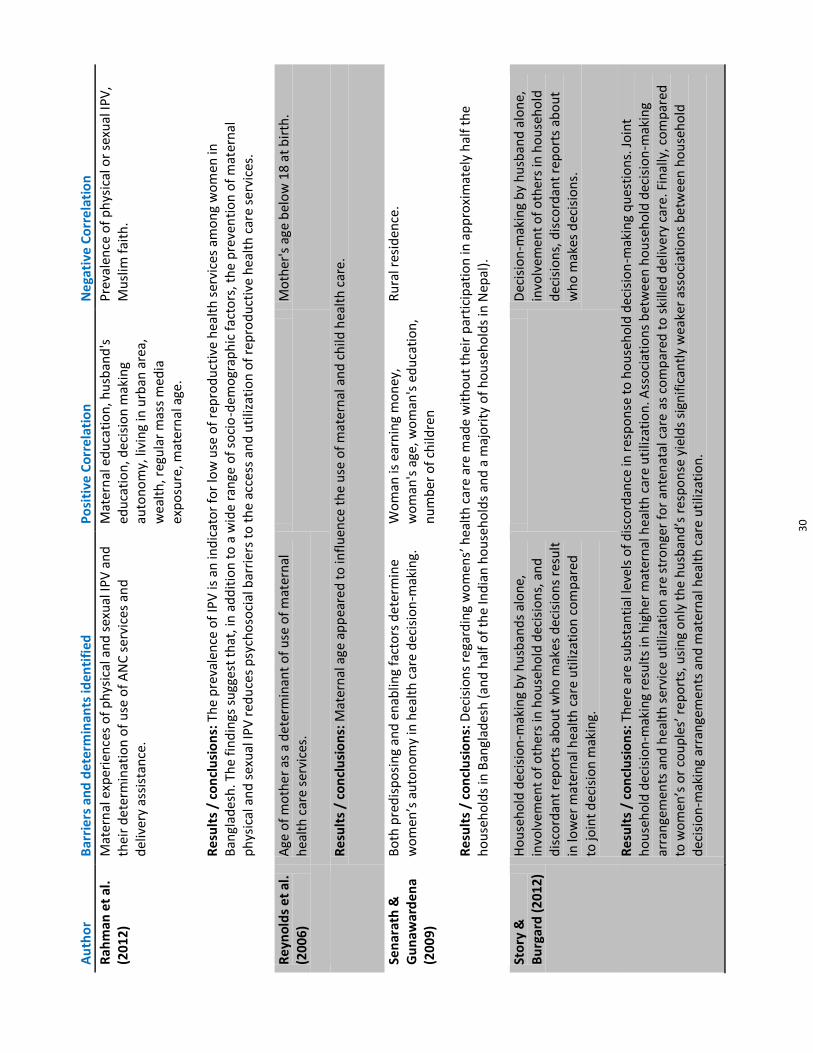
3
0
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Rah
man
et
al.
(20
12
) M
ater
nal
exp
erie
nce
s o
f p
hys
ical
an
d s
exu
al IP
V a
nd
th
eir
de
term
inat
ion
of
use
of
AN
C s
ervi
ces
and
d
eliv
ery
assi
stan
ce.
Mat
ern
al e
du
cati
on
, hu
sban
d's
ed
uca
tio
n, d
ecis
ion
mak
ing
auto
no
my,
livi
ng
in u
rban
are
a,
wea
lth
, reg
ula
r m
ass
med
ia
exp
osu
re, m
ater
nal
age
.
Pre
vale
nce
of
ph
ysic
al o
r se
xual
IPV
, M
usl
im f
aith
.
R
esu
lts
/ co
ncl
usi
on
s: T
he
pre
vale
nce
of
IPV
is a
n in
dic
ato
r fo
r lo
w u
se o
f re
pro
du
ctiv
e h
ealt
h s
ervi
ces
amo
ng
wo
men
in
Ban
glad
esh
. Th
e fi
nd
ings
su
gges
t th
at, i
n a
dd
itio
n t
o a
wid
e r
ange
of
soci
o-d
emo
grap
hic
fac
tors
, th
e p
reve
nti
on
of
mat
ern
al
ph
ysic
al a
nd
sex
ual
IPV
red
uce
s p
sych
oso
cial
bar
rier
s to
th
e a
cces
s an
d u
tiliz
atio
n o
f re
pro
du
ctiv
e h
ealt
h c
are
serv
ices
.
Re
yno
lds
et
al.
(20
06
) A
ge o
f m
oth
er
as a
de
term
inan
t o
f u
se o
f m
ater
nal
h
ealt
h c
are
ser
vice
s.
M
oth
er's
age
bel
ow
18
at
bir
th.
R
esu
lts
/ co
ncl
usi
on
s: M
ater
nal
age
ap
pea
red
to
infl
uen
ce t
he
use
of
mat
ern
al a
nd
ch
ild h
ealt
h c
are.
Sen
arat
h &
G
un
awar
de
na
(20
09
)
Bo
th p
red
isp
osi
ng
and
en
ablin
g fa
cto
rs d
ete
rmin
e w
om
en’s
au
ton
om
y in
he
alth
car
e d
ecis
ion
-mak
ing.
W
om
an is
ear
nin
g m
on
ey,
wo
man
's a
ge, w
om
an's
ed
uca
tio
n,
nu
mb
er o
f ch
ildre
n
Ru
ral r
esid
ence
.
R
esu
lts
/ co
ncl
usi
on
s: D
ecis
ion
s re
gard
ing
wo
men
s’ h
ealt
h c
are
are
mad
e w
ith
ou
t th
eir
par
tici
pat
ion
in a
pp
roxi
mat
ely
hal
f th
e h
ou
seh
old
s in
Ban
glad
esh
(an
d h
alf
of
the
Ind
ian
ho
use
ho
lds
and
a m
ajo
rity
of
ho
use
ho
lds
in N
epal
).
Sto
ry &
B
urg
ard
(2
01
2)
Ho
use
ho
ld d
ecis
ion
-mak
ing
by
hu
sban
ds
alo
ne,
in
volv
emen
t o
f o
ther
s in
ho
use
ho
ld d
ecis
ion
s, a
nd
d
isco
rdan
t re
po
rts
abo
ut
wh
o m
akes
dec
isio
ns
resu
lt
in lo
wer
mat
ern
al h
ealt
h c
are
uti
lizat
ion
co
mp
ared
to
join
t d
ecis
ion
mak
ing.
D
ecis
ion
-mak
ing
by
hu
sban
d a
lon
e,
invo
lvem
ent
of
oth
ers
in h
ou
seh
old
d
ecis
ion
s, d
isco
rdan
t re
po
rts
abo
ut
wh
o m
akes
dec
isio
ns.
R
esu
lts
/ co
ncl
usi
on
s: T
her
e ar
e s
ub
stan
tial
leve
ls o
f d
isco
rdan
ce in
res
po
nse
to
ho
use
ho
ld d
ecis
ion
-mak
ing
qu
esti
on
s. J
oin
t h
ou
seh
old
dec
isio
n-m
akin
g re
sult
s in
hig
her
mat
ern
al h
ealt
h c
are
uti
lizat
ion
. Ass
oci
atio
ns
bet
we
en h
ou
seh
old
dec
isio
n-m
akin
g ar
ran
gem
ents
an
d h
ealt
h s
ervi
ce u
tiliz
atio
n a
re s
tro
nge
r fo
r an
ten
atal
car
e a
s co
mp
ared
to
ski
lled
del
iver
y ca
re. F
inal
ly, c
om
par
ed
to w
om
en’s
or
cou
ple
s’ r
ep
ort
s, u
sin
g o
nly
th
e h
usb
and
’s r
esp
on
se y
ield
s si
gnif
ican
tly
wea
ker
asso
ciat
ion
s b
etw
een
ho
use
ho
ld
dec
isio
n-m
akin
g ar
ran
gem
ents
an
d m
ater
nal
hea
lth
car
e u
tiliz
atio
n.

3
1
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Ud
din
et
al.
(20
09
) Ex
trem
e vu
lner
abili
ty o
f st
ree
t-d
wel
lers
mas
ks s
om
e o
f th
e u
nd
erl
yin
g p
red
isp
osi
ng
and
en
ablin
g fa
cto
rs/b
arri
ers.
Wo
man
is m
arri
ed, m
an is
u
nem
plo
yed
.
R
esu
lts
/ co
ncl
usi
on
s: H
om
eles
s p
eop
le a
re v
ery
vuln
erab
le a
nd
hav
e li
ttle
acc
ess
to h
ealt
h s
ervi
ces.
Yo
un
g e
t al
. (2
00
6)
Det
erm
inan
ts o
f u
tiliz
atio
n g
rou
ped
into
"p
red
isp
osi
ng
fact
ors
" (a
ge, r
elig
ion
, sex
), "
enab
ling
fact
ors
" (e
du
cati
on
, mar
ital
sta
tus,
ho
use
ho
ld s
ize)
, "n
eed
fac
tors
" (h
ealt
h s
tatu
s, m
ob
ility
) an
d
"hea
lth
care
sys
tem
fac
tors
" (r
esid
ence
in p
rogr
am o
r co
mp
aris
on
are
a); a
ll fa
cto
rs im
ply
dif
fere
nce
s in
h
ealt
hca
re s
eeki
ng;
co
mp
lex
inte
ract
ion
s.
Age
if m
ale,
rel
igio
n M
usl
im,
edu
cati
on
, nev
er-
mar
ried
if m
ale.
A
ge if
fem
ale,
rel
igio
n H
ind
u,
ho
use
ho
ld s
ize,
nev
er-m
arri
ed if
fe
mal
e.
R
esu
lts
/ co
ncl
usi
on
s: E
lder
ly w
om
en, n
ever
-mar
ried
wo
men
, an
d H
ind
us
we
re le
ss li
kely
to
vis
it a
ny
pra
ctit
ion
er, w
hic
h m
ay
ind
icat
e le
ss h
ealt
h e
mp
ow
erm
ent
for
thes
e g
rou
ps.
Ob
tain
ing
care
is in
vers
ely
rela
ted
to
ho
use
ho
ld s
ize
and
po
siti
vely
rel
ated
to
ag
e (f
or
men
), e
du
cati
on
, po
or
hea
lth
sta
tus,
an
d im
pai
red
mo
bili
ty.

Ghana The review identified eight studies from Ghana that address access to health services with a focus on non-financial access barriers (Table 2a). Six of the eight studies are based on data from Ghanaian Demographic and Health Surveys (GDHS). The remaining two studies (Buor 2003; Buor 2004) use data from the same cross-sectional survey that was conducted by the author in two districts of the Ashanti Region, one rural and one urban.
Since Ghana embarked on introducing a National Health Insurance Scheme (NHIS) in 2003, financial access barriers have incrementally declined (McIntyre et al. 2008). As the studies show, non-financial factors have also played a major role in reducing barriers. However, most of the studies are too old to reflect any influence the NHIS may have had on promoting access to health care.
Many of the studies done in Ghana – in fact, five of the eight studies – focus on MCH services, including antenatal care, professional support at birth and postnatal care for mother and child and use only data on women aged 15-49. The two studies by Buor (2003 and 2004) focus on general health care access and analyze data on the general adult population. Boateng and Flanagan (2008) also focus on the uptake of general health services, but only analyze women's behavior.

Tab
le 2
a:
Gh
ana
- el
igib
le p
ub
licat
ion
s an
d s
tud
y d
esig
n
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Ad
dai
(2
00
0)
Per
inat
al h
ealt
h
serv
ices
.
Wo
men
1
5-4
9 y
ears
Fa
cto
rs d
ete
rmin
ing
wo
men
’s p
rop
ensi
ty
to u
se m
ater
nal
h
ealt
h s
ervi
ces
in
rura
l Gh
ana.
Gh
ana
Dem
ogr
aph
ic
and
He
alth
Su
rvey
(G
DH
S)
4,5
62
wo
men
1
99
3
Logi
stic
reg
ress
ion
m
od
el, b
ivar
iate
an
d
mu
ltiv
aria
te a
nal
ysis
. (+
)
M
eas
ure
d o
utc
om
es:
Pre
nat
al c
are,
an
ten
atal
ch
eck-
up
, pla
ce o
f d
eliv
ery,
fam
ily p
lan
nin
g.
A
mo
ako
Jo
hn
son
et
al.
(20
09
)
Per
inat
al h
ealt
h
serv
ices
. W
om
en
15
-49
yea
rs
The
exte
nt
of
chan
ges
in s
pat
ial
ineq
ual
itie
s as
soci
ated
wit
h t
ype
of
del
iver
y ca
re in
w
ith
a f
ocu
s o
n
rura
l–u
rban
d
iffe
ren
tial
s w
ith
in
and
acr
oss
3
eco
logi
cal z
on
es
(Sav
ann
ah, F
ore
st
and
Co
asta
l).
GD
HS
A t
ota
l nu
mb
er o
f 2
,34
2
(19
98
) an
d 2
,75
7 (
20
03)
m
oth
ers
wh
o h
ad a
b
irth
(la
st)
in t
he
5
year
s p
rece
din
g th
e
surv
eys
19
98
an
d
20
03
Two
-lev
el
mu
ltin
om
ial
regr
essi
on
. (+
)
M
eas
ure
d o
utc
om
es:
Pla
ce o
f d
eliv
ery.
Bo
ate
ng
&
Flan
agan
2
00
8
Gen
eral
ser
vice
s.
Wo
men
1
5-4
9 y
ears
P
hys
ical
an
d
psy
cho
logi
cal a
cces
s to
hea
lth
car
e.
GD
HS
2
,13
3 w
om
en f
rom
th
e G
DH
S co
up
le’s
d
atas
et
20
03
M
ult
ivar
iate
an
alys
is,
logi
stic
reg
ress
ion
. (+
)
M
eas
ure
d o
utc
om
es:
Sel
f-d
eter
min
atio
n, p
hys
ical
acc
ess,
psy
cho
logi
cal a
cces
s.

3
4
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Bu
or
(20
03
) G
ener
al s
ervi
ces
G
ener
al
po
pu
lati
on
(s
trat
ifie
d b
y ag
e,
sex,
ed
uca
tio
n,
emp
loym
ent,
in
com
e).
Imp
act
of
dis
tan
ce
on
uti
lizat
ion
, an
d
ho
w d
ista
nce
co
mp
ares
wit
h t
rave
l ti
me
and
tra
nsp
ort
co
st -
Ah
afo
-An
o
Sou
th (
rura
l) d
istr
ict
Gh
ana:
cro
ss-
sect
ion
al
surv
ey
cove
rin
g a
dep
rive
d r
ura
l d
istr
ict
Sam
ple
of
40
0 d
raw
n
fro
m 1
,73
2
ho
use
ho
lds
No
t R
epo
rted
M
ult
iple
reg
ress
ion
(s
tep
wis
e).
(+)
M
eas
ure
d o
utc
om
es:
Uti
lizat
ion
of
hea
lth
se
rvic
es.
B
uo
r (2
00
4)
Gen
eral
ser
vice
s P
op
ula
tio
n (
soci
o-
eco
no
mic
ally
an
d
cult
ura
lly d
iver
se)
ove
r 1
8 y
ear
s.
To e
volv
e a
mo
del
of
uti
lizat
ion
by
gen
der
an
d r
eco
mm
end
ef
fect
ive
inte
rven
tio
ns.
Gh
ana:
cro
ss-
sect
ion
al
surv
ey
cove
rin
g tw
o
dis
tric
ts,
Ah
afo
-An
o
Sou
th (
rura
l)
and
Ku
mas
i M
etro
po
lis
(urb
an)
3,1
08
ho
use
ho
lds
(1,7
32
ru
ral,
1,3
76
u
rban
)
Au
g 2
00
0 -
Fe
b
20
01
Mu
ltip
le r
egre
ssio
n
(ste
pw
ise)
. (+
)
M
eas
ure
d o
utc
om
es:
Uti
lizat
ion
of
hea
lth
se
rvic
es.
D
oku
et
al.
(20
12
) P
erin
atal
hea
lth
. W
om
en
15
-49
yea
rs
Fact
ors
det
erm
inin
g ti
min
g o
f an
ten
atal
ca
re v
isit
an
d t
ype
of
del
iver
y as
sist
ance
GD
HS
2,0
99
wo
men
wh
o
rece
ntl
y ga
ve b
irth
Se
p -
N
ov
20
08
Mu
ltiv
aria
te lo
gist
ic
regr
essi
on
. (+
)
M
eas
ure
d o
utc
om
es:
Tim
ing
of
ante
nat
al c
are,
del
iver
y as
sist
ance
.

3
5
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Gyi
mah
et
al.
(20
06
) M
ater
nal
hea
lth
.
Wo
men
1
5-4
9 y
ears
A
sses
sin
g as
soci
atio
n
bet
we
en r
elig
ion
an
d
uti
lizat
ion
of
mat
ern
al h
ealt
h
serv
ices
.
GD
HS
2,0
84
wo
men
wh
o
rece
ntl
y ga
ve b
irth
2
00
3
Bin
ary
and
m
ult
ivar
iate
mo
del
s,
bin
ary
logi
t m
od
els.
(+
)
M
eas
ure
d o
utc
om
es:
Im
mu
niz
atio
n, a
nte
nat
al v
isit
s, d
eliv
ery
at h
ealt
h c
entr
e.
Sm
ith
G
reen
away
et
al. (
20
12
)
Per
inat
al h
ealt
h
serv
ices
, va
ccin
atio
ns.
Wo
men
1
5-4
9 y
ears
R
ole
of
hea
lth
kn
ow
led
ge in
th
e
asso
ciat
ion
bet
we
en
mo
ther
s’ e
du
cati
on
an
d u
se o
f m
ater
nal
an
d c
hild
hea
lth
se
rvic
es.
GD
HS
1,7
80
mo
ther
s fr
om
1
1,7
78
ho
use
ho
lds
20
03
-
20
08
P
rob
it r
egre
ssio
n.
(++)
M
eas
ure
d o
utc
om
es:
Use
of
hea
lth
ser
vice
s, f
orm
al e
du
cati
on
, wo
men
’s h
ealt
h k
no
wle
dge
.

Access barriers: Predisposing factors Boateng and Flannagan (2008), based on the 2003 GDHS data, present an innovative analysis of women’s “physical” and “psychological” access to health care. In addition to considering physical access (geographically close, transportation available), the authors analyzed psychological barriers such as a women's knowledge, a sense of her right to access care, and her subordinate position in family decision making. They took into account a set of predisposing factors, including Akan lineage (i.e. ethnicity) and age. Still, age had no strong effect on either physical or psychological access, but matrilineal lineage had a significant positive effect on physical access. However, this effect was not significant for psychological access. In a separate paper based on the GDHS 1998 and 2003, Buor (2004) investigates gender influence on the utilization of health services in the Ashanti Region. The study demonstrates that despite greater needs, women utilize health services less than males, and income levels have a greater impact on female utilization than on males. Men’s perceived quality of services is more influential on uptake of services as compared to women. Education, distance and service cost strongly affect both male and female service uptake. Still, the effect of these enabling factors is greater on male utilization. The author concludes that gender inequity is apparent in access to health care in Ghana and that poor access is ultimately determined by abject poverty. He also emphasizes the role of education influencing female use of health services and the need to examine this relationship further. The respondents’ religious background as a predisposing factor stands out in Addai’s (2000) multivariate analysis of the GDHS 1993, a survey conducted long before the introduction of the National Health Insurance Scheme (NHIS) in Ghana. Addai distinguishes the following types of maternal health services: prenatal care (provided by a doctor or non-doctor), antenatal care (antenatal check-up 0-3, or more than 3 times, for last birth), place of delivery (medical facility or home), and family planning (use of any contraceptive method). Women who adhere to traditional beliefs use prenatal care and antenatal check-ups significantly less and are far less likely to give birth in an institutional setting than members of other religions. Another study using data from the GDHS 2008 highlights the roles of age and religion on the timing of the first ANC visit and the presence of a trained assistant during delivery (Doku et al. 2012). Christian and Muslim women were more likely to have an assisted delivery than women of traditional faith. The relevance of religion in maternal health service utilization in Ghana is the focus of a study by Gyimah and colleagues (2006) in an analysis utilizing the GDHS 2003 data. Even after controlling for socio-economic variables, results indicate that Christian women are more likely to deliver at a health facility and use antenatal care more frequently than women belonging to other religious groups; women adhering to traditional beliefs make the least use of maternal health services in Ghana. Access barriers: Enabling factors Education is the key focus of a study by Smith Greenaway and colleagues (2012). Their research explores the pathways from mothers’ formal education to use of health services (ANC, delivery services, child vaccination) using data from the GDHS 2008, restricting the sample to mothers who had given birth within the five years preceding the survey and whose children had survived. The

37
results confirm there is a close positive relationship between formal education and health knowledge, depicted by a latent construct based on a set of health-related questions. Each additional year of formal education significantly increases the predicted probability of use of specific services: antenatal care, giving birth with the supervision of a trained professional and complete child vaccination. The analysis further demonstrates that health knowledge is a predictor, independent of the strong influence of household wealth (reflected by an asset index) and husband’s education, two variables that reflect family socioeconomic status. In Boateng and Flannagan (2008) the level of education (entering the analysis as a binary variable) is a significant predictor of physical access. And, the analysis from Addai (2000) also indicates that lack of education dramatically reduces the probability of using MCH services. The author emphasizes the lack of health-related information among the less educated. The study by Doku et al. 2012 also highlights the role of partner’s education on the timing of the first ANC visit and having a trained assistant during delivery. Apart from formal education, mass media, as a potential source of health knowledge, should be considered. Interestingly, Smith Greenaway and colleagues (2012) showed that indicators for women’s access to mass media and media exposure are not associated with use of services. Buor’s study (2003) of health service utilization in a rural district, based on a sample of 400 individuals, examined the impact of distance in light of other predisposing and enabling factors. The study confirms the negative impact of distance to services on utilization and indicates that income, service cost and education are relevant determinants, in order of importance. Income showed a strong positive relationship with utilization, whereas the negative effect of service costs was comparatively weaker. Again, there was a significant positive effect of education on health care utilization. Not surprisingly, Boateng and Flannagan (2008) found urban residence is also a strong determinant of both physical and psychological access. In using two successive rounds of the GDHS 1998 and 2003, Amoako Johnson et al. (2009) found spatial variations in the use of delivery care services at the national level, even though more than half of all births continue to occur at home without skilled obstetric care. The variations occur within rural and urban settings across Ghana’s three ecological zones (Savannah, Forest, Coastal). Differences in services uptake by regions are not pronounced. Results indicate that barriers arise at lower geographical levels and may be specific to the local context. (Addai 2000).
Tab
le 2
b:
Gh
ana
– f
ind
ings
A
uth
or
Bar
rie
rs a
nd
de
term
inan
ts id
enti
fied
P
osi
tive
Co
rre
lati
on
N
ega
tive
Co
rre
lati
on
Ad
dai
(2
00
0)
Fin
anci
al a
nd
no
n-f
inan
cial
fac
tors
det
erm
inin
g w
om
en’s
pro
pen
sity
to
use
mat
ern
al h
eal
th s
ervi
ces
in r
ura
l Gh
ana.
Edu
cati
on
, wo
rk.
Trad
itio
nal
rel
igio
us
bac
kgro
un
d,
livin
g in
ru
ral a
rea.
R
esu
lts
/ co
ncl
usi
on
s: T
he
up
take
of
MC
H s
erv
ices
ten
ds
to b
e sh
aped
mo
stly
by
leve
l of
edu
cati
on
, rel
igio
us
bac
kgro
un
d a
nd
re
gio
n o
f re
sid
ence
, an
d p
arti
ally
by
eth
nic
ity
and
occ
up
atio
n.
Am
oak
o
Joh
nso
n e
t al
. (2
00
9)
Res
iden
tial
are
a d
iffe
ren
ces
as f
acto
rs d
ete
rmin
ing
ineq
ual
itie
s as
soci
ated
wit
h t
ype
of
del
iver
y ca
re in
G
han
a.
Mu
slim
or
Ch
rist
ian
wo
men
, w
om
en f
rom
wea
lth
y b
ackg
rou
nd
, ag
e, e
du
cati
on
, att
end
ed p
ren
atal
ca
re.
Bir
th o
rder
, liv
ing
in r
ura
l are
a.
R
esu
lts
/ co
ncl
usi
on
s: N
o s
ign
ific
ant
chan
ges
bet
we
en 1
99
8 a
nd
20
03
, bu
t la
rge
sp
atia
l dif
fere
nce
s in
Gh
ana
wit
hin
urb
an a
nd
ru
ral
area
s b
etw
een
eco
logi
cal z
on
es.
Bo
ate
ng
&
Flan
agan
20
08
Infl
uen
ce o
f d
emo
grap
hic
var
iab
les
chan
ges
bet
we
en p
hys
ical
acc
ess
an
d p
sych
olo
gica
l acc
ess
Wo
man
's e
du
cati
on
, mat
rilin
y,
nu
mb
er o
f ch
ildre
n u
nd
er 6
, as
sert
ive
atti
tud
e ag
ain
st
vio
len
ce.
Livi
ng
in r
ura
l are
a.
R
esu
lts
/ co
ncl
usi
on
s: T
he
stu
dy
sho
ws
a m
ed
iati
ng
effe
ct o
f ed
uca
tio
n (
in t
he
co
nte
xt o
f p
hys
ical
acc
ess)
an
d u
rban
res
iden
ce o
n
ph
ysic
al a
nd
psy
cho
logi
cal a
cces
s to
hea
lth
car
e. T
he
effe
cts
of
edu
cati
on
on
ph
ysic
al h
ealt
h w
ere
red
uce
d w
ith
th
e in
tro
du
ctio
n o
f th
e va
riab
les
self
de
term
inat
ion
an
d s
oci
al s
up
po
rt. S
imila
rly,
th
e ef
fect
s o
f u
rban
res
iden
ce o
n p
sych
olo
gica
l acc
ess
wer
e r
edu
ced
w
hen
sel
f d
eter
min
atio
n w
as in
tro
du
ced
.
Bu
or
(20
03
) D
ista
nce
to
hea
lth
care
fac
ility
. W
ealt
h, e
du
cati
on
. C
ost
of
serv
ice.
R
esu
lts
/ co
ncl
usi
on
s: R
eco
mm
end
atio
ns
to r
edu
ce d
ista
nce
to
hea
lth
care
fac
ility
, im
pro
ve f
orm
al e
du
cati
on
, an
d r
edu
ce p
ove
rty.

3
9
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Bu
or
(20
04
) Fi
nan
cial
an
d n
on
-fin
anci
al d
ete
rmin
ants
fo
r u
se o
f ge
ner
al h
eal
thca
re s
ervi
ces
by
men
an
d w
om
en.
Edu
cati
on
, qu
alit
y o
f se
rvic
e.
Bei
ng
fem
ale,
dis
tan
ce, s
ervi
ce c
ost
.
R
esu
lts
/ co
ncl
usi
on
s: A
lth
ou
gh f
emal
es h
ave
a gr
eate
r n
eed
fo
r h
ealt
h s
ervi
ces
than
mal
es, t
hey
do
no
t u
tiliz
e h
ealt
h s
ervi
ces
as
mu
ch. W
her
eas
qu
alit
y o
f se
rvic
e, h
eal
th s
tatu
s, s
ervi
ce c
ost
an
d e
du
cati
on
hav
e gr
eate
r ef
fect
on
mal
e u
tiliz
atio
n, d
ista
nce
an
d
inco
me
hav
e h
igh
er im
pac
t o
n f
emal
e u
tiliz
atio
n.
D
oku
et
al.
(20
12
) P
arit
y an
d im
pac
ts o
f fi
nan
cial
an
d n
on
-fin
anci
al
det
erm
inan
ts o
n e
arly
an
ten
atal
car
e u
pta
ke a
nd
tr
ain
ed b
irth
ass
ista
nce
.
Age
, wea
lth
, Ch
rist
ian
or
Mu
slim
re
ligio
n (
and
no
t tr
adit
ion
al),
p
artn
er's
ed
uca
tio
n.
Par
ity.
R
esu
lts
/ co
ncl
usi
on
s: D
esp
ite
the
rela
tive
ly h
igh
an
ten
atal
car
e u
tiliz
atio
n a
mo
ng
Gh
anai
an w
om
en, s
ign
ific
ant
vari
atio
ns
exis
t ac
ross
th
e so
cio
-dem
ogr
aph
ic s
pec
tru
m.
G
yim
ah e
t al
(2
00
6)
Rel
igio
n a
s a
det
erm
inan
t fo
r th
e u
tiliz
atio
n o
f m
ater
nal
hea
lth
ser
vice
s.
Wea
lth
, ed
uca
tio
n, m
on
oga
mo
us
mar
riag
e, e
thn
icit
y A
kan
, Cat
ho
lic
fait
h.
Nu
mb
er o
f liv
ing
child
ren
, liv
ing
in
rura
l are
a, li
vin
g in
no
rth
ern
reg
ion
.
R
esu
lts
/ co
ncl
usi
on
s: O
vera
ll, t
her
e is
evi
den
ce t
hat
MH
ser
vice
uti
lizat
ion
is s
ign
ific
antl
y h
igh
er a
mo
ng
Ch
rist
ian
wo
men
, an
d in
m
ost
cas
es, s
uch
dif
fere
nce
s w
ere
fo
un
d t
o p
ersi
st a
fter
co
ntr
olli
ng
for
ob
serv
ed c
har
acte
rist
ics.
Smit
h
Gre
enaw
ay e
t al
. (2
01
2)
Hea
lth
kn
ow
led
ge a
s a
de
term
inan
t in
th
e as
soci
atio
n b
etw
een
mo
ther
s’ e
du
cati
on
an
d u
se o
f m
ater
nal
an
d c
hild
hea
lth
ser
vice
s.
Mo
ther
s’ f
orm
al e
du
cati
on
, m
oth
er's
hea
lth
kn
ow
led
ge,
fam
ily s
oci
oec
on
om
ic s
tatu
s.
R
esu
lts
/ co
ncl
usi
on
s: E
ach
incr
ease
in t
he
fact
or
sco
re f
or
wo
men
’s e
du
cati
on
an
d h
ealt
h k
no
wle
dge
co
rres
po
nd
s w
ith
an
incr
ease
in
th
e p
red
icte
d p
rob
abili
ty o
f u
se o
f h
ealt
h s
ervi
ces.
Up
on
incl
usi
on
of
dem
ogr
aph
ic a
nd
so
cio
-eco
no
mic
co
ntr
ols
, ass
oci
atio
n
bet
we
en m
oth
ers’
fo
rmal
ed
uca
tio
n a
nd
use
of
hea
lth
ser
vice
s b
eco
mes
no
n-s
ign
ific
ant.

Rwanda In 1999 the Government of Rwanda began establishing Mutuelles, community-based health insurance schemes, as part of the national health strategy to provide universal health coverage. Over the last decade many researchers have studied the impact of Mutuelles on health service utilization and its potential to protect households against catastrophic health expenditure (Schneider and Diop 2005; Lu et al. 2012). Studies on the impact of health insurance or related policy interventions have been systematically presented elsewhere (Bucagu et al. 2012; Giedion et al. 2013) and are not the subject of this review. Only one Rwandan study was identified for review; it examines factors affecting maternal health care seeking behavior and highlights a range of non-financial determinants of access (Chandrasekhar et al. 2011) (Tables 3a and 3b). Access barriers Chandrasekhar et al. (2011) focused on determinants that influence the choice of place for delivery. Based on the data of three Rwandan Demographic and Health Surveys (RDHS) conducted in 1992, 2000 and 2005, descriptive statistics show little increase in deliveries at a health facility between 1992 (26 %), before the genocide, 2000 (26 %) and 2005 (30 %). Further, a multivariate analysis based on the pooled data from the surveys shows a range of statistically significant relationships between predisposing and enabling factors, and the choice of delivery service.4 A woman from a male-headed household is more likely to give birth at a health facility; the likelihood increases with education, age and lower order births (i.e., first birth or women with fewer children). There is a strong positive relationship between the number of antenatal visits and assistance during delivery care; household wealth also promotes delivery at a health facility. Interestingly, women who work − irrespective of paid or unpaid work − were less likely to deliver in a health facility compared to women who are not working. The authors suggest this is because over 70% of the working women were engaged in non-remunerative agriculture, laboring far from services and with less time to access care than their jobless counterparts.
4 The pooling of three surveys is certainly not ideal. Within 13 years relevant parameters are subject to significant changes; these
can be expected to be even more pronounced given Rwanda’s history having resulted in dramatic social change. The interpretation
of a wealth index based on household assets from pooled survey data over a long time span using principal component analysis is
hardly possible.

Tab
le 3
a:
Rw
and
a -
elig
ible
pu
blic
atio
ns
and
stu
dy
des
ign
A
uth
or
Serv
ice
Targ
et
Stu
dy
Qu
esti
on
s D
ata
sou
rce
Po
pu
lati
on
Ti
me
An
alys
is &
Qu
alit
y
Ch
and
rase
khar
e
t al
. (2
01
1)
Mat
ern
al h
ealt
h
(del
iver
y p
lace
).
Mo
ther
s ag
ed
15
–49
Ex
amin
atio
n o
f fa
cto
rs a
ffec
tin
g m
ater
nal
hea
lth
car
e se
ekin
g b
ehav
ior.
Rw
and
a D
emo
grap
hic
an
d H
eal
th
Surv
eys
(RD
HS)
19
92
, 2
00
0, 2
00
5
6,5
51
(1
99
2)
10
,42
1 (
20
00)
1
1,3
21
(2
00
5)
19
92
, 2
00
0,
20
05
Mu
ltiv
aria
te a
nal
ysis
(m
ult
ino
mia
l lo
git
mo
del
).
(++)
M
eas
ure
d o
utc
om
es:
Fac
tors
infl
uen
cin
g ch
oic
e o
f p
lace
of
del
iver
y.
Tab
le 3
b:
Rw
and
a -
fin
din
gs
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Ch
and
rase
khar
e
t al
. (2
01
1)
Fin
anci
al a
nd
no
n-f
inan
cial
det
erm
inan
ts f
or
the
use
o
f m
ater
nal
hea
lth
car
e.
Nu
mb
er o
f an
ten
atal
car
e vi
sits
, w
ealt
h o
f fa
mily
, age
, ed
uca
tio
n,
bir
th o
rder
.
Wo
man
wo
rkin
g, f
emal
e h
ead
ed
ho
use
ho
ld, b
irth
ord
er, l
ivin
g in
ru
ral
area
.
R
esu
lts
/ co
ncl
usi
on
s: A
nte
nat
al c
are
sho
uld
be
imp
rove
d t
o in
crea
se u
pta
ke o
f p
rofe
ssio
nal
hel
p a
t b
irth
. War
/gen
oci
de
has
led
to
m
any
fem
ale
hea
ded
ho
use
ho
lds
that
ten
d t
o a
void
hea
lth
car
e fo
r b
irth
(la
ck o
f re
sou
rces
, op
po
rtu
nit
y co
sts)
.
Vietnam Eight very diverse studies were identified for Vietnam (Table 4a); a country whose health system has been subject to dramatic changes over the past 25 years. After a period of deregulation in the 1990s, following the introduction of Doi Moi, and rapid economic growth, private provision of services has continuously gained momentum. Within the four levels of public service provision (the central level with central and regional hospitals, the provincial level, the district and the commune level), staff is allowed to practice privately after working hours. Analysis of public versus private service provision plays a role in most of the studies reviewed. A recent comprehensive analysis of inequalities in health outcomes, conducted on behalf of UNICEF, describes how a moderate degree of inequality in child mortality in Vietnam has persisted since the early 1990s, despite reductions in overall infant mortality rates during this period, disfavoring poorer women and their children (Knowles et al. 2009). Of the eight studies reviewed, seven (Do 2009, Duong et al 2004, Goland et al 2012, Hong et al 2003, Ngo and Hill 2011, Sepehri et al 2008b and Thang et al 2007) examined MCH interventions, and one, Sepehri et al (2008a), general health services. A broad range of surveys was utilized, including the Vietnam National Household Survey, Vietnam Demographic and Health Surveys and the Multiple Indicator Cluster Survey (MICS 3). Hong et al (2003) used cross-sectional household survey data from 1998-1999, all remaining studies used data collected after 2000.

Tab
le 4
a:
Vie
tnam
- e
ligib
le p
ub
licat
ion
s an
d s
tud
y d
esig
n
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Do
(2
00
9)
Per
inat
al h
ealt
h
(ski
lled
bir
th
atte
nd
ant)
Wo
men
1
5-4
9 y
ears
Fa
cto
rs r
elat
ed t
o
wo
men
’s d
ecis
ion
to
h
ave
skill
ed b
irth
at
ten
dan
t an
d
wh
eth
er it
was
a
pu
blic
or
pri
vate
se
cto
r p
rovi
der
.
Vie
tnam
D
emo
grap
hic
an
d H
eal
th
Surv
ey
13
05
mo
ther
s o
f si
ngl
e
live
bir
ths
in t
he
pre
vio
us
3 y
ears
.
19
99
-
20
02
M
ult
ivar
iate
logi
stic
re
gres
sio
ns,
mu
lti-
leve
l mo
del
. (+
)
M
eas
ure
d o
utc
om
es:
Use
of
skill
ed b
irth
att
end
ants
in p
riva
te a
nd
pu
blic
sec
tor.
Du
on
g e
t al
. (2
00
4)
Per
inat
al h
ealt
h
Wo
men
1
5-4
9 y
ears
In
vest
igat
ion
of
fact
ors
th
at in
flu
ence
th
e u
tiliz
atio
n o
f d
eliv
ery
serv
ices
at
the
pri
mar
y h
ealt
h
care
leve
l (C
HC
) in
ru
ral V
ietn
am.
No
t re
po
rted
2
00
wo
men
wh
o h
ad
give
n b
irth
in p
ast
3
mo
nth
s.
Jun
–A
ug
20
00
Mu
ltiv
aria
te lo
gist
ic
regr
essi
on
an
alys
is
(mix
ed m
eth
od
s).
(+)
M
eas
ure
d o
utc
om
es:
Pai
d c
ost
s an
d a
cces
s to
ser
vice
s, p
erce
ived
qu
alit
y o
f se
rvic
es, d
emo
grap
hic
s, a
nd
rel
ated
info
rmat
ion
. G
ola
nd
et
al.
(20
12
) M
ater
nal
hea
lth
W
om
en
15
-49
yea
rs
Uti
lizat
ion
of
ante
nat
al c
are
an
d
skill
ed b
irth
at
ten
dan
ce in
re
lati
on
to
so
cial
d
eter
min
ants
to
re
veal
ineq
uit
ies
and
id
enti
fy
dis
adva
nta
ged
gr
ou
ps.
Mu
ltip
le
Ind
icat
or
Clu
ster
Su
rvey
(M
ICS
3).
1,0
23
inte
rvie
wed
w
om
en w
ho
had
giv
en
bir
th t
o a
live
ch
ild t
wo
ye
ars
pre
ced
ing
the
su
rvey
.
20
06
M
ult
ivar
iate
an
alys
es, s
trat
ifie
d
logi
stic
reg
ress
ion
, G
-co
mp
uta
tio
n.
(++)
M
eas
ure
d o
utc
om
es:
An
ten
atal
car
e c
ove
rage
an
d s
kille
d b
irth
att
end
ance
.

4
4
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Ho
ng
et
al.
(20
03
) C
hild
ho
od
an
d in
fan
t m
ort
alit
y C
hild
ren
C
har
acte
rist
ics
asso
ciat
ed w
ith
th
e
use
of
hea
lth
se
rvic
es f
or
the
tr
eatm
ent
of
child
ho
od
dia
rrh
ea in
3
so
uth
ern
pro
vin
ces
Cro
ss-
sect
ion
al
ho
use
ho
ld
clu
ster
su
rvey
s.
1,9
35
ch
ildre
n u
nd
er 5
ye
ars,
1
,63
2 m
oth
ers
(72
0 h
ou
seh
old
s).
No
v 1
99
8 -
Ja
n
19
99
Un
i-va
riat
e an
alys
es
and
a C
ox
pro
po
rtio
nal
haz
ard
m
od
el.
(+)
M
eas
ure
d o
utc
om
es:
Up
take
of
trea
tmen
t fo
r d
iarr
hea
. N
go &
Hil
l (2
01
1)
Rep
rod
uct
ive
he
alth
an
d f
amily
pla
nn
ing
Wo
men
1
5-4
9 y
ears
Ex
plo
res
soci
o-
dem
ogr
aph
ic
det
erm
inan
ts o
f R
H
serv
ice
uti
lizat
ion
at
the
CH
S le
vel.
Cro
ss-
sect
ion
al
surv
ey
Vie
tnam
67
8 w
om
en (
48
%)
in
Vin
h L
on
g an
d 7
39
w
om
en (
52
%)
in T
hu
a Th
ien
Hu
e.
Ap
r -
May
2
01
0
Mu
ltip
le lo
gist
ic
regr
essi
on
an
alys
es.
(+)
M
eas
ure
d o
utc
om
es:
Fam
ily p
lan
nin
g se
rvic
e u
se, a
nte
nat
al c
are
serv
ice
use
, del
iver
y se
rvic
e u
se, g
ynae
colo
gica
l ch
eck
-up
ser
vice
use
.
Sep
ehri
et
al.
(20
08
a)
Gen
eral
he
alth
se
rvic
es
Ind
ivid
ual
s ag
e 6
an
d o
lder
In
flu
ence
of
ind
ivid
ual
an
d
ho
use
ho
ld-l
evel
fa
cto
rs o
n t
he
use
of
hea
lth
car
e s
ervi
ces.
Vie
tnam
N
atio
nal
H
ou
seh
old
Su
rvey
.
30
,96
0 h
ou
seh
old
s w
ho
h
ad r
epo
rted
an
illn
ess
wit
hin
a 4
-we
ek r
ecal
l p
erio
d
20
01
-2
00
2
Mu
lti-
leve
l (ra
nd
om
in
terc
ept)
logi
stic
m
od
el.
(++)
M
eas
ure
d o
utc
om
es:
Th
e u
se o
f h
ealt
h c
are
serv
ices
by
ind
ivid
ual
s an
d b
y h
ou
seh
old
s.
Sep
ehri
et
al.
(20
08
b)
Mat
ern
al h
ealt
h
serv
ices
W
om
en 1
2-4
9
year
s w
ho
gav
e b
irth
wit
hin
pas
t fi
ve y
ears
Infl
uen
ce o
f in
div
idu
al,
ho
use
ho
ld-
and
co
mm
un
e-le
vel
fact
ors
on
use
of
pre
nat
al h
ealt
h
serv
ices
an
d t
he
ch
oic
e b
etw
een
h
om
e b
irth
at
a h
ealt
h f
acili
ty.
Vie
tnam
N
atio
nal
H
ou
seh
old
Su
rvey
.
9,4
00
wo
men
age
d 1
5-
49
wh
o h
ad g
iven
bir
th
in t
he
pas
t 5
ye
ars
plu
s in
terv
iew
s w
ith
clin
ics
20
01
-
20
02
M
ult
i-le
vel (
ran
do
m
inte
rcep
t) lo
gist
ic
mo
del
. (+
+)
M
eas
ure
d o
utc
om
es:
An
ten
atal
car
e a
nd
giv
ing
bir
th a
t a
hea
lth
fac
ility

4
5
Au
tho
r Se
rvic
e Ta
rge
t St
ud
y Q
ues
tio
ns
Dat
a so
urc
e P
op
ula
tio
n
Tim
e A
nal
ysis
& Q
ual
ity
Than
g e
t al
. (2
00
7)
Vac
cin
atio
n
Ch
ildre
n
Det
erm
ine
ove
rall
per
form
ance
an
d
ineq
ual
itie
s in
th
e im
mu
niz
atio
n o
f ch
ildre
n in
Vie
tnam
.
Vie
tnam
D
emo
grap
hic
an
d H
eal
th
Surv
ey.
Mo
ther
s o
f 3
,09
2
child
ren
. 1
99
7
and
2
00
2
Des
crip
tive
an
alys
is
and
m
ult
i-le
vel l
ogi
stic
re
gres
sio
n.
(+)
M
eas
ure
d o
utc
om
es:
Im
mu
niz
atio
n

The studies conducted reveal similar patterns of predisposing and enabling factors. Different studies using data from the Vietnam Demographic and Health Surveys highlight the same interrelationships of individual and household-related access factors and health service uptake (Table 4b). Access barriers: Predisposing factors Among the individual characteristics identified as predisposing factors, ethnicity is a recurring theme. Do (2009) finds that professionally attended childbirths are more likely if the mother is of Kinh (Vietnamese) descent or if she is a member of a religious group (Buddhist or other). Birth order matters; with an increasing number of births, the likelihood of giving birth in an institutional environment diminishes. The significance of ethnicity as a predictor of health service utilization was demonstrated in a study using a cross-sectional household survey conducted between November 1998 and January 1999 in three southern provinces, with a focus on childhood diarrhea (Hong et al. 2003). While maternal ethnicity had the strongest effect on mothers seeking advice on treatment for children with diarrhea (Kinh mothers were more than twice as likely to seek health care for their child as mothers of ethnic minorities), maternal education and disease severity were also important predictors of service uptake. A small-scale study applying a mixed-method approach (Duong et al. 2004) explored factors determining the perceived quality of services at a health setting, i.e., a commune health center or district hospital, and influencing the delivery choice option. The sample comprised 200 women from Quang Xuong District in Thanh Hoa Province who had given birth within three months prior to the survey. The logistic regression analysis shows that women with a higher level of education were more likely to choose an institutional setting for delivery, more likely to choose an institutional birth for their first child, and women living with an extended family were more likely to give birth at home. While the surveys shed some light on the role of perceived quality as a determinant of choice (the perceived quality of the services offered at commune health centers is significantly higher among users than among women delivering at home), the underlying root causes only become apparent in the qualitative components of the study. Regarding the choice of delivery place, a comprehensive study of individual, household and commune characteristics, found that Kinh women are nearly four times as likely as ethnic minorities to give birth at health facilities (Sepehri 2008b). Other important explanatory variables include household income, urban residence, the communal poverty rate and distance to the nearest hospital. A later study conducted in two provinces (surveying 739 women in Thua Thien Hue and 678 in Vinh Long) examined reproductive health and family planning service utilization and found that many women “bypassed” commune health centers (Ngo and Hill 2011). Interestingly, higher birth order was positively correlated with the use of the local commune health center, just as belonging to an ethnic minority (for delivery only). The relationship between service utilization and birth order was unexpected since studies typically report higher levels of service for first and lower

47
order births, as compared to higher order births where women are more experienced in delivery (Moyer 2013).
Goland and colleagues (2012) dig deeper and develop a causal effects model inspired by a conceptual model authored by the Commission on Social Determinants of Health (CSDH). The study uses data from the Multiple Indicator Cluster Survey (MICS) conducted in Vietnam in 2006. Recognizing that social determinants of health inequities are complex and interactive, the authors distinguish structural determinants − such as education, ethnicity and wealth − and intermediary determinants − such as living area, maternal age at delivery and marital status − to explain the choice of skilled birth attendance and antenatal care attendance. Using logistic regression to separate structural and intermediary determinants, the authors perform G-computation as a method to estimate causal inference. The results show that maternal health care utilization in 2006 was highly inequitable, as determined by ethnicity, education and wealth. The stratified analysis outlines the effects along different pathways. While the role of ethnicity varies, the most striking result is the high relevance of ethnicity as a determinant of health service uptake. Access barriers: Enabling factors Do (2009), using data from the VDHS 2002, confirms that the higher a woman’s level of education, the more likely it is she will deliver in an institutional environment. Based on data from the VDHS 1997 and 2002, Thang and colleagues (2007) analyze barriers to immunization coverage in Vietnam. Overall, the percentage of fully immunized children aged 11 to 23 months has increased from 50.2 % to 66.7 % in the five-year period between the two surveys. The authors employ alternative logistic regression models that take into account interactions between socioeconomic status and other variables. The study finds that neither gender, nor birth order had any effect on the likelihood of a child being fully immunized; however, mother’s education is an important determinant. The eligible studies for Vietnam indicate once more that enabling factors cannot be viewed independent of predisposing individual factors since there are close interlinkages. Sepehri and colleagues use data from the Vietnam National Health Survey 2001-02 in two papers on determinants of health service uptake (Sepehri et al. 2008a, 2008b). Their first study (Sepehri et al. 2008a) assesses the influence of individual and household-level factors on the use of general health care services (four-week recall period) using a multilevel logistic regression model. The approach indicates a high degree of homogeneity in seeking treatment among persons within a household; in other words, the effect of an enabling household factor influences all individual household members in the same manner. This study also takes into account insurance status. The three health insurance schemes − compulsory, voluntary and the insurance scheme for the poor − promote the uptake of health services; though the influence of compulsory insurance is strongest. As indicated in many studies, our findings suggest that the likelihood of using health services in the case of illness increases with the level of education and socioeconomic status. Additionally, the severity of the underlying illness determines uptake; a new chronic illness strongly influences the likelihood of service utilization. The researchers’ second study (Sepehri et al. 2008b) evaluates the

48
importance of individual, household and commune characteristics as determinants of maternal health services uptake. The authors use a random intercept model (rather than a standard binary regression model, such as a logistic model) to depict the dependence among community members’ health seeking behavior. This approach eliminates any bias that would arise from the assumption that unobserved community characteristics are correlated with the likelihood of commune members seeking care.5 A woman’s decision to utilize prenatal care is modeled using a hurdle (or two-parts) model to reflect the two separate processes of deciding whether to use services and, if so, to what extent. There is only a small influence of the mother’s insurance status on the utilization of prenatal care, but it is strongly influenced by the mother’s education level. The household’s economic status (“income”) has a strong effect on the likelihood of a mother utilizing prenatal care. Interestingly, in contrast to other studies, there is no significant effect of ethnicity on prenatal use, once other individual, household and commune characteristics are accounted for. Beyond this, only health insurance for the poor increases the extent of use, i.e. the frequency of antenatal visits. Household wealth, as already mentioned in relation to the comprehensive study by Goland and colleagues (2012), consistently stands out in household survey analysis as the single most important enabling factor for MCH services. Do (2009) finds a positive significant relationship between wealth (based on a pre-calculated asset index) and the uptake of delivery services by any provider. Community-level variables confirm that distance matters. Proximity of a public sector health center reduces the likelihood of using private sector services. Thang and colleagues (2007) find there is a positive correlation between the mother’s regular TV consumption and fully immunized children. However, no conclusion can be drawn regarding whether this is due to the success of TV campaigns, or whether TV consumption in this context merely reflects another indicator of socioeconomic context. Their analysis also shows once more that poverty and rural residence predict a low probability of full immunization. Ngo and Hill (2011) identify working as a farmer and being poor as the main indicators of low access to quality health services. Private practice, where clients have access to higher grades of care and perceive better quality, appears to be the provider of choice for those more affluent.
5 The logistic random-intercept model treats commune-level unobserved heterogeneity in the same way that observed
heterogeneity is modeled - by adding a random intercept to the logistic linear predictor.

Tab
le 4
b:
Vie
tnam
– f
ind
ings
A
uth
or
Bar
rie
rs a
nd
de
term
inan
ts id
enti
fied
P
osi
tive
Co
rre
lati
on
N
ega
tive
Co
rre
lati
on
Do
(2
00
9)
Dif
fere
nt
ind
ivid
ual
an
d c
om
mu
nit
y-le
vel v
aria
ble
s A
nte
nat
al c
are
visi
ts, e
du
cati
on
, co
mm
un
ity
wea
lth
, pro
xim
ity
of
pu
blic
hea
lth
cen
ter,
ho
use
ho
ld
wea
lth
.
Eth
nic
ity,
ord
er o
f ch
ild b
irth
.
R
esu
lts
/ co
ncl
usi
on
s: T
he
up
take
of
MC
H s
erv
ices
ten
ds
to b
e sh
aped
mo
stly
by
leve
l of
edu
cati
on
, rel
igio
us
bac
kgro
un
d a
nd
re
gio
n o
f re
sid
ence
, an
d p
arti
ally
by
eth
nic
ity
and
occ
up
atio
n.
Du
on
g e
t al
. (2
00
4)
Fin
anci
al a
nd
no
n-f
inan
cial
fac
tors
th
at in
flu
ence
th
e u
tiliz
atio
n o
f d
eliv
ery
serv
ices
at
the
pri
mar
y h
ealt
h
care
leve
l (C
HC
) in
ru
ral V
ietn
am.
Wea
lth
, ed
uca
tio
n, b
ein
g
mar
ried
, lik
elih
oo
d o
f co
mp
licat
ion
s d
uri
ng
bir
th.
Wo
men
livi
ng
wit
h e
xten
de
d f
amily
, o
rder
of
child
bir
th, 1
99
3 N
atio
nal
P
op
ula
tio
n P
olic
y, n
o f
amily
mem
ber
s ab
le t
o t
ake
tim
e o
ff w
ork
to
ac
com
pan
y m
oth
er t
o C
HC
, nee
d t
o
wo
rk in
th
e fi
eld
up
to
del
iver
y, lo
w
per
ceiv
ed q
ual
ity
of
care
in C
HC
, CH
C
clo
se t
o a
pla
ce a
sso
ciat
ed w
ith
d
emo
ns,
pre
fere
nce
of
mo
ther
or
mo
ther
in la
w f
or
ho
me
bir
th.
Re
sult
s /
con
clu
sio
ns:
Dis
tan
ce f
rom
clin
ic h
ad n
o im
pac
t o
n u
se. C
lien
t-p
erc
eive
d q
ual
ity
of
serv
ices
an
d s
oci
o-c
ult
ura
l an
d
eco
no
mic
fac
tors
, rat
her
th
an g
eogr
aph
ical
acc
ess,
can
aff
ect
th
e u
tiliz
atio
n o
f d
eliv
ery
serv
ices
Go
lan
d e
t al
. (2
01
2)
Soci
al d
eter
min
ants
wit
h t
he
aim
to
rev
eal h
eal
th
ineq
uit
ies
and
iden
tify
dis
adva
nta
ged
gro
up
s w
ith
re
gard
to
th
e u
pta
ke o
f m
ater
nal
hea
lth
car
e in
ru
ral
Vie
tnam
.
Edu
cati
on
, wea
lth
. Et
hn
icit
y.
R
esu
lts
/ co
ncl
usi
on
s: A
dju
sted
fo
r liv
ing
area
, ed
uca
tio
n, w
ealt
h a
nd
eth
nic
ity
(Kin
h/C
hin
ese)
wer
e a
ll si
gnif
ican
tly
asso
ciat
ed
wit
h
ante
nat
al c
are
co
vera
ge. 2
5%
of
the
cau
sal e
ffec
t o
f et
hn
icit
y o
n s
kille
d b
irth
att
end
ance
an
d 1
8%
on
an
ten
atal
car
e a
tten
dan
ce
wer
e n
ot
du
e to
po
vert
y.

5
0
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Ho
ng
et
al.
(20
03
) D
eter
min
ants
ass
oci
ated
wit
h t
he
use
of
he
alth
se
rvic
es f
or
the
tre
atm
ent
of
child
ho
od
dia
rrh
ea in
th
ree
so
uth
ern
pro
vin
ces
of
Vie
tnam
.
Mat
ern
al e
thn
icit
y is
Kin
h,
mat
ern
al e
du
cati
on
, se
veri
ty o
f d
isea
se.
R
esu
lts
/ co
ncl
usi
on
s: T
he
stro
nge
st e
ffec
t w
as f
rom
mat
ern
al e
thn
icit
y, w
ith
mo
ther
s fr
om
th
e K
inh
eth
nic
gro
up
bei
ng
mo
re t
han
tw
ice
as li
kely
to
see
k h
ealt
h c
are
for
thei
r ch
ild t
han
mo
ther
s fr
om
eth
nic
min
ori
ties
.
Ngo
& H
ill
(20
11
) Fi
nan
cial
an
d n
on
-fin
anci
al d
ete
rmin
ants
fo
r th
e u
pta
ke o
f m
ater
nal
he
alth
ser
vice
s an
d t
hei
r ch
oic
e o
f p
rovi
der
s (p
riva
te-p
ub
lic).
Use
of
CH
S in
ru
ral a
rea,
dis
tan
ce
to p
riva
te s
ervi
ce, C
HS
staf
fed
by
a d
oct
or,
rel
igio
n is
Bu
dd
his
t, b
irth
o
rder
, pro
vin
ce T
hu
a Ti
en H
ue.
Wo
man
wo
rks
in n
on
-agr
icu
ltu
ral
sect
or,
livi
ng
in u
rban
are
a, in
com
e.
R
esu
lts
/ co
ncl
usi
on
s: W
om
en w
ho
wer
e f
arm
ers,
ear
nin
g a
low
er in
com
e, h
avin
g m
ore
th
an 2
ch
ildre
n, a
nd
livi
ng
in a
ru
ral a
rea
wer
e m
ore
like
ly t
han
oth
ers
to u
se A
NC
, del
iver
y, a
nd
/or
gyn
aeco
logi
cal c
he
ck-u
p s
ervi
ces
at t
he
CH
S ra
ther
th
an a
t p
riva
te
pro
vid
ers.
Wo
men
's c
ho
ice
of
pro
vid
ers
for
FP a
nd
RH
ser
vice
s th
at h
elp
th
em p
lan
an
d p
rote
ct t
hei
r p
regn
anci
es is
dri
ven
by
soci
o-
eco
no
mic
fac
tors
.
Sep
ehri
et
al.
(20
08
a)
Ob
serv
ed in
div
idu
al-
and
ho
use
ho
ld-l
evel
ch
arac
teri
stic
s as
wel
l as
un
ob
serv
ed h
ou
seh
old
-le
vel e
ffec
ts.
Hea
lth
insu
ran
ce, i
nco
me,
se
veri
ty o
f ill
nes
s, p
rese
nce
of
you
ng
child
ren
in t
he
ho
use
ho
ld.
Mem
ber
s o
f h
ou
seh
old
sic
k.
R
esu
lts
/ co
ncl
usi
on
s: T
he
vari
abili
ty im
plie
d b
y th
e u
no
bse
rvab
le h
ou
seh
old
-lev
el e
ffec
ts o
utw
eigh
s th
e va
riab
ility
imp
lied
by
the
ob
serv
ed c
ova
riat
es, i
nd
icat
ing
a h
igh
deg
ree
of
ho
mo
gen
eity
in h
eal
th-s
eeki
ng
beh
avio
r am
on
g th
e h
ou
seh
old
mem
ber
s.
Sep
ehri
et
al.
(20
08
b)
Infl
uen
ce o
f in
div
idu
al, h
ou
seh
old
- an
d c
om
mu
ne-
leve
l fac
tors
on
th
e u
se o
f p
ren
atal
hea
lth
ser
vice
s an
d o
n t
he
cho
ice
be
twe
en g
ivin
g b
irth
at
ho
me
or
at a
he
alth
fac
ility
.
Wea
lth
, ed
uca
tio
n, b
ein
g o
f K
inh
et
hn
icit
y, h
avin
g co
mp
uls
ory
h
ealt
h in
sura
nce
, an
ten
atal
car
e
visi
ts, w
ealt
h o
f co
mm
un
ity.
Dis
tan
ce t
o h
ealt
h f
acili
ty.
R
esu
lts
/ co
ncl
usi
on
s: P
ren
atal
car
e an
d d
eliv
ery
assi
stan
ce is
lim
ited
by
ob
serv
ed b
arri
ers
such
as
low
inco
me,
low
ed
uca
tio
n,
eth
nic
ity,
geo
grap
hic
al is
ola
tio
n a
nd
a h
igh
po
vert
y ra
te in
th
e co
mm
un
ity.
Th
e e
xist
ing
safe
mo
ther
ho
od
pro
gram
s sh
ou
ld b
e lin
ked
wit
h t
he
ob
ject
ives
of
soci
al d
evel
op
men
t p
rogr
ams
such
as
po
vert
y re
du
ctio
n, a
nd
th
at p
olic
y m
aker
s n
eed
to
vie
w b
oth
th
e in
div
idu
al a
nd
th
e co
mm
un
e as
ap
pro
pri
ate
un
its
for
po
licy
targ
eti
ng.

5
1
Au
tho
r B
arri
ers
an
d d
ete
rmin
ants
iden
tifi
ed
Po
siti
ve C
orr
ela
tio
n
Ne
gati
ve C
orr
ela
tio
n
Than
g e
t al
. (2
00
7)
Fin
anci
al a
nd
no
n-f
inan
cial
det
erm
inan
ts f
or
imm
un
izat
ion
leve
ls o
f ch
ildre
n.
Wea
lth
, mo
the
r's
edu
cati
on
, m
oth
er w
atch
es t
elev
isio
n
regu
larl
y.
Livi
ng
in r
ura
l are
a, b
elo
ngi
ng
to
eth
nic
min
ori
ty, b
irth
ord
er.
R
esu
lts
/ co
ncl
usi
on
s: P
oo
r h
ou
seh
old
s, m
ino
rity
ch
ildre
n, c
hild
ren
in r
ura
l are
as, a
nd
esp
eci
ally
ch
ildre
n w
ith
a c
om
bin
atio
n o
f b
ein
g p
oo
r an
d a
min
ori
ty, w
ere
gro
up
s w
her
e im
mu
niz
atio
n c
ou
ld b
e im
pro
ved
to
nar
row
th
e g
ap in
fu
ll im
mu
niz
atio
n.

DISCUSSION
The objective of the literature review is to synthesize existing evidence on explanatory quantitative models, not limited to the analysis of financial access barriers, but rather highlighting non-financial barriers to health service access. The systematic selection identified studies that clearly focus on non-financial factors and service uptake rather than health outcomes. Most of the studies focus on MCH services which are particularly well suited to the analysis of non-financial barriers since the need for these service can be anticipated and are often relatively affordable (with the exception of a few interventions to reduce maternal mortality, such as management of the complications of pregnancy). Establishing an objective need for service utilization is otherwise a complex task and determinants driving service for unforeseen needs differ. This is demonstrated by comparing the findings of the Sepehri studies (2008a and 2008b) that utilize the same data set, one study addressing general treatment seeking and the other analyzing uptake of maternal care. The cause or the type of need matters and influences the uptake of services. Most of the studies included in this review under the theme of access barriers do not specifically use this term. They mainly discuss the concept in terms of utilization of health services and underlying determinants. There is merely a notional or theoretical link to access barriers, with utilization as a proxy for access. Similarly, equity implications can be derived from coverage discussed in terms of individual and household characteristics. Several studies classify variables as predisposing or enabling factors. Although, variables are not always easily or consistently categorized among studies, the range of variables is largely similar, due in part to the large number of studies using DHS data sets. Although most data sources are reported at the national level, there is abundant evidence to indicate that local context matters, albeit many barriers were common across countries, e.g. lack of education. There are many common themes between the findings of this review and those of the parallel qualitative review (Bedford et al. 2013). Whereas the barriers identified in the qualitative review were structured into six thematic areas (perception of condition, home management and local treatment, influence of family or community, lack of autonomy and agency to act, physical accessibility, health facility/biomedical deterrents), no clear theme arises in the quantitative review of individual or household variables. However, the quantitative evidence substantiates the qualitative findings. Rural-urban differences in MCH service utilization are most obvious in the Ghanaian studies. In addition to geographical considerations, other local factors give rise to access barriers, such those related to spatial and sociocultural differences; but quantitative analysis provides limited insight as to the underlying reasons. On the other hand, qualitative studies offer some explanations, such as in the Ghanaian studies that suggest travelling to a distant health facility is not only concerned with geographic movement, but also with social movement (Bedford et al. 2013). Moreover, in Bangladesh and Vietnam, the role of local context becomes clear as ethnicity and religious affiliation constitute significant factors of health service uptake, findings richly illustrated in the qualitative research.

53
Non-financial and financial barriers are often evaluated separately. Many of the studies interpret household wealth as one enabling factor. Yet, there is a complex relationship between material status, psychosocial circumstances and behavioral factors. Goland et al. (2012) addresses these complexities and furthermore, highlights that apart from other factors and interactions, ethnicity constitutes a risk in itself, strengthening the argument that local context matters. Other studies ignore the interactions between enabling factors, apart from designating a specific subset of variables as predisposing to imply variables can act jointly to define a socioeconomic position that limits an individuals or households freedom of action. Just as research focused on economic aspects of health equity often ignores the non-financial sphere, research on determinants of health service utilization often do not consider the influence of financial barriers. The breadth of findings indicates that local context ought to be considered when designing conceptual frameworks to guide analysis and shape policy at different health system levels. The Frenz-Vega model (Frenz and Vega 2010) provides a framework for the conceptualization of equity of access, taking into account the different elements of relevance. It highlights the determinants of unmet needs in a health systems context. This review demonstrates that large parts of these unmet needs arise from non-financial barriers that can only partly be addressed at the national policy level, requiring interventions at lower administrative levels. As discussed, barriers arise as a manifestation of lack of fit between need and services along different dimensions. The studies reviewed have mainly been concerned with predisposing and enabling factors associated with potential patients or clients. Most of these factors cannot be influenced directly by health policy interventions. And yet, these factors still need to be taken into account in policy design. There is obvious room for improvement in all four countries when it comes to the above-mentioned “fit” within the separate access dimensions. Strategies should be guided by an understanding of the local context of access barriers, acknowledging that barriers are dynamic. The Frenz-Vega model could be amended to conceptualize and incorporate health policy to directly address the level where health services and their potential users interact. This is the level at which barriers arise. The amended model would allow for the development of evidence-based strategies to reduce economic, social and cultural distance between providers and patients and achieve UHC with equity. Barriers and survey data - limits of the data sources The identification of access barriers using household surveys is not straight forward. First, access to health services can only be approximated by analyzing service uptake. In their seminal paper, Andersen and Aday (1974) characterize utilization (along with satisfaction) as an “outcome indicator” of access. Neither the underlying need, nor the degree of autonomy in the decision underlying utilization, is satisfactorily captured by survey variables. Second, the barrier itself, as a manifestation of the lack of fit between the underlying need and the service, is not reflected in the household survey variables; the variables rather describe particular aspects of the socio-economic and socio-cultural background that promote barriers.

54
By providing a broad set of variables that can be conceptualized as predisposing and enabling factors of health care utilization, household surveys only provide one side of the access paradigm. The interpretation of all variables in the respective survey requires a good understanding of service provision in context. And, the interpretation of a particular variable may change with context, e.g. the significance of education in a rural vs. urban settings. Evidence from qualitative research highlights some areas that are relevant, but not addressed in household surveys. Areas that are largely the exclusive domain of qualitative research include information that cannot easily be captured quantitatively, such as emotions, e.g. shame and guilt in the context of health service utilization, or knowledge and awareness. Other information may well be available in routine surveys, but has not yet been fully analyzed. Qualitative research on decision-making autonomy, the lack thereof and the potential root causes, has been described to some degree in the Bedford’s review (Bedford et al. 2013). The corresponding household structures and linked variables, as captured in surveys from the focus countries, have not been analyzed in the context of health equity. The analysis of non-financial access barriers on the basis of a national household survey can only provide limited results to guide further quantitative and/or qualitative analysis at sub-national and sub-provincial levels. The review of studies in the four focus countries shows that a) non-financial access barriers play an important role in explaining service uptake; b) there are important predisposing, enabling and need factors that can be expected to vary widely according to local context; and c) factors interact in complex ways. Quantitative studies focused on non-financial barriers do not shed enough light on access barriers to allow for the derivation of targeted policy guidelines. This implies that smaller scale surveys, targeted to pre-identified problem areas, should routinely complement large scale surveys in order to generate information on barriers and guide strategies to strengthen services at lower administrative levels. When it comes to non-financial barriers, geographical barriers are typically a primary focus since an objective of health systems strengthening is to make services physically accessible. Yet, in the context of the reviewed literature, spatial analysis has not played a major role due to the limited availability of spatial data in surveys. As mentioned above, certain standardized health surveys, such as the DHS and MICS, do not allow for analysis of monetary factors due to lack of detailed income, expenditure and cost information, which is typically found in household expenditure surveys (HES). This limits the opportunity to analyze the relative role and interactions of monetary factors identified in HES with non-financial access barriers. In the context of access barriers, it is useful to distinguish household wealth (assessed on the basis of particular household characteristics and durables) from liquid assets that can easily be converted to cover cash payments (for user fees, copayments and other costs associated with utilizing health services). This sets the household asset measure as distinct from the affordability dimension (Howe et al. 2009).

55
A final observation relates to the time lag between data collection and publication. In many of the publications, the time lag was substantial enough to reduce the potential relevance of survey analysis in a health policy context. Selected approaches - methodological constraints and pitfalls The methodological approaches applied in the studies are mainly restricted to standard multivariate analysis. Few studies were based on an explicit conceptual framework or analytical model (e.g. Rahman et al. 2008, Young et al. 2006 for Bangladesh; Goland et al. 2012 for Vietnam) and few explicitly acknowledge the relevant sequence of care seeking. Moreover, few publications include a discussion of the study limitations or potential sources of bias Clinical need is rarely captured. As indicated, MCH lends itself to health equity analysis because a concrete need for services is more apparent than is the case for many other health services. In the analysis of equity in the delivery of general health services, it is difficult to precisely establish the level of need in terms the type and severity of illness. Authors acknowledge that measures of health seeking behavior are influenced by recall bias and limited to reported illness and treatment action, rather than “directly observed as the illness process unfolds” (Ahmed et al. 2001). Occasionally, authors determine their own paradigm and create a particular terminology. For example, in a Ghanaian study, Boateng and Flanagan (2008) present an analysis of GDHS 2003 data that includes a set of derived exogenous variables into a model to predict “physical” and “psychological” access. The dependent variables are problematic as they are constructs of other factors that may − at different levels − help explain access. Despite their originality such approaches are not necessarily constructive and do not lend themselves to replication for implementation at local levels. Overall the finding suggest a need for the development of additional methodological approaches to analyzing survey data in order to identify strategies for jointly modeling financial and non-financial access barriers. Policy implications of the findings Multiple factors give rise to access barriers that manifest as a lack of fit between identified or potential health care need and the respective services. Health policy has little direct influence on most factors, yet an understanding of these factors is a precondition for a full identification and understanding of barriers. Policy instruments can tackle access barriers and be implemented to address information gaps between services and households. There are strong implications for health systems strengthening at the district level, as evidence suggests that local context plays an important role in the manifestation of barriers. Evaluating access along the myriad dimensions can guide district level strategies and the design of monitoring and evaluation tools.
CONCLUSIONS AND RECOMMENDATIONS
This review has confirmed the importance of socio-cultural and economic factors as determinants of access to health services. Beyond an identification of relevant factors and a summary of studies, the overview illustrates that barriers arise from the interplay of individual, household and

56
community level factors on the one hand, and corresponding health service factors on the other. The manifestation of access barriers is influenced by context and the reviewed analyses of household surveys provide an initial orientation as to the relative importance of barriers in different contexts. The highly complex interactions between enabling, predisposing and need factors are scarcely reflected in these studies. Demographic and life-course variables are not among the most important predictors of MCH service utilization. The close relationship between education and health knowledge demonstrates the importance of health information comprehension as a predictor of service uptake. As well, the type of information and means of communication should be tailored to the specific context to reduce barriers and strengthen local services. The development of communication strategies to strengthen services needs to take into account content, communication vehicles and targets, e.g. the empowerment of women often requires a strengthening of men’s health awareness. Quantitative data can support district level health communications and policies to address access barriers and in the creation of an evidence base for UHC policies. Ideally, a mixed methods approach should be employed, utilizing qualitative data to inform quantitative approaches. Existing quantitative evidence of non-financial barriers is limited and may fail to account for factors not adequately captured in surveys. For instance, there is only patchy evidence of religion as a barrier in quantitative studies. Most available resources and efforts flow into policy interventions aimed at addressing affordability. Yet, the analysis gives rise to the call for an increased focus on non-financial aspects at the district level. Implementation should initially focus on problematic geographic areas and include some degree of standardization to allow for comparative analyses. Routine monitoring and evaluation of the progress towards a reduction of access barriers and increases in service uptake should be incorporated as well. Initially, existing qualitative and quantitative research on access barriers should be jointly assessed with the explicit objective of mapping common findings and identifying potential gaps or areas for improvement in survey design, e.g. regarding measures of need. The acknowledged limitations of national-level household surveys, such as the shortage of economic variables, should be taken into account. Further operational research should be directed toward the development of a comprehensive approach to simultaneously analyze financial and non-financial barriers, taking into account complex interrelationships within and between dimensions of access. Taken together such mixed method approaches and improved methodologies will foster a better understanding of the demand-side of access. The information generated may support the development of policy interventions to optimize the “degree of fit” between the individual or household and the health system.

57
REFERENCES
1. Addai, I. (2000). Determinants of use of maternal-child health services in rural Ghana. J Biosoc Sci 32: 1-15.
2. Ahmed, S.M. (2001). Differing health and health-seeking behavior: ethnic minorities of the Chittagong Hill Tracts, Bangladesh. Asia Pac J Public Health 13: 100-8.
3. Ahsan, G., J. Ahmed, P. Singhasivanon, J. Kaewkungwal, K. Okanurak, N. Suwannapong, P. Akarasewi, M.A. Majid, V. Begum, K. Belayetali (2004). Gender difference in treatment seeking behaviors of tuberculosis cases in rural communities of Bangladesh. Southeast Asian J Trop Med Public Health 35: 126-35.
4. Alam, N., J.K. van Ginneken, I. Timaeus (2009). Determinants of perceived morbidity and use of health services by children less than 15 years old in rural Bangladesh. Matern Child Health J 13: 119-129.
5. Amoako Johnson, F., S.S. Padmas, J.J. Brown (2009). On the spatial inequalities of institutional versus home births in Ghana: a multilevel analysis. J. Community Health 34: 64-72.
6. Andersen, R., L. Aday (1974). A framework for the study of access to medical care. Health Serv Res 9: 208-220.
7. Andersen, R., J.F. Newman (1973). Social and individual determinants of medical care utilization in the United States. Milbank Memorial Quarterly 51: 95-105.
8. Arifeen, E.S., L.S. Blum, D.M. Hoque, E.K. Chowdhury, R. Khan, R.E. Black, C.G. Victora, J. Bryce (2008). Integrated Management of Childhood Illness (IMCI) in Bangladesh: early findings from a cluster-randomized study. Lancet 364(9445): 1595-602.
9. Bedford, J., A. Singh, M. Ponferrada, L. Eldred (2013). Access to health services: analyzing non-financial barriers in Ghana, Bangladesh, Vietnam and Rwanda using qualitative methods. A review of the literature. UNICEF Working Paper.
10. Bhuiya, A., S. Hanifi, F. Urni, S. Mahmood (2009). Three methods to monitor utilization of healthcare services by the poor. Int J Eq Health 8: 29.
11. Bishai, D., E. Suzuki, M. McQuestion, J. Chakraborty, M. Koenig (2002). The role of public health programmes in reducing socioeconomic inequities in childhood immunization coverage. Health Policy Plan 17: 412-9.
12. Boateng, J., C. Flanagan (2008). Women’s access to health care in Ghana: effects of education, residence, lineage and self-determination. Biodemography and Social Biology 54: 56-73.
13. Bucagu, M., Kagubare, J.M., Basinga, P., Ngabo, F., Timmons, B.K., Lee, A.C. (2012). Impact of health systems strengthening on coverage of maternal health services in Rwanda, 2000–2010: a systematic review. Reproductive Health Matters 20(39): 50-61.
14. Buor, D. (2003). Analysing the primacy of distance in the utilization of health services in the Ahafo-Ano South district, Ghana. Int J Health Plann Manage 18: 293-311.
15. Buor, D. (2004). Gender and the utilisation of health services in the Ashanti Region, Ghana. Health Policy 69: 375-88.
16. Chakraborty, N., M.A. Islam, R.I. Chowdhury, W. Bari, H.H. Akhter (2003). Determinants of the use of maternal health services in rural Bangladesh. Health Promot Int 18: 327-37.
17. Chandrasekhar, S., T. Gebreselassie, A. Jayaraman (2011). Maternal health care seeking behavior in a post-conflict HIPC: the case of Rwanda. Popul Res Policy Rev 30: 25-41.

58
18. Chowdhury, R., M.A. Islam, J. Gulshan, N. Chakraborty (2007). Delivery complications and healthcare-seeking behavior: The Bangladesh Demographic Health Survey, 1999-2000. Health and Social Care in the Community 15: 254-64.
19. Do, M. (2009). Utilization of skilled birth attendants in public and private sectors in Vietnam. J Biosoc Sci 41: 289-308.
20. Doku, D., S. Neupane, P.N. Doku (2012). Factors associated with reproductive health care utilization among Ghanaian women. BMC International Health and Human Rights 12: 29.
21. Duong, D.V., C.W. Binns, A.H. Lee (2004). Utilization of delivery services at the primary health care level in rural Vietnam. Soc Sci Med 2004 59: 2585-95.
22. Filmer, D., and L. Pritchett (2001). Estimating wealth effects without expenditure data - or tearsan application to educational enrollments in states of India. Demography 38: 85-120.
23. Frenz, P., J. Vega (2010). Universal health coverage with equity. Background paper for the Global Symposium on Health Systems Research, 16-19 November 2010. Montreux, Switzerland.
24. Giedion, U., Alfonso, E. A., & Díaz, Y. (2013). The Impact of Universal Coverage Schemes in the Developing World: A Review of the Existing Evidence. Universal Health Coverage Studies Series (UNICO) , UNICO Studies Series (25).
25. Goland, E., D.T.P. Hoa, M. Malqvist (2012). Inequity in maternal health care utilization in Vietnam. Int J Eq Health 11: 24.
26. Gyimah, S.O., B.K. Takyi, I. Addai (2006). Challenges to the reproductive-health needs of African women: on religion and maternal health utilization in Ghana. Soc Sci Med 62: 2930-44.
27. Halder, A.K., U.R. Saha, M. Kabir (2007). Inequalities in reproductive healthcare utilization: Evidence from Bangladesh Demographic and Health Survey 2004. World Health Popul 9: 48-63.
28. Hong, T.K., M.J. Dibley, T. Tuan (2003). Factors affecting utilization of health care services by mothers of children ill with diarrhea in rural Vietnam. Southeast Asian J Trop Med Public Health 34: 187-98.
29. Howe, L.D., J R Hargreaves, S Gabrysch, S R A Huttly (2009). Is the wealth index a proxy for consumption expenditure? A systematic review. J Epidemiol Community Health 63: 11 871-877.
30. Joseph, A.E., A. Poyner (1982). Interpreting patterns of public service utilization in rural areas. Econ Geogr 58: 262–273.
31. Kamal, S.M. (2009). Factors affecting utilization of skilled maternity care services among married adolescents in Bangladesh. Asian Population Studies 5: 153-170.
32. Knowles, J.C., S. Bales, L.Q. Cuong, T.T.M. Oanh, D.H. Luon (2009). Health Equity in Viet Nam: a Situation Analysis focused on Maternal and Child Mortality. Background paper prepared for the UNICEF Consultancy on Equity in Access to Quality Healthcare for Women and Children, April 8-10, 2009. UNICEF: Ha Long, Viet Nam.
33. Lu, C., B. Chin, G. Li, C. Murray (2009). Limitations of methods for measuring out-of-pocket and catastrophic private health expenditures. Bull World Health Organ 87: 238-244.
34. Lu, C., B. Chin, J.L. Lewandowski, P. Basinga, L.R. Hirschhorn, K. Hill, M. Murray, A. Binagwaho (2012). Towards Universal Health Coverage: An Evaluation of Rwanda Mutuelles in Its First Eight Years. PLoS ONE 7(6): e39282.
35. Mashreky, S.R., A. Rahman, S.M. Chowdhury, L. Svanström, S. Shafinaz, T.F. Khan, F. Rahman (2010). Health seeking behavior of parents of burned children in Bangladesh is related to family socioeconomics. Injury, Int. J. Care Injured 41: 528-32.

59
36. McIntyre, D., B. Garshong, G. Mtei, F. Meheus, M. Thiede, J. Akazili et al. (2008). Beyond fragmentation and towards universal coverage: insights from Ghana, South Africa and the United Republic of Tanzania. Bull World Health Organ 86: 871-876.
37. McIntyre, D., M. Thiede and S. Birch (2009). Access as a policy-relevant concept in low- and middle-income countries. Health Economics, Policy and Law 4: 179-193.
38. Moyer, C. A., & Mustafa, A. (2013). Drivers and deterrents of facility delivery in sub-Saharan Africa: a systematic review. Reproductive health, 10(1): 40.
39. Najnin, N., C.M. Bennett, S.P. Luby (2011). Inequalities in care-seeking for febrile illness of under-five children in urban Dhaka, Bangladesh. J Health Popul Nutr 29: 523-31.
40. Ngo, A.D., P.S. Hill (2011). The use of reproductive healthcare at commune health stations in a changing health system in Vietnam. BMC Health Services Research 11: 237.
41. O'Connell, T. (2012). National Health Insurance in Asia and Africa: Advancing Equitable Social Health Protection to Achieve Universal Health Coverage. New York NY: UNICEF.
42. O'Donnell, O., E. van Doorslaer, R. Rannan-Eliya, A. Somanathan, S.R. Adhikari, B. Akkazieva, D. Harbianto, C.C. Garg, P. Hanvoravongchai, A.N. Herrin, M.N. Huq, S. Ibragimova, A. Karan, S.M. Kwon, G.M. Leung, J.F. Lu, Y. Ohkusa, B.R. Pande, R. Racelis, K. Tin, K. Tisayaticom, L. Trisnantoro, Q. Wan, B.M. Yang, Y. Zhao (2008). Who pays for health care in Asia? J Health Econ 27(2): 460-75.
43. Oliver, A., E. Mossialos (2004). Equity of access to health care: outlining the foundations for action. J Epidemiol Community Health 58: 655-658.
44. Rabbani, A., G.C. Alexander (2009). The association between family structure, reports of illness and health care demand for children: evidence from rural Bangladesh. J Biosoc Sci 41: 645–660
45. Rahman, M.H., W.H. Mosley, S. Ahmed, H.H. Akhter (2008). Does service accessibility reduce socioeconomic differentials in maternity care seeking? Evidence from rural Bangladesh. J Biosoc Sci 40: 19-33.
46. Rahman, M., K. Nakamura, K. Seino, M. Kizuki (2012). Intimate partner violence and use of reproductive health services among married women: evidence from a national Bangladeshi sample. BMC Public Health 12: 913.
47. Reynolds, H.W., E.L. Wong, H. Tucker (2006). Adolescents' use of maternal and child healthservices in developing countries. Int Fam Plan Perspect 32: 6-16.
48. Schneider, P., F. Diop (2005). Community-based health insurance in Rwanda. In: Preker, A.S., G. Carrin, editors. Health Financing for Poor People: Resource Mobilization and Risk Sharing. Washington, DC: World Bank.
49. Senarath, U., N.S. Gunawardena (2009). Women’s autonomy in decision making for health care in South Asia. Asia Pac J Public Health 21: 137-143.
50. Sepehri, A., S. Moshiri, W. Simpson, S. Sarma (2008a). Taking account of context: how important are household characteristics in explaining adult health-seeking behavior? The case of Vietnam. Health Policy Plan 23: 397-407.
51. Sepehri, A., S. Sarma, W. Simpson, S. Moshiri (2008b). How important are individual, household and commune characteristics in explaining utilization of maternal health services in Vietnam? Soc Sci Med 67: 1009-17.
52. Smith Greenaway, E., J. Leon, D.P. Baker (2012). Understanding the association between maternal education and use of health services in Ghana: exploring the role of health knowledge. J Biosoc Sci 44: 733-747.

60
53. Story, W.T., S.A. Burgard (2012). Couples’ reports of household decision-making and the utilization of maternal health services in Bangladesh. Soc Sci Med 75: 2403-2411.
54. Tanahashi, T. (1978). Health service coverage and its evaluation. Bulletin of the World Health Organisation, 56(2): 295-303
55. Thang, N.M., I. Bhushan, E. Bloom, S. Bonu (2007). Child immunization in Vietnam: Situation and barriers to coverage. J Biosoc Sci 39, 41–58.
56. Thiede, M. (2005). Information and access to health care: Is there a role for trust? Soc Sci Med 61: 1452-1462.
57. Thiede, M., P. Akweongo, D. McIntyre (2007). Exploring the dimensions of access. In: McIntyre, D., G. Mooney (eds). The Economics of Health Equity. Cambridge: Cambridge University Press.
58. Uddin, M.J., T.L. Koehlmoos, A. Ashraf, A.I. Khan, N.C. Saha, M. Hossain (2009). Health needs and health-care-seeking behavior of street-dwellers in Dhaka, Bangladesh. Health Policy Plan 24: 385-394.
59. Wagstaff, A., M. Bilger, Z. Sajaia, M. Lokshin (2011). Health Equity and Financial Protection. Washington DC: The World Bank.
60. Wagstaff A, van Doorslaer E (2003). Catastrophe and impoverishment in paying for health care: with applications to Vietnam 1992-1998. Health Econ 12(11): 921-34.
61. Xu, K., F. Ravndal, D.B. Evans, G. Carrin (2009). Assessing the reliability of household expenditure data: results from the World Health Survey. Health Policy 91: 297-305.
62. Young, J.T., J. Menken, J. Williams, N. Khan, R.S. Kuhn (2006). Who receives healthcare? Age and sex differentials in adult use of healthcare services in rural Bangladesh. World Health Popul 8: 83-100.

61
APPENDIX
Following exploratory searches, the search strings were designed as follows (here in PubMed format):
Bangladesh ((health services accessibility[MeSH Terms]) OR (utilization OR bottleneck* OR access*)) AND (survey* OR cross sectional surveys[MeSH Terms] OR health care surveys[MeSH Terms]) AND Bangladesh AND ("2000/01/01"[PDAT] : "2013/01/31"[PDAT]) Ghana ((health services accessibility[MeSH Terms]) OR (utilization OR bottleneck* OR access*)) AND (survey* OR cross sectional surveys[MeSH Terms] OR health care surveys[MeSH Terms]) AND Ghana AND ("2000/01/01"[PDAT] : "2013/01/31"[PDAT]) Rwanda ((health services accessibility[MeSH Terms]) OR (utilization OR bottleneck* OR access*)) AND (survey* OR cross sectional surveys[MeSH Terms] OR health care surveys[MeSH Terms]) AND Rwanda AND ("2000/01/01"[PDAT] : "2013/01/31"[PDAT]) Vietnam ((health services accessibility[MeSH Terms]) OR (utilization OR bottleneck* OR access*)) AND (survey* OR cross sectional surveys[MeSH Terms] OR health care surveys[MeSH Terms]) AND Vietnam AND ("2000/01/01"[PDAT] : "2013/01/31"[PDAT])