abdominal emergency cases
TRANSCRIPT

Abdominal Emergency Cases
Jeff Dunkle, MD
February 2011

Case: Trauma

Case: Trauma

Dx?

Dx: “Shock Bowel”
Hypoperfusion complex
Seen in patients with hypovolemic shock.
Poor prognostic indicator.
CT findings are generally reversible.
Increased permeability.
Edema
Enhancement

Dx: Hypoperfusion complex
Small bowel mucosal
enhancement
Adrenal hyperenhancement
Abnormal parenchymal
organ enhancement
Small IVC, Aorta

Blunt Abdominal Trauma
A few stats:
Trauma is the leading cause of death in US for those < 44 y.o.
For those age 15-34, MVA is single leading cause of death.

Blunt Abdominal Trauma
Prevailing trends:
MDCT is test of choice
Non-operative management is favored whenever feasible.

Case: Pain.

Case: Pain.

Dx?
Dx: Pneumoperitoneum.

Case: Pregnant, pain.

Case: Pregnant, pain.
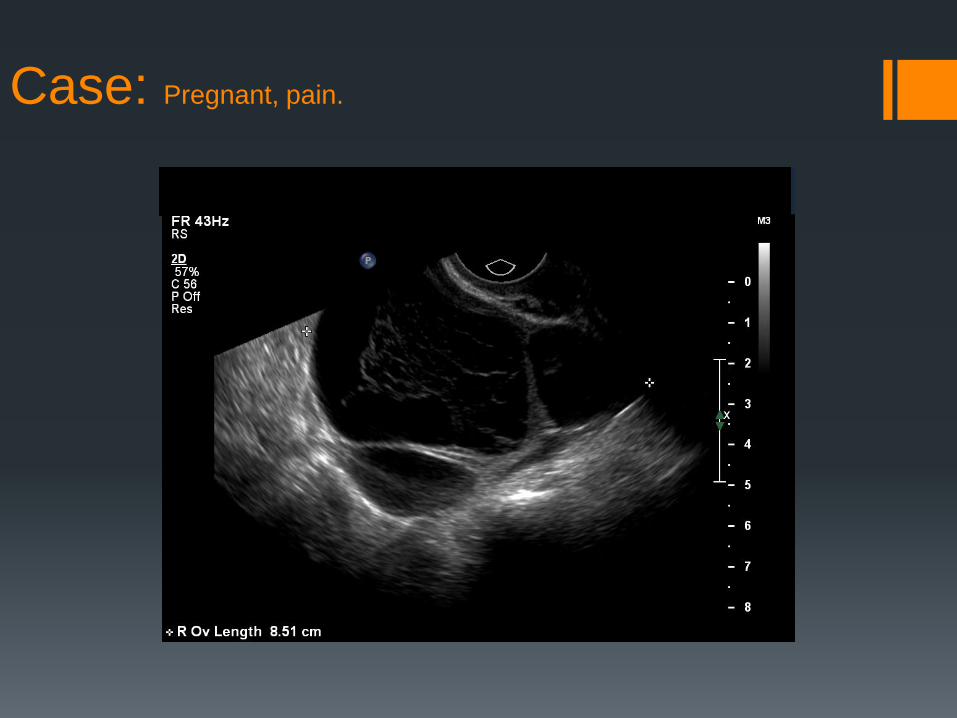
Case: Pregnant, pain.

Case: Pregnant, pain.

Case: Pregnant, pain.

Dx?

Dx: Ectopic Pregnancy
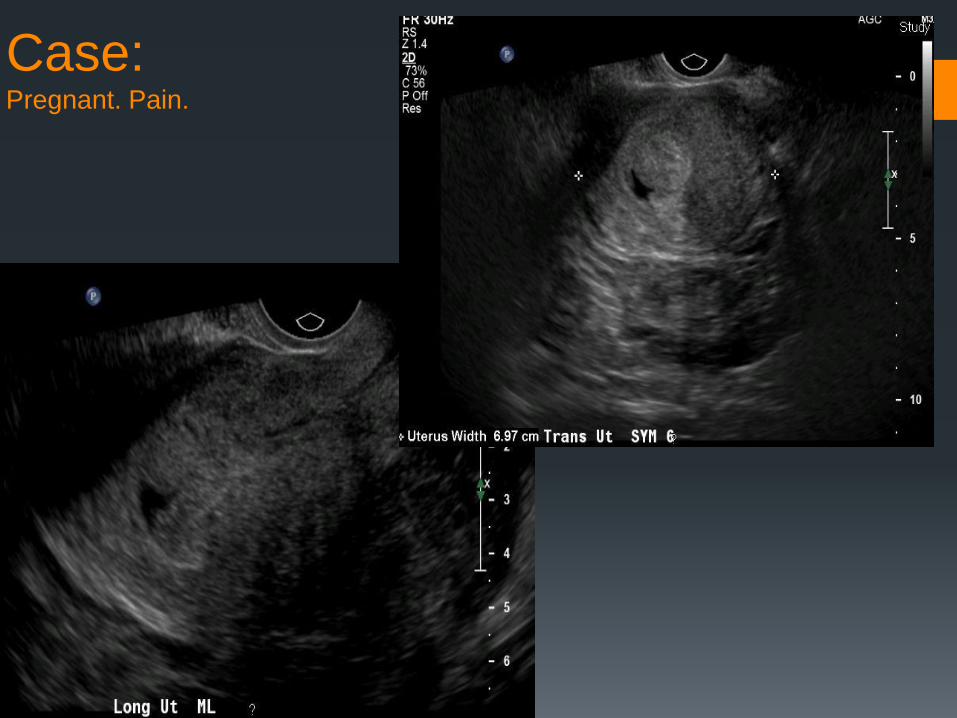
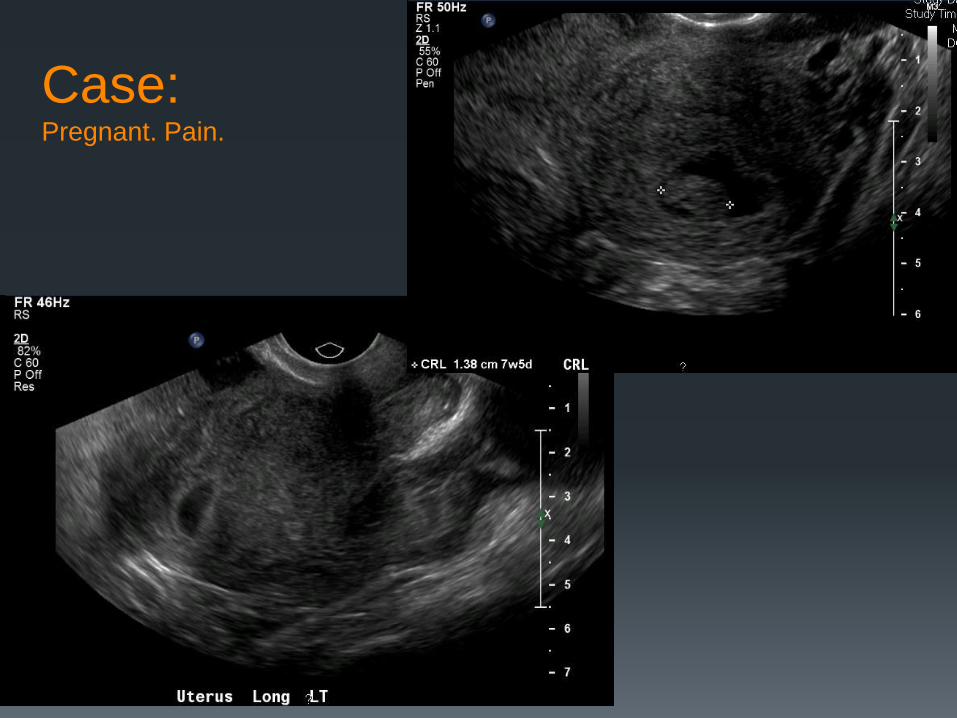
Case: Pregnant. Pain.

Case: cont’d

Dx?

Dx: Ectopic Pregnancy
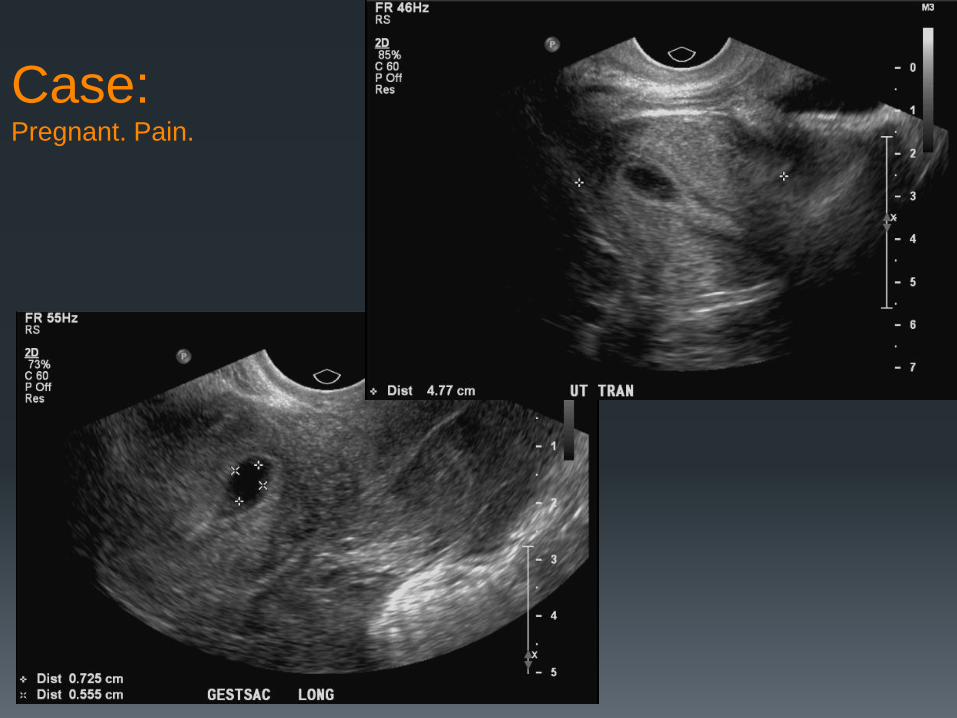
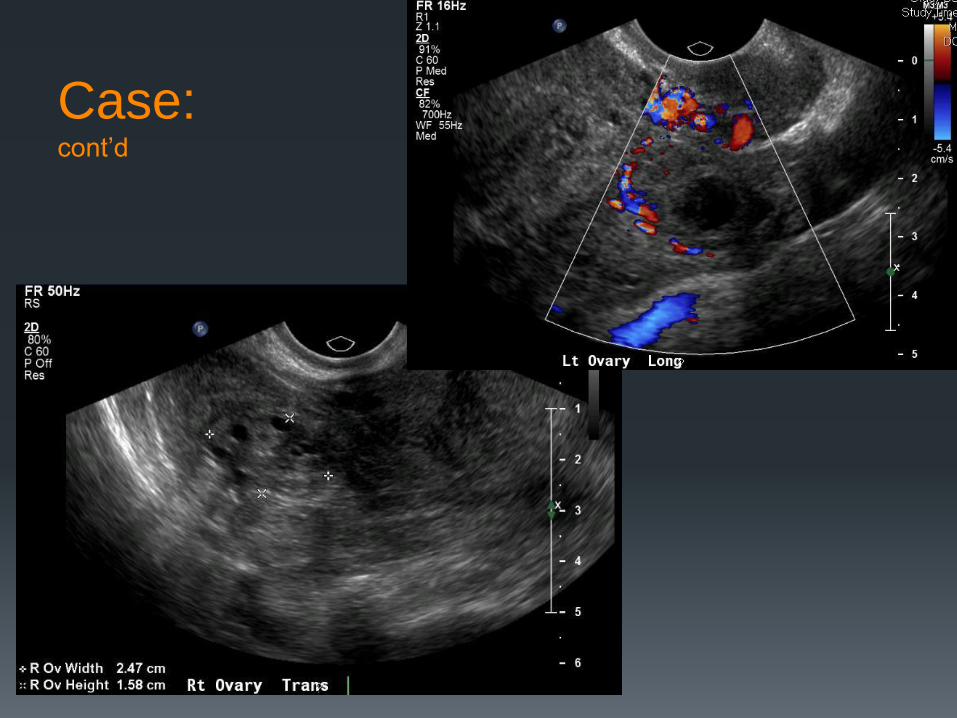
Case: Pregnant. Pain.

Case: cont’d

Dx?

Dx: Ectopic Pregnancy
Case: Pregnant. Pain.
Case: cont’d

Case: cont’d

Dx?

Dx: Ectopic Pregnancy

Case: Trauma.

Case: Trauma.

Dx?
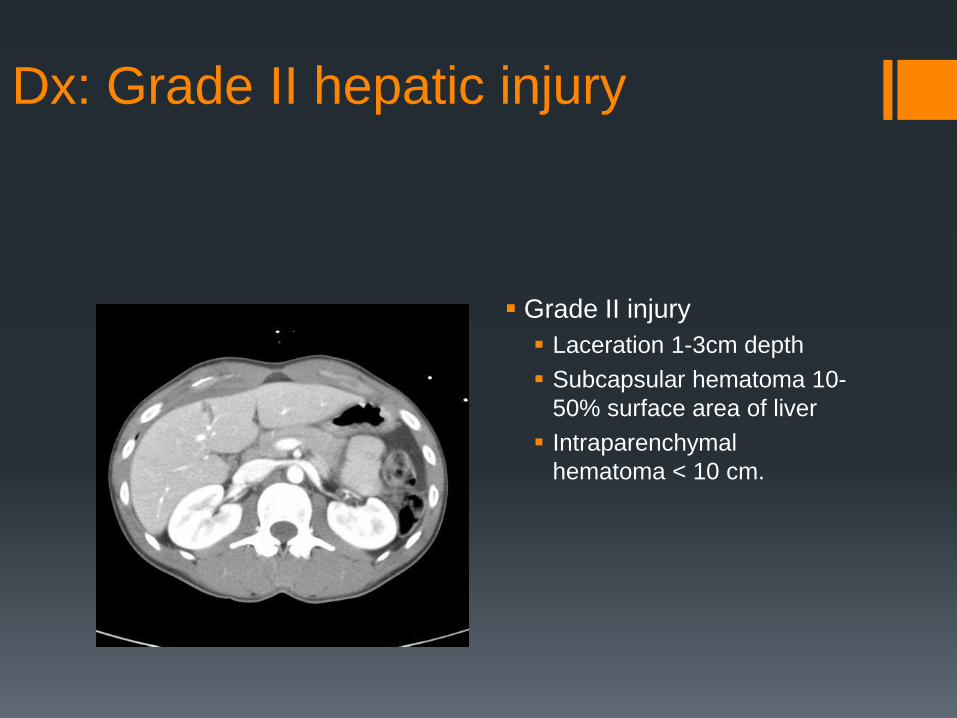
Dx: Grade II hepatic injury
Grade II injury
Laceration 1-3cm depth
Subcapsular hematoma 10-
50% surface area of liver
Intraparenchymal
hematoma < 10 cm.

AAST Liver Injury Grading
I Hematoma: subcapsular, <10% surface area
Laceration: capsular tear, <1 cm in parenchymal depth
II Hematoma: subcapsular, 10%–50% surface area; intraparenchymal, <10 cm in diameter
Laceration: 1–3 cm in parenchymal depth
III Hematoma: subcapsular, >50% surface area or expanding or ruptured subcapsular hematoma with active bleeding; intraparenchymal, >10 cm or expanding or ruptured
Laceration: >3 cm in parenchymal depth
IV Hematoma: ruptured intraparenchymal hematoma with active bleeding
Laceration: parenchymal disruption involving 25%–75% of a hepatic lobe or 1- 3 Couinaud segments within a single lobe
V Laceration: parenchymal disruption involving >75% of a hepatic lobe or >3 Couinaud segments within a single lobe
Vascular: juxtahepatic venous injuries (i.e.: retrohepatic vena cava or central major hepatic veins)
Advance 1 grade for multiple injuries up to Grade III

Injury grading
AAST injury grading. Why?
Why not?
AAST grade of injury is an independent predictor of failure of non-operative management
Other predictors of NOM failure: Need for multiple blood transfusions
Hypotension
Age

AAST injury grading
Higher grade increases probability of delayed complications
Delayed complications: delayed hemorrhage, pseudoaneurysm formation, AV fistula, biloma, infected hematoma, pseudocyst, urinoma
Surgeons use grading system to triage management

Pitfalls of CT Grading
Congenital clefts; most commonly in spleen
Streak artifact simulating linear laceration
Patient’s arms
Ribs
Cardiac leads
Other: focal fatty infiltration (liver) or other hypoattenuating
lesions

Case: Trauma.

Case: Trauma.

Dx?

Dx: Grade IV liver injury
Grade III Laceration >3cm in depth
Large subcapsular or intraparenchymal hematoma
Grade IV Laceration involving 25-75% of a
lobe
Ruptured intraparenchymal hematoma with active bleeding
Grade V Laceration involving > 75% of a
lobe
Major juxta-hepatic venous injury

Case: Trauma.

Case: Trauma.

Dx?

Dx: Grade II splenic injury
Grade II injury:
Laceration 1-3cm in depth
Parenchymal hematoma
<5cm
Subcapsular hematoma 10-
50% surface area of spleen

AAST Splenic Injury Grading
I Subcapsular hematoma < 10% surface area
Capsular laceration < 1 cm parenchymal depth
II Subcapsular hematoma, 10%–50% surface area
Intraparenchymal hematoma <5 cm diameter
Laceration with 1–3 cm parenchymal depth, not involving a trabecular vessel
III Subcapsular hematoma >50% surface area or expanding
Ruptured subcapsular or parenchymal hematoma; intraparenchymal hematoma
>5 cm
Laceration >3 cm parenchymal depth or involving trabecular vessels
IV Laceration of segmental or hilar vessels that produces major devascularization >25% of spleen
V Completely shattered spleen; vascular hilar injury with devascularized spleen
Advance 1 grade for multiple injuries up to Grade III

Case: Trauma.

Case: Trauma.

Dx?

Dx: Grade III splenic injury
Grade III:
Subcapsular hematoma
>50% surface or expanding
Ruptured subcapsular or
intraparenchymal
hematoma.
Hematoma > 5cm
Laceration > 3cm in depth
Case:
Pain.

Case:
Pain.

Dx?

Dx: Free subdiaphragmatic air

Case: Abdominal pain.

What next?

Case: cont’d

Dx?

Dx: BAD things: portal venous gas,
pneumatosis, bowel infarction.

Case: Trauma.

Case: Trauma.

Dx?

Dx: Grade IV injury

AAST Renal Injury Grading
I Contusion or nonexpanding subcapsular hematoma without parenchymal
laceration
II Nonexpanding perirenal hematoma confined to the retroperitoneum Lacerations <1 cm depth in the renal cortex
III Lacerations >1 cm depth without extension into the collecting system or
urinary extravasation
IV Lacerations extending through the renal cortex, medulla, and collecting system
Injuries to the main renal artery or vein with contained hemorrhage
V Completely shattered kidney Injuries to the renal hilum with devascularization of the kidney: traumatic
renal arterial disruption, traumatic renal arterial occlusion
(Advance one grade for bilateral injuries, up to Grade III)
Blunt Renal Injury:
10% of all blunt abdominal injuries involve kidneys.
Mechanism:
MVA
Direct blow
Fall
Grand majority of these are minor injuries
70-85% are Grade I
Contrast-enhanced MDCT is imaging modality of choice
Blunt Renal Injury:
Management:
Conservative management is the rule!
Grade I and II: Watch
Grade III and IV: Controversial. When in doubt, watch.
Nephrectomy rate is higher in patients who undergo operative
exploration (35%) versus those who have conservative management (12%)
Intervention: Main renal artery/vein and UPJ injuries
Active arterial bleeding & devascularization
Urinary extravasation

Case: Trauma

Dx?

Dx: Grade II renal injury:
Grade I:
Subcapsular hematoma
Contusion
Grade II:
Perinephric hematoma
Laceration < 1cm
Grade III:
Laceration > 1cm
NO collecting system injury

Case: Trauma

Case: Trauma

Dx?
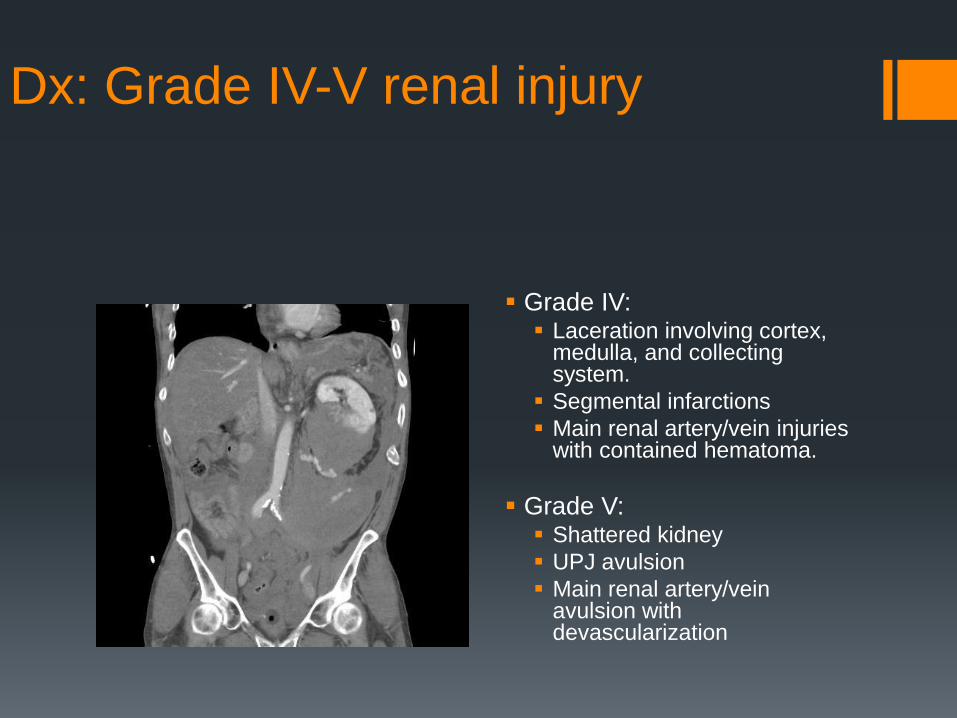
Dx: Grade IV-V renal injury
Grade IV: Laceration involving cortex,
medulla, and collecting system.
Segmental infarctions
Main renal artery/vein injuries with contained hematoma.
Grade V: Shattered kidney
UPJ avulsion
Main renal artery/vein avulsion with devascularization
Management?

Management?
Active Contrast Extravasation
Arterial injury:
Active extravasation with free spill of contrast: focal high
attenuation jet (matches arteries in density) that fades into an
enlarged, enhanced hematoma on delayed imaging.
Pseudoaneurysm: defined collection, often round, that becomes
less apparent on delayed imaging. No change in hematoma.

Active Contrast Extravasation
Differentiate from:
Bone fragments: unusual shapes, high attenuation on all
imaging.
Venous injury: initial nonvisualization, which becomes more
apparent on delayed imaging.
Caution.
Density of blood:
Simple free fluid: 0-15 HU
Unclotted blood: 20-40 HU
Clotted blood / hematoma: 40-70 HU
Active extravasation: matches origin vessel
Usually within 10 HU

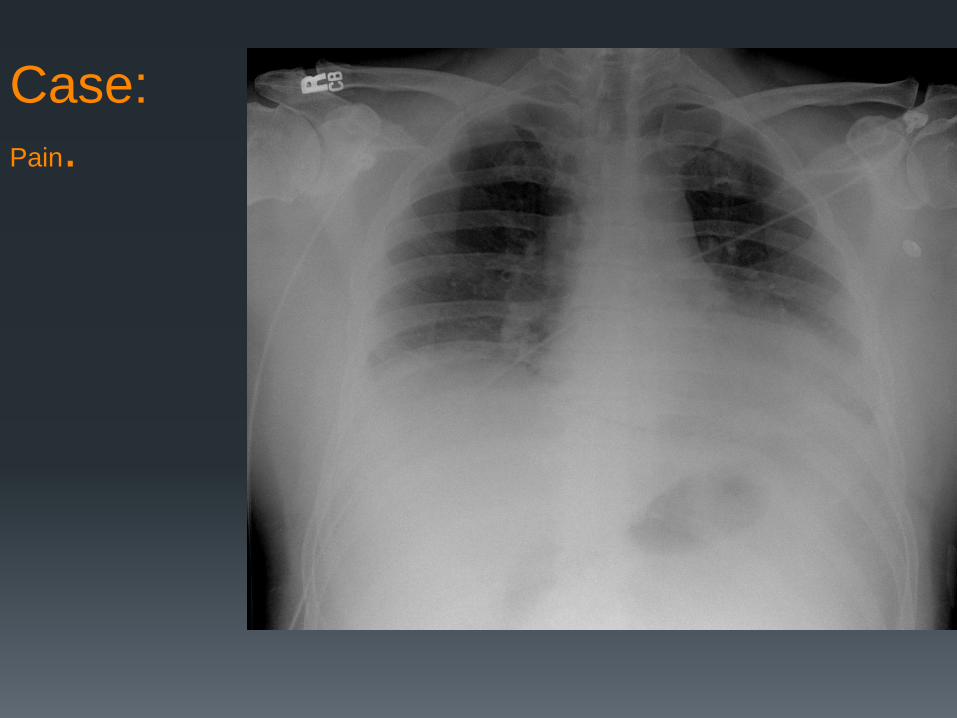
Case: Pain.

Case: Pain.

Dx?

Dx: Free subdiaphragmatic air
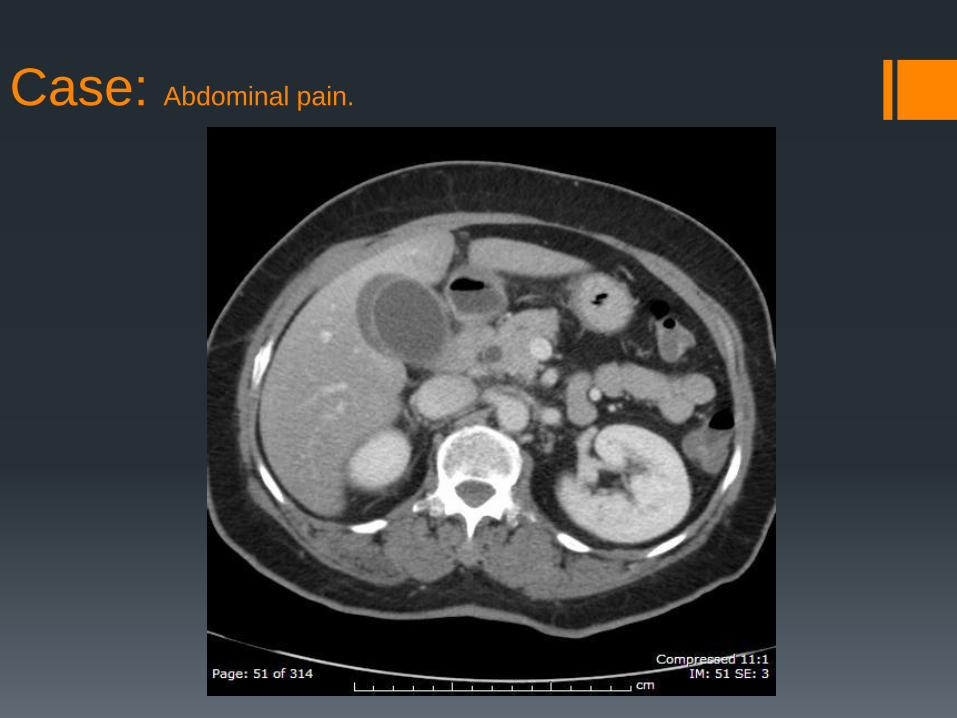
Case: Abdominal pain.

Case: Abdominal pain.

Dx?
Dx: Acute cholecystitis.
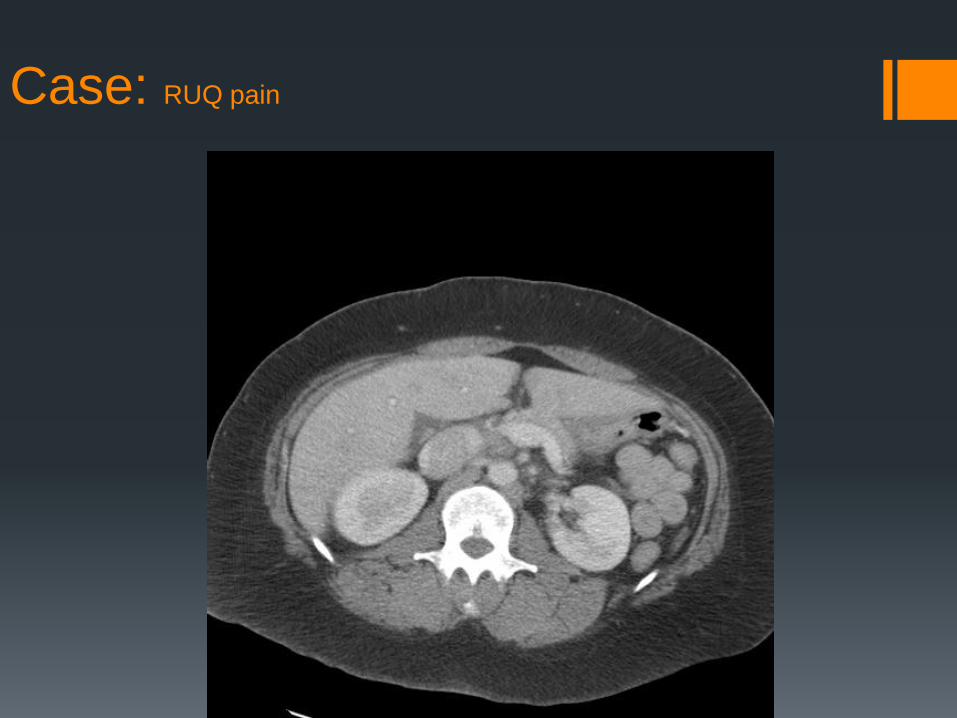
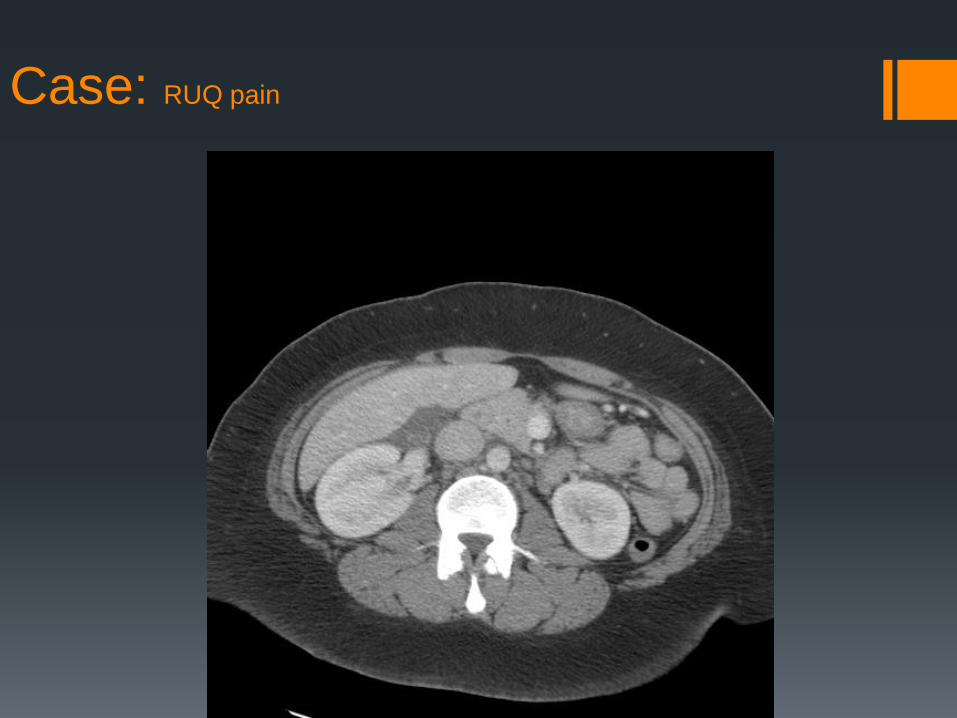
Case: RUQ pain

Case: RUQ pain
Case: RUQ pain

Case: RUQ pain

Case: RUQ pain

Case: RUQ pain

Case: RUQ pain

Case: RUQ pain

Dx?

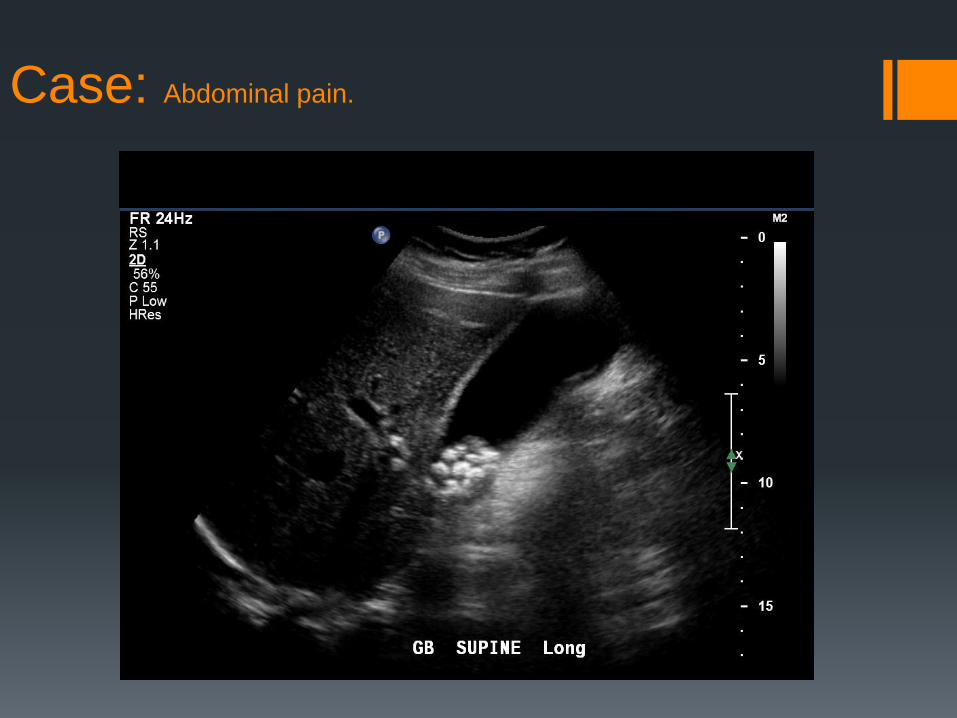
Additional imaging

Additional imaging:

Dx: Normal Gallbladder
Case: Abdominal pain.

Case 18: abdominal pain
Case: Abdominal pain.

Dx: ?

Case: later that day…

Dx: Acute Cholecystitis
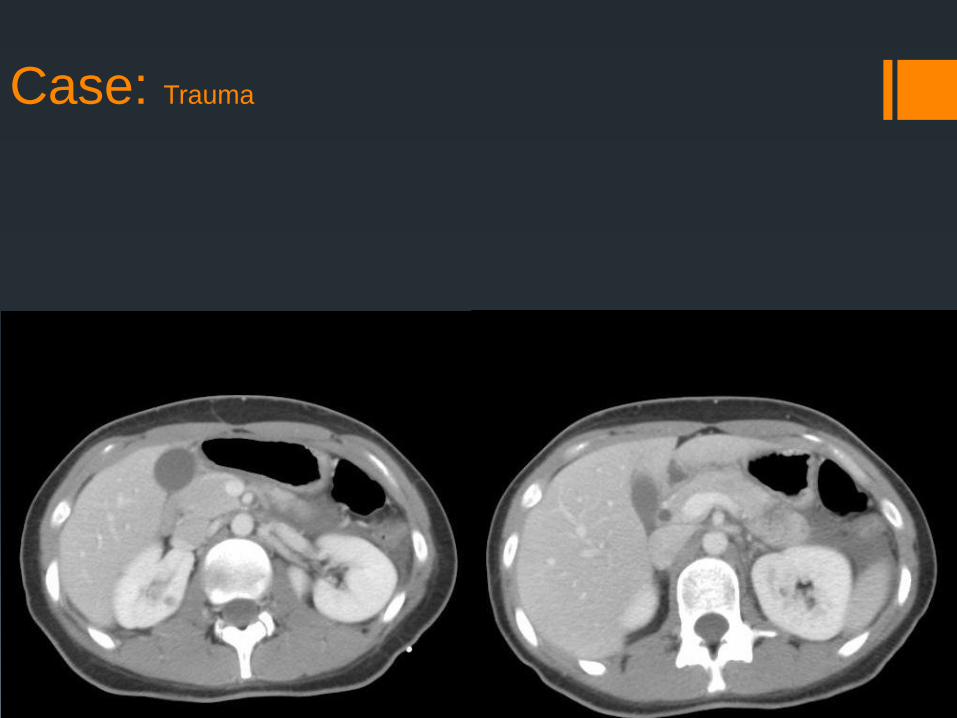
Case: Trauma

Case: Trauma

Dx?

Dx: Grade III pancreatic injury

AAST Pancreatic Injury Grading
I Minor contusion without ductal injury
Superficial laceration without ductal injury
II Major contusion without ductal injury
Major laceration without ductal injury
III Distal transection or parenchymal injury with ductal laceration
IV Proximal transection or parenchymal injury involving the ampulla
V Massive disruption of the pancreatic head
*proximal: to the right of the SMV

Blunt pancreatic injury:
Rare (<2% of abdominal injuries)
Mechanism:
MVA
Direct blow
Rare isolated injury
Usually multiple concomitant intra-abdominal injuries.
Associated with relatively high morbidity and mortality
Usually from non-pancreatic causes
Blunt pancreatic injury:
Late or missed diagnosis can result in significant morbidity (or death)
Mortality if diagnosed early (<24hrs): 11%
Mortality if diagnosed late (>24hrs): 40%
Complications:
Pancreatitis
Pseudocyst
Fistula formation
Abscess
Sepsis

Detection of Pancreatic Injury
Overall CT sensitivity in detecting all grades of pancreatic injury is approx. 80%
Accuracy of detecting ductal injury may be as low as 40%
CT may be normal in the first 12 hrs. after injury in 20-40% of patients
Serum amylase levels drawn within 3 hrs. of injury are unreliable

Management of Pancreatic Injury
Grade I and II injuries best treated with hemostasis +/- external drainage
Grade III injuries treated with distal pancreatectomy
Grade IV and V injuries treated with surgery (Whipple)

Case: Trauma

Case: Trauma

Dx?

Dx: Grade III pancreatic injury
Grade I: superficial laceration
Duct intact
Grade II: major laceration
Duct intact
Grade III: distal transection
Duct injury
Grade IV: Proximal
transection
Involves ampulla or bile duct
Grade V: Massive disruption
of pancreatic head.

Post-therapy follow-up:
The End.