a systems biology study to tailored treatment in chronic ... · heart failure-related...
TRANSCRIPT

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
A systems biology study to tailored treatment in chronic heart failure
Ouwerkerk, W.
Link to publication
Citation for published version (APA):Ouwerkerk, W. (2017). A systems biology study to tailored treatment in chronic heart failure
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 27 Aug 2018

SUMMARY OF FINDINGS


161
The aim of this thesis was to identify patients at low or high risk of mortality and/orheart failure-related hospitalization, and patients who were likely or not likely to achieve ESC-recommended pharmaceutical treatment.
Part IFirst, a meta-analysis in Chapter 2 found 117 different prediction models, using 249 distinctpredictor variables. The best predictors were: blood urea nitrogen (BUN), presence of cancer, tro-ponin, serum creatinine, systolic blood pressure (SBP) and sodium. These predictors have beenused often before in prediction models, but frequently supported by easy collectable predictorssuch as age and gender. The published prediction models performed moderately for mortality,but exhibited poor performance in predicting heart failure-related hospitalization, and in predict-ing the first occurrence of heart failure-related hospitalization or death. In addition to predictingmortality, better c-statistic values were achieved in models using more variables, data acquired inprospective clinical studies, and data from a registry type data source. Not surprisingly, modelspredicting events over a shorter time span also resulted in more accurate predictions.
We developed new prediction models in Chapter 3, predicting mortality, heart failure-relatedhospitalization and the first occurrence of heart failure-related hospitalization or death. In ourmodel development process, we used only 42 easily obtainable variables. We found that ourmodels performed as well as existing models. C-statistic values of our models were 0.73, 0.68,0.70 for predicting mortality, heart failure hospitalization and the first occurrence of heart fail-ure hospitalization or death, respectively. These models consisted of 16, 10, and 15 predictorvariables, respectively. To make our models more usable in daily clinical practice, we limited thenumber of variables in the models to 5 for predicting mortality and heart failure hospitalization,and 9 for the composite endpoint. This model reduction let to reduced c-statistic values (0.69,0.66, 0.69, respectively). The mortality model consisted of: age, BUN, N-terminal pro B-typenatriuretic peptide (NT-proBNP), hemoglobin, and the use of beta-blockers at time of inclusioninto the study. Variables in the heart failure hospitalization model consisted of: age, heartfailure hospitalization in the year before inclusion, peripheral edema and estimated glomerularfiltration rate (eGFR). The combined model comprised variables from both the mortality andheart failure hospitalization model, with the exception of eGFR and BUN, and the addition ofhigh density lipoprotein (HDL)-cholesterol and sodium. External validation of both the full andcompact model performance gave comparable results in the validation cohort. We also developedan online calculator where individual survival curves can be calculated using the reduced models.We also developed a point score model from the reduced models, which can easily be calculatedby adding a point for each variable reaching specific cut-off value in those cases when the onlinecalculator could not be consulted. Because heart failure with reduced ejection fraction (HFrEF)and heart failure with preserved ejection fraction (HFpEF) patients are different, we looked atthe difference in prediction performance between them. There were differences in c-statistic val-ues between these two groups in the index cohort, but these differences were not observed in thevalidation cohort.
European Society of Cardiology (ESC)-recommended angiotensin-converting-enzyme inhibitor(ACE-inhibitor)/angiotensin II receptor blocker (ARB) and beta-blocker treatment doses werebased on results from large randomized controlled trials, and showed that higher doses were asso-ciated with better survival. In Chapter 4 we developed models to identify patients who wouldlikely achieve lower or higher doses of recommended pharmaceutical treatment. We could confirmthat achieving lower ACE-inhibitor/ARB and beta-blocker doses (<50% of recommended treat-ment dose) resulted in significantly worse survival. There was no significant difference in survivalbetween patients who reach 50-99% of recommended dose and those who achieved the recom-

162 Summary of findings
mended doses for beta-blockers, and only marginally significant differences for ACE-inhibitors/ARBs. Despite the incentive to up-titrate patients to ESC-recommended doses, only 22% and12% of patients achieved recommended ACE-inhibitor/ARB and beta-blocker doses, respectively.The number of patients achieving recommended ACE-inhibitor/ARB and beta-blocker doses werelower than reported in randomized controlled trials. We also looked at reasons why patients werenot up-titrated to recommended doses. Unfortunately, in most cases, no specific reason was givenfor the lack of up-titration. But we did observe that patients who did not reach recommendeddoses due to drug-intolerance had worse survival. There was no significant difference in survivalbetween patients who achieved recommended beta-blocker dose and patients who did not reachrecommended beta-blocker doses for other reasons.
Only a small portion of patients achieved recommended ACE-inhibitor/ARB and beta-blockertreatment doses; most patients did not. These patients did not fully benefit from treatment, butdid endure the negative effects of pharmaceutical treatment. In Chapter 5 we developed atreatment-selection model to determine if a patient should or should not be up-titrated to ≥50%of recommended treatment dose. We evaluated three different hypothetical treatment scenario’s:Scenario A) where all patients were successfully treated; scenario B) where our biomarker-based-model determined if a patient was up-titrated or not, and scenario C) where all patients weresub-optimally treated. First, we developed two models to estimate mortality and/or heart failurehospitalization in patients up-titrated to ≥50% of recommended treatment dose, and in patientsnot up-titrated to that level for both ACE-inhibitor/ARB and beta-blocker. Secondly, we pre-dicted the risk of death and/or heart failure hospitalization for each patient using both models.For Scenario B), the lowest hazard on death and/or heart failure hospitalization out of bothmodels, for each patient, was chosen. Scenario C), where all patients were sub-optimally treated,had the highest event-rate. Scenario B), where all patients were treated according to a biomarker-based-model, had the least number of events. The difference with scenario A), where all patientswere optimally treated, was minor, however, with a large error estimation. Our recommendation,therefore, is to start up-titration in all patients, regardless of the biomarker profile.
Part II
Heart failure is known to be heterogeneous in nature. Cluster methods are frequently and suc-cessfully applied to group patients based on clinically meaningful phenotypes. The use of clusteralgorithms has been criticized in connection with their robustness and reproducibility. In Chap-ter 6 we compared four well-established cluster methods (gaussian mixture for model-basedclustering (Mclust), polytomous latent class analysis (poLCA), partitioning around k-medoids(PAM) and hierarchical cluster analysis (Hclust)). We found that the number of created clustersvaried over the different methods, ranging from 4 (Hclust) to 20 (PAM). Cohen’s kappa was high-est for poLCA in determining clusters and in reproducing clusters in the index cohort. Cohen’skappa was highest for Hclust in reproducing clusters in validation cohort. Clusters produced byMclust and PAM did not only had low Cohen’s kappa values, but also differed in survival andclinical characteristics between index and validation cohorts, where poLCA and Hclust clustersshowed similar results between the clusters in these cohorts. This chapter showed that differentclustering methods gave different results depending on the methods as well as on the variablesused for input. We proposed a step-wise approach to ensure more clinical relevant and robustresults by assessing:
• The number and type of variables, handling of missing data should be well chosen
• Data redundancy should be taken care of

163
• Clustering results should be evaluated for robustness, independent reproducibility as wellas clinical implications of the results
We performed our own unsupervised cluster analyses (PAM) in Chapter 7, using the ap-proach suggested in Chapter 6, to distinguish relevant heart failure subtypes. We used principalcomponents with eigenvalue >1, from a principal component analysis (PCA) of 92 pathophys-iological biomarkers in BIOSTAT-CHF. We found 8 different subgroups (endotypes), all witha distinctive biomarker profiles and phenotypes. These endotypes also differed in up-titrationrates, survival, and treatment benefit. We found one and three endotypes that did not profit fromup-titration to ESC-recommended treatment doses for ACE-inhibitors/ARBs and beta-blockers,respectively. We were able to identify patients to endotypes based on only a small numberof biomarker values. Furthermore, we could validate these results in the separate independentvalidation cohort of BIOSTAT-CHF.
In Chapter 8 we introduced a probabilistic formulation of the alternative splicing recon-struction problem, using a finite mixture model based on the maximum likelihood principle ingene-expression data. A systematic approach was used to determine the probability of the pres-ence of splice variants. Our model was based on the assumption that the expected expressionlevel of exons in a particular splice variant is the same for all exons in that variant, but the modelallowed measurement error. The number of possible splice variants in our model was dependenton the number of exons in the gene. With small genes, all splice variants were analyzed, includ-ing biologically improbable variants. These variants were also given low prevalence in the results.For larger genes we used a scenario-based method to analyze possible splice variants. With thismethod, the improbable splice variants were already excluded. Our model showed good perfor-mance in simulations. Using our model, we found four possible splice variants not yet present ingene databases, but possibly present in three genes in Marfan syndrome patients.
In Chapter 9 we developed a penalized canonical correlation analysis (pCCA) to ana-lyze multiple high-dimensional biological data sets, such as genetic and methylation markers,(mi)ribonucleic acid (RNA), protein and peptide expression measurements and phenotypes, allmeasured on the same sample of individuals. The results are described by sparse canonical vari-ates featuring highly associated markers, molecules and phenotypes. When the multiple datasets are (epi)genetic markers, RNA, protein and peptide expression variables and phenotypes,the set of canonical variates and associated variables should correspond to nodes in pathogenetic-molecular pathways that describe the sequential transfer of information from deoxyribonucleicacid (DNA), its transcription to messenger ribonucleic acid (mRNA), its translation and to pro-teins and peptides and their metabolism into metabolites to observable (disease) phenotypes.Applying pCCA to the BIOSTAT-CHF study, we demonstrated that heart failure phenotypes(mortality, heart failure hospitalization and treatment success) of 2,245 patients could be welldescribed by associated canonical variates in genetic, proteomic and metabolomic spaces, sug-gesting key biological processes in heart failure. In this data example we used genetic, genomic,known heart failure (bio-)markers, and phenotypic variables. The pCCA method has a two-stage approach. In the first stage we determined the optimal penalty parameters by 10-foldcross-validation, after which we determined the final canonical variates and enriched the data byexploring knowledge bases. We extracted eight canonical variates, and did the enrichment forone of them. We found that this canonical variate was involved in the GPCR pathway, a groupof membrane receptors which is targeted by 40% of all modern drugs, including ACE-inhibitors/ARBs and beta-blockers. Given that we identified these relevant signals in heart failure patients,we concluded that pCCA is a useful statistical tool to jointly analyze phenotypic and variousomics data gathered from the same samples of patients.


SAMENVATTING


167
Het doel van dit proefschrift was om patiënten te identificeren die een laag of hoog risicohebben op overlijden en/of aan hartfalen gerelateerde ziekenhuisopname en patiënten die de doorde ESC aanbevolen medicamenteuze behandeling waarschijnlijk wel of niet verdragen.
Deel IIn een meta-analyse in Hoofdstuk 2, hebben we 117 verschillende predictie modellen gevondenmet in totaal 249 verschillende variabelen. De best voorspellende variabelen waren: BUN, hethebben van kanker, troponine, serum creatinine, SBP en natrium. Deze variabelen werden danook vaak gebruikt in predictie modellen, samen met variabelen die makkelijk te verzamelen zijn,zoals leeftijd en geslacht. De gepubliceerde modellen hadden een acceptabele accuraatheid in hetvoorspellen van het risico op overlijden, maar het voorspellen van ziekenhuisopname en de gecom-bineerde uitkomst van overlijden en/of ziekenhuisopname waren slechter. Naast het voorspellenvan overlijden, werden meer accurate voorspellingen gedaan wanneer gebruik werd gemaakt vanmeerdere variabelen, data uit prospectieve studies, klinische data, en data uit registratieonder-zoek. En niet geheel onverwacht was het voorspellen van uitkomsten voor een kortere periodemakkelijker dan voor een langere.
We hebben in Hoofdstuk 3 nieuwe predictie modellen ontwikkelt voor het voorspellen vanoverlijden, aan hartfalen gerelateerde ziekenhuisopname, en de gecombineerde uitkomst van over-lijden en/of aan hartfalen gerelateerde ziekenhuisopname. Voor het ontwikkelen van onze mo-dellen hebben we gebruik gemaakt van 42 variabelen die in de dagelijkse praktijk standaardgedocumenteerd worden. We vonden dat onze modellen net zo goed voorspelden als reeds ge-publiceerde modellen. C-statistiek waarden van onze modellen waren respectievelijk 0.73, 0.68,0.70 voor het voorspellen van overlijden, aan hartfalen gerelateerde ziekenhuisopname, en de ge-combineerde uitkomst van overlijden en/of aan hartfalen gerelateerde ziekenhuisopname. Dezemodellen bestonden uit 16, 10 en 15 variabelen. Om onze modellen makkelijker toepasbaar temaken in de dagelijkse praktijk hebben we het aantal variabelen terug gebracht naar 5 voorhet overlijden- en ziekenhuisopname-model en 9 voor de gecombineerde uitkomst. Deze reductieverlaagde de c-statistiek waarden naar respectievelijk 0.69, 0.66, en 0.69. Het overlijdens-modelbestond uit: leeftijd, BUN, NT-proBNP, hemoglobine, en het gebruik van beta-blockers op hetmoment van inclusie in de studie. Het model dat hartfalen gerelateerde ziekenhuisopname voor-spelde bestond uit: Leeftijd, hartfalen gerelateerde ziekenhuisopname in het jaar voorafgaandaan de inclusie in de studie, perifeer oedeem, SBP en eGFR. Het model voor de gecombineerdeuitkomst bestond uit de combinatie van beide vorige modellen, waarbij eGFR en BUN werdenverwijderd en HDL-cholesterol en natrium werden toegevoegd. We konden de resultaten vanzowel de volledige en de gereduceerde modellen goed reproduceren in het validatie cohort. Ookhebben we een online calculator gemaakt waar individuele overleving-curves uitgerekend kunnenworden. Als toevoeging bij de online calculator hebben we point score modellen ontwikkeld ge-baseerd op de gereduceerde modellen, deze kunnen makkelijk berekend worden door het optellenvan het aantal variabelen dat een bepaalde waarde bereikt. Omdat HFrEF en HFpEF patiëntenverschillen, hebben we ook gekeken naar het verschil in kwaliteit van de voorspellingen tussenHFrEF en HFpEF patiënten. Er waren verschillen tussen de kwaliteit van de voorspellingen indeze twee groepen in het index cohort, deze verschillen waren niet te zien in het validatie cohort.
De door het ESC aanbevolen medicamenteuze ACE-inhibitor/ARB en beta-blocker doses zijngebaseerd of grote gerandomiseerde klinische onderzoeken (RCTs) en hebben laten zien dat ho-gere doseringen tot betere overleving leiden. In Hoofdstuk 4 hebben we modellen gemaakt ompatiënten te identificeren die waarschijnlijk een lagere of hogere dosis zouden behalen. We kon-den bevestigen dat lagere ACE-inhibitor/ARB en beta-blocker doses (<50% van de aanbevolendosis) resulteerde in een significant lagere overleving. Er was geen significant verschil in overle-

168 Samenvatting
ving tussen patiënten die 50-99% van de aanbevolen beta-blocker doses haalden, en slechts eenmarginaal significant verschil voor ACE-inhibitors/ARBs doses. Ondanks dat artsen werden aan-gemoedigd om patiënten naar ESC aanbevolen doses op te titreren haalden slechts 22% en 12%van de patiënten de aanbevolen doses voor respectievelijk ACE-inhibitor/ARB en beta-blocker.Het aantal mensen dat aanbevolen doses haalde was lager dan we aanvankelijk verwachtten opbasis van de RCTs. We hebben ook gekeken naar redenen waarom de patiënten niet werdenopgetitreerd naar de aanbevolen doses. Helaas werd er vaker niet dan wel een reden opgegevenvoor het niet optitreren van een patiënt. We vonden wel dat patiënten die de aanbevolen dosesniet haalden omdat ze de medicatie niet konden tolereren een slechtere overleving hadden. Erwas geen significant verschil in overleving tussen patiënten die de aanbevolen beta-blocker dosishaalden en patiënten die de aanbevolen beta-blocker dosis niet haalden om andere redenen.
Slechts een klein deel van de patiënten haalden de aanbevolen ACE-inhibitor/ARB en beta-blocker doses, de meeste patiënten ondervonden daarmee niet de voordelen van de medicamen-teuze behandeling, maar wel de nadelige gevolgen. In Hoofdstuk 5 hebben we gekeken of wekonden de keuze - welke patiënten we wel en welke we niet moesten gaan optitreren - kondenvoorspellen. We hebben een model gemaakt om de kijken welke van drie hypothetische scenario’sde beste was: scenario A) alle patiënten werden succesvol behandeld, scenario B) optitreren ofniet wordt gebaseerd op basis van een biomarker waarden, scenario C) alle patiënten wordensub-optimaal behandeld (<50% aanbevolen doses). Allereest hebben we modellen ontwikkeld omhet overlijden en/of ziekenhuisopname te schatten in succesvol en niet succesvol opgetitreerdepatiënten voor zowel ACE-inhibitor/ARB en beta-blocker. Succesvol optitratie was, op basisvan de resultaten uit Hoofdstuk 4, gedefinieerd als optitratie naar ≥50% van aanbevolen ACE-inhibitor/ARB en beta-blocker doses. Daarna hebben we voor alle patiënten het risico op over-lijden en/of ziekenhuisopname geschat in beide modellen. Scenario B) werd gevormd door voorelke patiënt het laagte risico te nemen van beide modellen. Scenario C), waarin alle patiëntensub-optimaal werden behandeld, had het hoogste aantal events. Scenario B), waar alle patiëntenwerden behandeld aan de hand van onze biomarker-modellen, had het minst aantal events. Hetverschil met scenario A), waar alle patiënten optimaal behandeld werden, was klein en had eenvrij grote foutmarge. Ons advies luidt daarom om bij alle patiënten te starten met optitrerennaar de aanbevolen doses.
Deel IIHartfalen is een heterogene ziekte. Cluster-methoden zijn regelmatig en succesvol toegepastom patiënten te groeperen op basis van klinisch relevante fenotypes. Het gebruik van dit soortcluster-methoden wordt echter bekritiseerd door het gebrek van robuustheid en reproduceerbaar-heid. In Hoofdstuk 6 hebben we vier bekende veel gebruikte cluster-methoden (normal mixturemodelling (Mclust), latente klasse analyse (poLCA), PAM and hiërarchisch clustering (Hclust))vergeleken. We vonden dat het aantal gevonden clusters varieerde tussen 4 (Hclust) en 20 (PAM).Cohen’s kappa waarden voor het opstellen van de clusters en in het reproduceren van clusters inhet index cohort waren het hoogst voor poLCA. Cohen’s kappa waarden waren het hoogst voorHclust in het reproduceren van clusters in het validatie cohort. Clusters in Mclust en PAM had-den niet alleen lage Cohen’s kappa waarden, maar verschilde ook in klinische karakteristieken enprognose tussen het index en validatie cohort. poLCA en Hclust clusters lieten hier meer verge-lijkbare resultaten zien. In dit hoofdstuk hebben we laten zien dat cluster-methoden verschillenderesultaten laten zien aan de hand van verschillende methodes en variabelen die gebruikt worden.We hebben een methode voorgesteld dat moet zorgen voor een meer klinisch relevant en robuustresultaat:
1. Het aantal en type variabelen, hoe om te gaan met missende data moet wel overwogen

169
worden
2. Er moet met data redundancy worden afgerekend
3. Cluster resultaten moeten worden beoordeeld op robuustheid, onafhankelijke reproduceer-baarheid en klinische relevantie
In Hoofdstuk 7 hebben we onze eigen cluster analyse uitgevoerd (PAM), waar we de me-thode voorgesteld in Hoofdstuk 6 hebben gebruikt om onderscheidt te maken tussen hart falensubtypen (endotypen). We gebruikten principale componenten met een eigenwaarde >1, uit eenprincipale-componentenanalyse (PCA) van 92 biomarkers in BIOSTAT-CHF. We vonden 8 ver-schillende endotypen, allen met een kenmerkend biomarker profiel en fenotypen. Patiënten indeze endotypen verschilden in optitratie, overleving, en profijt van medicamenteuze behandeling.We vonden één en drie endotypen die geen profijt hadden bij optitratie naar ESC aanbevolendoses voor respectievelijk ACE-inhibitors/ARBs en beta-blockers. We konden patiënten aan en-dotypen koppelen op basis van slechts een klein aantal biomarkers. Ook konden we de gevondenresultaten goed reproduceren in het validatie cohort van BIOSTAT-CHF.
In Hoofdstuk 8 hebben we een methode bedacht om het alternatieve splicing reconstructieprobleem in gen-expressie data op te lossen. We hebben hier een mixture model voor gebruikdat gebaseerd is op het maximum likelihood principe. We hebben op een systematische maniergeprobeerd om de waarschijnlijkheid van een bepaalde splice variant te schatten. Ons modelwas gebaseerd op de assumptie dat de verwachtte expressie van één exon in een willekeurigesplice variant gelijk is voor alle exonen in die variant, maar met een bepaalde foutmarge. Hetaantal mogelijke splice varianten in ons model was afhankelijk van het aantal exonen in een gen.Bij kleine genen werden alle varianten geanalyseerd, inclusief de biologisch onwaarschijnlijkevarianten. Deze varianten kregen een lage prevalentie in onze resultaten. In grotere genengebruikten we een selectie van verschillende scenario’s van mogelijke splice varianten. In dezescenario’s konden de onwaarschijnlijke splice varianten weg gelaten worden. In simulaties gaf onsmodel een accurate schattingen. Met dit model hebben we vier mogelijk splice varianten gevondenin drie genen, die niet in de genetische databases staan, in patiënten met Marfan syndroom.
In Hoofdstuk 9 hebben we een penalized canonical correlation analysis (pCCA) om meer-dere hoog dimensionale biologische datasets te analyseren, bijvoorbeeld genetische en methylatiemarkers, (mi)RNA, eiwit en peptide expressie en fenotypen, gemeten in dezelfde individuen. Deresultaten worden weergegeven door sparse canonische variaten bestaande uit hoog-correlerendemarkers, moleculen en fenotypen. Wanneer de verschillende datasets bestaan uit (epi)genetischemarkers, RNA, eiwitten en peptide expressie variabelen en fenotypen, corresponderen de cano-nische varianten en de geassocieerde variabelen met de punten in de onderlinge pathogenetische-moleculaire pathways. Deze beschrijven het process van DNA, DNA transcriptie naar mRNA,en de translatie en proteïnen en peptiden en de metabolisme naar metabolieten en uiteindelijknaar observeerbare (ziekte-)fenotypen. Wanneer we pCCA toepasten op 2,245 BIOSTAT-CHFpatiënten, zagen we dat fenotypen voor hartfalen (overlijden, door hartfalen gerelateerde zie-kenhuisopname, en succesvolle behandeling) goed konden worden beschreven door geassocieerdecanonische variaten in genetische, proteomische en metabolische datasets. Onze pCCA bestaatuit twee facetten. Als eerste bepaalden we de optimale penalty parameters door 10-splits kruis-validatie, waarna we de uiteindelijke canonische variaten bepaalden. Vervolgens, werd er opdeze variaten nog een enrichment gedaan door bekende databanken door te zoeken. We heb-ben acht variaten berekend en hebben de enrichment voor één van hen uitgevoerd. We vondendat deze canonische variaat was betrokken bij de GPCR pathway, welke bestaat uit een groepvan cell-membraan receptoren en 40% van alle moderne medicatie is hier op gericht, inclusiefACE-inhibitor/ARB en beta-blocker. Dat we deze relevante resultaten vonden in patiënten met

170 Samenvatting
hartfalen, geeft aan dat pCCA een goede statistische methode is om fenotypen en verschillendeomic datasets gezamenlijk te analyseren.



LIST OF CONTRIBUTING AUTHORS

175
Stefan D. Anker, MD, PhDInnovative Clinical Trials, Department of Cardiology and Pneumology,University Medical Centre Göttingen (UMG), Göttingen, Germany
John G.F. Cleland, MD, PhDNational Heart & Lung Institute, Royal Brompton and Harefield Hospitals,Imperial College, London, UK
Biniyam G. Demissei, MD, PhDUniversity of Groningen, University Medical Center Groningen, The Netherlands
Kenneth Dickstein, MD, PhDUniversity of Stavanger, Stavanger, Norway andUniversity of Bergen, Bergen, Norway
Gerasimos Filippatos, MD, PhDDepartment of Cardiology, Heart Failure Unit,Athens University Hospital Attikon, Athens, Greece
Pim van der Harst, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Hans L. Hillege, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Michel H. Hof, PhDDepartment of Epidemiology, Biostatistics and Bioinformatics,Academic Medical Centre, Amsterdam, the Netherlands
Mohsin A.F Khan, PhDDepartment of Cardiology, Academic Medical Centre, Amsterdam, the Netherlands
Chim C. Lang, MD, PhDSchool of Medicine Centre for Cardiovascular and Lung Biology,Division of Medical Sciences,University of Dundee, Ninewells Hospital & Medical School, Dundee, UK
Peter van der Meer, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Jozine M. ter Maaten, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Marco Metra, MD, PhDInstitute of Cardiology, Department of Medical and Surgical Specialties,Radiological Sciences and Public Health, University of Brescia, Italy

176 List of contributing authors
Leong L. Ng, MD, PhDDepartment of Cardiovascular Sciences, University of Leicester, Glenfield Hospital andCardiovascular Theme, NIHR Leicester Biomedical Research Centre,Glenfield Hospital, Leicester, UK
Piotr Ponikowski, MD, PhDDepartment of Heart Diseases,Wroclaw Medical University, Poland andCardiology Department, Military Hospital, Wroclaw, Poland
Michiel Rienstra, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Nilesh J. Samani, MD, PhDDepartment of Cardiovascular Sciences, University of Leicester, Glenfield Hospital andCardiovascular Theme, NIHR Leicester Biomedical Research Centre,Glenfield Hospital, Leicester, UK
Jasper Tromp, MDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Dirk-Jan van Veldhuisen, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Adriaan A. Voors, MD, PhDDepartment of Cardiology, University of Groningen, Groningen, the Netherlands
Faiez Zannad, MD, PhDInserm CIC 1433, Université de Lorrain, CHU de Nancy, Nancy, France
Aeilko H. Zwinderman, PhDDepartment of Epidemiology, Biostatistics and Bioinformatics,Academic Medical Centre, Amsterdam, the Netherlands



ACKNOWLEDGEMENTS


181
Een proefschrift schrijven is een project dat mijn leven zowel op wetenschappelijk, profes-sioneel als op sociaal gebied enorm veranderd heeft. Dit proces heb ik uiteraard niet alleenkunnen doorlopen en is in grote mate een resultaat dat ontstaan is door bijdrage van veel ver-schillende mensen. Ik wil daarom iedereen bedanken die, in welke vorm dan ook, een aandeelheeft gehad aan de totstandkoming van dit proefschrift. Ik wil hier dan ook van de gelegenheidgebruik maken om een aantal personen in het bijzonder te bedanken voor hun bijdrage aan ditproefschrift.
Allereerst wil ik mijn eerste promotor, prof. dr. A.H. Zwinderman bedanken. Koos, enorm be-dankt voor de kans die je me gegeven hebt om mijn onderzoek onder jouw supervisie te voltooien.Het was een genoegen om onder jouw begeleiding aan dit proefschrift te kunnen werken. Je hebtme veel dingen geleerd, wat ik in de toekomst nog veelvuldig hoop toe te kunnen passen. Juistde ontspannen sfeer die je creëert en de persoonlijke aandacht die je geeft zijn enorm fijn om meete werken. Ondanks dat je enorm druk bent met van alles en nog wat, en mensen continu ietsvan je willen, krijg je het altijd voor elkaar tijd voor me vrij te maken. Ook wanneer ik ergensniet uit kwam, en ik plots binnen kwam lopen. Je hebt me altijd enorm vrij gelaten in mijnwerkzaamheden, wat uiteindelijk heeft geresulteerd in dit proefschrift.
Mijn tweede promotor, prof. dr. A.A. Voors. Beste Adriaan, je bent pas op het einde vanmijn promotietraject officieel betrokken als mijn promotor. Echter ben je, als hoofd en kartrekkervan BIOSTAT-CHF, al vanaf het allereerste begin van mijn promotietraject betrokken bij al mijnwerk binnen Work Package 7 - Systems Biology. Ik wil je danken voor alle teksten die je hebtdoorgelezen en aangepast. Vooral wanneer Koos en ik vanuit onze visie weer met een stuk aankwamen zetten die vol stond met statistiek waar jij je scherpe klinische blik op los liet om het stuktoch meer klinisch relevant te maken. Ik bewonder in het bijzonder hoe snel je op mails reageertmet alle teksten al nagekeken in de bijlage. Ik heb altijd bijzonder fijn met je samengewerkt.
Promotiecommissie, Yigel Pinto, Rudolf de Boer, Ameen Abu-Hanna, Bert Groen, Natal vanRiel en Dave Speijer, enorm bedankt voor het lezen en beoordelen van dit proefschrift. Ondanksjullie strakke schema hebben jullie de tijd genomen om dit proefschrift door te nemen en met mijin het openbaar van gedachten te wisselen tijden mijn verdediging van dit proefschrift.
Ook wil ik mijn Groningse collega promovendi, Jasper, bedanken. Jasper, we hebben veelgebrainstormd over hoe we nu weer een probleem konden oplossen. We konden altijd even bellen,ook al zat je merendeel van de tijd aan de andere kant van de wereld. Ik heb altijd bijzonderprettig met je samengewerkt. En ik hoop dat we in de toekomst nog een paar mooie projectenkunnen afronden.
I also want to thank all the members of the BIOSTAT-CHF consortium. With all yourenthusiasm, ideas and comments for many of the chapters in this PhD thesis. You all had a greatcontribution to many of the chapters in this thesis. The monthly and yearly BIOSTAT-CHFmeetings, first on congresses and later at Schiphol always were inspiring. I always left with newinsights for existing projects and new ideas for future projects.
Ook wil ik graag alle collega’s en oud-collega’s op de afdeling Klinische Epidemiologie, Bio-statistiek en Bioinformatica bedanken. Ik heb me vanaf het eerste moment altijd thuis gevoeldop de afdeling en daardoor altijd mezelf kunnen zijn. De KEBB-uitjes waren ook elk jaar weereen feest. Ik zal nog frequent langs blijven komen en hoop ook altijd contact te houden met hetmerendeel van de afdeling.
In het bijzonder wil ik mijn 207 kamergenoten bedanken. Erik, Michel, Raha en Marit. Toenik op de KEBB kwam werken had 207 de naam een echte rebelse kamer te zijn. Er werd tegenme gezegd: ’maak je borst maar nat’ wanneer ik zei dat ik op kamer J1B-207 kwam te zitten. Ikheb altijd met plezier op de kamer gezeten, en dat rebelse is er in de loop van de jaren wel eenbeetje af gegaan. Het lijkt er nu eerder op dat 207 een zeer vruchtbare kamer is waar iedereenop een gegeven moment ouder wordt. Ik hoop wel dat er wat nieuw bloed komt die de naam van

182 Acknowledgements
207 hoog weet te houden. Ook wil ik Marit bedanken dat ze bereid was om mij, als paranimf,bij te staan tijdens mijn verdediging.
Sam Garrett, bedankt voor het redigeren van een aantal hoofdstukken in dit proefschrift. Ikvoel me vereerd dat ik kan zeggen dat Sam Garrett aan een deel van mijn proefschrift heeftgewerkt.
Pap, mam, jullie hebben mij altijd gesteund in wat ik ook maar wilde doen. Of het nu wasom me zondag ’s ochtends om 8 uur naar volleybal training te brengen. Of wanneer ik bedachtom toch nog een extra Master te gaan doen. De mogelijkheden die jullie me geboden hebben zalik altijd blijven onthouden. En ik hoop dat ik dat ook aan mijn dochter kan bieden.
Maaike, je bent inmiddels zelf net begonnen met je PhD. Ik hoop dat je net zo een leuke tijdgaat hebben als dat ik heb gehad. Deze periode is zeer speciaal en gaat voorbij voor je het doorhebt. Dus geniet er van zolang het duurt! Jij bent degene geweest waardoor ik ben gaan kijkennaar een PhD positie. Dus eigenlijk heb ik dit gehele proefschrift aan jou te danken. Ik ga ervan uit dat er over een jaar of 3 ook een boekje van jou op de planken ligt. Ik ben er ook trotsop dat je de uitdaging bent aangegaan, en dat je bij mijn promotie als paranimf aanwezig wildezijn.
Niet in de laatste plaats wil ik in het bijzonder mijn steun en toeverlaat bedanken. Rosa,zonder jou was ik waarschijnlijk nooit op dit punt gekomen. Je hebt al mijn overdenkingen aanmoeten horen, ook als je er niet alles van snapte. Je was altijd mijn luisterend oor. Tijdens mijnPhD heb je zelf even een Master afgerond. Waar ik voltijd bezig was heb jij alles gewoon naastje werk gedaan. Het was af en toe best zwaar, maar je hebt het toch maar mooi geflikt! Ik hebdaar nog steeds enorm veel bewondering voor. Ik denk niet dat ik dat gekund had. Ik hoop nogheel lang met je samen te kunnen zijn.
Als laatste wil ik mijn kleine meisje bedanken. Terwijl ik dit aan het schrijven ben zit je nogin de buik van mamma. Ze zeggen dat je promotie onderzoek een zeer bijzondere ervaring is. Ikdenk dat het krijgen van een kind daar nog even voorbij schiet. Ik heb enorm veel zin om je opdeze wereld te mogen verwelkomen. Ik denk nu al enorm veel aan je. En dat zal de komende tijdalleen maar meer worden.



PHD PORTFOLIO


187
Name PhD student: Wouter OuwerkerkPhD period: 2012-2017Name PhD supervisors: Prof. dr. A.H. Zwinderman
Prof. dr. A.A. Voors
Conferences• 34th Annual Conference of the ISCB 2013 Munich
Poster: Contribution of Alternative splicing Isoforms in gene expression data
• European Society of Cardiology Congress 2014 BarcelonaPresentation: Baseline characteristics and mortality and heart failure hospitalization risks of Biostat-CHF
• 35th Annual Conference of the ISCB 2014 ViennaPoster: Contribution of Alternative splicing Isoforms in gene expression data
• American College of Cardiology Congress 2015 San Diego
• 36th Annual Conference of the ISCB 2015 UtrechtPoster: Integration of genomewide genetic, molecular and clinical censored outcome
• IBS Channel Network Conference 2015 NijmegenPoster: Integration of genomewide genetic, molecular and clinical censored outcome
• 37th Annual Conference of the ISCB 2016 BirminghamPoster: Penalized Canonical Corelation Analysis combining genomic, proteomic, laboratory and clinicalphenotypic data
• Annual BIOSTAT-CHF meeting 2012-2016Progress presentations
Teaching
• 2nd years medicine 2012-2014Tutorial: Medical statistics (SPSS)
• 3rd years medicine 2012-2014Tutorial: Medical statistics (SPSS)
• Master medical biochemistry and molecular biology 2013Workgroup: homosysteinemea; a risk factor for CVD
• Graduate-school: Advanced topics in biostatistics 2014R tutorial: Longitudinal data analysis
• Graduate-school: Genetic epidemiology 2014R tutorial: Genetic analysis

188 PhD Portfolio
Courses
• ISCB Munich 2013Prediction models
• ISCB Vienna 2014Statistical methods in Systems Medicine
• ISCB Utrecht 2015Applied multiple imputation in R
• IBS Nijmegen 2015Splines
• Weekly KEBB seminar 2012-2016
List of Publications• W. Ouwerkerk, A. A. Voors, S. D. Anker, J. G. Cleland, K. Dickstein, G. Filippatos, P.
van der Harst, H. L. Hillege, C. C. Lang, J. M. ter Maaten, L. Ng, P. Ponikowski, N. J.Samani, D. J. van Veldhuisen, F. Zannad, M. Metra, and A. H. Zwinderman, ”Determinantsand clinical outcome of uptitration of ACE-inhibitor and beta-blocker in patients with heartfailure: a prospective European study,” Eur. Heart J., in press (2017)
• A. A. Voors*, W. Ouwerkerk*, F. Zannad, D. J. van Veldhuisen, N. J. Samani, P.Ponikowski, L. Ng, M. Metra, J. M. ter Maaten, C. C. Lang, H. L. Hillege, P. van derHarst, G. Filippatos, K. Dickstein, J. G. Cleland, S. D. Anker, and A. H. Zwinderman,”Development and validation of multivariable models to predict mortality and hospitaliza-tion in patients with heart failure,” Eur. J. Heart Fail., in press (2017)
• W. Ouwerkerk and A. H. Zwinderman, ”Alternative Splice Variants in Gene ExpressionValues in Patients with Marfan’s Syndrome,” J. Proteomics Bioinform. 8, 1-8 (2015)
• W. Ouwerkerk, A. A. Voors, and A. H. Zwinderman, ”Factors influencing the predictivepower of models for predicting mortality and/or heart failure hospitalization in patientswith heart failure.,” JACC. Heart Fail. 2, 429-36 (2014)
• I. M. Visman, G. M. Bartelds, W. Ouwerkerk, A. C. J. Ravelli, L. M. Peelen, B. A.C. Dijkmans, M. Boers, and M. T. Nurmohamed, ”Effect of the application of trial inclu-sion criteria on the efficacy of adalimumab therapy in a rheumatoid arthritis cohort.,” J.Rheumatol., 38, 1884-90 (2011)
* Authors contributed equally


CURRICULUM VITAE


193
Wouter Ouwerkerk was born in Apeldoorn on 7 December1983. After receiving his pre-university degree at the Heemgaard,Apeldoorn, in 2002, he started with Medical Informatics at theAcademic Medical Center, University of Amsterdam. His masterthesis, titled: The place of biologicals (’the Eldorado gold’) inthe battle against rheumatism, was published in 2011 (Visman etal. J Rheumatol 2011). In this study his interest in personalizedmedicine were triggered. During his medical informatics study heworked as data-manager at the Jan van Breemen Institute, Ams-terdam, a specialized center which focused on complaints relatingto the musculoskeletal system, and rheumatic diseases. He wasresponsible for developing study databases for research projects,and facilitating research staff in ICT solutions.
After obtaining his masters degree medical informatics in 2006,he started another masters programme ’Management, Policy Anal-ysis and Entrepreneurship’, at the Vrije University, Amsterdam.In this master he focussed on governmental policy, qualitativeresearch methods, knowledge integration and patient participation, and followed several manage-ment courses.
In 2009 he started working at Factory-CRO, Bilthoven. A contract research organisationspecialized in medical devices and in-vitro diagnostics. He worked as data-manager on severaldifferent projects and was responsible for the creation of case report forms and study databases,the process of data cleaning and validation and export of study data. He also developed andimproved software applications for documenting and reporting in data-management and clinicaltrial processes. At Factory-CRO, he got additional training in good clinical practice (ICH-GCP),clinical investigation of medical devices for human subjects (ISO 14155), and adaptive trial de-signs.
In 2012 he started his PhD at the Department of Clinical Epidemiology, Biostatistics andBioinformatics at the Academic Medical Center, University of Amsterdam: A Systems biologystudy to tailored treatment in chronic heart failure. This PhD was part of a large multicenterEuropean project (BIOSTAT-CHF). BIOSTAT-CHF was especially designed to find biologicalmechanisms involved with response to ESC guideline-recommended pharmacological treatmentand patients prognosis. In this project he collaborated with the consortium members and workedon studies presented in this PhD thesis.
In 2016 he started working as a post-doc on a new research project at the ExperimentalDermatology Department at the Academic Medical Center, University of Amsterdam. Thisproject tries to identify a set of genetic auto-immune and vitiligo markers in melanoma patientsthat is able to predict response to immune checkpoint inhibitor treatment.


TERMS AND ABBREVIATIONS


197
Notation Description Page List
ACE-inhibitor angiotensin-converting-enzyme inhibitor
vii, ix, x, xiii–xv, 7, 9–11, 13, 14,23, 31, 40, 43–58, 62–78, 83, 84,87, 90, 94, 96, 102–106, 109, 110,112, 115–117, 136, 140, 143, 144,149–154, 161–163, 167–169, 197,219–221, 227, 229, 232, 234–243,
Glossary:angiotensin-converting-enzyme
inhibitor
ADHF acute decompensated heart failure xiii, xiv, 19, 21, 22, 24–26, 219,222, 224–226
AF atrial fibrillation3, 9, 48–50, 54, 56, 67, 73, 84, 87,96, 103, 108–110, 115, 117, 227,
228, 232–244AIC Akaike information criterion 32, 120, 123–131ALAT alanine aminotransferase 84, 227, 228, 230, 233, 244
albumin 8, 70, 71, 86, 87, 94, 96, 153, 227,230, 232, 234–243
ALCAM CD166 antigen 230, 245, 247
alkalinephosphatase
34, 35, 48, 50, 57, 58, 71, 72, 84,86, 87, 96, 98, 105, 227, 228, 230,
232–244angiotensin IIreceptor blocker ARBs block the action of angiotensin II by preventing an-
giotensin II from binding to angiotensin II receptors on themuscles surrounding blood vessels
7, 31, 45, 63, 83, 103, 140, 149,161, 197, 219–221
angiotensin-converting-enzymeinhibitor
ACE inhibitors block the conversion of angiotensin I to an-giotensin II
7, 31, 45, 63, 83, 103, 140, 149,161, 197, 219–221
ANP-propeptide atrial natriuretic peptide-propeptide 230, 232AP-N aminopeptidase N 230, 245, 247
ARB angiotensin II receptor blocker
vii, ix, x, xiii–xv, 7, 9–11, 13, 14,23, 31, 40, 43–58, 62–78, 83, 84,87, 90, 94, 96, 102–106, 109, 110,112, 115–117, 136, 140, 143, 144,149–154, 161–163, 167–169, 197,219–221, 227, 229, 232, 234–243,
Glossary: angiotensin II receptorblocker
ASAT aspartate aminotransferase 70–72, 84, 87, 96, 153, 227, 228,230, 232–242, 244
AXL tyrosine-protein kinase receptor UFO 230, 246, 250
AZU1 azurocidin 71, 72, 113, 114, 230, 233, 245,247
beta-blocker Beta blockers block the action of endogenous catecholaminesepinephrine (adrenaline) and norepinephrine (noradrenaline)on adrenergic beta receptors, of the sympathetic nervous sys-tem, which mediates the fight-or-flight response. Some blockall activation of β-adrenergic receptors and others are selec-tive.
vii, ix, x, xiii–xv, 7, 9–11, 13, 14,22, 30, 31, 34–36, 40, 43–58,62–78, 83, 84, 87, 90, 94, 96,102–106, 109, 110, 112, 113,115–117, 136, 140, 143, 144,
149–154, 161–163, 167–169, 227,229, 233–243
BIC Bayesian information criterion 84–88, 97, 120, 123–131bio-ADM bioactive adrenomedullin 70, 72, 228, 230, 232, 244
BIOSTAT-CHF The BIOlogy STudy to TAilored Treatment in Chronic HeartFailure
ix, xiii, 8–11, 13, 14, 30–32, 36,39–41, 44–48, 51, 56–58, 61–64,76, 78, 82, 83, 98, 102, 103, 105,106, 110, 112, 116, 117, 137, 140,141, 149–153, 155, 156, 163, 169
BLM hydrolase Bleomycin hydrolase 230, 245, 247
BMI body mass index8, 9, 22, 47–50, 54, 56–58, 65, 67,73, 84, 86, 87, 96, 105, 109, 115,
220, 227, 228, 232–244

198
Notation Description Page List
BNP B-type natriuretic peptide8–10, 31, 41, 45, 63, 64, 67, 72,73, 84, 103, 137, 151, 228, 230,
233, 244
BUN blood urea nitrogen
8, 9, 18, 20–23, 25, 30, 34–36, 40,64, 66–73, 76, 78, 84, 105, 110,
151, 153, 161, 167, 219–221, 227,228, 230, 232, 233, 244
CABG coronary artery bypass graft 9, 67, 73, 84, 109, 115, 227, 228,244
CASP-3 caspase-3 72, 113, 114, 231, 245, 247CCA canonical correlation analysis 14, 137, 155CCL15 C-C motif chemokine 15 231, 245, 247CCL16 C-C motif chemokine 16 231, 233, 245, 247CCL22 C-C motif chemokine 22 230, 245, 247CCL24 C-C motif chemokine 24 230, 245, 247CD163 scavenger receptor cysteine-rich type 1 protein m130 230, 246, 250CD93 complement component C1q receptor 231, 245, 247CDH5 cadherin-5 230, 245, 247
CHF chronic heart failure xiii, xiv, 19, 21, 22, 24–26, 56,219, 222–226
CHI3L1 chitinase-3-like protein 1 71, 231, 245, 247
CHIT1 chitoriosidase-1 71, 113, 114, 117, 154, 230, 233,245, 247
CI confidence intervalxiv, 3, 22–24, 36, 44, 51, 53, 54,
68–70, 72, 74, 102, 110, 112,219–221
CNTN1 contactin-1 230, 245, 247COL1A1 collagen alpha-1 (I) chain 231, 245, 247
COPD chronic obstructive pulmonary disease8, 9, 34, 35, 67, 68, 73, 84, 86, 87,
96, 98, 109, 115, 227, 228,232–244
CPA1 carboxypeptidase A1 231, 245, 247CPB1 carboxypeptidase B 231, 245, 247CRP C-reactive protein 72, 77, 231, 233CSTB cystatin-B 71, 72, 230, 245, 247CTSD cathepsin D 231, 245, 247CTSZ cathepsin Z 231, 245, 247CXCL16 C-X-C motif chemokine 16 230, 245, 247cystatin C 69, 72, 231
DBP diastolic blood pressure9, 23, 34, 35, 48–50, 54, 56–58, 67,68, 73, 84, 105, 109, 115, 152, 219,
228, 232, 233, 244DLK-1 protein delta homolog 1 230, 246, 249
DM diabetes mellitus
3, 8, 9, 19, 22, 23, 34, 35, 48–50,54, 56, 67, 68, 73, 84, 87, 92, 96,108, 109, 115, 116, 154, 219–221,
227, 228, 232–244
DNA deoxyribonucleic acid 4, 6, 131, 137, 141, 144, 154, 163,169
EGFR epidermal growth factor receptor 114, 231, 245, 248
eGFR estimated glomerular filtration rate
8, 9, 30, 34–36, 40, 47–50, 54,56–58, 67, 71, 73, 84, 86, 87, 90,
92, 96, 98, 105, 109, 110, 115, 151,153, 161, 167, 197, 219, 220, 227,
228, 232–244, Glossary:estimated glomerular filtration
rateEp-Cam epithelial cell adhesion molecule 114, 230, 245, 248EPHB4 ephrin type-B receptor 4 230, 245, 248ESAM-1 endothelial cell selective adhesion molecule 1 66, 230, 233
ESC European Society of Cardiologyxiii, 7, 8, 11, 13, 40, 45, 56–58,
63–66, 77, 83, 103, 104, 140, 149,152, 155, 156, 161–163, 167–169

199
Notation Description Page List
estimatedglomerularfiltration rate
We used two equations to calculation eGFR: MDRD, andCKD-EPIMDRD = 175 × sCr−1.154 × Age−0.203 × (0.742 if female) ×(1.212 if African American)?
CKD-EPI = 141 × min(sCr/λ, 1)α × max(sCr/λ, 1)−1.209 ×0.993Age × (1.018 if female) × (1.159 if African American)?
where: sCr is serum creatinine in mg/dL, λ is 0.7 for femalesand 0.9 for males, α is -0.329 for females and -0.411 for males,min indicates the minimum of sCr/λ or 1, and max indicatesthe maximum of sCr/λ or 1
8, 9, 34–36, 47–50, 54, 56, 67, 73,84, 87, 96, 105, 109, 115, 151, 161,
197, 219, 220, 227, 232–243
ET-1 endothlin-1 72, 230, 233
FABP4 fatty acid-binding protein, adipocyte 114, 230, 245, 248FAS tumor necrosis factor receptor superfamily member 6 231, 246, 250FGF-23 fibroblast growth factor 23 69–72, 153, 230, 232FT4 free thyroxine 228, 230, 233, 244
Gal-3 galectin-3 68, 230–233, 245Gal-4 galectin-4 72, 231, 245, 248Gamma-GT gamma glutamyl transferase 228, 230, 233, 244GDF-15 growth/differentiation factor 15 66, 114, 230, 231, 233, 245, 248GRN granulins 230, 245, 248GWAS genome wide association study 4, 12, 140, 156
Hclust hierarchical cluster analysis x, xv, 82–85, 88, 90, 92, 93, 95–98,153, 154, 162, 168, 242, 243
HDL high density lipoprotein34–36, 40, 64, 66, 71, 72, 84, 87,94, 96, 106, 109, 110, 115, 161,
167, 227, 228, 230, 232, 234–244hematocrit 34, 35, 64, 66, 84, 227, 230, 233
hemoglobin
8, 9, 22, 30, 34–36, 64, 66, 67, 69,71–73, 76–78, 84, 87, 96, 105, 109,115, 153, 161, 167, 227, 228, 230,
232, 234–244HFmrEF heart failure with mid-range ejection fraction 109, 114–116, 154, 156
HFpEF heart failure with preserved ejection fractionxiii, 4, 7, 9, 14, 32, 36, 39, 41, 97,109, 114–116, 150, 151, 154, 156,
161, 167, 227
HFrEF heart failure with reduced ejection fractionxiii, 3, 4, 7, 14, 32, 36, 39, 41, 44,
75, 97, 103, 109, 115, 116, 150,151, 154, 156, 161, 167
HR hazard ratio xiv, 20–23, 34–36, 44, 51, 53, 54,68, 71, 72, 102, 110, 112, 219–221
ICAM-2 intercellular adhesion molecule 2 231, 245, 248IGFBP insulin-like growth factor-binding protein 112
IGFBP-1 insulin-like growth factor-binding protein 1 71, 72, 113, 114, 230, 233, 245,248
IGFBP-2 insulin-like growth factor-binding protein 2 70–72, 114, 231, 232, 245, 248IGFBP-7 insulin-like growth factor-binding protein 7 114, 231, 245, 248IL-17RA interleukin-17 receptor A 71, 230, 245, 248IL-18BP interleukin-18 binding protein 231, 245, 248IL-1RT1 interleukin-1 receptor type 1 230, 245, 248IL-1RT2 interleukin-1 receptor type 2 231, 245, 248IL2-RA interleukin-2 receptor subunit Alpha 230, 245, 248IL6-RA interleukin-6 receptor subunit Alpha 114, 230, 245, 248IPW inverse probability weighting xiii, 47, 58, 106, 117
IQR interquartile range9, 10, 31, 33, 48, 50, 54, 56, 64,67, 73, 87, 88, 90, 96, 137, 140,
227, 228, 230, 231, 234–244, 247ITGB2 integrin beta-2 230, 245, 248
JAM-A junctional adhesion molecule A 113, 114, 231, 245, 248
JVP jugular venous pressure3, 8, 9, 34, 35, 67, 68, 73, 84, 87,
96, 98, 109, 115, 227, 228,232–244

200
Notation Description Page List
KLK6 kallikrein-6 231, 245, 248
LCA latent class analysis 83, 84LDL low density lipoprotein 64, 66, 84, 230, 232, 233LDL-receptor low-density lipoprotein receptor 71, 72, 114, 230, 245, 249LTβR lymphotoxin beta receptor 66, 230LTBR lympotoxin-beta receptor 230, 245
LVEF left ventricular ejection fraction
xiii, 3, 7–10, 22, 30, 31, 33, 44, 45,47–50, 54, 56, 63, 64, 66–68, 71,73, 78, 84, 86, 87, 90, 96, 103,
109, 115, 116, 151, 154, 227, 228,230, 232–244
m/z mass-to-charge ratio 140, 141MALDI matrix assisted laser desorption and ionization 140MALDI-TOF MALDI time-of-flight 6MALDI-TOF-MS MALDI-TOF mass spectrometry 137MB myoglobin 231, 245, 249
Mclust gaussian mixture for model-based clusteringx, xv, 82–86, 88, 89, 92, 95, 97,98, 124, 153, 154, 162, 168, 234,
235MCP-1 monocypte chemotactic protein 1 230, 245MEPE matrix extracellular phosphoglycoprotein 230, 249
MI myocardial infarction 3, 8, 9, 19, 67, 73, 84, 227, 228,232, 244
MMP-2 matrix metalloproteinase-2 230, 245, 249MMP-3 matrix metalloproteinase-3 231, 233, 245, 249MMP-9 matrix metalloproteinase-9 70, 71, 230, 245, 249MPO myeloperoxidase 66, 71, 230, 233, 245MRA mineralocorticoid receptor antagonist 7
mRNA messenger ribonucleic acid 6, 14, 121, 122, 124, 131, 137, 154,163, 169
NGAL neutrophil gelatinase associated lipocalin 71, 231–233NOTCH3 neurogenic locus notch homolog protein 3 230, 245, 249NPX normalized protein expression units 64, 71, 72, 104, 230–233
NT-proBNP N-terminal pro B-type natriuretic peptide
8–10, 21–23, 30, 31, 34–36, 41, 45,48–50, 54, 56, 63, 64, 67, 69–73,
76, 77, 84, 86, 87, 90, 92, 94,96–98, 103, 105, 107–110, 115,
116, 137, 141, 151, 153, 161, 167,219–221, 227, 228, 230–245
NT-proCNP N-terminal pro C-type natriuretic peptide 230
NYHA class New York Heart Association class
7–9, 22, 23, 30, 33–35, 65, 67, 71,73, 78, 84, 86, 87, 90, 92, 94, 96,97, 107–109, 115, 116, 137, 151,153, 219–221, 227, 228, 232–244
OPG osteoprotegerin 230, 233, 245, 249OPN osteopontin 66, 230, 231, 245, 249OR odds ratio 20–23, 219–221, 232, 233
PAI plasminogen activator inhibitor 1 230, 233, 245, 249
PAM partitioning around k-medoidsx, xv, 82–85, 88, 90, 92, 95, 97,98, 102, 105, 106, 153, 154, 162,
163, 168, 169, 238–241PCA principal component analysis 14, 105, 106, 117, 154, 163, 169
pCCA penalized canonical correlation analysis vii, 135–138, 140, 142, 144, 155,156, 163, 169, 170
PCI percutaneous coronary intervention 9, 67, 73, 84, 109, 115, 227, 228,232, 233, 244
PCSK9 proprotein convertase subtilisin/kexin type 9 231, 246, 249PCT procalcitonin 230PDGF platelet-derived growth factor subunit A 70, 72, 114, 231, 233, 246, 249PEA proximity extension assay 64, 104PECAM-1 platelet endothelial cell adhesion molecule 113, 114, 231, 245, 249PGLYRP1 peptidoglycan recognition protein 1 231, 245, 249PI3 elafin 72, 230, 245, 248

201
Notation Description Page List
PIGR-1 polymeric immunoglobulin receptor 1 231, 233PLC perlecan 230, 245, 249
poLCA polytomous latent class analysisx, xv, 82, 84, 85, 87, 88, 91, 92,95–98, 153, 154, 162, 168, 236,
237PON3 paraoxnase 72, 113, 114, 231, 245, 249
potassium 9, 64, 66, 67, 73, 84, 87, 96, 115,140, 227, 228, 230, 233–244
pro-ENK pro-enkephalin 69–72, 153, 230, 232, 233proADM pro-adrenomedullin 77, 136, 144, 231, 233PRTN3 myeloblastin 113, 114, 231, 245PSAP-B prosaposin B 66, 230PSP-D pulmonary surfactant-associated protein D 71, 230, 246, 249
RAGE receptor for advanced glycation endproducts 231RARRES2 retinoic acid receptor responder protein 2 231, 233, 246, 249
RCT randomized controlled trial7, 20, 25, 27, 31, 39, 45, 46, 56,
62–64, 77, 106, 116, 149, 152, 161,162, 168, 222–226
RETN resistin 230, 233, 246, 249
RNA ribonucleic acid 6, 120, 124, 125, 131, 136, 137,144, 154, 163, 169
RSS residual sum of squares 125, 126
SBP systolic blood pressure
8, 9, 21–23, 30, 34–36, 47–50, 54,56, 67, 73, 84, 86, 87, 90, 96, 106,
109, 110, 115, 152, 161, 167,219–221, 227, 228, 232–244
SCGB3A2 secretoglobin family 3A member 2 231, 246, 250
SD standard deviation9, 33, 48, 50, 54, 56, 67, 68, 73,84, 86–88, 90, 92, 96, 227, 228,
230, 231, 234–244
SE standard error 21, 24, 25, 47, 49, 50, 71, 72, 232,233
SELE E-selectin 230, 233, 245, 248SELP p-selectin 113, 114, 230, 245, 249
serum creatinine 8, 9, 64, 67, 69, 71, 73, 84, 140,161, 167, 220, 230, 232
SHPS-1 tyrosine-protein phosphatase non-receptor type substrate 1 231, 246, 250
SNP single nucleotide polymorphism xi, 4, 6, 12, 14, 141, 143, 145, 155,156
sodium
8, 9, 18, 20–22, 25, 34–36, 40, 64,66, 67, 71–73, 78, 84, 87, 96, 106,110, 115, 153, 161, 167, 220, 221,
227, 228, 230, 233–244SPON1 spondin-1 71, 230, 246, 250
ST2 69, 71, 72, 76, 77, 113, 114, 136,144, 231–233, 246, 250
sTfR soluble transferrin receptor 71, 72, 228, 230, 233, 244
t-PA tissue-type plasminogen activator 71, 113, 114, 231, 232, 246, 250TFF3 trefoil factor 3 71, 72, 230, 246, 250TFPI tissue factor pathway inhibitor 72, 230, 233, 246, 250TIMP4 metalloproteinase inhibitor 4 230, 245, 249TLT-2 trem-like transcript 2 protein 113, 114, 230, 246, 250TNF-R1 tumor necrosis factor receptor 1 231–233, 246, 250TNF-R1A tumor necrosis factor receptor 1A 231TNF-R2 tumor necrosis factor receptor 2 230, 246, 250TNFRSF10C tumor necrosis factor receptor superfamily member 10C 230, 246, 250TNFRSF14 tumor necrosis factor receptor superfamily member 14 114, 230, 233, 246, 250TNFSF13B tumor necrosis factor ligand superfamily member 13B 231, 246, 250TR trassferrin receptor protein 1 230, 246, 250TR-AP tartrate-resistant acid phosphatase type 5 230, 246, 250TRIPOD the Transparent Reporting of a multivariable prediction model
for Individual Prognosis Or Diagnosis12, 31, 150, 151
TSH hyroid-stimulating hormone 228, 230, 233, 244
U-PAR urokinase plasminogen activator surface receptor 69, 71, 72, 231, 246, 250

202
Notation Description Page List
uPA urokinase-type plasminogen activator 231, 246, 250
VEGFR-1 vascular endothelial growth factor receptor 71, 231vWF von Willebrand factor 114, 231, 233, 246, 250
WAP-4C WAP Four-Disulphide Core Domain Protein HE4 77, 231, 233



REFERENCES


207
[1] Stewart, S., MacIntyre, K., Hole, D. J., Capewell, S. & McMurray, J. J. More ’malignant’ than cancer? Five-yearsurvival following a first admission for heart failure. Eur. J. Heart Fail. 3, 315–22 (2001).
[2] Ceia, F. et al. Prevalence of chronic heart failure in Southwestern Europe: the EPICA study. Eur. J. Heart Fail. 4,531–9 (2002).
[3] Redfield, M. M. et al. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating thescope of the heart failure epidemic. JAMA 289, 194–202 (2003).
[4] Bleumink, G. S. et al. Genetic polymorphisms and heart failure. Genet. Med. 6, 465–74 (2004).[5] Mosterd, A. & Hoes, A. W. Clinical epidemiology of heart failure. Heart 93, 1137–46 (2007).[6] Jhund, P. S. et al. Long-term trends in first hospitalization for heart failure and subsequent survival between 1986 and
2003: a population study of 5.1 million people. Circulation 119, 515–23 (2009).[7] Stewart, S., Ekman, I., Ekman, T., Odén, A. & Rosengren, A. Population impact of heart failure and the most common
forms of cancer: a study of 1 162 309 hospital cases in Sweden (1988 to 2004). Circ. Cardiovasc. Qual. Outcomes 3,573–80 (2010).
[8] Holmström, A. et al. Increased comorbidities in heart failure patients � 85 years but declined from >90 years: datafrom the Swedish Heart Failure Registry. Int. J. Cardiol. 167, 2747–52 (2013).
[9] Roger, V. L. Epidemiology of heart failure. Circ. Res. 113, 646–59 (2013).[10] Gerber, Y. et al. A contemporary appraisal of the heart failure epidemic in Olmsted County, Minnesota, 2000 to 2010.
JAMA Intern. Med. 175, 996–1004 (2015).[11] Stewart, S. et al. The current cost of heart failure to the National Health Service in the UK. Eur. J. Heart Fail. 4,
361–71 (2002).[12] Fang, J., Mensah, G. a., Croft, J. B. & Keenan, N. L. Heart failure-related hospitalization in the U.S., 1979 to 2004.
J. Am. Coll. Cardiol. 52, 428–34 (2008).[13] Dickstein, K. et al. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2008: the Task
Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2008 of the European Society of Cardiology.Developed in collaboration with the Heart. Eur. Heart J. 29, 2388–442 (2008).
[14] Davie, a. P., Francis, C. M., Caruana, L., Sutherland, G. R. & McMurray, J. J. Assessing diagnosis in heart failure:which features are any use? QJM 90, 335–9 (1997).
[15] Fonseca, C. Diagnosis of heart failure in primary care. Heart Fail. Rev. 11, 95–107 (2006).[16] Mant, J. et al. Systematic review and individual patient data meta-analysis of diagnosis of heart failure, with modelling
of implications of different diagnostic strategies in primary care. Health Technol. Assess. 13, 1–207, iii (2009).[17] Kelder, J. C. et al. The diagnostic value of physical examination and additional testing in primary care patients with
suspected heart failure. Circulation 124, 2865–73 (2011).[18] Oudejans, I. et al. Clinical evaluation of geriatric outpatients with suspected heart failure: value of symptoms, signs,
and additional tests. Eur. J. Heart Fail. 13, 518–27 (2011).[19] Lee, D. S. et al. Association of parental heart failure with risk of heart failure in offspring. N. Engl. J. Med. 355,
138–47 (2006).[20] Franz, W. M., Müller, O. J. & Katus, H. A. Cardiomyopathies: from genetics to the prospect of treatment. Lancet
(London, England) 358, 1627–37 (2001).[21] Towbin, J. a. & Bowles, N. E. The failing heart. Nature 415, 227–33 (2002).[22] Morita, H., Seidman, J. & Seidman, C. E. Genetic causes of human heart failure. J. Clin. Invest. 115, 518–26 (2005).[23] Lopes, L. R. & Elliott, P. M. Genetics of heart failure. Biochim. Biophys. Acta 1832, 2451–61 (2013).[24] Touze, J.-e. & Fourcade, L. Cardiomyopathies in Tropical Countries: Causes and Nosological Perspective. World J.
Cardiovasc. Surg. 03, 201–208 (2013).[25] McMurray, J. J. V. et al. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012:
The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society ofCardiology. Developed in collaboration with the Heart. Eur. J. Heart Fail. 14, 803–69 (2012).
[26] Kumar, V., Abbas, A. K. & Aster, J. Robbins and Cotran Pathologic Basis of Disease (Elsevier - Health SciencesDivision, 2014), 9 edn.
[27] O’Connor, S. Examination Medicine (The Examination) (Edinburgh: Churchill Livingstone, 2009).[28] Jessup, M. & Brozena, S. Heart failure. N. Engl. J. Med. 348, 2007–18 (2003).[29] Mann, D. L. & Bristow, M. R. Mechanisms and models in heart failure: the biomechanical model and beyond.
Circulation 111, 2837–49 (2005).[30] National Institute for Health and Clinical Excellence. Chronic Heart Failure: National clinical guideline for diagnosis
and management in primary and secondary care. Tech. Rep. (2010).[31] Philbin, E. F., Rocco, T. A., Lindenmuth, N. W., Ulrich, K. & Jenkins, P. L. Systolic versus diastolic heart failure
in community practice: clinical features, outcomes, and the use of angiotensin-converting enzyme inhibitors. Am. J.Med. 109, 605–13 (2000).
[32] Badano, L. P. et al. Prevalence, clinical characteristics, quality of life, and prognosis of patients with congestive heartfailure and isolated left ventricular diastolic dysfunction. J. Am. Soc. Echocardiogr. 17, 253–61 (2004).
[33] Hogg, K., Swedberg, K. & McMurray, J. Heart failure with preserved left ventricular systolic function; epidemiology,clinical characteristics, and prognosis. J. Am. Coll. Cardiol. 43, 317–27 (2004).
[34] Peyster, E., Norman, J. & Domanski, M. Prevalence and predictors of heart failure with preserved systolic function:community hospital admissions of a racially and gender diverse elderly population. J. Card. Fail. 10, 49–54 (2004).
[35] Rutten, F. H. et al. Unrecognized heart failure in elderly patients with stable chronic obstructive pulmonary disease.Eur. Heart J. 26, 1887–94 (2005).
[36] Abhayaratna, W. P. et al. Prevalence of heart failure and systolic ventricular dysfunction in older Australians: theCanberra Heart Study. Med. J. Aust. 184, 151–4 (2006).
[37] Somaratne, J. B. et al. The prognostic significance of heart failure with preserved left ventricular ejection fraction: aliterature-based meta-analysis. Eur. J. Heart Fail. 11, 855–62 (2009).

208 References
[38] Magaña-Serrano, J. a. et al. Prevalence of heart failure with preserved ejection fraction in Latin American, MiddleEastern, and North African Regions in the I PREFER study (Identification of Patients With Heart Failure andPREserved Systolic Function: an epidemiological regional stu. Am. J. Cardiol. 108, 1289–96 (2011).
[39] Boonman-de Winter, L. J. M. et al. High prevalence of previously unknown heart failure and left ventricular dysfunctionin patients with type 2 diabetes. Diabetologia 55, 2154–62 (2012).
[40] Mureddu, G. F. et al. Prevalence of preclinical and clinical heart failure in the elderly. A population-based study inCentral Italy. Eur. J. Heart Fail. 14, 718–29 (2012).
[41] Tiller, D. et al. Prevalence of symptomatic heart failure with reduced and with normal ejection fraction in an elderlygeneral population-the CARLA study. PLoS One 8, e59225 (2013).
[42] van Riet, E. E. S. et al. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion.Eur. J. Heart Fail. 16, 772–7 (2014).
[43] van Riet, E. E. S. et al. Epidemiology of heart failure: the prevalence of heart failure and ventricular dysfunction inolder adults over time. A systematic review. Eur. J. Heart Fail. 18, 242–52 (2016).
[44] McMurray, J. J. V. et al. Angiotensin-neprilysin inhibition versus enalapril in heart failure. N. Engl. J. Med. 371,993–1004 (2014).
[45] Braunwald, E., Ross, J. & Sonnenblick, E. H. Mechanisms of contraction of the normal and failing heart. N. Engl. J.Med. 277, 962–71 contd (1967).
[46] Harrison, T. R. Tinsley Randolph Harrison 1900-1978. ”The pathogenesis of congestive heart failure”: then and now.1935. Medicine (Baltimore). 70, 67–80; discussion 80–1 (1991).
[47] Onwuanyi, A. & Taylor, M. Acute decompensated heart failure: pathophysiology and treatment. Am. J. Cardiol. 99,25D–30D (2007).
[48] Greyson, C. R. Pathophysiology of right ventricular failure. Crit. Care Med. 36, S57–65 (2008).[49] Haddad, F., Doyle, R., Murphy, D. J. & Hunt, S. A. Right ventricular function in cardiovascular disease, part II:
pathophysiology, clinical importance, and management of right ventricular failure. Circulation 117, 1717–31 (2008).[50] Lijnen, P. & Petrov, V. Antagonism of the renin-angiotensin-aldosterone system and collagen metabolism in cardiac
fibroblasts. Methods Find. Exp. Clin. Pharmacol. 21, 215–27 (1999).[51] Unger, T. & Li, J. The role of the renin-angiotensin-aldosterone system in heart failure. J. Renin. Angiotensin.
Aldosterone. Syst. 5 Suppl 1, S7–10 (2004).[52] Joseph, J. & Gilbert, E. M. The sympathetic nervous system in chronic heart failure. Prog. Cardiovasc. Dis. 41, 9–16
(1998).[53] Triposkiadis, F. et al. The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical
implications. J. Am. Coll. Cardiol. 54, 1747–62 (2009).[54] Zhang, D. Y. & Anderson, A. S. The sympathetic nervous system and heart failure. Cardiol. Clin. 32, 33–45, vii
(2014).[55] Schrier, R. W. & Abraham, W. T. Hormones and hemodynamics in heart failure. N. Engl. J. Med. 341, 577–85
(1999).[56] Deswal, A. et al. Cytokines and cytokine receptors in advanced heart failure: an analysis of the cytokine database
from the Vesnarinone trial (VEST). Circulation 103, 2055–9 (2001).[57] Chen, D., Assad-Kottner, C., Orrego, C. & Torre-Amione, G. Cytokines and acute heart failure. Crit. Care Med. 36,
S9–16 (2008).[58] Mann, D. L., Zipes, D. P., Libby, P. & Bonow, R. O. Braunwald’s Heart Disease: A Textbook of Cardiovascular
Medicine, 10th Edition (Saunders, 2014), 10th edn.[59] Shah, A. M. & Mann, D. L. In search of new therapeutic targets and strategies for heart failure: recent advances in
basic science. Lancet (London, England) 378, 704–12 (2011).[60] Noble, D. The future: putting Humpty-Dumpty together again. Biochem. Soc. Trans. 31, 156–8 (2003).[61] Kirschner, M. W. The meaning of systems biology. Cell 121, 503–4 (2005).[62] Board on Life Sciences & Division on Earth and Life Studies. A New Biology for the 21st Century (National Academies
Press, Washington, D.C., 2009).[63] Hood, L., Balling, R. & Auffray, C. Revolutionizing medicine in the 21st century through systems approaches. Biotech-
nol. J. 7, 992–1001 (2012).[64] Kaneko, K. Life: An Introduction to Complex Systems Biology. Understanding Complex Systems (Springer Berlin
Heidelberg, Berlin, 2006), 1 edn.[65] Alon, U. An introduction to systems biology : design principles of biological circuits / Uri Alon (2007).[66] Crick, F. H. On protein synthesis. Symp. Soc. Exp. Biol. 12, 138–63 (1958).[67] Crick, F. Central dogma of molecular biology. Nature 227, 561–3 (1970).[68] Medvedeva, Y. A. et al. Effects of cytosine methylation on transcription factor binding sites. BMC Genomics 15, 119
(2014).[69] Jaenisch, R. & Bird, A. Epigenetic regulation of gene expression: how the genome integrates intrinsic and environmental
signals. Nat. Genet. 33 Suppl, 245–54 (2003).[70] Borgel, J. et al. Targets and dynamics of promoter DNA methylation during early mouse development. Nat. Genet.
42, 1093–100 (2010).[71] Oda, M. et al. DNA methylation regulates long-range gene silencing of an X-linked homeobox gene cluster in a
lineage-specific manner. Genes Dev. 20, 3382–94 (2006).[72] Farthing, C. R. et al. Global mapping of DNA methylation in mouse promoters reveals epigenetic reprogramming of
pluripotency genes. PLoS Genet. 4, e1000116 (2008).[73] Tomazou, E. M. & Meissner, A. Epigenetic regulation of pluripotency. Adv. Exp. Med. Biol. 695, 26–40 (2010).[74] Christensen, B. C. et al. Aging and environmental exposures alter tissue-specific DNA methylation dependent upon
CpG island context. PLoS Genet. 5, e1000602 (2009).[75] Rakyan, V. K. et al. Human aging-associated DNA hypermethylation occurs preferentially at bivalent chromatin
domains. Genome Res. 20, 434–9 (2010).

209
[76] Miller, C. A. & Sweatt, J. D. Covalent modification of DNA regulates memory formation. Neuron 53, 857–69 (2007).[77] Fraga, M. F. et al. Epigenetic differences arise during the lifetime of monozygotic twins. Proc. Natl. Acad. Sci. U. S.
A. 102, 10604–9 (2005).[78] Jirtle, R. L. & Skinner, M. K. Environmental epigenomics and disease susceptibility. Nat. Rev. Genet. 8, 253–62
(2007).[79] Kucharski, R., Maleszka, J., Foret, S. & Maleszka, R. Nutritional control of reproductive status in honeybees via DNA
methylation. Science 319, 1827–30 (2008).[80] Clancy, S. & Brown, W. Translation: DNA to mRNA to Protein | Learn Science at Scitable. Nat. Educ. 1, 1–7 (2008).[81] Bauman, J., Jearawiriyapaisarn, N. & Kole, R. Therapeutic potential of splice-switching oligonucleotides. Oligonu-
cleotides 19, 1–13 (2009).[82] Graveley, B. R. Alternative splicing: increasing diversity in the proteomic world. Trends Genet. 17, 100–7 (2001).[83] Modrek, B. & Lee, C. A genomic view of alternative splicing. Nat. Genet. 30, 13–9 (2002).[84] Johnson, J. M. et al. Genome-wide survey of human alternative pre-mRNA splicing with exon junction microarrays.
Science 302, 2141–4 (2003).[85] Lareau, L. F., Green, R. E., Bhatnagar, R. S. & Brenner, S. E. The evolving roles of alternative splicing. Curr. Opin.
Struct. Biol. 14, 273–82 (2004).[86] Pan, Q., Shai, O., Lee, L. J., Frey, B. J. & Blencowe, B. J. Deep surveying of alternative splicing complexity in the
human transcriptome by high-throughput sequencing. Nat. Genet. 40, 1413–5 (2008).[87] Wang, E. T. et al. Alternative isoform regulation in human tissue transcriptomes. Nature 456, 470–6 (2008).[88] Wang, T. J. Significance of circulating troponins in heart failure: if these walls could talk. Circulation 116, 1217–20
(2007).[89] Kong, S. W. et al. Heart Failure-Associated Changes in RNA Splicing of Sarcomere Genes, vol. 3 (2010).[90] Lara-Pezzi, E., Gómez-Salinero, J., Gatto, A. & García-Pavía, P. The alternative heart: impact of alternative splicing
in heart disease. J. Cardiovasc. Transl. Res. 6, 945–55 (2013).[91] Dlamini, Z., Tshidino, S. C. & Hull, R. Abnormalities in Alternative Splicing of Apoptotic Genes and Cardiovascular
Diseases. Int. J. Mol. Sci. 16, 27171–90 (2015).[92] Savage, N. Proteomics: High-protein research. Nature 527, S6–7 (2015).[93] Wishart, D. S. Current progress in computational metabolomics. Brief. Bioinform. 8, 279–93 (2007).[94] Duarte, N. C. et al. Global reconstruction of the human metabolic network based on genomic and bibliomic data. Proc.
Natl. Acad. Sci. U. S. A. 104, 1777–82 (2007).[95] Smith, C. A. et al. METLIN: a metabolite mass spectral database. Ther. Drug Monit. 27, 747–51 (2005).[96] Karas, M. & Krüger, R. Ion formation in MALDI: the cluster ionization mechanism. Chem. Rev. 103, 427–40 (2003).[97] MacRae, C. A. The genetics of congestive heart failure. Heart Fail. Clin. 6, 223–30 (2010).[98] Cowley, A. J., Stainer, K., Wynne, R. D., Rowley, J. M. & Hampton, J. R. Comparison of the effects of captopril and
enoximone in patients with severe heart failure: a placebo controlled double-blind study. Int. J. Cardiol. 24, 311–6(1989).
[99] Packer, M. et al. Double-blind, placebo-controlled study of the efficacy of flosequinan in patients with chronic heartfailure. Principal Investigators of the REFLECT Study. J. Am. Coll. Cardiol. 22, 65–72 (1993).
[100] Ekman, I., Cleland, J. G. F., Andersson, B. & Swedberg, K. Exploring symptoms in chronic heart failure. Eur. J.Heart Fail. 7, 699–703 (2005).
[101] Ponikowski, P. et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: TheTask Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology(ESC). Developed with the special contribution . Eur. J. Heart Fail. 18, 891–975 (2016).
[102] Owan, T. E. et al. Trends in prevalence and outcome of heart failure with preserved ejection fraction. N. Engl. J. Med.355, 251–9 (2006).
[103] Bhatia, R. S. et al. Outcome of heart failure with preserved ejection fraction in a population-based study. N. Engl. J.Med. 355, 260–9 (2006).
[104] Yusuf, S. et al. Effects of candesartan in patients with chronic heart failure and preserved left-ventricular ejectionfraction: the CHARM-Preserved Trial. Lancet (London, England) 362, 777–81 (2003).
[105] Cleland, J. G. F. et al. The perindopril in elderly people with chronic heart failure (PEP-CHF) study. Eur. Heart J.27, 2338–45 (2006).
[106] Massie, B. M. et al. Irbesartan in patients with heart failure and preserved ejection fraction. N. Engl. J. Med. 359,2456–67 (2008).
[107] Robson, A. O., Kerr, D., Ashcroft, R. & Teasdale, G. The diuretic response to frusemide. Lancet (London, England)2, 1085–8 (1964).
[108] Sherman, L. G. et al. Piretanide, a potent diuretic with potassium-sparing properties, for the treatment of congestiveheart failure. Clin. Pharmacol. Ther. 40, 587–94 (1986).
[109] Bayliss, J., Norell, M., Canepa-Anson, R., Sutton, G. & Poole-Wilson, P. Untreated heart failure: clinical andneuroendocrine effects of introducing diuretics. Br. Heart J. 57, 17–22 (1987).
[110] Anand, I. S. et al. Diuretics as initial and sole treatment in chronic cardiac failure. Cardioscience 2, 273–8 (1991).[111] Patterson, J. H., Adams, K. F., Applefeld, M. M., Corder, C. N. & Masse, B. R. Oral torsemide in patients with
chronic congestive heart failure: effects on body weight, edema, and electrolyte excretion. Torsemide InvestigatorsGroup. Pharmacotherapy 14, 514–21 (1941).
[112] Wilson, J. R., Reichek, N., Dunkman, W. B. & Goldberg, S. Effect of diuresis on the performance of the failing leftventricle in man. Am. J. Med. 70, 234–9 (1981).
[113] Parker, J. O. The effects of oral ibopamine in patients with mild heart failure–a double blind placebo controlledcomparison to furosemide. The Ibopamine Study Group. Int. J. Cardiol. 40, 221–7 (1993).
[114] The CONSENSUS Trial Study Group. Effects of enalapril on mortality in severe congestive heart failure. Results ofthe Cooperative North Scandinavian Enalapril Survival Study (CONSENSUS). N. Engl. J. Med. 316, 1429–35 (1987).

210 References
[115] The SOLVD Investigators* & The Solvd Investigators. Effect of enalapril on survival in patients with reduced leftventricular ejection fractions and congestive heart failure. The SOLVD Investigators. N. Engl. J. Med. 325, 293–302(1991).
[116] Packer, M. et al. Comparative effects of low and high doses of the angiotensin-converting enzyme inhibitor, lisinopril,on morbidity and mortality in chronic heart failure. ATLAS Study Group. Circulation 100, 2312–8 (1999).
[117] The SOLVD Investigators. Effect of enalapril on mortality and the development of heart failure in asymptomaticpatients with reduced left ventricular ejection fractions. N. Engl. J. Med. 327, 685–91 (1992).
[118] Packer, M. et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. U.S.Carvedilol Heart Failure Study Group. N. Engl. J. Med. 334, 1349–55 (1996).
[119] CIBIS-II Investigators and Committees. The Cardiac Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial.Lancet (London, England) 353, 9–13 (1999).
[120] MERIT-HF Study Group. Effect of metoprolol CR/XL in chronic heart failure: Metoprolol CR/XL RandomisedIntervention Trial in Congestive Heart Failure (MERIT-HF). Lancet (London, England) 353, 2001–7 (1999).
[121] Hjalmarson, A. et al. Effects of controlled-release metoprolol on total mortality, hospitalizations, and well-being inpatients with heart failure: the Metoprolol CR/XL Randomized Intervention Trial in congestive heart failure (MERIT-HF). MERIT-HF Study Group. JAMA 283, 1295–302 (2000).
[122] Packer, M. et al. Effect of carvedilol on survival in severe chronic heart failure. N. Engl. J. Med. 344, 1651–8 (2001).[123] Packer, M. et al. Effect of carvedilol on the morbidity of patients with severe chronic heart failure: results of the
carvedilol prospective randomized cumulative survival (COPERNICUS) study. Circulation 106, 2194–9 (2002).[124] Flather, M. D. et al. Randomized trial to determine the effect of nebivolol on mortality and cardiovascular hospital
admission in elderly patients with heart failure (SENIORS). Eur. Heart J. 26, 215–25 (2005).[125] Pitt, B. et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N. Engl.
J. Med. 341, 709–717 (1999).[126] Zannad, F. et al. Eplerenone in Patients with Systolic Heart Failure and Mild Symptoms. N. Engl. J. Med. 364, 11–21
(2011).[127] Swedberg, K. et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study.
Lancet (London, England) 376, 875–85 (2010).[128] Swedberg, K. et al. Effects on outcomes of heart rate reduction by ivabradine in patients with congestive heart failure:
is there an influence of beta-blocker dose?: findings from the SHIFT (Systolic Heart failure treatment with the I(f)inhibitor ivabradine Trial) study. J. Am. Coll. Cardiol. 59, 1938–45 (2012).
[129] Askoxylakis, V. et al. Long-term survival of cancer patients compared to heart failure and stroke: a systematic review.BMC Cancer 10, 105 (2010).
[130] Zarrinkoub, R. et al. The epidemiology of heart failure, based on data for 2.1 million inhabitants in Sweden. Eur. J.Heart Fail. 15, 995–1002 (2013).
[131] Ziaeian, B. & Fonarow, G. C. Epidemiology and aetiology of heart failure. Nat. Rev. Cardiol. 13, 368–78 (2016).[132] Alla, F., Zannad, F. & Filippatos, G. Epidemiology of acute heart failure syndromes. Heart Fail. Rev. 12, 91–5 (2007).[133] Maggioni, A. P. et al. EURObservational Research Programme: regional differences and 1-year follow-up results of
the Heart Failure Pilot Survey (ESC-HF Pilot). Eur. J. Heart Fail. 15, 808–17 (2013).[134] Ohlmeier, C. et al. Incidence, prevalence and 1-year all-cause mortality of heart failure in Germany: a study based on
electronic healthcare data of more than six million persons. Clin. Res. Cardiol. 104, 688–96 (2015).[135] Pagidipati, N. J. & Gaziano, T. A. Estimating deaths from cardiovascular disease: a review of global methodologies
of mortality measurement. Circulation 127, 749–56 (2013).[136] Heidenreich, P. a., Sahay, A., Kapoor, J. R., Pham, M. X. & Massie, B. Divergent trends in survival and readmission
following a hospitalization for heart failure in the Veterans Affairs health care system 2002 to 2006. J. Am. Coll.Cardiol. 56, 362–8 (2010).
[137] Lum, H. D., Studenski, S. a., Degenholtz, H. B. & Hardy, S. E. Early hospital readmission is a predictor of one-yearmortality in community-dwelling older Medicare beneficiaries. J. Gen. Intern. Med. 27, 1467–74 (2012).
[138] Felker, G. M. et al. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARMProgram and the Duke Databank. J. Am. Coll. Cardiol. 50, 40–7 (2007).
[139] Allen, L. a. et al. Liver function abnormalities and outcome in patients with chronic heart failure: data from theCandesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity (CHARM) program. Eur. J.Heart Fail. 11, 170–7 (2009).
[140] Jackson, C. E. et al. Albuminuria in chronic heart failure: prevalence and prognostic importance. Lancet (London,England) 374, 543–50 (2009).
[141] Wedel, H. et al. Predictors of fatal and non-fatal outcomes in the Controlled Rosuvastatin Multinational Trial in HeartFailure (CORONA): incremental value of apolipoprotein A-1, high-sensitivity C-reactive peptide and N-terminal proB-type natriuretic peptide. Eur. J. Heart Fail. 11, 281–91 (2009).
[142] Ketchum, E. S. & Levy, W. C. Establishing prognosis in heart failure: a multimarker approach. Prog. Cardiovasc. Dis.54, 86–96 (2011).
[143] Komajda, M. et al. Factors associated with outcome in heart failure with preserved ejection fraction: findings fromthe Irbesartan in Heart Failure with Preserved Ejection Fraction Study (I-PRESERVE). Circ. Heart Fail. 4, 27–35(2011).
[144] Apple, F. S. et al. Simultaneous rapid measurement of whole blood myoglobin, creatine kinase MB, and cardiactroponin I by the triage cardiac panel for detection of myocardial infarction. Clin. Chem. 45, 199–205 (1999).
[145] Straface, A. L., Myers, J. H., Kirchick, H. J. & Blick, K. E. A rapid point-of-care cardiac marker testing strategyfacilitates the rapid diagnosis and management of chest pain patients in the emergency department. Am. J. Clin.Pathol. 129, 788–95 (2008).
[146] Olink Bioscience. Proseek Multiplex CVD III 96x96 (2015).[147] Ross, J. S. et al. Statistical models and patient predictors of readmission for heart failure: a systematic review. Arch.
Intern. Med. 168, 1371–86 (2008).

211
[148] Giamouzis, G. et al. Hospitalization epidemic in patients with heart failure: risk factors, risk prediction, knowledgegaps, and future directions. J. Card. Fail. 17, 54–75 (2011).
[149] Kansagara, D. et al. Risk prediction models for hospital readmission: a systematic review. JAMA 306, 1688–98 (2011).[150] Betihavas, V. et al. What are the factors in risk prediction models for rehospitalisation for adults with chronic heart
failure? Aust. Crit. Care 25, 31–40 (2012).[151] Voors, A. A. et al. A systems BIOlogy Study to TAilored Treatment in Chronic Heart Failure: rationale, design, and
baseline characteristics of BIOSTAT-CHF. Eur. J. Heart Fail. 18, 716–26 (2016).[152] Collins, G. S., Reitsma, J. B., Altman, D. G. & Moons, K. G. M. Transparent Reporting of a multivariable prediction
model for Individual Prognosis or Diagnosis (TRIPOD): the TRIPOD statement. Ann. Intern. Med. 162, 55–63(2015).
[153] Cleland, J. G. F. Contemporary management of heart failure in clinical practice. Heart 88 Suppl 2, ii5–8 (2002).[154] Komajda, M. et al. The EuroHeart Failure Survey programme–a survey on the quality of care among patients with
heart failure in Europe. Part 2: treatment. Eur. Heart J. 24, 464–74 (2003).[155] Kalra, P. R. et al. Discontinuation of beta-blockers in cardiovascular disease: UK primary care cohort study. Int. J.
Cardiol. 167, 2695–9 (2013).[156] Newby, L. K. et al. Long-term adherence to evidence-based secondary prevention therapies in coronary artery disease.
Circulation 113, 203–12 (2006).[157] Gislason, G. H. et al. Persistent use of evidence-based pharmacotherapy in heart failure is associated with improved
outcomes. Circulation 116, 737–44 (2007).[158] Shah, S. J. et al. Phenomapping for novel classification of heart failure with preserved ejection fraction. Circulation
131, 269–79 (2015).[159] Ahmad, T. et al. Clinical Implications of Cluster Analysis-Based Classification of Acute Decompensated Heart Failure
and Correlation with Bedside Hemodynamic Profiles. PLoS One 11, e0145881 (2016).[160] Kanungo, T. et al. An efficient k-means clustering algorithm: analysis and implementation. IEEE Trans. Pattern
Anal. Mach. Intell. 24, 881–892 (2002).[161] Celebi, M. E. Improving the performance of k-means for color quantization. Image Vis. Comput. 29, 260–271 (2011).[162] Celebi, M. E., Kingravi, H. A. & Vela, P. A. A comparative study of efficient initialization methods for the k-means
clustering algorithm. Expert Syst. Appl. 40, 200–210 (2013).[163] Francis, G. S., Cogswell, R. & Thenappan, T. The heterogeneity of heart failure: will enhanced phenotyping be
necessary for future clinical trial success? J. Am. Coll. Cardiol. 64, 1775–6 (2014).[164] Altman, R. B. & Ashley, E. A. Using ”big data” to dissect clinical heterogeneity. Circulation 131, 232–3 (2015).[165] Sakharkar, M. K., Chow, V. T. K. & Kangueane, P. Distributions of exons and introns in the human genome. In
Silico Biol. 4, 387–93 (2004).[166] Daskalaki, A. Handbook of Research on Systems Biology Applications in Medicine (IGI Global, Hershey - New York,
2009).[167] Prokop, A. & Michelson, S. Systems Biology in Biotech and Pharma, vol. 2 of SpringerBriefs in Pharmaceutical
Science and Drug Development (Springer Netherlands, Dordrecht, 2012).[168] GTEx Consortium. The Genotype-Tissue Expression (GTEx) project. Nat. Genet. 45, 580–5 (2013).[169] Carithers, L. J. et al. A Novel Approach to High-Quality Postmortem Tissue Procurement: The GTEx Project.
Biopreserv. Biobank. 13, 311–9 (2015).[170] GTEx Consortium. Human genomics. The Genotype-Tissue Expression (GTEx) pilot analysis: multitissue gene
regulation in humans. Science 348, 648–60 (2015).[171] Karamizadeh, S., Abdullah, S. M., Manaf, A. A., Zamani, M. & Hooman, A. An Overview of Principal Component
Analysis. J. Signal Inf. Process. 04, 173–175 (2013).[172] Gromski, P. S. et al. A tutorial review: Metabolomics and partial least squares-discriminant analysis–a marriage of
convenience or a shotgun wedding. Anal. Chim. Acta 879, 10–23 (2015).[173] Hotelling, H. Relations Between Two Sets of Variates. Biometrika 28, 321 (1936).[174] Waaijenborg, S., Verselewel de Witt Hamer, P. C. & Zwinderman, A. H. Quantifying the association between gene
expressions and DNA-markers by penalized canonical correlation analysis. Stat. Appl. Genet. Mol. Biol. 7, Article3(2008).
[175] Waaijenborg, S. & Zwinderman, A. H. Associating multiple longitudinal traits with high-dimensional single-nucleotidepolymorphism data: application to the Framingham Heart Study. BMC Proc. 3 Suppl 7, S47 (2009).
[176] McCullough, P. a. et al. Confirmation of a heart failure epidemic: findings from the Resource Utilization AmongCongestive Heart Failure (REACH) study. J. Am. Coll. Cardiol. 39, 60–9 (2002).
[177] Roger, V. L. et al. Trends in heart failure incidence and survival in a community-based population. JAMA 292, 344–50(2004).
[178] Thom, T. et al. Heart disease and stroke statistics–2006 update: a report from the American Heart AssociationStatistics Committee and Stroke Statistics Subcommittee. Circulation 113, e85–151 (2006).
[179] Hunt, S. A. et al. 2009 Focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis andManagement of Heart Failure in Adults A Report of the American College of Cardiology Foundation/American HeartAssociation Task Force on Practice Guidelines Developed . J. Am. Coll. Cardiol. 53, e1–e90 (2009).
[180] Antman, E. M. et al. The TIMI risk score for unstable angina/non-ST elevation MI: A method for prognosticationand therapeutic decision making. JAMA 284, 835–42 (2000).
[181] Lip, G. Y. H., Nieuwlaat, R., Pisters, R., Lane, D. a. & Crijns, H. J. G. M. Refining clinical risk stratification forpredicting stroke and thromboembolism in atrial fibrillation using a novel risk factor-based approach: the euro heartsurvey on atrial fibrillation. Chest 137, 263–72 (2010).
[182] Steyerberg, E. Applications of Prediction Models. In Clin. Predict. Model. A Pract. Approach to Dev. Validation,Updat., Statistics for Biology and Health, chap. 2, 9–30 (Springer New York, New York, NY, 2009).
[183] Nutter, A. L., Tanawuttiwat, T. & Silver, M. a. Evaluation of 6 prognostic models used to calculate mortality rates inelderly heart failure patients with a fatal heart failure admission. Congest. Heart Fail. 16, 196–201 (2010).

212 References
[184] Kalogeropoulos, A. P. et al. Utility of the Seattle Heart Failure Model in patients with advanced heart failure. J. Am.Coll. Cardiol. 53, 334–42 (2009).
[185] Hartigan, J. A. Clustering Algorithms. In Clust. Algorithms, 365 (Wiley, New York, 1975).[186] Everitt, B. S., Landau, S., Leese, M. & Stahl, D. Cluster Analysis (Halsted, New York, 1980), fifth edn.[187] Ploner, A. Heatplus: Heatmaps with row and/or column covariates and colored clusters (2012).[188] Borenstein, M., Hedges, L. V., Higgins, J. P. & Rothstein, H. R. A basic introduction to fixed-effect and random-effects
models for meta-analysis. Res. Synth. Methods 1, 97–111 (2010).[189] Shah, S., Vanclay, F. & Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin.
Epidemiol. 42, 703–9 (1989).[190] Martín-Sánchez, F. J. et al. Barthel Index-Enhanced Feedback for Effective Cardiac Treatment (BI-EFFECT) Study:
contribution of the Barthel Index to the Heart Failure Risk Scoring System model in elderly adults with acute heartfailure in the emergency department. J. Am. Geriatr. Soc. 60, 493–8 (2012).
[191] Yamokoski, L. M. et al. Prediction of rehospitalization and death in severe heart failure by physicians and nurses ofthe ESCAPE trial. J. Card. Fail. 13, 8–13 (2007).
[192] Tabak, Y. P., Johannes, R. S. & Silber, J. H. Using automated clinical data for risk adjustment: development andvalidation of six disease-specific mortality predictive models for pay-for-performance. Med. Care 45, 789–805 (2007).
[193] Ky, B. et al. High-sensitivity ST2 for prediction of adverse outcomes in chronic heart failure. Circ. Heart Fail. 4,180–7 (2011).
[194] Ketchum, E. S. et al. Selective improvement in Seattle Heart Failure Model risk stratification using iodine-123 meta-iodobenzylguanidine imaging. J. Nucl. Cardiol. 19, 1007–16 (2012).
[195] Wang, L. et al. Predicting risk of hospitalization or death among patients with heart failure in the veterans healthadministration. Am. J. Cardiol. 110, 1342–9 (2012).
[196] Levy, W. C. et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation 113, 1424–33(2006).
[197] Selker, H. P., Griffith, J. L. & D’Agostino, R. B. A time-insensitive predictive instrument for acute hospital mortalitydue to congestive heart failure: development, testing, and use for comparing hospitals: a multicenter study. Med. Care32, 1040–52 (1994).
[198] Krumholz, H. M. et al. An administrative claims model suitable for profiling hospital performance based on 30-daymortality rates among patients with heart failure. Circulation 113, 1693–701 (2006).
[199] McAlister, F. A., Stewart, S., Ferrua, S. & McMurray, J. J. J. V. Multidisciplinary strategies for the management ofheart failure patients at high risk for admission: a systematic review of randomized trials. J. Am. Coll. Cardiol. 44,810–9 (2004).
[200] Whellan, D. J., Hasselblad, V., Peterson, E., O’Connor, C. M. & Schulman, K. A. Metaanalysis and review of heartfailure disease management randomized controlled clinical trials. Am. Heart J. 149, 722–9 (2005).
[201] de la Porte, P. W. et al. Added value of a physician-and-nurse-directed heart failure clinic: results from the Deventer-Alkmaar heart failure study. Heart 93, 819–25 (2007).
[202] Jaarsma, T. et al. Effect of moderate or intensive disease management program on outcome in patients with heartfailure: Coordinating Study Evaluating Outcomes of Advising and Counseling in Heart Failure (COACH). Arch. Intern.Med. 168, 316–24 (2008).
[203] Fonarow, G. C. et al. Improving evidence-based care for heart failure in outpatient cardiology practices: primary resultsof the Registry to Improve the Use of Evidence-Based Heart Failure Therapies in the Outpatient Setting (IMPROVEHF). Circulation 122, 585–96 (2010).
[204] Ouwerkerk, W., Voors, A. A. & Zwinderman, A. H. Factors influencing the predictive power of models for predictingmortality and/or heart failure hospitalization in patients with heart failure. JACC. Heart Fail. 2, 429–36 (2014).
[205] Harrell ,, F. E. Regression Modeling Strategies. Springer Series in Statistics (Springer International Publishing, NewYork, 2015), 2 edn.
[206] Grambsch, P. M. & Therneau, T. M. Proportional Hazards Tests and Diagnostics Based on Weighted Residuals.Biometrika 81, 515 (1994).
[207] van Buuren, S. & Groothuis-Oudshoorn, K. mice : Multivariate Imputation by Chained Equations in R. J. Stat. Softw.45, 1–67 (2011).
[208] Breiman, L., Freidman, J. H., Olshen, R. & Stone, C. Classification and Regression (Chapman and Hall, New York,1984).
[209] Harrell, F. E., Lee, K. L. & Mark, D. B. Multivariable prognostic models: issues in developing models, evaluatingassumptions and adequacy, and measuring and reducing errors. Stat. Med. 15, 361–87 (1996).
[210] Musoro, J. Z., Zwinderman, A. H., Puhan, M. a., ter Riet, G. & Geskus, R. B. Validation of prediction models basedon lasso regression with multiply imputed data. BMC Med. Res. Methodol. 14, 116 (2014).
[211] Pocock, S. J. et al. Predicting survival in heart failure: a risk score based on 39 372 patients from 30 studies. Eur.Heart J. 34, 1404–13 (2013).
[212] Calvillo-King, L. et al. Impact of social factors on risk of readmission or mortality in pneumonia and heart failure:systematic review. J. Gen. Intern. Med. 28, 269–82 (2013).
[213] Dharmarajan, K. et al. Diagnoses and timing of 30-day readmissions after hospitalization for heart failure, acutemyocardial infarction, or pneumonia. JAMA 309, 355–63 (2013).
[214] Kociol, R. D. et al. Are we targeting the right metric for heart failure? Comparison of hospital 30-day readmissionrates and total episode of care inpatient days. Am. Heart J. 165, 987–994.e1 (2013).
[215] Krumholz, H. M. et al. Relationship between hospital readmission and mortality rates for patients hospitalized withacute myocardial infarction, heart failure, or pneumonia. JAMA 309, 587–93 (2013).
[216] Bello, N. A. et al. Influence of previous heart failure hospitalization on cardiovascular events in patients with reducedand preserved ejection fraction. Circ. Heart Fail. 7, 590–5 (2014).

213
[217] Gheorghiade, M. et al. Assessing and grading congestion in acute heart failure: a scientific statement from the acuteheart failure committee of the heart failure association of the European Society of Cardiology and endorsed by theEuropean Society of Intensive Care Medicine. Eur. J. Heart Fail. 12, 423–33 (2010).
[218] Filippatos, G. et al. Prognostic value of blood urea nitrogen in patients hospitalized with worsening heart failure:insights from the Acute and Chronic Therapeutic Impact of a Vasopressin Antagonist in Chronic Heart Failure (ACTIVin CHF) study. J. Card. Fail. 13, 360–4 (2007).
[219] Cleland, J. G. et al. Predictors of postdischarge outcomes from information acquired shortly after admission foracute heart failure: a report from the Placebo-Controlled Randomized Study of the Selective A1 Adenosine ReceptorAntagonist Rolofylline for Patients Hospitalized W. Circ. Heart Fail. 7, 76–87 (2014).
[220] Mehra, M. R. et al. High-density Lipoprotein Cholesterol Levels and Prognosis in Advanced Heart Failure. J. HeartLung Transplant. 28, 876–880 (2009).
[221] Connelly, M. A., Shalaurova, I. & Otvos, J. D. High-density lipoprotein and inflammation in cardiovascular disease.Transl. Res. 173, 7–18 (2016).
[222] Gheorghiade, M. et al. Relationship between admission serum sodium concentration and clinical outcomes in patientshospitalized for heart failure: an analysis from the OPTIMIZE-HF registry. Eur. Heart J. 28, 980–8 (2007).
[223] Khazanie, P. et al. Predictors of clinical outcomes in acute decompensated heart failure: Acute Study of ClinicalEffectiveness of Nesiritide in Decompensated Heart Failure outcome models. Am. Heart J. 170, 290–7 (2015).
[224] Pogue, J., Walter, S. D. & Yusuf, S. Evaluating the benefit of event adjudication of cardiovascular outcomes in largesimple RCTs. Clin. Trials 6, 239–51 (2009).
[225] Cohn, J. N. et al. A comparison of enalapril with hydralazine-isosorbide dinitrate in the treatment of chronic congestiveheart failure. N. Engl. J. Med. 325, 303–10 (1991).
[226] Garg, R. & Yusuf, S. Overview of randomized trials of angiotensin-converting enzyme inhibitors on mortality andmorbidity in patients with heart failure. Collaborative Group on ACE Inhibitor Trials. JAMA 273, 1450–6 (1995).
[227] Poole-Wilson, P. a. et al. Comparison of carvedilol and metoprolol on clinical outcomes in patients with chronicheart failure in the Carvedilol Or Metoprolol European Trial (COMET): randomised controlled trial. Lancet (London,England) 362, 7–13 (2003).
[228] Bristow, M. R. et al. Carvedilol produces dose-related improvements in left ventricular function and survival in subjectswith chronic heart failure. MOCHA Investigators. Circulation 94, 2807–16 (1996).
[229] Konstam, M. A. et al. Effects of high-dose versus low-dose losartan on clinical outcomes in patients with heart failure(HEAAL study): a randomised, double-blind trial. Lancet (London, England) 374, 1840–8 (2009).
[230] Lawless, J. F. & Singhal, K. Efficient Screening of Nonnormal Regression Models. Biometrics 34, 318 (1978).[231] Altman, D. G. & Andersen, P. K. Bootstrap investigation of the stability of a Cox regression model. Stat. Med. 8,
771–83 (1989).[232] Box, G. E. P. & Cox, D. R. An Analysis of Transformations Revisited, Rebutted. J. Am. Stat. Assoc. 77, 209 (1982).[233] Clark, J. E., Osborne, J. W., Gallagher, P. & Watson, S. A simple method for optimising transformation of non-
parametric data: an illustration by reference to cortisol assays. Hum. Psychopharmacol. 31, 259–67 (2016).[234] Eilers, P. H. C. & Marx, B. D. Flexible smoothing with B -splines and penalties. Stat. Sci. 11, 89–121 (1996).[235] Holland, P. W. Statistics and Causal Inference. J. Am. Stat. Assoc. 81, 945–960 (1986).[236] Rubin, D. B. Causal Inference Using Potential Outcomes. J. Am. Stat. Assoc. 100, 322–331 (2005).[237] Adelson, J. L. Educational Research with Real-World Data: Reducing Selection Bias with Propensity Scores. Pract.
Assessment, Res. Eval. 18, 1–11 (2013).[238] Robins, J. M., Rotnitzky, A. & Zhao, L. P. Estimation of Regression Coefficients When Some Regressors are not
Always Observed. J. Am. Stat. Assoc. 89, 846–866 (1994).[239] Zetterqvist, J. & Sjölander, A. Doubly Robust Estimation with the R Package drgee. Epidemiol. Method. 4 (2015).[240] van der Wal, W. M. & Geskus, R. B. ipw : An R Package for Inverse Probability Weighting. J. Stat. Softw. 43, 1–22
(2011).[241] The NETWORK investigators. Clinical outcome with enalapril in symptomatic chronic heart failure; a dose comparison.
The NETWORK Investigators. Eur. Heart J. 19, 481–9 (1998).[242] Willenheimer, R. et al. Effect on survival and hospitalization of initiating treatment for chronic heart failure with biso-
prolol followed by enalapril, as compared with the opposite sequence: results of the randomized Cardiac InsufficiencyBisoprolol Study (CIBIS) III. Circulation 112, 2426–35 (2005).
[243] McMurray, J. J. V. et al. Dual angiotensin receptor and neprilysin inhibition as an alternative to angiotensin-convertingenzyme inhibition in patients with chronic systolic heart failure: rationale for and design of the Prospective comparisonof ARNI with ACEI to Determine Impact. Eur. J. Heart Fail. 15, 1062–73 (2013).
[244] Deedwania, P. C. et al. Efficacy, safety and tolerability of beta-adrenergic blockade with metoprolol CR/XL in elderlypatients with heart failure. Eur. Heart J. 25, 1300–9 (2004).
[245] Anand, I. S., Deswal, A., Kereiakes, D. J., Purkayastha, D. & Zappe, D. H. Comparison of once-daily versus twice-dailydosing of valsartan in patients with chronic stable heart failure. Vasc. Health Risk Manag. 6, 449–455 (2010).
[246] Chatterjee, S. et al. Benefits of β blockers in patients with heart failure and reduced ejection fraction: networkmeta-analysis. BMJ 346, f55 (2013).
[247] Düngen, H.-D. et al. Titration to target dose of bisoprolol vs. carvedilol in elderly patients with heart failure: theCIBIS-ELD trial. Eur. J. Heart Fail. 13, 670–80 (2011).
[248] Persson, H. et al. Improved pharmacological therapy of chronic heart failure in primary care: a randomized Studyof NT-proBNP Guided Management of Heart Failure–SIGNAL-HF (Swedish Intervention study–Guidelines and NT-proBNP AnaLysis in Heart Failure). Eur. J. Heart Fail. 12, 1300–8 (2010).
[249] Goldenberg, I. et al. Inverse relationship of blood pressure levels to sudden cardiac mortality and benefit of theimplantable cardioverter-defibrillator in patients with ischemic left ventricular dysfunction. J. Am. Coll. Cardiol. 49,1427–33 (2007).
[250] Güder, G. et al. Reverse epidemiology in systolic and nonsystolic heart failure: cumulative prognostic benefit ofclassical cardiovascular risk factors. Circ. Heart Fail. 2, 563–71 (2009).

214 References
[251] Merlo, M. et al. Prevalence and prognostic significance of left ventricular reverse remodeling in dilated cardiomyopathyreceiving tailored medical treatment. J. Am. Coll. Cardiol. 57, 1468–76 (2011).
[252] Brenyo, A. et al. Predictors of spontaneous reverse remodeling in mild heart failure patients with left ventriculardysfunction. Circ. Heart Fail. 7, 565–72 (2014).
[253] Güder, G. et al. Nurse-coordinated collaborative disease management improves the quality of guideline-recommendedheart failure therapy, patient-reported outcomes, and left ventricular remodelling. Eur. J. Heart Fail. 17, 442–52(2015).
[254] Sokol, S. I., Cheng, A., Frishman, W. H. & Kaza, C. S. Cardiovascular drug therapy in patients with hepatic diseasesand patients with congestive heart failure. J. Clin. Pharmacol. 40, 11–30 (2000).
[255] Alvarez, A. M. & Mukherjee, D. Liver abnormalities in cardiac diseases and heart failure. Int. J. Angiol. 20, 135–42(2011).
[256] Massie, B. M. et al. Toleration of high doses of angiotensin-converting enzyme inhibitors in patients with chronic heartfailure: results from the ATLAS trial. The Assessment of Treatment with Lisinopril and Survival. Arch. Intern. Med.161, 165–71 (2001).
[257] Clemens, M. et al. The Seattle Heart Failure Model predicts survival in patients with cardiac resynchronization therapy:a validation study. J. Card. Fail. 18, 682–7 (2012).
[258] Nanas, J. N. et al. Outcome of patients with congestive heart failure treated with standard versus high doses ofenalapril: a multicenter study. High Enalapril Dose Study Group. J. Am. Coll. Cardiol. 36, 2090–5 (2000).
[259] Dobre, D. et al. Tolerability and dose-related effects of nebivolol in elderly patients with heart failure: data fromthe Study of the Effects of Nebivolol Intervention on Outcomes and Rehospitalisation in Seniors with Heart Failure(SENIORS) trial. Am. Heart J. 154, 109–15 (2007).
[260] Voors, A. A. et al. Development and validation of multivariable models to predict mortality and hospitalization inpatients with heart failure. Eur. J. Heart Fail. 2, 429–36 (2017).
[261] Ouwerkerk, W. et al. Determinants and clinical outcome of uptitration of ACE-inhibitors and beta-blockers in patientswith heart failure: a prospective European study. Eur. Heart J. in press (2017).
[262] R Core Team. R: A Language and Environment for Statistical Computing (2016). URL https://www.r-project.org/.[263] Liu, L. C. Y., Voors, A. A., Valente, M. A. E. & van der Meer, P. A novel approach to drug development in heart
failure: towards personalized medicine. Can. J. Cardiol. 30, 288–95 (2014).[264] Schuetz, P., Aujesky, D., Müller, C. & Müller, B. Biomarker-guided personalised emergency medicine for all - hope for
another hype? Swiss Med. Wkly. 145, w14079 (2015).[265] Demissei, B. G. et al. Risk-based evaluation of efficacy of rolofylline in patients hospitalized with acute heart failure -
Post-hoc analysis of the PROTECT trial. Int. J. Cardiol. 223, 967–975 (2016).[266] Horwich, T. B., Fonarow, G. C., Hamilton, M. A., MacLellan, W. R. & Borenstein, J. Anemia is associated with worse
symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advancedheart failure. J. Am. Coll. Cardiol. 39, 1780–6 (2002).
[267] Toth, P. P. High-density lipoprotein and cardiovascular risk. Circulation 109, 1809–12 (2004).[268] Cauthen, C. a. et al. Relation of blood urea nitrogen to long-term mortality in patients with heart failure. Am. J.
Cardiol. 101, 1643–7 (2008).[269] Schrier, R. W. Blood urea nitrogen and serum creatinine: not married in heart failure. Circ. Heart Fail. 1, 2–5 (2008).[270] Iqbal, N. et al. Cardiac biomarkers: new tools for heart failure management. Cardiovasc. Diagn. Ther. 2, 147–64
(2012).[271] de Boer, R. A. et al. The WAP four-disulfide core domain protein HE4: a novel biomarker for heart failure. JACC.
Heart Fail. 1, 164–9 (2013).[272] Shah, K. S. & Maisel, A. S. Novel biomarkers in heart failure with preserved ejection fraction. Heart Fail. Clin. 10,
471–9 (2014).[273] van Deursen, V. M. et al. Prognostic value of plasma neutrophil gelatinase-associated lipocalin for mortality in patients
with heart failure. Circ. Heart Fail. 7, 35–42 (2014).[274] van Veldhuisen, D. J. et al. High- versus low-dose ACE inhibition in chronic heart failure: a double-blind, placebo-
controlled study of imidapril. J. Am. Coll. Cardiol. 32, 1811–8 (1998).[275] Shah, S. J., Katz, D. H. & Deo, R. C. Phenotypic spectrum of heart failure with preserved ejection fraction. Heart
Fail. Clin. 10, 407–18 (2014).[276] Rienstra, M. et al. Cluster Individuals Based on Phenotype and Determine the Risk for Atrial Fibrillation in the
PREVEND and Framingham Heart Study Populations. PLoS One 11, e0165828 (2016).[277] Wolfe, J. H. Pattern clustering by multivariate mixture analysis. Multivariate Behav. Res. 5, 329–50 (1970).[278] Scott, A. J. & Symons, M. J. Clustering Methods Based on Likelihood Ratio Criteria. Biometrics 27, 387 (1971).[279] Banfield, J. D. & Raftery, A. E. Model-Based Gaussian and Non-Gaussian Clustering. Biometrics 49, 803 (1993).[280] Fraley, C. & Raftery, a. E. How Many Clusters? Which Clustering Method? Answers Via Model-Based Cluster
Analysis. Comput. J. 41, 578–588 (1998).[281] McLachlan, G. & Peel, D. Finite Mixture Models. Wiley Series in Probability and Statistics (John Wiley and Sons,
Inc., Hoboken, NJ, USA, 2000).[282] Fraley, C. & Raftery, A. E. Model-Based Clustering, Discriminant Analysis, and Density Estimation. J. Am. Stat.
Assoc. 97, 611–631 (2002).[283] Raftery, A. E. & Dean, N. Variable Selection for Model-Based Clustering. J. Am. Stat. Assoc. 101, 168–178 (2006).[284] Lazarsfeld, P. & Henry, N. Latent structure analysis (Houghton Mifflin, Boston, 1968).[285] Rindskopf, D. Joint Statistical Meetings - Social Statistics Section (1986).[286] Cassidy, F., Pieper, C. F. & Carroll, B. J. Subtypes of mania determined by grade of membership analysis. Neuropsy-
chopharmacology 25, 373–83 (2001).[287] Kim, J. et al. Prognostic value of a novel classification scheme for heart failure: the Minnesota Heart Failure Criteria.
Am. J. Epidemiol. 164, 184–93 (2006).

215
[288] Starkstein, S. et al. Diagnostic criteria for depression in Parkinson’s disease: a study of symptom patterns using latentclass analysis. Mov. Disord. 26, 2239–45 (2011).
[289] Crow, S. J. et al. Latent class analysis of eating disorders: relationship to mortality. J. Abnorm. Psychol. 121, 225–31(2012).
[290] Grayson, P. C. et al. Distribution of arterial lesions in Takayasu’s arteritis and giant cell arteritis. Ann. Rheum. Dis.71, 1329–34 (2012).
[291] Jaeger, S. et al. Adherence styles of schizophrenia patients identified by a latent class analysis of the MedicationAdherence Rating Scale (MARS): a six-month follow-up study. Psychiatry Res. 200, 83–8 (2012).
[292] Kao, D. P., Wagner, B. D., Robertson, A. D., Bristow, M. R. & Lowes, B. D. A personalized BEST: characterizationof latent clinical classes of nonischemic heart failure that predict outcomes and response to bucindolol. PLoS One 7,e48184 (2012).
[293] Ogden, L. G. et al. Cluster analysis of the national weight control registry to identify distinct subgroups maintainingsuccessful weight loss. Obesity (Silver Spring). 20, 2039–47 (2012).
[294] Shiboski, S. C. et al. American College of Rheumatology classification criteria for Sjögren’s syndrome: a data-driven,expert consensus approach in the Sjögren’s International Collaborative Clinical Alliance cohort. Arthritis Care Res.(Hoboken). 64, 475–87 (2012).
[295] Lanza, S. T. & Rhoades, B. L. Latent class analysis: an alternative perspective on subgroup analysis in preventionand treatment. Prev. Sci. 14, 157–68 (2013).
[296] Murtagh, F. & Legendre, P. Ward’s Hierarchical Agglomerative Clustering Method: Which Algorithms ImplementWard’s Criterion? J. Classif. 31, 274–295 (2014).
[297] Everitt, B. S., Landau, S., Leese, M. & Stahl, D. Hierarchical Clustering. Wiley Series in Probability and Statistics,71–110 (John Wiley and Sons, Ltd, Chichester, UK, 2011).
[298] Chen, Y. T., Wang, Y., Radford, M. J. & Krumholz, H. M. Angiotensin-converting enzyme inhibitor dosages in elderlypatients with heart failure. Am. Heart J. 141, 410–7 (2001).
[299] Nodari, S., Metra, M. & Dei Cas, L. Beta-blocker treatment of patients with diastolic heart failure and arterialhypertension. A prospective, randomized, comparison of the long-term effects of atenolol vs. nebivolol. Eur. J. HeartFail. 5, 621–7 (2003).
[300] Gustafsson, F. et al. Treatment with beta-blockers in nurse-led heart failure clinics: titration efficacy and predictorsof failure. Eur. J. Heart Fail. 9, 910–6 (2007).
[301] Fiuzat, M. et al. Heart Rate or Beta-Blocker Dose? Association With Outcomes in Ambulatory Heart Failure PatientsWith Systolic Dysfunction: Results From the HF-ACTION Trial. JACC. Heart Fail. 4, 109–15 (2016).
[302] Basagaña, X., Barrera-Gómez, J., Benet, M., Antó, J. M. & Garcia-Aymerich, J. A framework for multiple imputationin cluster analysis. Am. J. Epidemiol. 177, 718–25 (2013).
[303] Fraley, C., Raftery, A. E., Murphy, T. B. & Scrucca, L. mclust Version 4 for R: Normal Mixture Modeling forModel-Based Clustering, Classification, and Density Estimation. Tech. Rep., University of Washington,Department ofStatistics, Washington (2012).
[304] Linzer, D. A. & Lewis, J. B. poLCA : An R Package for Polytomous Variable Latent Class Analysis. J. Stat. Softw.42, 1–29 (2011).
[305] Reynolds, A. P., Richards, G., de la Iglesia, B. & Rayward-Smith, V. J. Clustering Rules: A Comparison of Partitioningand Hierarchical Clustering Algorithms. J. Math. Model. Algorithms 5, 475–504 (2006).
[306] Maechler, M., Rousseeu, P., Struyf, A., Hubert, M. & Hornik, K. cluster: Cluster Analysis Basics and Extensions(2016).
[307] Wit, E., van den Heuvel, E. & Romeijn, J.-W. ‘All models are wrong...’: an introduction to model uncertainty. Stat.Neerl. 66, 217–236 (2012).
[308] Rousseeuw, P. J. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. J. Comput. Appl.Math. 20, 53–65 (1987).
[309] Cohen, J. A Coefficient of Agreement for Nominal Scales. Educ. Psychol. Meas. 20, 37–46 (1960).[310] Kent, P., Stochkendahl, M. J., Christensen, H. W. & Kongsted, A. Could the clinical interpretability of subgroups
detected using clustering methods be improved by using a novel two-stage approach? Chiropr. Man. Therap. 23, 20(2015).
[311] Wittkop, T. et al. Partitioning biological data with transitivity clustering. Nat. Methods 7, 419–20 (2010).[312] Wiwie, C., Baumbach, J. & Röttger, R. Comparing the performance of biomedical clustering methods. Nat. Methods
12, 1033–8 (2015).[313] Petricoin, E. F. et al. Use of proteomic patterns in serum to identify ovarian cancer. Lancet (London, England) 359,
572–7 (2002).[314] Yancy, C. W. et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report
of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines.Circulation 128, 1810–52 (2013).
[315] Calinski, T. & Harabasz, J. A dendrite method for cluster analysis. Commun. Stat. - Theory Methods 3, 1–27 (1974).[316] Kaufman, L. & Rousseeuw, P. J. Finding groups in data: An introduction to cluster analysis (Wiley, 1990).[317] Duda, R. O., Hart, P. E. & Stork, D. G. No Title (Wiley, 2001), 2 edn.[318] Hennig, C. & Liao, T. F. How to find an appropriate clustering for mixed-type variables with application to socio-
economic stratification. J. R. Stat. Soc. Ser. C (Applied Stat. 62, 309–369 (2013).[319] Leisch, F. A toolbox for -centroids cluster analysis. Comput. Stat. Data Anal. 51, 526–544 (2006).[320] Leisch, F. & Gr, B. Extending Standard Cluster Algorithms to Allow for Group Constraints ∗. Physica 885–892 (2006).[321] Ahmad, T. et al. Clinical implications of chronic heart failure phenotypes defined by cluster analysis. J. Am. Coll.
Cardiol. 64, 1765–74 (2014).[322] Go, A. S. et al. Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with
chronic heart failure: the Anemia in Chronic Heart Failure: Outcomes and Resource Utilization (ANCHOR) Study.Circulation 113, 2713–23 (2006).

216 References
[323] Korolenko, T. A., Pisareva, E. E., Filyushina, E. E., Johnston, T. P. & Machova, E. Serum cystatin C and chitotriosi-dase in acute P-407 induced dyslipidemia: Can they serve as potential early biomarkers for atherosclerosis? Exp.Toxicol. Pathol. 67, 459–66 (2015).
[324] Kotecha, D. et al. Efficacy of β blockers in patients with heart failure plus atrial fibrillation: an individual-patientdata meta-analysis. Lancet (London, England) 384, 2235–43 (2014).
[325] Wang, G.-S. & Cooper, T. a. Splicing in disease: disruption of the splicing code and the decoding machinery. Nat.Rev. Genet. 8, 749–61 (2007).
[326] Sammeth, M., Foissac, S. & Guigó, R. A general definition and nomenclature for alternative splicing events. PLoSComput. Biol. 4, e1000147 (2008).
[327] Wang, H. et al. Gene structure-based splice variant deconvolution using a microarray platform. Bioinformatics 19Suppl 1, i315–22 (2003).
[328] Pan, Q. et al. Revealing global regulatory features of mammalian alternative splicing using a quantitative microarrayplatform. Mol. Cell 16, 929–41 (2004).
[329] Heber, S., Alekseyev, M., Sze, S.-H., Tang, H. & Pevzner, P. a. Splicing graphs and EST assembly problem. Bioinfor-matics 18 Suppl 1, S181–8 (2002).
[330] Xing, Y., Resch, A. & Lee, C. The multiassembly problem: reconstructing multiple transcript isoforms from ESTfragment mixtures. Genome Res. 14, 426–41 (2004).
[331] Malde, K., Coward, E. & Jonassen, I. A graph based algorithm for generating EST consensus sequences. Bioinformatics21, 1371–5 (2005).
[332] Leipzig, J., Pevzner, P. & Heber, S. The Alternative Splicing Gallery (ASG): bridging the gap between genome andtranscriptome. Nucleic Acids Res. 32, 3977–83 (2004).
[333] Florea, L. et al. Gene and alternative splicing annotation with AIR. Genome Res. 15, 54–66 (2005).[334] Kim, P. et al. ECgene: genome annotation for alternative splicing. Nucleic Acids Res. 33, D75–9 (2005).[335] Nelder, J. & Mead, R. A simplex method for function minimization. Comput. J. 7, 308–131 (1964).[336] Kersey, P. J. et al. Ensembl Genomes: an integrative resource for genome-scale data from non-vertebrate species.
Nucleic Acids Res. 40, D91–7 (2012).[337] Bruning, O. et al. RNA isolation for transcriptomics of human and mouse small skin biopsies. BMC Res. Notes 4, 438
(2011).[338] Loeys, B. L. et al. The revised Ghent nosology for the Marfan syndrome. J. Med. Genet. 47, 476–85 (2010).[339] Radonic, T. et al. Critical appraisal of the revised Ghent criteria for diagnosis of Marfan syndrome. Clin. Genet. 80,
346–53 (2011).[340] Patel, H. J. & Deeb, G. M. Ascending and arch aorta: pathology, natural history, and treatment. Circulation 118,
188–95 (2008).[341] Van Hemelrijk, C., Renard, M. & Loeys, B. The Loeys-Dietz syndrome: an update for the clinician. Curr. Opin.
Cardiol. 25, 546–51 (2010).[342] Coucke, P. J. et al. Mutations in the facilitative glucose transporter GLUT10 alter angiogenesis and cause arterial
tortuosity syndrome. Nat. Genet. 38, 452–7 (2006).[343] Hoffjan, S. Genetic dissection of marfan syndrome and related connective tissue disorders: an update 2012. Mol.
Syndromol. 3, 47–58 (2012).[344] Swertz, M. A. et al. The MOLGENIS toolkit: rapid prototyping of biosoftware at the push of a button. BMC
Bioinformatics 11 Suppl 1, S12 (2010).[345] Sudlow, C. et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases
of middle and old age. PLoS Med. 12, e1001779 (2015).[346] Witten, D. M., Tibshirani, R. & Hastie, T. A penalized matrix decomposition, with applications to sparse principal
components and canonical correlation analysis. Biostatistics 10, 515–34 (2009).[347] Wold, H. Path models with latent variables: The NIPALS approach. In Blalock, H. M., Aganbegian, A., Borodkin,
F. M., Boudon, R. & Capecchi, V. (eds.) Quant. Sociol. Int. Perspect. Math. Stat. Model., 307–357 (New York: SeminarPress, 1975).
[348] Lê Cao, K.-A., Martin, P. G. P., Robert-Granié, C. & Besse, P. Sparse canonical methods for biological data integration:application to a cross-platform study. BMC Bioinformatics 10, 34 (2009).
[349] Wegelin, J. A. A Survey of Partial Least Squares (PLS) Methods, with Emphasis on the Two-Block Case. Tech. Rep.,University of Washington, Department of Statistics, Seattle (2000).
[350] Waaijenborg, S. & Zwinderman, A. H. Penalized canonical correlation analysis to quantify the association betweengene expression and DNA markers. BMC Proc. 1 Suppl 1, S122 (2007).
[351] Zou, H. & Hastie, T. Regularization and variable selection via the elastic net. J. R. Stat. Soc. Ser. B (StatisticalMethodol. 67, 301–320 (2005).
[352] Friedman, J., Hastie, T., Höfling, H. & Tibshirani, R. Pathwise coordinate optimization. Ann. Appl. Stat. 1, 302–332(2007).
[353] Cattell, R. B. The Scree Test For The Number Of Factors. Multivariate Behav. Res. 1, 245–76 (1966).[354] Gene Ontology Consortium. Gene Ontology Consortium: going forward. Nucleic Acids Res. 43, D1049–56 (2015).[355] Kanehisa, M. & Goto, S. KEGG: kyoto encyclopedia of genes and genomes. Nucleic Acids Res. 28, 27–30 (2000).[356] Kanehisa, M., Sato, Y., Kawashima, M., Furumichi, M. & Tanabe, M. KEGG as a reference resource for gene and
protein annotation. Nucleic Acids Res. 44, D457–62 (2016).[357] Subramanian, A. et al. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide
expression profiles. Proc. Natl. Acad. Sci. U. S. A. 102, 15545–50 (2005).[358] Hoerl, A. Application of ridge analysis to regression problems. Chem. Eng. Prog. 58, 54–59 (1962).[359] Tibshirani, R. Regression Shrinkage and Selection Via the Lasso. J. R. Stat. Soc. Ser. B 58, 267–288 (1994).[360] Radonic, T. et al. Losartan therapy in adults with Marfan syndrome: study protocol of the multi-center randomized
controlled COMPARE trial. Trials 11, 3 (2010).

217
[361] De Paepe, A., Devereux, R. B., Dietz, H. C., Hennekam, R. C. & Pyeritz, R. E. Revised diagnostic criteria for theMarfan syndrome. Am. J. Med. Genet. 62, 417–26 (1996).
[362] Guthridge, M. A. et al. Mechanism of activation of the GM-CSF, IL-3, and IL-5 family of receptors. Stem Cells 16,301–13 (1998).
[363] Tian, R. & Ingwall, J. S. How does folic acid cure heart attacks? Circulation 117, 1772–4 (2008).[364] Bazzano, L. A. Folic Acid Supplementation and Cardiovascular Disease: The State of the Art. Am. J. Med. Sci. 338,
48–49 (2009).[365] Blom, H. J. & Smulders, Y. Overview of homocysteine and folate metabolism. With special references to cardiovascular
disease and neural tube defects. J. Inherit. Metab. Dis. 34, 75–81 (2011).[366] Li, Y. et al. Folic Acid Supplementation and the Risk of Cardiovascular Diseases: A Meta‐Analysis of Randomized
Controlled Trials. J. Am. Heart Assoc. 5, e003768 (2016).[367] Tao, G. et al. Collagen XIV is important for growth and structural integrity of the myocardium. J. Mol. Cell. Cardiol.
53, 626–38 (2012).[368] Gil-Cayuela, C. et al. RNA sequencing analysis identifies new human collagen genes involved in cardiac remodeling. J.
Am. Coll. Cardiol. 65, 1265–7 (2015).[369] Tomita, Y., Kim, D. H., Magoori, K., Fujino, T. & Yamamoto, T. T. A novel low-density lipoprotein receptor-related
protein with type II membrane protein-like structure is abundant in heart. J. Biochem. 124, 784–9 (1998).[370] Ohkawara, B. et al. LRP4 third β-propeller domain mutations cause novel congenital myasthenia by compromising
agrin-mediated MuSK signaling in a position-specific manner. Hum. Mol. Genet. 23, 1856–68 (2014).[371] Shivamurthy, P. & Parker, M. W. Cardiac manifestations of myasthenia gravis: A systematic review. IJC Metab.
Endocr. 5, 3–6 (2014).[372] Filmore, D. It’s a GPCR world. Mod. Drug Discov. 7, 24–28 (2004).[373] Overington, J. P., Al-Lazikani, B. & Hopkins, A. L. How many drug targets are there? Nat. Rev. Drug Discov. 5,
993–6 (2006).[374] Mogi, M., Iwai, M. & Horiuchi, M. Emerging concepts of regulation of angiotensin II receptors: new players and
targets for traditional receptors. Arterioscler. Thromb. Vasc. Biol. 27, 2532–9 (2007).[375] Belmonte, S. L. & Blaxall, B. C. Conducting the G-protein Coupled Receptor (GPCR) Signaling Symphony in
Cardiovascular Diseases: New Therapeutic Approaches. Drug Discov. Today. Dis. Models 9, e85–e90 (2012).[376] Horiuchi, M., Iwanami, J. & Mogi, M. Regulation of angiotensin II receptors beyond the classical pathway. Clin. Sci.
(Lond). 123, 193–203 (2012).[377] Singh, K. D. & Karnik, S. S. Angiotensin Receptors: Structure, Function, Signaling and Clinical Applications. J. cell
Signal. 1, 1–8 (2016).[378] Peacock, W. F. et al. Cardiac troponin and outcome in acute heart failure. N. Engl. J. Med. 358, 2117–26 (2008).[379] Januzzi, J. L., Filippatos, G., Nieminen, M. & Gheorghiade, M. Troponin elevation in patients with heart failure: on
behalf of the third Universal Definition of Myocardial Infarction Global Task Force: Heart Failure Section. Eur. HeartJ. 33, 2265–71 (2012).
[380] Grodin, J. L. & Tang, W. H. W. Treatment strategies for the prevention of heart failure. Curr. Heart Fail. Rep. 10,331–40 (2013).
[381] Guha, K. & McDonagh, T. Heart failure epidemiology: European perspective. Curr. Cardiol. Rev. 9, 123–7 (2013).[382] Ponikowski, P. et al. Heart failure: preventing disease and death worldwide. ESC Hear. Fail. 1, 4–25 (2014).[383] Haider, A. W., Larson, M. G., Franklin, S. S., Levy, D. & Framingham Heart Study. Systolic blood pressure, diastolic
blood pressure, and pulse pressure as predictors of risk for congestive heart failure in the Framingham Heart Study.Ann. Intern. Med. 138, 10–6 (2003).
[384] Kooij, J. A. V. D. Prediction Accuracy and Stability of Regression with Optimal Scaling Transformations. Dissertations,Leiden University (2007).
[385] Young, F. W., de Leeuw, J. & Takane, Y. Regression with qualitative and quantitative variables: An alternating leastsquares method with optimal scaling features. Psychometrika 41, 505–529 (1976).
[386] Burg, E. & Leeuw, J. Non-linear canonical correlation†. Br. J. Math. Stat. Psychol. 36, 54–80 (1983).[387] Waaijenborg, S. & Zwinderman, A. H. Correlating multiple SNPs and multiple disease phenotypes: penalized non-linear
canonical correlation analysis. Bioinformatics 25, 2764–71 (2009).[388] Gamazon, E. R. et al. A gene-based association method for mapping traits using reference transcriptome data. Nat.
Genet. 47, 1091–8 (2015).[389] Waaijenborg, S. Penalized canonical correlation analysis: unraveling the genetic background of complex diseases.
Dissertation, University of Amsterdam (2010).[390] Aaronson, K. D. et al. Development and prospective validation of a clinical index to predict survival in ambulatory
patients referred for cardiac transplant evaluation. Circulation 95, 2660–7 (1997).[391] Chin, M. H. & Goldman, L. Correlates of early hospital readmission or death in patients with congestive heart failure.
Am. J. Cardiol. 79, 1640–4 (1997).[392] Philbin, E. F. & DiSalvo, T. G. Prediction of hospital readmission for heart failure: development of a simple risk score
based on administrative data. J. Am. Coll. Cardiol. 33, 1560–6 (1999).[393] Alla, F. et al. Differential clinical prognostic classifications in dilated and ischemic advanced heart failure: the EPICAL
study. Am. Heart J. 139, 895–904 (2000).[394] Krumholz, H. M. et al. Predictors of readmission among elderly survivors of admission with heart failure. Am. Heart
J. 139, 72–7 (2000).[395] Rosenthal, G. E. et al. Relationships between in-hospital and 30-day standardized hospital mortality: implications for
profiling hospitals. Health Serv. Res. 34, 1449–68 (2000).[396] Bouvy, M. L., Heerdink, E. R., Leufkens, H. G. M. & Hoes, a. W. Predicting mortality in patients with heart failure:
a pragmatic approach. Heart 89, 605–9 (2003).[397] Kearney, M. T. et al. A prognostic index to predict long-term mortality in patients with mild to moderate chronic
heart failure stabilised on angiotensin converting enzyme inhibitors. Eur. J. Heart Fail. 5, 489–97 (2003).

218 References
[398] Lee, D. S. et al. Predicting mortality among patients hospitalized for heart failure: derivation and validation of aclinical model. JAMA 290, 2581–7 (2003).
[399] Brophy, J. M., Dagenais, G. R., McSherry, F., Williford, W. & Yusuf, S. A multivariate model for predicting mortalityin patients with heart failure and systolic dysfunction. Am. J. Med. 116, 300–4 (2004).
[400] Felker, G. M. et al. Risk stratification after hospitalization for decompensated heart failure. J. Card. Fail. 10, 460–6(2004).
[401] Adlam, D., Silcocks, P. & Sparrow, N. Using BNP to develop a risk score for heart failure in primary care. Eur. HeartJ. 26, 1086–93 (2005).
[402] Auble, T. E. et al. A prediction rule to identify low-risk patients with heart failure. Acad. Emerg. Med. 12, 514–21(2005).
[403] Fonarow, G. C. et al. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classificationand regression tree analysis. JAMA 293, 572–80 (2005).
[404] Heywood, J. T., Elatre, W., Pai, R. G., Fabbri, S. & Huiskes, B. Simple clinical criteria to determine the prognosis ofheart failure. J. Cardiovasc. Pharmacol. Ther. 10, 173–80 (2005).
[405] O’Connor, C. M., Stough, W. G., Gallup, D. S., Hasselblad, V. & Gheorghiade, M. Demographics, clinical charac-teristics, and outcomes of patients hospitalized for decompensated heart failure: observations from the IMPACT-HFregistry. J. Card. Fail. 11, 200–5 (2005).
[406] Pocock, S. J. et al. Predictors of mortality and morbidity in patients with chronic heart failure. Eur. Heart J. 27,65–75 (2006).
[407] Abraham, W. T. et al. Predictors of in-hospital mortality in patients hospitalized for heart failure: insights from theOrganized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). J.Am. Coll. Cardiol. 52, 347–56 (2008).
[408] Keenan, P. S. et al. An administrative claims measure suitable for profiling hospital performance on the basis of 30-dayall-cause readmission rates among patients with heart failure. Circ. Cardiovasc. Qual. Outcomes 1, 29–37 (2008).
[409] O’Connor, C. M. et al. Efficacy and safety of exercise training in patients with chronic heart failure: HF-ACTIONrandomized controlled trial. JAMA 301, 1439–50 (2009).
[410] Levy, W. C. et al. Maximizing survival benefit with primary prevention implantable cardioverter-defibrillator therapyin a heart failure population. Circulation 120, 835–42 (2009).
[411] Vazquez, R. et al. The MUSIC Risk score: a simple method for predicting mortality in ambulatory patients withchronic heart failure. Eur. Heart J. 30, 1088–96 (2009).
[412] Amarasingham, R. et al. An automated model to identify heart failure patients at risk for 30-day readmission or deathusing electronic medical record data. Med. Care 48, 981–8 (2010).
[413] Lee, D. S. et al. Early deaths in patients with heart failure discharged from the emergency department: a population-based analysis. Circ. Heart Fail. 3, 228–35 (2010).
[414] O’Connor, C. M. et al. Triage after hospitalization with advanced heart failure: the ESCAPE (Evaluation Study ofCongestive Heart Failure and Pulmonary Artery Catheterization Effectiveness) risk model and discharge score. J. Am.Coll. Cardiol. 55, 872–8 (2010).
[415] van Walraven, C. et al. Derivation and validation of an index to predict early death or unplanned readmission afterdischarge from hospital to the community. CMAJ 182, 551–7 (2010).
[416] Allen, L. a. et al. Identifying patients hospitalized with heart failure at risk for unfavorable future quality of life. Circ.Cardiovasc. Qual. Outcomes 4, 389–98 (2011).
[417] Axente, L., Sinescu, C. & Bazacliu, G. Heart failure prognostic model. J. Med. Life 4, 210–25 (2011).[418] Manzano, L. et al. Predictors of clinical outcomes in elderly patients with heart failure. Eur. J. Heart Fail. 13, 528–36
(2011).[419] Senni, M. et al. Predicting heart failure outcome from cardiac and comorbid conditions: the 3C-HF score. Int. J.
Cardiol. 163, 206–11 (2013).[420] Smith, D. H. et al. Predicting poor outcomes in heart failure. Perm. J. 15, 4–11 (2011).[421] Subramanian, D., Subramanian, V., Deswal, A. & Mann, D. L. New predictive models of heart failure mortality using
time-series measurements and ensemble models. Circ. Heart Fail. 4, 456–62 (2011).[422] Van Spall, H. G. C. et al. Prediction of emergent heart failure death by semi-quantitative triage risk stratification.
PLoS One 6, e23065 (2011).[423] Au, A. G. et al. Predicting the risk of unplanned readmission or death within 30 days of discharge after a heart failure
hospitalization. Am. Heart J. 164, 365–72 (2012).[424] Barlera, S. et al. Predictors of mortality in 6975 patients with chronic heart failure in the Gruppo Italiano per lo
Studio della Streptochinasi nell’Infarto Miocardico-Heart Failure trial: proposal for a nomogram. Circ. Heart Fail. 6,31–9 (2013).
[425] Bayes-Genis, A. et al. Combined use of high-sensitivity ST2 and NTproBNP to improve the prediction of death inheart failure. Eur. J. Heart Fail. 14, 32–8 (2012).
[426] de la Cámara, A. G. et al. Role of biological and non biological factors in congestive heart failure mortality: PREDICE-SCORE: a clinical prediction rule. Cardiol. J. 19, 578–85 (2012).
[427] Lee, D. S. et al. Prediction of heart failure mortality in emergent care: a cohort study. Ann. Intern. Med. 156, 767–75,W–261, W–262 (2012).
[428] O’Connor, C. M. et al. Factors related to morbidity and mortality in patients with chronic heart failure with systolicdysfunction: the HF-ACTION predictive risk score model. Circ. Heart Fail. 5, 63–71 (2012).
[429] Oh, C. et al. Prognostic Estimation of Advanced Heart Failure With Low Left Ventricular Ejection Fraction and WideQRS Interval. Korean Circ. J. 42, 659–67 (2012).
[430] Perrotta, L. et al. Application of the Seattle Heart Failure Model in patients on cardiac resynchronization therapy.Pacing Clin. Electrophysiol. 35, 88–94 (2012).
[431] Postmus, D. et al. The COACH risk engine: a multistate model for predicting survival and hospitalization in patientswith heart failure. Eur. J. Heart Fail. 14, 168–75 (2012).

219
[432] Regoli, F. et al. Validation of Seattle Heart Failure Model for mortality risk prediction in patients treated with cardiacresynchronization therapy. Eur. J. Heart Fail. 15, 211–20 (2013).
[433] Richter, B. et al. A multi-biomarker risk score improves prediction of long-term mortality in patients with advancedheart failure. Int. J. Cardiol. 168, 1251–7 (2013).


SUPPLEMENTARY DATA


223
Table S1: The 10 variables with the highest predicted values (highest z-score), used in morethan 5 chronic heart failure models
# z-score Mean 95% CI
10 highest odds ratiosBlood urea nitrogen 24 61.50 2.37 2.34-2.39Systolic blood pressure 45 54.72 1.16 1.15-1.16Cancer 9 38.00 1.84 1.81-1.88Troponin 8 34.59 1.73 1.69-1.76Creatinine 36 34.19 1.12 1.11-1.13Sodium 44 33.50 1.41 1.39-1.43Heart Failure 9 27.92 1.28 1.26-1.30Arterial pH 6 27.75 1.87 1.83-1.92Diastolic blood pressure 11 22.01 1.15 1.14-1.16Renal failure 8 21.11 1.26 1.24-1.28
10 highest hazard ratiosSodium 44 36.53 1.07 1.06-1.07Race 10 27.03 1.11 1.10-1.12Diabetes mellitus 41 21.23 1.44 1.41-1.47Age 73 20.65 1.06 1.06-1.07Systolic blood pressure 45 18.65 1.18 1.16-1.19New York Heart Association class 34 17.51 1.41 1.37-1.44N-terminal pro B-type natriuretic peptide 15 15.24 1.47 1.42-1.52Angiotensin-converting-enzyme inhibitor/Angiotensin II receptor blocker 8 14.01 1.19 1.17-1.21Ejection fraction 23 12.84 1.08 1.07-1.10Blood urea nitrogen 24 12.01 1.07 1.06-1.08#: Number of times used; CI: confidence interval
Table S2: The 10 variables with the highest predicted values (highest z-score), used in acutedecompensated heart failure models
# z-score Mean 95% CI
10 highest odds ratiosHeart Failure admissions 2 12.44 1.44 1.39-1.50Age 4 8.45 1.46 1.37-1.55Dementia/Alzheimers disease or senility 1 6.31 2.42 2.15-2.70Systolic blood pressure 6 2.18 1.22 1.04-1.41Mode of arrival 1 2.13 5.07 3.57-6.57Metastatic cancer 1 1.92 4.60 3.04-6.16Depression or anxiety 1 1.85 1.72 1.15-2.30Hepatic cirrhosis 1 1.09 3.22 1.11-5.33Nitrates 1 1.08 2.00 0.74-3.26Cancer 1 0.83 1.86 0.39-3.33
10 highest hazard ratiosSodium 2 1.66 1.33 0.99-1.67New York Heart Association class 1 0.85 1.94 0.41-3.47Heart Failure admissions 2 0.74 2.00Gender 1 0.44 1.33Systolic blood pressure 6 0.38 1.28 -0.01-2.57Blood urea nitrogen 4 0.34 1.33 -0.32-2.98Age 4 0.25 1.27 -0.57-3.11N-terminal pro B-type natriuretic peptide 1 0.09 1.08Estimated glomerular filtration rate 1 0.06 1.01Systolic blood pressure 1 0.06 1.01#: Number of times used; CI: confidence interval

224 Supplementary data
Table S3: The 10 variables with the highest predicted values (highest z-score), used in mortalityprediction models
# z-score Mean 95% CI
10 highest odds ratiosBlood urea nitrogen 24 65.19 3.02 2.99-3.05Systolic blood pressure 45 42.75 1.17 1.16-1.17Cancer 9 38.00 1.84 1.81-1.88Troponin 8 34.59 1.73 1.69-1.76Sodium 44 34.41 1.44 1.42-1.46Creatinine 36 32.69 1.12 1.11-1.12Cardiac arrest or mechanical ventilation 5 32.61 13.26 13.1-13.41Arterial pH 6 27.75 1.87 1.83-1.92Prothrombin time/international normalized ratio 4 27.03 1.40 1.38-1.42Arterial pCo2 5 25.39 1.42 1.40-1.45
10 highest hazard ratiosSodium 44 30.34 1.09 1.08-1.09Age 73 17.93 1.06 1.05-1.06New York Heart Association class 34 16.83 1.40 1.36-1.44N-terminal pro B-type natriuretic peptide 15 15.24 1.47 1.42-1.52Diabetes mellitus 41 14.58 1.38 1.33-1.42Angiotensin-converting-enzyme inhibitor/angiotensin II receptor blocker 8 14.01 1.19 1.17-1.21Serum creatinine 36 10.20 1.06 1.05-1.08Body mass index 21 10.19 1.08 1.07-1.10Systolic blood pressure 45 9.91 1.11 1.09-1.13Ejection fraction 23 8.97 1.04 1.03-1.05#: Number of times used; CI: confidence interval
Table S4: The 10 variables with the highest prediction values (highest z-score), used in mortalityand/or heart failure related hospitalization prediction models
# z-score Mean 95% CI
10 highest odds ratiosHeart Failure admissions 3 12.47 1.40 1.35-1.45Depression or anxiety 1 8.82 1.12 1.10-1.15Acuity of Admission 1 6.56 1.47 1.35-1.59Nitrates 1 6.42 1.48 1.36-1.60Creatinine 2 6.10 1.25 1.18-1.32Length of stay 1 5.94 1.56 1.41-1.71Cancer 1 5.75 1.19 1.13-1.24Emergency department visits 1 5.59 1.21 1.14-1.28Blood urea nitrogen 4 5.24 1.33 1.22-1.44Drug/Alcohol 2 4.96 1.07 1.04-1.10
10 highest hazard ratiosRace 1 27.03 1.11 1.10-1.12Age 4 23.73 1.51 1.48-1.54Estimated glomerular filtration rate 1 21.41 2.34 2.26-2.42Systolic blood pressure 6 17.75 1.23 1.20-1.25Diabetes mellitus 1 17.51 1.52 1.47-1.57Anemia 1 15.93 1.69 1.62-1.75Blood pressure treatment 1 15.91 1.20 1.18-1.23N-terminal pro B-type natriuretic peptide 1 14.46 1.62 1.55-1.68Ejection fraction 1 10.65 1.13 1.10-1.15Gender 1 10.28 1.20 1.17-1.24#: Number of times used; CI: confidence interval

225
Table S5: The 10 variables with the highest prediction values (highest z-score), used in heartfailure related hospitalization prediction models
# z-score Mean 95% CI
10 highest odds ratiosBlood urea nitrogen 24 60.70 2.28 2.26-2.31Cancer 9 38.00 1.84 1.81-1.88Troponin 8 34.59 1.73 1.69-1.76Creatinine 36 34.19 1.12 1.11-1.13Sodium 44 33.50 1.41 1.39-1.43Systolic blood pressure 45 31.80 1.30 1.29-1.32Heart Failure 9 27.92 1.28 1.26-1.30Cardiac arrest or mechanical ventilation 5 27.91 6.54 6.41-6.67Arterial pH 6 27.75 1.87 1.83-1.92Prothrombin time/international normalized ratio 4 27.03 1.40 1.38-1.42
10 highest hazard ratiosSodium 44 30.34 1.09 1.08-1.09Race 10 27.03 1.11 1.10-1.12Diabetes mellitus 41 21.23 1.44 1.41-1.47Age 73 20.73 1.06 1.06-1.07Systolic blood pressure 45 19.35 1.16 1.15-1.18New York Heart Association class 34 17.68 1.41 1.37-1.45Anemia 5 15.93 1.69 1.62-1.75Blood pressure treatment 4 15.91 1.20 1.18-1.23N-terminal pro B-type natriuretic peptide 15 15.32 1.44 1.39-1.49angiotensin-converting-enzyme inhibitor/angiotensin II receptor blocker 15 14.01 1.19 1.17-1.21#: Number of times used; CI: confidence interval

226 Supplementary data
Table S6: Papers and models selected for meta-analysis
Paper N Pop SM Pt Du P # E C DS V Type Age ♂Selker et al.197 1 CHF RR 5773 2 D 4 M 0.9 MR P COH 74 50Aaronson 2 CHF RR 268 365 D 7 M 0.74 MR P COH 50 80et al.390 2 CHF RR 199 365 V 7 M 0.69 MR P COH 52 81
3 CHF RR 231 365 D 8 M 0.74 MR P COH 50 803 CHF RR 199 365 V 8 M 0.66 MR P COH 52 81
Chin and 4 CHF RR 257 60 D 6 M MR P COH 67 49Goldman391 4 CHF RR 257 60 D 6 MH MR P COH 67 49Philbin et al.392 5 CHF RR 52010 365 D 16 H 0.62 CD R REG 74 44
6 CHF AR 52010 365 D 16 H 0.6 CD R REG 74 446 CHF AR 21504 365 V 16 H 0.6 CD R REG 74 447 CHF AR 52010 365 D 16 H 0.61 CD R REG 74 44
Alla et al.393 8 CHF RR 219 549 D 5 M MR P COH 66 839 CHF RR 182 549 D 8 M MR P COH 64 76
Krumholz 10 CHF RR 1129 183 D 4 H MR R REG 79 41et al.394 10 CHF RR 1047 183 V 4 H MR R REG 79 41Rosenthalet al.395 11 CHF RR 13834 30 D 27 M 0.8 CD R REG 79 42
Bouvy et al.396 12 CHF RR 152 549 D 7 M 0.77 MR P RCT 70 6613 CHF RR 152 549 D 8 M 0.80 MR P RCT 70 6614 CHF RR 152 549 D 9 M 0.84 MR P RCT 70 6615 CHF RR 152 549 D 10 M 0.85 MR P RCT 70 66
Kearney et al.397 16 CHF RR 553 1825 D 7 M 0.74 MR P COH 63 7616 CHF RR 553 1825 D 7 M 0.78 MR P COH 63 76
Lee et al.398 17 CHF RR 2624 30 D 10 M 0.8 CD R REG 76 5017 CHF RR 2624 30 D 10 M 0.82 CD R REG 76 5017 CHF RR 1407 30 V 10 M 0.79 CD R REG 75 5018 CHF RR 2624 365 D 11 M 0.77 CD R REG 76 5018 CHF RR 1407 365 V 11 M 0.76 CD R REG 75 50
Brophy et al.399 19 CHF RR 4277 365 D 9 M MR P RCT 63 7819 CHF RR 2145 365 V 9 M MR P RCT 63 7820 CHF RR 4277 1095 D 11 M MR P RCT 63 7820 CHF RR 2145 1095 V 11 M MR P RCT 63 78
Felker et al.400 21 ADHF RR 949 60 D 5 M 0.76 MR P RCT 68 6622 ADHF RR 949 60 D 5 MH 0.68 MR P RCT 68 66
Adlam et al.401 23 CHF RR 532 1825 D 6 M 0.75 MR P COH 75 4124 CHF AR 532 1825 D 6 M 0.75 MR P COH 75 41
Auble et al.402 25 CHF CA 33533 0 D 21 MH MR R COH 83.1 44Fonarow et al.403 26 ADHF CA 33046 0 D 3 M 0.69 MR R REG 73 48
26 ADHF CA 32229 0 V 3 M 0.67 MR R REG 73 4927 ADHF RR 33046 0 D 4 M 0.76 MR R REG 73 4827 ADHF RR 32229 0 V 4 M 0.76 MR R REG 73 49
Heywood et al.404 28 CHF RR 680 365 D 5 M MR P COH 62 6628 CHF RR 680 1825 D 5 M MR P COH 62 66
O’Connoret al.405 29 ADHF RR 930 60 D 6 MH MR P COH 62 52
Krumholz 30 CHF RR 222424 30 D 24 M 0.71 CD R REG 80 41et al.198 30 CHF RR 222157 30 V 24 M 0.7 CD R REG 80 41
30 CHF RR 422552 30 V 24 M 0.7 CD R REG 80 4130 CHF RR 426576 30 V 24 M 0.7 CD R REG 80 4130 CHF RR 422351 30 V 24 M 0.7 CD R REG 80 4131 CHF RR 46700 30 D 21 M 0.78 CD R REG 80 4131 CHF RR 46700 30 V 21 M 0.7 CD R REG 80 41
Levy et al.196 32 CHF RR 1125 365 D 14 M 0.73 MR P RCT 65 7632 CHF RR 925 365 V 14 M 0.68 MR P RCT 62 7832 CHF RR 2987 365 V 14 M 0.68 MR P RCT 71 6932 CHF RR 5010 365 V 14 M 0.69 MR P RCT 63 8032 CHF RR 872 365 V 14 M 0.75 MR R COH 64 7632 CHF RR 148 365 V 14 M 0.81 MR P COH 53 78
Pocock et al.406 33 CHF RR 7599 730 D 21 MH 0.75 MR P COH 66 7234 CHF RR 7599 730 D 21 M 0.75 MR P COH 66 68
Tabak et al.192 35 CHF RR 273034 0 D 1 M 0.61 MR R COH 77 4536 CHF RR 273034 0 D 13 M 0.77 MR R COH 77 4537 CHF RR 273034 0 D 15 M 0.77 MR R COH 77 4538 CHF RR 273034 0 D 18 M 0.8 MR R COH 77 4539 CHF RR 273034 0 D 20 M 0.81 MR R COH 77 45
TableS6– Continued on next page

227
TableS6– Continued from previous pagePaper N Pop SM Pt Du P # E C DS V Type Age ♂Yamokoski 40 CHF RR 373 180 D 3 M 0.6 MR P RCT 56 74et al.191 CHF 373 180 D M 0.61 MR P RCT 56 74
CHF 373 180 D H 0.58 MR P RCT 56 7441 CHF RR 373 180 D 2 H 0.52 MR P RCT 56 74
CHF 373 180 D M 0.68 MR P RCT 56 74CHF 373 180 D H 0.57 MR P RCT 56 74
Abraham et al.407 42 CHF RR 37548 680 D 17 M 0.77 MR R REG 73 4843 CHF AR 40201 680 D 7 M 0.76 MR R REG 73 4843 CHF AR 40201 680 V 7 M 0.75 MR R REG 73 4843 CHF AR 181830 680 V 7 M 0.75 MR R REG 73 4844 CHF CA 37548 680 D 4 M 0.68 MR R REG 73 48
Keenan et al.408 45 CHF RR 283919 30 D 34 H 0.6 CD R REG 80 4245 CHF RR 283528 30 V 34 H 0.6 CD R REG 80 4245 CHF RR 561763 30 V 34 H 0.61 CD R REG 80 046 CHF RR 64329 20 D 20 H 0.58 CD R REG 4246 CHF RR 64329 20 V 20 H 0.61 CD R REG 42
O’Connor 47 CHF RR 4402 90 D 13 M 0.72 MR R REG 73 48et al.409 48 CHF RR 4402 90 D 14 M 0.77 MR R REG 73 48
49 CHF AR 4402 60 D 8 M 0.72 MR R REG 73 4850 CHF RR 4014 90 D 15 MH 0.64 MR R REG 73 48
Levy et al.410 49 CHF RR 2521 365 D 17 M 0.71 MR P RCT 60 7749 CHF RR 10038 365 V 17 M 0.71 MR P COH 0
Vazquez et al.411 50 CHF RR 992 1338 D 8 M 0.78 MR P COH 65 7250 CHF RR 992 1338 V 8 M 0.78 MR P COH 65 7251 CHF RR 992 1338 D 6 M 0.8 MR P COH 65 7251 CHF RR 992 1338 V 6 M 0.78 MR P COH 65 7252 CHF RR 992 1338 D 5 M 0.77 MR P COH 65 7252 CHF RR 992 1338 V 5 M 0.74 MR P COH 65 7253 CHF RR 992 1338 D 9 M 0.76 MR P COH 65 7253 CHF RR 992 1338 V 9 M 0.75 MR P COH 65 72
Wedel et al.141 54 CHF RR 3368 1095 D 20 MH 0.653 MR P RCT 73 7554 CHF RR 3368 1095 D 20 M 0.667 MR P RCT 73 7554 CHF RR 3368 1095 D 20 M 0.742 MR P RCT 73 7555 CHF RR 3368 1095 D 14 MH 0.666 MR P RCT 73 7555 CHF RR 3368 1095 D 14 M 0.684 MR P RCT 73 7555 CHF RR 3368 1095 D 14 M 0.757 MR P RCT 73 7556 CHF RR 3368 1095 D 14 MH 0.701 MR P RCT 73 7556 CHF RR 3368 1095 D 14 M 0.719 MR P RCT 73 7556 CHF RR 3368 1095 D 14 M 0.8 MR P RCT 73 75
Amarasingham 57 CHF RR 1372 30 D 12 MH 0.73 MR P COH 57 61et al.412 57 CHF RR 1372 30 V 12 MH 0.69 MR P COH 57 61
27 CHF RR 1341 30 V 4 H 0.56 MR R COH 57 6127 CHF RR 1372 30 V 4 M 0.73 MR R COH 57 6130 CHF RR 1372 30 V 24 M 0.72 MR R COH 57 6139 CHF RR 1372 30 V 20 M 0.84 MR R COH 57 6139 CHF RR 1341 30 V 20 H 0.61 MR R COH 57 6157 CHF RR 1372 30 V 12 M 0.86 MR R COH 57 6130 CHF RR 1341 30 V 24 H 0.66 MR R COH 57 6157 CHF RR 1341 30 V 12 H 0.72 MR R COH 57 61
Lee et al.413 58 CHF RR 50816 7 D 7 M 0.81 CD R REG 74 4958 CHF RR 50816 30 D 12 M 0.76 CD R REG 74 49
O’Connor 59 CHF RR 433 182 D 4 M 0.78 MR P RCT 56 73et al.414 60 CHF RR 433 182 D 2 M 0.68 MR P RCT 56 73
60 CHF RR 433 182 V 2 M 0.74 MR P RCT 65 76Van Walraven 61 CHF RR 2406 30 D 4 MH 0.7 MR P COH 61 47et al.415 62 CHF AR 2406 30 D 4 MH 0.71 MR P COH 61 47
62 CHF AR 2406 30 V 4 MH 0.69 MR P COH 61 4762 CHF AR 4812 30 D 4 MH 0.80 MR P COH 61 4762 CHF AR 4812 30 V 4 MH 0.70 MR P COH 61 4762 CHF AR 1M 30 V 4 MH 0.68 MR P COH 59 5262 CHF AR 4812 30 D 4 H 0.688 MR P COH 61 47
Allen et al.416 63 CHF RR 2033 168 D 8 M 0.74 MR P RCT 67 7564 CHF RR 2033 168 D 9 M 0.72 MR P RCT 67 7565 CHF AR 2033 168 D 9 M 0.72 MR P RCT 67 7565 CHF AR 2033 168 V 9 M 0.73 MR P RCT 67 75
Axente et al.417 66 CHF RR 101 1342 D 5 M MR P COH 71 51Ky et al.193 49 CHF RR 1141 365 V 17 MH 0.81 MR P COH 56 67
TableS6– Continued on next page

228 Supplementary data
TableS6– Continued from previous pagePaper N Pop SM Pt Du P # E C DS V Type Age ♂
67 CHF RR 1141 365 D 1 MH 0.75 MR P COH 56 6770 CHF RR 1141 365 D 18 MH 0.83 MR P COH 56 6771 CHF RR 1141 365 D 18 MH 0.82 MR P COH 56 6772 CHF RR 1141 365 D 19 MH 0.82 MR P COH 56 6768 CHF RR 1141 365 D 1 MH 0.77 MR P COH 56 6769 CHF RR 1141 365 D 2 MH 0.80 MR P COH 56 67
Manzano et al.418 73 CHF RR 1400 640 D 10 MH 0.68 MR P RCT 76 6773 CHF RR 728 640 V 10 MH 0.66 MR P RCT 76 6474 CHF RR 1400 640 D 9 M 0.72 MR P RCT 76 6774 CHF RR 728 640 V 9 M 0.69 MR P RCT 76 64
Senni et al.419 75 CHF RR 2012 365 D 14 M 0.88 MR P COH 68 7075 CHF RR 4049 365 V 14 M 0.83 MR P COH 70 6176 CHF AR 2012 365 D 11 M 0.87 MR P COH 68 7076 CHF AR 4049 365 V 11 M 0.82 MR P COH 70 61
Smith et al.420 58 CHF RR 68380 7 V 7 M 0.75 MR R COH 74 4977 CHF RR 4696 1825 D 4 MH 0.63 MR R COH 4978 CHF RR 4696 1825 D 8 MH 0.67 MR R COH 4979 CHF RR 4696 1825 D 10 MH 0.68 MR R COH 4980 CHF RR 4696 1825 D 14 MH 0.69 MR R COH 4981 CHF RR 4696 1825 D 22 MH 0.71 MR R COH 49
Subramanian 82 CHF RR 963 365 D 5 M 0.73 MR P RCT 61 78et al.421 83 CHF RR 963 365 D 5 M 0.74 MR P RCT 61 78
84 CHF RR 963 365 D 5 M 0.81 MR P RCT 61 78Van Spall 58 ADHF RR 68380 1 V 7 M 0.81 MR R COH 74 49et al.422 58 ADHF RR 68380 0 V 7 M 0.88 MR R COH 74 49
85 ADHF RR 68380 30 D 2 M 0.65 MR R COH 76 4985 ADHF RR 68380 7 D 2 M 0.68 MR R COH 76 4985 ADHF RR 68380 1 D 2 M 0.72 MR R COH 76 4985 ADHF RR 68380 0 D 2 M 0.82 MR R COH 76 4958 ADHF RR 68380 30 V 12 M 0.71 MR R COH 74 49
Au et al.423 45 CHF RR 59652 30 V 34 M 0.69 CD R REG 76 5045 CHF RR 59652 40 V 34 H 0.59 CD R REG 76 5045 CHF RR 23454 40 V 34 M 0.68 CD R REG 76 5045 CHF RR 23454 30 V 34 H 0.59 CD R REG 76 5045 CHF RR 19764 30 V 34 H 0.58 CD R REG 76 5045 CHF RR 19764 30 V 34 M 0.66 CD R REG 76 5045 CHF RR 59652 30 V 34 MH 0.61 CD R REG 76 5045 CHF RR 23454 40 V 34 MH 0.60 CD R REG 76 5045 CHF RR 19764 30 V 34 MH 0.59 CD R REG 76 5045 CHF RR 59652 30 V 34 M 0.72 CD R REG 76 5045 CHF RR 23454 40 V 34 M 0.69 CD R REG 76 5045 CHF RR 19764 30 V 34 M 0.67 CD R REG 76 5086 CHF AR 59652 40 V 4 M 0.67 CD R REG 76 5086 CHF AR 23454 30 V 4 M 0.64 CD R REG 76 5086 CHF AR 19764 30 V 4 M 0.66 CD R REG 76 5086 CHF AR 59652 40 V 4 H 0.60 CD R REG 76 5086 CHF AR 23454 30 V 4 H 0.61 CD R REG 76 5086 CHF AR 19764 30 V 4 H 0.60 CD R REG 76 5086 CHF AR 59652 40 V 4 MH 0.61 CD R REG 76 5086 CHF AR 23454 40 V 4 MH 0.61 CD R REG 76 5086 CHF AR 19764 30 V 4 MH 0.60 CD R REG 76 5086 CHF AR 59652 30 V 4 M 0.66 CD R REG 76 5086 CHF AR 23454 30 V 4 M 0.66 CD R REG 76 5086 CHF AR 19764 30 V 4 M 0.65 CD R REG 76 5062 CHF AR 59652 30 V 4 M 0.55 CD R REG 76 5062 CHF AR 23454 30 V 4 M 0.55 CD R REG 76 5062 CHF AR 19764 40 V 4 M 0.56 CD R REG 76 5062 CHF AR 59652 30 V 4 H 0.58 CD R REG 76 5062 CHF AR 23454 40 V 4 H 0.58 CD R REG 76 5062 CHF AR 19764 30 V 4 H 0.58 CD R REG 76 5062 CHF AR 59652 30 V 4 MH 0.59 CD R REG 76 5062 CHF AR 23454 40 V 4 MH 0.59 CD R REG 76 5062 CHF AR 19764 40 V 4 MH 0.58 CD R REG 76 5062 CHF AR 59652 30 V 4 M 0.61 CD R REG 76 5062 CHF AR 23454 30 V 4 M 0.61 CD R REG 76 5062 CHF AR 19764 30 V 4 M 0.60 CD R REG 76 5011 CHF RR 59652 30 V 4 MH 0.60 CD R REG 76 5011 CHF RR 23454 30 V 4 MH 0.59 CD R REG 76 50
TableS6– Continued on next page

229
TableS6– Continued from previous pagePaper N Pop SM Pt Du P # E C DS V Type Age ♂
11 CHF RR 19764 40 V 4 MH 0.59 CD R REG 76 5011 CHF RR 59652 30 V 4 H 0.68 CD R REG 76 5011 CHF RR 23454 30 V 4 H 0.64 CD R REG 76 5011 CHF RR 19764 40 V 4 MH 0.58 CD R REG 76 5011 CHF RR 19764 40 V 4 H 0.66 CD R REG 76 5011 CHF RR 59652 30 V 4 MH 0.58 CD R REG 76 5011 CHF RR 23454 30 V 4 MH 0.58 CD R REG 76 5011 CHF RR 19764 40 V 4 M 0.66 CD R REG 76 5011 CHF RR 59652 30 V 4 M 0.71 CD R REG 76 5011 CHF RR 23454 30 V 4 M 0.68 CD R REG 76 50
Barlera et al.424 32 CHF RR 6975 1058 V 14 M 0.74 MR P RCT 77 7587 CHF RR 6975 1058 D 25 M 0.76 MR P RCT 77 7588 CHF RR 6975 1058 D 12 M 0.75 MR P RCT 77 75
Bayes-Genis 89 CHF RR 891 1018 D 11 M 0.76 MR P COH 70 72et al.425 90 CHF RR 891 1018 D 12 M 0.77 MR P COH 70 72
91 CHF RR 891 1018 D 12 M 0.78 MR P COH 70 7292 CHF RR 891 1018 D 13 M 0.79 MR P COH 70 72
Clemens et al.257 32 CHF RR 427 365 V 14 M 0.74 MR P COH 62 7332 CHF RR 427 1825 V 14 M 0.76 MR P COH 62 7332 CHF RR 427 730 V 14 M 0.80 MR P COH 62 7393 CHF RR 427 365 D 15 M 0.74 MR P COH 62 7393 CHF RR 427 1825 D 15 M 0.76 MR P COH 62 7393 CHF RR 427 730 D 15 M 0.79 MR P COH 62 7394 CHF RR 427 1825 D 15 M 0.76 MR P COH 62 7394 CHF RR 427 365 D 15 M 0.78 MR P COH 62 7394 CHF RR 427 730 D 15 M 0.81 MR P COH 62 7395 CHF RR 427 1825 D 15 M 0.76 MR P COH 62 7395 CHF RR 427 365 D 15 M 0.79 MR P COH 62 7395 CHF RR 427 730 D 15 M 0.81 MR P COH 62 7396 CHF RR 427 1825 D 15 M 0.77 MR P COH 62 7396 CHF RR 427 365 D 15 M 0.77 MR P COH 62 7396 CHF RR 427 730 D 15 M 0.80 MR P COH 62 7397 CHF RR 427 1825 D 15 M 0.75 MR P COH 62 7397 CHF RR 427 365 D 15 M 0.76 MR P COH 62 7397 CHF RR 427 730 D 15 M 0.80 MR P COH 62 7398 CHF RR 427 365 D 15 M 0.74 MR P COH 62 7398 CHF RR 427 1825 D 15 M 0.76 MR P COH 62 7398 CHF RR 427 730 D 15 M 0.80 MR P COH 62 7399 CHF RR 427 365 D 15 M 0.76 MR P COH 62 7399 CHF RR 427 1825 D 15 M 0.76 MR P COH 62 7399 CHF RR 427 730 D 15 M 0.80 MR P COH 62 73100 CHF RR 427 1825 D 16 M 0.78 MR P COH 62 73100 CHF RR 427 365 D 16 M 0.81 MR P COH 62 73100 CHF RR 427 730 D 16 M 0.82 MR P COH 62 73
de la Cámaraet al.426 101 CHF RR 600 365 D 5 M 0.76 MR P COH 74 49
Ketchum et al.194 53 CHF RR 961 365 V 17 M 0.69 MR P COH 62 80102 CHF RR 961 365 V 1 M 0.66 MR P COH 62 80103 CHF RR 961 365 D 18 M 0.73 MR P COH 62 80
Lee et al.427 104 CHF RR 7433 7 D 10 M 0.81 MR P COH 75 52104 CHF RR 5158 7 V 10 M 0.83 MR P COH 76 52
Martín-Sánchez 17 ADHF RR 1068 30 V 10 M 0.69 CD R REG 80 47et al.190 105 ADHF RR 1068 30 D 11 M 0.75 CD R REG 80 47
ADHF RR 1068 30 V 10 M 0.65 CD R REG 80 47O’Connor 106 CHF RR 2331 912 D 9 MH 0.64 MR P RCT 59 72et al.428 107 CHF RR 2331 912 D 10 M 0.74 MR P RCT 59 72
108 CHF AR 2331 912 D 4 MH 0.63 MR P RCT 59 72109 CHF AR 2331 912 D 4 M 0.7 MR P RCT 59 72
Oh et al.429 110 CHF RR 239 730 D 4 M 0.78 MR P COH 67 67110 CHF RR 66 730 V 4 M 0.8 MR P COH 67 70
Perrotta et al.430 32 CHF RR 342 730 V 14 M 0.69 MR P COH 72 7932 CHF RR 342 1825 V 14 M 0.69 MR P COH 72 7932 CHF RR 342 365 V 14 M 0.70 MR P COH 72 79
Postmus et al.431 111 CHF RR 1023 549 D 11 M 0.73 MR P RCT 71 62111 ADHF RR 576 549 V 11 M 0.70 MR P RCT 74 51112 CHF RR 1023 549 D 5 H 0.66 MR P RCT 71 62
Regoli et al.432 32 CHF RR 1139 365 V 14 M 0.66 MR R REG 67 77TableS6– Continued on next page

230 Supplementary data
TableS6– Continued from previous pagePaper N Pop SM Pt Du P # E C DS V Type Age ♂
32 CHF RR 1139 730 V 14 M 0.67 MR R REG 67 7732 CHF RR 1139 1825 V 14 M 0.68 MR R REG 67 77
Richter et al.433 113 CHF RR 349 1825 D 8 M 0.81 MR P COH 75 66114 CHF RR 349 1825 D 13 M 0.77 MR P COH 75 66115 CHF RR 349 1825 D 8 M 0.80 MR P COH 75 66
Wang et al.195 116 CHF RR 198640 30 D 49 MH 0.80 MR R COH 73 98116 CHF RR 198640 30 D 49 M 0.80 MR R COH 73 98116 CHF RR 198640 30 D 49 H 0.82 MR R COH 73 98117 CHF RR 198640 365 D 65 M 0.76 MR R COH 73 98117 CHF RR 198640 365 D 65 MH 0.77 MR R COH 73 98117 CHF RR 198640 365 D 65 H 0.82 MR R COH 73 98
N: Model number; Pt: Number of patients; Du: Duration; C: C-statistic; ♂: % male;Pop: Diagnosis of patients; CHF: chronic heart failure; ADHF: acute decompensated heart failure;SM: Statistical model; RR: regression; AR: Point-based additive risk score; CA: CART Model;V: View of study; P: Prospective; R: Retrospective;E: Event type; M: Mortality; H: Hospitalization; MH: Mortality or Hospitalizaion;DS: data source; MR: Medical Record; CD: Claims DataP: Procedure (Derivation or Validation); D: Derivation, V: Validation; #: Number of variables in model;Type: Type of study; COH: cohort; REG: registry; RCT: randomized controlled trial

231
Table S7: Description of the variables used in development of multivariate risk prediction models(Chapter 3) (percentage (number), mean ± standard deviation (SD) or median (interquartilerange (IQR)), with the percentage and number of values missing for patients
Index Validationmissing missing
Sex (male) 73.4% (1846) 0% (0) 65.9 (1145) 0% (0)Age (years) 68.9 ± 12 0% (0) 73.7 ± 10.7 0% (0)Smoking 0% (0) 1% (12)
Past 48% (1220) 35% (602)Current 14% (353) 13.7% (236)
Alcohol usage 28% (700) 1% (4) 47% (790) 2% (40)Body mass index (kg/m2) 27.9 ± 5.5 2% (38) 28.1 ± 6.4 2% (35)Heart rate (beats/ min) 80 ± 19.5 1% (6) 74.2 ± 16.6 2% (38)Systolic blood pressure (mmHg) 124.7 ± 21.9 1% (5) 125.9 ± 22.6 2% (28)Systolic blood pressure (mmHg) 74.9 ± 13.4 1% (5) 69.2 ± 13.2 2% (28)Left ventricular ejection fraction (%) 31 ± 10.6 11% (274) 41 ± 13.0 9% (163)HFpEF (LVEF>45%) 7 (162) 11% (274) 34% (529) 9% (163)NYHA class 3% (70) 1% (1)
I 2.2% (56) 1.0% (17)II 34.5% (868) 41.0% (712)III 48.8% (1228) 44.4% (772)IV 11.7% (294) 13.6% (236)
Ischemic heart disease 60.5% (1358) 11% (273) 64.9% (1128) 0% (0)Hospitalization in year before inclusion 31.6% (794) 0% (0) 26.5% (460) 0% (0)History of atrial fibrillation 45.4% (1143) 0% (0) 43.7% (760) 1% (14)Diabetes mellitus 32.6% (819) 0% (0) 32.3% (561) 1% (9)Hypertension 62.4% (1569) 0% (0) 57.9% (1007) 1% (7)eGFR (CKD-EPI) (mL/ min /1.73 m2) 64.4 (47.5-83.4) 6% (155) 66.1 (47.5-83.4) 1% (6)Myocardial infarction 38.3% (963) 0% (0) 48.8% (849) 1% (4)Coronary artery bypass graft 17.2% (433) 0% (0) 17.7% (308) 1% (2)Percutaneous coronary intervention 21.6% (544) 0% (0) 18.7% (325) 1% (18)Stroke 9.3% (233) 0% (0) 18.1% (315) 1% (16)Peripheral artery disease 10.9% (273) 0% (0) 21.5% (374) 3% (45)Chronic obstructive pulmonary disease 17.3% (436) 0% (0) 18.4% (319) 1% (15)Pulmonary congestion 3% (71) 5% (84)
Single base 12.7% (311) 5.7% (95)Bi-basilar 40.1% (980) 38.7% (639)
Edema 29.7 (624) 17% (417) 54.9 (955) 11% (192)Elevated jugular venous pressure 22% (554) 34% (861) 25.9% (450) 0% (0)Hepatomegaly 14.3% (358) 1% (7) 3.5% (60) 10% (171)Rales >1⁄3 up lung fields 19.2% (248) 49% (1225) 2.9% (50) 0% (0)Baseline medication
ACE-inhibitor/ARB 72.3% (1820) 0% (0) 70.1% (1218) 0% (0)Beta-blocker 83.2% (2093) 0% (0) 72.7% (1264) 0% (0)
Hematocrit (%) 40.1% (36.3-43.7) 11% (274) 40.5% (37.0-44.3) 1% (18)Blood urea nitrogen (mmol/L) 11.1 (7.4-17.6) 12% (301) 8.6 (6.5-11.9) 1% (9)NT-proBNP (pg/mL) 4275 (2360-8486) 53% (1334) 1376 (510-3548) 2% (29)Sodium (mmol/L) 140 (137-142) 8% (189) 139.0 (137.0-141.0) 1% (7)Potassium(mmol/L) 4.2 (3.9-4.6) 8% (192) 4.3 (4.0-4.6) 1% (13)Bilirubin (µmol/L) 14 (10-21) 45% (1135) 10 (7-15) 1% (20)HDL-cholesterol (mmol/L) 1 (0.8-1.3) 54% (1350) 1 (0.9-1.4) 4% (72)Alkaline phosphatase (µg/L) 84 (65-117) 6% (156) 89 (72-116) 1% (10)Hemoglobin (g/dL) 13.3 (11.9-14.5) 9% (223) 13.2 (11.8-14.5) 1% (16)Albumin (g/L) 33 (27-38) 6% (156) 38 (34-42) 1% (13)ALAT (U/L) 25 (19-35) 39% (981) 22 (17-33) 1% (23)ASAT (U/L) 25 (17-38) 28% (712) 23 (18-31) 6% (105)Glucose (mmol/L) 6.3 (5.5-7.9) 25% (622) 6.3 (5.2-8.4) 14% (248)ALAT: alanine aminotransferase; ALAT: alanine aminotransferase; eGFR: estimated glomerular filtration rate;HDL: high density lipoprotein; HFpEF: heart failure with preserved ejection fraction;LVEF: left ventricular ejection fraction; NYHA class: New York Heart Association class;NT-proBNP: N-terminal pro B-type natriuretic peptide

232 Supplementary data
Table S8: Variables used in the stepwise regression methods (Chapter 4) to predict successfulor not successful up-titration, with number (percentage), mean ± SD, or median (IQR)
Description of baseline patient characteristicsN 2100 LaboratoryDemographics eGFR (CKD-EPI) (mL/ min /1.73 m2) 66.7 ± 23.66Sex (Male) 1589 (75.7%) Hematocrit (%) 40.5 ± 5.26Age (years) 67.7 ± 11.95 Blood urea nitrogen (mmol/L) 10.8 (7.3-17.17)Country NT-proBNP (pg/mL) 4138 (2249-8220)
Netherlands 276 (13.1%) Hemoglobin (g/L) 13.4 ± 1.85Germany 84 (4%) Sodium (mmol/L) 139.2 ± 3.83France 195 (9.3%) Potassium (mmol/L) 4.3 ± 0.55Greece 278 (13.2%) BNP (pg/mL) 637 (291-1197)Italy 289 (13.8%) Bilirubin (µmol/L) 14 (9.92-20.61)Norwegen 93 (4.4%) Total-cholesterol (mmol/L) 4.3 ± 1.36Poland 244 (11.6%) HDL-cholesterol (mmol/L) 1.1 ± 0.39Serbia 366 (17.4%) Hepcidin (nmol/L) 6.5 (2.3-17)Slovenia 22 (1%) STfR (mg/L) 1.5 (1.14-2.02)Sweden 96 (4.6%) FT4 (pmol/L) 15.8 (13.16-18.9)United Kingdom 157 (7.5%) HbA1c (%) 6.3 (5.74-7.12)
Smoking ASAT (U/L) 25 (17-38)No 772 (36.8%) ALAT (U/L) 25 (19-35)Past 1026 (48.9%) TSH (µU/L) 1.8 (1.19-2.9)Current 302 (14.4%) Gamma-GT (U/L) 54 (28-103)
Alcohol usage 595 (28.4%) Alkaline phosphatase (µg/L) 84 (64.98-117)Body mass index (kg/m2) 28 ± 5.52 TnI (pg/mL) 12.2 (6.56-25.87)NYHA class ET-1 (pg/mL) 5.2 (3.93-6.93)
I 54 (2.6%) Bio-ADM (pg/mL) 31.8 (21.95-49.67)II 760 (37.1%) Proteinuria (pg/dL) 5.0 (0-19.25)III 1004 (49%) Troponin (µg/L) 0.04 (0.01-0.10)IV 232 (11.3%)
Clinical ProfileLeft ventricular ejection fraction (%) 28.6 ± 7.49Heart Rate (beats/ min) 79.8 ± 19.43Systolic blood pressure (mmHg) 124.2 ± 21.24Diastolic blood pressure (mmHg) 75.5 ± 13.05Pulmonary congestion
Single base 260 (12.7%)Bi-basilar 756 (37%)
Peripheral oedema 988 (47%)Elevated jugular venous pressure 442 (30%)Hepatomegaly 291 (13.9%)3rd Heart Tone 220 (10.5%)Rales >1⁄3 up lung fields 183 (18%)Orthopnea present 678 (32.3%)Medical HistoryIschemic heart disease 1154 (55%)Hospitalizationin year before inclusion 669 (31.9%)Heart failure duration (years) 8 (3.55-13.27)Diabetes mellitus 676 (32.2%)Atrial fibrillation 901 (42.9%)Myocardial infarction 822 (39.1%)Coronary artery bypass graft 344 (16.4%)Coronary artery disease 957 (45.6%)Percutaneous coronary intervention 473 (22.5%)Stroke 187 (8.9%)Peripheral arterial disease 214 (10.2%)COPD 344 (16.4%)

233
Table S9: CRF page on how ACE-inhibitor/ARB and beta-blocker medication was recorded
ACE-inhibitor/ARB
Drug name* Total dailydose (mg)
Start date(dd/mm/yyyy)
End date(dd/mm/yyyy) Ongoing at 9
month visitReason # Specify reason
Beta-blocker
Drug name* Total dailydose (mg)
Start date(dd/mm/yyyy)
End date(dd/mm/yyyy) Ongoing at 9
month visitReason # Specify reason
*also include drugs stopped within 3 months before inclusion
reasons #1=Non optimal dose acc. to ESC guidelines;2=Symptoms;3=Side effects ;4=Non-cardiac organ dysfunction;99=Other, specify

234 Supplementary data
Table S10: Description of the variables used in development of treatment-selection model, withmean ± SD, or median (IQR)
Mean ± SD ormedian (IQR))
%Missing
Mean ± SD ormedian (IQR))
%Missing
Standard laboratory results Olink Proseek Multiplex panel (NPX)Hematocrit (%) 40.13 ± 5.3 6% TNFRSF14 (NPX) 4.20 ± 0.84 0%Total Cholesterol(mmol/L) 4.32 ± 1.34 41% LDL-receptor (NPX) 3.01 ± 0.87 0%Serum creatinine(µmol/L) 101.0 (83.1-127.0) 0% ITGB2 (NPX) 4.40 ± 0.73 10%BUN (mmol/L) 14.51 ± 11.65 12% IL-17RA (NPX) 3.25 ± 0.71 0%LVEF (%) 31.05 ± 10.58 10% TNF-R2 (NPX) 4.35 ± 0.88 0%NT-proBNP (ng/L) 3949 (2254-7690) 51% MMP-9 (NPX) 3.09 ± 1.05 0%Hemoglobin (g/dL) 13.25 ± 1.88 4% EPHB4 (NPX) 1.54 ± 0.58 0%Sodium (mmol/L) 139.31 ± 3.79 2% IL2-RA (NPX) 3.65 ± 0.82 0%Potassium (mmol/L) 4.26 ± 0.56 2% OPG (NPX) 2.63 ± 0.71 0%BNP (local) (pg/mL) 662 (354-1281) 88% ALCAM (NPX) 4.1 ± 0.63 0%Total Bilirubin (µmol/L) 13.68 (9.80-20.52) 41% TFF3 (NPX) 5.22 ± 0.93 0%Glucose (mmol/L) 6.27 (5.38-7.9) 20% SELP (NPX) 8.21 ± 1.13 0%LDL-cholesterol(mmol/L) 2.61 ± 1.07 54% CSTB (NPX) 4.63 ± 0.87 0%HDL-cholesterol(mmol/L) 1.11 ± 0.38 51% MCP-1 (NPX) 2.26 ± 0.69 0%Serum Iron (local)(µmol/L) 12.0 (8.0-16.7) 78% CD163 (NPX) 6.77 ± 0.8 0%Calcium (mmol/L) 1.77 (1.51-2.03) 4% Gal-3 (NPX) 4.42 ± 0.71 0%Phosphate (mmol/L) 0.85 (0.68-1.03) 4% GRN (NPX) 2.99 ± 0.64 0%Albumin (g/L) 32 (27-38) 4% MEPE (NPX) 2.21 ± 0.72 0%Serum Iron (UMCG)(µg/L) 8 (5-13) 4% BLM hydrolase (NPX) 4.51 ± 0.66 0%Ferritin (µg/L) 102 (50-192) 4% PLC (NPX) 6.41 ± 0.76 0%Transferrin (g/L) 2.0 (1.6-2.5) 4% LTBR (NPX) 3.00 ± 0.75 0%Hepcidin (nmol/L) 6.7 (2.2-17.0) 4% NOTCH3 (NPX) 3.18 ± 0.75 0%sTfR (mg/L) 1.51 (1.16-2.06) 5% TIMP4 (NPX) 4.46 ± 0.82 0%FT4 pmol/L) 16 (13.6-19.13) 77% CNTN1 (NPX) 1.85 ± 0.67 0%HbA1c (%) 6.58 ± 1.49 79% CDH5 (NPX) 2.74 ± 0.71 0%ASAT (U/L) 25 (17-38) 23% TLT-2 (NPX) 3.49 ± 0.77 0%ALAT (U/L) 25 (19-35) 31% FABP4 (NPX) 5.28 ± 1.32 0%TSH (mU/L) 1.8 (1.1-2.8) 60% TFPI (NPX) 7.68 ± 0.73 0%Proteinuria (mg/dL) 5 (0-17) 90% PAI (NPX) 4.89 ± 1.19 0%Gamma-GT (mU/L) 54 (28-107) 50% CCL24 (NPX) 4.83 ± 1.08 0%Alkaline phosphatase(µg/L) 83.59 (64.78-116) 49% TR (NPX) 5.01 ± 0.83 0%Troponin I (pg/mL) 12.35 (6.75-26.69) 3% TNFRSF10C (NPX) 5.23 ± 0.77 0%ET-1 (pg/mL) 5.27 (4.00-6.99) 4% GDF-15 (NPX) 4.92 ± 1.02 0%pro-ENK (pmol/L) 84.45 (62.77-116.71) 0% SELE (NPX) 1.49 ± 0.78 0%bio-ADM (pg/mL) 32.99 (22.41-51.55) 0% AZU1 (NPX) 2.13 ± 0.95 0%Troponin (µg/L) 0.03 (0.01-0.10) 72% DLK-1 (NPX) 4.20 ± 0.94 0%FGF-23 (RU/mL) 211.7 (118.1-524.2) 0% SPON1 (NPX) 1.70 ± 0.65 0%Erythrocytes(10 · 1012/L) 4.48 (4.05-4.88) 26% MPO (NPX) 3.51 ± 0.71 0%Platelets (10 · 109/L) 215 (173-260) 17% CXCL16 (NPX) 5.50 ± 0.67 0%Leucocytes(10 · 109/L) 7.8 (6.41-9.46) 16% IL6-RA (NPX) 10.08 ± 0.66 0%
Alere Luminex Panel RETN (NPX) 5.96 ± 0.84 0%ANP-propeptide(ng/mL) 20.47 (12.71-31.02) 3% IGFBP-1 (NPX) 4.58 ± 1.35 0%BNP (pg/mL) 223.12 (90.58-452.6) 3% CHIT1 (NPX) 2.16 ± 1.51 0%ESAM-1 (ng/mL) 63.84 (57.31-70.4) 3% TR-AP (NPX) 4.31 ± 0.70 0%LTβR (ng/mL) 0.15 (0.10-0.23) 3% CCL22 (NPX) 1.58 ± 0.98) 0%Mesothelin (ng/mL) 54.73 ± 12.66 3% PSP-D (NPX) 2.1 ± 0.80 0%MPO (ng/mL) 31.51 ± 14.69 3% PI3 (NPX) 3.27 ± 0.85 0%Neuropilin (ng/mL) 21.8 ± 7.67) 3% Ep-Cam (NPX) 2.93 ± 1.00 0%NT-proCNP (pg/mL) 12.31 ± 14.26 3% AP-N (NPX) 4.24 ± 0.71 0%OPN (ng/mL) 220.44 ± 63.96 3% AXL (NPX) 7.07 ± 0.72 0%PCT (pg/mL) 15.95 (5.97-36.58) 3% IL-1RT1 (NPX) 5.83 ± 0.71 0%PSAP-B (ng/mL) 31.46 (22.94-37.85) 3% MMP-2 (NPX) 2.77 ± 0.79 0%
TableS10– Continued on next page

235
TableS10– Continued from previous pageMean ± SD ormedian (IQR))
%Missing
Mean ± SD ormedian (IQR))
%Missing
VEGFR-1 (ng/mL) 0.14 (0.14-0.23) 3% FAS (NPX) 4.15 ± 0.71 0%D-dimer (ng/mL) 101.92 (101.92-135.41) 3% MB (NPX) 6.22 ± 1.00 0%Pentraxin-3 (ng/mL) 2.03 (1.24-3.41) 3% TNFSF13B (NPX) 5.35 ± 0.78 0%PIGR-1 (ng/mL) 123.89 (76.6-200.64) 3% PRTN3 (NPX) 3.99 ± 0.81 0%RAGE (ng/mL) 2.75 (1.93-4.03) 3% PCSK9 (NPX) 1.84 ± 0.58 0%Syndecan-1 (ng/mL) 2.17 (1.16-3.87) 3% U-PAR (NPX) 4.06 ± 0.75 0%TNF-R1A (ng/mL) 1.02 (0.61-1.67) 3% OPN (NPX) 4.79 ± 0.95 0%Troy (ng/mL) 0.24 (0.13-0.41) 3% CTSD (NPX) 3.21 ± 0.70 0%GDF-15 (ng/mL) 3.44 (2.72-4.30) 3% PGLYRP1 (NPX) 6.56 ± 0.84 0%ProADM (ng/mL) 0.49 (0.32-0.78) 3% CPA1 (NPX) 3.70 ± 1.10 0%ST2 (ng/mL) 8.51 (3.81-18.36) 3% JAM-A (NPX) 4.64 ± 1.24 0%WAP-4C (ng/mL) 1.41 (0.77-2.83) 3% Gal-4 (NPX) 3 ± 0.80 0%Periostin (ng/mL) 6.12 (3.52-9.85) 3% IL-1RT2 (NPX) 4.02 ± 0.67 0%Angiogenin (ng/mL) 4565 (3147-7002) 3% SHPS-1 (NPX) 2.93 ± 0.70 0%Cystatin C (ng/mL) 15074 (10282-22083) 3% CCL15 (NPX) 6.55 ± 0.81 0%CRP (ng/mL) 12898 (5739-26146) 3% CASP-3 (NPX) 6.74 ± 1.72 0%Gal-3 (ng/mL) 20.84 (15.13-29.09) 3% uPA (NPX) 3.87 ± 0.69 0%NGAL (ng/mL) 58.85 (37.48-93.25) 3% CPB1 (NPX) 3.41 ± 1.05 0%
CHI3L1 (NPX) 5.63 ± 1.20 0%(NPX) 3.75 ± 1.02 0%t-PA (NPX) 5.05 ± 1.44 0%SCGB3A2 (NPX) 2.17 ± 1.04 0%EGFR (NPX) 0.59 ± 0.51 0%IGFBP-7 (NPX) 3.69 ± 0.91 0%CD93 (NPX) 8.86 ± 0.68 0%IL-18BP (NPX) 5.67 ± 0.77 0%COL1A1 (NPX) 1.61 ± 0.67 0%PON3 (NPX) 4.22 ± 1.02 0%CTSZ (NPX) 4.15 ± 0.70 0%MMP-3 (NPX) 6.71 ± 1.01 0%RARRES2 (NPX) 10.97 ± 0.60 0%ICAM-2 (NPX) 4.26 ± 0.72 0%KLK6 (NPX) 2.74 ± 0.48 0%PDGF(NPX) 1.86 ± 1.18 0%TNF-R1 (NPX) 4.95 ± 0.93 0%IGFBP-2 (NPX) 7.59 ± 0.92 0%vWF (NPX) 6.08 ± 1.36 0%PECAM-1 (NPX) 4.29 ± 0.99 0%NT-proBNP (NPX) 2.96 ± 1.35 0%CCL16 (NPX) 5.37 ± 0.86 0%

236 Supplementary data
Table S11: Biomarkers predictive for successful up-titration to recommended ACE-inhibitors/ARBs doses (Chapter 5)
log(OR) SE p log(OR) SE pIntercept 1.1389 1.4057 0.42 BUN (mmol/L) -0.0059 0.011 0.59NYHA class -0.0147 0.0467 0.75 LVEF (%) -0.0216 0.0152 0.15Ischemic etiology -0.0642 0.0558 0.25 NT-proBNP (ng/L) <0.00001 <0.00001 0.86Atrial fibrillation -0.0322 0.0911 0.72 Hemoglobin (g/dL) <0.00001 <0.00001 0.82Diabetes mellitus -0.1097 0.1919 0.57 Glucose (mmol/L) 0.0059 0.0251 0.82Hypertension 0.1547 0.1219 0.20 LDL (mmol/L) 0.0328 0.0301 0.28Smoking 0.1567 0.1361 0.25 HDL (mmol/L) 0.0701 0.1831 0.70Alcohol use 0.0387 0.1071 0.72 Calcium (mmol/L) 0.0075 0.0112 0.50Coronary artery disease 0.1307 0.1576 0.41 Phosphate (mmol/L) 0.084 0.1558 0.59Renal disease -0.0733 0.1898 0.70 Albumin (g/L) 0.072 0.1858 0.70Myocardial infarction -0.2858 0.2139 0.18 ASAT (U/L) 0.0105 0.0316 0.74Valvular surgery -0.0512 0.1532 0.74 Proteinuria (mmol/dL) -0.0076 0.0223 0.73
PCI -0.2062 0.2174 0.34 Alkaline phosphatase(µg/mL) -0.0001 0.0006 0.81
Device therapy -0.0371 0.0931 0.69 Troponin I (pg/mL) -0.0013 0.0021 0.54Height (m) -0.1533 0.1026 0.14 Pro-ENK (pmol/L) -0.0002 0.0009 0.83Weight (kg) 0.0024 0.0065 0.711 Bio-ADM (pg/mL) -0.0006 0.0015 0.70Heart rate (beats/ min) 0.0087 0.0076 0.26 FGF-23 RU/mL -0.0001 0.0002 0.74
SBP (mmHg) 0.0001 0.0074 0.99 ANP-propeptide(ng/mL) -0.0002 0.0002 0.39
DBP (mmHg) 0.0109 0.0036 0.003 Periostin (ng/mL) 0.0007 0.0226 0.98Pulmonary congestion -0.0199 0.0825 0.81 Gal-3 (ng/mL) -0.0009 0.003 0.77Elevated JVP -0.1024 0.0805 0.20 NGAL (ng/mL) -0.0042 0.005 0.40
Hepatomegaly -0.0665 0.1763 0.71 Serum creatinine(µmol/L) -0.0003 0.0012 0.80
3rd heart tone -0.3022 0.2297 0.19 T-PA (NPX) -0.0026 0.0382 0.94BMI (kg/m2) 0.0007 0.009 0.94 TNF-R1 (NPX) -0.0245 0.0715 0.73Rales >1⁄3 up lung fields 0.0049 0.018 0.78 IGFBP-2 (NPX) -0.1036 0.099 0.30Total cholesterol(mmol/L) 0.0047 0.0217 0.83 ST2 (NPX) -0.0053 0.0295 0.86
BMI: body mass index; BUN: Blood urea nitrogen;COPD:Chronic obstructive pulmonary disease;DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; JVP: Jugular venous pressure;LVEF: Left ventricular ejection fraction; NPX: normalized protein expression units;NYHA class: New York Heart Association class; OR: Odds ratio; PCI: Percutaneous coronary intervention;p: p-value; SBP: Systolic blood pressure; SE: standard error

237
Table S12: Biomarkers predictive for successful beta-blocker up-titration to recommended doses(Chapter 5)
log(OR) SE p log(OR) SE pIntercept -5.8903 3.9583 0.14 FT4 (pmol/L) -0.0815 0.0812 0.32Male gender 0.0866 0.2228 0.70 ASAT (U/L) 0.0107 0.0305 0.73Race 0.229 0.2594 0.38 ALAT (U/L) 0.0023 0.0031 0.462Previous heart failurehospitalization in yearbefore inclusion
-0.1046 0.2018 0.60 TSH (mU/L) 0.0077 0.0225 0.73
Valvular disease -0.029 0.0848 0.73 CRP (ng/mL) <0.000001 <0.000001 0.72Heart failure duration 0.1421 0.1381 0.30 Proteinuria (mg/dL) 0.0196 0.0346 0.57NYHA class -0.0052 0.0069 0.46 Gamma-GT (U/L) -0.0008 0.0036 0.81
Ischemic etiology -0.0218 0.044 0.62 Alkaline phosphatase(µg/L) 0.0001 0.0022 0.98
Atrial fibrillation 0.0093 0.0524 0.86 Troponin I (pg/mL) -0.0017 0.0017 0.31Diabetes mellitus 0.0581 0.1033 0.57 ET-1 (pg/mL) -0.0123 0.029 0.67Hypertension -0.0325 0.0958 0.73 pro-ENK (pmol/mL) -0.053 0.0414 0.20Alcohol use 0.0639 0.1645 0.70 BNP (UMCG) (pg/mL) 0.0001 0.0003 0.72Coronary arterydisease 0.3228 0.124 0.01 ESAM-1 (ng/mL) 0.0004 0.0005 0.39Renal disease 0.1843 0.1632 0.26 MPO (ng/mL) -0.003 0.0076 0.69PCI 0.0073 0.0684 0.91 Neuropilin (ng/mL) -0.0114 0.0083 0.17Stroke 0.0023 0.1155 0.98 D-dimer (ng/mL) -0.0003 0.0008 0.70Peripheral arterydisease -0.0423 0.1262 0.74 Pentraxin-3 (ng/mL) 0.0247 0.067 0.71COPD -0.1949 0.1676 0.24 PIGR-1 ng/mL) 0.1158 0.0937 0.22Device therapy -0.0269 0.1432 0.85 GDF-15 (ng/mL) 0.0043 0.0279 0.88Weight (kg) 0.0864 0.0618 0.16 proADM (pg/mL) 0.0494 0.1336 0.71Height (m) 0.0063 0.0083 0.44 (ng/mL) 0.2341 0.247 0.34Heart rate(beats/ min) 0.0028 0.0069 0.69 WAP-4C (ng/mL) -0.0119 0.0135 0.38SBP (mmHg) 0.0123 0.008 0.13 Periostin (ng/mL) -0.029 0.0577 0.6DBP (mmHg) 0.0034 0.0085 0.69 NGAL (ng/mL) -0.0034 0.0054 0.53Pulmonary congestion -0.0325 0.1178 0.78 Gal-3 (ng/mL) -0.0015 0.0043 0.72Elevated JVP -0.1798 0.0735 0.01 CCL16 (NPX) 0.0225 0.0644 0.73Hepatomegaly -0.0321 0.0868 0.71 TNFRSF14 (NPX) -0.0008 0.0014 0.58eGFR (CKD-EPI)(mL/ min /1.73 m2) -0.0363 0.0912 0.69 OPG (NPX) -0.0576 0.1058 0.59
Hematocrit (%) -0.0197 0.0756 0.79 TFPI (NPX) -0.0602 0.1546 0.70BUN (mmol/L) -0.0033 0.0088 0.71 PAI (NPX) -0.1717 0.1959 0.38LVEF (%) -0.0113 0.017 0.51 SELE (NPX) 0.038 0.0976 0.70NT-proBNP (ng/L) 0.0112 0.0086 0.19 AZU1 (NPX) 0.1564 0.1206 0.19Sodium (mg/dL) 0.0043 0.0122 0.72 RETN (NPX) 0.0315 0.0929 0.73Potassium (mg/dL) 0.0163 0.016 0.31 IGFBP-1 (NPX) -0.0066 0.0234 0.78BNP (local) (pg/mL) 0.0376 0.1008 0.71 CHIT1 (NPX) -0.0118 0.0339 0.73Total bilirubin (µg/dL) -0.0025 0.0068 0.71 MMP-3 (NPX) 0.0409 0.1048 0.70Glucose (mg/dL) -0.0129 0.0097 0.19 RARRES2 (NPX) 0.1598 0.1377 0.25LDL-cholesterol(mmol/L) 0.0151 0.0271 0.58 PDGF
(NPX) -0.011 0.0311 0.72Serum iron (µmol/L) -0.034 0.1942 0.86 TNF-R1 (NPX) -0.0562 0.0464 0.23Calcium (mmol/L) -0.062 0.16 0.70 vWF (NPX) -0.0088 0.0463 0.85Phosphate(mmol/L) -0.1603 0.1689 0.34 Leucocytes
(10 · 109 cells/L) 0.0007 0.0009 0.43
Serum iron (µmol/L) 0.0081 0.0207 0.69 Erythrocytes(10 · 1012/L
0.0682 0.0822 0.41
Ferritin (µg/L) 0.0109 0.0184 0.55 Platelets(10 · 109 cells/L) 0.019 0.0567 0.74
sTfR (µg/L) -0.0156 0.0496 0.75BMI: body mass index; BUN: Blood urea nitrogen;COPD:Chronic obstructive pulmonary disease;DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; JVP: Jugular venous pressure;LVEF: Left ventricular ejection fraction; NPX: normalized protein expression units;NYHA class: New York Heart Association class; OR: Odds ratio; PCI: Percutaneous coronary intervention;p: p-value; SBP: Systolic blood pressure; SE: standard error

238 Supplementary dataTa
ble
S13:
Dem
ogra
phic
sofM
clus
tclu
ster
ing
(Cha
pter
6)in
the
inde
xco
hort
,with
perc
enta
ges(
num
bers
),m
ean
±SD
,orm
edia
n(I
QR
),an
d%
ofm
issin
gva
lues
Clu
ster
s1
23
45
67
89
1011
p-v
alu
eN
654
5309
31276
19191
306
6702
17Sex(m
ale)
37%
(241)
80%
(4)
75%
(233)
87%
(27)
78%
(215)
89%
(17)
100%
(191)
82%
(251)
83%
(5)
93%
(650)
71%
(12)
<0.00001
Age
72(±
11.7)
72(±
7.9)
72(±
9.1)
63(±
15)
71(±
10.6)
57(±
11.4)
67(±
13.7)
68(±
11.2)
63(±
12.3)
66(±
12.3)
59(±
12.5)
<0.00001
race
(Cau
casian
)100%
(654
)100%
(5)
100%
(309)
65%
(20)
100%
(276)
95%
(18)
100%
(191)
100%
(306)
100%
(6)
100%
(702)
12%
(2)
<0.00001
Smok
ing
<0.00001
Past
37%
(239)
40%
(2)
62%
(192)
45%
(14)
57%
(157)
47%
(9)
46%
(88)
50%
(152)
33%
(2)
51%
(356)
53%
(9)
Currently
8%
(54)
40%
(2)
18%
(56)
19%
(6)
16%
(45)
32%
(6)
18%
(35)
14%
(44)
17%
(1)
14%
(100)
24%
(4)
Alcoh
oluse
17%
(113)
60%
(3)
31%
(96)
35%
(11)
28%
(77)
58%
(11)
40%
(76)
31%
(96)
0%
(0)
30%
(212)
29%
(5)
<0.00001
BMI
28(±
5.8)
25(±
5.3)
27(±
5.5)
26(±
4.3)
28(±
5.3)
28(±
5.1)
27(±
4.5)
28(±
5.8)
25(±
5.9)
28(±
5.3)
27(±
8.3)
0.95
Heart
rate
82(±
20.6)
105(±
33.2)
79(±
18.7)
86(±
17.7)
78(±
18.4)
91(±
24.6)
88(±
23.4)
81(±
18.6)
78(±
10.4)
76(±
17.1)
83(±
16.1)
0.0002
NYHA
class
<0.00001
I2%
(10)
0%
(0)
0%
(1)
0%
(0)
1%
(3)
0%
(0)
1%
(2)
1%
(4)
0%
(0)
5%
(35)
7%
(1)
II31
%(195)
40%
(2)
29%
(85)
14%
(4)
29%
(77)
22%
(4)
23%
(42)
18%
(54)
33%
(2)
58%
(398)
33%
(5)
III
53%
(336)
60%
(3)
54%
(159)
54%
(15)
55%
(148)
56%
(10)
59%
(108)
66%
(196)
50%
(3)
35%
(242)
53%
(8)
IV15
%(96)
0%
(0)
17%
(49)
32%
(9)
15%
(41)
22%
(4)
17%
(31)
15%
(45)
17%
(1)
2%
(17)
7%
(1)
LVEF
33(±
11.3)
24(±
8)31
(±10.9)
27(±
12)
32(±
10.8)
25(±
12.6)
29(±
11.3)
29(±
10.2)
27(±
12.6)
30(±
9)28
(±7)
<0.00001
HFho
spitalizationin
year
before
inclusion
34%
(220)
40%
(2)
30%
(94)
32%
(10)
37%
(101)
5%
(1)
17%
(33)
41%
(124)
33%
(2)
29%
(202)
29%
(5)
0.00001
Ischem
icHF
50%
(327)
40%
(2)
57%
(176)
45%
(14)
72%
(200)
26%
(5)
44%
(84)
52%
(159)
33%
(2)
55%
(383)
35%
(6)
<0.00001
AF
45%
(293)
80%
(4)
50%
(153)
39%
(12)
50%
(139)
37%
(7)
47%
(90)
53%
(161)
50%
(3)
40%
(278)
18%
(3)
0.0009
DM
44%
(286)
20%
(1)
33%
(102)
42%
(13)
51%
(140)
16%
(3)
1%
(2)
36%
(109)
0%
(0)
23%
(159)
24%
(4)
<0.00001
COPD
0%
(0)
0%
(0)
99%
(307)
13%
(4)
20%
(56)
11%
(2)
1%
(1)
21%
(64)
17%
(1)
0%
(0)
6%
(1)
<0.00001
Peripheralartery
disease
0%
(0)
0%
(0)
0%
(0)
0%
(0)
99%
(272)
5%
(1)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
<0.00001
Pulmon
arycong
estion
<0.00001
Sing
leba
se20
%(126)
0%
(0)
11%
(34)
16%
(5)
13%
(34)
0%
(0)
21%
(40)
15%
(44)
17%
(1)
3%
(23)
24%
(4)
Bi-ba
silar
53%
(331)
60%
(3)
43%
(131)
48%
(15)
48%
(129)
58%
(11)
75%
(141)
53%
(162)
50%
(3)
7%
(46)
47%
(8)
Peripheraledem
a52
%(343)
60%
(3)
55%
(169)
74%
(23)
56%
(154)
68%
(13)
55%
(106)
69%
(210)
83%
(5)
32%
(224)
35%
(6)
<0.00001
Rales
1 ⁄3lung
fields
16%
(75)
33%
(1)
22%
(36)
30%
(6)
22%
(36)
9%
(1)
17%
(30)
18%
(37)
25%
(1)
30%
(21)
33%
(4)
0.15
ElevatedJV
P28
%(116)
20%
(1)
28%
(60)
52%
(12)
41%
(82)
36%
(5)
40%
(50)
62%
(158)
50%
(3)
13%
(63)
36%
(4)
<0.00001
Hepatom
egaly
0%
(0)
0%
(0)
0%
(0)
35%
(11)
12%
(34)
5%
(1)
1%
(2)
100%
(306)
67%
(4)
0%
(0)
0%
(0)
<0.00001
Hyp
ertension
70%
(459)
40%
(2)
60%
(185)
45%
(14)
77%
(213)
47%
(9)
35%
(67)
62%
(189)
33%
(2)
59%
(416)
76%
(13)
<0.00001
SBP
129
110
123
113
126
120
121
120
107
125
120
(mm
Hg)
(±24.1)
(±20.8)
(±20.4)
(±16.1)
(±24.4)
(±19.2)
(±24.4)
(±19.4)
(±10.8)
(±19.2)
(±17.3)
0.0002
Hem
oglobin(g
/dL)
13(±
1.8)
13(±
2.6)
13(±
1.8)
13(±
2)13
(±1.8)
13(±
1.6)
14(±
2.1)
13(±
1.9)
13(±
1.5)
14(±
1.9)
14(±
1.5)
<0.00001
Sodium
(mm
ol/L)
139(±
4.3)
133(±
9)139(±
3.8)
137(±
5)139(±
3.8)
137(±
4.2)
139(±
4.1)
139(±
4.1)
135(±
3.3)
140(±
3.5)
140(±
2.2)
0.19
eGFR
(MDRD
for-
mula)
7645
6861
6359
6766
7373
750.16
(mL
/m
in/
1.73
m2)
(±34.7)
(±22.7)
(±28.4)
(±27.3)
(±26.3)
(±28.7)
(±23.7)
(±27.3)
(±12.2)
(±27.9)
(±19.7)
0.16
Potassium
4.21
4.08
4.33
4.11
4.25
4.36
4.24
4.23
3.89
4.32
3.98
(mm
ol/L)
(±0.56)
(±0.93)
(±0.65)
(±0.46)
(±0.57)
(±0.5)
(±0.55)
(±0.61)
(±0.41)
(±0.49)
(±0.47)
0.03
Alkaline
phos-
phatase
84102
8084
94100
8587
336
8077
(µg /
L)
(66-112)
(69-138)
(65-113)
(71-104)
(77-130)
(71-188)
(67-111)
(67-122)
(94-578)
(62-117)
(71-92)
0.03
Total
bilirub
in(µ
mol
/L)
13(9-19)
36(32-36)
14(10-21)
27(15-58.1)
14(10-21)
32(20-40)
17(12-25)
18(12-26)
28(19-83)
13(10-19)
16(10-19)
<0.00001
HDL
1.17
1.14
1.14
0.87
1.07
0.96
1.04
0.98
0.60
1.12
1.05
(mm
ol/L)
(±0.39)
(±0.76)
(±0.34)
(±0.62)
(±0.42)
(±0.37)
(±0.32)
(±0.27)
(±0.07)
(±0.39)
(±0.25)
<0.00001
Album
in(g
/L)
32(±
8.6)
34(±
6.3)
32(±
8.5)
32(±
7.1)
31(±
9.7)
29(±
10)
32(±
8.6)
32(±
8.5)
31(±
2.9)
34(±
8.6)
35(±
10.8)
<0.00001
24172
23172
22553
3324
3226
36ASA
T(U
/L)
(16-35)
(127-208)
(16-35)
(69-341)
(15-31)
(234-1343)
(19-69)
(17-34)
(22-211)
(18-36)
(32-45)
<0.00001
4208
29054
4479
9846
4206
8191
5654
5734
3186
3036
2142
NT-proBNP
2585
20596
2542
6613
2449
4961
2767
2500
3040
1776
1278
(pg /
mL)
--
--
--
--
--
-
( 8186
)( 41
989
)( 86
44
)( 18
122
)( 98
05
)( 13
428
)( 90
91
)( 10
236
)( 33
33
)( 59
40
)( 37
35
)<0.00001
Use
ofbe
ta-blocker
atba
selin
e69
%(450)
80%
(4)
72%
(224)
58%
(18)
76%
(209)
68%
(13)
65%
(124)
72%
(220)
83%
(5)
85%
(600)
100%
(17)
<0.00001
Use
ofACE-inh
ibitor/
ARB
atba
selin
e57
%(374)
60%
(3)
66%
(204)
74%
(23)
59%
(163)
79%
(15)
62%
(118)
63%
(192)
67%
(4)
74%
(517)
82%
(14)
<0.00001
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;eG
FR:estimated
glom
erular
filtrationrate;
HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure
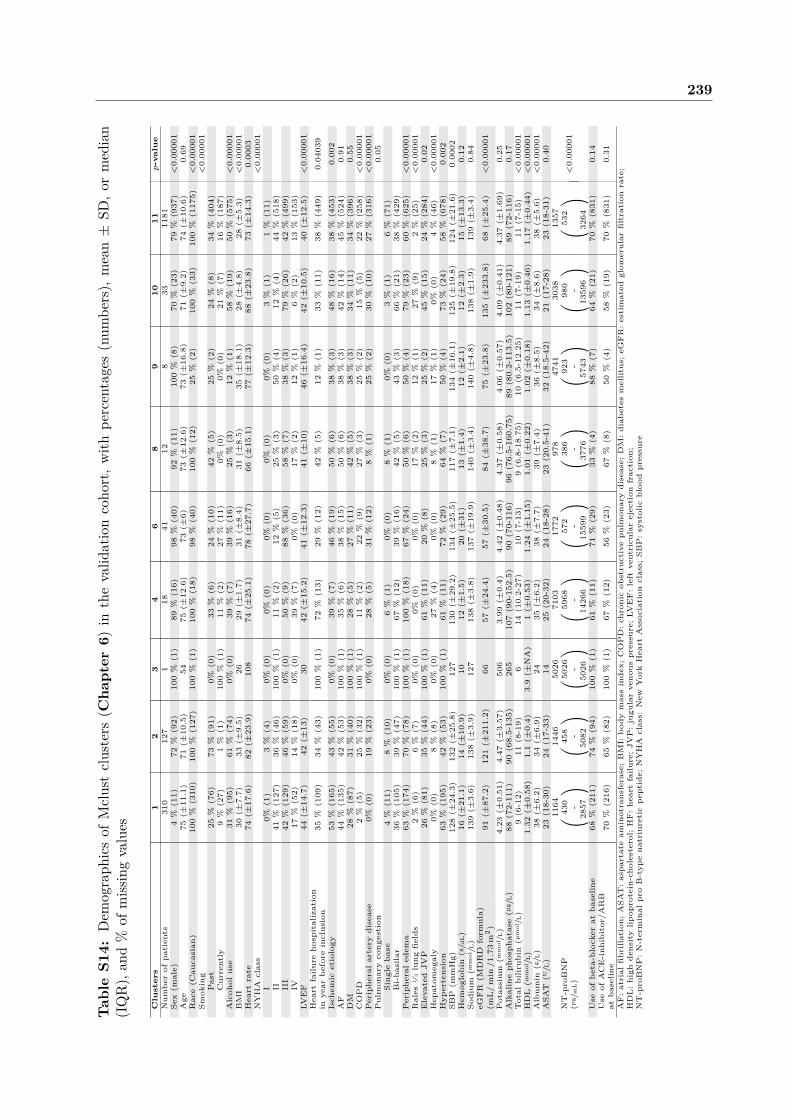
239Ta
ble
S14:
Dem
ogra
phic
sof
Mcl
ust
clus
ters
(Cha
pter
6)in
the
valid
atio
nco
hort
,with
perc
enta
ges
(num
bers
),m
ean
±SD
,or
med
ian
(IQ
R),
and
%of
miss
ing
valu
es
Clu
ster
s1
23
46
89
1011
p-v
alu
eNum
berof
patients
310
127
118
4112
833
1181
Sex(m
ale)
4%
(11)
72%
(92)
100%
(1)
89%
(16)
98%
(40)
92%
(11)
100%
(8)
70%
(23)
79%
(937)
<0.00001
Age
75(±
11.1)
71(±
10.5)
5475
(±12.6)
73(±
6)73
(±12.6)
73(±
16.8)
71(±
9.2)
74(±
10.6)
0.69
Race(C
aucasian
)100%
(310)
100%
(127)
100%
(1)
100%
(18)
98%
(40)
100%
(12)
25%
(2)
100%
(33)
100%
(1175)
<0.00001
Smok
ing
<0.00001
Past
25%
(76)
73%
(91)
0%(0)
33%
(6)
24%
(10)
42%
(5)
25%
(2)
24%
(8)
34%
(404)
Currently
9%
(27)
1%
(1)
100%
(1)
11%
(2)
27%
(11)
0%(0)
0%(0)
21%
(7)
16%
(187)
Alcoh
oluse
31%
(95)
61%
(74)
0%(0)
39%
(7)
39%
(16)
25%
(3)
12%
(1)
58%
(19)
50%
(575)
<0.00001
BMI
30(±
7.7)
33(±
9.5)
2629
(±1.7)
31(±
8.4)
31(±
8.5)
35(±
18.1)
28(±
4.8)
28(±
5.3)
<0.00001
Heart
rate
74(±
17.6)
82(±
23.9)
108
74(±
25.1)
78(±
27.7)
66(±
15.1)
77(±
12.3)
88(±
23.8)
73(±
14.3)
0.0003
NYHA
class
<0.00001
I0%
(1)
3%
(4)
0%(0)
0%(0)
0%(0)
0%(0)
0%(0)
3%
(1)
1%
(11)
II41
%(127)
36%
(46)
100%
(1)
11%
(2)
12%
(5)
25%
(3)
50%
(4)
12%
(4)
44%
(518)
III
42%
(129)
46%
(59)
0%(0)
50%
(9)
88%
(36)
58%
(7)
38%
(3)
79%
(26)
42%
(499)
IV17
%(52)
14%
(18)
0%(0)
39%
(7)
0%(0)
17%
(2)
12%
(1)
6%
(2)
13%
(153)
LVEF
44(±
14.7)
42(±
13)
3042
(±15.2)
41(±
12.3)
41(±
10)
46(±
16.4)
42(±
10.5)
40(±
12.5)
<0.00001
Heart
failu
reho
spitalization
inyear
before
inclusion
35%
(109)
34%
(43)
100%
(1)
72%
(13)
29%
(12)
42%
(5)
12%
(1)
33%
(11)
38%
(449)
0.04039
Ischem
icetiology
53%
(165)
43%
(55)
0%(0)
39%
(7)
46%
(19)
50%
(6)
38%
(3)
48%
(16)
38%
(453)
0.002
AF
44%
(135)
42%
(53)
100%
(1)
35%
(6)
38%
(15)
50%
(6)
38%
(3)
42%
(14)
45%
(524)
0.91
DM
28%
(87)
31%
(40)
100%
(1)
28%
(5)
27%
(11)
42%
(5)
38%
(3)
34%
(11)
34%
(396)
0.55
COPD
2%
(5)
25%
(32)
100%
(1)
11%
(2)
22%
(9)
27%
(3)
25%
(2)
15%
(5)
22%
(258)
<0.00001
Peripheralartery
disease
0%(0)
19%
(23)
0%(0)
28%
(5)
31%
(12)
8%
(1)
25%
(2)
30%
(10)
27%
(316)
<0.00001
Pulmon
arycong
estion
0.05
Sing
leba
se4%
(11)
8%
(10)
0%(0)
6%
(1)
0%(0)
8%
(1)
0%(0)
3%
(1)
6%
(71)
Bi-ba
silar
36%
(105)
39%
(47)
100%
(1)
67%
(12)
39%
(16)
42%
(5)
43%
(3)
66%
(21)
38%
(429)
Peripheraledem
a63
%(174)
70%
(78)
100%
(1)
100%
(18)
67%
(24)
50%
(6)
50%
(4)
79%
(23)
60%
(625)
<0.00001
Rales
1 ⁄3lung
fields
2%
(6)
6%
(7)
0%(0)
0%(0)
0%(0)
17%
(2)
12%
(1)
27%
(9)
2%
(25)
<0.00001
ElevatedJV
P26
%(81)
35%
(44)
100%
(1)
61%
(11)
20%
(8)
25%
(3)
25%
(2)
45%
(15)
24%
(284)
0.02
Hepatom
egaly
0%(0)
8%
(8)
0%(0)
27%
(4)
0%(0)
8%
(1)
17%
(1)
0%(0)
4%
(46)
<0.00001
Hyp
ertension
63%
(195)
42%
(53)
100%
(1)
61%
(11)
72%
(29)
64%
(7)
50%
(4)
73%
(24)
58%
(678)
0.002
SBP
(mm
Hg)
128(±
24.3)
132(±
25.8)
127
130(±
29.2)
134(±
25.5)
117(±
7.1)
134(±
16.1)
125(±
19.8)
124(±
21.6)
0.0002
Hem
oglobin(g
/dL)
16(±
21.1)
14(±
10.9)
1012
(±1.5)
20(±
31)
13(±
1.4)
12(±
2.1)
12(±
2.3)
15(±
13.3)
0.12
Sodium
(mm
ol/L)
139(±
3.6)
138(±
3.9)
127
138(±
3.8)
137(±
19.9)
140(±
3.4)
140(±
4.8)
138(±
1.9)
139(±
3.4)
0.84
eGFR
(MDRD
form
ula)
(mL
/m
in/
1.73
m2)
91(±
87.2)
121(±
211.2)
6657
(±24.4)
57(±
30.5)
84(±
38.7)
75(±
23.8)
135(±
233.8)
68(±
25.4)
<0.00001
Potassium
(mm
ol/L)
4.23
(±0.51)
4.47
(±3.57)
506
3.99
(±0.4)
4.42
(±0.48)
4.37
(±0.58)
4.06
(±0.57)
4.09
(±0.41)
4.37
(±1.69)
0.25
Alkalineph
osph
atase(µ
g /L)
88(72-111)
90(68.5-135)
265
107(90-152.5)
90(70-116)
96(76.5-160.75)
89(80.2-113.5)
102(80-12
1)89
(72-116)
0.17
Total
bilirub
in(µ
mol
/L)
9(6-12)
11(8-19)
614
(10.2-27)
10(7-13)
9(6.8-18.75)
10(6.5-12.25)
11(7-19)
11(7-15)
<0.00001
HDL(m
mol
/L)
1.32
(±0.58)
1.1(±
0.4)
3.9(±
NA)
1(±
0.53)
1.24
(±1.15)
1.01
(±0.22)
1.02
(±0.18)
1.13
(±0.46)
1.17
(±0.44)
<0.00001
Album
in(g
/L)
38(±
6.2)
34(±
6.9)
2435
(±6.2)
38(±
7.7)
39(±
7.4)
36(±
8.5)
34(±
8.6)
38(±
5.6)
<0.00001
ASA
T(U
/L)
23(18-30)
24(17-33)
1425
(20-32)
24(18-28)
23(20.5-41)
32(18.5-42)
21(17-28)
23(18-31)
0.40
1164
1446
5026
7103
1772
978
4741
3038
1357
NT-proBNP
430
458
5026
5968
572
386
923
980
532
(pg /
mL)
--
--
--
--
( 2857
)( 50
82
)( 50
26
)( 14
266
)( 15
599
)( 37
76
)( 57
43
)( 13
596
)( 32
64
)<0.00001
Use
ofbe
ta-blocker
atba
selin
e68
%(211)
74%
(94)
100%
(1)
61%
(11)
71%
(29)
33%
(4)
88%
(7)
64%
(21)
70%
(831)
0.14
Use
ofACE-inh
ibitor/A
RB
atba
selin
e70
%(216)
65%
(82)
100%
(1)
67%
(12)
56%
(23)
67%
(8)
50%
(4)
58%
(19)
70%
(831)
0.31
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;eG
FR:estimated
glom
erular
filtrationrate;
HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure

240 Supplementary data
Table S15: poLCA demographics (Chapter 6) in the index cohort with percentages (numbers),mean ± SD, or median (IQR), and % of missing values
Clusters 1 2 3 4 p-valueNumber of patients 675 811 440 590Sex (male) 89 % (603) 79 % (641) 20 % (88) 87 % (514) <0.00001Age 74 (±8.6) 68 (±11) 77 (±9.2) 58 (±10) <0.00001Race (caucasian) 100 % (672) 100 % (808) 100 % (438) 97 % (571) 0.00003Smoking <0.00001
Past 63 % (427) 51 % (417) 23 % (102) 46 % (274)Smoking (currently) 6 % (43) 12 % (97) 6 % (28) 31 % (185)Alcohol use 29 % (196) 26 % (207) 14 % (63) 40 % (234) <0.00001BMI 28 (±5.2) 28 (±5.1) 27 (±5.4) 28 (±6.2) 0.98Heart rate 78 (±16.9) 73 (±14) 83 (±20.2) 90 (±22.9) <0.00001NYHA class <0.00001
I 0 % (3) 5 % (36) 1 % (4) 2 % (13)II 12 % (79) 68 % (546) 25 % (104) 25 % (139)III 66 % (435) 27 % (214) 61 % (258) 57 % (321)IV 22 % (142) 0 % (3) 13 % (57) 16 % (92)
LVEF 31 (±10.4) 31 (±8.4) 39 (±12.2) 25 (±8.4) <0.00001HF hospitalizationin year before inclusion 48 % (322) 33 % (264) 21 % (93) 19 % (115) <0.00001Ischemic etiology 73 % (496) 58 % (474) 35 % (155) 39 % (233) <0.00001AF 61 % (415) 39 % (313) 51 % (223) 33 % (192) <0.00001DM 50 % (335) 28 % (227) 33 % (146) 19 % (111) <0.00001COPD 25 % (169) 14 % (115) 13 % (57) 16 % (95) <0.00001Peripheral artery disease 18 % (121) 8 % (66) 9 % (38) 8 % (48) <0.00001Pulmonary congestion <0.00001
Single base 16 % (108) 3 % (20) 18 % (76) 19 % (107)Bi-basilar 61 % (406) 2 % (17) 59 % (257) 52 % (300)
Peripheral edema 71 % (476) 22 % (182) 62 % (274) 55 % (324) <0.00001Rales 1⁄3 lung fields 22 % (111) 36 % (14) 20 % (65) 14 % (58) 0.001Elevated JVP 51 % (255) 9 % (48) 35 % (96) 37 % (155) <0.00001Hepatomegaly 29 % (198) 3 % (22) 7 % (32) 18 % (106) <0.00001Hypertension 71 % (477) 64 % (519) 74 % (327) 42 % (246) <0.00001SBP (mmHg) 121 (±19.7) 126 (±19.4) 133 (±24.5) 121 (±23.4) 0.25Hemoglobin (g/dL) 12 (±1.9) 14 (±1.7) 12 (±1.5) 14 (±1.5) <0.00001Sodium (mmol/L) 138 (±4.8) 140 (±3.1) 140 (±4.3) 139 (±3.5) 0.04EGFR (MDRD formula)(mL/ min /1.73 m2) 48 (±18.2) 74 (±27.7) 82 (±36.2) 82 (±23) <0.00001
Potassium (mmol/L) 4.32 (±0.61) 4.39 (±0.55) 4.04 (±0.48) 4.19 (±0.52) <0.00001Alkaline phosphatase(µg/L) 91 (67-122.5) 79 (62-112) 86 (70.1-118.75) 82 (66-112) 0.003Total bilirubin (µmol/L) 16 (10.4-23.32) 12 (8.7-16.07) 13 (9-19.2) 17 (12-27.6025) <0.00001HDL-cholesterol (mmol/L) 0.97 (±0.33) 1.19 (±0.38) 1.28 (±0.39) 1 (±0.35) <0.00001Albumin (g/L) 29 (±9.1) 35 (±8.5) 30 (±8.4) 34 (±7.7) <0.00001ASAT (U/L) 22 (15-30.45) 23 (17-33) 22 (15-33) 36 (25-58.5) <0.00001NT-proBNP (pg/mL) 7150 (3529-13259) 2682 (1389-4455) 4678 (2621-8391) 4347 (2364-8000) <0.00001Use of beta-blockerat baseline 71 % (481) 83 % (673) 66 % (291) 74 % (439) <0.00001Use of ACE-inhibitor/ARB at baseline 56 % (376) 74 % (598) 54 % (237) 71 % (416) <0.00001
AF: atrial fibrillation; ASAT: aspartate aminotransferase; BMI: body mass index;COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; eGFR: estimated glomerular filtration rate;HDL: high density lipoprotein-cholesterol; HF: heart failure; JVP: jugular venous pressure;LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro B-type natriuretic peptide;NYHA class: New York Heart Association class; SBP: systolic blood pressure

241
Table S16: Demographics of poLCA clusters (Chapter 6) in the validation cohort, with per-centages (numbers), mean ± SD, or median (IQR), and % of missing values
Clusters 1 2 3 4 p-valueNumber of patients 181 1079 268 203Sex (male) 90 % (163) 71 % (768) 25 % (66) 70 % (142) <0.00001Age 80 (±7.4) 71 (±11.1) 80 (±7.4) 76 (±8.6) 0.00004Race (Caucasian) 99 % (179) 100 % (1072) 100 % (267) 99 % (200) 0.27Smoking
Past 42 % (76) 37 % (394) 24 % (64) 34 % (68) <0.00001Currently 8 % (15) 15 % (163) 7 % (19) 19 % (39)
Alcohol use 47 % (82) 50 % (532) 30 % (77) 49 % (99) <0.00001BMI 27 (±5.4) 29 (±6.3) 29 (±7) 29 (±6.9) 0.58Heart rate 74 (±15.3) 72 (±15.9) 75 (±17) 82 (±20) <0.00001NYHA class
I 1 % (1) 1 % (15) 0% (0) 0% (1) <0.00001II 11 % (20) 55 % (592) 21 % (56) 21 % (42)III 55 % (100) 38 % (406) 55 % (147) 57 % (115)IV 33 % (60) 6 % (65) 24 % (65) 22 % (45)
LVEF 42 (±13.3) 39 (±12.6) 48 (±12) 42 (±13.2) 0.00009HF hospitalization inyear before inclusion 63 % (114) 30 % (328) 43 % (116) 42 % (86) <0.00001Ischemic etiology 46 % (83) 43 % (467) 41 % (110) 32 % (64) 0.011AF 54 % (97) 40 % (424) 48 % (127) 54 % (109) 0.00001DM 43 % (78) 31 % (338) 30 % (81) 31 % (62) 0.01COPD 26 % (45) 16 % (176) 21 % (55) 20 % (41) 0.02Peripheral artery disease 28 % (49) 20 % (216) 22 % (56) 24 % (48) 0.14Pulmonary congestion
Single base 9 % (15) 5 % (52) 8 % (19) 5 % (9) <0.00001Bi-basilar 70 % (124) 25 % (251) 52 % (132) 66 % (132)
Peripheral edema 87 % (146) 48 % (453) 79 % (194) 86 % (160) <0.00001Rales 1⁄3 lung fields 4 % (8) 3 % (28) 4 % (10) 2 % (4) 0.37JVP 43 % (77) 18 % (195) 29 % (77) 49 % (100) <0.00001Hepatomegaly 9 % (15) 3 % (28) 3 % (8) 5 % (9) 0.002Hypertension 62 % (111) 54 % (580) 76 % (202) 54 % (109) <0.00001SBP (mmHg) 119 (±22.2) 127 (±22.2) 130 (±22.8) 123 (±23.3) 0.10Hemoglobin (g/dL) 12 (±2) 16 (±18.8) 13 (±6.6) 13 (±2) 0.07Sodium (mmol/L) 138 (±3.9) 139 (±5.1) 139 (±3.8) 138 (±3.5) 0.96eGFR (MDRD formula)(mL/ min /1.73 m2) 50 (±19.8) 82 (±98.3) 78 (±32) 74 (±28) 0.14
Potassium (mmol/L) 4.25 (±0.54) 4.94 (±15.47) 4.12 (±0.48) 4.08 (±0.47 0.47Alkaline phosphatase (µg/L) 113 (82-156.5) 85 (69-109) 91 (73.2-115) 101 (82.5-138.5) <0.00001Total bilirubin (µmol/L) 13 (9-20) 10 (7-13) 9 (7-14) 14 (9-21) <0.00001HDL (mmol/L) 0.99 (±0.35) 1.19 (±0.43) 1.33 (±0.45) 1.23 (±0.84) <0.00001Albumin (g/L) 34 (±5.9) 39 (±5.8) 37 (±6) 36 (±5.9) <0.00001ASAT (U/L) 28 (22-43) 22 (16-28) 25 (21-32.5) 28 (23-40) <0.00001NT-proBNP (pg/mL) 5402 (2552-10535) 952 (362-2305) 1916 (717-4627) 2239 (1218-5455) <0.00001Use of beta-blocker at base-line
67 % (121) 74 % (795) 59 % (159) 66 % (134) 0.00003
Use of ACE-inhibitor/ARBat baseline 54 % (97) 76 % (819) 57 % (154) 62 % (126) <0.00001
AF: atrial fibrillation; ASAT: aspartate aminotransferase; BMI: body mass index;COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; eGFR: estimated glomerular filtration rate;HDL: high density lipoprotein-cholesterol; HF: heart failure; JVP: jugular venous pressure;LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro B-type natriuretic peptide;NYHA class: New York Heart Association class; SBP: systolic blood pressure

242 Supplementary dataTa
ble
S17:
Dem
ogra
phic
sof
first
10PA
Mcl
uste
rs(C
hapt
er6)
inth
ein
dex
coho
rt,w
ithpe
rcen
tage
s(n
umbe
rs),
mea
n±
SD,o
rm
edia
n(I
QR
),an
d%
ofm
issin
gva
lues
Clu
ster
s1
23
45
67
89
10p
-val
ue
Num
berof
patients
160
104
29157
82168
276
161
76483
Sex(m
ale)
87%
(139)
63%
(66)
72%
(21)
83%
(131)
55%
(45)
71%
(119)
71%
(195)
88%
(142)
82%
(62)
79%
(382)
<0.00001
Age
72(±
10.8)
68(±
12.9)
64(±
13.6)
65(±
11.1)
67(±
11.8)
70(±
10.6)
68(±
12.2)
64(±
13.1)
57(±
11.5)
71(±
10.5)
0.0002
Race(C
aucasian
)99
%(159)
97%
(101)
100%
(29)
98%
(154)
99%
(81)
99%
(166)
99%
(273)
99%
(160)
100%
(76)
99%
(479)
0.37
Smok
ing
<0.00001
Past
59%
(94)
39%
(41)
34%
(10)
50%
(78)
43%
(35)
45%
(76)
44%
(122)
50%
(81)
51%
(39)
60%
(289)
Currently
9%
(15)
16%
(17)
21%
(6)
20%
(32)
11%
(9)
11%
(18)
13%
(37)
20%
(33)
28%
(21)
10%
(49)
Alcoh
oluse
26%
(42)
25%
(26)
38%
(11)
31%
(48)
13%
(11)
22%
(37)
32%
(88)
39%
(62)
42%
(32)
28%
(137)
0.0001
BMI
27(±
4.4)
27(±
5)26
(±4.6)
28(±
4.4)
28(±
4.8)
28(±
5.5)
26(±
4.5)
29(±
5.6)
30(±
5.4)
29(±
5.2)
0.002
Heart
rate
75(±
15.8)
80(±
19.2)
84(±
22.4)
80(±
23.1)
77(±
17.2)
77(±
16.4)
76(±
16.7)
81(±
22)
80(±
20.5)
76(±
15.1)
<0.00001
NYHA
class
<0.00001
I0%
(0)
55%
(56)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
II18
%(28)
7%
(7)
14%
(4)
75%
(114)
88%
(71)
77%
(124)
95%
(256)
57%
(89)
60%
(43)
9%
(45)
III
75%
(118)
29%
(29)
68%
(19)
25%
(39)
12%
(10)
23%
(38)
5%
(13)
43%
(67)
40%
(29)
90%
(430)
IV7%
(11)
9%
(9)
18%
(5)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
1%
(1)
0%
(0)
0%
(1)
LVEF
32(±
9.9)
34(±
11.5)
26(±
12.3)
31(±
10.8)
30(±
7.3)
33(±
9.2)
30(±
8.7)
29(±
8.5)
29(±
8.5)
30(±
9.2)
0.03
HFho
spitalization
inyear
before
inclusion
45%
(72)
19%
(20)
34%
(10)
19%
(30)
22%
(18)
31%
(52)
24%
(67)
25%
(41)
41%
(31)
39%
(188)
<0.00001
Ischem
icetiology
84%
(135)
33%
(34)
17%
(5)
64%
(101)
37%
(30)
48%
(80)
42%
(115)
31%
(50)
43%
(33)
92%
(445)
<0.00001
AF
49%
(78)
36%
(37)
52%
(15)
34%
(54)
38%
(31)
43%
(72)
40%
(111)
43%
(69)
22%
(17)
48%
(230)
<0.00001
DM
55%
(88)
35%
(36)
21%
(6)
21%
(33)
16%
(13)
29%
(48)
9%
(25)
14%
(22)
22%
(17)
50%
(242)
<0.00001
COPD
19%
(30)
11%
(11)
14%
(4)
7%
(11)
6%
(5)
20%
(34)
9%
(24)
19%
(31)
9%
(7)
19%
(92)
<0.00001
Peripheralartery
Ddisease
50%
(80)
6%
(6)
3%
(1)
15%
(23)
4%
(3)
1%
(1)
3%
(7)
1%
(2)
4%
(3)
15%
(73)
<0.00001
Pulmon
arycong
estion
<0.00001
Sing
leba
se21
%(32)
10%
(10)
7%
(2)
9%
(14)
6%
(5)
7%
(11)
11%
(28)
5%
(8)
3%
(2)
14%
(65)
Bi-ba
silar
48%
(74)
35%
(36)
59%
(17)
20%
(30)
26%
(21)
13%
(22)
24%
(62)
17%
(26)
22%
(16)
46%
(216)
Peripheraledem
a68
%(108)
41%
(43)
66%
(19)
32%
(50)
29%
(24)
27%
(45)
26%
(72)
34%
(54)
36%
(27)
55%
(267)
<0.00001
Rales
1 ⁄3lung
fields
22%
(23)
27%
(12)
21%
(4)
9%
(4)
12%
(3)
24%
(8)
13%
(12)
17%
(6)
11%
(2)
18%
(50)
0.03
JVP
42%
(50)
35%
(22)
37%
(7)
20%
(22)
4%
(2)
10%
(11)
18%
(33)
21%
(26)
13%
(7)
32%
(110)
<0.00001
Hepatom
egaly
25%
(40)
8%
(8)
17%
(5)
6%
(9)
2%
(2)
2%
(4)
4%
(11)
7%
(11)
11%
(8)
13%
(64)
<0.00001
Hyp
ertension
74%
(118)
60%
(62)
55%
(16)
66%
(104)
67%
(55)
71%
(120)
50%
(137)
53%
(86)
61%
(46)
71%
(344)
<0.00001
SBP
(mm
Hg)
122(±
19.1)
129(±
24.5)
123(±
25.1)
126(±
21.2)
130(±
20.6)
129(±
20.2)
121(±
18.2)
130(±
22.5)
123(±
18.9)
122(±
19.4)
0.23
Hem
oglobin(g
/dL)
12(±
1.9)
13(±
1.9)
13(±
2.1)
14(±
1.8)
14(±
1.5)
13(±
1.8)
13(±
1.6)
14(±
1.5)
14(±
1.9)
13(±
1.9)
0.70
Sodium
(mm
ol/L)
138(±
5.6)
139(±
4.2)
138(±
5.8)
139(±
3.6)
140(±
3.4)
140(±
3.2)
140(±
3.1)
140(±
3)139(±
3.3)
139(±
4)0.52
eGFR
(MDRD
form
ula)
(mL
/m
in/
1.73
m2)
46(±
20.4)
80(±
50.7)
50(±
27.6)
78(±
27.4)
88(±
29.3)
76(±
28.6)
79(±
28.3)
74(±
25.2)
90(±
26.5)
65(±
24.1)
0.06
Potassium
(mm
ol/L)
4.44
(±0.73)
4.25
(±0.52)
4.47
(±0.49)
4.33
(±0.5)
4.25
(±0.55)
4.38
(±0.55)
4.31
(±0.48)
4.45
(±0.59)
4.28
(±0.45)
4.27
(±0.54)
<0.00001
104
7997
8479
7682
7674
83Alkalineph
osph
atase(µ
g /L)
(82-142)
(64-126)
(71-142)
(64-108)
(63-130)
(62-111)
(66-109)
(59-108)
(62-116)
(67-111)
0.0003
Total
bilirub
in(µ
mol
/L)
15(10-22)
13(10-21)
32(17-50)
14(10-19)
11(9-17)
13(9-17)
12(9-18)
12(10-19)
14(10-18)
14(10-20)
<0.00001
HDL(m
mol
/L)
0.98
(±0.32)
1.27
(±0.67)
0.83
(±0.39)
1.14
(±0.37)
1.26
(±0.33)
1.15
(±0.36)
1.27
(±0.39)
1.03
(±0.27)
0.99
(±0.25)
1.05
(±0.35)
<0.00001
Album
in(g
/L)
29(±
9.2)
33(±
8.4)
29(±
9.2)
35(±
8.3)
35(±
9)34
(±8.6)
34(±
8.9)
34(±
8.1)
35(±
7.9)
33(±
8.2)
<0.00001
2323
497
3024
2225
2833
23ASA
T(U
/L)
(16-32)
(17-32)
(24-1336)
(22-41)
(16-35)
(15-34)
(17-42)
(20-44)
(24-46)
(16-34)
7408
4820
35000
3661
3198
3181
3136
2874
3448
3975
NT-proBNP
3092
2451
8384
2240
2494
1836
1620
1247
1744
2439
(pg /
mL)
--
--
--
--
--
( 16214)
( 7542
)( 59
882)
( 5670
)( 54
24
)( 53
38
)( 57
85
)( 57
18
)( 51
56
)( 78
37
)<0.00001
Use
ofbe
ta-blocker
atba
selin
e74
%(119)
77%
(80)
62%
(18)
85%
(134)
88%
(72)
74%
(124)
78%
(216)
78%
(125)
88%
(67)
77%
(371)
<0.00001
Use
ofACE-inh
ibitor/A
RB
atba
selin
e51
%(81)
63%
(66)
62%
(18)
73%
(115)
84%
(69)
65%
(109)
66%
(181)
77%
(124)
76%
(58)
65%
(313)
<0.00001
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;
eGFR:estimated
glom
erular
filtrationrate;HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure

243Ta
ble
S18:
Dem
ogra
phic
sofs
econ
d10
PAM
clus
ters
(Cha
pter
6)in
the
inde
xco
hort
,with
perc
enta
ges(
num
bers
),m
ean
±SD
,orm
edia
n(I
QR
),an
d%
ofm
issin
gva
lues
1112
1314
1516
1718
1920
p-v
alu
eNum
berof
patients
103
52107
9471
95141
6773
17Sex(m
ale)
81%
(83)
77%
(40)
77%
(82)
72%
(68)
63%
(45)
81%
(77)
55%
(77)
27%
(18)
60%
(44)
59%
(10)
<0.00001
Age
73(±
9.4)
73(±
8.9)
73(±
11.1)
72(±
10.9)
68(±
13.1)
64(±
13.8)
70(±
12)
73(±
11.7)
73(±
9.9)
69(±
13.6)
0.0002
Race(C
aucasian
)100%
(103)
98%
(51)
98%
(105)
97%
(91)
99%
(70)
98%
(93)
100%
(141)
100%
(67)
100%
(73)
100%
(17)
0.37
Smok
ing
<0.00001
Past
45%
(46)
42%
(22)
54%
(58)
44%
(41)
51%
(36)
42%
(40)
38%
(54)
48%
(32)
27%
(20)
35%
(6)
Currently
6%
(6)
10%
(5)
15%
(16)
12%
(11)
11%
(8)
22%
(21)
23%
(32)
12%
(8)
11%
(8)
6%
(1)
Alcoh
oluse
27%
(28)
27%
(14)
30%
(32)
15%
(14)
34%
(24)
31%
(29)
22%
(31)
16%
(11)
26%
(19)
24%
(4)
0.0001
BMI
27(±
4.2)
28(±
5.2)
27(±
6.8)
27(±
4.9)
28(±
5.3)
33(±
9.2)
28(±
5.1)
26(±
5)28
(±6.5)
27(±
4.1)
0.002
Heart
rate
77(±
14.2)
79(±
15.7)
80(±
18)
81(±
20)
94(±
23)
84(±
19.6)
96(±
26.7)
84(±
19.7)
85(±
21.5)
90(±
19.2)
<0.00001
NYHA
class
<0.00001
I0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
0%
(0)
II21
%(22)
30%
(14)
8%
(8)
6%
(6)
6%
(4)
9%
(9)
5%
(6)
11%
(7)
15%
(11)
0%
(0)
III
79%
(81)
63%
(29)
38%
(38)
28%
(26)
29%
(20)
79%
(75)
33%
(43)
83%
(55)
75%
(53)
100%
(16)
IV0%
(0)
7%
(3)
54%
(54)
66%
(61)
66%
(46)
12%
(11)
62%
(81)
6%
(4)
10%
(7)
0%
(0)
LVEF
32(±
11.2)
33(±
14)
28(±
12)
30(±
10.7)
28(±
10.2)
27(±
9)33
(±13.4)
39(±
11.6)
39(±
14.5)
33(±
12.5)
0.03
HF
hospitalization
inbe
fore
inclusion
48%
(49)
54%
(28)
41%
(44)
48%
(45)
28%
(20)
19%
(18)
26%
(36)
21%
(14)
11%
(8)
18%
(3)
<0.00001
Ischem
icetiology
53%
(55)
63%
(33)
67%
(72)
60%
(56)
37%
(26)
22%
(21)
28%
(39)
21%
(14)
11%
(8)
35%
(6)
<0.00001
AF
64%
(66)
60%
(31)
52%
(56)
50%
(47)
46%
(33)
36%
(34)
57%
(80)
46%
(31)
60%
(44)
41%
(7)
<0.00001
DM
49%
(50)
48%
(25)
39%
(42)
39%
(37)
31%
(22)
27%
(26)
34%
(48)
24%
(16)
26%
(19)
24%
(4)
<0.00001
COPD
30%
(31)
27%
(14)
32%
(34)
24%
(23)
11%
(8)
7%
(7)
26%
(37)
21%
(14)
25%
(18)
6%
(1)
<0.00001
Peripheralartery
disease
2%
(2)
46%
(24)
12%
(13)
16%
(15)
10%
(7)
2%
(2)
8%
(11)
0%
(0)
0%
(0)
0%
(0)
<0.00001
Pulmon
arycong
estion
<0.00001
Sing
leba
se17
%(17)
12%
(6)
15%
(16)
18%
(17)
16%
(11)
22%
(21)
12%
(17)
22%
(14)
14%
(10)
29%
(5)
Bi-ba
silar
47%
(47)
49%
(24)
62%
(65)
70%
(65)
51%
(36)
52%
(49)
69%
(97)
43%
(28)
56%
(40)
53%
(9)
Peripheraledem
a75
%(77)
56%
(29)
71%
(76)
68%
(64)
61%
(43)
72%
(68)
64%
(90)
61%
(41)
64%
(47)
71%
(12)
<0.00001
Rales
1 ⁄3lung
fields
9%
(6)
17%
(5)
29%
(23)
24%
(20)
32%
(15)
14%
(10)
25%
(28)
24%
(10)
10%
(5)
14%
(2)
0.03
JVP
56%
(42)
48%
(16)
59%
(46)
61%
(39)
49%
(22)
36%
(24)
44%
(43)
33%
(16)
27%
(15)
8%
(1)
<0.00001
Hepatom
egaly
65%
(66)
29%
(15)
32%
(34)
34%
(32)
6%
(4)
20%
(19)
10%
(14)
3%
(2)
11%
(8)
12%
(2)
<0.00001
Hyp
ertension
67%
(69)
77%
(40)
56%
(60)
56%
(53)
54%
(38)
45%
(43)
54%
(76)
57%
(38)
73%
(53)
65%
(11)
<0.00001
SBP
(mm
Hg)
122(±
18.2)
125(±
25.5)
118(±
19.7)
123(±
19.7)
129(±
26.8)
120(±
17.9)
130(±
31.4)
132(±
27.4)
132(±
26.7)
133(±
23.3)
0.23
Hem
oglobin(g
/dL)
13(±
2)13
(±1.8)
12(±
2)13
(±2.1)
13(±
1.8)
14(±
1.8)
13(±
1.8)
13(±
1.5)
13(±
1.7)
14(±
2.1)
0.70
Sodium
(mm
ol/L)
139(±
3.3)
140(±
3.4)
137(±
4.9)
138(±
4)139(±
3.6)
138(±
5.3)
139(±
3.3)
140(±
3.7)
139(±
3.9)
137(±
5.4)
0.52
eGFR
(MDRD
form
ula)
(mL
/m
in/
1.73
m2)
59(±
23)
60(±
22.5)
57(±
25.6)
63(±
28.1)
80(±
27.8)
66(±
23.2)
73(±
25.5)
92(±
30.3)
75(±
33.4)
76(±
27.3)
0.06
Potassium
(mm
ol/L)
4.18
(±0.53)
4.24
(±0.55)
4.2(±
0.55)
4.04
(±0.57)
3.97
(±0.59)
4.25
(±0.66)
4.09
(±0.5)
4.06
(±0.49)
4.1(±
0.53)
4.05
(±0.73)
<0.00001
8899
9694
9878
8572
8494
Alkalineph
osph
atase(µ
g /L)
(70-121)
(67-147)
(70-121)
(80-122)
(70-144)
(60-109)
(68-120)
(61-84)
(63-98)
(76-133)
0.0003
Total
bilirub
in(µ
mol
/L)
15(10-23)
20(12-24)
17(12-26)
15(10-28)
16(12-27)
19(14-28)
14(10-24)
13(9-15)
15(9-27)
12(10-26)
<0.00001
HDL(m
mol
/L)
1.07
(±0.32)
1.15
(±0.48)
0.9(±
0.31)
1.01
(±0.4)
1(±
0.25)
0.95
(±0.35)
1.15
(±0.32)
1.33
(±0.42)
1.21
(±0.35)
1.42
(±0.7)
<0.00001
Album
in(g
/L)
31(±
9.4)
28(±
10)
28(±
9)27
(±9.9)
31(±
8.1)
34(±
6.6)
31(±
7.6)
30(±
8.2)
32(±
8.8)
35(±
8.1)
<0.00001
1922
2323
3032
2825
2420
ASA
T(U
/L)
(13-25)
(15-35)
(16-33)
(15-34)
(17-62)
(19-63)
(18-40)
(16-37)
(17-39)
(16-58)
4339
5428
10995
8500
3949
7000
4462
4292
3719
3205
NT-proBNP
2360
3077
6232
4450
2355
3900
2560
2303
2615
2098
(pg /
mL)
--
--
--
--
--
( 8489
)( 12
128)
( 21280)
( 12793)
( 6085
)( 10
781)
( 8118
)( 88
50
)( 64
80
)( 99
98
)<0.00001
Use
ofBeta-blocker
atba
selin
e59
%(61)
69%
(36)
78%
(83)
77%
(72)
61%
(43)
78%
(74)
61%
(86)
72%
(48)
58%
(42)
76%
(13)
<0.00001
Use
ofACE-inh
ibitor/A
RB
atba
selin
e56
%(58)
56%
(29)
57%
(61)
65%
(61)
54%
(38)
74%
(70)
61%
(86)
51%
(34)
60%
(44)
71%
(12)
<0.00001
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;
eGFR:estimated
glom
erular
filtrationrate;HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure

244 Supplementary dataTa
ble
S19:
Dem
ogra
phic
sof
first
10PA
Mcl
uste
rs(C
hapt
er6)
inth
eva
lidat
ion
coho
rt,
with
perc
enta
ges
(num
bers
),m
ean
±SD
,or
med
ian
(IQ
R),
and
%of
miss
ing
valu
es
12
34
56
78
910
p-v
alu
eNum
berof
patients
3551
7564
5183
107
114
123
156
Sex(m
ale)
63%
(22)
55%
(28)
55%
(41)
72%
(46)
39%
(20)
59%
(49)
66%
(71)
69%
(79)
70%
(86)
67%
(105)
0.00005
Age
75(±
9.4)
75(±
9.3)
76(±
10.9)
74(±
9)76
(±9.8)
75(±
10.1)
75(±
9.4)
72(±
9.6)
71(±
10.3)
73(±
11)
0.55
Race(C
aucasian
)100%
(35)
100%
(51)
100%
(75)
100%
(64)
100%
(50)
100%
(83)
100%
(107)
100%
(114)
99%
(122)
100%
(156)
0.69
Smok
ing
0.0002
Past
44%
(15)
31%
(16)
36%
(27)
56%
(36)
33%
(17)
39%
(32)
30%
(32)
31%
(35)
33%
(40)
29%
(46)
Currently
12%
(4)
24%
(12)
15%
(11)
9%
(6)
12%
(6)
5%
(4)
19%
(20)
22%
(25)
10%
(12)
10%
(15)
Alcoh
oluse
44%
(15)
58%
(29)
74%
(55)
71%
(45)
33%
(17)
28%
(23)
46%
(49)
49%
(55)
47%
(57)
47%
(70)
<0.00001
BMI
31(±
8.8)
28(±
6.2)
28(±
6.2)
28(±
5.4)
31(±
8.6)
30(±
6.8)
30(±
6.1)
29(±
5.4)
28(±
5.4)
29(±
5.1)
0.88
Heart
rate
78(±
16.1)
87(±
23.7)
84(±
19.7)
74(±
15.1)
76(±
13.4)
76(±
17.3)
72(±
16.3)
70(±
16.4)
69(±
13.7)
70(±
16.8)
0.02
NYHA
class
<0.00001
I0
00%
(0)
0%(0)
0%(0)
0%(0)
0%(0)
0%(0)
0%(0)
3%
(4)
II20
%(7)
12%
(6)
20%
(15)
53%
(34)
37%
(19)
57%
(47)
30%
(32)
57%
(65)
80%
(98)
68%
(106)
III
57%
(20)
47%
(24)
53%
(40)
34%
(22)
43%
(22)
25%
(21)
68%
(73)
41%
(47)
15%
(18)
19%
(30)
IV23
%(8)
41%
(21)
27%
(20)
12%
(8)
20%
(10)
18%
(15)
2%
(2)
2%
(2)
6%
(7)
10%
(15)
LVEF
44(±
15.6)
44(±
13.5)
46(±
13.4)
37(±
11.6)
43(±
12.9)
43(±
13.2)
42(±
13.8)
36(±
11.5)
41(±
12.2)
41(±
13.8)
0.88
HFho
spitalizationin
before
inclusion
23%
(8)
43%
(22)
41%
(31)
25%
(16)
41%
(21)
66%
(55)
42%
(45)
34%
(39)
25%
(31)
25%
(39)
<0.00001
Ischem
icetiology
49%
(17)
43%
(22)
49%
(37)
38%
(24)
35%
(18)
43%
(36)
49%
(52)
49%
(56)
50%
(61)
43%
(67)
0.04
AF
50%
(17)
47%
(24)
45%
(33)
39%
(25)
41%
(20)
60%
(50)
43%
(46)
47%
(53)
29%
(35)
36%
(56)
0.006
DM
35%
(12)
42%
(21)
15%
(11)
19%
(12)
46%
(23)
41%
(34)
47%
(50)
25%
(28)
24%
(29)
32%
(50)
<0.00001
COPD
18%
(6)
37%
(19)
23%
(17)
31%
(20)
16%
(8)
19%
(15)
21%
(22)
19%
(21)
4%
(5)
7%
(11)
<0.00001
Peripheralartery
disease
21%
(7)
19%
(9)
19%
(14)
28%
(18)
22%
(11)
22%
(18)
30%
(31)
23%
(26)
15%
(17)
17%
(25)
0.37
Pulmon
arycong
estion
<0.00001
Sing
leba
se0%
(0)
6%
(3)
7%
(5)
6%
(4)
10%
(5)
7%
(6)
9%
(9)
7%
(8)
5%
(6)
5%
(7)
Bi-ba
silar
59%
(19)
72%
(36)
57%
(41)
35%
(22)
42%
(21)
46%
(38)
32%
(33)
23%
(25)
19%
(22)
18%
(27)
Peripheraledem
a94
%(29)
83%
(38)
70%
(48)
67%
(40)
74%
(31)
67%
(51)
78%
(77)
53%
(51)
37%
(37)
33%
(46)
<0.00001
Rales
1 ⁄3lung
fields
17%
(6)
0%(0)
1%
(1)
6%
(4)
4%
(2)
2%
(2)
3%
(3)
2%
(2)
2%
(2)
1%
(1)
<0.00001
JVP
23%
(8)
41%
(21)
27%
(20)
39%
(25)
47%
(24)
39%
(32)
20%
(21)
18%
(20)
15%
(19)
16%
(25)
<0.00001
Hepatom
egaly
3%
(1)
2%
(1)
0%(0)
0%(0)
7%
(3)
5%
(4)
1%
(1)
2%
(2)
3%
(3)
3%
(4)
<0.00001
Hyp
ertension
44%
(15)
61%
(30)
57%
(43)
47%
(30)
49%
(25)
57%
(47)
72%
(76)
56%
(64)
60%
(73)
78%
(121)
<0.00001
SBP
(mm
Hg)
121(±
23.8)
129(±
24.2)
133(±
23.4)
123(±
20.7)
117(±
18.5)
119(±
21.7)
131(±
23.7)
131(±
23)
126(±
21.1)
132(±
21.8)
0.11
Hem
oglobin(g
/dL)
16(±
22)
13(±
2.1)
17(±
23.4)
17(±
20.8)
17(±
24.5)
20(±
31.2)
18(±
25.3)
13(±
1.9)
15(±
13.9)
15(±
11.4)
0.005
Sodium
(mm
ol/L)
140(±
2.8)
138(±
4.1)
139(±
3.7)
139(±
3.3)
139(±
2.9)
139(±
3.3)
139(±
3.2)
140(±
3)139(±
3.1)
139(±
3)0.24
eGFR
(MDRD
form
ula)
285
7677
7880
6668
7676
75(m
L/
min
/1.
73m
2)
(±481.4)
(±39)
(±26.9)
(±28.5)
(±39.3)
(±35.5)
(±33.4)
(±29.3)
(±24.4)
(±26.4)
<0.00001
Potassium
(mm
ol/L)
4.16
(±0.6)
4.97
(±5.6)
4.18
(±0.5)
4.19
(±0.4)
4.17
(±0.62)
4.3(±
0.59)
4.35
(±0.49)
4.98
(±5.22)
4.34
(±0.4)
4.35
(±0.49)
0.25
8890
9592
99107
9586
8182
Alkalineph
osph
atase(µ
g /L)
(74-117)
(76-110)
(74-121)
(72-120)
(80-139)
(79-149)
(69-110)
(67-120)
(65-101)
(63-103)
0.00001
Total
bilirub
in(µ
mol
/L)
9(7-13.5)
11(7-17)
11(8-17.5)
11(7.5-16)
9(6-13.5)
11(7-15.5)
11(8-14)
10(7-13)
10(7-14)
9(7-13)
0.16
HDL(m
mol
/L)
1.16
(±0.37)
1.14
(±0.48)
1.23
(±0.4)
1.23
(±0.42)
1.43
(±1.36)
1.26
(±0.51)
1.11
(±0.41)
1.28
(±0.51)
1.24
(±0.43)
1.2(±
0.41)
0.0003
Album
in(g
/L)
35(±
7.1)
35(±
6.6)
36(±
6.2)
37(±
6.9)
37(±
5.9)
37(±
6.6)
38(±
5.8)
39(±
5.9)
40(±
4.7)
40(±
5)<0.00001
2225
2427
2423
2423
2423
ASA
T(U
/L)
(17-36)
(18-40)
(19-30)
(20-36)
(19-34)
(18-32)
(19-28)
(18-30)
(19-31)
(18-28)
2203
2393
1627
1197
1888
1513
1278
1448
1079
819
NT-proBNP
854
888
653
367
762
687
416
419
364
301
(pg /
mL)
--
--
--
--
--
( 4310
)( 71
39
)( 40
30
)( 39
32
)( 38
18
)( 32
02
)( 36
50
)( 29
54
)( 18
94
)( 19
63
)<0.00001
Use
ofbe
ta-blocker
atba
se-
line
71%
(25)
65%
(33)
60%
(45)
77%
(49)
53%
(27)
59%
(49)
74%
(79)
90%
(103)
85%
(105)
65%
(101)
<0.00001
Use
ofACE-inh
ibitor/A
RB
atba
selin
e49
%(17)
49%
(25)
67%
(50)
70%
(45)
63%
(32)
52%
(43)
80%
(86)
89%
(102)
82%
(101)
67%
(105)
<0.00001
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;
eGFR:estimated
glom
erular
filtrationrate;HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure

245Ta
ble
S20:
Dem
ogra
phic
sof
seco
nd10
PAM
clus
ters
(Cha
pter
6)in
the
valid
atio
nco
hort
,with
perc
enta
ges
(num
bers
),m
ean
±SD
,or
med
ian
(IQ
R),
and
%of
miss
ing
valu
es
1112
1314
1516
1718
1920
p-v
alu
eNum
berof
patients
174
7465
8352
77112
6266
107
Sex(m
ale)
74%
(128)
82%
(61)
66%
(43)
69%
(57)
67%
(35)
60%
(46)
59%
(66)
53%
(33)
76%
(50)
68%
(73)
0.00005
Age
71(±
12)
73(±
11.8)
75(±
10.2)
75(±
10.9)
76(±
10.3)
72(±
12)
73(±
11.3)
73(±
11.9)
75(±
10.1)
76(±
9.7)
0.55
Race(C
aucasian
)97
%(168)
99%
(73)
98%
(64)
100%
(81)
98%
(51)
100%
(77)
100%
(112)
100%
(62)
100%
(66)
100%
(107)
0.69
Smok
ing
0.0002
Past
30%
(53)
41%
(30)
36%
(23)
43%
(36)
38%
(20)
38%
(29)
25%
(27)
33%
(20)
42%
(28)
38%
(40)
Currently
18%
(32)
20%
(15)
9%
(6)
22%
(18)
6%
(3)
14%
(11)
15%
(16)
11%
(7)
8%
(5)
8%
(8)
Alcoh
oluse
31%
(53)
47%
(34)
41%
(26)
52%
(43)
52%
(26)
59%
(45)
28%
(30)
29%
(17)
66%
(43)
56%
(58)
<0.00001
BMI
30(±
7)29
(±5.4)
27(±
5.1)
29(±
5.7)
28(±
6.4)
27(±
6.4)
30(±
7.7)
31(±
7.8)
29(±
6.7)
29(±
6.3)
0.88
Heart
rate
73(±
14)
75(±
14.9)
73(±
15.9)
74(±
16.8)
76(±
17.7)
74(±
15.7)
78(±
19)
70(±
15.3)
75(±
17.1)
74(±
15.6)
0.02
NYHA
class
<0.00001
I3%
(5)
3%
(2)
3%
(2)
0%(0)
0%(0)
0%(0)
0%(0)
0%(0)
3%
(2)
2%
(2)
II34
%(60)
45%
(33)
43%
(28)
33%
(27)
25%
(13)
34%
(26)
15%
(17)
23%
(14)
41%
(27)
34%
(36)
III
32%
(56)
38%
(28)
43%
(28)
51%
(42)
69%
(36)
61%
(47)
55%
(62)
77%
(48)
56%
(37)
63%
(67)
IV30
%(53)
15%
(11)
11%
(7)
17%
(14)
6%
(3)
5%
(4)
29%
(33)
0%(0)
0%(0)
2%
(2)
LVEF
40(±
11.9)
40(±
14.1)
41(±
12.4)
43(±
12.3)
42(±
9.9)
36(±
11.4)
43(±
13.4)
42(±
12.1)
46(±
13.5)
42(±
14.3)
0.88
HFho
spitalizationin
year
before
inclusion
41%
(72)
43%
(32)
38%
(25)
30%
(25)
37%
(19)
45%
(35)
42%
(47)
44%
(27)
41%
(27)
26%
(28)
<0.00001
Ischem
icetiology
37%
(64)
36%
(27)
37%
(24)
39%
(32)
37%
(19)
43%
(33)
28%
(31)
52%
(32)
50%
(33)
36%
(39)
0.04
AF
41%
(71)
44%
(32)
40%
(26)
40%
(33)
45%
(23)
57%
(44)
46%
(52)
55%
(34)
50%
(32)
48%
(51)
0.006
DM
47%
(81)
36%
(27)
40%
(26)
39%
(32)
27%
(14)
21%
(16)
27%
(30)
23%
(14)
30%
(20)
27%
(29)
<0.00001
COPD
23%
(39)
14%
(10)
18%
(12)
44%
(36)
20%
(10)
17%
(13)
20%
(22)
8%
(5)
8%
(5)
20%
(21)
<0.00001
Peripheralartery
disease
21%
(35)
16%
(12)
18%
(12)
25%
(20)
17%
(9)
30%
(22)
25%
(27)
27%
(17)
19%
(12)
26%
(27)
0.37
Pulmon
ary
cong
estion
<0.00001
Sing
leba
se5%
(8)
4%
(3)
13%
(8)
5%
(4)
4%
(2)
1%
(1)
5%
(5)
5%
(3)
2%
(1)
7%
(7)
Bi-ba
silar
26%
(43)
58%
(40)
50%
(31)
44%
(36)
40%
(20)
35%
(24)
52%
(56)
38%
(23)
40%
(25)
56%
(57)
Peripheraledem
a49
%(75)
69%
(46)
47%
(26)
61%
(46)
60%
(28)
67%
(44)
85%
(89)
72%
(39)
60%
(36)
78%
(76)
<0.00001
Rales
1 ⁄3lung
fields
0%(0)
8%
(6)
0%(0)
2%
(2)
2%
(1)
8%
(6)
2%
(2)
0%(0)
2%
(1)
8%
(9)
<0.00001
JVP
20%
(35)
38%
(28)
15%
(10)
13%
(11)
21%
(11)
31%
(24)
31%
(35)
23%
(14)
29%
(19)
44%
(47)
<0.00001
Hepatom
egaly
3%
(4)
3%
(2)
25%
(15)
5%
(4)
6%
(3)
3%
(2)
1%
(1)
7%
(4)
7%
(4)
2%
(2)
<0.00001
Hyp
ertension
58%
(101)
54%
(40)
58%
(37)
68%
(56)
37%
(19)
34%
(26)
55%
(62)
73%
(45)
67%
(44)
45%
(48)
<0.00001
SBP
(mm
Hg)
125(±
23.2)
123(±
25.6)
121(±
18.6)
126(±
23.3)
117(±
19.6)
124(±
20.9)
128(±
22.6)
133(±
25.5)
125(±
18.2)
119(±
20.9)
0.11
Hem
oglobin(g
/dL)
13(±
2.1)
15(±
12.6)
15(±
14.5)
13(±
2)13
(±1.7)
17(±
20.4)
15(±
16)
13(±
1.7)
13(±
1.9)
13(±
2.1)
0.005
Sodium
(mm
ol/L)
138(±
3.8)
137(±
15)
139(±
3.2)
139(±
4)139(±
3.6)
139(±
2.8)
139(±
3.5)
139(±
3.4)
138(±
4.1)
138(±
4.2)
0.24
eGFR
(MDRD
form
ula)
7271
6573
7374
7267
7174
(mL
/m
in/
1.73
m2)
(±35)
(±32.5)
(±25.1)
(±35.9)
(±30.5)
(±28.1)
(±27.3)
(±28)
(±32.5)
(±31.2)
<0.00001
Potassium
(mm
ol/L)
4.29
(±0.47)
4.34
(±0.53)
4.31
(±0.56)
4.28
(±0.43)
4.25
(±0.48)
4.31
(±0.44)
4.18
(±0.48)
12.52(±
64.24)
4.27
(±0.52)
4.26
(±0.48)
0.25
8992
9487
9183
8691
9091
Alkalineph
osph
atase(µ
g /L)
(71-112)
(72-124)
(79-126)
(76-124)
(80-116)
(66-111)
(74-122)
(74-120)
(68-112)
(78-120)
0.00001
Total
bilirub
in(µ
mol
/L)
10(7-14)
11(8-15)
10(8-14)
9(6-16)
11(7.5-13)
10(7-13)
11(8-16)
10(7-15)
11(8-17)
11(8-16)
0.15
HDL(m
mol
/L)
1.04
(±0.29)
1.05
(±0.32)
1.24
(±0.47)
1.24
(±0.41)
1.25
(±0.46)
1.32
(±0.7)
1.2(±
0.43)
1.14
(±0.48)
1.15
(±0.44)
1.17
(±0.52)
0.0003
Album
in(g
/L)
39(±
5.9)
36(±
6.5)
38(±
5.9)
36(±
5.5)
36(±
6)38
(±6.4)
37(±
6.8)
37(±
6.5)
37(±
5.7)
36(±
5.3)
<0.00001
2324
2222
2325
2422
2324
ASA
T(U
/L)
(18-29)
(19-31)
(17-32)
(18-28)
(18-32)
(21-34)
(17-30)
(16-30)
(18-28)
(18-33)
1093
1644
1126
1485
2067
1915
1988
1674
1508
1605
NT-proBNP
522
530
436
556
751
713
562
427
516
729
(pg /
mL)
--
--
--
--
--
( 3477
)( 34
66
)( 41
11
)( 31
56
)( 38
92
)( 46
46
)( 49
23
)( 39
08
)( 47
29
)( 48
11
)<0.00001
Use
ofbe
ta-blocker
atba
selin
e80
%(140)
69%
(51)
66%
(43)
36%
(30)
60%
(31)
70%
(54)
62%
(70)
76%
(47)
76%
(50)
72%
(77)
<0.00001
Use
ofACE-inh
ibitor
/ARB
atba
selin
e74
%(129)
61%
(45)
58%
(38)
43%
(36)
81%
(42)
75%
(58)
71%
(79)
81%
(50)
71%
(47)
62%
(66)
<0.00001
AF:atrial
fibrilla
tion
;ASA
T:aspa
rtateam
inotransferase;BMI:bo
dymassindex;
COPD:chronicob
structivepu
lmon
arydisease;
DM:diab
etes
mellitus;
eGFR:estimated
glom
erular
filtrationrate;HDL:high
densitylip
oprotein-cho
lesterol;HF:heartfailu
re;JV
P:jugu
larveno
uspressure;LV
EF:left
ventricularejection
fraction
;NT-proBNP:N-terminal
proB-typ
ena
triureticpe
ptide;
NYHA
class:
New
YorkHeart
Association
class;
SBP:systolic
bloo
dpressure

246 Supplementary data
Table S21: Demographics of Hclust clustering (Chapter 6) in the index cohort, with percent-ages (numbers), mean ± SD, or median (IQR), and % of missing values
Clusters 1 2 3 4 p-valueNumber of patients 1433 989 80 14Sex (male) 68 % (972) 82 % (810) 69 % (55) 64 % (9) <0.00001Age 68 (±12.7) 71 (±10.3) 71 (±12.5) 60 (±10) <0.00001Race (caucasian) 99 % (1422) 100 % (987) 100 % (80) 0 % (0) <0.00001Smoking <0.00001
Past 41 % (589) 60 % (589) 46 % (37) 36 % (5)Currently 15 % (222) 11 % (111) 18 % (14) 43 % (6)
Alcohol use 30 % (430) 25 % (244) 28 % (22) 29 % (4) 0.04BMI 28 (±5.9) 28 (±4.7) 25 (±4.7) 27 (±8.9) 0.0007Heart rate 83 (±21) 75 (±16) 81 (±19.1) 85 (±19.7) <0.00001NYHA class <0.00001
I 3 % (38) 2 % (17) 1 % (1) 0 % (0)II 38 % (528) 34 % (326) 13 % (10) 33 % (4)III 48 % (663) 53 % (515) 56 % (44) 50 % (6)IV 11 % (156) 12 % (113) 29 % (23) 17 % (2)
LVEF 31 (±11.3) 31 (±9.5) 30 (±9.9) 29 (±11.3) 0.10Heart failure hospitalizationin year before inclusion 27 % (383) 37 % (370) 44 % (35) 43 % (6) <0.00001Ischemic etiology 27 % (383) 93 % (922) 60 % (48) 36 % (5) <0.00001AF 47 % (675) 44 % (431) 42 % (34) 21 % (3) 0.09DM 25 % (363) 44 % (434) 21 % (17) 36 % (5) <0.00001COPD 17 % (246) 18 % (174) 18 % (14) 14 % (2) 0.98Peripheral artery disease 2 % (25) 24 % (242) 8 % (6) 0 % (0) <0.00001Pulmonary congestion 0.005
Single base 12 % (173) 13 % (125) 14 % (11) 14 % (2)Bi-basilar 39 % (550) 39 % (376) 62 % (48) 43 % (6)
Peripheral edema 50 % (723) 47 % (461) 78 % (62) 71 % (10) <0.00001Rales 1⁄3 lung fields 18 % (133) 20 % (101) 22 % (13) 12 % (1) 0.74Elevated JVP 32 % (311) 30 % (211) 47 % (29) 33 % (3) 0.002Hepatomegaly 14 % (199) 14 % (140) 24 % (19) 0 % (0) 0.04Hypertension 57 % (813) 71 % (700) 60 % (48) 57 % (8) <0.00001SBP (mmHg) 126 (±23.3) 123 (±19.6) 123 (±22.7) 121 (±15.5) 0.0004Hemoglobin (g/dL) 13 (±1.9) 13 (±1.9) 12 (±1.9) 14 (±2) <0.00001Sodium (mmol/L) 139 (±3.9) 139 (±3.9) 136 (±6.3) 140 (±3) <0.00001eGFR (MDRD formula)(mL/ min /1.73 m2) 76 (±30.5) 65 (±26) 42 (±26.1) 70 (±24.6) <0.00001
Potassium (mmol/L) 4.24 (±0.57) 4.28 (±0.54) 4.36 (±0.63) 4.11 (±0.43) 0.10Alkaline phosphatase (µg/L) 82 (64-117) 88 (67-116) 98 (71-134) 71 (67-72) 0.03Total bilirubin (µmol/L) 14 (10-21.88) 14 (9.5-20) 20 (11.8-29.19) 14 (10.1-20.19) 0.001HDL-cholesterol (mmol/L) 1.12 (±0.37) 1.08 (±0.39) 0.97 (±0.37) 1.35 (±0.79) 0.05Albumin (g/L) 33 (±8.4) 32 (±9.1) 29 (±9.9) 37 (±9.1) 0.0002ASAT (U/L) 26 (17-41.77) 23 (16-33.5) 25 (15.6-53.5) 31 (15-36) 0.001NT-proBNP 4055 3975 30975 1272(pg/mL) (2303-7391) (2327-8130) (26489-35000) (931-4199) <0.00001
Use of beta-blocker at baseline 72 % (1038) 78 % (771) 79 % (63) 86 % (12) 0.01Use of ACE-inhibitor/ARBat baseline 67 % (957) 62 % (610) 60 % (48) 86 % (12) 0.02
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus;eGFR: estimated glomerular filtration rate; HDL: high density lipoprotein-cholesterol; JVP: jugular venous pressure;LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro B-type natriuretic peptide;NYHA class: New York Heart Association class; SBP: systolic blood pressure

247
Table S22: Demographics of Hclust clusters (Chapter 6) in the validation cohort, with per-centages (numbers), mean ± SD, or median (IQR), and % of missing values
Clusters 1 2 3 4 p-valueNumber of patients 988 712 22 9Sex (male) 63 % (627) 69 % (489) 73 % (16) 78 % (7) 0.11Age 73 (±10.5) 74 (±10.9) 78 (±9.1) 72 (±10.8) 0.05Race (Caucasian) 100 % (985) 100 % (711) 100 % (22) 0% (0) <0.00001Smoking 0.23
Past 34 % (337) 36 % (255) 41 % (9) 11 % (1)Currently 14 % (134) 13 % (95) 27 % (6) 11 % (1)
Alcohol use 49 % (473) 43 % (304) 55 % (11) 22 % (2) 0.03BMI 29 (±6.6) 29 (±6.2) 25 (±4.5) 28 (±4.8) 0.01Heart rate 75 (±17.1) 73 (±16.5) 77 (±16.1) 71 (±12.2) 0.04NYHA class 0.14
I 1 % (9) 1 % (8) 0% (0) 0% (0)II 42 % (418) 40 % (286) 9 % (2) 44 % (4)III 44 % (439) 44 % (310) 68 % (15) 44 % (4)IV 12 % (121) 15 % (108) 23 % (5) 11 % (1)
LVEF 41 (±12.9) 42 (±13.1) 34 (±9.7) 41 (±14.7) 0.63HF hospitalization inyear before inclusion 33 % (328) 42 % (299) 64 % (14) 33 % (3) 0.0001Ischemic etiology 27 % (268) 63 % (446) 36 % (8) 22 % (2) <0.00001AF 44 % (430) 45 % (316) 41 % (9) 22 % (2) 0.57DM 28 % (276) 39 % (276) 9 % (2) 56 % (5) <0.00001COPD 19 % (189) 18 % (126) 5 % (1) 11 % (1) 0.28Peripheral Artery Disease 16 % (156) 30 % (206) 29 % (6) 11 % (1) <0.00001Pulmonarycongestion 0.0007
Single base 5 % (45) 7 % (50) 0% (0) 0% (0)Bi-basilar 40 % (377) 36 % (242) 81 % (17) 38 % (3)
Peripheral edema 63 % (552) 60 % (380) 95 % (19) 22 % (2) 0.005Rales 1⁄3 lung fields 3 % (26) 3 % (23) 5 % (1) 0% (0) 0.80JVP 27 % (269) 24 % (168) 41 % (9) 33 % (3) 0.32Hepatomegaly 4 % (34) 3 % (21) 24 % (4) 12 % (1) 0.0002Hypertension 57 % (562) 60 % (423) 59 % (13) 44 % (4) 0.61SBP (mmHg) 126 (±22.5) 126 (±22.6) 123 (±27.7) 128 (±30.3) 0.87Hemoglobin (g/dL) 16 (±18.9) 14 (±7.9) 13 (±2.7) 12 (±1.8) 0.0007Sodium (mmol/L) 139 (±3.4) 139 (±3.6) 134 (±27.2) 140 (±3.5) 0.004eGFR (MDRD formula)(mL/ min /1.73 m2) 83 (±102.1) 70 (±30.9) 54 (±45.1) 85 (±33.4) 0.002Potassium (mmol/L) 4.82 (±16.09) 4.4 (±2.11) 4.1 (±0.77) 4.17 (±0.58) 0.47Alkaline phosphatase(µg/L) 88 (71-117) 91 (72-115) 116 (75-180) 76 (66-85) 0.09Total bilirubin(µmol/L) 10 (7-15) 10 (7-15) 14 (8.2-31.25) 9 (5-12) 0.14HDL (mmol/L) 1.21 (±0.46) 1.18 (±0.56) 0.95 (±0.35) 0.93 (±0.21) 0.002Albumin (g/L) 38 (±6) 37 (±6) 31 (±7.6) 38 (±5.4) 0.001ASAT (U/L) 24 (19-32) 23 (17-29) 43 (26.2-259.5) 22 (14.8-32.25) 0.00001NT-proBNP (pg/mL) 1295 (462-3080) 1444 (546-4617) 22060 (6932-36814) 1404 (568-4741) <0.00001Use of beta-blockerat baseline 66 % (657) 74 % (528) 73 % (16) 89 % (8) 0.004Use of ACE-inhibitor/ARB at baseline 70 % (696) 69 % (490) 27 % (6) 44 % (4) 0.00008
AF: atrial fibrillation; BMI: body mass index; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus;eGFR: estimated glomerular filtration rate; HDL: high density lipoprotein-cholesterol; JVP: jugular venous pressure;LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro B-type natriuretic peptide;NYHA class: New York Heart Association class; SBP: systolic blood pressure

248 Supplementary data
Table S23: Variables used for indication-bias correction (Chapter 7), with number (percent-age), mean ±SD, or median (IQR)
Description of baseline patient characteristicsN 2174 LaboratoryDemographics eGFR (CKD-EPI) (mL/ min /1.73 m2) 66.7 ± 23.66Sex (Male) 1593 (73%) Hematocrit (%) 40 ± 5.3Age (years) 69 ± 12 Blood urea nitrogen (mmol/L) 11.1 (7.5-17.9)Country NT-proBNP (pg/mL) 4148 (2330-8136)
Netherlands 392 (18%) Hemoglobin (g/L) 13.2 ± 1.90Germany 73 (3%) Sodium (mmol/L) 139.2 ± 3.95France 241 (11%) Potassium (mmol/L) 4.3 ± 0.56Greece 254 (11%) BNP (pg/mL) 667 (365-1281)Italy 263 (12%) Bilirubin (µmol/L) 14 (9.8-20.7)Norway 102 (5%) Total-cholesterol (mmol/L) 4.3 ± 1.33Poland 204 (9%) HDL-cholesterol (mmol/L) 1.1 ± 0.38Serbia 352 (16%) Hepcidin (nmol/L) 6.5 (2.2-16.6)Slovenia 44 (2%) STfR (mg/L) 1.5 (1.16-2.09)Sweden 97 (4%) FT4 (pmol/L) 16 (13.4-10.0)United Kingdom 152 (7%) HbA1c (%) 6.3 (5.79-7.11)
Smoking ASAT (U/L) 25 (16.6-38.0)No 795 (37%) ALAT (U/L) 25 (19-35)Past 1061 (49%) TSH (µU/L) 1.8 (1.15-2.92)Current 318 (15%) Gamma-GT (U/L) 55 (28-108)
Alcohol usage 616 (28%) Alkaline phosphatase (µg/L) 84 (65-117)Body mass index (kg/m2) 28 ± 5.5 TnI (pg/mL) 13 (7.0-28.4)NYHA class ET-1 (pg/mL) 5.3 (4.04-7.14)
I 45 (2%) Bio-ADM (pg/mL) 33.7 (22.6-53.8)II 762 (36%) Proteinuria (pg/dL) 5 (0-20)III 1039 (49%) Troponin (µg/L) 0.04 (0.01-0.10)IV 266 (13%)
Clinical ProfileLeft ventricular ejection fraction (%) 31 ± 11Heart Rate (beats/ min) 80 ± 20Systolic blood pressure (mmHg) 124 ± 22Diastolic blood pressure (mmHg) 75 ± 13Pulmonary congestion
Single base 262 (12%)Bi-basilar 873 (41%)
Peripheral oedema 1069 (49%)Elevated jugular venous pressure 579 (37%)Hepatomegaly 302 (14%)3rd heart tone 215 (100%)Rales >1⁄3 up lung fields 226 (20%)Orthopnea present 754 (35%)Medical HistoryIschemic heart disease 1156 (53%)HF-hospitalizationin year before inclusion 678 (31%)Heart failure duration (years) 8 (3.5-13.3)Diabetes mellitus 701 (32%)Atrial fibrillation 991 (46%)Myocardial infarction 801 (37%)Coronary artery bypass graft 367 (17%)Coronary artery disease 951 (44%)Percutaneous coronary intervention 449 (21%)Stroke 205 (9%)Peripheral arterial disease 240 (11%)COPD 373 (15%)

249
Table S24: Disease domains of all 92 biomarkers measured by Olink®
Biomarker A B C D E F G H I J K L MNAminopeptidase N X XAzurocidin X X X XBleomycin hydrolase XC-C motif chemokine 15 X X XC-C motif chemokine 16 X X XC-C motif chemokine 22 X X XC-C motif chemokine 24 X X X XC-X-C motif chemokine 16 XCadherin-5 XCarboxypeptidase A1 XCarboxypeptidase B XCaspase-3 X X X X XCathepsin D XCathepsin Z X XCD166 antigen X XChitinase-3-like protein 1 X X XChitoriosidase-1 XCollagen alpha-1 (I) chain X X X X X XComplement component C1q receptor X XContactin-1 XCystatin-B XE-selectin X XElafin XEphrin type-B receptor 4 X XEpidermal growth factor receptor X X XEpithelial cell adhesion molecule XFatty acid-binding protein, adipocyte X XGalectin-3 X XGalectin-4 XGranulins XGrowth/differentiation factor 15 XInsulin-like growth factor-binding protein 1 X XInsulin-like growth factor-binding protein 2 XInsulin-like growth factor-binding protein 7 XIntegrin beta-2 X X X XIntercellular adhesion molecule 2 XInterleukin-1 receptor type 1 XInterleukin-1 receptor type 2 XInterleukin-17 receptor A XInterleukin-18 binding protein XInterleukin-2 receptor subunit Alpha X X XInterleukin-6 receptor subunit Alpha X X XJunctional adhesion molecule A XKallikrein-6 X X XLow-density lipoprotein receptor XLympotoxin-beta receptor X XMonocypte chemotactic protein 1 XMatrix metalloproteinase-2 X X X XMatrix metalloproteinase-3 X XMatrix metalloproteinase-9 X XMetalloproteinase inhibitor 4 X X XMonocypte chemotactic protein 1 X X X X X X XMyeloblastin X X XMyeloperoxidase XMyoglobin XN-terminal pro B-type natriuretic peptide XNeurogenic locus notch homolog protein 3 XOsteopontin X XOsteoprotegerin XP-selectin X X X X XParaoxnase XPeptidoglycan recognition protein 1 X XPerlecan X XPlasminogen activator inhibitor 1 X X X X X X XPlatelet endothelial cell adhesion molecule X
TableS24– Continued on next page

250 Supplementary data
TableS24– Continued from previous pageBiomarker A B C D E F G H I J K L MPlatelet-derived growth factor subunit A X X X X X XProprotein convertase subtilisin/kexin type 9 X X XProtein delta homolog 1 XPulmonary surfactant-associated protein D X XResistin XRetinoic acid receptor responder protein 2 X X X X
Scavenger receptor cysteine-rich type 1 protein m130 XSecretoglobin family 3A member 2 XSpondin-1 X
XTartrate-resistant acid phosphatase type 5 X XTissue factor pathway inhibitor X XTissue-type plasminogen activator X X X XTrassferrin receptor protein 1 X XTrefoil factor 3 XTrem-like transcript 2 protein XTumor necrosis factor ligand superfamily member 13B XTumor necrosis factor receptor 1 XTumor necrosis factor receptor 2 X X X XTumor necrosis factor receptor superfamily member10C
X
Tumor necrosis factor receptor superfamily member 14 X X XTumor necrosis factor receptor superfamily member 6 X X X X X XTyrosine-protein kinase receptor UFO X X X X XTyrosine-protein phosphatase non-receptor type sub-strate 1
X
Urokinase plasminogen activator surface receptor X X XUrokinase-type plasminogen activator X X X X X X XVon Willebrand factor X X X XA: Wound healing; B: Response to peptide hormone; C: Hypoxia; D: Proteolysis; E: Platelet activation;F: MAPK cascade; G: Inflammation; H: Coagulation; I: Chemotaxis; J: Cell adhesion;K: Angiogenesis/blood vessel morphogenesis; L: Catabolic process; M: Other

251Ta
ble
S25:
Biom
arke
rsva
lues
for
each
endo
type
inth
ein
dex
coho
rt,w
ithm
edia
n(I
QR
)
End
otyp
es1
23
45
67
8p-v
alue
N39
130
221
433
823
418
142
391
AP-N
4.2
3.9
4.4
4.1
4.8
4.0
4.3
4.2
<0.00
1(3.9-4.6)
(3.4-4.4)
(4.0-4.9)
(3.6-4.6)
(4.4-5.3)
(3.5-4.4)
(4.0-4.6)
(3.8-4.7)
1.9
1.5
2.8
1.5
2.2
2.1
1.7
1.8
AZU
1(1.5-2.5)
(1.5-1.8)
(2.0-4.1)
(1.5-1.8)
(1.7-2.8)
(1.5-3.1)
(1.5-2.2)
(1.5-2.2)
<0.00
1
4.5
4.1
4.7
4.1
4.7
4.9
4.5
4.4
BLM
hydrolase
(4.1-4.8)
(3.6-4.5)
(4.3-5.1)
(3.7-4.6)
(4.3-5.1)
(4.5-5.3)
(4.2-4.9)
(3.8-5.1)
<0.00
1
6.4
6.6
6.8
6.1
7.1
6.5
6.5
6.7
CCL1
5(6.0-6.8)
(6.1-7.2)
(6.3-7.2)
(5.7-6.5)
(6.8-7.7)
(5.9-7.0)
(6.0-6.9)
(6.2-7.3)
<0.00
1
CCL1
65.5
5.4
5.5
5.0
5.8
5.4
5.3
5.4
<0.00
1(5.0-6.0)
(4.7-6.0)
(5.0-6.0)
(4.6-5.5)
(5.3-6.2)
(4.9-5.9)
(4.8-5.8)
(4.9-6.1)
1.7
1.2
1.1
1.0
1.4
2.5
1.5
1.4
CCL2
2(1.2-2.3)
(0.7-1.8)
(0.7-1.5)
(0.6-1.5)
(1.0-1.9)
(1.8-3.1)
(1.1-1.9)
(0.9-2.0)
<0.00
1
CCL2
45.0
4.2
5.0
4.6
5.1
4.9
4.8
4.8
<0.00
1(4.3-5.7)
(3.5-5.1)
(4.5-5.8)
(3.8-5.3)
(4.4-5.7)
(4.1-5.6)
(4.3-5.5)
(4.0-5.7)
5.5
5.4
5.8
5.1
6.1
5.4
5.5
5.6
CXCL1
6(5.2-5.8)
(4.9-5.9)
(5.4-6.1)
(4.8-5.5)
(5.7-6.4)
(5.0-5.7)
(5.2-5.9)
(5.2-6.0)
<0.00
1
CDH5
2.7
2.4
2.7
2.4
3.2
2.6
2.9
2.6
<0.00
1(2.4-3.2)
(2.0-3.0)
(2.4-3.2)
(2.0-2.8)
(2.8-3.7)
(2.1-3.0)
(2.5-3.2)
(2.2-3.1)
3.8
3.6
3.4
3.7
4.3
3.5
3.3
3.7
CPA
1(3.3-4.4)
(2.9-4.3)
(2.8-4.0)
(3.1-4.4)
(3.7-5.2)
(3.0-4.3)
(2.8-3.9)
(3.1-4.4)
<0.00
1
CPB1
3.5
3.3
3.2
3.4
4.0
3.3
3.1
3.3
<0.00
1(3.0-4.1)
(2.5-4.1)
(2.6-3.7)
(2.7-4.1)
(3.4-4.7)
(2.7-3.9)
(2.5-3.6)
(2.6-4.0)
6.2
6.4
6.5
5.7
6.1
9.6
7.1
6.5
CASP
-3(5.4-7.0)
(5.2-7.6)
(5.6-7.5)
(4.8-6.8)
(5.4-7.2)
(8.6-10.4)
(6.1-8.3)
(5.3-8.1)
<0.00
1
CTSD
3.2
2.9
3.4
2.9
3.9
3.1
3.1
3.3
<0.00
1(2.8-3.6)
(2.4-3.4)
(2.9-3.8)
(2.5-3.4)
(3.4-4.3)
(2.7-3.6)
(2.7-3.5)
(2.7-3.9)
4.2
4.2
4.3
3.6
4.6
4.0
4.2
4.3
CTSZ
(3.8-4.5)
(3.8-4.7)
(3.9-4.7)
(3.3-4.0)
(4.2-5.0)
(3.5-4.5)
(3.8-4.6)
(3.8-4.6)
<0.00
1
ALC
AM
4.1
3.9
4.3
3.7
4.7
3.9
4.2
4.1
<0.00
1(3.8-4.4)
(3.5-4.4)
(3.9-4.6)
(3.4-4.1)
(4.3-5.0)
(3.5-4.3)
(3.9-4.5)
(3.7-4.6)
5.4
5.9
6.4
5.0
6.4
5.4
5.4
5.8
CHI3L1
(4.7-6.2)
(5.1-6.7)
(5.7-7.2)
(4.3-5.6)
(5.6-7.2)
(4.7-6.3)
(4.6-6.2)
(5.1-6.9)
<0.00
1
CHIT
12.4
2.4
2.3
1.7
2.8
2.6
2.4
-2.6
<0.00
1(1.7-3.0)
(1.6-3.1)
(1.7-3.0)
(0.9-2.3)
(2.0-3.3)
(2.0-3.4)
(1.9-3.2)
(-2.6–
2.6)
1.5
1.6
1.5
1.4
2.2
1.4
1.7
1.7
COL1
A1
(1.1-1.9)
(1.1-2.1)
(1.1-2.0)
(0.9-1.8)
(1.7-2.5)
(1.1-1.8)
(1.3-2.0)
(1.2-2.0)
<0.00
1
CD93
8.8
8.9
9.1
8.5
9.3
8.7
9.0
8.9
<0.00
1(8.4-9.1)
(8.5-9.4)
(8.7-9.4)
(8.1-8.9)
(9.0-9.7)
(8.3-9.2)
(8.6-9.4)
(8.5-9.3)
1.9
1.5
1.9
1.5
2.4
1.7
2.1
1.8
CNTN1
(1.6-2.3)
(1.1-2.0)
(1.4-2.2)
(1.1-1.9)
(1.9-2.7)
(1.3-2.1)
(1.8-2.4)
(1.4-2.2)
<0.00
1
CST
B4.3
4.8
4.8
3.8
5.3
4.6
4.3
4.6
<0.00
1(3.8-4.8)
(4.0-5.4)
(4.3-5.5)
(3.8-4.3)
(4.9-6.0)
(4.0-5.3)
(3.8-4.8)
(3.9-5.2)
TableS
25–
Con
tinue
don
next
page

252 Supplementary dataTa
bleS
25–
Con
tinue
dfr
ompr
evio
uspa
geE
ndot
ypes
12
34
56
78
p-v
alue
1.8
1.3
1.6
1.1
1.9
1.3
1.6
1.5
SELE
(1.2-2.2)
(0.7-1.8)
(1.2-2.1)
(0.7-1.6)
(1.3-2.3)
(0.8-1.8)
(1.1-2.0)
(0.9-2.0)
<0.00
1
PI3
3.0
3.4
3.4
2.5
3.6
3.0
3.0
3.2
<0.00
1(2.5-3.5)
(2.8-4.4)
(2.9-4.2)
(2.5-2.9)
(3.1-4.3)
(2.5-3.7)
(2.5-3.5)
(2.7-3.7)
1.4
1.6
1.7
1.1
2.0
1.4
1.5
1.5
EPHB4
(1.1-1.7)
(1.2-2.1)
(1.4-2.1)
(0.8-1.4)
(1.6-2.3)
(1.1-1.7)
(1.2-1.8)
(1.1-1.9)
<0.00
1
EGFR
0.7
0.3
0.6
0.3
0.8
0.6
0.8
0.5
<0.00
1(0.5-1.0)
(-0.1-0.6)
(0.3-0.9)
(0.0-0.6)
(0.5-1.1)
(0.2-0.8)
(0.5-1.0)
(0.2-0.9)
2.8
2.5
2.7
2.3
3.3
2.7
3.3
2.8
Ep-Cam
(2.3-3.5)
(1.9-3.3)
(2.1-3.3)
(1.8-2.9)
(2.7-4.0)
(2.3-3.5)
(2.6-4.0)
(2.1-3.7)
<0.00
1
FABP4
5.3
5.6
5.5
4.7
6.8
4.8
4.7
5.4
<0.00
1(4.5-6.2)
(4.7-6.5)
(4.7-6.4)
(4.0-5.4)
(6.0-7.6)
(4.2-5.6)
(4.1-5.4)
(4.5-6.4)
2.9
3.0
3.1
2.5
3.6
3.0
3.1
3.0
Gal-4
(2.4-3.4)
(2.3-3.6)
(2.6-3.5)
(2.1-3.0)
(3.1-4.1)
(2.5-3.6)
(2.6-3.5)
(2.5-3.7)
<0.00
1
GRN
3.1
2.9
3.1
2.7
3.5
2.9
3.0
3.1
<0.00
1(2.7-3.3)
(2.4-3.3)
(2.8-3.4)
(2.3-3.1)
(3.2-3.9)
(2.6-3.3)
(2.7-3.3)
(2.7-3.3)
3.3
3.8
3.9
3.7
4.4
2.7
2.9
3.7
GDF-15
(2.7-3.9)
(3.1-4.7)
(3.1-4.7)
(3.0-4.5)
(3.5-5.5)
(2.3-3.4)
(2.4-3.6)
(2.9-4.6)
<0.00
1
IGFB
P-1
3.6
4.5
4.9
4.5
6.3
4.5
5.0
4.5
<0.00
1(2.7-4.4)
(3.6-5.3)
(3.9-5.9)
(3.9-5.2)
(5.6-6.9)
(3.8-5.4)
(4.2-5.6)
(3.6-5.6)
7.2
7.8
8.2
7.4
8.5
7.5
7.6
7.7
IGFB
P-2
(6.6-7.7)
(7.3-8.5)
(7.7-8.7)
(6.9-7.9)
(8.1-9.0)
(6.9-8.1)
(6.9-8.1)
(7.1-8.5)
<0.00
1
IGFB
P-7
3.5
3.4
3.8
3.4
4.7
3.4
3.6
3.7
<0.00
1(3.1-4.0)
(2.9-4.2)
(3.4-4.3)
(2.9-4.0)
(4.1-5.4)
(3.0-4.0)
(3.1-4.0)
(3.2-4.4)
4.6
4.1
4.5
4.0
4.8
4.4
4.6
4.3
ITGB2
(4.2-5.0)
(3.7-4.5)
(4.1-4.9)
(3.5-4.3)
(4.4-5.1)
(4.0-4.8)
(4.2-5.0)
(3.8-4.7)
<0.00
1
ICAM-2
4.2
4.1
4.4
3.9
4.8
4.1
4.3
4.3
<0.00
1(3.9-4.6)
(3.6-4.6)
(4.0-4.8)
(3.6-4.3)
(4.5-5.2)
(3.7-4.6)
(3.9-4.7)
(3.8-4.8)
5.8
5.7
6.0
5.5
6.5
5.6
5.9
5.9
IL-1RT
1(5.5-6.1)
(5.2-6.2)
(5.7-6.5)
(5.2-5.9)
(6.1-6.9)
(5.2-6.1)
(5.5-6.2)
(5.4-6.4)
<0.00
1
IL-1RT
24.2
3.6
4.2
3.8
4.3
3.9
4.1
4.0
<0.00
1(3.8-4.5)
(3.2-4.0)
(3.9-4.7)
(3.4-4.2)
(4.0-4.7)
(3.4-4.2)
(3.8-4.4)
(3.5-4.5)
3.3
3.0
3.4
2.9
3.7
3.6
3.3
3.2
IL-17R
A(2.9-3.6)
(2.4-3.5)
(2.9-3.7)
(2.5-3.2)
(3.2-4.0)
(3.2-4.0)
(2.9-3.7)
(3.0-3.6)
<0.00
1
IL-18B
P5.6
5.8
5.8
5.1
6.2
5.5
5.7
5.7
<0.00
1(5.2-6.0)
(5.3-6.5)
(5.4-6.4)
(4.7-5.5)
(5.8-6.7)
(5.0-6.0)
(5.3-6.1)
(5.3-6.3)
3.5
3.8
4.0
3.1
4.2
3.4
3.6
3.7
IL2-RA
(3.1-3.9)
(3.2-4.4)
(3.5-4.5)
(2.6-3.6)
(3.7-4.7)
(2.9-3.9)
(3.2-4.0)
(3.1-4.2)
<0.00
1
IL6-RA
10.2
9.9
10.2
9.6
10.3
10.5
10.1
10.1
<0.00
1(9.9-10.6)
(9.4-10.3)
(9.8-10.5)
(9.2-10.1)
(9.9-10.6)
(10.0-10
.7)
(9.8-10.5)
(9.9-10.6)
4.2
4.4
4.4
3.8
4.8
7.1
4.5
4.7
JAM-A
(3.7-4.7)
(3.8-5.1)
(3.9-5.0)
(3.3-4.4)
(4.3-5.3)
(6.3-7.8)
(3.9-5.3)
(3.8-5.5)
<0.00
1
KLK
62.5
2.6
2.7
2.4
3.0
2.5
2.7
2.7
<0.00
1(2.4-2.9)
(2.4-3.1)
(2.4-3.1)
(2.4-2.5)
(2.7-3.4)
(2.4-2.9)
(2.4-3.0)
(2.4-2.9)
TableS
25–
Con
tinue
don
next
page

253Ta
bleS
25–
Con
tinue
dfr
ompr
evio
uspa
geE
ndot
ypes
12
34
56
78
p-v
alue
3.4
2.5
3.0
2.4
3.0
3.2
3.2
2.9
LDL-receptor
(2.9-4.0)
(2.1-3.1)
(2.5-3.5)
(1.9-2.8)
(2.6-3.5)
(2.6-3.6)
(2.8-3.7)
(2.3-3.4)
<0.00
1
MEPE
2.2
2.2
2.3
1.7
2.6
2.1
2.3
2.2
<0.00
1(1.8-2.6)
(1.7-2.7)
(1.9-2.7)
(1.3-2.1)
(2.2-3.0)
(1.7-2.6)
(1.9-2.6)
(1.8-2.8)
2.6
2.4
3.0
2.7
3.5
2.5
2.8
2.8
MMP-2
(2.2-3.1)
(1.9-2.9)
(2.6-3.5)
(2.2-3.2)
(3.2-3.9)
(2.1-3.1)
(2.4-3.3)
(2.3-3.4)
<0.00
1
MMP-3
6.5
6.6
7.3
6.4
7.2
6.6
6.7
6.8
<0.00
1(6.0-7.0)
(5.9-7.3)
(6.6-8.2)
(5.8-7.0)
(6.6-7.8)
(6.1-7.2)
(6.1-7.2)
(6.2-7.3)
3.5
2.4
4.0
2.6
3.5
3.2
3.0
2.9
MMP-9
(2.8-4.1)
(1.7-3.0)
(3.3-4.6)
(1.9-3.2)
(2.8-4.1)
(2.6-3.9)
(2.5-3.6)
(2.2-3.6)
<0.00
1
TIM
P4
4.4
4.3
4.7
4.1
5.1
4.6
4.4
4.5
<0.00
1(3.9-4.8)
(3.8-4.9)
(4.3-5.3)
(3.6-4.6)
(4.7-5.6)
(4.1-5.1)
(3.9-4.8)
(4.1-5.0)
6.1
6.2
6.6
5.6
6.8
5.9
6.1
6.2
MB
(5.5-6.6)
(5.6-6.9)
(6.0-7.4)
(5.1-6.2)
(6.3-7.6)
(5.3-6.6)
(5.6-6.6)
(5.6-6.7)
<0.00
1
NOTCH3
3.1
3.0
3.3
3.1
3.9
3.0
3.3
3.1
<0.00
1(2.7-3.5)
(2.5-3.5)
(2.9-3.7)
(2.6-3.4)
(3.5-4.3)
(2.6-3.4)
(2.8-3.6)
(2.7-3.6)
4.7
4.9
5.3
4.5
5.7
4.5
4.7
4.9
OPN
(4.2-5.2)
(4.3-5.5)
(4.8-5.8)
(3.9-5.1)
(5.4-6.1)
(3.9-5.0)
(4.2-5.2)
(4.4-5.5)
<0.00
1
OPG
2.5
2.5
2.9
2.3
3.3
2.5
2.7
2.7
<0.00
1(2.2-2.9)
(2.0-3.0)
(2.5-3.3)
(1.9-2.7)
(2.9-3.8)
(2.0-2.9)
(2.3-3.0)
(2.3-3.1)
8.0
7.8
8.2
7.4
8.3
10.1
8.3
8.1
SELP
(7.6-8.5)
(7.1-8.5)
(7.7-8.7)
(6.9-8.0)
(7.7-8.8)
(9.3-10.8)
(7.8-8.9)
(7.5-8.8)
<0.00
1
PON3
4.4
3.6
4.3
3.6
4.3
4.4
4.8
4.0
<0.00
1(3.8-5.0)
(3.0-4.4)
(3.6-4.9)
(2.9-4.3)
(3.7-4.9)
(3.7-5.0)
(4.3-5.4)
(3.4-4.6)
6.6
6.7
7.0
5.9
7.0
6.6
6.4
6.5
PGLY
RP1
(6.2-7.1)
(6.1-7.2)
(6.6-7.5)
(5.5-6.4)
(6.7-7.5)
(6.2-7.3)
(5.9-6.8)
(6.1-7.1)
<0.00
1
PLC
6.3
6.7
6.6
6.0
7.1
6.5
6.3
6.4
<0.00
1(6.0-6.7)
(6.0-7.1)
(6.1-7.0)
(5.5-6.4)
(6.7-7.5)
(6.0-7.0)
(5.9-6.7)
(6.0-6.9)
5.0
4.3
4.6
4.2
5.5
6.0
5.0
5.0
PAI
(4.3-5.8)
(3.5-5.0)
(3.8-5.5)
(3.6-5.1)
(4.7-6.1)
(5.5-6.6)
(4.2-5.8)
(4.0-5.9)
<0.00
1
PECAM-1
4.1
3.8
4.1
3.8
4.4
6.0
4.3
4.2
<0.00
1(3.7-4.5)
(3.2-4.4)
(3.8-4.6)
(3.3-4.1)
(4.0-4.9)
(5.2-6.8)
(3.8-4.8)
(3.5-4.7)
1.8
1.3
1.4
1.1
1.8
3.4
2.2
1.5
PDGF
(0.9-2.6)
(0.6-2.1)
(0.8-2.3)
(0.5-1.8)
(1.2-2.5)
(2.7-4.0)
(1.4-2.9)
(0.9-2.5)
<0.00
1
PCSK
91.9
1.6
1.9
1.5
2.0
1.9
1.9
1.8
<0.00
1(1.6-2.3)
(1.2-2.0)
(1.6-2.2)
(1.2-1.8)
(1.6-2.4)
(1.5-2.3)
(1.6-2.2)
(1.4-2.2)
4.1
4.5
4.2
3.5
4.8
3.9
4.3
4.4
DLK
-1(3.7-4.6)
(3.8-5.2)
(3.7-4.8)
(3.1-3.9)
(4.3-5.4)
(3.4-4.4)
(3.8-4.8)
(3.9-4.9)
<0.00
1
PSP
-D2.0
1.8
2.4
1.9
2.3
1.7
2.1
2.1
<0.00
1(1.5-2.6)
(1.1-2.5)
(1.9-3.0)
(1.3-2.4)
(1.7-2.8)
(1.2-2.5)
(1.6-2.7)
(1.4-2.6)
5.9
6.1
6.5
5.4
6.4
6.4
5.8
6.1
RETN
(5.5-6.4)
(5.6-6.6)
(6.0-6.9)
(4.9-5.7)
(6.0-6.8)
(5.8-6.9)
(5.3-6.2)
(5.4-6.5)
<0.00
1
RARRES2
11.1
11.0
11.0
10.5
11.3
11.3
11.1
11.1
<0.00
1(10.8-11
.4)
(10.6-11
.4)
(10.7-11
.3)
(10.2-10
.8)
(10.9-11
.5)
(11.0-11
.6)
(10.7-11
.4)
(10.7-11
.4)
TableS
25–
Con
tinue
don
next
page

254 Supplementary dataTa
bleS
25–
Con
tinue
dfr
ompr
evio
uspa
geE
ndot
ypes
12
34
56
78
p-v
alue
6.8
6.6
7.0
6.4
7.4
6.5
6.8
7.0
CD16
3(6.4-7.2)
(6.1-7.1)
(6.5-7.5)
(5.9-6.9)
(6.9-7.9)
(6.1-7.0)
(6.4-7.2)
(6.3-7.5)
<0.00
1
SCGB3A
21.8
2.0
2.4
1.7
2.9
2.0
2.3
2.4
<0.00
1(1.2-2.3)
(1.4-2.6)
(1.8-3.0)
(1.2-2.3)
(2.4-3.5)
(1.5-2.6)
(1.7-2.9)
(1.7-2.9)
1.5
1.5
1.9
1.4
2.4
1.4
1.6
1.6
SPON1
(1.2-1.9)
(1.1-1.9)
(1.5-2.3)
(1.2-1.8)
(2.0-2.8)
(1.1-1.8)
(1.3-1.9)
(1.3-2.1)
<0.00
1
ST2
6.3
8.4
23.9
14.2
19.9
4.7
4.9
9.8
<0.00
1(3.3-11.8)
(4.0-19.6)
(11.1-47
.5)
(7.7-27.1)
(9.7-36.4)
(2.4-9.5)
(2.4-11.3)
(4.3-21.3)
4.5
4.1
4.4
3.8
4.3
4.4
4.5
4.4
TR-A
P4(4.1-4.9)
(3.6-4.6)
(4.0-4.8)
(3.4-4.1)
(4.0-4.8)
(4.1-4.9)
(4.1-4.9)
(3.8-4.7)
<0.00
1
TFP
I7.8
7.4
8.0
7.3
8.0
7.9
7.9
7.7
<0.00
1(7.4-8.2)
(6.9-7.8)
(7.5-8.3)
(6.8-7.7)
(7.6-8.4)
(7.3-8.2)
(7.4-8.2)
(7.3-8.1)
5.3
4.0
5.0
4.5
5.6
7.0
4.6
5.0
t-PA
(4.5-6.3)
(3.3-4.6)
(4.4-5.7)
(3.8-5.4)
(5.0-6.3)
(5.6-8.1)
(4.1-5.3)
(4.1-5.9)
<0.00
1
TR
5.0
4.8
5.3
4.8
5.6
4.8
4.9
5.1
<0.00
1(4.5-5.4)
(4.3-5.5)
(4.8-5.8)
(4.3-5.4)
(5.2-6.2)
(4.2-5.3)
(4.4-5.5)
(4.5-5.8)
5.0
5.6
5.5
4.7
6.1
5.0
5.0
5.3
TFF
3(4.5-5.4)
(4.8-6.2)
(5.0-6.1)
(4.3-5.1)
(5.6-6.7)
(4.4-5.5)
(4.6-5.5)
(4.7-5.8)
<0.00
1
TLT
-23.5
3.5
3.6
2.8
3.8
3.8
3.6
3.4
<0.00
1(3.1-3.9)
(3.0-4.1)
(3.1-4.0)
(2.4-3.2)
(3.3-4.2)
(3.3-4.2)
(3.3-4.0)
(3.0-3.9)
5.3
5.1
5.5
5.1
5.9
5.1
5.4
5.4
TNFS
F13B
(4.9-5.7)
(4.6-5.7)
(4.9-6.0)
(4.7-5.6)
(5.5-6.4)
(4.6-5.5)
(5.0-5.8)
(4.9-5.9)
<0.00
1
TNF-R1
4.6
5.3
5.2
4.3
5.7
4.5
4.6
4.9
<0.00
1(4.2-5.0)
(4.6-5.9)
(4.7-5.8)
(4.1-4.6)
(5.2-6.2)
(4.1-5.2)
(4.2-5.1)
(4.3-5.4)
4.2
4.7
4.6
3.7
5.1
4.1
4.2
4.5
TNF-R2
(3.8-4.6)
(4.1-5.3)
(4.1-5.3)
(3.3-4.1)
(4.6-5.6)
(3.5-4.7)
(3.8-4.7)
(3.9-4.9)
<0.00
1
5.3
5.3
5.6
4.7
5.6
5.1
5.4
5.3
<0.00
1TNFR
SF10
C(4.9-5.7)
(4.8-5.8)
(5.3-6.1)
(4.2-5.1)
(5.3-6.0)
(4.6-5.6)
(4.9-5.8)
(4.7-5.8)
3.9
4.5
4.4
3.6
4.8
4.5
4.1
4.3
TNFR
SF14
(3.6-4.3)
(4.0-5.1)
(3.9-4.9)
(3.1-3.9)
(4.3-5.3)
(4.0-5.1)
(3.7-4.5)
(3.7-4.7)
<0.00
1
FAS
4.1
4.1
4.3
3.7
4.6
4.3
4.2
4.2
<0.00
1(3.8-4.4)
(3.6-4.6)
(4.0-4.7)
(3.3-4.0)
(4.2-5.0)
(3.8-4.6)
(3.9-4.5)
(3.7-4.6)
7.1
7.0
7.3
6.7
7.7
7.0
7.1
7.1
AXL
(6.7-7.5)
(6.5-7.5)
(6.9-7.7)
(6.3-7.1)
(7.3-8.1)
(6.6-7.3)
(6.8-7.5)
(6.7-7.6)
<0.00
1
SHPS-1
2.9
2.9
3.1
2.5
3.5
2.7
3.0
3.0
<0.00
1(2.5-3.3)
(2.5-3.4)
(2.7-3.5)
(2.1-2.9)
(3.1-4.0)
(2.4-3.3)
(2.6-3.4)
(2.5-3.6)
4.0
4.2
4.4
3.6
4.8
3.9
3.9
4.1
U-PAR
(3.6-4.3)
(3.7-4.7)
(4.0-4.9)
(3.3-4.0)
(4.5-5.2)
(3.5-4.5)
(3.6-4.3)
(3.6-4.7)
<0.00
1
uPA
3.9
3.5
3.8
3.6
4.3
4.1
3.9
3.9
<0.00
1(3.6-4.3)
(3.0-4.0)
(3.4-4.1)
(3.2-4.0)
(4.0-4.7)
(3.7-4.5)
(3.6-4.3)
(3.4-4.3)
6.5
5.3
5.9
5.7
6.2
7.9
5.6
5.8
vWF
(5.7-7.4)
(4.5-6.0)
(5.2-6.9)
(4.9-6.6)
(5.5-7.1)
(6.9-8.6)
(5.0-6.3)
(5.1-6.9)
<0.00
1