a host of problemsgo.medicaleconomics.com/acton/attachment/12262/f-012a/1...ophthalmology times...
TRANSCRIPT

Ophthalmology Times Resident Writer’s Award Program
A Host of Problems
Rohini Rao MD1, Hajirah N Saeed MD1,2, Deborah S. Jacobs, MD1,2,3, Reza Dana, MD, MPH, MSc1,2
1 Department of Ophthalmology, Harvard Medical School, Boston, Massachusetts 2 Division of Cornea and Refractive Surgery, Massachusetts Eye and Ear Infirmary, Boston, Massachusetts 3 BostonSight, Needham MA Corresponding Author: Rohini Rao, MD Massachusetts Eye and Ear Infirmary 243 Charles Street Boston, MA 02114 Telephone: 858.349.1813 Email: [email protected] Financial support: none

Abstract: A 64-year-old male with a history of myelofibrosis-myelodysplasia overlap syndrome treated with a stem cell transplant from an unrelated donor developed intermittent bilateral eye redness, tearing, and mucoid discharge of six weeks duration about 1 year after his transplant. On exam, his visual acuity was at baseline but he was found to have fine telangiectasias along the margins of all four eyelids as well as bilateral superficial punctate keratopathy and corneal filaments. This presentation and time course was consistent with mild ocular graft versus host disease. The patient was treated with lubrication tears, punctual plug placement, and oral doxycycline. Although he responded well initially, his ocular disease proved to be aggressive, leading him down a path of escalating therapy to autologous serum tears, PROSE device, punctal thermal cautery, and increasing topical and systemic immunosuppression. His case highlights the evolution of ocular GVHD and the variety of treatments that are available and often required in the proper management of this complicated process.

History: A 64-year-old man was referred to the cornea service at Massachusetts Eye and Ear (MEE) for evaluation of ocular graft versus host disease (GVHD). He had a past medical history significant for a myelofibrosis-myelodysplasia overlap syndrome, treated with a hematopoietic stem cell transplant (SCT) from an unrelated donor one year prior to this presentation. He had previously experienced GVHD of his skin, with symptoms of a diffuse erythematous rash. Six weeks prior to initial evaluation at MEE, he began experiencing intermittent bilateral eye redness, mucoid discharge, and tearing. His medical history was otherwise significant for hemicolectomy for colon cancer ten years prior. His past ocular history was significant for decreased vision in his left eye with the diagnosis of a tacrolimus-induced non-arteritic anterior ischemic optic neuropathy. His medications included sulfamethoxazole and trimethoprim DS, famciclovir, fluconazole, mycophenolate mofetil, low dose oral prednisone, and tacrolimus. He was not on any ophthalmic medications. Exam: Upon initial presentation, ophthalmic examination revealed a best-corrected visual acuity of 20/20 in the right eye and 20/80 in the left eye. External exam was unremarkable, and motility and intraocular pressure were normal. His pupillary exam revealed a left afferent pupillary defect, noted previously in context of his left optic neuropathy. Anterior segment examination revealed fine telangiectasias along the margins of all four eyelids with bilateral superficial punctate keratopathy inferiorly and bilateral corneal filaments. He was also noted to have 1+ nuclear sclerosis bilaterally. A dilated fundus exam showed trace pallor of the left optic nerve, without edema or cupping. The macula, vessels, and periphery of the retina were all without abnormality. Patient’s Course, Discussion and Diagnosis: Our patient initially presented with signs of dry eye disease and ocular surface irritation 11 months after SCT – hallmarks of ocular GVHD.1,2 He was treated for mild GVHD with silicone punctal plug placement in the bilateral lower puncta, eyelid cleansing, lubrication with artificial tears, and oral doxycycline to help stabilize his oil gland dysfunction.1 In an attempt to reduce local inflammation, he was also placed on cyclosporine 0.05% eye drops, but he was unable to tolerate them secondary to a burning sensation. This treatment plan was promising and he showed signs of improvement on follow-up examination two months later. However, three months later he was found to have worsening of his ocular GVHD, with development of an epithelial erosion superior to the visual axis in the left eye, measuring 2mm by 3mm. The exam also revealed evidence of mild conjunctival chalasis in the right eye which resulted in functional partial occlusion of the lower punctum. Tear break-up time was 3-4 seconds in the right eye, and 0 seconds in the left eye. Given the progression of disease, his treatment was escalated to include the use of autologous serum tears, which are thought to promote lubrication and protect corneal and conjunctival structure with components such as epidermal growth factors and vitamin A.1,3–5 Unfortunately, his disease progression persisted despite this measure.
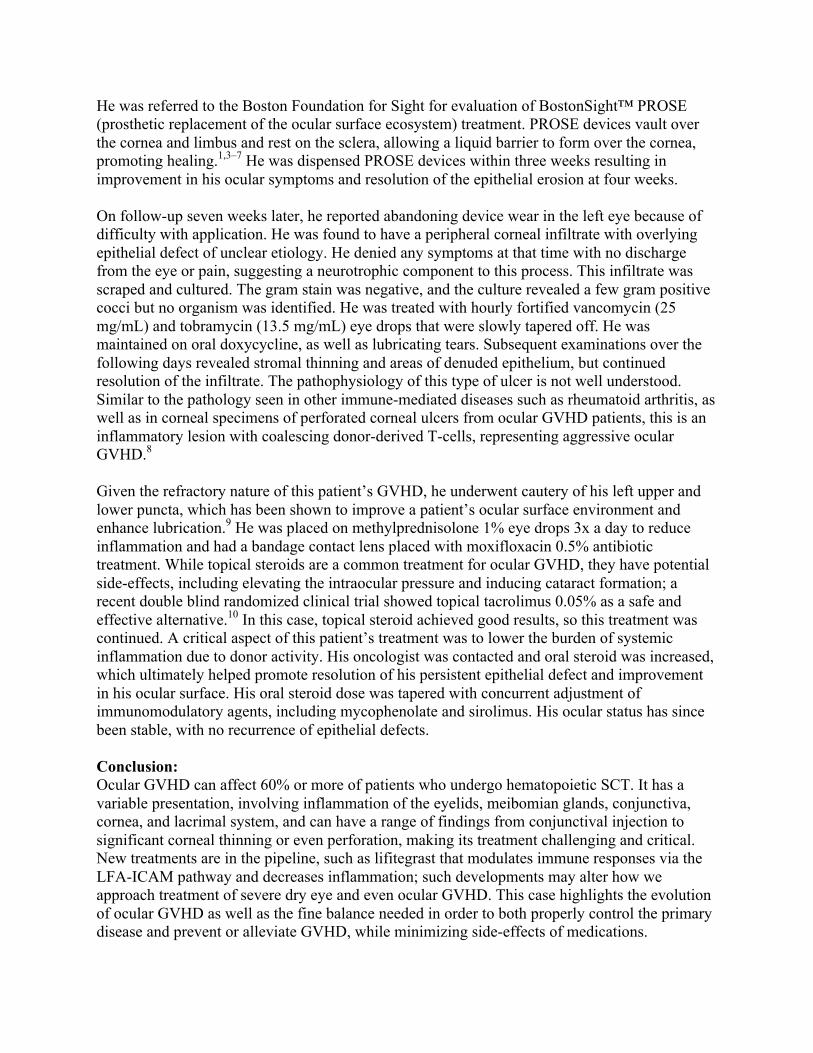
He was referred to the Boston Foundation for Sight for evaluation of BostonSight™ PROSE (prosthetic replacement of the ocular surface ecosystem) treatment. PROSE devices vault over the cornea and limbus and rest on the sclera, allowing a liquid barrier to form over the cornea, promoting healing.1,3–7 He was dispensed PROSE devices within three weeks resulting in improvement in his ocular symptoms and resolution of the epithelial erosion at four weeks. On follow-up seven weeks later, he reported abandoning device wear in the left eye because of difficulty with application. He was found to have a peripheral corneal infiltrate with overlying epithelial defect of unclear etiology. He denied any symptoms at that time with no discharge from the eye or pain, suggesting a neurotrophic component to this process. This infiltrate was scraped and cultured. The gram stain was negative, and the culture revealed a few gram positive cocci but no organism was identified. He was treated with hourly fortified vancomycin (25 mg/mL) and tobramycin (13.5 mg/mL) eye drops that were slowly tapered off. He was maintained on oral doxycycline, as well as lubricating tears. Subsequent examinations over the following days revealed stromal thinning and areas of denuded epithelium, but continued resolution of the infiltrate. The pathophysiology of this type of ulcer is not well understood. Similar to the pathology seen in other immune-mediated diseases such as rheumatoid arthritis, as well as in corneal specimens of perforated corneal ulcers from ocular GVHD patients, this is an inflammatory lesion with coalescing donor-derived T-cells, representing aggressive ocular GVHD.8 Given the refractory nature of this patient’s GVHD, he underwent cautery of his left upper and lower puncta, which has been shown to improve a patient’s ocular surface environment and enhance lubrication.9 He was placed on methylprednisolone 1% eye drops 3x a day to reduce inflammation and had a bandage contact lens placed with moxifloxacin 0.5% antibiotic treatment. While topical steroids are a common treatment for ocular GVHD, they have potential side-effects, including elevating the intraocular pressure and inducing cataract formation; a recent double blind randomized clinical trial showed topical tacrolimus 0.05% as a safe and effective alternative.10 In this case, topical steroid achieved good results, so this treatment was continued. A critical aspect of this patient’s treatment was to lower the burden of systemic inflammation due to donor activity. His oncologist was contacted and oral steroid was increased, which ultimately helped promote resolution of his persistent epithelial defect and improvement in his ocular surface. His oral steroid dose was tapered with concurrent adjustment of immunomodulatory agents, including mycophenolate and sirolimus. His ocular status has since been stable, with no recurrence of epithelial defects. Conclusion: Ocular GVHD can affect 60% or more of patients who undergo hematopoietic SCT. It has a variable presentation, involving inflammation of the eyelids, meibomian glands, conjunctiva, cornea, and lacrimal system, and can have a range of findings from conjunctival injection to significant corneal thinning or even perforation, making its treatment challenging and critical. New treatments are in the pipeline, such as lifitegrast that modulates immune responses via the LFA-ICAM pathway and decreases inflammation; such developments may alter how we approach treatment of severe dry eye and even ocular GVHD. This case highlights the evolution of ocular GVHD as well as the fine balance needed in order to both properly control the primary disease and prevent or alleviate GVHD, while minimizing side-effects of medications.

References: 1. Shikari H, Antin JH, Dana R. Ocular graft-versus-host disease: A review. Surv
Ophthalmol 2013;58(3):233-251. 2. Ogawa Y, Kim SK, Dana R, et al. International Chronic Ocular Graft-vs-Host-Disease
(GVHD) Consensus Group: proposed diagnostic criteria for chronic GVHD (Part I). Sci Rep 2013;3:3419.
3. Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjögren’s syndrome. Br J Ophthalmol 1999;83(4):390-395.
4. Ogawa Y, Okamoto S, Mori T, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Transplant 2003;31(7):579-583.
5. Azari AA, Karadag R, Kanavi MR, et al. Safety and Efficacy of Autologous Serum Eye Drop for Treatment of Dry Eyes in Graft-versus-host Disease. Cutan Ocul Toxicol July 2016:1-20.
6. DeLoss KS, Le H-G, Gire A, Chiu GB, Jacobs DS, Carrasquillo KG. PROSE Treatment for Ocular Chronic Graft-Versus-Host Disease as a Clinical Network Expands. Eye Contact Lens 2015;42(4):262-266.
7. Jacobs DS, Rosenthal P. Boston scleral lens prosthetic device for treatment of severe dry eye in chronic graft-versus-host disease. Cornea 2007;26(10):1195-1199.
8. Stevenson W, Shikari H, Saboo US, Amparo F, Dana R. Bilateral corneal ulceration in ocular graft-versus-host disease Clin Ophthalmol. 2013;7:2153-2158.
9. Yaguchi S, Ogawa Y, Kamoi M, et al. Surgical management of lacrimal punctal cauterization in chronic GVHD-related dry eye with recurrent punctal plug extrusion. Bone Marrow Transplant 2012;47(11):1465-1469.
10. Abud TB, Amparo F, Saboo US, et al. A Clinical Trial Comparing the Safety and Efficacy of Topical Tacrolimus versus Methylprednisolone in Ocular Graft-versus-Host Disease. Ophthalmology 2016;123(7):1449-1457.
A Host of Problems Ophthalmology Times Resident Writer’s Award Program
Rohini Rao, MD Massachusetts Eye and Ear
Harvard Medical School
§ No Financial Disclosures
Chief Complaint• 64 year-old man with intermittent bilateral
eye redness, tearing, and mucoid discharge of six weeks duration
§ Myelofibrosis-myelodysplasia overlap syndrome s/p stem cell transplant from unrelated donor ~1 year prior
§ Colon cancer s/p hemicolectomy 10 years prior
Past Medical History
Past Ocular History§ Tacrolimus-induced non-
arteritic anterior ischemic optic neuropathy
Social History§ Non-smoker/ Non-drinker
Medications§ Sulfamethoxazole &
trimethoprim DM§ Famciclovir§ Fluconazole§ Mycophenolate Mofetil§ Prednisone§ Tacrolimus
Allergies§ No known drug allergies
Family History§ Non-contributory

VA (sc): OD: 20/20OS: 20/80
Pupils: APD OS* IOP: 13/14 EOMs: Full OU CVF: Full OU
Orbits: no resistance to retropulsion
Initial Examination
* Due to presumed NAION in the left eye
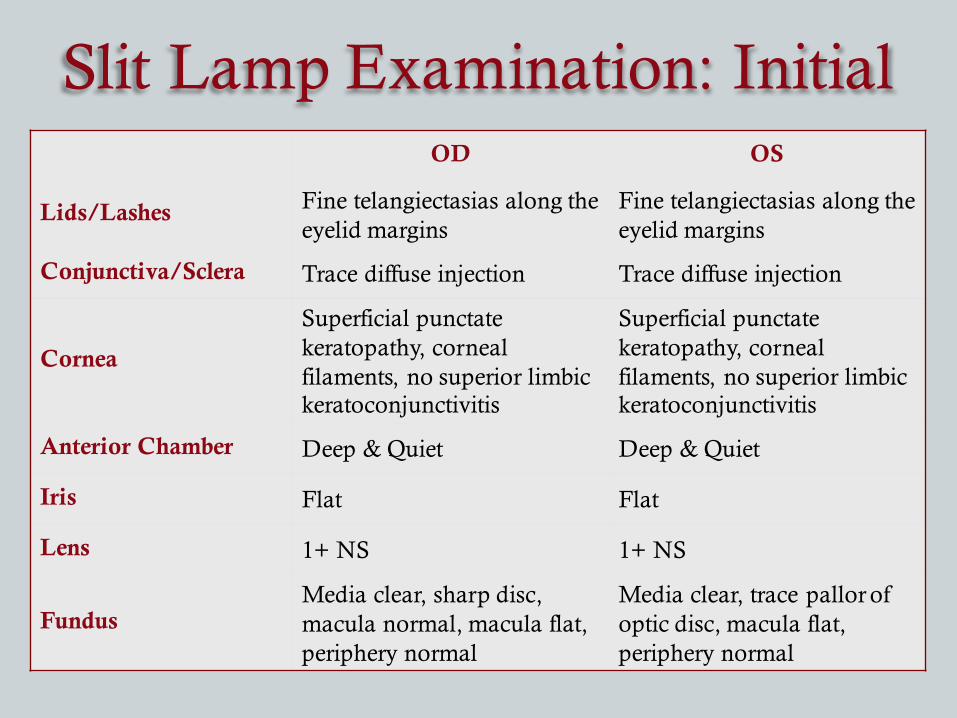
OD OS
Lids/Lashes Fine telangiectasias along the eyelid margins
Fine telangiectasias along the eyelid margins
Conjunctiva/Sclera Trace diffuse injection Trace diffuse injection
Cornea
Superficial punctate keratopathy, corneal filaments, no superior limbic keratoconjunctivitis
Superficial punctate keratopathy, corneal filaments, no superior limbic keratoconjunctivitis
Anterior Chamber Deep & Quiet Deep & Quiet
Iris Flat Flat
Lens 1+ NS 1+ NS
FundusMedia clear, sharp disc, macula normal, macula flat, periphery normal
Media clear, trace pallor of optic disc, macula flat, periphery normal
Slit Lamp Examination: Initial
Differential Diagnosis
Corneal FilamentsSuperficial Punctate Keratitis
• Posterior blepharitis• Lid malposition• Severe dry eye
• Dry eye syndrome• Posterior Blepharitis• Exposure keratitis• Viral conjunctivits
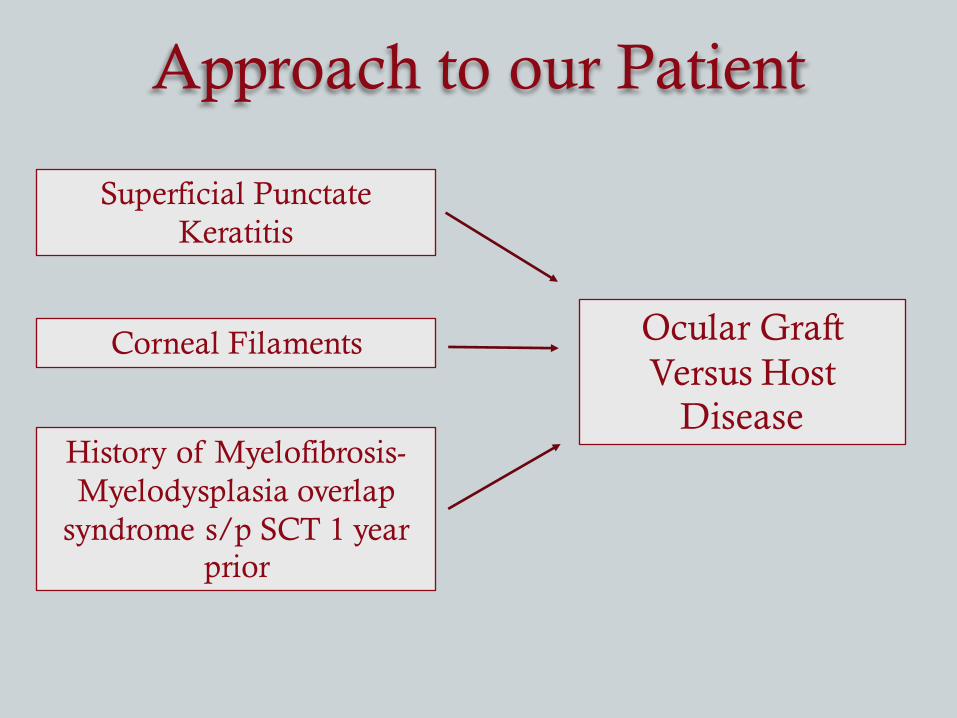
Approach to our Patient
Corneal Filaments
Superficial Punctate Keratitis
History of Myelofibrosis-Myelodysplasia overlap
syndrome s/p SCT 1 year prior
Ocular Graft Versus Host
Disease
Ocular GVHD
• Incidence depends on source of donor tissue, primary disease, host conditioning prior to transplant, histocompatibility• Occurs in at least 40-60% of patients receiving an allo-SCT• 1-2 years after SCT, on average
• T-cell mediated process: Donor lymphocytes attack host antigens à inflammation and scarring
• Limited regenerative capacity: exocrine tissues, such as the lacrimal gland, can lose function indefinitely after inflammation
Ocular GVHD
ChronicAcute
• Cicatricial conjunctival changes
• Meibomian gland dysfunction and atrophy
• Punctate keratopathy• Corneal filaments• Non-healing epithelial
defects and ulcerations• Corneal perforation
Can occur with no other systemic GVHD
• Conjunctival hyperemia• Conjunctival chemosis• Pseudomembranous
conjunctivitis• Corneal epithelial
sloughing• Persistent corneal
epitheliopathy
Severity correlates to primary disease activity
Ocular GVHD: Prophylaxis
Calcineurin inhibitors are commonly used in the prevention of GVHD:
• Cyclosporine• Tacrolimus
Other Immunomodulatory Agents Used:• Mycophenolate• Methotrexate
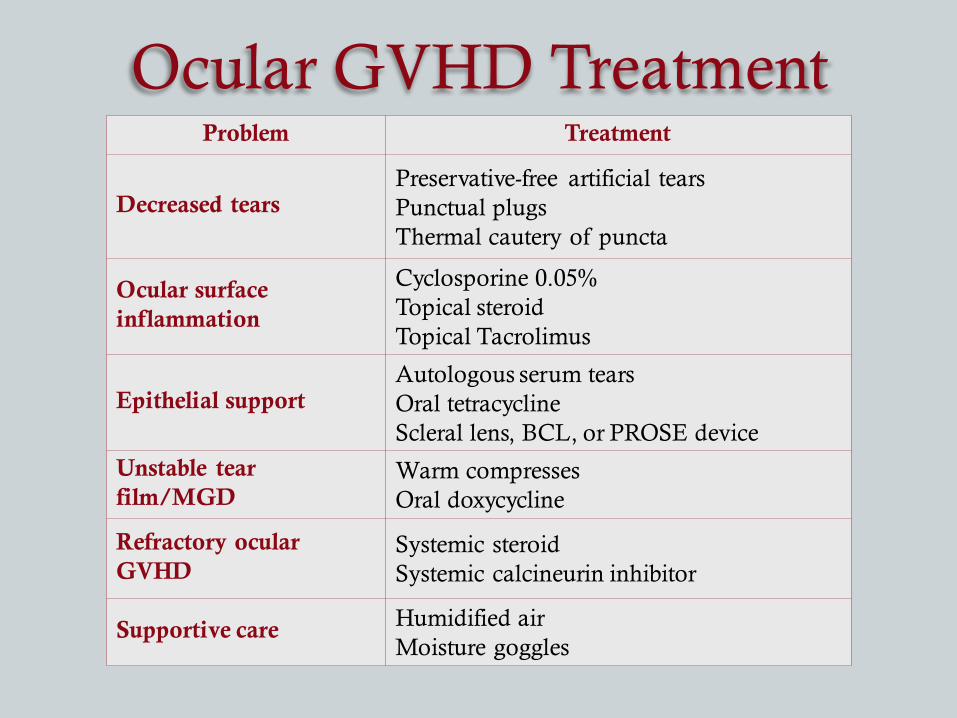
Ocular GVHD TreatmentProblem Treatment
Decreased tearsPreservative-free artificial tearsPunctual plugsThermal cautery of puncta
Ocular surface inflammation
Cyclosporine 0.05%Topical steroidTopical Tacrolimus
Epithelial supportAutologous serum tearsOral tetracyclineScleral lens, BCL, or PROSE device
Unstable tearfilm/MGD
Warm compressesOral doxycycline
Refractory ocularGVHD
Systemic steroidSystemic calcineurin inhibitor
Supportive care Humidified airMoisture goggles
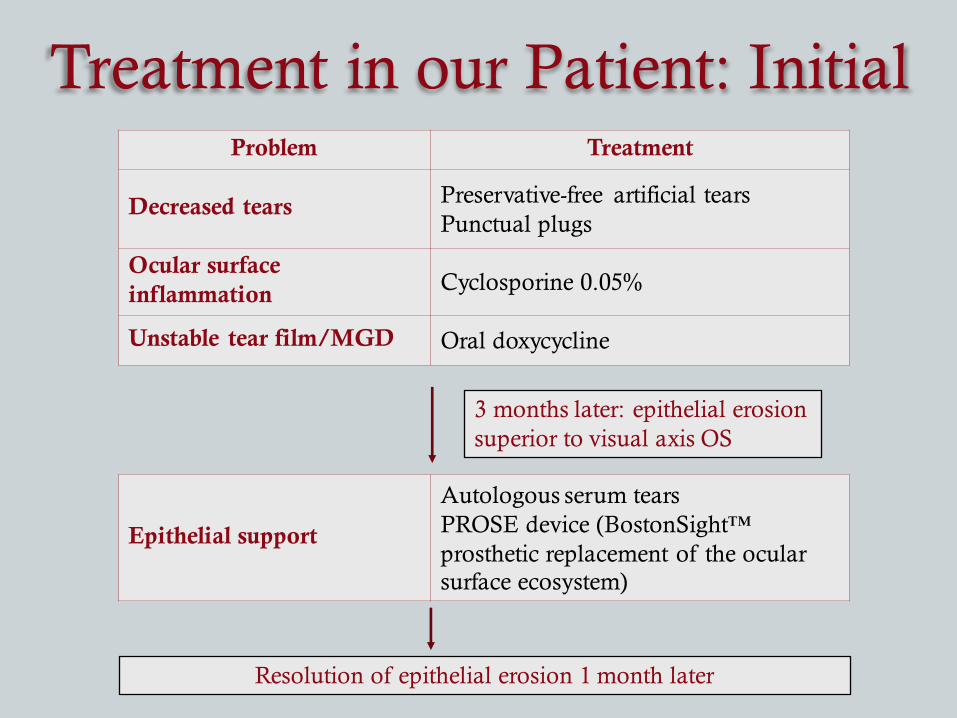
Treatment in our Patient: InitialProblem Treatment
Decreased tears Preservative-free artificial tearsPunctual plugs
Ocular surface inflammation Cyclosporine 0.05%
Unstable tear film/MGD Oral doxycycline
Epithelial support
Autologous serum tearsPROSE device (BostonSight™ prosthetic replacement of the ocular surface ecosystem)
3 months later: epithelial erosion superior to visual axis OS
Resolution of epithelial erosion 1 month later
On routine follow-up exam, with no symptoms…
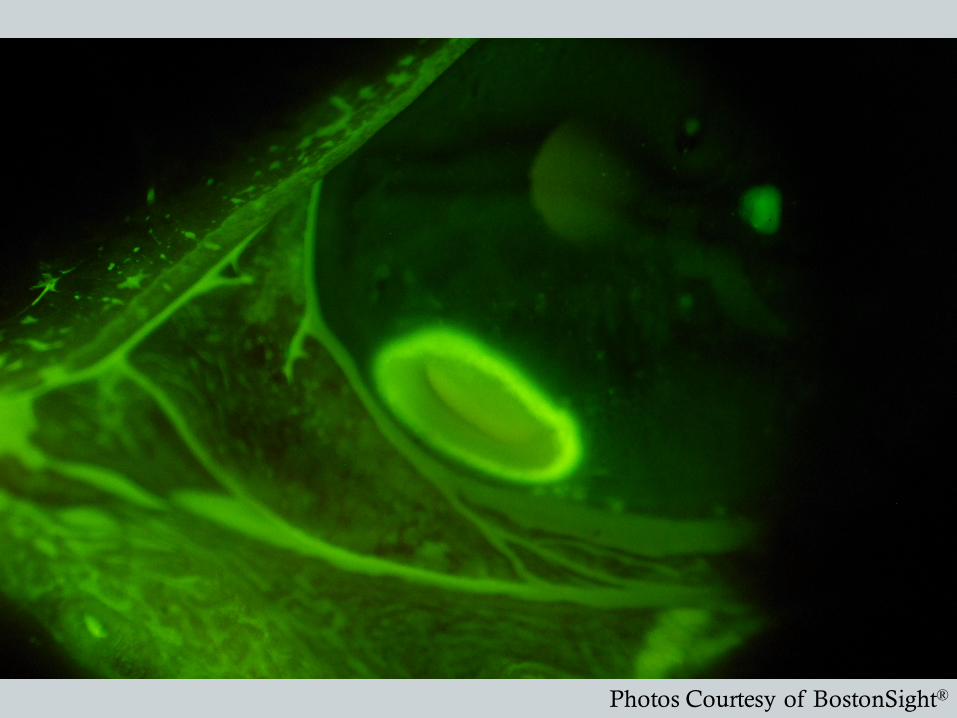
Photos Courtesy of BostonSight®
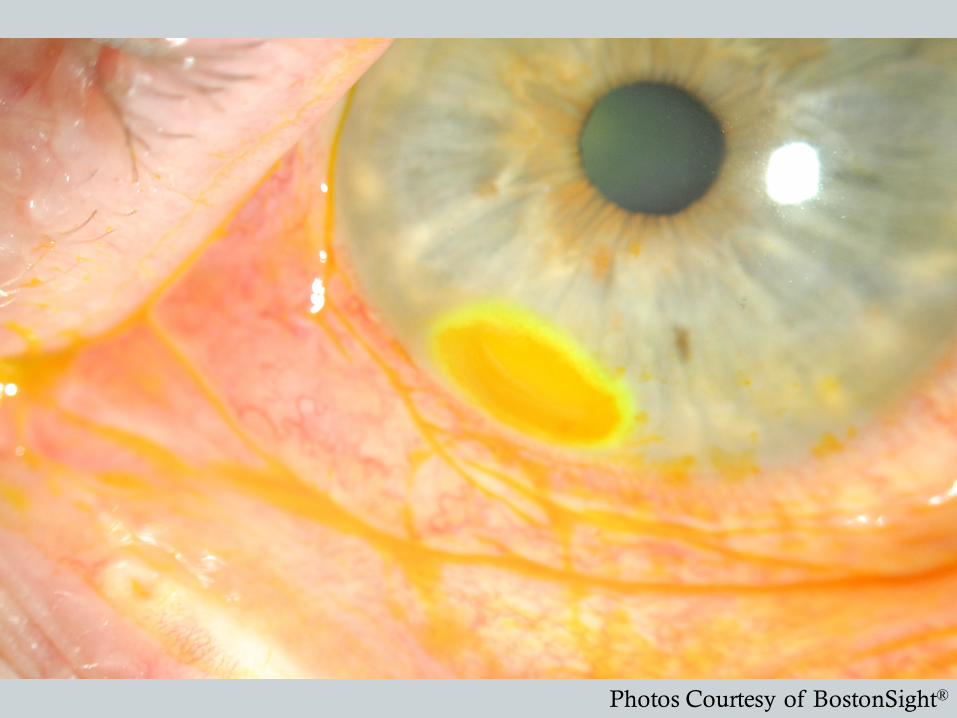
Photos Courtesy of BostonSight®
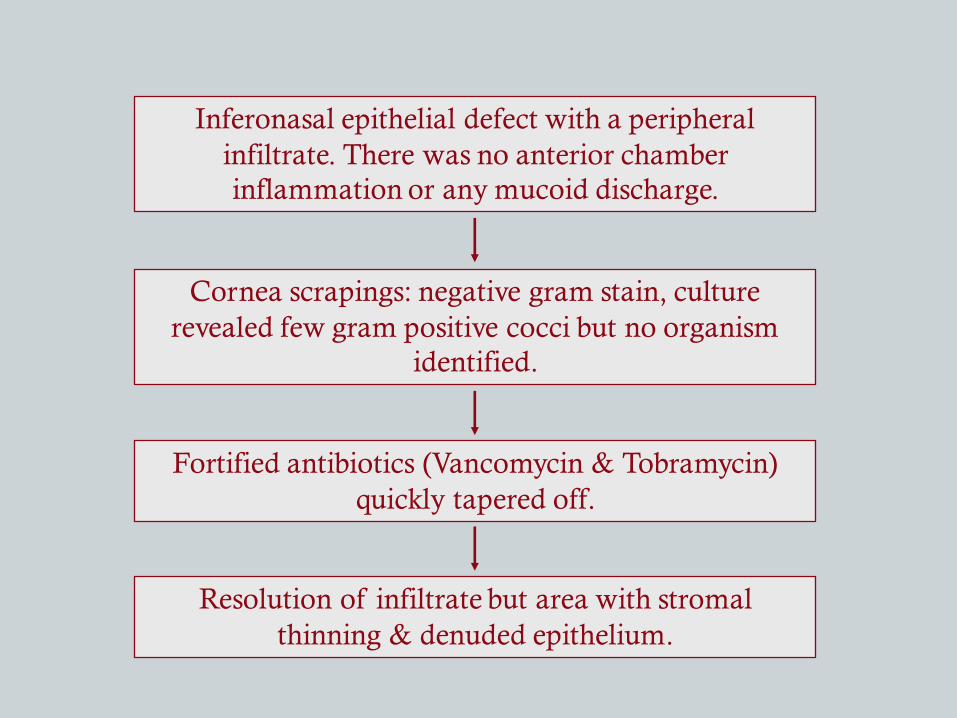
Inferonasal epithelial defect with a peripheral infiltrate. There was no anterior chamber inflammation or any mucoid discharge.
Cornea scrapings: negative gram stain, culture revealed few gram positive cocci but no organism
identified.
Fortified antibiotics (Vancomycin & Tobramycin) quickly tapered off.
Resolution of infiltrate but area with stromal thinning & denuded epithelium.
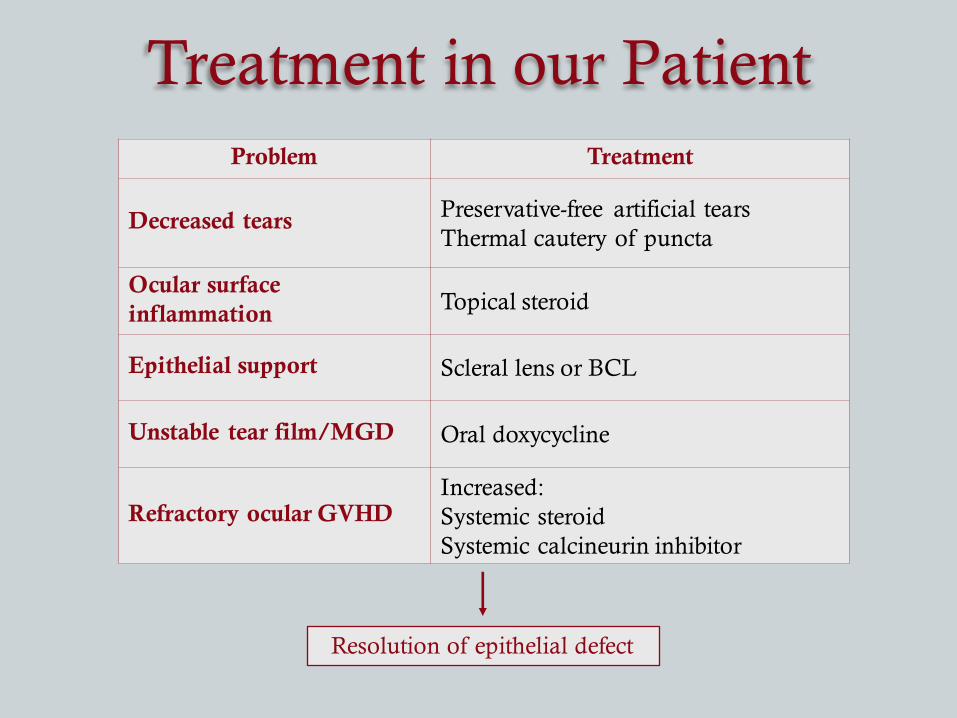
Treatment in our PatientProblem Treatment
Decreased tears Preservative-free artificial tearsThermal cautery of puncta
Ocular surface inflammation Topical steroid
Epithelial support Scleral lens or BCL
Unstable tear film/MGD Oral doxycycline
Refractory ocular GVHDIncreased:Systemic steroidSystemic calcineurin inhibitor
Resolution of epithelial defect
Conclusions• Ocular GVHD can affect up to 60% of patients who undergo
hematopoietic stem cell transplant
• It has a variable presentation, involving inflammation of the eyelids, meibomian glands, conjunctiva, cornea, and lacrimal system
• There are a wide range of findings from tearing and injection to significant corneal thinning or even perforation
• There are many options in treatment of ocular GVHD• New treatments on the horizon may alter how we treat these
patients: lifitegrast – recently FDA approved for dry eye
• A fine balance is needed in order to both properly control the primary disease and prevent or alleviate GVHD, while minimizing side-effects of medications

Acknowledgements
§ Reza Dana, MD, MPH, MScDirector, Cornea and Refractive Surgery Service, Massachusetts Eye and Ear
§ Hajirah N. Saeed, MDFaculty, Cornea Service, Massachusetts Eye and Ear
§ Deborah S. Jacobs, MDMedical Director, BostonSightFaculty, Cornea Service, Massachusetts Eye and Ear
ReferencesShikari H, Antin JH, Dana R. Ocular graft-versus-host disease: A review. Surv Ophthalmol 2013;58(3):233-251. Ogawa Y, Kim SK, Dana R, et al. International Chronic Ocular Graft-vs-Host-Disease (GVHD) Consensus Group: proposed diagnostic criteria for chronic GVHD (Part I). Sci Rep 2013;3:3419. Tsubota K, Goto E, Fujita H, et al. Treatment of dry eye by autologous serum application in Sjögren’s syndrome. Br J Ophthalmol 1999;83(4):390-395. Ogawa Y, Okamoto S, Mori T, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Transplant 2003;31(7):579-583. AzariAA, Karadag R, Kanavi MR, et al. Safety and Efficacy of Autologous Serum Eye Drop for Treatment of Dry Eyes in Graft-versus-host Disease. Cutan Ocul Toxicol July 2016:1-20. DeLoss KS, Le H-G, Gire A, Chiu GB, Jacobs DS, Carrasquillo KG. PROSE Treatment for Ocular Chronic Graft-Versus-Host Disease as a Clinical Network Expands. Eye Contact Lens 2015;42(4):262-266. Jacobs DS, Rosenthal P. Boston scleral lens prosthetic device for treatment of severe dry eye in chronic graft-versus-host disease. Cornea 2007;26(10):1195-1199. Stevenson W, Shikari H, Saboo US, Amparo F, Dana R. Bilateral corneal ulceration in ocular graft-versus-host disease. Clin Ophthalmol 2013;7:2153-2158. Yaguchi S, Ogawa Y, Kamoi M, et al. Surgical management of lacrimal punctal cauterization in chronic GVHD-related dry eye with recurrent punctal plug extrusion. Bone Marrow Transplant 2012;47(11):1465-1469. Abud TB, Amparo F, Saboo US, et al. A Clinical Trial Comparing the Safety and Efficacy of Topical Tacrolimus versus Methylprednisolone in Ocular Graft-versus-Host Disease Ophthalmology. 2016;123(7):1449-1457.