7ds taunton durham&darlington ian briggs
TRANSCRIPT

www.cddft.nhs.uk
7 Day Services – Beyond Assessment

www.cddft.nhs.uk
County Durham & Darlington Profile
• Population base served:
– 610,000 approximately
• 3 Clinical Commissioning Groups
– North Durham, DDES &Darlington
– 82 GP practices
• County Durham and Darlington NHS Foundation Trust – integrated acute / community health care provider
– 2 Acute hospitals
– Access to six community hospitals
• Tees, Esk and Wear Valley NHS Foundation Trust
– Provides inpatient and community services
• Two local authorities
– Darlington Borough Council
– Durham County Council
• North East Ambulance Service (NEAS)

www.cddft.nhs.uk
Approach to 7 Day Services
• Whole economy integrated approach
• Health
• Social Care
• Third Sector
• Patient groups
• Service Transformation
• Integrated governance and planning across all partners
• Align with locality strategies such as ‘Better Care Fund’.
• Programme Methodology for delivery with three priority areas
• Frail elderly
• Urgent Care
• Diagnostics

www.cddft.nhs.uk
High Performing 7DS – Some Key Areas
Career Structure
Goal Setting
System
Culture
Disciplinary
SystemStakeholder
engagement &
Communication
Clinical
Governance
Contractual and
competitive
strategy
Pay
Training &
development
LHE and local
Organisation
Structure
Professional
body, Trade
Union
Relationship
Planning
Service ,
investment &
people
Strategic
Decision Making
Information
Systems &
Sharing
Performance
monitoring
&mgt
Job Roles
Local High
Performance
7Ds

www.cddft.nhs.uk
A shared vision creates aligned policy?
2014
7 day access
BCF
PMCF
Federated
GP
GP, IT
system
Medical
contracts
Competition
& Cost reduction
DES
2019Vision &
position
2014
7 day access
DES
BCF
New contracts
Competition
and cost
reduction
“Without a sensible shared vision, a transformation effort can easily dissolve
into a list of confusing and incompatible projects that can take the
organisation in the wrong direction or nowhere at all.”
John P Kotter

www.cddft.nhs.uk
Lessons learned from previous programmes of joint work
Lack of clarity about
performance gains
to be delivered in
each org
Rushing to solutions
Change
infrastructure and
plans not in place
No concrete
management
support,
management not
aligned
Resource needs not
recognised
Assumptions &
givens not clarified
and communicated
Visioning just a
paper exercise – not
a real picture of the
future
Change activity &
communications
confined to
‘specialists’
Change
process begins
in the old way –
imposition not
involvement
Key staff issues and
concerns not
addressed
Not enough
information about the
case for change
Once-off
communications no
continuous process
Sheep dip
training/
engagement
Failure to
achieve
tangible
goals
Poor role
modelling
Programme
taking too
long
No redesign – so the new
organisation has the wrong
configuration
Technical system redesign
only – people side short-
changed
Imposed by ‘experts’
Using pilots to
prove/disprove viability
rather than test the design
Inadequate
implementation
planning and
preparation
Resources not available
Performance dip
Training practicalities ignored
Contingent systems changes
not ready
No effective learning
processes
Failure to
evaluate
and review
effectiveness of
the changesPlateau effect
Leaders stuck in old
ways of working
Reverting to old ways
in times of crisis
Roles not clear
Deliverables not clear
Going too far too fast
Poor role modelling from the
top

www.cddft.nhs.uk
Our bespoke change program
B
(1)
A
(2) Local Critical Success
Failure / Factors (5)
Gap
(3)
Change
Priorities (4)
+
Change programme

www.cddft.nhs.uk
Programme Methodology
Establish
The
programme
• Agree key 7
day principles
• Define point B
& understand
point A
• 7 day working
gap analysis &
change agenda
• Programme
Plan
• Business case
• Create steering
group, change
support team &
key pathway
teams
• Preparing key
clinicians &
mangers to
lead change
Mobilise
• Establish
the case for
change
• Stakeholde
r analysis &
comms
strategy
• Creating a
shared
7DS vision
• External
visits\
benchmark
• Staff input
into 7DS
change
agenda
• Simple
wins
Breakthrough
3 Key pathfinder
areas
• Frail Elderly
• Diagnostics
• Urgent care
• Cascade vision
into pathfinder
areas
• Early Wins
System re-design
• Re-designing work
process and systems
• Social systems
design
• Service configuration
• Governance &
Infrastructure design
• Define capability
needs
• Performance mgt
design
• HR\Workforce
systems design
• Review &
evaluate
pathfinders
• Finalise 7
day working
system &
design
• Consultation
• Develop
phased full
roll-out
business
case & Plan
* Red Text –
Areas of
Progress
www.cddft.nhs.uk
Areas of Progress
• County Durham and Darlington Foundation Trust acute
baseline assessment
• Multi-disciplinary team development:
• Acute based
• Community based
• Analysis of key barriers to change
• Integrated planning documentation including vision,
principles and service blueprints
• Information sharing Agreements (ISA)
• Template and populated ISAs
• Case study on information sharing

www.cddft.nhs.uk
Standard 3 - Multi-disciplinary Team (MDT)
review
“All emergency inpatients must be assessed for complex or on-going needs
within 14 hours by a multi-professional team, overseen by a competent
decision-maker, unless deemed unnecessary by the responsible consultant. An
integrated management plan with estimated discharge date and physiological
and functional criteria for discharge must be in place along with completed
medicines reconciliation within 24 hours.”
Supporting information:
• The MDT will vary by specialty but as a minimum will include
Nursing, Medicine, Pharmacy, Physiotherapy and for medical patients,
Occupational Therapy.
• Other professionals that may be required include but are not limited
to: dieticians, podiatrists, speech and language therapy and
psychologists and consultants in other specialist areas such as
geriatrics.
• Reviews should be informed by patients existing primary and
community
• Appropriate staff must be available for the treatment/management
plan to be carried out

www.cddft.nhs.uk
Achievements
7 DAY MDT
Average Discharge Increase by 7%
Reduction in LOS 5%
Medical Boarders Per Day
Reduction of 67%
AM discharges
Increase by 13%
Non acute tfr of patients per week
Increase by 27%
ED Activity
Increase by 5%
Falls per week
Reduced by 25%

www.cddft.nhs.uk
Further 7 day Projects Which Have Stemmed
From The Implementation Of Standard 3…
There are 4 key issues which are blocking medically fit patients from leaving the ward…
On average the information centres across the six wards are typically seeing 30 patients
per week who are now medically fit for discharge but are “blocked” in the system due to
problems which are being addressed.
Just over one
third of the
patients ready to
move on are
under the Trust’s
control
By making problems visible on information centres, the teams have highlighted 4 key areas
of focus: CHC assessments, Nursing Home discharges, Diagnostics and community
hospitals.

www.cddft.nhs.uk
Community / primary based
MDT’s
Engaging the LHE in the process – cross organisational
changes to break down barriers

www.cddft.nhs.uk
What We Are Trying To Achieve
• Improve patient experience
• More effective care planning and packages centred on
individual needs
• Care in the community or at home where preferred option
• Increase in self-management
• Increased involvement of Voluntary Care sector
• Prevent unnecessary acute admission/re-admission
• Reduce length of stay (e.g. through ‘in-reach’)
• Reduce number of patients transferred to long term care

www.cddft.nhs.uk
Stakeholders Involved
• Darlington CCG & Associated Practices
• County Durham and Darlington FT
• Darlington Borough Council
• Tees, Esk and Wear Valley FT
• Voluntary Sector
• Care Home Sector
• Healthwatch
• NEAS
• North of England Commissioning Support

www.cddft.nhs.uk
Progress since March 2014 –
Primary Care
• Practice MDT’s take place monthly in place with attendance from
Social Workers, Community matrons and Voluntary Sector brokers
• Advanced care plans being developed for 2% of population at
highest risk of emergency admission
• Monthly meetings to discuss those who have had emergency
admission in previous month & agree how care plan/support
package needs to be amended to prevent re-occurrence
• Voluntary sector broker liaises with other VS organisations as
appropriate
• Referrals made to other teams as appropriate e.g. mental health
• Evolutionary development

www.cddft.nhs.uk
Progress since March 2014 – Care Homes and initial
feedback
• Community Matrons now working 9am – 5pm; 7 days a week
– linked to Top 10 Care Homes
• District Nurses pick up any referrals overnight
• Community Matrons attending all GP practices monthly MDT’s
• EHCP/Advanced Care Plans starting to be put in place for all
patients in care homes.
• NEAS aware of new ways of working and ring Matrons prior to
patients conveyance to hospital

www.cddft.nhs.uk
Outcomes So Far:
Emergency Admissions from Care Homes –
April to November 2014
Local
authority Location Name Apr-14
May-
14
Jun-
14 Jul-14
Aug-
14
Sep-
14
Oct-
14
Nov-
14
Curren
t Total
Darlington
Darlington Manor Care
Home 6 4 6 3 4 1 24
Darlington Eastbourne Care Home 6 8 1 8 6 8 4 2 43
Darlington Eden Cottage Care Home 6 8 1 8 6 8 4 2 43
Darlington
Grosvenor Park Care
Home 8 7 9 8 5 9 6 52
Darlington Rydal Care Home 3 2 2 4 2 10 2 25
Darlington
St Georges Hall and
Lodge 4 5 6 4 7 4 2 32
Darlington The Gardens Care Home 9 5 8 8 6 7 5 2 50
Darlington The Grange 8 17 16 5 7 6 6 2 67
Darlington Ventress Hall Care Home 4 5 7 11 8 4 4 2 45
Darlington Willow Green Care Home 14 9 8 7 5 3 3 1 50
Monthly total 68 65 63 68 49 66 38 14 431

www.cddft.nhs.uk
Issues – Or Challenges
And Opportunities
• Multi organisation working
• Aligning national strategies against challenging timelines
• Information sharing
• IM & T
• Communication

www.cddft.nhs.uk
Future direction and next
steps
• Community Rapid Assessment Service - Front of House
• Geriatrician telephone advice line 12:00 – 14:00 Monday to
Friday
• Hospital to Home
• Additional matrons/assistant practitioners to support
remaining care homes
• Identification of areas for future development/investment

www.cddft.nhs.uk
Overcoming the IG ‘Barriers’
• It’s not ‘we can’t share’ – its ‘how can we share’
• An Information Sharing Agreement (ISA) is a document
for all parties to agree :
• Assist compliance with information rights law and
practice.
• Set’s out standards and consistency that have to be met
by all signatories.
• Ensure patient consent is achieved in process

www.cddft.nhs.uk
How will we know where we
are going?
shared vision – shared understanding - shared outcomes

www.cddft.nhs.uk
Arriving at a GP practice at 2pm on a Saturday, we note that
• The practice is open and offering both emergency appointments and clinical sessions to patients who have booked there appointment through the multi-agency SPA.
• A mixture of local point of testing, locality based x ray and digital health care systems providing a local integrated diagnostic support system.
• We note the GPs working on the Saturday sessions are from a range of local practices, the local GP federation providing a locality based approach to 7 day working and medical cover.
• A frail elderly MDT meeting is in progress with a local specialist GPwSI, Social worker, a NA&S collaborative nurse , a community diabetic specialist nurse and CPN are holding a video conference with a community geriatrician who is linked in from the local community hospital where she is helping on assessments of patients to move back to home based settings.
• The MDT are all using TPP Systmone as the core single record and basis of the case mgt of both high risk patients and those who are being discharged from hospital. The social and community staff linking in through their mobile working laptop system, all patients on the MDT system having agreed to share their information
• Leaving the practice we note that a program of LTC support sessions are planned for Monday, at these sessions consultants and specialist nurses are booked to provide integrated support sessions to frail elderly patients with multiple conditions - diabetes, vascular and supporting podiatry and retinal screening sessions being carefully planned to allow access to clients until 7pm

www.cddft.nhs.uk
Travelling to a local care home on Sunday we note
• A NA&S collaborative nurse is undertaking a review of 6 patients, 3 identified
in a local MDT meeting from risk stratification process as having a risk of
escalation and 3 recent arrivals from a planned discharge process 2 from a
community hospital and one from a DGH.
• The patient discharged from hospital, arrived an hour ago, the community led
integrated intermediate care / discharge team planned the discharge from the
hospital with essential medication being provided from the new 7 day pharmacy
service. The script being sent electronically from the hospital
• The patients hospital discharge information pack, included a web generated
nutrition plan, and a digital health monitoring pack. This cheap and flexible
digital health pack, brought by the ISIS HCA in the boot of his car, was
connected and put on line and started taking readings within 10 mins. The
information being cloud based, allows decisions around additional care to be
made by local GPs accessing clinical information. This INR dependant patient
is also utilising the digital monitoring system to dose check as required.
• The care home staff are preparing for a visit from a local care home support
team of GP, a NA&S collaborative nurse and pharmacist who provide focussed
support to help avoid hospital admissions
www.cddft.nhs.uk
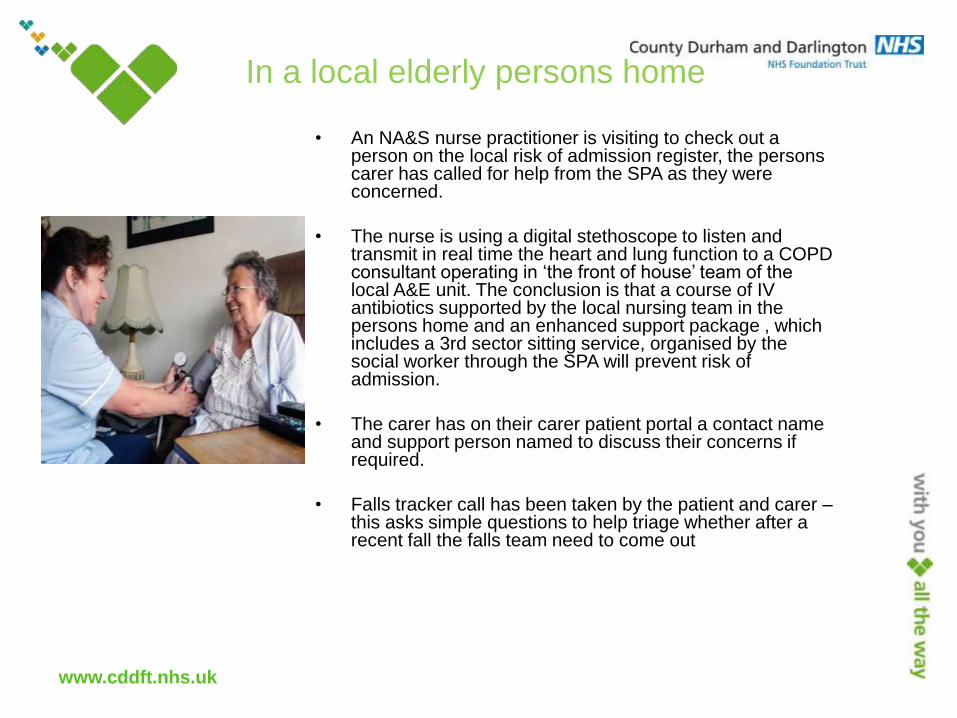
In a local elderly persons home
• An NA&S nurse practitioner is visiting to check out a person on the local risk of admission register, the persons carer has called for help from the SPA as they were concerned.
• The nurse is using a digital stethoscope to listen and transmit in real time the heart and lung function to a COPD consultant operating in ‘the front of house’ team of the local A&E unit. The conclusion is that a course of IV antibiotics supported by the local nursing team in the persons home and an enhanced support package , which includes a 3rd sector sitting service, organised by the social worker through the SPA will prevent risk of admission.
• The carer has on their carer patient portal a contact name and support person named to discuss their concerns if required.
• Falls tracker call has been taken by the patient and carer –this asks simple questions to help triage whether after a recent fall the falls team need to come out
www.cddft.nhs.uk
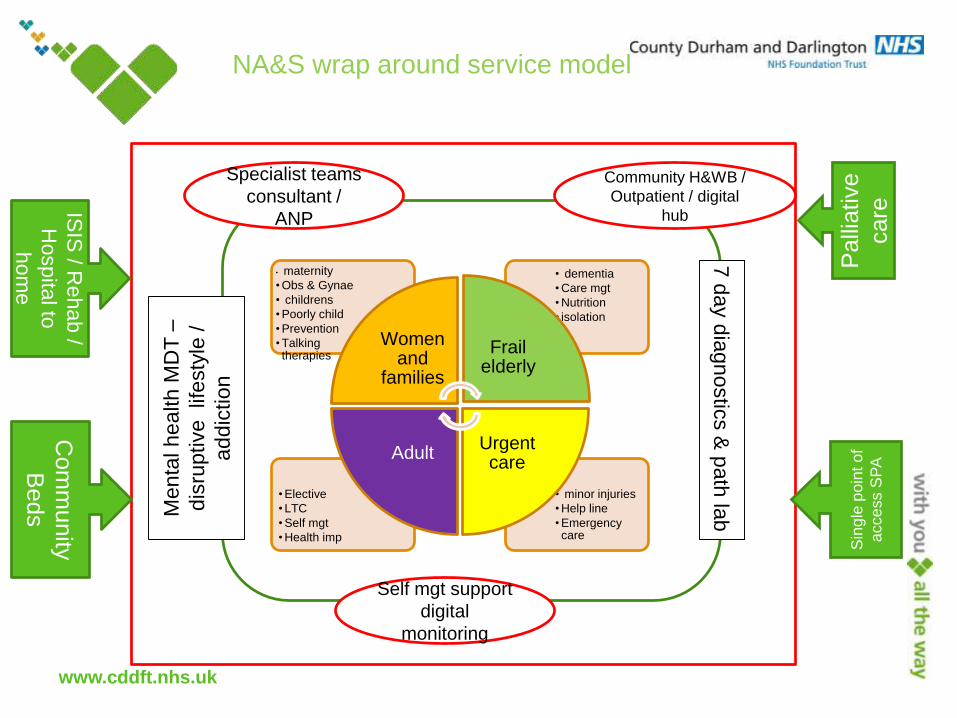
NA&S wrap around service model
• minor injuries
• Help line
• Emergency care
• Elective
• LTC
• Self mgt
• Health imp
• dementia
• Care mgt
• Nutrition
• isolation
• maternity
• Obs & Gynae
• childrens
• Poorly child
• Prevention
• Talking therapies
Women and
families
Frail elderly
Urgent care
Adult
7 d
ay d
iagnostic
s &
pa
th la
b
Men
tal h
ea
lth
MD
T –
dis
rup
tive
lif
esty
le /
addic
tion
Specialist teams
consultant /
ANP
Community H&WB /
Outpatient / digital
hub
Self mgt support
digital
monitoring
Palli
ative
care
Sin
gle
po
int o
f
acce
ss S
PA
ISIS
/ Rehab /
Hospita
l to
hom
e
Com
munity
Beds

www.cddft.nhs.uk
Clinical Programme Board
(Transformation Board)
County Durham and Darlington Strategic Programme
Board
Darlington
Organisational
Leads
Better Care Fund
7 Day
Working
Care
Closer To
Home
Unschedul
ed Care
Planned
Care
County Durham
Organisational
Leads
Strategic Enabling Programmes Informatics, Estates, Workforce, etc
County Durham and Darlington Transformation Hub
Darlington Transformation Hub
PROGRAMME
PORTFOLIO
GOVERNANCE
RESOURCES
Clinical
Advisory
Group
Darlington
Unit of Planning
County Durham
Unit of Planning PLANNING
Health and Wellbeing Boards
County Durham Transformation Hub

www.cddft.nhs.uk
IM&T & Equipment infrastructure
• Shared records based on NHS Number
• Community and primary teams on same system
• Portal technology to link acute /primary/ community/ social care / tewv/3rd sector and patient / carer
• Mobile working with common communications / Wi-Fi to allow access at any part of LHE system
• Digital health systems with multi input capability and able to link to patient record electronically
• All infrastructure (wires / kit / support from common supplier / maintenance / helpdesk system )
• All clinical equipment standardised
• Single process for immunisation & vaccinations management – managed by upgraded child health approach