6. augsburger forum für medizinprodukterecht · • 7 billion euro in 2009 (estimated turnover)...
TRANSCRIPT

6. Augsburger Forum für Medizinprodukterecht
Augsburg, 15. September 2010
Reimbursement of Medical Devices in Italy
Dr.med. Lucio Fumi, MD Wyfold Medical Consultancy, UK
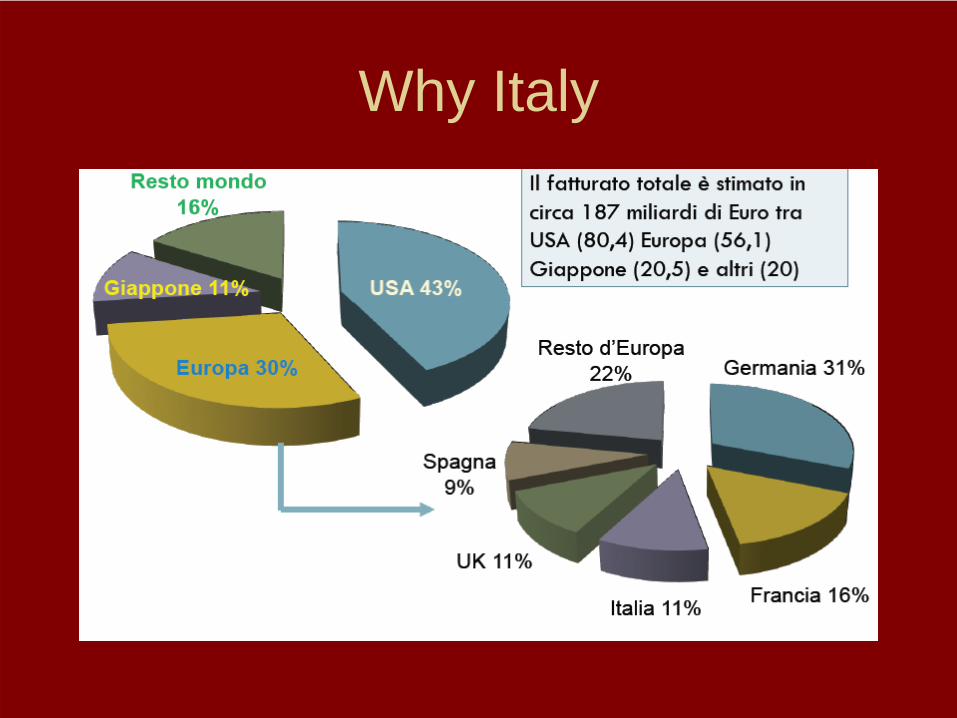
Why Italy

Size of the Italian Market for Medical Devices
• 7 billion Euro in 2009 (estimated turnover)• 20% from Italian manufacturers• Total Healthcare spending = 110 billion
Euro

Market by Therapeutic Areas

Types of Health Structures

Medical Devices spending: trend 1998-2008 (S.Orsola)

The Institutional Actors
• National Level: Ministero della Salute• Regional level: 20 Regions• Local level: 185 ASL + 95 Independent
Hospitals

The Non-Institutional Actors
• Assobiomedica = Industry Association for Medical Devices and IVD (www.assobiomedica.it)
• CERGAS of Università Bocconi (Milan) Prof. Rosanna Tarricone and Prof Aleksandra Torbica

Terminology
• Dispositivo Medico (= Medical Device = Medizinprodukt)
• Ministero della Salute = Ministry of Health • Ministero della Sanità (former name)• SSN = Servizio Sanitario Nazionale
(= National Health Service)• Assessorato Regionale = Regional Ministry• ASL = Azienda Sanitaria Locale
(= Local Health Authority)

Ministero della Salute: website
• www.salute.gov.it/dispositivi/dispomed.jsp

CUD = Commissione Unica per i Dispositivi
• Law n.289 of 27.12.2002• Set up of the CUD, with the following
tasks:– To define and keep updated a list
(“repertorio”) of Medical Devices– To classify them specifically– To indicate reference prices

The Italian Regions: some history

Assessorati Regionali
• The Regional Health Authorities are responsible for managing the Reimbursement System, through 3 tools:– DRG system for Hospital Services (1995)– Positive List for Outpatient Services– List of Medical Devices to be supplied to end-
users (e.g. ostomy, wound care, incontinence, hearing aids)
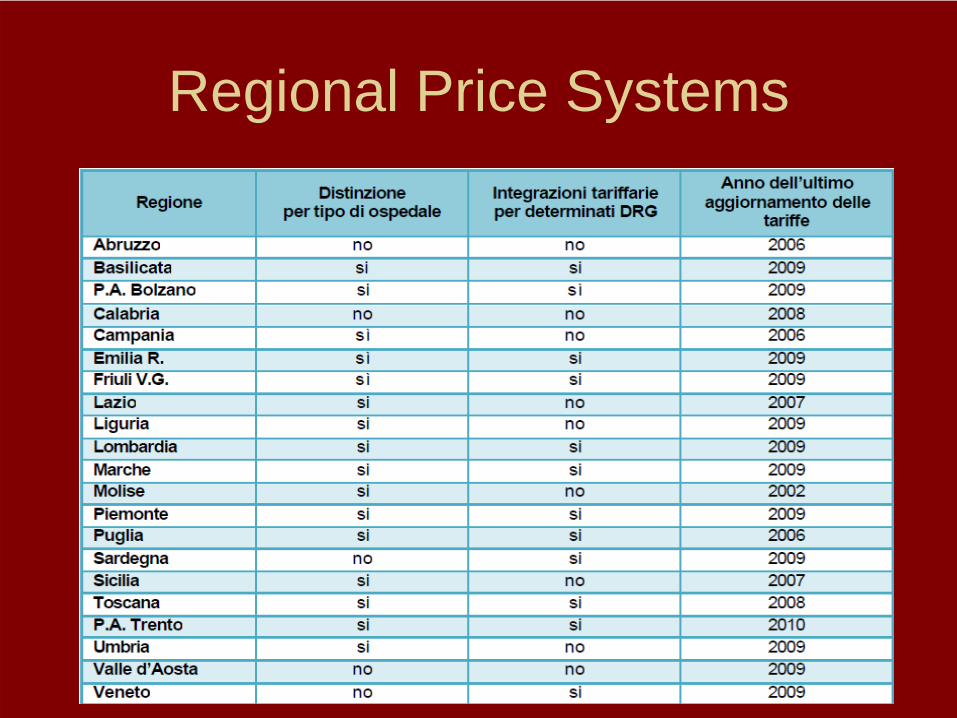
Regional Price Systems

Budget management: an Italian issue
• Healthcare = 80% of Regional Budget• Some Regions are bankrupt: heavy support from
the Central Government (example of Catania)• Corruption: Italy ranks 63rd in the latest Report
from Transparency International (after Malaysia and Namibia)
• Public Media Control: Italy ranks 49th in the latest Reporters sans Frontières (after Jamaica and Ghana)

Centralization of purchasing

DSO (Days of Outstanding Sales)
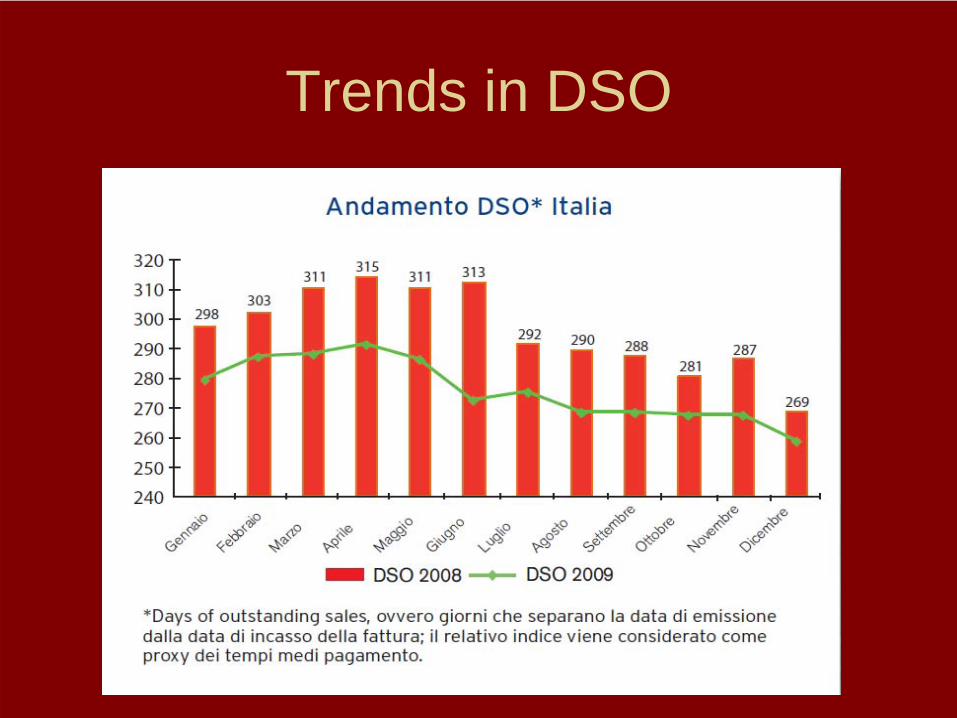
Trends in DSO

DSO by Region

Different Levels of HTA Agencies
• National: Age.na.s (= agenzia nazionale per la salute = National Agency for Healthcare)
• Regional: Emilia-Romagna, Veneto, Toscana
• Local: S.Orsola (Bologna), Policlinico Gemelli (Roma)
Available models for HTA

HTA and reimbursement
Hyperthermic Chemotherapy
HIPEC
Hyperthermic Peritoneal Chemotherapy for Peritoneal Carcinomatosis

Peritoneal Carcinomatosis • Spread of cancerous cells on the surface of the
peritoneum (both visceral and parietal)
• Origins or carcinomatosis:– Primary peritoneal tumours (mesothelioma)– From cancers of peritoneal organs or viscera
(psuedomyxoma peritonei , colorectal cancer, gastric cancer, ovarian cancer)
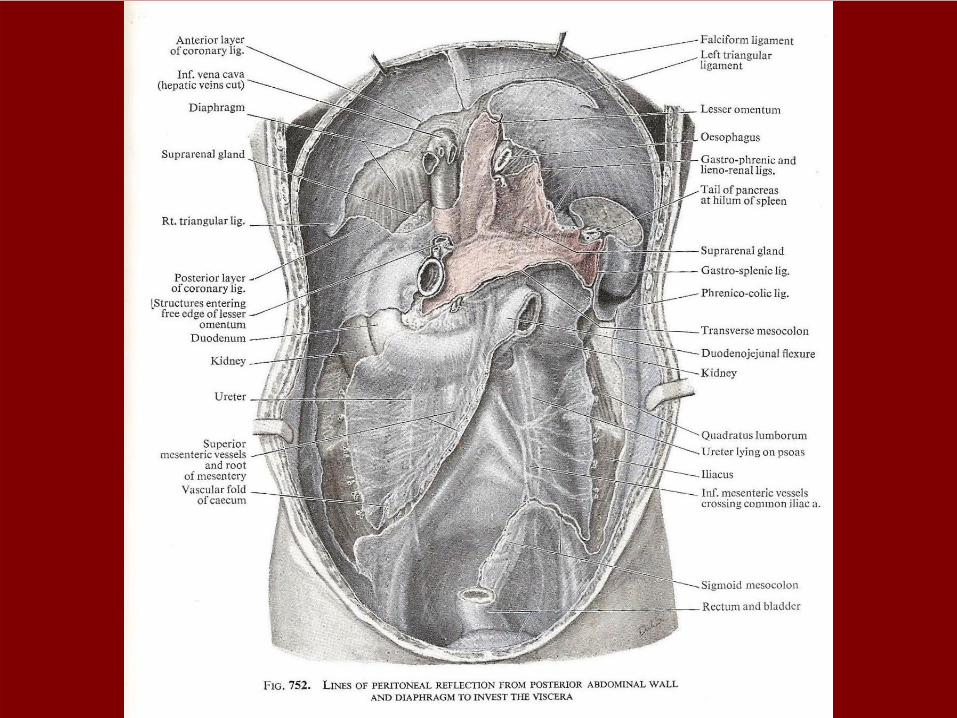
Peritoneum

Peritoneal Carcinomatosis - therapy
• The peritoneal cavity is poorly accessible by systemic chemotherapy
• Drugs injected systemically achieve a very low concentration in the peritoneal cavity (“plasma- peritoneum barrier”)
• The barrier is represented by the sub-mesothelial tissue and the basal membrane of the capillaries, which limit the passage of hydrophylic or high-molecular weight drugs, like mitomycin C, cisplatin and doxorubicin

Peritoneal Carcinomatosis - therapy (2)
• Current therapy consists of an association of Cyto- reductice Surgery (CRS) and HIPEC (Hyperthermic Intra PEritoneal Chemotherapy ) in the same surgical session in the Operating Room
• Surgical phase = CRS (Cyto-Reductive Surgery): surgical resection of the tumour mass + carcinomatosis - maximum number of neoplastic cells (“macroscopic cyto-reduction”)
• HIPEC = pharmacologic removal of micro-foci of neoplastic cells inevitably residual (“microscopic cyto-reduction”).

Cyto-reductive Surgery (CRS)Surgical exeresis of:
• abdominal organs / viscera hit by the tumour (multivisceral resection)
• lympho-adenectomy
• visceral peritonectomy of conserved organs
• partial or total parietal peritonectomy
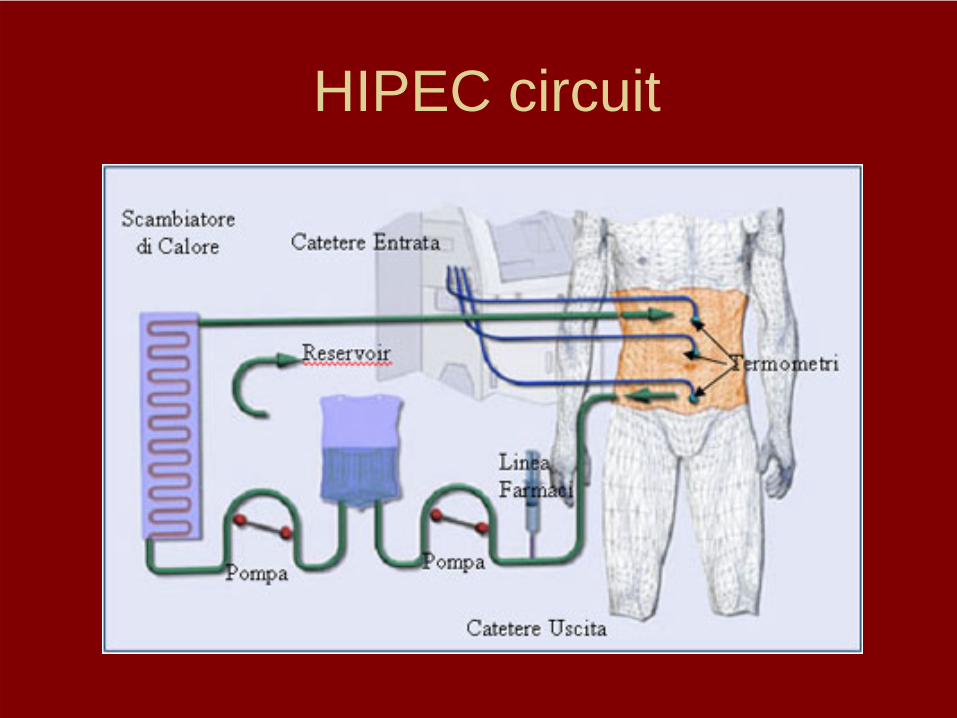
HIPEC circuit

Principles of HIPECPharmacological advantages of HIPEC vs
systemic chemotherapy:
• Higher (> more effective) concentrations of cytotoxic agent
• Reduced systemic absorption through visceral and abdominal wall surface (even after peritonectomy) >lower systemic toxicity
• Hyperthermia (= higher than physiologic temperature: 41°- 43°)
CRS + HIPEC in peritoneal carcinomatosis:
published clinical results
• Colorectal cancer• Gastric cancer• Ovarian cancer• Pseudo-myxoma peritonei• Peritoneal mesothelioma
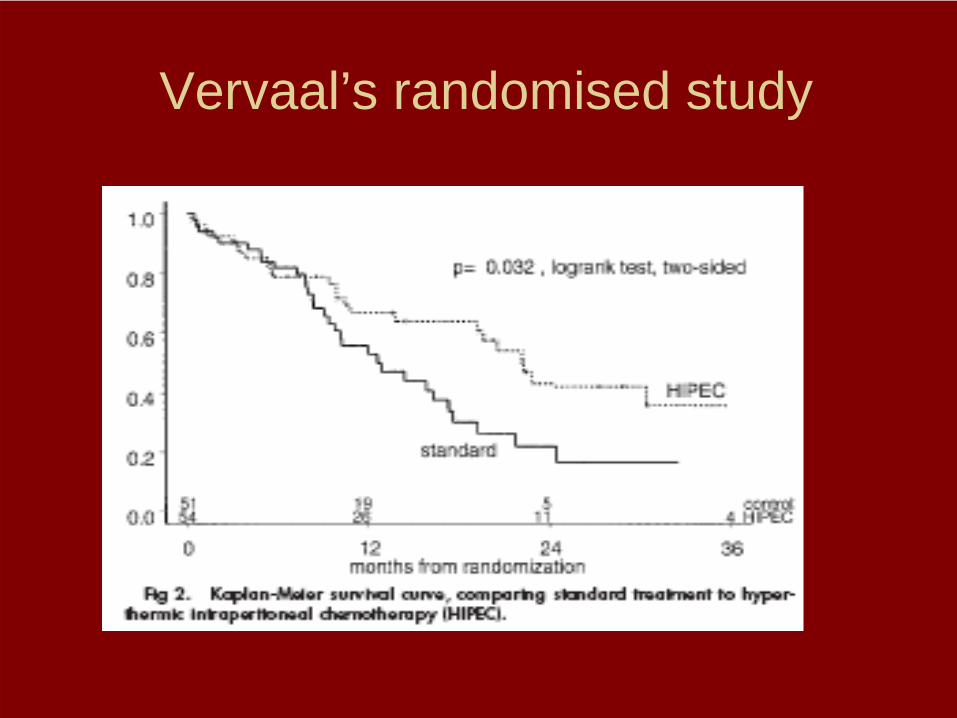
Vervaal’s randomised study
Levels of clinical evidence Cochrane Library Training Guide, 2007
• I Strong evidence from at least one systematic review of well designed randomised controlled trials (RCT)
• II Strong evidence from at least one properly designed RCT of appropriate size
• III Evidence from well designed trials without randomisation: single group pre-post; matched case-controlled
• IV Evidence from well designed non-experimental studies from more than one centre or research group
• V Opinions of respected authorities, based on clinical evidence, descriptive studies or reports of expert committees
• VI Expert personal opinion of professionals, anecdotal evidence

Are RCTs always necessary?
The parachute paradox
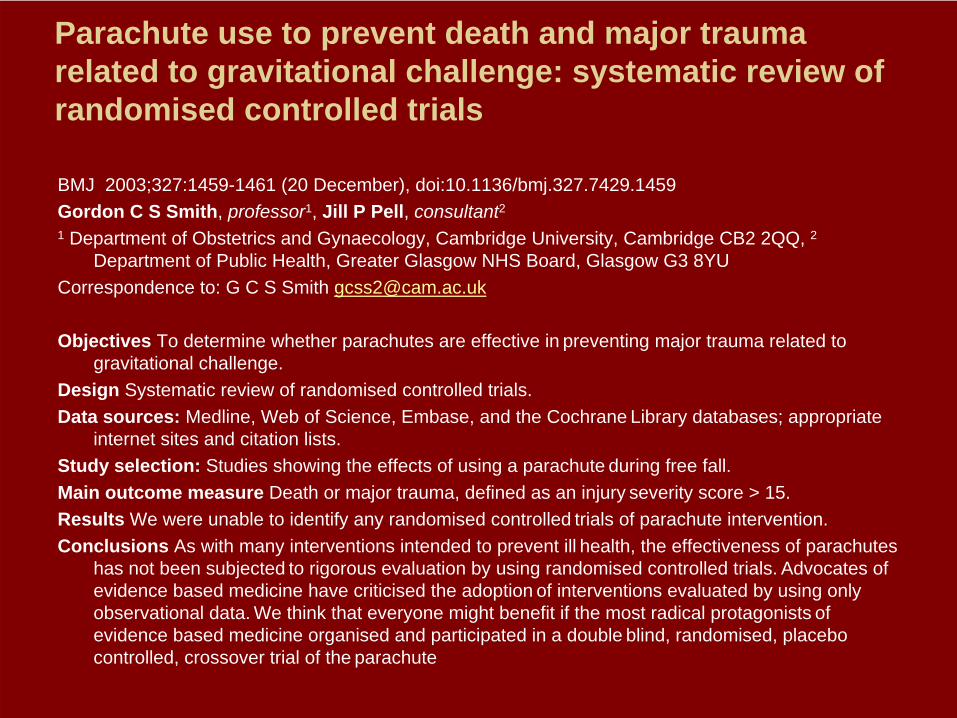
Parachute use to prevent death and major trauma related to gravitational challenge: systematic review of randomised controlled trials
BMJ 2003;327:1459-1461 (20 December), doi:10.1136/bmj.327.7429.1459 Gordon C S Smith, professor1, Jill P Pell, consultant21 Department of Obstetrics and Gynaecology, Cambridge University, Cambridge CB2 2QQ, 2
Department of Public Health, Greater Glasgow NHS Board, Glasgow G3 8YU Correspondence to: G C S Smith [email protected]
Objectives To determine whether parachutes are effective in preventing major trauma related to gravitational challenge.
Design Systematic review of randomised controlled trials.Data sources: Medline, Web of Science, Embase, and the Cochrane Library databases; appropriate
internet sites and citation lists.Study selection: Studies showing the effects of using a parachute during free fall.Main outcome measure Death or major trauma, defined as an injury severity score > 15.Results We were unable to identify any randomised controlled trials of parachute intervention.Conclusions As with many interventions intended to prevent ill health, the effectiveness of parachutes
has not been subjected to rigorous evaluation by using randomised controlled trials. Advocates of evidence based medicine have criticised the adoption of interventions evaluated by using only observational data. We think that everyone might benefit if the most radical protagonists of evidence based medicine organised and participated in a double blind, randomised, placebo controlled, crossover trial of the parachute

Parachute approach to evidence based medicine Malcolm Potts, Bixby professor, population and family planning1, Ndola Prata, lecturer1, Julia Walsh,
adjunct professor1, Amy Grossman, research assistant11 School of Public Health, University of California, 314 Warren Hall, Berkeley, CA 94720, USA Correspondence to: N Prata [email protected] for the results of randomised trials of public health interventions can cost hundreds of lives,
especially in poor countries with great need and potential to benefit. If the science is good, we should act before the trials are done
In 2003 Smith and Pell published an entertaining but profound article titled: "Parachute use to prevent death and major trauma due to gravitational challenge."1 They used the lack of randomised controlled trials in testing parachutes to show that situations still exist where such trials are unnecessary. We argue that the parachute approach, where policies are set based on good science but without randomised trials, is often more suitable in resource poor settings. We use the examples of oral rehydration therapy in children diarrhoea, male circumcision to prevent HIV infection, and misoprostol for postpartum haemorrhage to show how an overemphasis on randomised controlled trials in poor settings poses important ethical and logistic problems and may incur avoidable deaths.
Summary pointsRandomised controlled trials are usually required before new interventions are implemented If other evidence of effectiveness is good, and potential benefits large, the resultant delays may be
unethical Examples from poor countries show the price of delaying interventions

Are randomised trials needed in the era of rapidly evolving technologies?
Eur J Cardiothorac Surg 2009;35:474-478. doi:10.1016/j.ejcts.2008.08.032
Clinical Operational Research Unit, Department of Mathematics, UCL, London WC1H 0BT, United Kingdom
Received 19 June 2008; accepted 26 August 2008. Corresponding author. Tel.: +44 7957 168754. (Email: [email protected] ).
New technologies are expensive. The health care budget cannot expand indefinitely so if new treatments are introduced they may have to displace other treatments, or prevent other new treatments coming into practice. This is not simply a money saving exercise; it is accepted that new high technology treatments may cost more to implement but they must be worth the money spent in comparison with other treatments. Therefore cardiothoracic surgeons must first demonstrate that our treatments are effective. Then we need evidence of cost effectiveness in comparison with other therapies.
Key Words: Evidence based medicine • Clinical trials • Innovation • Emerging technology

Alternatives to RCTs in the Generation of Clinical Evidence
• Consensus• Guidelines• Registries

Conclusions
• Good contacts in Ministero della Salute• Good contacts in Regional Authorities
(local – capillarity)• Good contacts in Assobiomedica• Good contacts in CERGAS – Bocconi• Italian language (or an Italian
representative) essential• Good clinical outcome and health
economics data!
Acknowledgements
• The tables contained in the slides number 5, 6, 16, 18, 19, 20 and 21 are reproduced, with permission, from the Assobiomedica documents “Rapporto 2010” and “Analisi-10, 2010”.
Thank you for your attention!
Dr Lucio Fumi, MD
Phone +44 1491 680 072Mobile +44 7785 233 189