26.04.20051 lecture 12: economic incentives and the organization of private physician practice ii
TRANSCRIPT
26.04.2005 1
Lecture 12:Economic incentives and the organization of private physician practice II
2
A GP’s optimal number of patients and level of service provision
• Reference: Iversen 2004
• Problem to be addressed: Irrespective of whether a formal list patient system exists, a GP will often have a group of people who visit him regularly and consider him to be their personal doctor. An important decision for the GP is: How many people would he like to care for and what level of service provision would he like to offer? These decision also implicitly contains the choice of income and leisure.
• Are these decisions influenced by the payment system a GP is offered? For instance: Are there other incentives in a capitation fee compared with a fee for service? And what about combinations?
3
si
h(si)
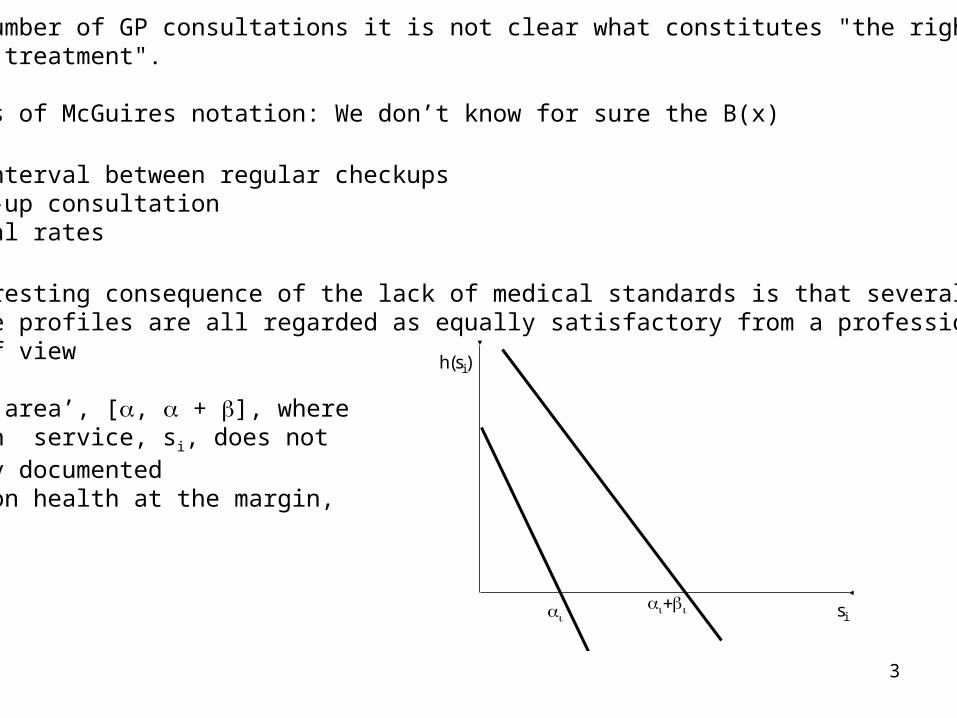
For a number of GP consultations it is not clear what constitutes "the right medical treatment".
In terms of McGuires notation: We don’t know for sure the B(x)
•Time interval between regular checkups•Follow-up consultation •Referral rates
An interesting consequence of the lack of medical standards is that severalpractice profiles are all regarded as equally satisfactory from a professional point of view
A ‘grey area’, [, + ], where a health service, si, does not have any documented effect on health at the margin,h(si)=0.
4
• Assume that the number of services per patient will be somewhere in this interval
• We assume that the physician can influence the number of patients (n) he takes care of.
• We assume that a physician decides the quantity of health services provided to each of his patients.
• We further assume that a physician has lexicographic preferences concerning his patients’ health and his own income and leisure. This assumption implies that a patient’s health is never balanced against the GP’s income or leisure. Health services are then provided until the marginal health effect is equal to zero. The implication of relaxing this assumption?
• We assume a quasilinear objective function formulated in monetary terms as V = c + v(l), where c is consumption (all income is consumed) and l is leisure. v(l) is assumed to be strictly concave with v'(l) > 0.
• Problem: What is the a GP’s optimal combination of patients and number of services per patient?
• The physician’s decision problem may formally be expressed as:
5
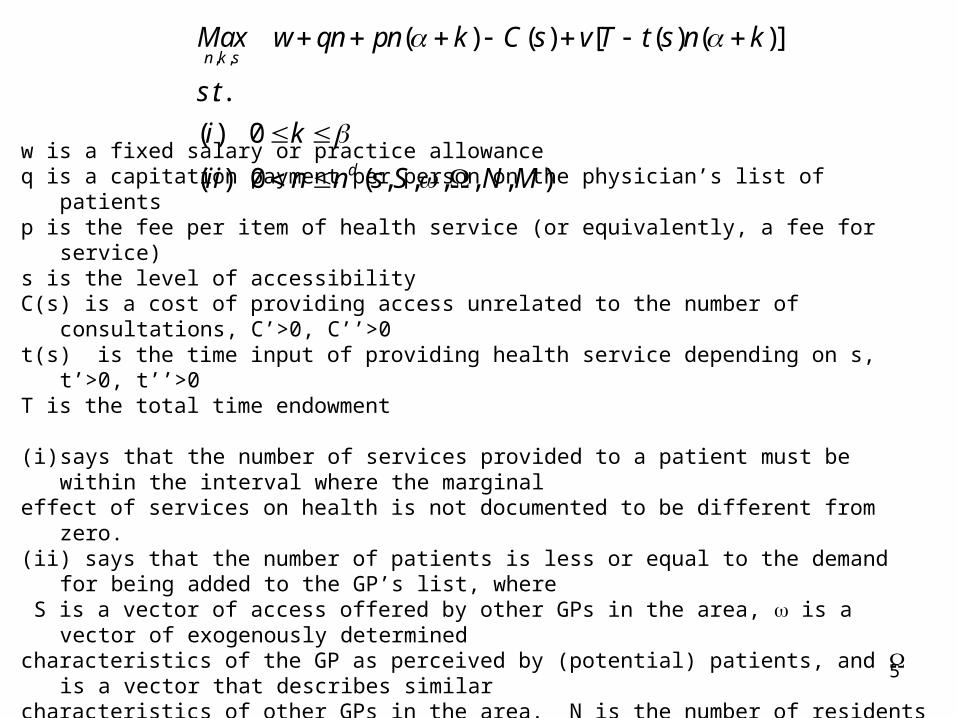
w is a fixed salary or practice allowanceq is a capitation payment per person on the physician’s list of patientsp is the fee per item of health service (or equivalently, a fee for service)s is the level of accessibilityC(s) is a cost of providing access unrelated to the number of consultations, C’>0, C’’>0 t(s) is the time input of providing health service depending on s, t’>0, t’’>0 T is the total time endowment
(i) says that the number of services provided to a patient must be within the interval where the marginal effect of services on health is not documented to be different from zero. (ii) says that the number of patients is less or equal to the demand for being added to the GP’s list, where S is a vector of access offered by other GPs in the area, is a vector of exogenously determined characteristics of the GP as perceived by (potential) patients, and is a vector that describes similar characteristics of other GPs in the area. N is the number of residents in the area and M is the number of GPs. We shall only consider cases where n is positive.
, ,( ) ( ) [ ( ) ( )]
. .
( ) 0
( ) 0 ( , , , , , )
n k s
d
Max w qn pn k C s v T t s n k
s t
i k
ii n n s S N M
6
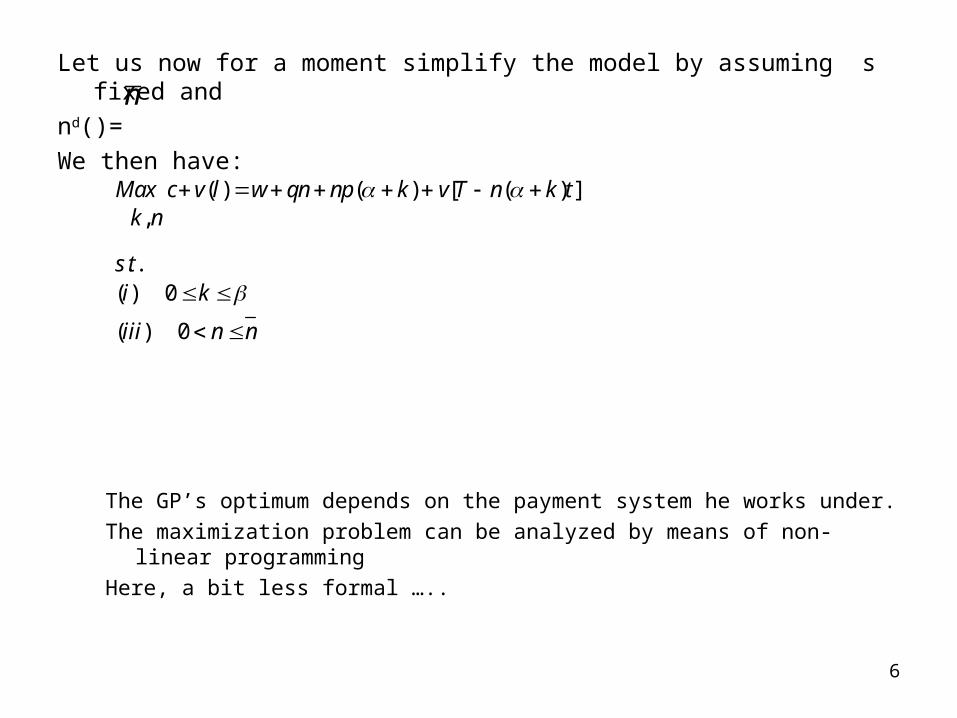
Let us now for a moment simplify the model by assuming s fixed and
nd()=
We then have:
The GP’s optimum depends on the payment system he works under.
The maximization problem can be analyzed by means of non-linear programming
Here, a bit less formal …..
( ) ( ) [ ( ) ],
. .( ) 0
( ) 0
Max c v l w qn np k v T n k tk n
s ti k
iii n n
n
7
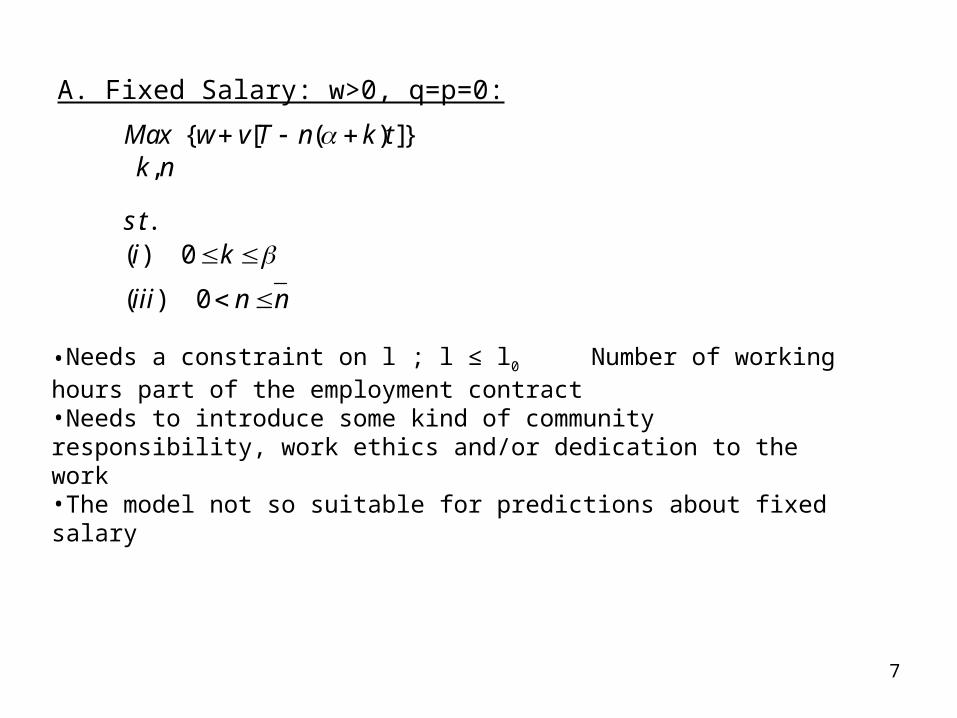
A. Fixed Salary: w>0, q=p=0:
{ [ ( ) ]},
. .( ) 0
( ) 0
Max w v T n k tk n
s ti k
iii n n
•Needs a constraint on l ; l ≤ l0 Number of working hours part of the employment contract•Needs to introduce some kind of community responsibility, work ethics and/or dedication to the work•The model not so suitable for predictions about fixed salary
8
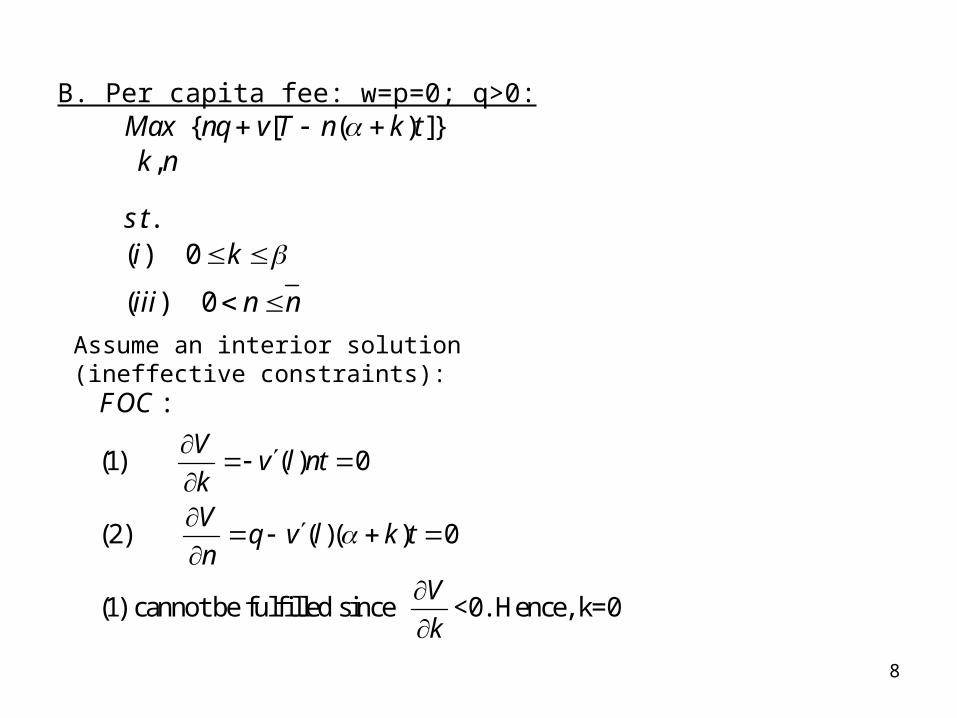
B. Per capita fee: w=p=0; q>0:{ [ ( ) ]}
,
. .( ) 0
( ) 0
Max nq v T n k tk n
s ti k
iii n n
Assume an interior solution (ineffective constraints):
:
(1) ( ) 0
(2) ( )( ) 0
(1) cannot be fulfilled since <0. Hence, k=0
FOC
Vv l nt
kV
q v l k tn
V
k

9
From (2):
Marginal income of patients equal to marginal costs in terms of reduced leisure.
What if n=n0; i.e. effective constraint:
Patient shortage
“Too much leisure”
( )( )q v l k t
0
( )( )
k
q v l k t

10
C. Fee for service: w=q=0; p>0
{ ( ) [ ( ) ]},
. .( ) 0
( ) 0
Max np k v T n k tk n
s ti k
iii n n
Assume interior solution
0
:
(1) ( ) ( )( ) 0 ( )
(2) ( ) 0 ( )
Marginal income of services equals marginal costs
of reduced leisure
Compostion of (n,k) indetermined in the intervals (0,n ) and (
FOC
Vp k v l k t p v l t
n
Vnp v l nt p v l t
k
0, )

11
• What if the constraint n=n0 is effective?Forced leisure – patient shortage:
(AC) Combination practice allowance/fee for service: w>0, p>0, q=0:
No influence on FOC from (C)
(BC) Combination per capita fee/fee for service: w>0, p>0, q=0:Show that we still have k=0 as the optimal solution: Still more rewarding with additional patients than additional servicesHint: Assume an interior solution (0<k<β) and show that FOC then contain a contradiction.Show also that n is determined fromq + pα = v’(l)αtMarginal income from patients equals marginal cost of reduced leisure
( )p v l t

12
(AC) Combination practice allowance/fee for service: w>0, p>0, q=0:No influence on FOC from (C)
(BC) Combination per capita fee/fee for service: w>0, p>0, q=0:Show that we still have k=0 as the optimal solution: Still more rewarding
with additional patients than additional services
Show that n is determined from
q + pα = v’(l)αt
Marginal income from patients equals marginal cost of reduced leisure

13
Questions:
• What are the expected effects of an increase in the number of GPs on provision of services under the various payment systems?
• What are the effect of the introduction of a capitation system, for instance from (AC) to (BC) on a GP’s optimal number of patients? What about the number of services?
• Consider the impact on previous conclusions of assuming that nd is not longer fixed, but may depend on s (accessibility) and k (service intensity)?

14
Example:Denmark: The change in payment system for GPs in Copenhagen
Krasnik, A. et al., 1990, Changing remuneration systems: effects on activity in general practice, British Medical Journal 300, 1698-1701.
Stæhr Johansen, A. K., 1995, Primary care in Denmark, in A. Alban and T. Christiansen, eds., The Nordic lights. New initiatives in health care systems (Odense University Press, Odense) 81-105.
Objective: To study the effects on GPs activities of a change in their remuneration system
from a capitation based system to a mixed capitation and fee per item based system.
What would we expect?
Central features of the study design: Before October 1987: GPs in the City of Copenhagen were paid on a capitation
basis From October 1987: GPs in the City of Copenhagen were paid according to the
same system as the GPs in the rest of Denmark
15
The behaviour of 100 GPs in the City of Copenhagen and 326 GPs in Copenhagen county was studied
GPs behaviour was measured in three periods: March 1987, March 1988, November 1988.
Central results of the study– No increase in the number of consultations– Increase in diagnostic services– Increase in curative services– Decrease in referrals to specialists– Decrease in referral to hospitals
Conclusions: The amount of services provided increased after the introduction of the
fee for service component. The number of consultations, that are partly patient initiated, did not
increase.

16
Example 2: Main results from Iversen (2004)
• Data from the Norwegian capitation trial (1993-1996) that preceded the capitation reform
• Four municipalities with 250 000 inhabitants• Some GPs got a shorter list of patients that they preferred at the start of the trial• Problem studied: Does this shortage of patients have any impact of their intensity of
services provision• Similar studies are now going on with data for the whole country after the capitation
reform
17
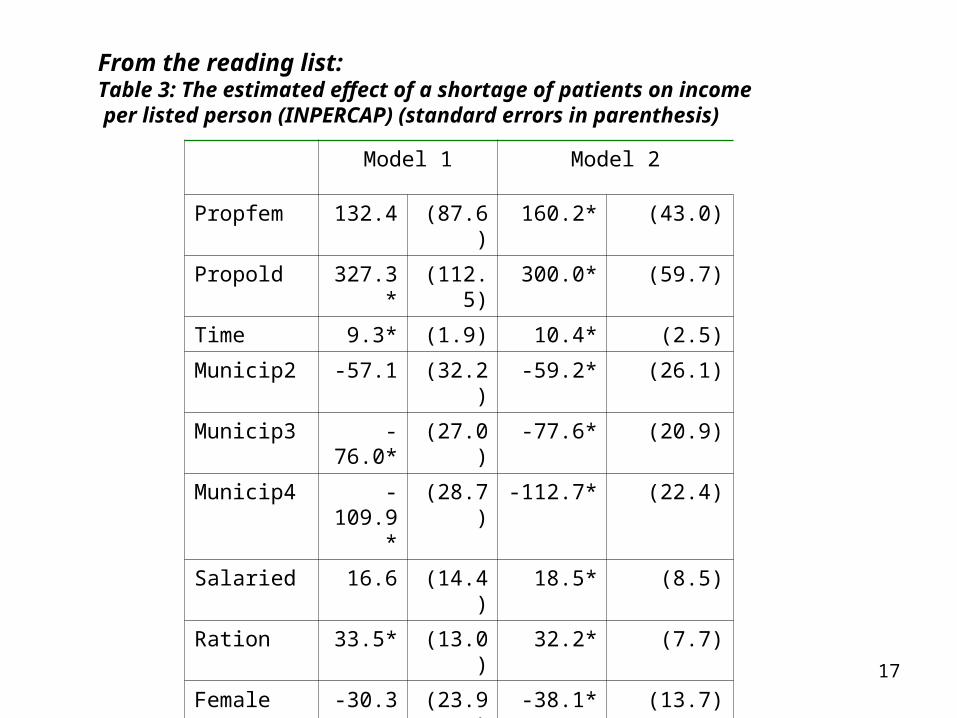
Model 1 Model 2
Propfem 132.4 (87.6) 160.2* (43.0)
Propold 327.3* (112.5) 300.0* (59.7)
Time 9.3* (1.9) 10.4* (2.5)
Municip2 -57.1 (32.2) -59.2* (26.1)
Municip3 -76.0* (27.0) -77.6* (20.9)
Municip4 -109.9* (28.7) -112.7* (22.4)
Salaried 16.6 (14.4) 18.5* (8.5)
Ration 33.5* (13.0) 32.2* (7.7)
Female -30.3 (23.9) -38.1* (13.7)
Constant 178.3* (49.2) 168.9* (31.9)
ρA 0.51 0.42
R2 0.28 0.29
Number of observations
489 489
From the reading list:Table 3: The estimated effect of a shortage of patients on income per listed person (INPERCAP) (standard errors in parenthesis)

18
From the evaluation of the capitation reform in Norway
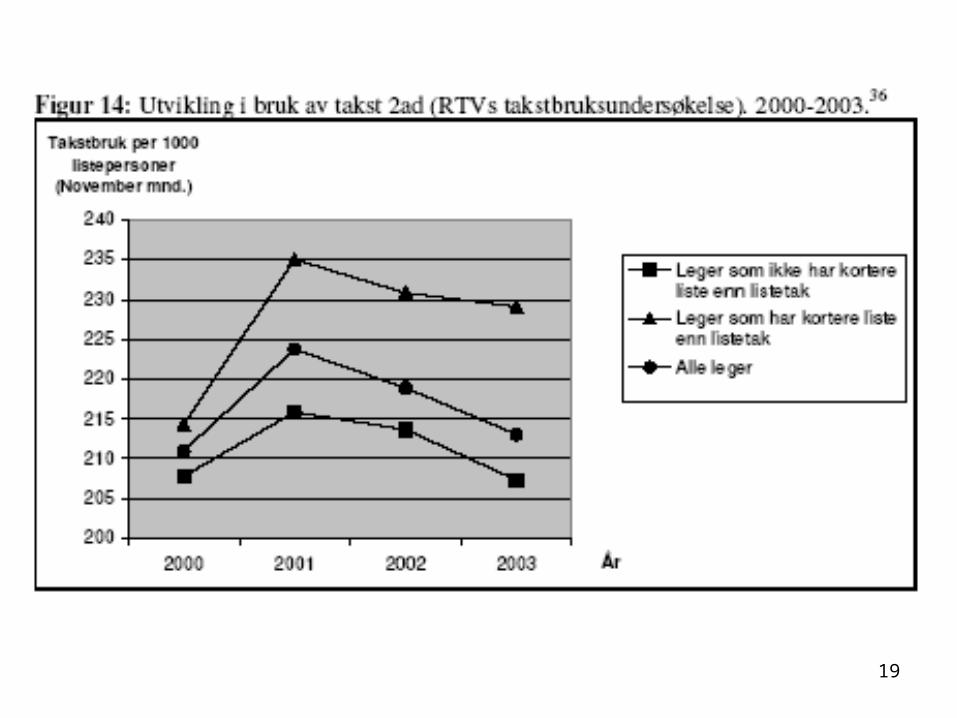
19

20
From the evaluation of the capitation reform in Norway

21

22
Preliminary results from the evaluation of the capitation system in Norway show:
Average income per list person from fees from National insurance: NOK 473
Results from regression analyses adjusted for list composition and
indicators of accessibility:
A shortage of patients increases income from fees per listed person
with (72/473)x100% = 15%
A shortage of patients increases consultations per 1000 listed people
per month with (26/213)x100% = 12%
A shortage of patients increases consultations per 1000 listed people
per month with(9/61)x100% = 15%
23
Policy implications:
• Physician and practice characteristics have an impact on the number and type of services provided and on the public expenditures per person listed
• Patient shortage is costly to the insurer because of income motivated behavior by GPs with unknown benefit to the patient
• The income motivated behavior is driven by the fee-for- service component
• An alternative would be to drop the fee for service component and let the payment system be based on the capitation fee only. The GPs would then compete for patients without considering the income from services per se. Services delivered would then be a means to attract patients to the list and hence, to generate capitation income.
• The problem is that under a pure capitation system not all patients are equally attractive
because of variation in need for services. A risk adjustment component would then be required to prevent risk selection by the GPs.
24
• It is well known from the literature that a risk adjusted capitation system is hard to construct in practice. The present study therefore demonstrates the classical trade off between patient selection and inefficiency in health care.
• We have so far only considered optimal choice from the physician’s perspective, and have not analyzed the relation to optimal service provision from the society’s point of view. An important challenge for future research is therefore to gain more knowledge of the optimal mix of salary, capitation and fee for service in general practice from the society’s perspective.
• Do patients prefer the extra services?We do not know. Important to distinguish between rationing of services and Physician Induced Demand (PID). According to McGuire (2000), “Physician-induced demand (PID) exists when the physician influences a patient’s demand for care against the physician’s interpretation of the best interest of the patient”.
• What we observe is probably a less strict rationing of services among those GPs who have patient shortage. On every list there are probably people who want more frequent and longer consultations. Patients become more satisfied and GPs with patient shortage obtain more income.

25
But is the public sector willing to pay for this?
The ”extra services” cannot be distinguished from the basic services in the fee schedule
Illustrates how difficult it is to direct GPs towards a social optimum by means of economic
incentives
The importance of practice guidelines. A long way to go: Only a minority of GPs say that
they use guidelines from their professional associations and the authorities regularly in
their practice.