2,246 runners congratulations radiance-trio€¦ · 2,246 runners celebrated heart health at. the...
TRANSCRIPT

2,246 runners celebrated heart health at
the Valentine’s 5K Presented by MHIF
MHIF Research Highlights Dashboard: February 2018
Radiance-TrioMHIF successfully completed enrollment in first study arm
Focus is on second arm for patients who’ve failed three or more hypertension medications, including a diuretic
AVERAGEPATIENTS
PERACTIVATED
SITE
ON NEWSTANDS NOW:Journal of the Minneapolis Heart Institute Foundation
Percutaneous Treatment of Mitral Regurgitation: Present and FutureGanesh Athappan, Paul Sorajja and Mario Gössl
…to Dr. Romero and Kelly Wilson for the first enrollment in the Vent-Avoid study
CONGRATULATIONS
MHIF research publishedAMERICAN HEART JOURNAL
“Resource Utilization and outcome among patients with selective vs. nonselective troponin testing”Alex Campbell, MD; Alexander Rodriguez, BS; David Larson, MD; Craig Strauss, MD; Ross Garberich, MS; Matthew Partridge, BA; Timothy Henry, MD; Scott Sharkey, MD
Page 1 of 40

C A R D I O L O G Y G R A N D R O U N D S Title: ACC Scientific Sessions – MHIF SCHOLARS PREVIEW
Speaker: Application of the Hybrid Approach for Percutaneous Coronary Interventions for Chronic Total Occlusions: Update from an International Multicenter Registry Peter Tajti, MD, Postgraduate Research Fellow Minneapolis Heart Institute Foundation® Percutaneous Coronary Intervention In Patients With Previous Coronary Artery Bypass Graft Surgery: Insights from a Multicenter Registry Peter Tajti, MD, Postgraduate Research Fellow Minneapolis Heart Institute Foundation® Impact of the Commercial Introduction of Transcatheter Mitral Valve Repair on Mitral Surgical Practice Hiroki Niikura, MD, Research Scholar, Valve Science Center Minneapolis Heart Institute Foundation® Contemporary Reasons and Clinical Outcomes for Patients with Severe, Symptomatic Aortic Stenosis Not Undergoing Aortic Valve Replacement Liang Tang, MD, Research Scholar, Valve Science Center Minneapolis Heart Institute Foundation®
Date: Monday, February 26, 2018 Time: 7:00 – 8:00 AM
Location: ANW Education Building, Watson Room OBJECTIVES At the completion of this activity, the participants should be able to: 1. Summarize emerging research that colleagues will present at upcoming national scientific meeting. 2. Synthesize ideas and input from across disciplines relevant to each presentation. 3. Recommend content revisions or areas of focus to the presenters.
ACCREDITATION Physician This activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of Allina Health and Minneapolis Heart Institute Foundation. Allina Health is accredited by the ACCME to provide continuing medical education for physicians.
Allina Health designates this live activity for a maximum of 1.0 AMA PRA Category 1 Credit(s)TM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nurse This activity has been designed to meet the Minnesota Board of Nursing continuing education requirements for 1.0 hours of credit. However, the nurse is responsible for determining whether this activity meets the requirements for acceptable continuing education.
Page 2 of 40

DISCLOSURE STATEMENTS Moderator(s)/Speaker(s) Dr. Tajti, Dr. Niikura and Dr. Tang have disclosed that he does not have a conflict of interest in making this presentation.
Planning Committee Dr. Alex Campbell, Jake Cohen, Jane Fox, Dr. Mario Goessl, Dr. Kevin Harris, Dr. Kasia Hryniewicz, Rebecca Lindberg, Amy McMeans, Dr. Michael Miedema, Dr. JoEllyn Moore, Pamela Morley, Laura Onstot, Dr. Scott Sharkey, and Jolene Bell Makowesky have declared that they do not have any conflicts of interest associated with the planning of this activity. Dr. David Hurrell declares the following relationship –Boston Scientific: Chair, Clinical Events Committee.
We gratefully acknowledge the following organizations for their commercial support for this activity. Actelion Pharmaceutical Companies of
Johnson & Johnson Portola Pharmaceuticals
PLEASE SAVE A COPY OF THIS FLIER AS YOUR CERTIFICATE OF ATTENDANCE
Signature: __________________________________________________________________________ My signature verifies that I have attended the above stated number of hours of the CME activity.
Allina Health - Learning & Development - 2925 Chicago Ave - MR 10701 - Minneapolis MN 55407
Page 3 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Percutaneous coronary intervention for chronic total occlusions:Insights from a Multicenter International Registry.
Peter Tajti MD
Minneapolis Heart Institute, Abbott Northwestern Hospital, MN, USA
University of Szeged, Division of Invasive Cardiology, Second Department of Internal Medicine and Cardiology Center, Hungary
ACC 2018
1. Application of the Hybrid Approach for Percutaneous Coronary Interventions for Chronic Total
Occlusions: Update from an International Multicenter Registry.
2. Percutaneous Coronary Intervention In Patients With Previous Coronary Artery Bypass Graft Surgery:
Insights from a Multicenter Registry.
3. Procedural Outcomes of Multiple CTO Intervention Carried Out In the Same Procedure: Insight from a
Multicenter CTO Registry
4. Percutaneous Coronary Interventions for AortoOstial Chronic Total Occlusions: Insights from a
Multicenter Registry.
Page 4 of 40
MHIF CV Grand Rounds – Feb. 26, 2018
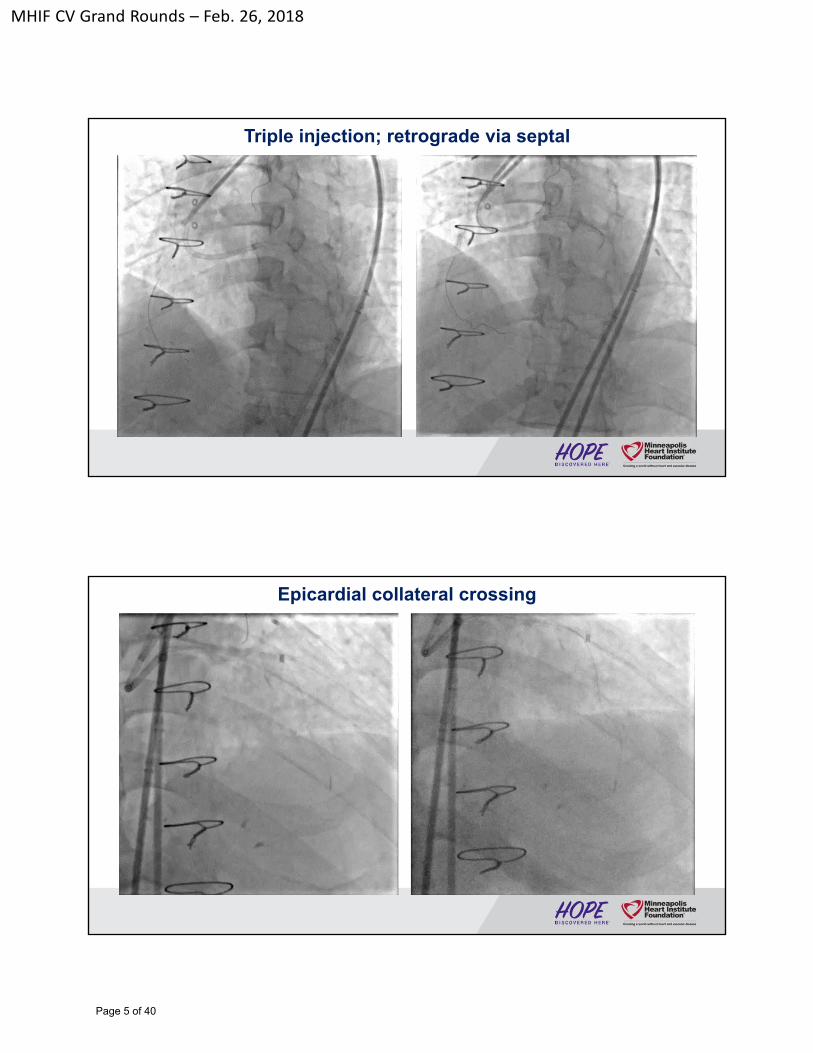
Triple injection; retrograde via septal
Epicardial collateral crossing
Page 5 of 40
MHIF CV Grand Rounds – Feb. 26, 2018
Final result
Page 6 of 40
MHIF CV Grand Rounds – Feb. 26, 2018
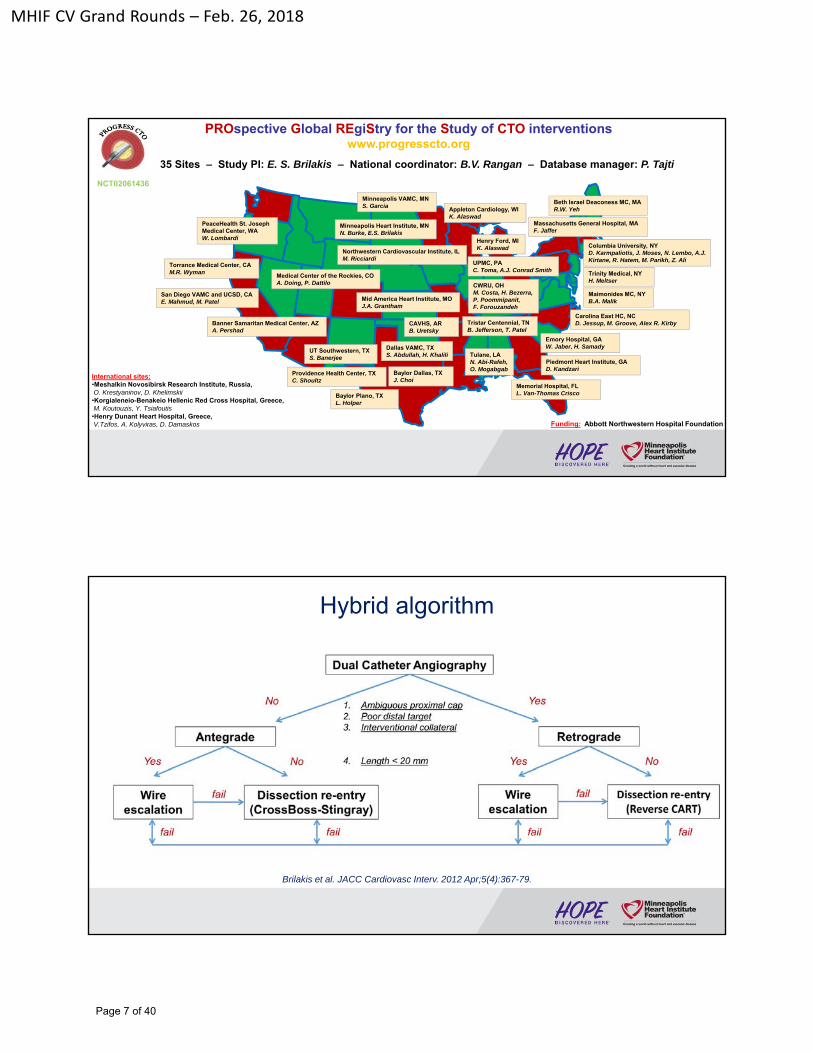
35 Sites – Study PI: E. S. Brilakis – National coordinator: B.V. Rangan – Database manager: P. Tajti
International sites:•Meshalkin Novosibirsk Research Institute, Russia, O. Krestyaninov, D. Khelimskii•Korgialeneio-Benakeio Hellenic Red Cross Hospital, Greece,M. Koutouzis, Y. Tsiafoutis•Henry Dunant Heart Hospital, Greece, V.Tzifos, A. Kolyviras, D. Damaskos Funding: Abbott Northwestern Hospital Foundation
Appleton Cardiology, WIK. Alaswad
Mid America Heart Institute, MO J.A. Grantham
Dallas VAMC, TXS. Abdullah, H. Khalili
Minneapolis VAMC, MNS. Garcia
Providence Health Center, TXC. Shoultz
PeaceHealth St. Joseph Medical Center, WA W. Lombardi Henry Ford, MI
K. Alaswad
CAVHS, ARB. Uretsky
Baylor Dallas, TXJ. Choi
Medical Center of the Rockies, COA. Doing, P. Dattilo
Tulane, LAN. Abi-Rafeh, O. Mogabgab
Piedmont Heart Institute, GAD. Kandzari
UT Southwestern, TXS. Banerjee
Northwestern Cardiovascular Institute, ILM. Ricciardi
Minneapolis Heart Institute, MN N. Burke, E.S. Brilakis
Baylor Plano, TXL. Holper
Banner Samaritan Medical Center, AZ A. Pershad
Memorial Hospital, FLL. Van-Thomas Crisco
Tristar Centennial, TNB. Jefferson, T. Patel
Emory Hospital, GAW. Jaber, H. Samady
UPMC, PAC. Toma, A.J. Conrad Smith
Trinity Medical, NYH. Meltser
Carolina East HC, NC D. Jessup, M. Groove, Alex R. Kirby
Maimonides MC, NYB.A. Malik
CWRU, OHM. Costa, H. Bezerra, P. Poommipanit, F. Forouzandeh
Columbia University, NYD. Karmpaliotis, J. Moses, N. Lembo, A.J. Kirtane, R. Hatem, M. Parikh, Z. Ali
San Diego VAMC and UCSD, CAE. Mahmud, M. Patel
Torrance Medical Center, CAM.R. Wyman
Massachusetts General Hospital, MAF. Jaffer
Beth Israel Deaconess MC, MAR.W. Yeh
PROspective Global REgiStry for the Study of CTO interventionswww.progresscto.org
NCT02061436
Hybrid algorithm
Brilakis et al. JACC Cardiovasc Interv. 2012 Apr;5(4):367-79.
Page 7 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
ACC 2018
1. Application of the Hybrid Approach for Percutaneous Coronary Interventions for Chronic Total
Occlusions: Update from an International Multicenter Registry.
2. Percutaneous Coronary Intervention In Patients With Previous Coronary Artery Bypass Graft Surgery:
Insights from a Multicenter Registry.
3. Procedural Outcomes of Multiple CTO Intervention Carried Out In the Same Procedure: Insight from a
Multicenter CTO Registry
4. Percutaneous Coronary Interventions for AortoOstial Chronic Total Occlusions: Insights from a
Multicenter Registry.
Application of the Hybrid Approach for CTO PCI
1. Appleton Cardiology, WI
2. Baylor Heart and Vascular Hospital, TX
3. Beth Israel Deaconess Medical Center, MA
4. Columbia University, NY
5. Central Arkansas VAMC, AR
6. Dallas VAMC/UTSW, TX
7. Henry Ford Hospital, MI
8. Korgialeneio-Benakeio Hellenic Red Cross General Hospital of Athens, Athens, Greece
9. Massachusetts General Hospital, MA
10. Medical Center of the Rockies, CO
11. Minneapolis VAMC, MN
12. Minneapolis Heart Institute, MN
13. Meshalkin Novosibirsk Research Institute, Novosibirsk, Russia
14. PeaceHealth St. Joseph MC, WA
15. Piedmont Heart Institute, GA
16. San Diego VAMC and UCSD, CA
17. St Luke’s Mid America Heart Institute, MO
18. The Heart Hospital Baylor Plano, TX
19. Torrance Medical Center, CA
20. UPMC Medical Center, PA
5/2012 to 12/201720 centers, 3,122 lesions in 3055 patients
87%
13%
Technical success Technical failure
Page 8 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Baseline patient demographics
Clinical characteristicsTechnical success
(n=2657)Technical failure
(n=398)p value
Age (years) * 64.6 ± 10.2 66.0 ± 9.6 0.014
Male gender 85% 89% 0.038
Diabetes 44% 40% 0.176
Dyslipidemia 92% 93% 0.678
Hypertension 90% 95% 0.004
Family history of CAD 33% 33% 0.842
CCS Angina Classification 0.477
• Class ≤1 12% 10%
• Class 2≤ 88% 90%
* mean ± SD; † median (IQR)
Baseline patient demographics
Clinical characteristicsTechnical success
(n=2657)Technical failure
(n=398)p value
Prior MI 45% 54% 0.002
Heart failure 29.71% 36% 0.016
Prior PCI 65% 71% 0.018
Prior CABG 31% 41% <0.001
Baseline creatinine (mg/dL) † 1.0 (0.9, 1.2) 1.1 (0.9, 1.3) 0.130
Prior CVD 12% 13% 0.457
Prior PAD 15% 18.29% 0.071
Left ventricular EF (%) † 55 (44, 60) 50 (40, 60) 0.036
* mean ± SD; † median (IQR)
Page 9 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Angiographic characteristicsTechnical success
(n=2711)Technical failure
(n=411)p value
Target vessel 0.064
• RCA 55% 57%
• LAD 25% 19%
• LCX 19% 23%
• Other 1% 1%
CTO length (mm)* 33.4 ± 24.1 37.8 ± 24.0 0.003
Proximal cap ambiguity 32% 54% <0.001
Blunt stump/no stump 51% 73% <0.001
Baseline angiographic characteristics
* mean ± SD; † median (IQR)
Angiographic characteristicsTechnical success
(n=2711)Technical failure
(n=411)p value
Side branch at proximal cap 48% 64% <0.001
Interventional collaterals 59% 44% <0.001
Moderate/severe calcification 52% 67% <0.001
Moderate/severe tortuosity 33% 45% <0.001
Previously failed CTO PCI 19% 27% <0.001
J-CTO score * 2.3 ± 1.3 3.1 ± 1.1 <0.001
PROGRESS-CTO score * 1.3 ± 1.0 1.8 ± 1.0 <0.001
PROGRESS complication score * 3.0 ± 1.9 3.5 ± 2.0 <0.001
Baseline angiographic characteristics
* mean ± SD; † median (IQR)
Page 10 of 40
MHIF CV Grand Rounds – Feb. 26, 2018
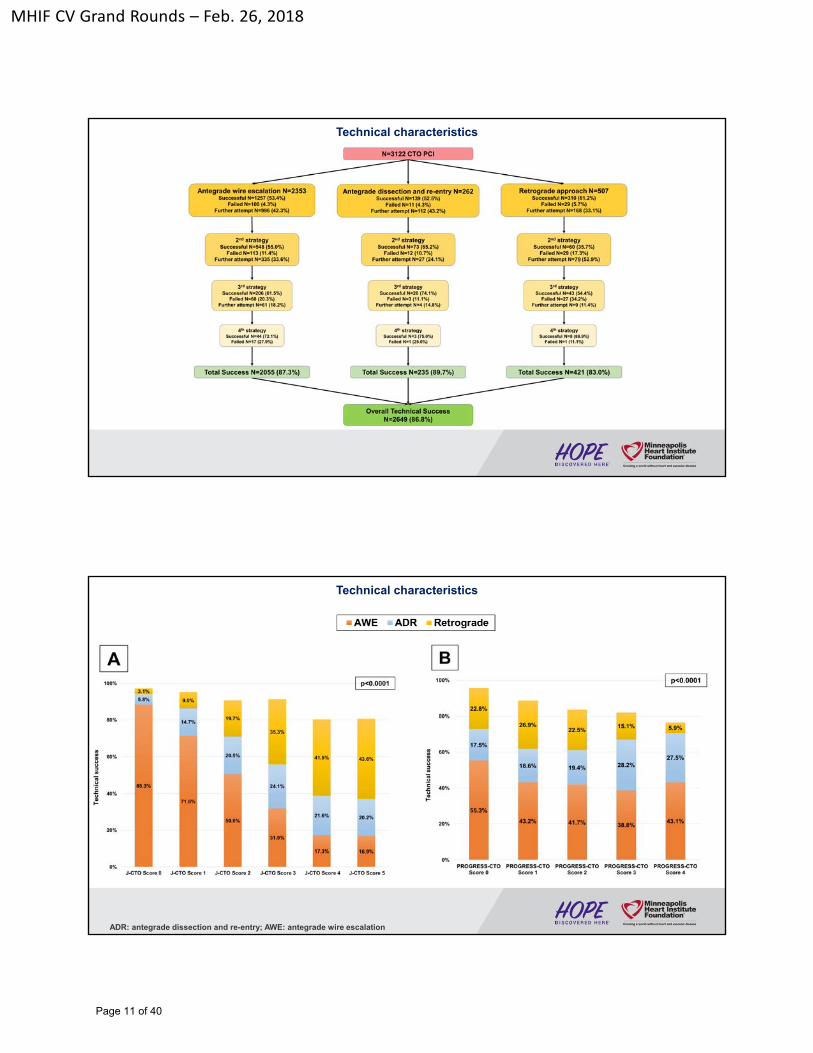
Technical characteristics
Technical characteristics
ADR: antegrade dissection and re-entry; AWE: antegrade wire escalation
Page 11 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Procedural outcomes Technical success Technical failure p value
Radial access 38% 33% 0.058
Femoral access 81% 85% 0.048
Procedure time (min) * 121 (80, 184) 140 (85, 224) <0.001
Contrast volume (mL) * 260 (200, 350) 300 (220, 400) <0.001
Fluoroscopy time (min) * 45.0 (27.3, 73.7) 66.0 (39.0, 93.6) <0.001
Patient AK dose (Gray) * 2.8 (1.6, 4.5) 3.9 (2.4, 6.0) <0.001
Number of stents †§ 2.4 ± 1.1 2.7 ± 1.6 0.556
Stent length (mm) †§ 71.7 ± 36.3 78.6 ± 47.6 0.660
Technical and procedural characteristics
* mean ± SD; † median (IQR)
§ Stents implanted: successful 97.10% vs. failed 4.89% PCIs, p<0.0001.
Procedural complications
ADR: antegrade dissection and re-entry; AWE: antegrade wire escalation; CABG: coronary artery bypass graft; MI: myocardial infraction; PCI: percutaneous coronary intervention
Page 12 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Annual CTO PCI volume
* mean ± SD; † median (IQR)
ACC 2018
1. Application of the Hybrid Approach for Percutaneous Coronary Interventions for Chronic Total
Occlusions: Update from an International Multicenter Registry.
2. Percutaneous Coronary Intervention In Patients With Previous Coronary Artery Bypass Graft
Surgery: Insights from a Multicenter Registry.
3. Procedural Outcomes of Multiple CTO Intervention Carried Out In the Same Procedure: Insight from a
Multicenter CTO Registry
4. Percutaneous Coronary Interventions for AortoOstial Chronic Total Occlusions: Insights from a
Multicenter Registry.
Page 13 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Percutaneous Coronary Intervention In Patients With Previous Coronary Artery
Bypass Graft Surgery: Insights from a Multicenter Registry.
5/2012 to 10/201720 centers, 2,860 lesions in 2,803 patients
32.8%
67.2%
Prior CABG No Prior CABG
Clinical characteristicsPrior CABG
(n=920)No Prior CABG
(n=1886)p value
Age (years) * 67.4 ± 9.2 63.5 ± 10.2 <0.001
Male gender 86.4% 84.3% 0.163
CAD presentation
<0.001• ACS 30.6% 22.2%
• Stabile angina 62.2% 65.1%
• Other 7.2% 12.7%
CCS angina score
<0.001• CCS 2 or more 92.4% 86.1%
• CCS <2 7.6% 13.9%
Diabetes 50.0% 39.6% <0.001
Dyslipidemia 96.8% 90.2% <0.001
Hypertension 94.2% 88.1% <0.001
Baseline patient demographics
* mean ± SD; † median (IQR)
Page 14 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Clinical characteristicsPrior CABG
(n=920)No Prior CABG
(n=1886)p value
Prior MI 55.7% 40.4% <0.001
Heart failure 37.7% 26.6% <0.001
Prior valve surgery or procedure 6.1% 1.6% <0.001
Prior PCI 74.5% 60.6% <0.001
eGFR (mL/min/1.73m^2) * 69.3 ± 21.3 74.5 ± 22.2 <0.001
Left ventricular EF (%) * 49.0 ± 12.9 50.7 ± 13.2 0.009
Baseline patient demographics
* mean ± SD; † median (IQR)
Baseline angiographic characteristics
* mean ± SD
Angiographic characteristics Prior CABG (n=938)No Prior CABG
(n=1924)p value
Target vessel
<0.001
RCA 55.7% 55.0%
LAD 16.1% 27.2%
LCX 26.6% 17.4%
Other 1.6% 0.5%
Bypassed target vessel 67.5% 0.0% <0.001
CTO length (mm) * 42.3 ± 29.0 30.1 ± 20.5 <0.001
Proximal cap ambiguity 40.7% 31.2% <0.001
Blunt stump/no stump 60.5% 50.0% <0.001
Page 15 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Baseline angiographic characteristics
* mean ± SD
Angiographic characteristics Prior CABG (n=938)No Prior CABG
(n=1924)p value
Interventional collaterals 57.9% 56.3% 0.495
Moderate/severe calcification 73.4% 46.8% <0.001
Moderate/severe tortuosity 46.7% 30.3% <0.001
Previously failed CTO PCI 19.7% 19.5% 0.890
J-CTO score * 2.9 ± 1.1 2.3 ± 1.3 <0.001
PROGRESS score * 1.5 ± 1.1 1.2 ± 1.0 <0.001
PROGRESS complication score * 3.8 ± 1.8 2.7 ± 1.9 <0.001
Technical characteristics
Technical characteristics Prior CABG (n=938) No Prior CABG (n=1924) p value
Dual injection 77.0% 65.8% <0.001
Balloon uncrossable 18.9% 7.8% <0.001
Balloon undilatable 15.4% 9.0% 0.013
IVUS used 43.3% 40.4% 0.248
Access site
• Radial access 33.7% 38.4% 0.015
• Bi-radial access 12.4% 14.9% 0.071
• Femoral access 90.5% 77.6% <0.001
• Bi-femoral access 61.2% 46.9% <0.001
Page 16 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
Crossing strategy used
73%
36%
55%
84%
30% 31%
0%
20%
40%
60%
80%
100%
AWE ADR Retrograde
38%
23%
38%
58%
21% 21%
0%
10%
20%
30%
40%
50%
60%
AWE ADR Retrograde
p<0.001 p<0.001
Prior CABG No prior CABG
Final crossing strategy
ADR: antegrade dissection and re-entry; AWE: antegrade wire escalation
82% 83%87% 89%
0%
20%
40%
60%
80%
100%
Procedural success Technical success
Prior CABG No prior CABG
Procedural outcomes
0.0
1.0
2.0
3.0
4.0
5.0
6.0
Prior CABG No prior CABG150
200
250
300
350
400
Prior CABG No prior CABG
Co
ntr
ast
volu
me
(ml)
Rad
iati
on
do
se (
Gra
y)
Radiation dose Contrast volume
p<0.001
p<0.001p<0.001
p<0.001
Page 17 of 40

MHIF CV Grand Rounds – Feb. 26, 2018
In-hospital major complications
In-hospitalMACE
Death Acute MI Stroke Re-PCI Re-CABGPericardiocen
tesisTamponade Perforation
Prior CABG 3.3% 1.1% 1.5% 0.1% 0.5% 0.2% 0.0% 0.1% 6.9%No prior CABG 2.8% 0.4% 1.0% 0.3% 0.3% 0.2% 1.3% 1.1% 3.2%
0%
2%
4%
6%
8%
p=0.039p<0.001
p<0.001
p=0.005
MACE: major adverse cardiac event; MI: myocardial infarction; PCI: percutaneous coronary intervention; CABG: coronary artery bypass graft
Conclusions
1. CTO PCI with using the hybrid approach : high procedural success, reasonably low
complication rate
2. Higher annual CTO PCI volume is associated with higher procedural success
3. Prior CABG patients are associated with lower procedural success and higher in-
hospital mortality
4. Immediate treatment of coronary perforation in prior CABG patients may result in
lower in-hospital mortality
Page 18 of 40
MHIF CV Grand Rounds – Feb. 26, 2018
Thank you for your attention!
Email: [email protected]
Phone: 612-295-5371
Page 19 of 40

MHIF CV Grand Rounds – February 26, 2018
Impact of the Commercial Introduction of Transcatheter Mitral Valve Repair on Mitral Surgical Practice
Hiroki Niikura, MDResearch scholar in the Valve Science Center
Mitral Regurgitation (MR)
Page 20 of 40

MHIF CV Grand Rounds – February 26, 2018
Background
Surgical treatment, with either mitral repair or valve replacement, is the standard of care for patients with severe MR who are symptomatic.
With the commercial introduction of transcatheter mitral valve repair with Mitraclip into the U.S. in 2013, there has been uncertainty regarding the effect of this therapy on mitral surgical practice.
The object of this study was to examine the impact (e.g. patient volume, outcomes) of the commercial introduction of Mitraclip on mitral surgical practice in a tertiary referral center.
Methods
• From January 2012 to December 2016, all patients who underwent surgical or transcatheter therapy for MR at our hospital were evaluated.
• This time period was chosen to examine surgical practice prior to and following the commercial introduction of MitraClip, which was approved for commercial use on October, 2013.
• The trend of patients volume, characteristics and outcomes were compared MitraClip with surgical repair/replacement.
Page 21 of 40

MHIF CV Grand Rounds – February 26, 2018
From January 2012 to December 2016at our hospital.
Methods
All(n=604)
Mitraclip(n=161)
Surgical repair/replacement
(n=443)p-value
Age (yrs) 69±14 83±7 64±12 <0.0001Male gender - (%) 367 (60.8) 85 (52.8) 282 (63.7) 0.02NYHA class Ⅲ or Ⅳ - (%) 289 (47.8) 148 (91.9) 141 (31.8) <0.0001
Medical history - (%)CAD 217 (35.9) 81 (50.3) 136 (30.7) <0.0001Hypertension 370 (61.3) 127 (78.9) 243 (54.9) <0.0001Diabetes mellitus 105 (17.4) 43 (26.7) 62 (14) <0.0001Atrial fibrillation 213 (35.3) 110 (68.3) 103 (23.3) <0.0001COPD 94 (15.6) 50 (31.1) 44 (9.9) <0.0001Prior MI 68 (11.3) 28 (17.4) 40 (9) 0.004Prior stroke 65 (10.8) 31 (19.3) 34 (7.7) 0.0001
Creatine, mg/dl 1.1±1.0 1.3±0.5 1.08±1.1 0.005Prior sternotomy 113 (18.7) 53 (32.9) 60 (13.5) <0.0001STS-PROM – (%) 3.8±5.0 7.2±2.5 2.5±4.5 <0.0001
Page 22 of 40

MHIF CV Grand Rounds – February 26, 2018
Patients demographicsAll
(n=604)Mitraclip(n=161)
Surgical repair/replacement
(n=443)p-value
Prior procedure - no. (%)
Prior sternotomy 113 (18.7) 53 (32.9) 60 (13.5) <0.0001
History of PCI 89 (14.7) 43 (26.7) 46 (10.4) <0.0001
History of CABG 61 (10.1) 39 (24.2) 22 (5) <0.0001
PM or ICD 64 (10.5) 35 (21.7) 29 (6.5) <0.0001
Medications - no. (%)
Aspirin 362 (59.9) 105 (65.2) 257 (58) 0.11
Anticoagulation 146 (24.2) 81 (50.3) 65 (14.7) <0.0001
Beta-receptor antagonist 299 (49.5) 113 (70.2) 186 (42) <0.0001
ACE-inhibitor or ARB 239 (39.6) 70 (43.5) 169 (38.1) 0.24
Diuretic 232 (38.4) 114 (70.8) 118 (26.6) <0.0001
STS-PROM – (%) 3.8±5.0 7.2±2.5 2.5±4.5 <0.0001
Echo demographicsAll
(n=604)Mitraclip(n=161)
Surgical repair/replacement
(n=443)p-value
Grade 3 or 4 Mitral regurgitation - (%) 558 (92.4) 160 (99.4) 398 (89.8) <0.0001
Effective regurgitant orifice (cm2) 0.48±0.29 0.46±0.3 0.49±0.29 0.42
Regurgltant volume (ml) 73.6±42.3 68.9±40.9 75.7±42.9 0.21
Mitral stenosis - (%) 50 (8.3) 2 (1.2) 48 (10.8) <0.0001
LVEF (%) 59.0±9.6 57.8±9.8 59.5±9.5 0.064
LVDd (cm) 5.1±1.5 5.1±2.5 5.2±0.8 0.48
LVDs (cm) 3.5±2.0 3.7±3.4 3.4±0.8 0.23
RVSP (mmHg) 35.7±13.8 41.3±13.9 33.3±13.0 <0.0001
Etiology of MR - (%)
Degenerative 467 (77.3) 128 (79.5) 339 (76.5) 0.44
Functional 42 (7) 7 (4.3) 35 (7.9) 0.13
Both degenerative and functional 7 (1.2) 3 (1.9) 4 (0.9) 0.33
Other 88 (14.6) 23 (14.3) 65 (14.7) 0.91
Page 23 of 40

MHIF CV Grand Rounds – February 26, 2018
(Year)
Annual volumes per year for procedures
Annual volumes per year for procedures
0
20
40
60
80
100
120
140
2012 2013 2014 2015 2016
All surgical mitral procedures Isolated mitral therapy MitraClip
The commercial introduction of MitraClip
(Year)
Nu
mb
er o
f P
atie
nts
14±2% / Year (P<0.001)
10±4% / year (P<0.001)
r=0.99, P<0.001
Page 24 of 40

MHIF CV Grand Rounds – February 26, 2018
Procedure and in-hospital outcome
Alln = 604
Mitraclipn = 161
Surgical repair/replacement
n = 443p value
Procedure success - (%) 98.1 98.1 99.3 0.19
Residual regurgitation grade ≦2 - (%) 561 (92.9) 134 (83.2) 427 (96.4) <0.0001
Mean gradient after procedure (mmHg) 4.6±2.2 4.1±2.1 4.8±2.1 <0.0001
In-hospital mortality - (%) 2.2 2.5 2 0.74
Length of stay after procedure (days) 6.5±4.2 3.4±4.1 7.5±3.7 <0.0001
Myocardial infarction - (%) 10 (1.7) 1 (0.6) 9 (2) 0.23
Stroke - (%) 13 (2.2) 4 (2.5) 9 (2) 0.74
New PPM and ICD implantation - (%) 32 (5.3) 0 32 (7.2) <0.0001
Major vascular complication - (%) 10 (1.7) 3 (1.9) 7 (1.6) 0.81
Survival at 30 days
MitraClip
Surgical repair/replacement
Log-rank test: p=0.24
Page 25 of 40

MHIF CV Grand Rounds – February 26, 2018
Survival at 30days
Mitraclip 96.3%
Surgical repair/replacement 98%
Log-rank test: p=0.24
Mitraclip 98.1%
Surgical repair/replacement 98.4%
Log-rank test: p=0.79
Freedom form Heart failure rehospitalization at 30days
Page 26 of 40

MHIF CV Grand Rounds – February 26, 2018
Mitraclip 94.4%
Surgical repair/replacement 96.4%
Log-rank test: p=0.28
Freedom from death and heart failure rehospitalization at 30days
Survival at 30 days
MitraClip
Surgical repair/replacement
Log-rank test: p=0.24
Page 27 of 40

MHIF CV Grand Rounds – February 26, 2018
Heart failure rehospitalization at 30 days
MitraClip
Surgical repair/replacement
Log-rank test: p=0.79
Death or heart failure rehospitalization at 30 days
MitraClip
Surgical repair/replacement
Log-rank test: p=0.28
Page 28 of 40

MHIF CV Grand Rounds – February 26, 2018
Conclusions
Transcatheter mitral valve repair could be introduced into a comprehensive valve center without detraction from surgery, and with growth in mitral surgical procedures and favorable clinical outcomes for treated patients.
Although the transcatheter patients were older, had more severe heart failure and comorbidities, the short-term outcomes were similar for transcatheter and surgical therapies.
Our findings demonstrate the potential benefits of complementary therapies in the treatment of patients with MR.
Page 29 of 40

MHIF CV Grand Rounds – February 26, 2018
Contemporary Reasons and Clinical Outcomes for Patients with Severe, Symptomatic Aortic Stenosis Not Undergoing Aortic Valve Replacement
Liang Tang, MD, Mario Gössl, MD, PhD, Aisha Ahmed, BS, Ross Garberich, MS, Steven M. Bradley, MD, MPH, Hiroki Niikura, MD, Dawn Witt, PhD, Wesley A. Pedersen, MD, Richard Bae, MD, John Lesser, MD, Kevin M. Harris, MD, Benjamin Sun, MD, Karol Mudy, MD, Paul Sorajja, MD
Valve Science Center, Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital
Disclosures
• I have no conflict of interest in relation to this presentation.
Page 30 of 40

MHIF CV Grand Rounds – February 26, 2018
Backgrounds
• Aortic stenosis (AS) affects 3 to 4% of people over 65 years of age, and therefore is expected to increase in prevalence with continued population aging. The mortality from untreated, symptomatic AS is comparable to or worse than that of many advanced malignancies.
• TAVR or SAVR is the only effective therapy and can be life-saving in appropriate patients. Nonetheless, a significant subset of these patients do not undergo appropriate therapy.
1. Nkomo VT, et al. Lancet. 2006; 368(9540):1005-1011.2. Iung B, et al. Eur Heart J. 2003; 24(13):1231-1243.3. Osnabrugge RL, et al. J Am Coll Cardiol. 2013; 62(11):1002-1012.
4. Varadarajan P, et al. Ann Thorac Surg. 2006; 82(6):2111-2115.5. Clark MA, et al. Circ Cardiovasc Qual Outcomes. 2012; 5(5):697-704.6. Thaden JJ, et al. Prog Cardiovasc Dis. 2014; 56(6):565-571. 7. Nishimura RA, et al. J Am Coll Cardiol.2014; 63(22):e57-185.
Objectives
• The present study was undertaken to determine the characteristics, clinical outcomes, and contemporary reasons for patients with severe, symptomatic AS not pursuing AVR.
• Our study aim was to gain insight into the barriers to appropriate care for patients with severe, symptomatic AS, in order to help guide efforts to improve the health of these patient populations.
Page 31 of 40

MHIF CV Grand Rounds – February 26, 2018
Methods
Inclusion criteria
1) Severe AS:
• calculated aortic valve area (AVA) < 1.0 cm2 or indexed AVA ≤0.6 cm2/m2, and
• MG ≥40 mm Hg or Vmax of ≥4 m/s, or
• Dimensionless index of <0.25.
2) Cardiac symptoms: dyspnea or other symptoms of heart failure, angina pectoris, syncope or pre-syncope
3) No AVR or balloon aortic valvuloplasty planned
Exclusion criteria
• Asymptomatic
• Patients with prior surgical or catheter-based aortic valve intervention
Study Population
All patients who were diagnosed with severe AS at the Allina Health system between January 2014 and March 2017 were considered for enrollment.
Nishimura RA, et al. J Am Coll Cardiol.2014; 63(22):e57-185.Martínez-Sellés M, et al. J Intern Med. 2014; 275(6):608-620.
Methods
Data Collection
• Medical record was manually reviewed for the clinical presentation, demographics, co-morbidities, rationale for no AVR therapy, and subsequent clinical outcomes.
• The rationale for the absence of AVR was determined by a thorough examination of all available clinical documentation, including records from primary care providers, cardiologists, surgeons, palliative care specialists, and any hospital records.
Page 32 of 40

MHIF CV Grand Rounds – February 26, 2018
MethodsDefinitions
1. Patients were classified into two groups:
• Appropriate (i.e., reasonable candidates for AVR)
• Medically futile (i.e., those likely to have no benefit from AVR).
2. Medical futility was defined as the presence of any of the following criteria:
• severe lung disease, severe liver disease (MELD >12), ESRD or dialysis treatment, excessive frailty, severe dementia, life-threatening malignancy(life expectancy ≤12 months), critical illness not related to AS, or any condition besides AS associated with a life expectancy of ≤12 months, as determined by the evaluating physicians and care providers.
All patients with severe AS confirmed by echo in the Allina Health System,January 2014 to March 2017
(n= 2,370 )
• 1,198 patients received SAVR• 386 patients received TAVR • 29 patients received PBAV• 10 patients planned to receive AVR ( 3 died
before TAVR)• 171 patients were asymptomatic• 22 Young patients with congenital severe AS• 6 patients with echocardiogram image
quality not well
Study population: Severe, symptomatic AS patients not received TAVR, SAVR or BAV
(n= 548)
Medical futile (n= 189)
Appropriate candidates for AVR (n= 359)
Exclude
Figure 1. Study flow chart
Results
Page 33 of 40

MHIF CV Grand Rounds – February 26, 2018
All
n=548
Appropriate
n=359
Futile
n=189
P-Value
Age, yrs 84.6 ± 9.4 84.2 ± 10.0 85.4 ± 7.9 0.15
Men — no. (%) 284 (51.8) 181 (50.4) 103 (54.5) 0.38
NYHA functional class — no. (%)
I 40 (7.3) 28 (7.8) 12 (6.3)
<0.001II 135 (24.6) 108 (30.1) 27 (14.3)
III 331 (60.4) 206 (57.4) 125 (66.1)
IV 42 (7.7) 17 (4.7) 25 (13.2)
Angina pectoris — no. (%) 42 (7.7) 28 (7.8) 14 (7.4) 0.96
Syncope or presyncope — no. (%) 73 (13.3) 53 (14.8) 20 (10.6) 0.17
Current smoker — no. (%) 21 (3.8) 12 (3.3) 9 (4.8) 0.41
Diabetes mellitus — no. (%) 166 (30.3) 101 (28.1) 65 (34.4) 0.13
Hypertension — no. (%) 446 (81.4) 292 (81.3) 154 (81.5) 0.97
Hyperlipidemia — no. (%) 347 (63.3) 229 (63.8) 118 (62.4) 0.75
Coronary artery disease — no. (%) 221 (40.3) 131 (36.5) 90 (47.6) 0.012
History of PCI — no. (%) 111 (20.3) 65 (18.1) 46 (24.3) 0.084
History of CABG — no. (%) 72 (13.1) 45 (12.5) 27 (14.3) 0.56
Previous MI — no. (%) 73 (13.3) 51 (14.2) 22 (11.6) 0.40
Atrial fibrillation — no. (%) 245 (44.7) 157 (43.7) 88 (46.6) 0.53
Cerebrovascular disease — no. (%) 103 (18.8) 67 (18.7) 36 (19.0) 0.91
Peripheral vascular disease — no. (%) 95 (17.3) 51 (14.2) 44 (23.3) 0.008
Table 1. Baseline clinical characteristics (n=548).Results
All
n=548
Appropriate
n=359
Futile
n=189
P-Value
Permanent pacemaker — no. (%) 61 (11.1) 39 (10.9) 22 (11.6) 0.78
Implanted defibrillator — no. (%) 16 (2.9) 10 (2.8) 6 (3.2) 0.80
Number of sternotomies ≥1 — no. (%) 74 (13.5) 46 (12.8) 28 (14.8) 0.52
COPD — no. (%) 84 (15.3) 43 (12.0) 41 (21.7) 0.003
Body mass index, kg/m2 27.9 ± 6.5 28.4 ± 6.7 26.9 ± 6.0 0.006
Anemia — no. (%) 361 (65.9) 218 (60.7) 143 (75.7) <0.001
Creatinine, mg/dL 1.5 ± 2.9 1.1 ± 0.3 2.3 ± 4.8 <0.001
eGFR, ml/min/1.73m2 47.4 ± 15.3 53.4 ± 9.3 36.9 ± 17.9 <0.001
Medication — no. (%)
Aspirin 334 (60.9) 223 (62.1) 111 (58.7) 0.44
P2Y12 receptor inhibitor 79 (14.4) 52 (14.5) 27 (14.3) 0.95
Anticoagulant therapy 164 (29.9) 109 (30.4) 55 (29.1) 0.76
ACEI/ARB 187 (34.1) 140 (39.0) 47 (24.9) 0.001
Beta-blockers 308 (56.2) 195 (54.3) 113 (59.8) 0.22
Diuretic 348 (63.5) 223 (62.1) 125 (66.1) 0.35
Aldosterone antagonist 18 (3.3) 12 (3.3) 6 (3.2) 0.92
STS-PROM, % 6.63 ± 4.99 5.46 ± 3.63 8.86 ± 6.31 <0.001
> 8% — no. (%) 162 (29.6) 74 (20.6) 88 (46.6)
<0.0014% ~ 8% — no. (%) 208 (38.0) 141 (39.3) 67 (35.4)
< 4% — no. (%) 178 (32.5) 144 (40.1) 34 (18.0)
Table 1. Baseline clinical characteristics (n=548).Results
Page 34 of 40
MHIF CV Grand Rounds – February 26, 2018
All
n=548
Appropriate
n=359
Futile
n=189
P-value
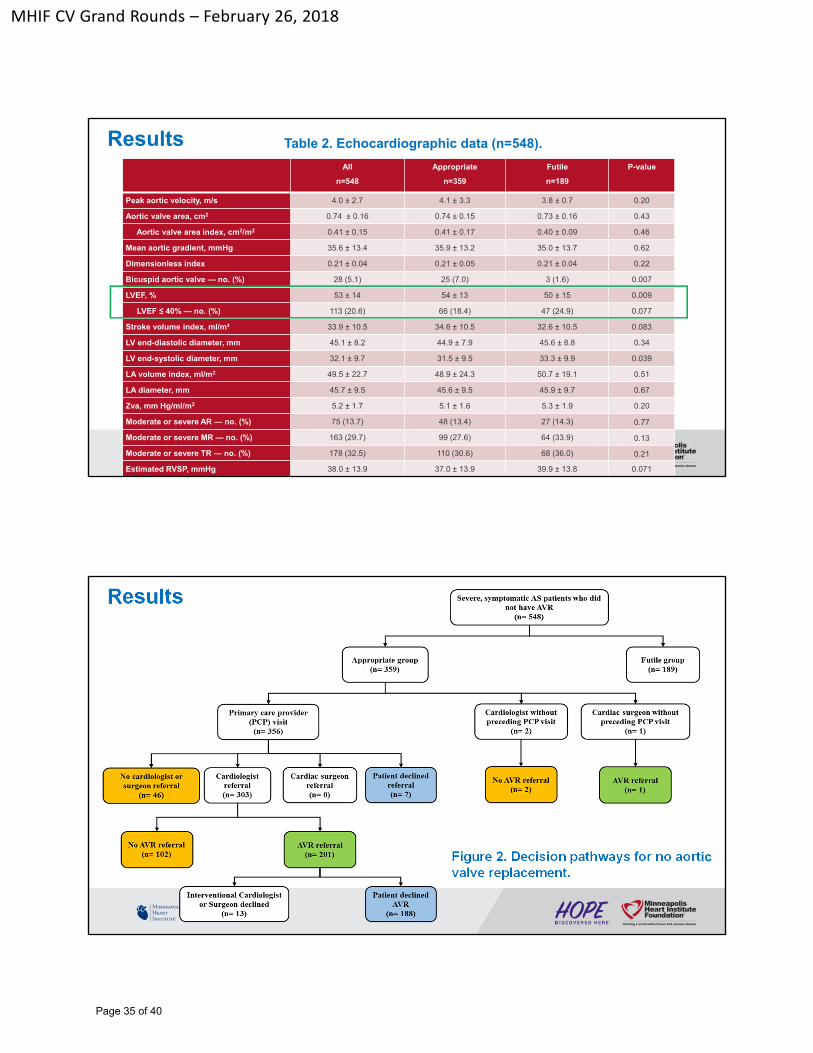
Peak aortic velocity, m/s 4.0 ± 2.7 4.1 ± 3.3 3.8 ± 0.7 0.20
Aortic valve area, cm2 0.74 ± 0.16 0.74 ± 0.15 0.73 ± 0.16 0.43
Aortic valve area index, cm2/m2 0.41 ± 0.15 0.41 ± 0.17 0.40 ± 0.09 0.46
Mean aortic gradient, mmHg 35.6 ± 13.4 35.9 ± 13.2 35.0 ± 13.7 0.62
Dimensionless index 0.21 ± 0.04 0.21 ± 0.05 0.21 ± 0.04 0.22
Bicuspid aortic valve — no. (%) 28 (5.1) 25 (7.0) 3 (1.6) 0.007
LVEF, % 53 ± 14 54 ± 13 50 ± 15 0.009
LVEF ≤ 40% — no. (%) 113 (20.6) 66 (18.4) 47 (24.9) 0.077
Stroke volume index, ml/m² 33.9 ± 10.5 34.6 ± 10.5 32.6 ± 10.5 0.083
LV end-diastolic diameter, mm 45.1 ± 8.2 44.9 ± 7.9 45.6 ± 8.8 0.34
LV end-systolic diameter, mm 32.1 ± 9.7 31.5 ± 9.5 33.3 ± 9.9 0.039
LA volume index, ml/m2 49.5 ± 22.7 48.9 ± 24.3 50.7 ± 19.1 0.51
LA diameter, mm 45.7 ± 9.5 45.6 ± 9.5 45.9 ± 9.7 0.67
Zva, mm Hg/ml/m2 5.2 ± 1.7 5.1 ± 1.6 5.3 ± 1.9 0.20
Moderate or severe AR — no. (%) 75 (13.7) 48 (13.4) 27 (14.3) 0.77
Moderate or severe MR — no. (%) 163 (29.7) 99 (27.6) 64 (33.9) 0.13
Moderate or severe TR — no. (%) 178 (32.5) 110 (30.6) 68 (36.0) 0.21
Estimated RVSP, mmHg 38.0 ± 13.9 37.0 ± 13.9 39.9 ± 13.8 0.071
Table 2. Echocardiographic data (n=548).Results
Figure 2. Decision pathways for no aortic valve replacement.
Results
Page 35 of 40

MHIF CV Grand Rounds – February 26, 2018
87.8
23.4
16.6 16.6
85.2
20.315.9 15.9
92.6
29.1
18.0 18.0
0
10
20
30
40
50
60
70
80
90
100
Cardiologyconsultation
Structuralinterventionalcardiologistconsultation
Surgicalconsultation
Heartteamevaluation
%ofpatients
AllAppropriateFutile
Figure 3. Proportion of patients seen by cardiovascular practitioner
p=0.012
p=0.528
p=0.021
p=0.528
Results
All
n=548
Appropriate
n=359
Futile
n=189
Patient or family refusal — no. (%) 221 (40.3) 196 (54.6) 25 (13.2)
AS incorrectly deemed not severe — no. (%) 56 (10.2) 47 (13.1) 9 (4.8)
Symptoms not attributable to AS — no. (%) 33 (6.0) 29 (8.1) 4 (2.1)
Mild symptoms — no. (%) 26 (4.7) 26 (7.2) 0 (0)
Malignancy — no. (%) 37 (6.8) 0 (0) 37 (19.6)
Excessive frailty — no. (%) 59 (10.8) 0 (0) 59 (31.2)
Critically ill not due to AS — no. (%) 85 (15.5) 0 (0) 85 (45.0)
No benefit due to short life expectancy — no. (%) 71 (13.0) 0 (0) 71 (37.6)
Dementia — no. (%) 36 (6.6) 0 (0) 36 (19.0)
Mental retardation — no. (%) 2 (0.4) 0 (0) 2 (1.1)
Severe pulmonary disease — no. (%) 29 (5.3) 0 (0) 29 (15.3)
Severe liver disease (MELD >12) — no. (%) 5 (0.9) 0 (0) 5 (2.6)
Porcelain aorta — no. (%) 1 (0.2) 1 (0.3) 0 (0)
Aortic annulus too large — no. (%) 3 (0.6) 3 (0.8) 0 (0)
LV apical thrombus — no. (%) 1 (0.2) 1 (0.3) 0 (0)
LAA and RAA massive thrombus — no. (%) 1 (0.2) 1 (0.3) 0 (0)
No medical insurance — no. (%) 3 (0.5) 3 (0.8) 0 (0)
Excessive obesity — no. (%) 1 (0.2) 1 (0.3) 0 (0)
Psychiatric disease — no. (%) 1 (0.2) 1 (0.3) 0 (0)
Table 3. Cited reasons for no aortic valve replacementResults
Page 36 of 40

MHIF CV Grand Rounds – February 26, 2018
40.3
10.2
64.7
54.6
13.1
8.1 7.2
13.2
4.82.1
00
10
20
30
40
50
60
Patientrefusal ASdeemednotsevere
SymptomsuncertainforAS
Mildorstablesymptoms
%ofpatients
Reasonsfornosurgicaltherapy
AllAppropriateFutile
Figure 4. The primary reasons for no surgical therapy. p<0.001
p=0.002p=0.004
p<0.001
Results
Results
Major adverse events All
n=548
Appropriate
n=359
Futile
n=189
P-Value
Death — no. (%) 300 (54.7) 162 (45.1) 138 (73.0) 0.000
Non-fatal MI — no. (%) 28 (5.1) 16 (4.5) 12 (6.4) 0.339
Non-fatal stroke — no. (%) 15 (2.7) 9 (2.5) 6 (3.2) 0.649
Rehospitalization for CHF — no. (%) 106 (19.3) 64 (17.8) 42 (22.2) 0.216
Table 5. Clinical outcomes.
Page 37 of 40

MHIF CV Grand Rounds – February 26, 2018
Figure 5A. Kaplan-Meier curve for survival free of all-cause mortality
Figure 5B. Kaplan-Meier curve for survival free of all-cause mortality and heart failure re-hospitalization
Results
Results
Figure 6A. Kaplan-Meier curve for survival free of all-cause mortality for appropriate patients stratified by STS-PROM group
Figure 6B. Kaplan-Meier curve for survival free of all-cause mortality and heart failure re-hospitalization for appropriate patients stratified by STS-PROM group
Page 38 of 40

MHIF CV Grand Rounds – February 26, 2018
Conclusion
• In this contemporary study, two-thirds of patients with severe symptomatic AS treated medically were appropriate AVR candidates and had poor outcomes.
• Most patients had incomplete heart team evaluations, and commonly had symptoms or lesion severity misinterpreted.
• Given the potential for beneficial outcomes among those untreated, further educational efforts to address these shortcomings are warranted.
Acknowledgments
I would like to express my sincere appreciation to:
• Dr. Paul Sorajja, Mario Gössl, Steven M. Bradley, John Lesser, Kevin M. Harris
• Ross Garberich
• Dawn Witt
• Aisha Ahmed
Page 39 of 40

MHIF CV Grand Rounds – February 26, 2018
Thank you!
Your advice will be highly appreciated!
Page 40 of 40