2017 htrc baltimore tendon transfers stern - asht 2017_htrc...• describe general goals,...
TRANSCRIPT

Tendon Transfers
Brocha Z. Stern, MOT, OTR/L, CHT
Curtis National Hand CenterBaltimore, MD
October 6-8, 2017
Objectives
• Describe general goals, principles, and mechanical considerations of tendon transfers
• Explain general preoperative and postoperative rehabilitative guidelines for tendon transfers
• Apply anatomical and surgical considerations to the rehabilitation of specific tendon transfers, with emphasis on median, ulnar, and radial nerve palsies
Fundamentals
(Brand, 2011; Brand, Beach, & Thompson, 1981; Brand & Hollister, 1985; Jones, 2013; Livermore & Tueting, 2016; Peljovich, Ratner, & Marino, 2010; Ratner & Kozin, 2011;
Sammer & Chung, 2009a, 2009b; Wilbur & Hammert, 2016)
Overview
• Restore balance that has been lost or compromised through disease or injury
• Indications
• Substitute for weak or paralyzed muscle
• Replace damaged tendon or muscle
• Correct muscle imbalance caused by CNS lesion
• Potential diagnoses
• Peripheral nerve injuries, cerebral palsy, spinal cord injury, thumb hypoplasia, rheumatoid arthritis
(http://www.ehealthstar.com/wp-content/uploads/2013/08/Froment-Sign.jpg)
Mechanism• “Altering the insertion or origin of a nearby, redundant,
strong, and voluntarily controlled muscle” (Pelojovich, Ratner, & Marino, 2010, p. 1365)
• Muscle is redirected by changing the insertion site of its tendinous portion
• Tendon-tendon coaptation
• Blood and nerve supply unaffected
**Differentiate from free muscle transfer or nerve transfer
(Baumeister, 2015; http://emedicine.medscape.com/article/1286712-treatment#d11)
Principles
• Donor properties• Must be expendable
• Adequate power to motor the recipient tendon
• Similar tendon excursion as the recipient
• Function synergistic with the recipient
• Normal PROM
• Tissue equilibrium
• Straight line of pull
• Single function per transfer

Strength & Work
• Strength• Ability to generate tension• Proportionate to cross-sectional area• Does not change with transfer
• Functional change in strength (~1 muscle grade)due to factors such as drag
• Work• Force x distance• Proportionate to muscle mass
(http
s://e
n.w
ikib
ooks
.org
/wik
i/Med
ical
_Phy
siol
ogy/
Cel
lula
r_P
hysi
olog
y/C
ell_
junc
tions
_and
_Tis
sues
)
Potential Excursion (Amplitude)
• The distance a muscle can contract if
• Freed from all its connective tissue attachments
• Stimulated from its fully stretched position
• Proportionate to muscle fiber length
• Dependent on number of sarcomeres in muscle fiber
(Wilhelmi, 2017; http://emedicine.medscape.com/
article/1245758-overview#a4)
Required Excursion
• The distance a muscle needs to contract to move the joint(s) through full range of motion
• Typically less than potential excursion• i.e. ECRB – 6 cm of potential excursion but only
~3.5 cm of required excursion
Wrist extensors and flexors 33 mm
Finger extensors 50 mm
Finger flexors 70 mm
Available Excursion
• The distance a muscle can contract as permitted by the surrounding connective tissue
• Varies from person to person• Dependent on recent use of joints and tendons
• Assessed intra-operatively after cutting tendon at its insertion
• Measured by stimulating after placement at full stretch
• Maintained with transfer only if minimal change in position and minimal scarring
Leverage
• Ability of a force to cause rotation on a lever
• Moment arm • Perpendicular distance between axis of rotation and
tendon as it crosses the joint
• Force Torque
• Torque = Force x moment arm
• Mechanical advantage• Moment arm of force / Moment arm of load• “Price of increased power is reduced range” (Brand, 2011)
Drag
• “Internal resistance in the form of friction and the need to stretch passive soft tissues” (Brand, 2011)
• Friction• Resisting force that occurs whenever two objects move
against each other
• Soft tissue• A transferred tendon becomes attached to its new area
by soft tissue• Living tissue has the ability to remodel or to grow in
response to mechanical force
(http
://oa
klan
dsps
.wik
isp
aces
.com
/fric
tion)

Synergy
• Facilitates post-operative retraining
• Increases excursion
(http://www.eatonhand.com/complic/figures/tenodesis2.htm)
Neuroplasticity
(Schultz, 2006, CC 3.0; https://commons.wikimedia.org/wiki/File:DTI-sagittal-fibers.jpg)
New Considerations
• Wide-awake surgery• “Tendon transfer is actually best indicated for such
wide-awake surgery” (Tang, 2015, p. 280)
• Improved ability to obtain optimal tension of transfer
Rehabilitation: General Guidelines
(Duff & Humpl, 2011; Schwartz, 2014)
(B. Stern)(B. Stern)
Preoperative Considerations
• Evaluation• Assess capabilities and impairments• Identify potential donor muscles• Establish goals
• Intervention• Increase joint and soft tissue mobility• Isolate and strengthen donor muscles• Orthosis fabrication• Patient education
(B. Stern)
Preoperative Evaluation
• History
• Physical Exam• AROM and PROM
• Note joint contractures
• Sensibility
• Manual muscle testing, grip/pinch• Observe muscle substitution or motor signs
• Motor learning aptitude
• Functional tests
(B. Stern)
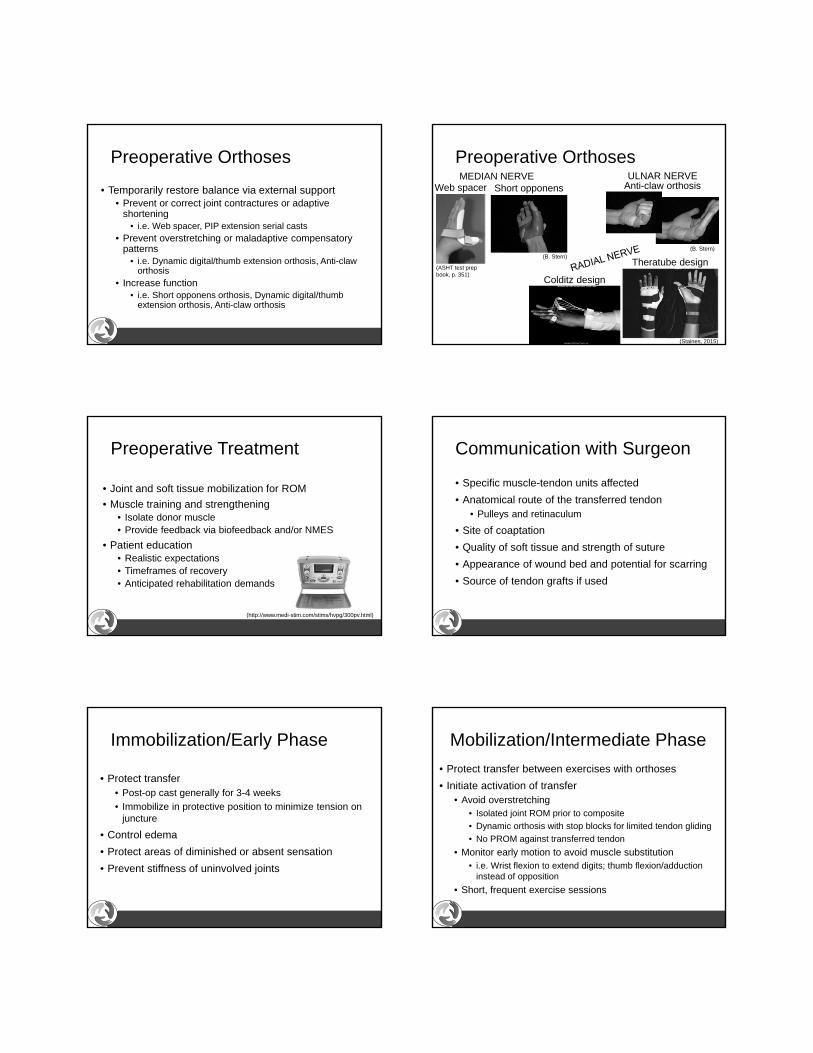
Preoperative Orthoses
• Temporarily restore balance via external support • Prevent or correct joint contractures or adaptive
shortening• i.e. Web spacer, PIP extension serial casts
• Prevent overstretching or maladaptive compensatory patterns
• i.e. Dynamic digital/thumb extension orthosis, Anti-claw orthosis
• Increase function• i.e. Short opponens orthosis, Dynamic digital/thumb
extension orthosis, Anti-claw orthosis
Short opponens
(B. Stern)
Preoperative Orthoses
Colditz design
Anti-claw orthosis
(B. Stern)
Web spacer
(ASHT test prep book, p. 351)
(Staines, 2015)
Theratube design
MEDIAN NERVE ULNAR NERVE
(http://www.medi-stim.com/stims/hvpg/300pv.html)
Preoperative Treatment
• Joint and soft tissue mobilization for ROM
• Muscle training and strengthening• Isolate donor muscle• Provide feedback via biofeedback and/or NMES
• Patient education• Realistic expectations• Timeframes of recovery• Anticipated rehabilitation demands
Communication with Surgeon
• Specific muscle-tendon units affected
• Anatomical route of the transferred tendon• Pulleys and retinaculum
• Site of coaptation
• Quality of soft tissue and strength of suture
• Appearance of wound bed and potential for scarring
• Source of tendon grafts if used
• Protect transfer• Post-op cast generally for 3-4 weeks
• Immobilize in protective position to minimize tension on juncture
• Control edema
• Protect areas of diminished or absent sensation
• Prevent stiffness of uninvolved joints
Immobilization/Early Phase
• Protect transfer between exercises with orthoses
• Initiate activation of transfer• Avoid overstretching
• Isolated joint ROM prior to composite
• Dynamic orthosis with stop blocks for limited tendon gliding
• No PROM against transferred tendon
• Monitor early motion to avoid muscle substitution• i.e. Wrist flexion to extend digits; thumb flexion/adduction
instead of opposition
• Short, frequent exercise sessions
Mobilization/Intermediate Phase

• Biofeedback and/or electrical stimulation (at sub-tetany contraction)
• Mobilize surrounding soft tissue to increase available excursion
• Scar management
• Sensory reeducation
• Introduce functional activities
Mobilization/Intermediate Phase• Add resistance to transfer
• Initiate when can activate transfer without assistance• Motion against gravity• Strengthen gradually• Continue to avoid muscle substitution patterns
• Restore passive motion• Gentle passive stretches, monitoring effect on transfer
• Focus on hand function• Blocked vs. random task practice• Feedback
Resistive/Late Phase
• Preoperative preparation
• Place and holds
• Start exercises in gravity eliminated plane
• Light tasks that result in unconscious activation• i.e. Opponensplasty – touch thumb to the SF tip
• Perform the original motion of the donor muscle• i.e. RF FDS FPL
Transfer Activation – Facilitation
(B. Stern)
Transfer Activation – Facilitation
• Tapping/vibration over muscle belly
• Biofeedback/NMES to encourage correct action
• Visual cues as adjunct
• Mirror visual feedback (Grangeon et al., 2010)
• Training orthoses • i.e. Lumbrical bar as assist following
intrinsic transfer
• Perform movements bilaterally
(B. Stern)
New Considerations
• Early mobilization • Systematic review• Within 1 week of surgery• Safe (no incidence of ruptures or pull-outs)• Improved hand function in short-term, reduced costs,
and decreased treatment time compared to immobilization
• Inconclusive findings for long-term outcomes(Sultana, MacDermid, Grewal, & Rath, 2013)
Common Tendon Transfers: Anatomy, Surgery, &
RehabilitationMedian, Ulnar, & Radial N. Injuries
(Chadderdon & Gaston, 2016; Cheah, Etcheson, & Yao, 2016; Cook, Gaston, & Lourie, 2016; Diaz-Garcia & Chung, 2016; Duff & Humpl, 2011; Giuffre, Bishop,
Spinner, & Shin, 2015; Isaacs & Ugwu-Oju, 2016; Ratner & Kozin, 2011; Sammer & Chung, 2009a, 2009b; Schwartz, 2014)
(Haymaker & Woodhall, 1953)
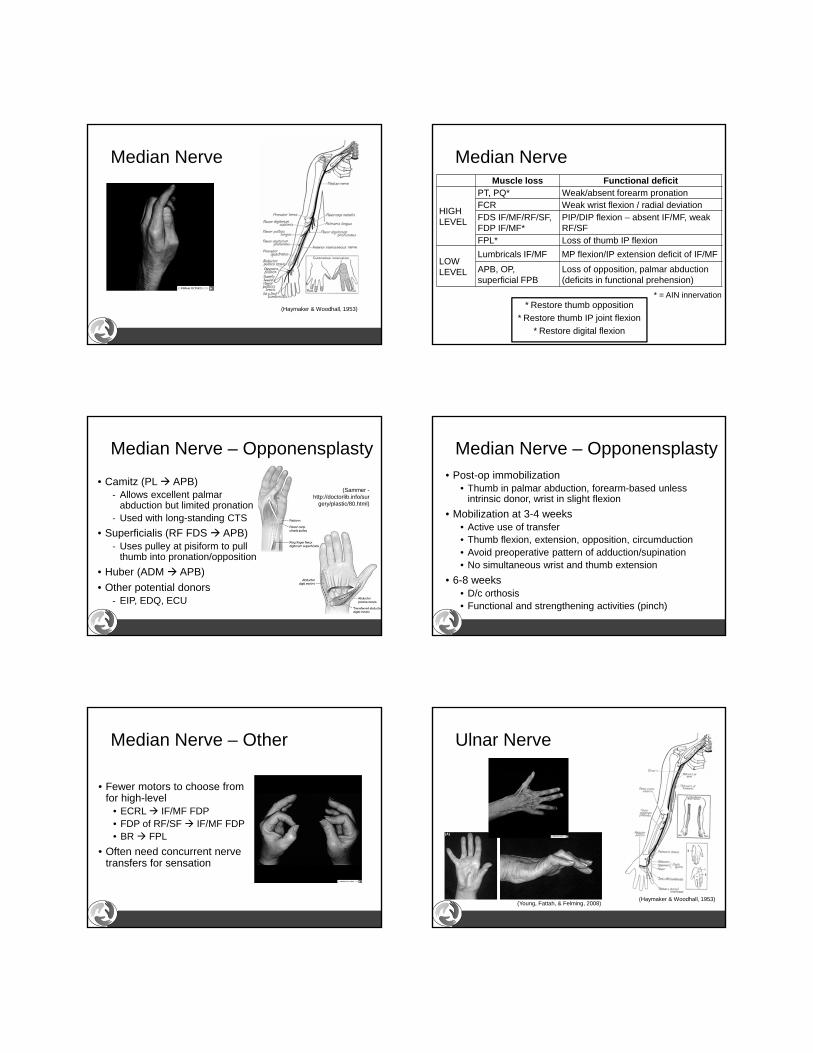
Median Nerve Median Nerve
* = AIN innervation
Muscle loss Functional deficit
HIGHLEVEL
PT, PQ* Weak/absent forearm pronationFCR Weak wrist flexion / radial deviationFDS IF/MF/RF/SF, FDP IF/MF*
PIP/DIP flexion – absent IF/MF, weak RF/SF
FPL* Loss of thumb IP flexion
LOW LEVEL
Lumbricals IF/MF MP flexion/IP extension deficit of IF/MF
APB, OP, superficial FPB
Loss of opposition, palmar abduction (deficits in functional prehension)
* Restore thumb opposition
* Restore thumb IP joint flexion
* Restore digital flexion
Median Nerve – Opponensplasty
• Camitz (PL APB)‐ Allows excellent palmar
abduction but limited pronation‐ Used with long-standing CTS
• Superficialis (RF FDS APB)‐ Uses pulley at pisiform to pull
thumb into pronation/opposition
• Huber (ADM APB)
• Other potential donors‐ EIP, EDQ, ECU
(Sammer -http://doctorlib.info/sur
gery/plastic/80.html)
Median Nerve – Opponensplasty• Post-op immobilization
• Thumb in palmar abduction, forearm-based unless intrinsic donor, wrist in slight flexion
• Mobilization at 3-4 weeks• Active use of transfer• Thumb flexion, extension, opposition, circumduction• Avoid preoperative pattern of adduction/supination• No simultaneous wrist and thumb extension
• 6-8 weeks• D/c orthosis• Functional and strengthening activities (pinch)
Median Nerve – Other
• Fewer motors to choose from for high-level
• ECRL IF/MF FDP• FDP of RF/SF IF/MF FDP• BR FPL
• Often need concurrent nerve transfers for sensation
Ulnar Nerve
(Haymaker & Woodhall, 1953)(Young, Fattah, & Felming, 2008)
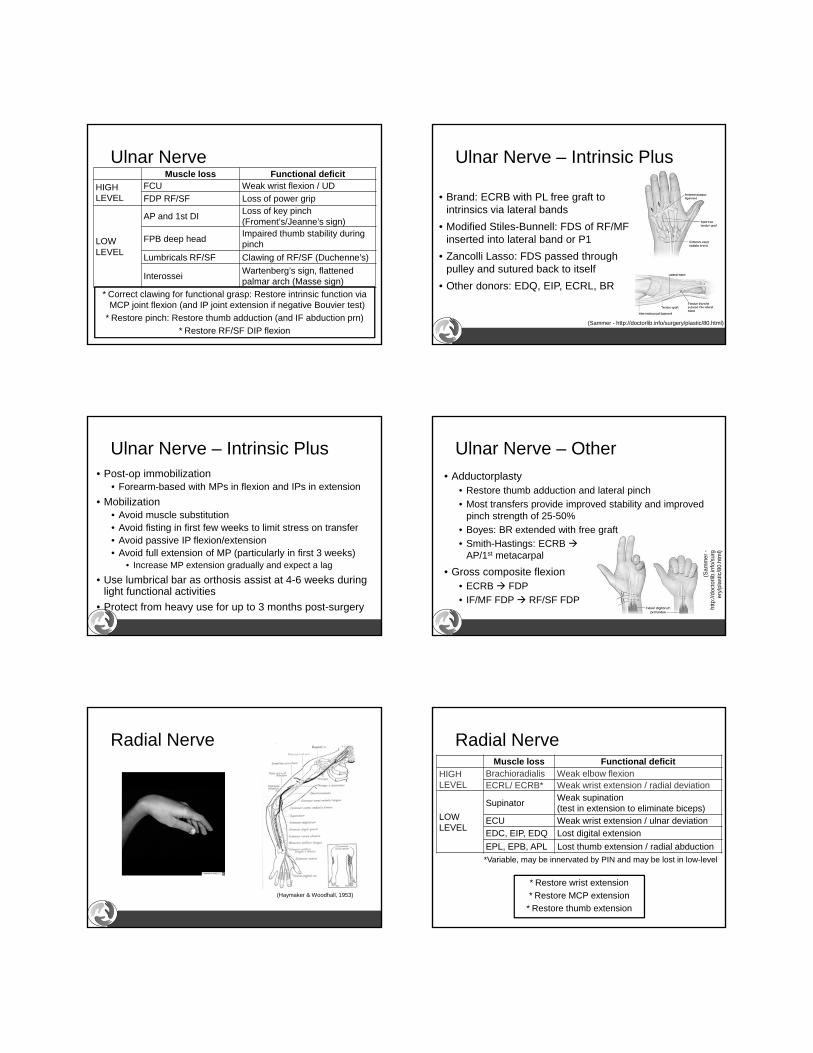
Ulnar NerveMuscle loss Functional deficit
HIGH LEVEL
FCU Weak wrist flexion / UD
FDP RF/SF Loss of power grip
LOW LEVEL
AP and 1st DILoss of key pinch (Froment’s/Jeanne’s sign)
FPB deep headImpaired thumb stability during pinch
Lumbricals RF/SF Clawing of RF/SF (Duchenne’s)
InterosseiWartenberg’s sign, flattened palmar arch (Masse sign)
* Correct clawing for functional grasp: Restore intrinsic function via MCP joint flexion (and IP joint extension if negative Bouvier test)
* Restore pinch: Restore thumb adduction (and IF abduction prn)
* Restore RF/SF DIP flexion
Ulnar Nerve – Intrinsic Plus
• Brand: ECRB with PL free graft to intrinsics via lateral bands
• Modified Stiles-Bunnell: FDS of RF/MF inserted into lateral band or P1
• Zancolli Lasso: FDS passed through pulley and sutured back to itself
• Other donors: EDQ, EIP, ECRL, BR
(Sammer - http://doctorlib.info/surgery/plastic/80.html)
Ulnar Nerve – Intrinsic Plus• Post-op immobilization
• Forearm-based with MPs in flexion and IPs in extension
• Mobilization• Avoid muscle substitution• Avoid fisting in first few weeks to limit stress on transfer• Avoid passive IP flexion/extension• Avoid full extension of MP (particularly in first 3 weeks)
• Increase MP extension gradually and expect a lag
• Use lumbrical bar as orthosis assist at 4-6 weeks during light functional activities
• Protect from heavy use for up to 3 months post-surgery
Ulnar Nerve – Other
• Adductorplasty• Restore thumb adduction and lateral pinch
• Most transfers provide improved stability and improved pinch strength of 25-50%
• Boyes: BR extended with free graft
• Smith-Hastings: ECRB AP/1st metacarpal
• Gross composite flexion• ECRB FDP
• IF/MF FDP RF/SF FDP
(Sam
mer
-ht
tp://
doct
orlib
.info
/sur
ger
y/pl
astic
/80.
htm
l)
Radial Nerve
(Haymaker & Woodhall, 1953)
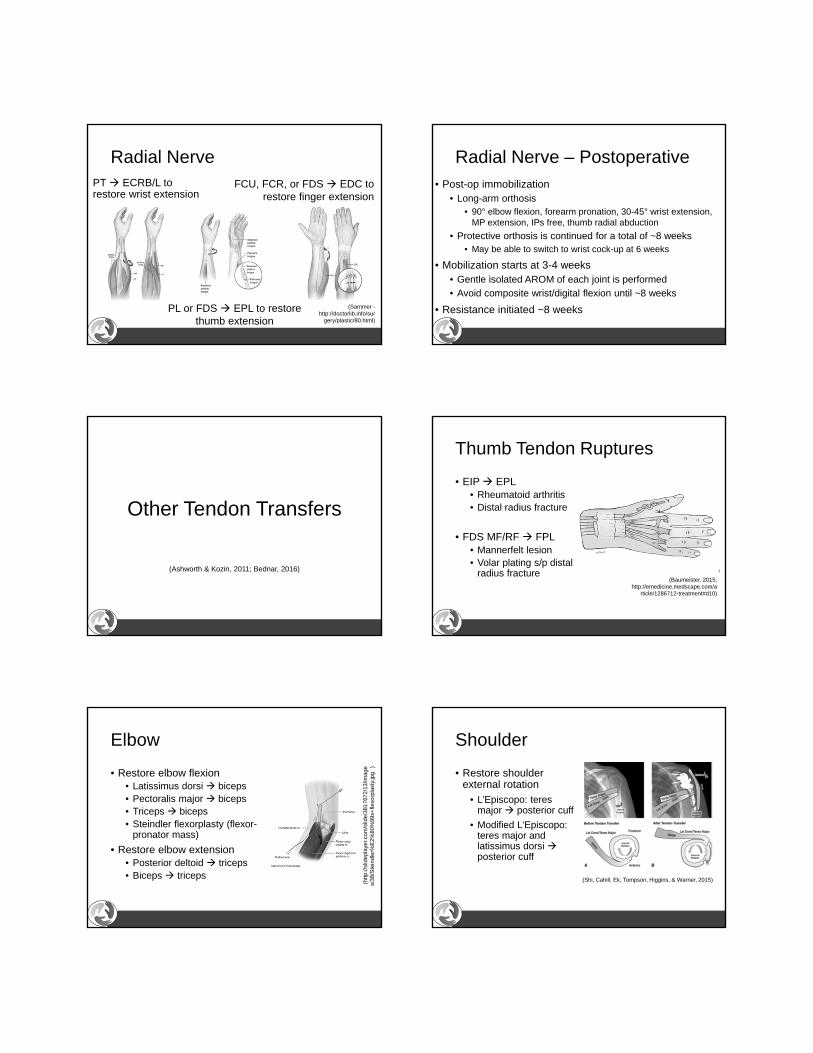
Radial Nerve
* Restore wrist extension
* Restore MCP extension
* Restore thumb extension
Muscle loss Functional deficitHIGH LEVEL
Brachioradialis Weak elbow flexionECRL/ ECRB* Weak wrist extension / radial deviation
LOWLEVEL
SupinatorWeak supination (test in extension to eliminate biceps)
ECU Weak wrist extension / ulnar deviationEDC, EIP, EDQ Lost digital extension
EPL, EPB, APL Lost thumb extension / radial abduction
*Variable, may be innervated by PIN and may be lost in low-level
Radial NervePT ECRB/L to restore wrist extension
FCU, FCR, or FDS EDC to restore finger extension
PL or FDS EPL to restore thumb extension
(Sammer -http://doctorlib.info/sur
gery/plastic/80.html)
Radial Nerve – Postoperative• Post-op immobilization
• Long-arm orthosis• 90° elbow flexion, forearm pronation, 30-45° wrist extension,
MP extension, IPs free, thumb radial abduction
• Protective orthosis is continued for a total of ~8 weeks• May be able to switch to wrist cock-up at 6 weeks
• Mobilization starts at 3-4 weeks• Gentle isolated AROM of each joint is performed
• Avoid composite wrist/digital flexion until ~8 weeks
• Resistance initiated ~8 weeks
Other Tendon Transfers
(Ashworth & Kozin, 2011; Bednar, 2016)
Thumb Tendon Ruptures
• EIP EPL• Rheumatoid arthritis• Distal radius fracture
• FDS MF/RF FPL• Mannerfelt lesion • Volar plating s/p distal
radius fracture(Baumeister, 2015;
http://emedicine.medscape.com/article/1286712-treatment#d10)
Elbow
• Restore elbow flexion• Latissimus dorsi biceps• Pectoralis major biceps• Triceps biceps• Steindler flexorplasty (flexor-
pronator mass)
• Restore elbow extension• Posterior deltoid triceps• Biceps triceps
(http
://sl
idep
laye
r.com
/slid
e/38
1767
2/13
/imag
es/
38/S
tein
dler
%E
2%80
%99
s+fle
xorp
last
y.jp
g)
Shoulder
• Restore shoulder external rotation
• L’Episcopo: teresmajor posterior cuff
• Modified L’Episcopo: teres major and latissimus dorsiposterior cuff
(Shi, Cahill, Ek, Tompson, Higgins, & Warner, 2015)

A Word (or Two) on Nerve Transfers
• Sensory and/or motor
• Potential advantages over tendon transfers• Restore sensation and motor• Restore function to multiple muscles• Preserve muscle balance• Avoid dissection to muscle bed, preserving excursion
• Limitation• More time-sensitive – cannot be done after motor end
plate degeneration (12-18 months)
References• Ashworth, S., & Kozin, S. H. (2011). Brachial plexus palsy reconstruction: Tendon
transfers, osteotomies, capsular release, and arthrodesis. In In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the hand and upper extremity (6th ed., pp. 792-812). Philadelphia, PA: Elsevier.
• Bednar, M. S., (2016). Tendon transfers for tetraplegia. Hand Clinics, 32, 389-396. doi:10.1016/j.hcl.2016.03.013
• Brand, P. W. (2011). Mechanics of tendon transfers. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the hand and upper extremity (6th ed., supplemental chapter available online.). Philadelphia, PA: Elsevier.
• Brand, P. W., & Hollister, A. (1985). Clinical mechanics of the hand (2nd ed.). St Louis: Mosby.
• Brand P. W., Beach, R. B., & Thompson, D. E. (1981). Relative tension and potential excursion of muscles in the forearm and hand. Journal of Hand Surgery, 6A, 209-219.
• Chadderton, R. C., & Gaston, R. G. (2016). Low median nerve transfers (opponensplasty). Hand Clinics, 32, 349-359. doi:10.1016/j.hcl.2016.03.005
• Cheah, A. E., Etcheson, J., & Yao, J. (2016). Radial nerve tendon transfers. Hand Clinics, 32, 232-338. doi:10.1016/j.hcl.2016.03.003
• Cook, S., Gaston, R. G., & Lourie, G. M. (2016). Ulnar nerve tendon transfers for pinch. Hand Clinics, 32, 369-376. doi:10.1016/j.hcl.2016.03.007
• Diaz-Garcia, R. J., & Chung, K. C. (2016). A comprehensive guide on restoring grasp using tendon transfer procedures for ulnar nerve palsy. Hand Clinics, 32, 361-368. doi:10.1016/j.hcl.2016.03.006
• Duff, S. V., & Humpl, D. (2011). Therapist’s management of tendon transfers. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the hand and upper extremity (6th ed., pp. 781-791). Philadelphia, PA: Elsevier.
• Grangeon, M., Guillot, A. , Sancho, P. O., Picot, M., Revol, P., Rode, G., & Collet, C. (2010). Rehabilitation of the elbow extension with motor imagery in a patient with quadriplegia after tendon transfer. Archives of Physical Medicine and Rehabilitation, 91, 1143-1146. doi:10.1016/j.apmr.2010.04.011
• Isaacs, J., & Ugwu-Oju, O. (2016). High median nerve injuries. Hand Clinics, 32, 339-348. doi:10.1016/j.hcl.2016.03.004
• Jones, N. F. (2013). Tendon transfers in the upper extremity. In P. C. Neligan(Ed.), Plastic surgery (3rd ed., pp. 745-776.e3). London: Elsevier.
• Livermore, A., & Tueting, J. L. (2016). Biomechanics of tendon transfers. Hand Clinics, 32, 291-302. doi:10.1016/j.hcl.2016.03.011
• Meals, C. G., & Meals, R. A. (2013). Tendon versus nerve transfers in elbow, wrist and hand reconstruction: A literature review. Hand Clinics, 29, 393-400. doi:10.1016/j.hcl.2013.04.010
• Peljovich, A., Ratner, J. A., & Marino, M. (2010). Update of the physiology and biomechanics of tendon transfer surgery. Journal of Hand Surgery, 35A, 1365-1369. doi:10.1016/j.jhsa.2010.05.014
• Ratner, J. A., & Kozin, S. H. (2011). Tendon transfers for upper extremity peripheral nerve injuries. In T. M. Skirven, A. L. Osterman, J. M. Fedorczyk, & P. C. Amadio (Eds.), Rehabilitation of the hand and upper extremity (6th ed., pp. 771-780). Philadelphia, PA: Elsevier.
• Sammer, D. M., & Chung, K. C. (2009). Tendon transfers part I: Principles of transfer and transfers for radial nerve palsy. Plastic Surgery and Reconstruction, 123, 169e-177e. doi:10.1097/PRS.0b013e3181a20526
• Sammer, D. M., & Chung, K. C. (2009). Tendon transfers part II: Transfers for ulnar nerve palsy and median nerve palsy. Plastic Surgery and Reconstruction, 124, 212e-221e. doi:10.1097/PRS.0b013e3181b037c7
• Schwartz, D. A. (2014). Tendon transfers. In Cooper, C. (Ed)., Fundamentals of hand therapy (2nd ed., pp. 438-456). St. Louis, MO: Elsevier.
• Sultana, S. S., MacDermid, J. C., Grewal, R., & Rath, S. (2013). The effectiveness of early mobilization after tendon transfers in the hand: A systematic review. Journal of Hand Therapy, 26, 1-20. doi:10.1016/j.jht.2012.06.006
• Tang, J. B. (2015). Wide awake flexor tendon repair, tenolysis, and tendon transfer. Clinics in Orthopedic Surgery, 7, 275-281. doi:10.4055/cios.2015.7.3.275
• Wilbur, D., & Hammert, W. C. (2016). Principles of tendon transfers. Hand Clinics, 32, 283-289. doi:10.1016/j.hcl.2016.03.001
References – Images • American Society of Hand Therapists. (2014). Test Prep for the CHT Exam (3rd ed.). Mt.
Laurel, NJ: Author.• Baumeister, S. (2015). Hand tendon transfers. Retrieved from Medscape,
http://emedicine.medscape.com/article/1286712-overview#showall• Haymaker, W. & Woodhall, B. (1953). Peripheral nerve injuries (2nd revised ed.).
Philadelphia, PA: Saunders.• Sammer, D. M. (n. d.). Principles of tendon transfers. Retrieved from
http://doctorlib.info/surgery/plastic/80.html• Shi, L. L., Cahill, K. E., Ek, E. T., Tompson, J. D., Higgins, L. D., & Warner, J. J. P.
(2015). Latissimus dorsi and teres major transfer with reverse shoulder arthroplasty restores active motion and reduces pain for posterosuperior cuff dysfunction. Clinical Orthopaedics and Related Research, 473, 3212-3217. doi:10.1007/s11999-015-4433-4
• Staines, K . G. (2015). Low-profile theratube splint for radial nerve palsy. ASHT Times, 22, 34-37.
• Wilhelmi, B. J. (2017). Tendon transfers. Retrieved from Medscape, http://emedicine.medscape.com/article/1245758-overview
• Young, P., Fattah, A., & Fleming, A. S. (2008). Ulnar nerve palsy after carpal tunnel decompression: Case report and review of the literature. Indian Journal of Plastic Surgery, 41, 73-75. doi:10.4103/0970-0358.41117
• When designated, images are courtesy of Primal Pictures

Contact Info
Brocha Z. Stern, MOT, OTR/L, CHT
PhD Candidate, New York University, NY, NY
Kessler Rehabilitation Center, NJ