2015 john gregg-navigate-menopause mkt research australia
TRANSCRIPT

PROJECT POKERMeasuring The Menopause
And VMS Market AndPotential Uptake Of XXXXXX
Prepared for:
Client XXXX Pharmaceuticals
Prepared by:
Navigate Consulting
June 24th, 2015

Contents
Research Background ......................................................................................................................................... 3
Overall Research Approach .............................................................................................................................. 4
Research Aims ....................................................................................................................................................... 5
RESARCH FINDINGS ..................................................................................................................................... 9
SECTION 1 - Our Sample In Context................................................................................................. 11
SECTION 2 – Menopausal Patient Population .................................................................................. 19
SECTION 3 – Menopausal Management .......................................................................................... 23
SECTION 4 – SSRI/SNRI Usage In Focus ............................................................................................. 34
SECTION 5 – XXXX In Focus ............................................................................................................... 43
SECTION 6 – Uptake Levels ................................................................................................................ 49
SECTION 7 – Brand Perceptions ......................................................................................................... 56
Driver Analysis .......................................................................................................................................62
CONCLUSIONS AND RECOMMENDATIONS ............................................................................................. 76
APPENDIX ................................................................................................................................................... 85
Spine Data .....................................................................................................................................................86
Frequency Data ...........................................................................................................................................93

Research Background
Therapies approved for the treatment of Vasomotor Symptoms (VMS) at present only include
hormone or oestrogen therapy (HT). These treatments offer high levels of symptom relief and are
considered the benchmark for comparison for any new market entrant in terms of efficacy.
However, recent media and medical controversy surrounding HT has lead to a significant fall in
usage levels and it is understood that both women and doctors are conservative in their approach
to these therapies. Certain groups of women are also contraindicated to HT such as menopausal
women with ER positive breast cancer or a strong family history of breast cancer, amongst others.
At present there are no non-hormonal therapies indicated for the treatment of VMS, although it is
thought that physicians are looking outside the available therapies with many off label prescriptions
written for VMS. Products utilised off label currently include Efexor (venlafaxine) and Aropax
(paroxetine), which belong to the SNRI / SRRI class of antidepressants, and other agents such as
Neurontin, an anti-convulsant agent, and Catapres, an anti-migraine agent.
XXXX (des-venlafaxine) is an active metabolite of Wyeth’s parent compound – Efexor. At present
trials are being undertaken to evaluate its usefulness in the treatment of VMS and results are
anticipated to be extremely positive for XXXX. It is anticipated that XXXX will compete with not
only HT’s but also Efexor and other off-label prescribing.
Due to the large number of off-label prescriptions and OTC therapies utilised in the treatment of
VMS, accurately defining the potential market for XXXX is not feasible via secondary data sources.
Therefore, primary market research is required to assess the potential market by sizing the total
female population experiencing the menopause and VMS and current treatment algorithms. The
research is also required to understand interest levels in XXXX, project adoption levels, and impact
on Efexor usage as well as to assess uptake under various reimbursement scenarios.

Research Aims
Developing a solid knowledge base in order to optimise the XXXX offering.
To size and define the menopausal
market with a particular focus on the
VMS cluster of symptoms
To profile current treatment
behaviours and usage levels of both
prescription and non-prescription
medications:
– including current usage of
SNRIs/SSRIs and positioning
within the competitive set
To gauge interest in, potential
adoption levels and likely success of
XXXX, including levers and barriers to
usage
To determine uptake of XXXX under
various reimbursement scenarios.
GP Consumer
Determine the incidence of the
Australian VMS market
Measure the number of patients on
prescription and non-prescription
therapy options and their related cost

A comprehensive approach.
Overall Research Approach
In looking at the research aims, we used a two pronged approach:
GP Research
Understanding GPs current treatment
approach, attitudes and interest
in XXXX Measuring the GP menopause and
VMS market and therapeutic
approach to scope potential markets
– measuring the patient population under GP care
– profiling treatment algorithms and current SNRI/SSRI usage within the competitive set
– gauging interest and uptake of XXXX– evaluating uptake of XXXX under
various reimbursement scenarios
Consumer Omnibus
Understanding usage and costs from
consumer perspective
– number of patients suffering from the
condition
– symptom’s suffered from the condition
– number of patients currently treated
with prescription medications
– number of patients on prescription
medication and/or OTC therapies and
their current costs to patients

Research Approach - GPs
Logistics:
– 30 minute survey
– all interviews conducted by trained medical interviewers
– all interviewers personally briefed by Navigate
– all respondents incentivised to encourage participation
– fieldwork conducted w/c 22nd April - w/c12th May, 2015
Sample:
– n=150 GPs
– representative Australian wide sample
– all aged between 30-69 years old
– treat 10 or more patients who currently experience symptoms of menopause or
perimenopause
– treat 5 or more patients per week who currently experience symptoms of menopause
or perimenopause
Methodology:
– CATI (Computer Assisted Telephone Interview)

What Our GP Sample Represents...
The 150 GPs we interviewed represent 14,760 GPs nation wide.
n=18,000 GPs
Target in Australia
n=14,760
Qualifying GPs
5%
participated
95%
declined
to
participate
18%
did not
qualify82%
qualified
3665 phone contacts 182 participants

Research Methodology - Consumers
Methodology:
– telephone omnibus
Sample:
– n=611 females
– all aged between 40-64 years
– representative sample Australia wide
– once prevalence established, those experiencing symptoms of menopause
to continue
Logistics:
– interviews conducted form central location
– conducted by trained interviewers
– research conducted 26th - 31st May and 2nd - 4th June, 20013

CONCLUSIONS AND
RECOMMENDATIONS

Conclusions
In the 40-64 year age group, around three quarters of women are suffering from
menopausal or perimenopausal symptoms. From the consumer omnibus this translates
into 2.4million potential menopausal patients
Though the type and prevalence of symptoms suffered varies by age, patient reporting
is much in line with GP perceptions… led by hot flushes, fatigue, difficulty sleeping and
night-time sweating. GPs note higher incidence of vaginal atrophy, mood swings and
disruption of quality of life - perhaps skewed by consultations with the more impacted
women in this age group.
Only around a tenth of patients are referred to a specialist (generally Gynaecologist or
Endocrinologist) but only a quarter of these then continue to be managed by the
specialist. This illustrates that menopausal management and treatment is well within the
GP realm and remit.

Conclusions (Cont’d)
Currently, HRT is the most widely employed and preferred treatment for menopausal
symptoms but around a third of patients are taking OTC or herbal remedies. Also some
off-label use of SSRI/SNRI classes noted, mostly Zoloft and Efexor:
38
29
10
10
Total prescribing: 1.2 products
% of patients treated:76%
HRT
OTC/Herbal remedies
Livial
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
SSRIs/SNRIs
Treatment Options
1
1

Conclusions (Cont’d)
GPs estimate that 76% of their menopausal patients are currently being treated…this
represents 1.8 million patients in total. In addition, a further fifth (<.5million) of their
menopausal patients choose not to be treated with prescription medications.
Consumer data indicates this could be higher, especially amongst younger women,
with 55% not treating and 22% utilising OTC remedies. It is not that those using OTC
treatments are suffering less - they still experience an average of nine symptoms each.
Already, GPs are employing the SSRI/SNRI classes in the treatment of menopausal
symptoms for more than just their affect on psychological symptoms, though they do
claim that 74% of women have depressive symptoms when initiated. Beyond that, GPs
see benefits for VMS, hot flushes and fatigue as well as providing an alternative to HRT
and its perceived risks.
They have been encouraged to use SSRI/SNRIs in the management of the menopause
by data in the literature and specialist advice and usage.
Key concerns are side effects, stigma and the fact that the anti-depressants alone can
not treat all symptoms of the menopause.

Conclusions (Cont’d)Much of this is echoed in GPs reactions to the unbranded XXXX profile - which has high appeal
to the GPs. Benefits are seen over and above those of the SSRI/SNRI classes and HRT with XXXX
seen to hold equal efficacy in both physical and psychological symptoms. Coupled with its
good tolerability profile, it makes an attractive addition to GPs armamentarium.
These positive perceptions result in good potential uptake for XXXX,and not surprisingly the PBS
scenario represents the best opportunity for XXXX, where it will not only gain new patients but
also take share from HRT especially:
With XXXX
HRT
OTC/Herbal remedies
Livial
SSRIs/SNRIs
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
Total prescribing: 1.2 products
27
28
24
8
7
XXXX
100%
Source Of
XXXX Volume
40
18
10
11
3
16
2
1
1
% of patients treated:
38
29
10
10
Current
1
1
1.2 products
New
80%76%

Conclusions (Cont’d)
This creates a clear positioning for XXXX to consider moving forward….selling the
benefits of both sets of symptoms will be a hook for XXXX prescribing in this market.
Looking forward to the future, it is clear that the cost, or PBS reimbursement status, of
XXXX will have a real impact on its uptake. GPs also feel that even at the lower private
script price of $40, an average of 50% of patients will refuse XXXX. This is not surprising
when considered in the context of the consumer feedback as most are spending less
than $30 a month on OTC or non-hormonal prescriptions.
Perceptual brand maps clearly show that while XXXX is perceived to be closer to
SSRI/SNRI classes than HRT on various attributes, it in fact straddles the two markets and
is seen to hold attributes of both. Already, XXXX is associated with few side effects and
being a low risk option as well as being useful in menopausal patients.

Conclusions (Cont’d)
Along with uptake levels, drivers for prescribing menopausal medications also vary
depending which market scenario is presented, but it is clear that confidence in the
new product and safety profile will be key selling messages for XXXX:
Secondary:
Primary:
Not
important:
$75
Confidence 13%
Efficacy in
menopausal 11%
Quality of life 9%
Not expensive 9%
Not reluctant to take 8%
Flexible 8%
Easy to dosing 3%
Usefulness 20%
Fast onset 19%
No HRT/Oestrogen, Safety,
Efficacy in depression
$40
Quality of life 7%
Not reluctant to take 6%
No HRT/Oestrogen 5%
Confidence 37%
Safety 18%
Efficacy in
menopausal 16%
Easy dosing 12%
Flexibility, Usefulness, Fast
onset, Efficacy in
depression, Not expensive
Authority
Easy dosing 7%
Efficacy in depression 7%
Quality of life 5%
PT Not reluctant
to take 4%
No HRT/Oestrogen 4%
Fast onset 4%
Usefulness 4%
Confidence 26%
Safety 14%
Efficacy in
menopausal 13%
Flexibility 11%
Not expensive
PBS
Usefulness 8%
No HRT/Oestrogen 8%
Efficacy in
menopausal 7%
Flexibility 6%
Efficacy in depression 5%
Fast onset 3%
Not expensive 2%
Easy dosing 2%
Confidence 31%
Safety 15%
PT Not reluctant
to take 13%
Quality of life

Conclusions (Cont’d)
The research also shows that with minimal information (the unbranded product profile),
the return on investment for such an education piece is clear. Even when the GPs are
exposed to this profile, the benefits of XXXX are clearly apparent, with the wide appeal
and fit for menopausal patients suffering from both sets of symptoms.
This is a really positive result for XXXX, and is an early indication that XXXX education will
be well received.

Recommendations
A positive and receptive market for XXXX launch.
Need to educate and inform that there is a product that can effectively and
safely treat their symptoms and encourage discussion with GP on matter
There are still many patients, especially amongst the younger age group who are
experiencing menopausal symptoms yet are not treating.
A good platform to position XXXX….straddling both HRT and SSRI territories
The PBS scenario results in best uptake for XXXX - with GPs not only switching patients
from HRT but also using the product in the previously untreated… expanding the market.
Employ Efexor’s halo effect to help build and strengthen GP confidence to use
XXXX Leverage XXXX use through KOL and specialist endorsement and
recommendation
Exploit Pristiq’s safety and tolerability perceptions and support efficacy measures
Even without an indication or PBS listing for the treatment of menopausal symptoms, GPs
have already accepted the benefits of using SSRI/SNRIs in this market.
There is early indication of the high return on investments for an education piece for
XXXX…GPs responding well to the product profile and showing a clear understanding of
the role of XXXX in the market.
Continue to push for PBS listing in this area

RESEARCH FINDINGS

A Note On Reading The Charts
All the data has been tested for statistical significance and through close examination
of the data and by using Jigsaw’s experience in this market we have been able to
identify skews and trends in the data which add to our general understanding of the
market:
– however, many of the bases here are too small to identify statistical
significance, so we have identified trends in the data instead
Therefore, when reading the charts we have noted interesting trends with a circle
around a number like this:
– 68%
Skews within the data have been noted through arrows indicating either a positive or
negative skew in a subset of our sample, for example:
– NSW
or:
total patient numbers

SECTION
- Our Sample In Context -

A good mix of demographics included in the omnibus research.
Consumer Demographics
Main Grocery Buyer SESHighest Education
Completed
Household
Income
– yes 95%
– no 5%
– white collar 61%
– blue collar 39%
– primary/
secondary
school 40%
– college/
apprenticeship 29%
– university
degree 31%
– >$30,000 22%
– $30-69,999 31%
– $70,000+ 30%
– refused 17%
State
– NSW 30%
– Vic 25%
– Qld 15%
– SA 13%
– WA 13%
– Tas 4%
Age Work Status Marital StatusChildren Under 18 In
Household
– 40-44 yrs 19%
– 45-49 yrs 22%
– 50-54 yrs 23%
– 55-59 yrs 18%
– 60-64 yrs 18%
– full time 36%
– part time 30%
– do not work 34%
– married/defacto 68%
– not married/ divorced/
separated 32%
– children 33%
– no children 67%
Base: All consumers, n=611

Consumers: The Majority Of Women In This Age Range Suffer From Symptoms Of Menopause
A minority refused to answer details.
4%
refused to
answer
73%
experience
menopausal
symptoms
Base: n=611 respondents
Women 40-64
23%
do not experience
menopausal
symptoms
Those suffering from menopausal
symptoms equivalent to 2.40 million

A good mix represented here.
GP Demographic Profile
Area AgeMetro/Rural
– NSW/ACT 35%
– Vic/Tas 33%
– Qld/NT 20%
– SA 6%
– WA 7%
Base: All GPs, n=150
Gender
– metro 69%
– rural 31%
– female 51%
– male 49%
– 30-39 years 15%
– 40-49 years 34%
– 50+ years 51% Rural
VIC/TAS
QLD/NT
QLD/NT
Work StatusNumber Of GPs
Work In PracticePractice Profile
Mean: 5
– full time 79%
– part time 21%
– solo 19%
– group 55%
– medical centre 26%
– 2-3 29%
– 4-5 29%
– 5 19%
– 6-7 19%
– 8-9 13%
– 10 + 10%
Male
Female Female
40-49
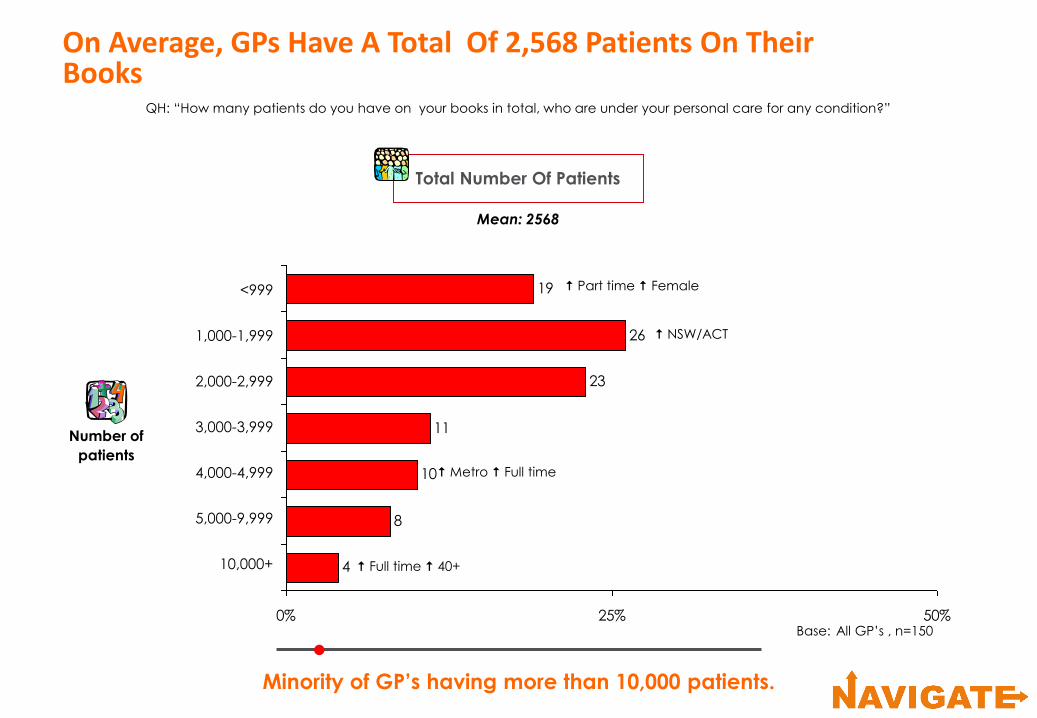
Minority of GP’s having more than 10,000 patients.
On Average, GPs Have A Total Of 2,568 Patients On Their Books
4
8
10
11
23
26
19
0% 25% 50%
QH: “How many patients do you have on your books in total, who are under your personal care for any condition?”
Mean: 2568
<999
1,000-1,999
2,000-2,999
3,000-3,999
4,000-4,999
5,000-9,999
10,000+
Base: All GP’s , n=150
Total Number Of Patients
Number of
patients
Part time Female
NSW/ACT
Metro Full time
Full time 40+

Those seeing 1,000+ menopause patients, skewed towards working in a group practice.
Nearly Ten Percent Of A GPs Patient Population Are Menopausal Women
6
10
5
10
17
7
21
16
7
0% 25%
QI: “How many patients do you have under your personal care in total, who currently experience symptoms of the menopause or perimenopause?”
<50
50-99
100-149
150-199
200-299
300-399
400-499
500-999
1,000+
Base: All GP’s. n=150
Number Of Menopausal/Perimenopausal Patients
Number of
patients Medical centre
Group
Mean: 300 patients with menopause

A minority seeing high numbers.
And, In A Typical Week, Treating 18 Menopausal PatientsQJ: “How many do you see in a typical week who currently experience symptoms of the menopause or perimenopause?”
3
5
7
21
9
25
11
20
0% 25%
5
6-9
10-14
15-19
20-29
30-49
50-69
70+
Base: All GP’s, n=150
Patients Experiencing Menopause/
Perimenopause Symptoms
Mean: 18 patients
Number of
patients
Rural
NSW/ACT

With an average of 4 new patients presenting
with menopause symptoms per week.
A High Number Of Menopausal Patients Are Repeat Patients
QK: “How many of these patients are presenting for the first time with their menopausal/perimenopausal symptoms? And how many are repeat patients?”
3
5
7
4
13
5
7
26
29
0% 25% 50%
1
2
3
4
5
6-9
10-19
20+
None
New Patients
Mean: 4
5
5
8
14
13
14
8
23
10
0% 25% 50%
1-3
4-5
6-7
8-9
10-14
15-19
20-29
30-39
40+
Repeat Patients
Mean: 14
New
Base: All GP’s, n=150
NSW/ACT
Part time
Full time

SECTION
- Menopausal Patient
Profile -

With over half experiencing night sweats,
disruption of quality of life and mood swings.
GP: From The GP Point Of View, The Majority Of Patients Suffer From Hot Flushes
Q1: “What proportion of your total menopausal and perimenopausal patients experience each of the following symptoms?”
20
30
31
34
34
37
37
42
46
50
51
52
53
57
68
49
0% 50% 100%
Hot flushes
Night sweats
Disruption of quality of life
Mood swings
Fatigue
Difficulty sleeping
Vasomotor symptoms
Vaginal atrophy
Daytime sweating
Difficulty concentrating
Depressive symptoms
Dry skin
Anxiety symptoms
Bladder urgency and/or frequency
Stiffness/pain joints
Palpitations
Menopausal Symptoms
NSW/ACT
Base: All GP’s, n=150

Consumers: Periods Stopping And Hot Flushes Are TheMain Symptoms Suffered Overall By Our Sample
Q: “Can you please tell me which of the following symptoms you experience on a regular basis
(once a week or more often) as part of the menopause or lead up to the menopause?”
Menopause Symptoms
3.8
14
11
21
22
24
24
28
29
32
34
35
36
37
38
38
40
41
42
53
0% 50% 100%
Periods have slowed/stopped
Hot flushes
Fatigue
Difficulty sleeping
Night time sweating
Tension/irritability
Stiffness/joint pain
Dry skin
Feelings of depression
Mood swings
Feelings of anxiety
Difficulty concentrating
Day time sweating
Bladder urgency
Vaginal dryness
Palpitations
Disruption of quality of life
Pain during sex
None
Refused
Base: All respondents, n= 611
Mean: 6 symptoms
-
68
51
50
57
-
30
34
37
52
34
37
42
31
46
20
53
-
-
-
GP Data
n=150

For the younger women, the psychological
symptoms are the main symptoms suffered.
Consumers: However, The Patient Research Tells Us That Experience Of Symptoms Does Vary By Age
Q: “Can you please tell me which of the following symptoms you experience on a regular basis
(once a week or more often) as part of the menopause or lead up to the menopause?”
Overall
(n=611)
Periods have slowed/stopped
Hot flushes
Fatigue
Difficulty sleeping
Night time sweating
Tension/irritability
Stiffness/Joint pain
Dry skin
Feelings of depression
Mood swings
Feelings of anxiety
Difficulty concentrating
Daytime sweating
Bladder urgency
Vaginal dryness
Palpitations
Disruption of quality of life
Pain during sex
Not experiencing menopause
53
42
41
40
38
38
37
36
35
34
32
29
28
24
24
22
21
11
9.5
40-44
(n=118)
19
9
23
15
16
30
21
16
21
29
21
18
7
12
7
9
8
2
21
60-64
(n=107)
55-59
(n=111)
50-54
(n=138)
45-49
(n=137)
28
32
41
37
28
36
33
27
29
31
27
29
23
18
15
19
18
6
5
75
63
58
55
53
42
47
48
42
40
36
40
40
30
34
24
27
15
1
82
59
44
54
54
44
43
48
49
44
42
31
45
63
37
33
31
15
2
76
53
43
49
46
41
48
49
40
25
35
30
32
31
36
30
25
22
4
% % % % % %

SECTION
- Menopausal Management -

Reflecting the high engagement of GPs in this area.
In The Management Of These Patients, On Average, Only A Tenth Of Total Menopausal Patients Have Been Referred To A Specialist
Specialist Type
(n=130)
5
1
2
2
4
5
7
7
38
88
0% 50% 100%
Q: “Which specialists do you typically refer
these patients to?”
Gynaecologist
Endocrinologist
Obstetrician
Psychologist/Psychiatrist
Urologist
Menopause specialist/clinic
Cardiologist/heart specialist
Women’s health
Surgeon
Other
n=130
GPs have
referred patients
Others include:
– dermatologist
– rheumatologist
Q: “Thinking again about menopausal/perimenopausal patients
you have on your books in total, how many have been referred to
a specialist at some point for their symptoms?”
13
5
13
10
11
7
17
14
8
0% 50% 100%
1-4
5-9
10-14
15-19
20-29
30-49
50-99
100+
None
Specialist Referred
(n=150)
Mean: 32 patients
Number of
patients

GPs only referring if there is a problem or at patient request.
This Engagement Is Demonstrated By Referral Rationale
Q: “And of the patients you have referred to specialists, typically what were the main reasons for the referrals?”
Base: GPs referred to specialist,
n=130
Physical symptoms 53%
– abnormal bleeding 19%
– urinary/bladder symptoms 12%
– not tolerating HRT 12%
– gynaecological problems 5%
– vaginal dryness 5%
– severe flushing/hot flushes 5%
– vaginal problems 3%
Poor control/Poor response to treatment 43%
– not responding to medication/
treatment 37%
– not responding to hormone
replacement therapy 8%
Patient request 30%
– patient wanting second opinion 28%
– patient worrying 2%
Psychological symptoms 15%
– anxiety/depression 8%
– loss of libido/problem with sex life 8%
– mood swings 2%
Metro
Rural
Confirmation/Advice/Assessment 14%
– to assess/advise patients for HRT 7%
– management issues/medical issues 5%
– confirming diagnosis/rule out
other problems 3%
Severe/Complicated cases 13%
– complicated cases 7%
– severe menopausal symptoms 7%
Safety concerns 8%
– concerns regarding HRT 5%
– cardiac/hypertension/stroke concerns 3%
Advice on alternative treatments 5%
Female
Medical
centre
Rural
History of breast cancer concerns 9%

The majority return to their GP’s care.
On Average, A Quarter Of Those ReferredTo A Specialist Continue To Be Managed By The Specialist
Q2d: “Thinking about the patients who have been referred to a specialist at some point, how many continue to be managed by the specialist?”
Mean: 8
8
12
6
16
22
8
5
22
0%
25%
1 2 3-4 5-9 10-19 20-29 30+ None
Percentage
Of GPs
Specialist Patient Management
Base: GPs referring to specialist,
n=130
Rural
VIC/TAS
Female
Number Of Patients

Currently, GPs Believe That While HRT Is A Lead Option, Patients Are Also Utilising OTC Remedies
Currently, lower use of the anti-depressant classes…reflecting their off-label status.
Also illustrating the importance of DTC as lots of OTC usage.
Base: All GPs, n=150
Q3a: “Thinking about the menopausal patients you have on your books in total, how many are treated with or use each of the fo llowing options?”
38
29
10
10
Total prescribing: 1.2 products
% of patients treated:76%
HRT
OTC/Herbal remedies
Livial
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
SSRIs/SNRIs
Treatment Options
1
1

A tiny minority admitting they use the SSRIs/SNRIs.
In Terms Of Preferred Choice, The Majority Of GPsFavour HRT
Q4a: “Thinking of therapies currently available for the treatment of
menopause or perimenopausal symptoms, which is your preferred therapy?”
61
20
2 1 1
106
0%
50%
100%
Hormone
Replacement
Therapy
Livial/
tibolone
Efexor/
Venlafaxine
Cipramil/
Citalopram
Luvox/
FLuvoxamine
OTC/Herbal
supplements
or remedies
Tailor therapy
to patient/
no preferred
therapy
Nett SSRIs/SNRIs
3%
Base: All GP’s, n=150
Percentage
Of GPs
Male
Female
50yrs +
rural
Low Efexor
prescribers
Using
SSRI/SNRI less
than a year

Similar to OTC therapies, which are also preferred
due to efficacy and lower risk profile.
Good Tolerability Profile Noted As A Reason To Use The SSRIs/SNRIs
– nett few side effects (n=6)
– effective for symptom relief (n=5)
– nett reduce HRT risk (n=4)
– safe (n=3)
– patients like it (n=2)
– patient prefers natural
treatment first (n=2)
OTC
(n=15)
Base: Those with preferred
therapy
Q4b: “And why is (Q4a) your preferred therapy?”
SSRI/SNRI(n=5)
– few side effects, simple
to use, not addictive (n=1)
Cipramil
(n=1)
Luvox
(n=1)
– improves quality of sleep,
has few side effects, less breast
cancer risks and not addictive (n=1)
Efexor
(n=3)
– low/no side effects (n=3)
– effective for hot flushes (n=1)
– proven in studies (n=1)

Still a high number of women who are suffering symptoms that are not treated
with prescription meds… either because they can’t or won’t take the medications.
Most Patients That Are Contraindicated To HRT Are Contraindicated To Oestrogen Therapy Specifically
Base: All GP’s, n=150
Q3b: “And of the menopausal/perimenopausal patients you have on your books,
in total, how many are contraindicated to treatment with…?”
Hormone Replacement Therapy
Mean: 38 patients
(None: 2% of GPs)
Oestrogen Therapy Specifically
Mean: 36 patients
(None: 2% of GPs)
Represents 11.4% of total patient
population
Represents 10.8% of total patient
population
Q3c: “And of the menopausal/perimenopausal patients you have on your books in total, how many
completely refuse or chose not to take prescription medication for their symptoms?”
Patients Refuse To Take
Prescribed Medication
Mean: 71 patients
(None: 5% of GPs)
Represents 21.3% of total patient
population

Consumer: In Line With This, Over Half The Consumer Sample Are Not On Any Form Of Menopausal Treatment
Maybe many potential patients out there
that have not consulted with their GP?
73%
experience
menopausal
symptoms
Q: “And which of the following treatment options do you use to manage your menopausal symptoms?”
Consumer SampleCurrent Therapies For
Menopause
23%
do not
experience
menopausal
symptoms4%
refused
to
answer
Base: All omnibus respondents
suffering menopausal
symptoms, n=448
55%
None ( 40-44)
22%
OTC/Herbal remedies
( full time work)
5%
Non-hormonal
prescriptions
medication
( 55-59)
24%
Hormone/oestrogen
replacement therapy
( 55-59) ( Blue SES)
Base: All respondents, n=611

Consumers: Whilst Symptoms Are Common To All, Variations Noted Amongst The Different Management Algorithms
Those taking over the counter/herbal remedies
reported slightly fewer symptoms.
63
72
51
60
42
67
47
41
64
63
59
52
37
45
60
75
43
27
Base: All on current treatment, n= 223
Hormone/Oestrogen
Replacement Therapy
Non-Hormonal
Prescription Medications
Over The
Counter/Herbal
Remedies Medication
Average no. of symptoms 10.6 11.2 9.7
Night time sweating
Hot flushes
Feelings of anxiety
Feelings of depression/low mood
Palpitations
Fatigue
Difficulty in concentrating
Disruption of quality of life
Tension/Irritability
Difficulty sleeping
Mood swings
Daytime sweating
Bladder urgency/frequency
Dry skin
Stiffness/joint pain
Periods have slowed/stopped
Vaginal dryness
Pain during sex
66
77
60
62
49
74
50
47
67
70
58
60
46
62
66
84
41
22
55
70
70
70
54
88
61
36
76
71
75
76
41
58
74
70
59
22

SECTION
- SSRI/SNRI Usage In Focus -

A minority have been using the medications in this way for quite some years.
GPs Started Using The SSRI/SNRI Medications In Menopausal Women An Average Of 5 Years Ago
1
8
11
7
34
27
13
0% 25% 50%
Q5c: “How long ago did you personally start using SSRI/SNRI medications for the treatment of menopausal/perimenopausal symptoms?”
Base: All GPs using SNRI/SSRI,
n=133
Time Since Started Using SSRI/SNRI
Mean: 5 years ago
<1 year
2-3 years
4-5 years
6-7 years
8-10 years
11+ years
Don’t know

Some also moved to act following specialist advice…
another leverage point for XXXX.
GPs Have Begun Using The Medications In This Way As They Know That The Depressive Symptoms Of Menopause Will Be Treated
Q5f: “And what prompted you to commence using these agents in menopausal/perimenopausal patients?”
Base: All GPs using SSRI/SNRI
medications, n=133
Treats psychological symptoms 40%
– depression/anxiety/stress 26%
– patient symptoms suit that drug 14%
– mood swings 5%
– helps insomnia/sleep disturbances 2%
Literature 36%
– clinical data/trials/studies 14%
– medical journal articles 13%
– reading articles/drug books 12%
– medical magazines 3%
Patients not wanting HRT 14%
Info from drug reps 14%
Relief of symptoms 12%
Failure of other therapies 5%
Contra-indications for other treatments 5%
Personal experiences with patients 17%
Specialist advice 32%
– specialist usage/advice 19%
– info from medical meetings/conferences 17%

Zoloft And Efexor Are The Currently Favoured SSRI/SNRI Medications Used In Treatment Of Menopausal Symptoms
Q3ai: “You said you prescribed patients SSRI/SNRI medications for their menopausal symptoms,
of those how do they fall out between the different brands of SSRI/SNRI?”
Base: All prescribing SSRI/SNRI,
n=133
Treatment Options
Not
treated
24%
Base: All patients of all GPs
SSRI/SNRI
10%
No one brand particularly associated with menopause…
GPs probably employing their favoured brand
6
6
8
9
9
21
29
<1
15
Zoloft/sertraline
Efexor/venlafaxine
Cipramil/citalopram
Lexapro/escitalopram
Prozac/Lovan/fluoxetine
Aropax/paroxetine
Avanza/mirtazapine
Luvox/fluvoxamine
Other
Others mentioned <1%:
– Tricyclics
– Aurorix/moclobemideSSRI/SNRI Brands

In addition, a third of GPs see physical benefits… and a lower risk profile.
Unsurprisingly, The Medications Are Utilised For Their Impact On Psychological Symptoms
Help control physical symptoms 31%
– hot flushes controlled 17%
– better for motor/vasomotor symptoms 8%
– less fatigue/better concentration 6%
HRT risks avoided 30%
– HRT risks avoided/alternative 25%
– HRT risk of breast cancer avoided 11%
Well tolerated 10%
– side effects are few 6%
– well tolerated 5%
Effective/fast acting 9%
Safe in overdose/long term safety 8%
Normal lifestyle maintained 7%
Easy to take/less stigma 5%
Cost effective/PBS listed 5%
None 5%
Q5a: “What are the key advantages you see of these medications for patients experiencing menopausal/perimenopausal symptoms?”
Base: All GPs, n=150
Psychological symptoms 84%
– anti depressant effect 58%
– mood is more stable/less irritability 37%
– anxiety control 31%
– sleep is better 15%
– treat mental/psychological/
emotional symptoms 6%

A quarter of GPs also perceiving the SSRI/SNRI class
to be incapable of treating all symptoms of menopause.
However, The SSRI/SNRIs Are Not WithoutTheir Own Concerns For GPs And Patients
Does not treat all symptoms 27%
– hot flushes will persist 13%
– does not always work or treat
all symptoms 13%
Does not address real menopause symptoms 12%
Long time to work/may have to be used longer 7%
Cost/expensive/2 costs if used with HRT 4%
None/not applicable 8%
Q5b: “What are the key disadvantages you see of these medications for patients experiencing menopausal/perimenopausal symptoms?”
Base: All GP’s, n=150
Side effects 63%
– side effects 21%
– nausea 17%
– insomnia 13%
– drowsiness/sedation 11%
– anxiety/agitation 9%
– cramps/urinary side effects 9%
– libido can decrease 8%
– headaches 8%
– gastro intestinal side effects 7%
– weight gain 7%
– dizziness 6%
– dry mouth 5%
– sweating 3%
Stigma attached/patient concern or reluctance 27%

Some effect seen for those suffering physical symptoms too. Opportunity for XXXX to build on this platform of understanding.
The Benefits Of The SSRI/SNRI Classes CentreOn Their Ability To Impact Psychological Symptoms
Q5c: “And which menopausal/perimenopausal patients in particular do you typically
see as benefiting from these agents? For example what is the typical patient profile?”
Base: All GPs, n=150
Psychological issues 81%
– depression 61%
– anxiety 32%
– mood swings 24%
– insomnia 13%
– irritable 8%
– emotional symptoms
(crying/getting upset easily) 5%
– history of depression 5%
– psychological issues/problems 4%
– relationship/family problems 4%
Physical Symptoms 20%
– hot flushes 11%
– tired/fatigued/lethargic 5%
– vasomotor symptoms 3%
– sweats 3%
Younger/Middle aged women 6%
– 40-45 years 3%
– younger age group 3%
Working/Active 5%
– working full time 3%
– have active lifestyle 2%
Breast cancer risks 9%
– previous/history of breast cancer 7%
– concerned about breast cancer 3%
Over 50 years 9%
Menopausal symptoms 7%
Don’t want to take HRT 7%
Perimenopausal 7%
Unable to tolerate HRT 17%
– unable to tolerate/respond to HRT 17%
– oestrogen contra-indication 4%

But again, efficacy seen for physical symptoms too.
Overwhelmingly, It Is The Psychological Symptoms That Lead GPs To Employ The SSRI/SNRI Classes
Q5d: “When you think of initiating a SSRI/SNRI in your menopausal/perimenopausal patients,
which symptoms of the menopause in particular are you targeting with this treatment?”
Base: All GPs, n=150
Physical Symptoms 48%
– hot flushes 25%
– fatigue 13%
– vasomotor symptoms 5%
– night sweats 5%
– daytime sweating 3%
– palpitations 3%
– stiffness and/or pain in joints 2%
Psychological symptoms 96%
– depression symptoms 76%
– anxiety symptoms 57%
– mood swings 48%
– difficulty in sleeping 27%
– tension/irritability 17%
– difficulty in concentrating 4%

… and high numbers of these patients seen.
It Follows Then That GPs Are Mostly Using These Medications Amongst Depressed Women…
2
43
7
13
7
3
11
4
3
5
5
0% 25% 50%
Q5e: “And of the patients currently treated with an SSRI or SNRI medication for their symptoms what proportion
were also experiencing depressive symptoms at the time you initiated their medication?”
Base: All GPs using SSRI/SNRI, n=133
Patients Experiencing Depressive Symptoms
Mean: 74% of patients1-10%
11-20%
21-30%
31-40%
41-50%
51-60%
61-70%
71-80%
81-90%
91-100%
None
percentage
of patients

SECTION
- XXXX In Focus -

What We Told GPs About XXXX (Product X)…
Product X:
− Product X is a non-hormone medication that works on the central nervous system to treat moderate to
severe vasomotor symptoms associated with the menopause
− Product X is a serotonin and norepinephrine reuptake inhibitor (SNRI). Product X will also be used as an
anti-depressant
– Product X has several benefits across several symptoms of the menopause:
• patients will experience a 60% reduction in both the severity and frequency of hot flushes
(those that occur both during the day and night)
• patients will experience relief within 21-28 days
• patients will experience fewer episodes of sleep disturbances associated with hot flushes, and
may have an improved quality of sleep
• patients will experience a positive impact on workplace efficiency, including achievement of
full activity and productive days and also experience improved quality of life (eg reduction in
symptoms, fewer side effects, improved social functioning)
− Safety:
• Product X has no hormone-related side effects or risks (for example no breakthrough bleeding,
no endometrial or breast tissue stimulation)
• at higher doses product X is associated with a 2mm hg increase in Systolic Blood Pressure in 2-
3% patients
− Tolerability:
• product X has a 25% incidence of mild to moderate nausea and/or dizziness (which is transient
for 2 to 3 weeks)
• Product X has no effect on sexual function
− Dosing product X is an oral tablet taken once daily

A really positive result for XXXX!
Upon Hearing Pristiq’s Profile, GPs IndicateThat They Are Very Interested In The New Product
1% 1%
3% 10% 22% 26% 37%
1 Not very interested 2 3 4 5 6 7 Very interested
Q6a: “Recognising that there are already a wide range of products available for use, on a scale of 1-7,
where 1 is not very interested and 7 = very interested, can you tell me how interested you are in this new product?”
Base: All GPs, n=150
Level Of Interest
Mean: 6
Not interested
5%
Neutral
32%
Interested
63%

Equal efficacy in physical and psychological symptoms.
A good tolerability profile is also helping positive perceptions.
The Biggest Advantage OfXXXX Is Considered To Be Its Efficacy Profile
Few side effects/well tolerated 63%
– low side effect profile 39%
– good safety profile 10%
– will not affect sexual function 10%
– well tolerated drug 8%
– not stimulate endometrial tissue 5%
Q6b: “Based on all the information you heard from Product X, what do you consider to be its main advantages?”
Base: All GPs, n=150
EFFICACY 83%
Efficacy: Physical Symptoms 39%
– good for hot flushes 24%
– helps vasomotor symptoms 11%
Efficacy: Psychological symptoms 39%
– good for depression 21%
– good for sleep disturbances 18%
– good for stabilising mood swings 6%
Overall efficacy profile 49%
– effective for menopause symptoms 20%
– treats a wide range of
menopausal symptoms 13%
No hormonal therapy 51%
– non hormonal therapy 41%
– no HRT risk 9%
Improve lifestyle 15%
– improves quality of life 11%
– better performance for patient 6%
Easy to use 12%
– once daily dosing 9%
– single pill 3%
– easy to take/use 3%
Fast acting 5%
– works quickly 3%
– relief within 21 days 3%
Alternative offer 5%
No breast cancer scare 17%
– no increase in breast cancer/can use on
patients with breast cancer 11%
– will not stimulate/affect breast tissue 7%

The lack of effect on hormones a concern for others.
However, For Some,The Potential Side Effects Raise Concerns
Q6c: “And based on all the information you have heard for Product X, what do you consider to be the main disadvantages?”
Base: All GPs, n=150
Side effect concerns 65%
– blood pressure rise 20%
– causes nausea 20%
– problem with side effects 15%
– causes dizziness 9%
– 25% nausea too high 9%
– nausea 2-3 weeks a concern 6%
– side effect with SSRI drug type 5%
Less effective than HRT 25%
– no bone protection 7%
– not as effective as HRT 5%
– no positive hormonal effects 5%
– lack of efficacy in controlling menopausal
symptoms 4%
Patients unwilling to take antidepressants 17%
– patients compliance issues 11%
– antidepressant puts patients off 10%
Slow onset of action 15%
– takes a month to work 14%
Unsure of cost 6%
– may be expensive 5%
Drug not proven yet 5%
None 11%

Greater emphasis on treating the physical and
overall menopause symptoms
Even With Limited Information Available, GPs Already Able To Perceive Benefits Of XXXX Above Those Of The SSRI/SNRI Classes In General
Q6d: “And which patients in particular do you anticipate that Product X would be useful for… typical patient profile?”
Base: All GPs, n=150
Those with psychological issues 57%
– depression 32%
– mood swings 15%
– insomnia 15%
– anxiety 15%
– loss of concentration 5%
– not coping with day to day activities 5%
Those with physical symptoms 35%
– hot flushes 22%
– vasomotor symptoms 13%
Menopausal symptoms 25%
Unable to tolerate HRT 22%
– unable to tolerate HRT 15%
– oestrogen contra-indications 7%
Don’t want to take HRT 21%
Perimenopausal 13%
All other treatments failed 6%
Severe symptoms 6%
Breast cancer risks 13%
– history of breast cancer 7%
– concerned about breast cancer 5%
(%) = SSRI/SNRI patient suitability profile
(20%)
(7%)
(7%)
(7%)
(81%) (9%)
(7%)
(-)
(-)

SECTION
- Uptake Levels -

What We Did….
Gauged uptake of XXXX , and where its share of market would come from in each scenario
After taking a measure of current prescribing in the market, we
presented the GPs with the XXXX profile.
In order to gauge uptake of XXXX in a range of hypothetical potential future
market reimbursement scenarios, we presented the GPs with four different
scenarios.

Pristiq’s presence in this scenario is unlikely to motivate GPs
to prescribe treatment to any new patients.
XXXX Can Gain 5% Share Mostly From HRT, If It Is Introduced As A Private Prescription For $75
100%
Source Of XXXX Volume
68
13
15
4 SSRIs/SNRIs
Cipramil 49%
Zoloft 28%
Prozac 16%
Avanza 4%
Tricyclics 2%
With XXXX
1.2 products
5
34
28
10
10
1
2
76%
XXXX
As A Private Prescription For $75
Q: “Thinking about the menopausal patients you have on your books in total, how many are treated with or use each of the following option?”
Q: “ Imagine that Product X is now available as a private prescription with a cost of $75 per month, how would your prescribing now typically
fall out between the different treatments available?”
Base: GPs, n=74
SSRIs/SNRIs
XXXX
1
1
38
29
10
10
Current
HRT
OTC/Herbal remedies
Livial
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
Total prescribing: 1.2 products
% of patients treated:76%

Cannibalisation of some Efexor use is also noted.
100%
Source Of XXXX Volume
16
30
3
13
6
29
SSRIs/SNRIs
Efexor 37%
Lexapro 25%
Zoloft 12%
Aropax 11%
Prozac 5%
Avanza 5%
Luvox 5%
Aurorix 1%
1
2
New
With XXXX
1.2 products
15
36
24
10
81
80%
XXXX
As A Private Prescription For $40
Q: “Thinking about the menopausal patients you have on your books in total, how many are treated with or use each of the following option?”
Q: “ Imagine that Product X is now available as a private prescription with a cost of $40 per month, how would your prescribing now typically
fall out between the different treatments available?”
Base: GPs, n=76
OTC/herbal remedies and to a lesser degree, HRT can expect to lose share to XXXX.
HRT
OTC/Herbal remedies
Livial
SSRIs/SNRIs
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
Total prescribing:
XXXX
% of patients treated:
38
29
10
10
Current
1
1
1.2 products
76%
Pristiq’s Introduction As A Private Prescription For $40 Is Expected To Bring In New Patients, As Well As Take Share From Some Current Treatment Options

Pristiq’s entry in this scenario also provides GPs a reason to prescribe
to patients currently not receiving any treatment.
100%
Source Of XXXX Volume
36
17
14
12
17
SSRIs/SNRIs
Efexor 24%
Zoloft 22%
Lexapro 11%
Cipramil 10%
Avanza 9%
Aropax 8%
Prozac 8%
Luvox 6%
Aurorix 1%
2
2
New
With XXXX
1.2 products
16
33
26
8
8
1
1
79%
XXXX
As PBS With Authority Requirement
Base: All GPs, n=150
HRT
OTC/Herbal remedies
Livial
SSRIs/SNRIs
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
Total prescribing:
XXXX
% of patients treated:
38
29
10
10
Current
1
1
1.2 products
76%
As A PBS Prescription With Authority Requirement, XXXX Is Likely To Take Share More From HRT Than OTC/Herbal Remedies
Q: “Thinking about the menopausal patients you have on your books in total, how many are treated with or use each of the following option?” Q: “ Imagine that Product X is now available as a PBS prescription with the following authority requirements, how would your prescribing now
typically fall out between the different treatments available?”

This can lead to HRT losing almost half of its current patient base.
Pristiq’s introduction will lead to an increase in market size.
XXXX Can Potentially Attain One Third Market Share If It Is Introduced As A PBS Prescription Without Restriction
100%
Source Of XXXX Volume
40
18
10
11
3
16
2
SSRIs/SNRIs
Zoloft 27%
Efexor 23%
Cipramil 9%
Aropax 9%
Lexapro 8%
Avanza 8%
Prozac 8%
Luvox 7%
New
With XXXX
1.2 products
27
28
24
8
7
1
1
80%
XXXX
As A PBS Prescription
Q: “Thinking about the menopausal patients you have on your books in total, how many are treated with or use each of the following option?”
Q: “ Assuming that Product X is now available as a PBS prescription, how would your prescribing now typically fall out between the different
treatments available?”
Base: All GPs, n=150
HRT
OTC/Herbal remedies
Livial
SSRIs/SNRIs
Topical/Vaginal oestrogen
Catapres
Anti-convulsant
Other
Total prescribing:
XXXX
% of patients treated:
38
29
10
10
Current
1
1
1.2 products
76%

Not surprisingly, refusal rates rise with increased cost of XXXX.
GPs Think Half Their Patients WillRefuse XXXX If It Is Priced Of $40 A Month
Refused With Cost
of $40 per month
(n=76)
Mean: 50% of patients
Q7: “Imagine a hypothetical scenario in which product X is
available on the market as a private prescription with a cost
of $40 per month, what proportion of your patients do you
think would refuse the product in the basis of this cost?”
Refused With Cost
of $75 per month
(n=74)
Mean: 75% of patients
Q7: “Imagine a hypothetical scenario in which product X is
available on the market as a private prescription with a cost
of $75 per month, what proportion of your patients do you
think would refuse the product in the basis of this cost?”
Base: All GPs, n=150
(None: 3% of GPs) (None: 1 % of GPs)
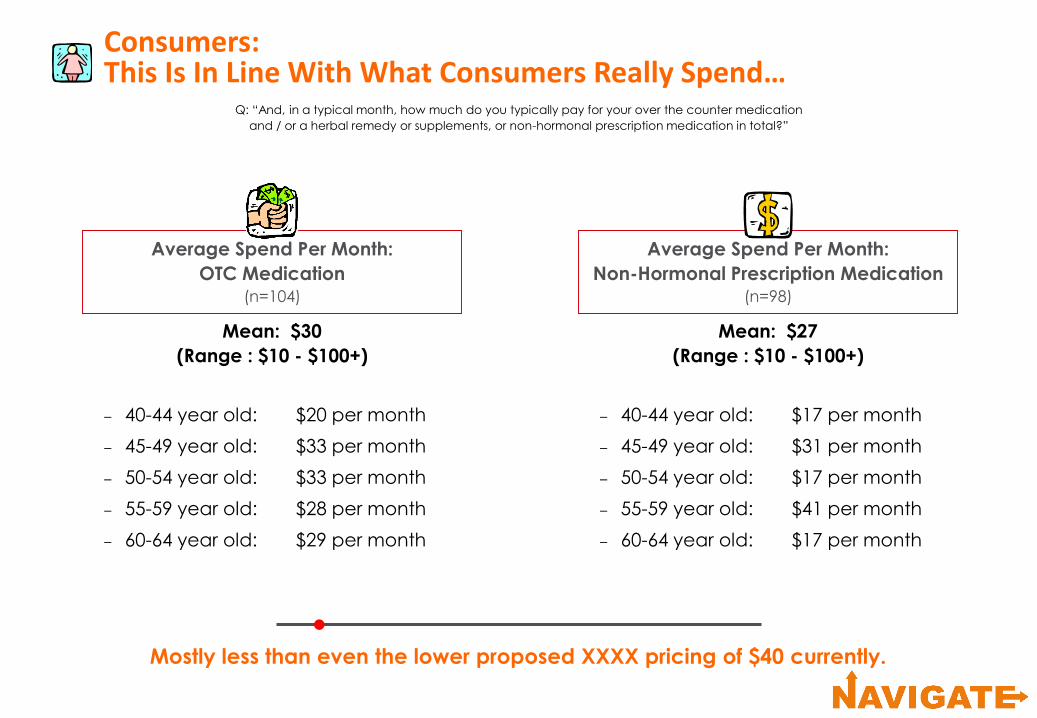
Mostly less than even the lower proposed XXXX pricing of $40 currently.
Consumers:This Is In Line With What Consumers Really Spend…
Q: “And, in a typical month, how much do you typically pay for your over the counter medication
and / or a herbal remedy or supplements, or non-hormonal prescription medication in total?”
Average Spend Per Month:
OTC Medication(n=104)
– 40-44 year old: $20 per month
– 45-49 year old: $33 per month
– 50-54 year old: $33 per month
– 55-59 year old: $28 per month
– 60-64 year old: $29 per month
Mean: $30
(Range : $10 - $100+)
Average Spend Per Month:
Non-Hormonal Prescription Medication(n=98)
Mean: $27
(Range : $10 - $100+)
– 40-44 year old: $17 per month
– 45-49 year old: $31 per month
– 50-54 year old: $17 per month
– 55-59 year old: $41 per month
– 60-64 year old: $17 per month

SECTION
- Brand Perceptions -

What We Did
The data not presented may be found in the Appendix.
No one technique is perfect… we need to look at all the techniques to get an idea of the market.
– Brand Mapping:
• allows us to look visually at how brands are perceived in the market
– Driver Analysis:
• takes a measure of behaviour and looks at what may be impacting this behaviour. The data is associative only, so we have to assume cause and effect
– XXXX/Efexor Performance Vs Driver Maps:
• looks at the strengths and weaknesses of XXXX and Efexor particularly
– Frequency Data:
• shows the differences in raw scores between products and allows us to look at
the absolute differences in scores
– Spine Data:
• looks at the profiles of each brand. It shows the relative strengths and weaknesses of each brand compared to the average
There are many ways to look at the performance of products. We have chosen 5 ways which
work together to tell a story:
Brand Maps
The closer an attribute is to a brand, the more it is associated with the brand.
Brand maps provide a visual summary of how the products are
perceived in the market, relative to the competitors shown. Attributes
nearer to the centre of the map are common to all brands.
The closer brands are together, the more similarly they are perceived. A brand
that sits apart on the map is more differentiated from its competitors.

Livial
HRTOther SSRI/SNRIs
Efexor
Product X
Expensive
Has data for use in menopausal
PT reluctant to take
Efficacy benefits in depressive
symptoms
Efficacy in Vasomotor
Confident in prescribing
Variety of dosages
Easy dosing schedule
Low risk option Reduces hot flushes severity
Reduces hotflushes frequency
Has a fast onsetof action
Improves PT sleep Improves PT quality of life
Variety of admin formats
Useful in menopausal PT
No oestrogenNo HRT
Few side effects
Safe
Approved for vasomotor treatment
HRT Is Perceived To Have Fast Onset OfAction And A Variety Of Administration Formats
It is also most associated with patients
reluctance to take the medication.

Efexor And The Other SSRI/SNRIsAre Positioned In A Very Similar Way
These medications own the
depressive symptom efficacy attribute in this market.
Livial
HRTOther SSRI/SNRIs
Efexor
Product X
Expensive
Has data for use in menopausal
PT reluctant to take
Efficacy benefits in depressive
symptoms
Efficacy in Vasomotor
Confident in prescribing
Variety of dosages
Easy dosing schedule
Low risk option Reduces hot flushes severity
Reduces hotflushes frequency
Has a fast onsetof action
Improves PT sleep Improves PT quality of life
Variety of admin formats
Useful in menopausal PT
No oestrogenNo HRT
Few side effects
Safe
Approved for vasomotor treatment

Livial
HRTOther SSRI/SNRIs
Efexor
Product X
Expensive
Has data for use in menopausal
PT reluctant to take
Efficacy benefits in depressive
symptoms
Efficacy in Vasomotor
Confident in prescribing
Variety of dosages
Easy dosing schedule
Low risk option Reduces hot flushes severity
Reduces hotflushes frequency
Has a fast onsetof action
Improves PT sleep Improves PT quality of life
Variety of admin formats
Useful in menopausal PT
No oestrogenNo HRT
Few side effects
Safe
Approved for vasomotor treatment
XXXX Is Perceived To HoldBenefits Of Both HRT And Anti-Depressants
Straddles both markets.
Likely to strengthen positive perceptions with further education.

- Driver Analysis -

Driver Analysis Methodology
A robust multivariate approach to understand menopausal/perimenopausal
prescribing choice with Product X under the different reimbursement scenarios.
Latent class multi-nominal logit modelling (MNL) is used to determine the relative
drivers.
Factor analysis is used to remove inter-correlation between the attributes tested,
simplifying them into common themes as perceived by GPs.
The factors derived have then been fed into four separate regression models
to understand their relationships to prescribing menopausal/perimenopausal
treatments with Product X available:
– as a private prescription scenario with a cost of $75 per month
2. as a private prescription scenario with a cost of $40 per month
3. as a PBS prescription with authority requirements (Oestrogen
contraindicated)
3. as a PBS prescription

From The List Of 21 Attributes,Twelve Correlating Groups Of Factors Emerged
Efficacy In Menopausal
– reduces the frequency of hot
flushes
– reduces the severity of hot
flushes
– has excellent efficacy benefits
in Vasomotor symptoms
– is approved for the treatment
of vasomotor symptoms
– has data for use in
menopausal patients
No HRT/Oestrogen
– use in patients who are
contraindicated to HRT
– use in patients who are
contraindicated in oestrogen
therapy
– is a low risk option
Flexibility
– has a good variety of
administration formats
– has a good variety of
dosages
Safety
– has few side effects
– is safe
Usefulness
– useful in all menopausal
patients
Quality Of Life
– improves patients quality of
life

12 Factors Emerged From The List Of Attributes (Cont’d)
GPs prescribe menopausal symptom treatments on 12 key dimensions.
Expensive
– is an expensive product
Confidence
– I feel confident prescribing
these agents
PT Reluctant to take
– patients are reluctant to take
this medication
Fast onset
– has a fast onset of action
Efficacy in depression
– has excellent efficacy benefits
in depressive symptoms of the
menopause
– improves patient sleep
Easy dosing
– easy dosing schedule

The Drivers Of Prescribing ChoiceAre Impacted By The Market Situation
In most scenarios, GP confidence and safety are key but a more expensive
product will also need to be highly useful for patients if they are to pay more.
Secondary:
Primary:
Not
important:
$75
Confidence 13%
Efficacy in
menopausal 11%
Quality of life 9%
Not expensive 9%
Not reluctant to take 8%
Flexible 8%
Easy to dosing 3%
Usefulness 20%
Fast onset 19%
No HRT/Oestrogen, Safety,
Efficacy in depression
$40
Confidence 37%
Safety 18%
Efficacy in
menopause 16%
Easy dosing 12%
Authority
Confidence 26%
Safety 14%
Efficacy in
menopausal 13%
Flexibility 11%
PBS
Confidence 31%
Safety 15%
PT Not reluctant
to take 13%
Quality of life 7%
Not reluctant to take 6%
No HRT/Oestrogen 5%
Flexibility, Usefulness, Fast
onset, Efficacy in
depression, Not expensive
Easy dosing 7%
Efficacy in depression 7%
Quality of life 5%
PT Not reluctant
to take 4%
No HRT/Oestrogen 4%
Fast onset 4%
Usefulness 4%
Not expensive
Usefulness 8%
No HRT/Oestrogen 8%
Efficacy in
menopausal 7%
Flexibility 6%
Efficacy in depression 5%
Fast onset 3%
Not expensive 2%
Easy dosing 2%
Quality of life

The Frequency Data Shows Pristiq’sStrength In The Safety Dimension
Even with minimal information available to GPs, XXXX is already associated with
efficacy measures. An excellent platform to start from.
Q8: “I’m now going to read out a list of statements associated with different therapies in the menopausal and perimenopausal market. I
would like you to nominate the product or products from the list you have written down which you feel most strongly are associated with
each statement read out to you”
LivialOther
SSRI/SNRIHRTProduct X Efexor
Confidence
− I feel confident in prescribing these agents 53 65 72 79 76
Safety
− has a few side effects
− is safe
57
64
21
54
27
57
30
37
49
55
Base: n=150
Efficacy in menopause
− reduces the frequency of hot flushes
− reduces the severity of hor flushes
− has excellent efficacy benefits in vasomotor
symptoms
− is approved for the treatment of vasomotor
symptoms
− has data for use in menopausal patients
65
69
58
58
46
31
29
12
21
38
23
24
11
17
39
91
94
80
79
91
64
63
46
50
80
See appendix for remainder of
frequency data

Unsurprisingly, XXXX Performs Less Well On Most Primary Drivers If Priced At $75
In addition to lack of GPs confidence, XXXX also needs to address
concerns surrounding ‘usefulness’ and ‘fast onset action’ as these are primary drivers.
Easy dosing
Flexibility
Not reluctant to take
Not expensive
Quality of life
Efficacy in menopausal
Confidence
Fast onset
Usefulness
High
Importance
Low
Importance
Low
Performance
High
Performance
Support Exploit
FixDe-Prioritise
$75 - XXXX

XXXX Performs Well On AllBut The Top Driver Of Confidence If Priced At $40
Safety and efficacy in menopausal area are attributes to exploit in this scenario.
No HRT/
Oestrogen
Not reluctant
to take
Quality of life
Easy dosing
Efficacy in menopausal
Safety
Confidence
High
Importance
Low
Importance
Low
Performance
High
Performance
SupportExploit
FixDe-Prioritise
$40 - XXXX

XXXX Has A Number Of Leverageable Assets, Including Efficacy In The PBS Scenario
But, at this early stage, as expected for a new product,
a need for confidence building.
Easy dosing
Not expensive
Fast onset
Efficacy in depression
Flexibility
Efficacy in menopausal
No HRT/Oestrogen
Usefulness
PT Not reluctant to take
Safety
ConfidenceHigh
Importance
Low
Importance
Low
Performance
High
Performance
Support
Exploit
Fix
De-Prioritise
PBS - XXXX