2013 pqrs: why it's important and tips for successful participation
TRANSCRIPT
8/12/2013
1
VBM
2015
QRUR
2012
2013 PQRS:
Why It’s Important and Tips for
Successful Participation
Physician Compare
2011
Objectives
Participants will be able to:1. Appreciate the timelines and implications for value-
based payment.2. Understand why it’s important to participate in PQRS.3. Understand the value-based modifier.4. Describe the options and methods for successful
participation in PQRS in 2013.5. Determine the best way for you and your practice to
participate in PQRS in 2013.
2
8/12/2013
2
Timelines and Implications
for Value-Based Payment
Background
� Since 2006, Legislation has called for value-based purchasing
(VBP) to transform Medicare from a passive payer to an active
purchaser by using specific performance measures aimed at
improving quality and reducing overall cost.
� Value-based purchasing involves three major elements for
physicians:
�Confidential feedback on performance and resource use
�Public Reporting
�Payment adjustment /value-based modifier (VBM)
4

8/12/2013
3
Confidential Feedback on
Performance and Resource Use
Quality and Resource Use Reports (QRURs) provide comparative
information so physicians can view the clinical care their patients
receive in relation to the average care and costs of other
physician’s Medicare patients:
� Physicians in IA, KS, MO, NE received them in March 2012
using 2010 data;
� Physicians in groups with > 25 eligible professionals (EPs)
in CA, IA, IL, KS, MI, MN, MO, NE, WI received them in
December 2012 using 2011 data;
� All groups with > 25 EPs will receive them in Fall 2013
using 2012 data; VBM information is expected to be
included in the reports.
5
Public Reporting
Physician Compare is a CMS website for publicly reporting
physician performance; similar to Hospital Compare
� Physician Compare currently reports that a physician has
successfully participated in quality programs:
�PQRS
�Electronic Prescribing
�Meaningful Use
� In 2014, Physician Compare will publicly report group-level
performance data on groups that participated in 2012 PQRS
using the GPRO web interface
6
8/12/2013
4
Payment Adjustment / Value Modifier
�CMS is phasing in the use of value-based modifiers
(VBM) to provide differential payments based on
quality and cost of care.
�The QRUR is intended as a precursor to the VBM and
currently includes cost of care measures for patients
seen by the physician and quality information
calculated using claims data and from PQRS.
�For further information on the QRUR, go to:http://www.cardiosource.org/~/media/Files/Advocacy/Physician%20Payment/CMSQu
alityandResourceUseReportsandImplicationsforValueBasedPayment.ashx
7
What Does It Mean?
�Think about physicians and other eligible
professionals as the supply side of value-based
purchasing; your fee-for-service is subject to value-
based payment
�Participation in CMS incentive programs (PQRS, e-Rx,
Meaningful Use) has been voluntary;
�CMS is phasing in payment adjustments for non-
participation .
8

8/12/2013
5
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
PQ
RS
Yes 1.5% 1.5% 2% 2% 1% 0.5% 0.5% 0.5%
No
2015
penalty
2016
penalty
2017
penalty
2018
penalty
2019
penalty
2020
penalty
Penalty -1.5% -2% -2% -2% -2% -2%
Payment adjustments for PQRS are moving from bonuses for
successful participation to penalties for non-participation.
Eligible professionals (EPs) who do not participate in PQRS in 2013 will
receive a -1.5% payment adjustment in 2015.
9
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
E-
Rx
Yes 2% 2% 1% 1% 0.5%
No 2012
penalty
2013
penalty
2014
penalty
Penalty -1% -1.5% -2%
Payment adjustments for E-prescribing are moving from
bonuses for successful participation to penalties for non-
participation.
Eligible professionals (EPs) who did not participate in E-Rx in 2012 are
experiencing a -1.5% payment adjustment in 2013.
10
8/12/2013
6
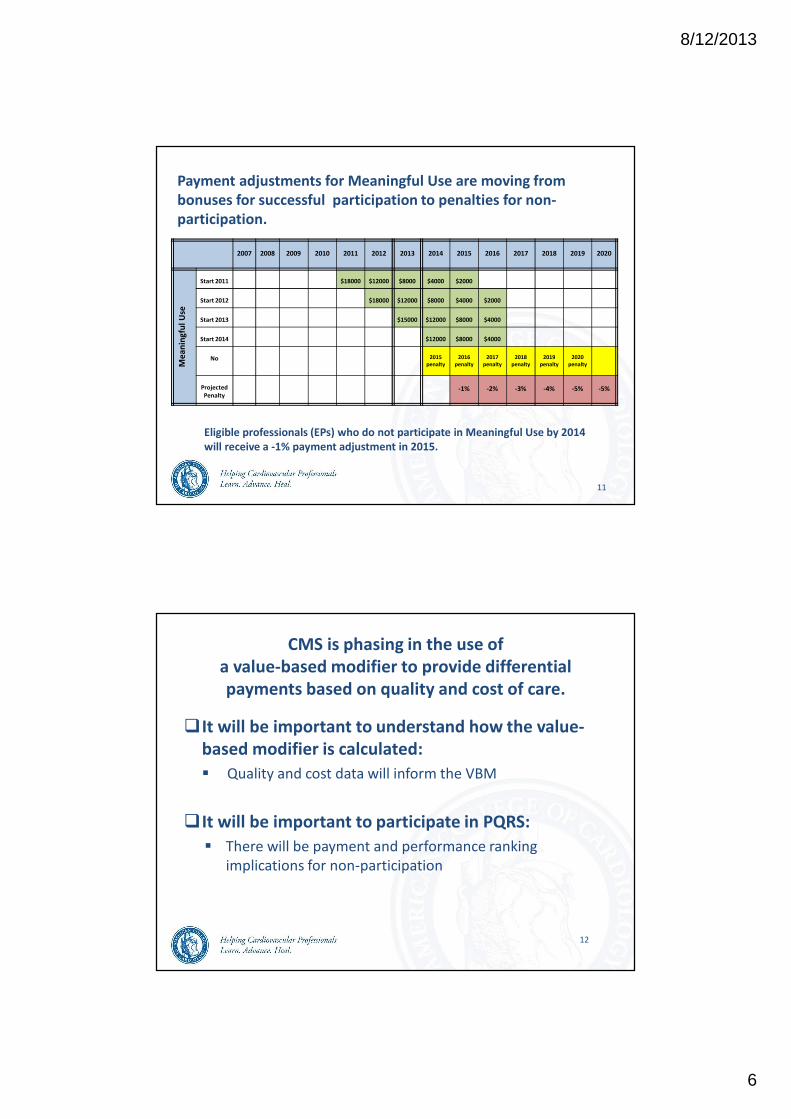
2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020
Me
an
ing
ful
Use
Start 2011 $18000 $12000 $8000 $4000 $2000
Start 2012 $18000 $12000 $8000 $4000 $2000
Start 2013 $15000 $12000 $8000 $4000
Start 2014 $12000 $8000 $4000
No 2015
penalty
2016
penalty
2017
penalty
2018
penalty
2019
penalty
2020
penalty
Projected
Penalty-1% -2% -3% -4% -5% -5%
Payment adjustments for Meaningful Use are moving from
bonuses for successful participation to penalties for non-
participation.
Eligible professionals (EPs) who do not participate in Meaningful Use by 2014
will receive a -1% payment adjustment in 2015.
11
CMS is phasing in the use of
a value-based modifier to provide differential
payments based on quality and cost of care.
�It will be important to understand how the value-
based modifier is calculated:
� Quality and cost data will inform the VBM
�It will be important to participate in PQRS:
� There will be payment and performance ranking
implications for non-participation
12
8/12/2013
7
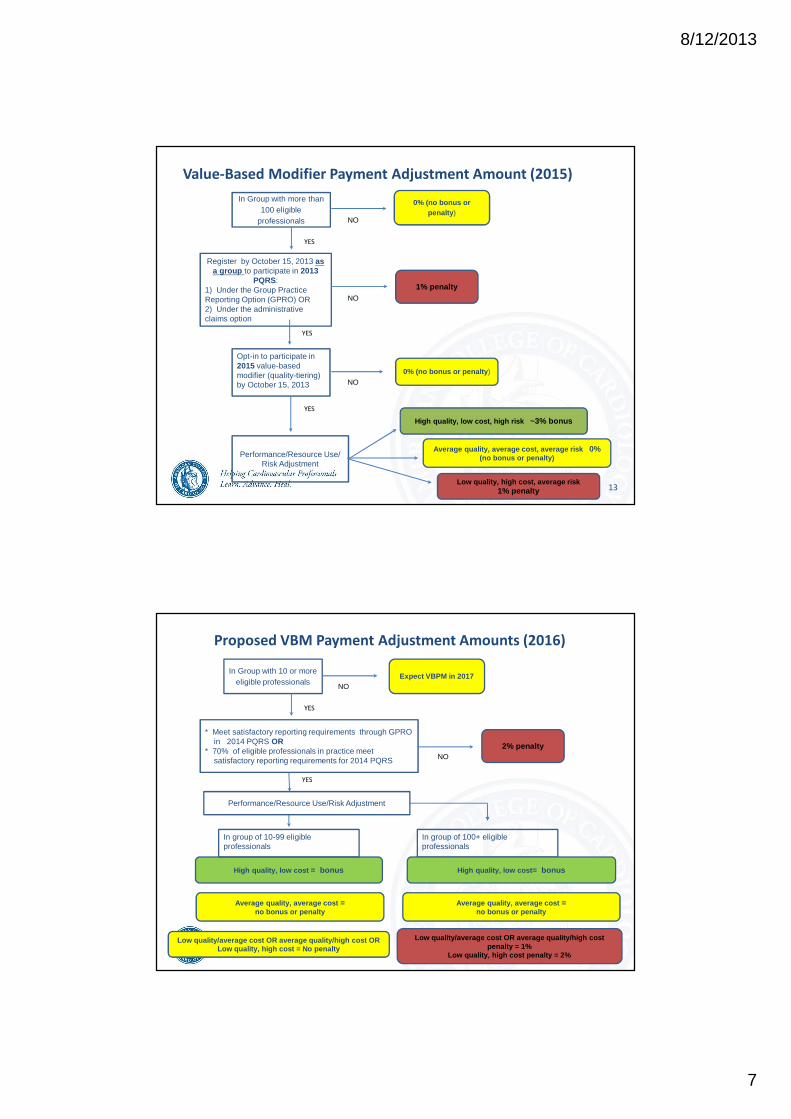
Value-Based Modifier Payment Adjustment Amount (2015)
In Group with more than 100 eligible
professionals
0% (no bonus or penalty)
Register by October 15, 2013 as a group to participate in 2013
PQRS:1) Under the Group Practice Reporting Option (GPRO) OR2) Under the administrative claims option
1% penalty
0% (no bonus or penalty)
Performance/Resource Use/Risk Adjustment
High quality, low cost, high risk ~3% bonus
Average quality, average cost, average risk 0% (no bonus or penalty)
Low quality, high cost, average risk 1% penalty
NO
NO
Opt-in to participate in 2015 value-based modifier (quality-tiering) by October 15, 2013 NO
YES
YES
YES
13
Proposed VBM Payment Adjustment Amounts (2016)
In Group with 10 or more eligible professionals
Expect VBPM in 2017
* Meet satisfactory reporting requirements through GPRO in 2014 PQRS OR
* 70% of eligible professionals in practice meet satisfactory reporting requirements for 2014 PQRS
2% penalty
Performance/Resource Use/Risk Adjustment
High quality, low cost = bonus
Average quality, average cost =no bonus or penalty
Low quality/average cost OR average quality/high cost penalty = 1%
Low quality, high cost penalty = 2%
NO
NO
In group of 10-99 eligible professionals
YES
YES
In group of 100+ eligible professionals
High quality, low cost= bonus
Average quality, average cost =no bonus or penalty
Low quality/average cost OR average quality/high cost OR Low quality, high cost = No penalty
8/12/2013
8
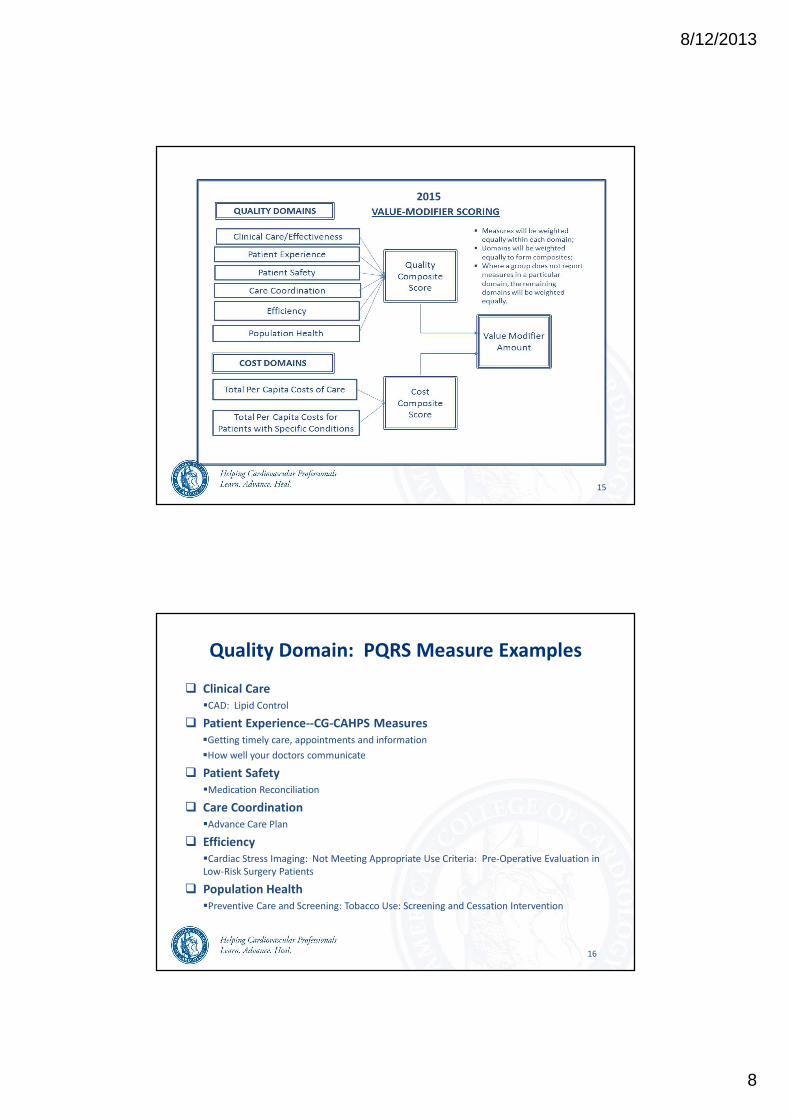
15
2015
Quality Domain: PQRS Measure Examples
� Clinical Care
�CAD: Lipid Control
� Patient Experience--CG-CAHPS Measures
�Getting timely care, appointments and information
�How well your doctors communicate
� Patient Safety
�Medication Reconciliation
� Care Coordination
�Advance Care Plan
� Efficiency
�Cardiac Stress Imaging: Not Meeting Appropriate Use Criteria: Pre-Operative Evaluation in
Low-Risk Surgery Patients
� Population Health
�Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
16
8/12/2013
9
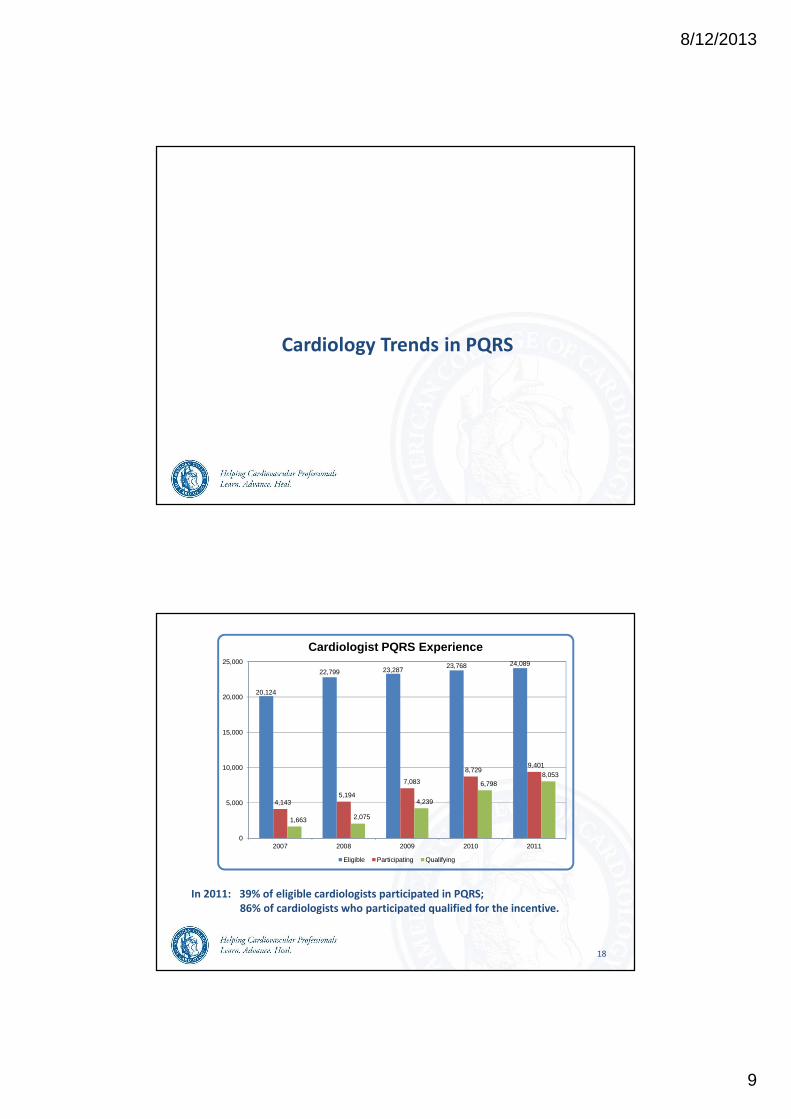
Cardiology Trends in PQRS
18
20,124
22,799 23,28723,768 24,089
4,1435,194
7,083
8,7299,401
1,663 2,075
4,239
6,7988,053
0
5,000
10,000
15,000
20,000
25,000
2007 2008 2009 2010 2011
Cardiologist PQRS Experience
Eligible Participating Qualifying
In 2011: 39% of eligible cardiologists participated in PQRS;
86% of cardiologists who participated qualified for the incentive.
8/12/2013
10
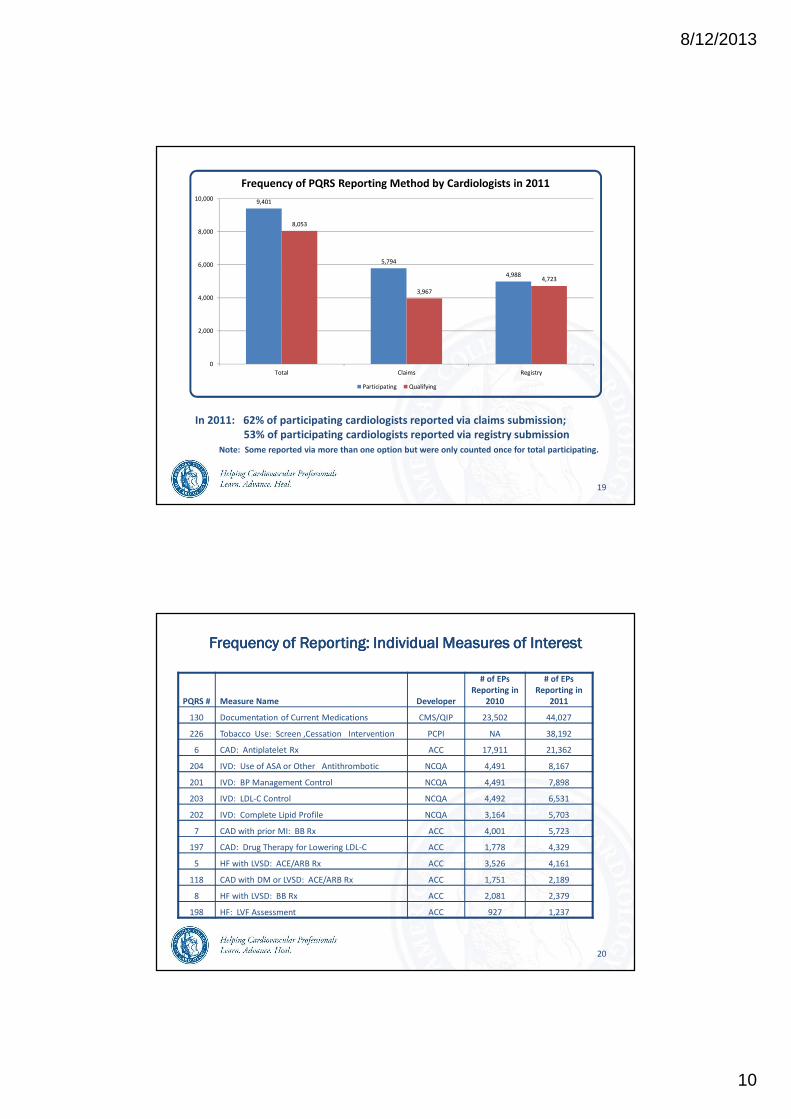
19
9,401
5,794
4,988
8,053
3,967
4,723
0
2,000
4,000
6,000
8,000
10,000
Total Claims Registry
Frequency of PQRS Reporting Method by Cardiologists in 2011
Participating Qualifying
In 2011: 62% of participating cardiologists reported via claims submission;
53% of participating cardiologists reported via registry submission
Note: Some reported via more than one option but were only counted once for total participating.
Frequency of Reporting: Individual Measures of InterestFrequency of Reporting: Individual Measures of InterestFrequency of Reporting: Individual Measures of InterestFrequency of Reporting: Individual Measures of Interest
20
PQRS # Measure Name Developer
# of EPs
Reporting in
2010
# of EPs
Reporting in
2011
130 Documentation of Current Medications CMS/QIP 23,502 44,027
226 Tobacco Use: Screen ,Cessation Intervention PCPI NA 38,192
6 CAD: Antiplatelet Rx ACC 17,911 21,362
204 IVD: Use of ASA or Other Antithrombotic NCQA 4,491 8,167
201 IVD: BP Management Control NCQA 4,491 7,898
203 IVD: LDL-C Control NCQA 4,492 6,531
202 IVD: Complete Lipid Profile NCQA 3,164 5,703
7 CAD with prior MI: BB Rx ACC 4,001 5,723
197 CAD: Drug Therapy for Lowering LDL-C ACC 1,778 4,329
5 HF with LVSD: ACE/ARB Rx ACC 3,526 4,161
118 CAD with DM or LVSD: ACE/ARB Rx ACC 1,751 2,189
8 HF with LVSD: BB Rx ACC 2,081 2,379
198 HF: LVF Assessment ACC 927 1,237
8/12/2013
11
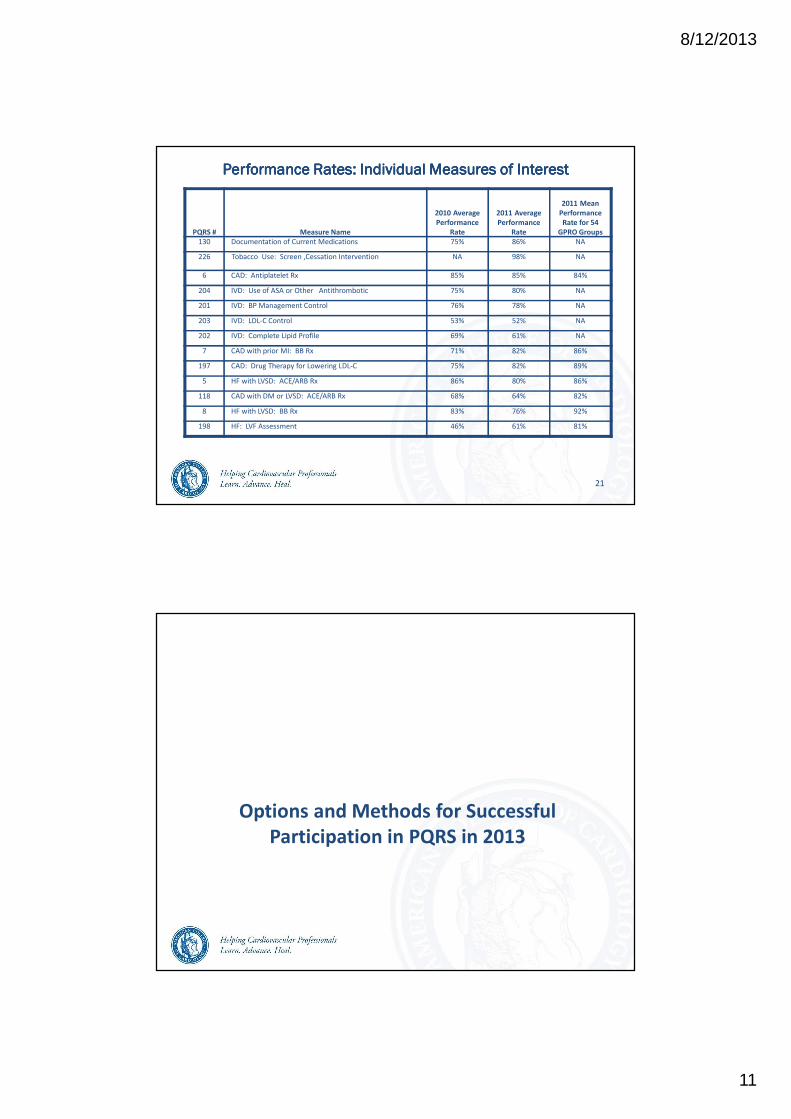
Performance Performance Performance Performance Rates: Individual Measures of InterestRates: Individual Measures of InterestRates: Individual Measures of InterestRates: Individual Measures of Interest
PQRS # Measure Name
2010 Average
Performance
Rate
2011 Average
Performance
Rate
2011 Mean
Performance
Rate for 54
GPRO Groups
130 Documentation of Current Medications 75% 86% NA
226 Tobacco Use: Screen ,Cessation Intervention NA 98% NA
6 CAD: Antiplatelet Rx 85% 85% 84%
204 IVD: Use of ASA or Other Antithrombotic 75% 80% NA
201 IVD: BP Management Control 76% 78% NA
203 IVD: LDL-C Control 53% 52% NA
202 IVD: Complete Lipid Profile 69% 61% NA
7 CAD with prior MI: BB Rx 71% 82% 86%
197 CAD: Drug Therapy for Lowering LDL-C 75% 82% 89%
5 HF with LVSD: ACE/ARB Rx 86% 80% 86%
118 CAD with DM or LVSD: ACE/ARB Rx 68% 64% 82%
8 HF with LVSD: BB Rx 83% 76% 92%
198 HF: LVF Assessment 46% 61% 81%
21
Options and Methods for Successful
Participation in PQRS in 2013
8/12/2013
12
2013 PQRS Reporting Options
�Report as an Individual Eligible Professional
�Report as a Group Practice
Group Practice = a single Tax Identification Number
(TIN) with 2 or more eligible professionals, as
identified by their individual NPI, who have
reassigned their Medicare billing rights to the TIN
23
Reporting as an Individual Eligible Professional
�Choose your reporting mechanism:
� Claims
� Registry
� EHR direct product
� EHR data submission vendor
� Administrative Claims
� Choose your measures:
� Individual Measures OR Measures Groups
24

8/12/2013
13
Individual Reporting Via Claims
Reporting
Period
Measure
Type
Reporting Criteria
Jan 1, 2013 –
Dec 31, 2013
Individual
Measures
Report at least 3 measures
AND
Report each measure for at least 50% of your Medicare
Part B FFS patients seen during the reporting period to
which the measure applies.
Jan 1, 2013 –
Dec 31, 2013
Measures
Groups
Report at least 1 measures group AND Report each
measures group for at least 20 Medicare Part B FFS
patients.
Measures groups containing a measure with a 0%
performance rate will not be counted.
25
Individual Reporting Via Registry
Reporting
Period
Measure
Type
Reporting Criteria
Jan 1, 2013 –
Dec 31, 2013
Individual
Measures
Report at least 3 measures AND Report each measure for at least
80% of your Medicare Part B FFS patients seen during the reporting
period to which the measure applies.
Jan 1, 2013 –
Dec 31, 2013
Measures
Groups
Report at least 1 measures group AND Report each measures group
for at least 20 patients, a majority (11) of which must be Medicare
Part B FFS patients, seen during the reporting period.
Measures groups containing a measure with a 0% performance rate
will not be counted.
July 1, 2013 –
Dec 31, 2013
Measures
Groups
26
8/12/2013
14
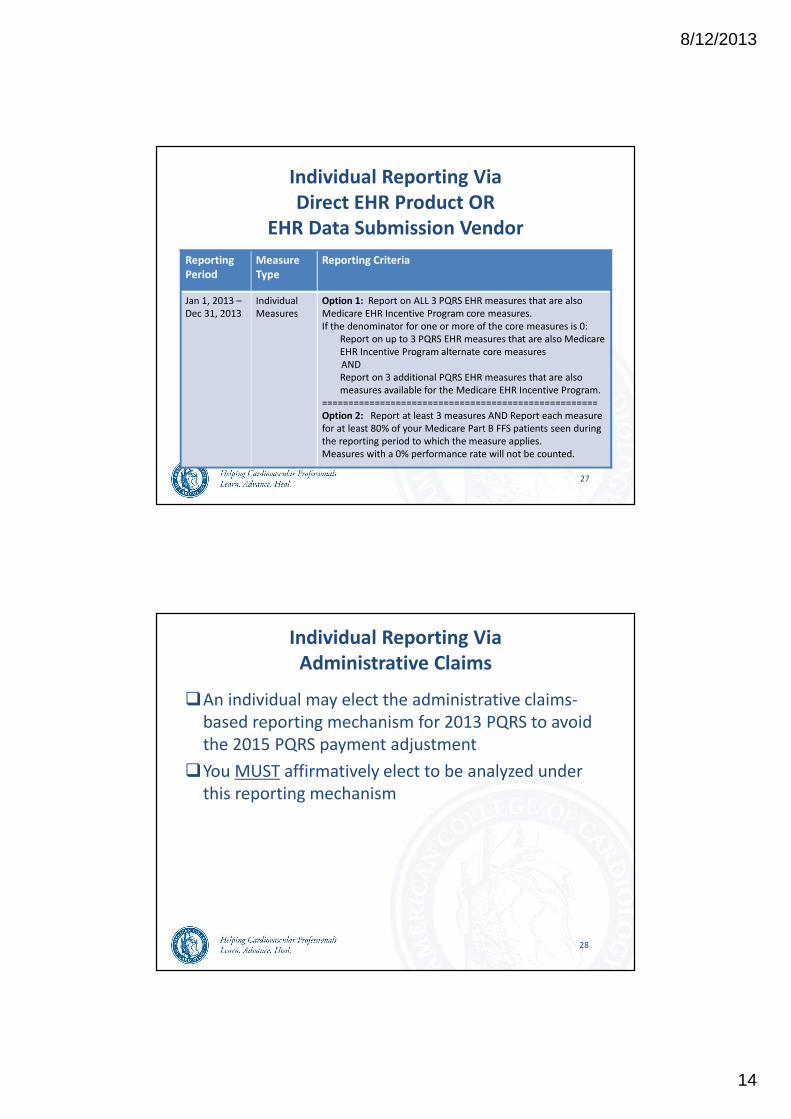
Individual Reporting Via
Direct EHR Product OR
EHR Data Submission Vendor
Reporting
Period
Measure
Type
Reporting Criteria
Jan 1, 2013 –
Dec 31, 2013
Individual
Measures
Option 1: Report on ALL 3 PQRS EHR measures that are also
Medicare EHR Incentive Program core measures.
If the denominator for one or more of the core measures is 0:
Report on up to 3 PQRS EHR measures that are also Medicare
EHR Incentive Program alternate core measures
AND
Report on 3 additional PQRS EHR measures that are also
measures available for the Medicare EHR Incentive Program.
====================================================
Option 2: Report at least 3 measures AND Report each measure
for at least 80% of your Medicare Part B FFS patients seen during
the reporting period to which the measure applies.
Measures with a 0% performance rate will not be counted.
27
Individual Reporting Via
Administrative Claims
�An individual may elect the administrative claims-
based reporting mechanism for 2013 PQRS to avoid
the 2015 PQRS payment adjustment
�You MUST affirmatively elect to be analyzed under
this reporting mechanism
28
8/12/2013
15
Reporting as a Group Practice
� Self-nominate to participate in the PQRS Group
Practice Reporting Option (GPRO):
� Submit a self-nomination statement via a CMS-
developed website
� Deadline to self-nominate: October 15, 2013
� Choose your reporting mechanism:
� GPRO Web Interface
� Registry
� Administrative Claims
29
Patient Experience of Care Survey: CG-CAHPS
� CMS will fund and administer the survey on behalf of the
groups participating in the GPRO Web Interface
� Clinician-Group Consumer Assessment of Health Plans and
Systems Survey (CG-CAHPS) Measures:�Getting timely care, appointments and information
�How well your doctors communicate
�Patients rating of doctor
�Access to specialists
�Health promotion and education
�Shared decision-making
�Courteous and helpful office staff
�Care coordination
�Between visit communication
�Educating patients about medication adherence
�Stewardship of patient resources
30
8/12/2013
16
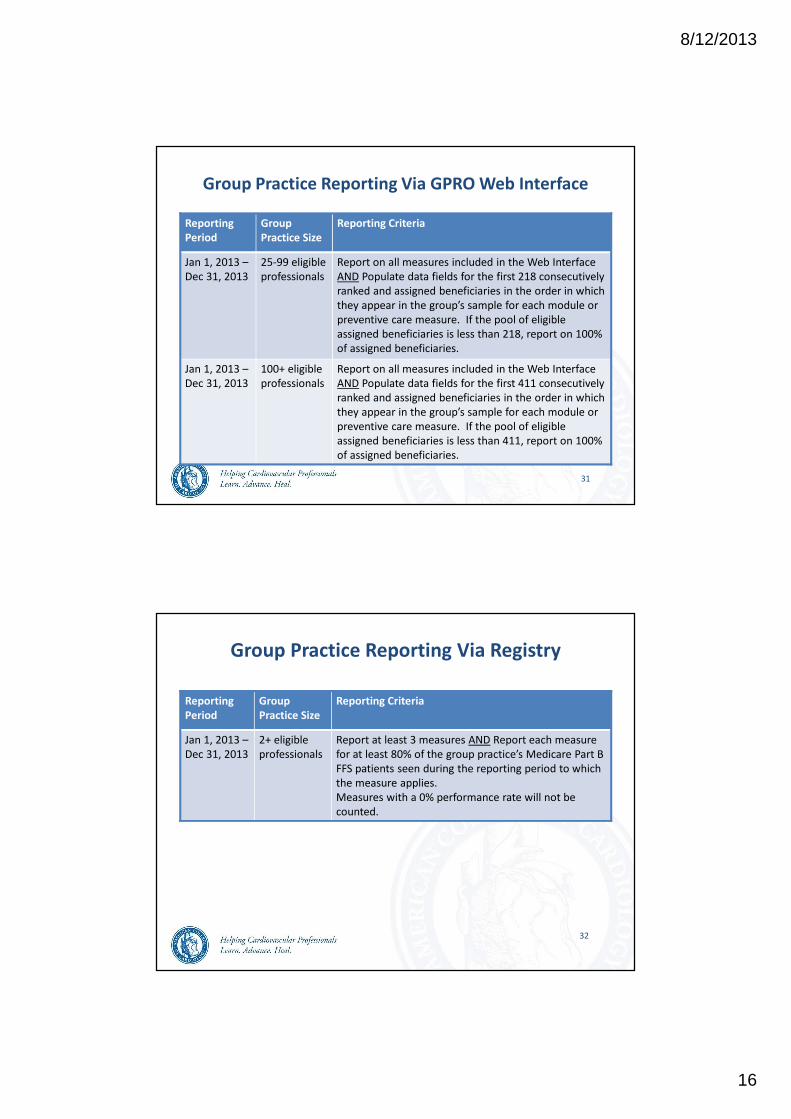
Group Practice Reporting Via GPRO Web Interface
Reporting
Period
Group
Practice Size
Reporting Criteria
Jan 1, 2013 –
Dec 31, 2013
25-99 eligible
professionals
Report on all measures included in the Web Interface
AND Populate data fields for the first 218 consecutively
ranked and assigned beneficiaries in the order in which
they appear in the group’s sample for each module or
preventive care measure. If the pool of eligible
assigned beneficiaries is less than 218, report on 100%
of assigned beneficiaries.
Jan 1, 2013 –
Dec 31, 2013
100+ eligible
professionals
Report on all measures included in the Web Interface
AND Populate data fields for the first 411 consecutively
ranked and assigned beneficiaries in the order in which
they appear in the group’s sample for each module or
preventive care measure. If the pool of eligible
assigned beneficiaries is less than 411, report on 100%
of assigned beneficiaries.
31
Group Practice Reporting Via Registry
Reporting
Period
Group
Practice Size
Reporting Criteria
Jan 1, 2013 –
Dec 31, 2013
2+ eligible
professionals
Report at least 3 measures AND Report each measure
for at least 80% of the group practice’s Medicare Part B
FFS patients seen during the reporting period to which
the measure applies.
Measures with a 0% performance rate will not be
counted.
32
8/12/2013
17
Group Practice Reporting Via
Administrative Claims
�A group practice may elect the administrative claims-
based reporting mechanism for 2013 PQRS to avoid
the 2015 PQRS payment adjustment
�The group practice will make this election when the
practice self-nominates to participate in PQRS via the
GPRO
33
Please note the CMS-calculated administrative claims method is not
an option for earning the PQRS incentive payment; this method only
allows the group to avoid the 1% value-modifier penalty.
What Is the Best Way for You and Your
Practice to Participate in PQRS in 2013?
8/12/2013
18
ACC-Sponsored Submission Options
�NCDR PINNACLE Registry:
Qualified EHR Data Submission Vendor
Individual Reporting of Individual Measures
23 measures available
�ACC PQRSwizard:
Qualified Registry
Individual Reporting of Measures Groups
2 ACC-approved measures groups available
35
36
Meaningful Use Core Clinical Quality Measures (CQMs)
� Measure #237: Hypertension (HTN): Blood Pressure Measurement
� Measure #226: Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
� Measure #128: Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up
Meaningful Use Alternate CQMs
� Measure #239: Weight Assessment and Counseling for Children and Adolescents
� Measure #240: Childhood Immunization Status
� Measure #110: Preventive Care and Screening: Influenza Immunization
Additional CQMs
� Measure #236: Hypertension (HTN): Controlling High Blood Pressure
� Measure #241: Ischemic Vascular Disease (IVD): Complete Lipid Panel and LDL Control
� Measure #313: Diabetes Mellitus: Hemoglobin A1c Control (<8%)
� Measure #1: Diabetes Mellitus: Hemoglobin A1c Poor Control in Diabetes Mellitus
� Measure #308: Smoking and Tobacco Use Cessation, Medical Assistance: a. Advising Smokers and Tobacco Users to Quit, b.
Discussing Smoking and Tobacco Use Cessation Medications, c. Discussing Smoking and Tobacco Use Cessation Strategies
� Measure #197: Coronary Artery Disease (CAD): Lipid Control
� Measure #2: Diabetes Mellitus: Low Density Lipoprotein (LDL-C) Control in Diabetes Mellitus
� Measure #200: Heart Failure: Warfarin Therapy for Patients with Atrial Fibrillation
� Measure #201: Ischemic Vascular Disease (IVD): Blood Pressure Management Control
� Measure #204: Ischemic Vascular Disease (IVD): Use of Aspirin or Another Antithrombotic
� Measure #3: Diabetes Mellitus: High Blood Pressure Control in Diabetes Mellitus
� Measure #5: Heart Failure: ACE- I or ARB Therapy for Left Ventricular Systolic Dysfunction (LVSD)
� Measure #6: Coronary Artery Disease (CAD): Antiplatelet Therapy
� Measure #7: Coronary Artery Disease (CAD): Beta-blocker Therapy for CAD Patients with Prior MI
� Measure #8: Heart Failure: Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD)
Other PQRS Measures
� Measure #47: Advance Care Plan
� Measure #316: Preventive Care and Screening: Cholesterol – Fasting Low Density Lipoprotein (LDL) Test Performed AND
Risk-Stratified Fasting LDL
NCDR PINNACLE Registry: 2013 PQRS Individual Measures
8/12/2013
19
37
� If your practice is not yet submitting data from your EHR
via the system integration (SI) solution, or at least in the
process of data mapping with the SI solution, you may
not be eligible to use the PINNACLE Registry for 2013
PQRS submission.
� If you have questions about the PINNACLE Registry and
participating in PQRS, contact the PINNACLE Registry
Support Team at (800) 257-4737 or [email protected].
PQRSwizard
https://acc.pqriwizard.com/default.aspx
38
8/12/2013
20
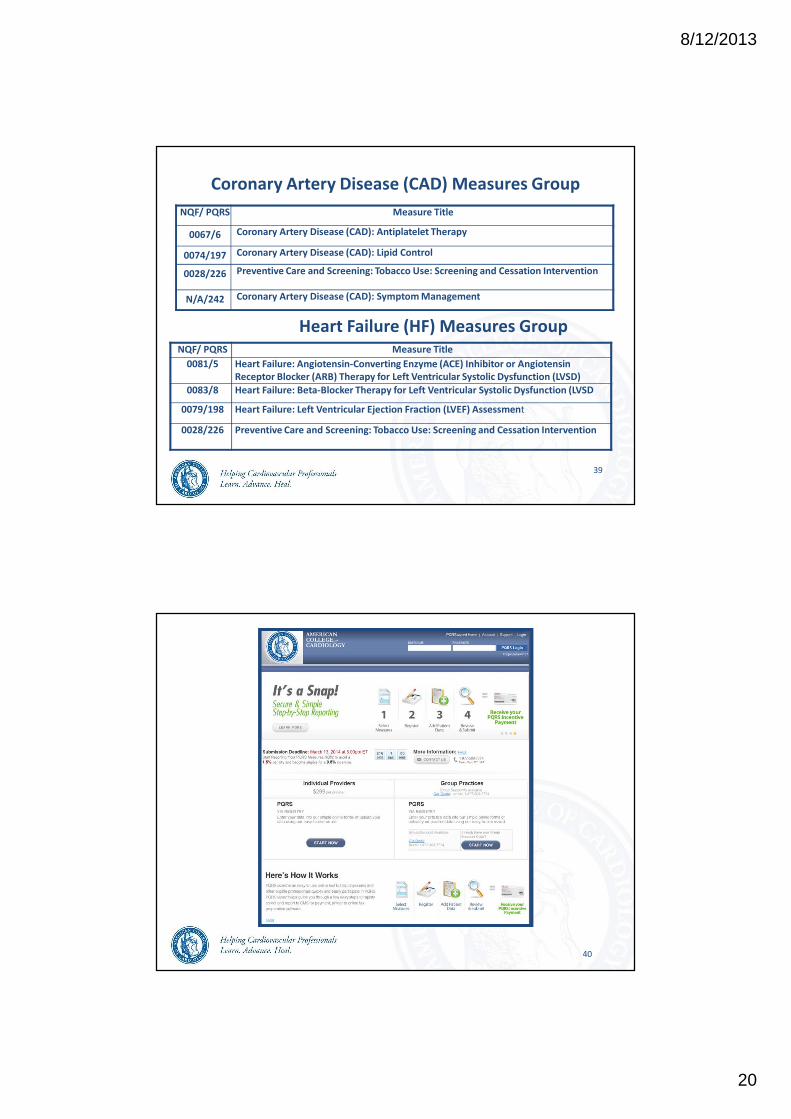
Coronary Artery Disease (CAD) Measures Group
NQF/ PQRS Measure Title
0067/6 Coronary Artery Disease (CAD): Antiplatelet Therapy
0074/197 Coronary Artery Disease (CAD): Lipid Control
0028/226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
N/A/242 Coronary Artery Disease (CAD): Symptom Management
39
Heart Failure (HF) Measures GroupNQF/ PQRS Measure Title
0081/5 Heart Failure: Angiotensin-Converting Enzyme (ACE) Inhibitor or Angiotensin
Receptor Blocker (ARB) Therapy for Left Ventricular Systolic Dysfunction (LVSD)
0083/8 Heart Failure: Beta-Blocker Therapy for Left Ventricular Systolic Dysfunction (LVSD
0079/198 Heart Failure: Left Ventricular Ejection Fraction (LVEF) Assessment
0028/226 Preventive Care and Screening: Tobacco Use: Screening and Cessation Intervention
40
8/12/2013
21
41
42
8/12/2013
22
Other Qualified Submission Vendors
�Qualified 2013 EHR Vendorshttp://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/Downloads/2013QualifiedEHRDirectVendors.pdf
�Qualified Data Submission Vendors http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/Downloads/2012QualifiedDSVs.pdf
�Qualified Registrieshttp://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-
Instruments/PQRS/Downloads/2012-Qualified-Registries-Posting-Phase2.pdf
43
Measures in the GPRO Web Interface for 2013
� Diabetes: Hemoglobin A1c Poor Control
� Heart Failure: Beta-Blocker Therapy for LVSD
� Medication Reconciliation
� Preventive Care and Screening: Influenza Immunization
� Pneumococcal Vaccination Status for Older Adults
� Preventive Care and Screening: Breast Cancer Screening
� Colorectal Cancer Screening
� Coronary Artery Disease: ACE/ ARB Therapy for Diabetes or LVSD
� Adult Weight Screening and Follow-Up
� Preventive Care and Screening: Screening for Clinical Depression
� Coronary Artery Disease: Lipid Control
� Ischemic Vascular Disease: Use of Aspirin or Another Antithrombotic
44
8/12/2013
23
Measures in the GPRO Web Interface for 2013 cont’d
� Preventive Care and Screening: Tobacco Use Screening and Cessation
Intervention
� Hypertension: Controlling High Blood Pressure
� Ischemic Vascular Disease: Complete Lipid Panel and LDL Control
� Preventive Care and Screening: Screening for High Blood Pressure and
Follow-Up Documented
� Falls: Screening for Fall Risk
� Diabetes Composite: Optimal Diabetes Care: Patients who meet all the
numerator targets of this composite measure:� A1c < 8.0%
� LDL < 100 mg/dL
� Blood pressure < 140/90 mmHg
� Tobacco non-user
� For patients with a diagnosis of ischemic vascular disease: Daily aspirin use unless
contraindicated
45
Measures in the 2013 Administrative Claims Option:
Process Measures
� Follow-Up After Hospitalization for Mental Illness
� Use of High-Risk Medications in the Elderly
� Lack of Monthly INR Monitoring for Beneficiaries on Warfarin
� Use of Spirometry Testing to Diagnose COPD
� Statin Therapy for Beneficiaries with Coronary Artery Disease
� Lipid Profile for Beneficiaries Who Started Lipid-Lowering Medications
� Osteoporosis Management in Women > Who Had Fracture
� Dilated Eye Exam for Beneficiaries < 75 with Diabetes
� HbA1c Testing for Beneficiaries < 75 with Diabetes
� Urine Protein Screening for Beneficiaries < 75 with Diabetes
� Lipid Profile for Beneficiaries with Ischemic Vascular Disease
� Antidepressant Treatment for Depression
� Breast Cancer Screening for Women < 69
46

8/12/2013
24
Measures in the 2013 Administrative Claims Option:
Outcome Measures
� Composite of Acute Prevention Quality Indicators (PQIs)
�Bacterial Pneumonia--Admissions per 100,000
�UTI--Discharges per 100,000
�Dehydration--Admissions per 100,000
� Composite of Chronic Prevention Quality Indicators (PQIs)
�Diabetes Composite
� Uncontrolled Diabetes--Discharges per 100,000
� Short-Term Diabetes Complications--Discharges per 100,000
� Long-Term Diabetes Complications--Discharges per 100,000
� Lower-Extremity Amputation for Diabetes--Discharges per 100,000
� COPD--Admissions per 100,000
� Heart Failure--Percent of population with admissions
� All Cause Readmissions
47
8/12/2013
25
49
Questions?Contact: [email protected]
Bookmark: http://www.cardiosource.org/Advocacy/Physician-Payment.aspx