mu - pqrs presentation
TRANSCRIPT

THE KEY TO MEANINGFUL USE STAGE 2 &
PQRSPRESENTER: MARCIA FASTAG, MA, OTR/L, CMUP
Professional Services Consultant
5/15/2015 MU 2 & PQRS Seminar 2
Agenda
MU Core and Menu Measures with key changes between stages 1 and 2 including exemptions.• Proposed MU Changes• Special emphasis will be placed on the following changes:
▪ CPOE▪ Clinical Decision Support▪ Patient Education▪ Medication Reconciliation ▪ Summary of Care ▪ Transition of Care
PQRS\CQM Crosswalk

5/15/2015 MU 2 & PQRS Seminar 3
MU Core Measures Stage 2 vs Stage 1 With Exclusions
EPs must satisfy the requirements of all 17 core objectives to meet Stage 2 of Meaningful Use. The core objectives follow:
1. Use Computerized Provider Order Entry (CPOE) for more than 60 percent of medication, 30 percent of laboratory tests, and 30 percent of radiology orders directly entered into the medical record. – STAGE 1 MEDICATION 30%
▪ EXCLUSION - CPOE for Medication, Laboratory, and Radiology Orders: Any EP who writes fewer than 100 medication, radiology, or laboratory orders.▪ Under proposed 2015 rule Stage 1 providers could claim exclusion for lab/radiology and select
Stage 1 CPOE for medication orders
2. More than 50% of all permissible prescriptions written by the EP are compared to at least one drug formulary STAGE 1 – 40%
▪ EXCLUSION – Prescribe less than 100 prescriptions during the recording period.▪ Under proposed 2015 rule Stage 1 providers may report on Stage 1 objective

5/15/2015 MU 2 & PQRS Seminar 4
MU Core Measures Stage 2 vs Stage 1 With Exclusions
EPs must satisfy the requirements of all 17 core objectives to meet Stage 2 of Meaningful Use. The core objectives follow:
3. Record demographics for more than 80 percent of all unique patients, including preferred language, sex, race, ethnicity, date of birth. STAGE 1 50%
▪ NO EXCLUSION▪ Under proposed 2015 rule providers would not have to report numerator/denominator.
4. Record and chart changes in vital signs for more than 80 percent of all unique patients, including height/length and weight (no age limit); blood pressure (ages 3 and over); calculate and display Body Mass Index (BMI); and plot and display growth charts for patients 0 to 20 years of age, including BMI. STAGE 1 40%
▪ EXCEMPTION: Record Vital Signs: Any EP who (1) sees no patients 3 years of age or older is excluded from recording blood pressure; (2) believes that all three vital signs of height/length, weight, and blood pressure have no relevance to their scope of practice is excluded from recording them; (3) believes that blood pressure alone is not relevant to the scope of practice is excluded from recording it; (4) believes that height/length and weight alone are not relevant to the scope of the practice is excluded from recording them.▪ Under proposed 2015 rule providers would not have to report numerator/denominator.

5/15/2015 MU 2 & PQRS Seminar 5
5. Record smoking status for more than 80 percent of patients 13 years of age or older. STAGE 1 50%
▪ EXCLUSION: Any EP who neither sees nor admits any patients 13 years of age or older.▪ Under proposed 2015 rule providers would not have to report numerator/denominator.
6. Use Clinical Decision Support (CDS) to improve performance on high-priority health conditions. Implement five CDS interventions related to four or more clinical quality measures and enable the functionality for drug-drug and drug-allergy interaction checks. STAGE 1 one measure
▪ Under proposed 2015 rule Stage 1 providers may report on current Stage 1 objective.
7. Provide more than 50 percent of all unique patients the ability to view online, download, and transmit their health information within four business days of the information being available to the EP. More than 5 percent of all unique patients must view, download, or transmit their health information to a third party. STAGE 1 More than 50% of all patients of the EP who request an electronic copy of their health information are provided it within 3 business days
▪ EXCLUSION: Patient Electronic Access: Any EP who (1) neither orders nor creates any of the information listed for inclusion as part of both measures—except for patient name, provider name, and office contact information—may exclude both measures; (2) conducts 50 percent or more of patient encounters in a county where fewer than 50 percent of housing units have 3 Mbps broadband availability according to the FCC may exclude only the second measure▪ Measure #1 unchanged under 2015 proposed rule.▪ Measure #2 threshold previously more than 5 percent proposed to change to ‘1’ patient.

5/15/2015 MU 2 & PQRS Seminar 6
8. Provide clinical summaries to patients for more than 50 percent of office visits within one business day. STAGE 1 – 3 days
▪ EXCLUSION: Clinical Summaries: Any EP who has no office visits.▪ Under proposed 2015 rule providers would not have to report numerator/denominator.
9. Protect electronic health information created or maintained by the certified EHR technology through the implementation of appropriate technical capabilities by conducting or reviewing a security risk analysis in accordance with the requirements under 45 C.F.R. § 164.308 (a)(1).
▪ NO EXCLUSION▪ Under proposed rule both Stage 1 and Stage 2 providers will need to address encryption.
• Microsoft 10 PRO includes device and file encryption via BitLocker, along with many other security enhancements• Hardware-based encryption allows for improved performance, because a dedicated processor encrypts all data that is
written to the hard disk• business smartphones that have a work / personal partition• MS Office 365 (Outlook) can be used for end-to-end encryption, for $2/user/month, with Azure Rights Management• For practices that need HIPAA-compliant file sharing, Sookasais affordable and convenient• For practices that want to text PHI, TigerText is affordable and convenient
10. Incorporate more than 55 percent of all clinical lab-test results into certified EHR technology as structured data. STAGE 1 40%
▪ EXCLUSION: Any EP who orders no lab tests where results are either in a positive/negative affirmation or numeric format.▪ Under proposed 2015 rule providers would not have to report numerator/denominator.

5/15/2015 MU 2 & PQRS Seminar 7
11. Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, research, or outreach.
▪ NO EXCLUSIONS▪ Under proposed 2015 rule objective is removed.
12. Use EHR to identify and provide reminders for preventive/follow-up care for more than 10% of patients with two or more office visits in the last 2 years STAGE 1 - More than 20% of all unique patients 65 years or older or 5 years old or younger were sent an appropriate reminder during the EHR reporting period
▪ EXCLUSION: Any EP who has had no office visits in the previous 24 months▪ Under proposed 2015 rule providers would not have to report numerator/denominator.
13. Patient-specific education resources identified by CEHRT are provided to patients for more than 10% of all unique patients with office visits seen by the EP during the EHR reporting period.
▪ EXCLUSION: Any EP who has had no office visits ▪ Under proposed 2015 rule a Stage 1 provider may claim exclusion if education was not a planned menu
objective.

5/15/2015 MU 2 & PQRS Seminar 8
14. The EP who receives a patient from another setting of care or provider of care, or who believes an encounter is relevant, should perform medication reconciliation for more than 50 percent of patients.
▪ EXCLUSION: Any EP who was not the recipient of any transitions of care▪ Under proposed 2015 rule a Stage 1 provider may claim exclusion if reconciliation was not a planned menu objective.
15. The EP who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide summary of care record for each transition of care or referral1. The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of care record
for more than 50% of transitions of care and referrals ▪ Under proposed 2015 rule objective is removed.
2. The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of care record either a) electronically transmitted to a recipient using CEHRT or b) where the recipient receives the summary of care record via exchange facilitated by an organization that is a NwHIN Exchange participant or is validated through an ONC‑established governance mechanism to facilitate exchange for 10% of transitions and referrals ▪ Under proposed 2015 rule Stage 1 providers may claim exclusion.
3. The EP who transitions or refers their patient to another setting of care or provider of care must either a) conduct one or more successful electronic exchanges of a summary of care record with a recipient using technology that was designed by a different EHR developer than the sender's, or b) conduct one or more successful tests with the CMS-designated test EHR during the EHR reporting period▪ EXCLUSION: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100 times is
excluded from all three measures.▪ Under proposed 2015 rule objective is removed.
5/15/2015 MU 2 & PQRS Seminar 9
16. Capability to submit electronic data to immunization registries or Immunization Information Systems and actual submission except where prohibited and in accordance with applicable law and practice
▪ EXCLUSION: Any EP who meets one or more of the following criteria may be excluded from this objective: (1) the EP does not administer immunizations to any of the populations for which data is collected in their jurisdiction; (2) the EP operates in a jurisdiction where no immunization registry is capable of accepting the data in the specific standards required for certification of the EHR; (3) the EP operates in a jurisdiction where no immunization registry provides timely information on capability to receive immunization data; or (4) the EP operates in a jurisdiction where no immunization registry can enroll additional EPs.▪ Under 2015 proposed rule objective remains.
17. Use secure electronic messaging to communicate with more than 5 percent of unique patients on relevant health information. (NEW)
▪ EXCLUSION: Any EP who has no office visits, or who conducts 50 percent or more of patient encounters in a county where fewer than 50 percent of housing units have 3 Mbps broadband availability according to the FCC.▪ Under proposed 2015 rule objective changed to self-attestation and minimum threshold removed.

5/15/2015 MU 2 & PQRS Seminar 10
EPs must meet 3 out of 6 of the menu objectives to demonstrate Stage 2 of Meaningful Use. All menu objectives must be achieved in accordance with applicable law and practice. The menu objectives follow:
1. Capability to submit electronic syndromic surveillance data to public health agencies. (Same)▪ EXCLUSION: Any EP that meets one or more of the following criteria may be excluded from this objective: (1) the EP is
not in a category of providers that collect ambulatory syndromic surveillance information on their patients; (2) the EP operates in a jurisdiction where no public health agency is capable of receiving such data in the standards required by certified EHR technology; (3) the EP operates in a jurisdiction where no public health agency provides timely information on capability to receive such data; or (4) the EP operates in a jurisdiction where no public health agency that can accept such data can enroll additional EPs.▪ Under 2015 proposed rule objective remains.
2. Record at least one electronic progress note in patient records for more than 30 percent of unique patients.(NEW)
▪ NO EXCLUSION▪ Under proposed 2015 rule objective removed.

5/15/2015 MU 2 & PQRS Seminar 11
3. More than 10 percent of all imaging results, consisting of the image itself and any explanation or other accompanying information, are accessible through certified EHR technology.(NEW)
▪ EXCLUSION: Any EP who orders fewer than 100 tests that result in an image; or any EP who has no access to electronic imaging results.▪ Under 2015 proposed rule objective is removed.
4. Record family health history as structure data for more than 20 percent of all unique patients. (NEW)▪ EXCLUSION: Any EP who has no office visits.▪ Under 2015 proposed rule objective is removed.
5. Capability to identify and report cancer cases to a public health central cancer registry.(NEW)▪ EXCLUSION: Any EP who meets at least one of the following criteria may be excluded from this objective: (1) the EP does not diagnose
or directly treat cancer; (2) the EP operates in a jurisdiction where no public health agency is capable of receiving electronic cancer case information in the standards required for certified EHR technology; (3) the EP operates in a jurisdiction where no such agency provides timely information on its capability to receive such information; or (4) the EP operates in a jurisdiction where no public health agency that can accept such information can enroll additional EPs. ▪ Under 2015 proposed rule objective remains, but public health measures have different structure.
6. Capability to identify and report specific cases to a specialized registry other than a cancer registry.(NEW)▪ EXCLUSON: Any EP who meets at least one of the following criteria may be excluded from this objective: (1) the EP does not diagnose
or directly treat any disease associated with a specialized registry sponsored by a national specialty society for which the EP is eligible, or the public health agencies in their jurisdiction; (2) the EP operates in a jurisdiction where no specialized registry sponsored by a public health agency or by an applicable national specialty society is capable of receiving electronic specific case information in the standards required by certified EHR technology; (3) the EP operates in a jurisdiction where no such agency or applicable national specialty society provides timely information on capability to receive such information; or (4) the EP operates in a jurisdiction where no such registry can enroll additional EPs. ▪ Under 2015 proposed rule objective remains, but public health measures have different structure.

5/15/2015 MU 2 & PQRS Seminar 12
CPOEUse computerized provider order entry (CPOE) for medication, laboratory, and radiology orders directly entered by any licensed healthcare professional who can enter orders into the medical record per state, local, and professional guidelines• More than 60 percent of medication, 30 percent of laboratory, and 30 percent of radiology orders created
by the EP during • the EHR reporting period are recorded using CPOE

5/15/2015 MU 2 & PQRS Seminar 13
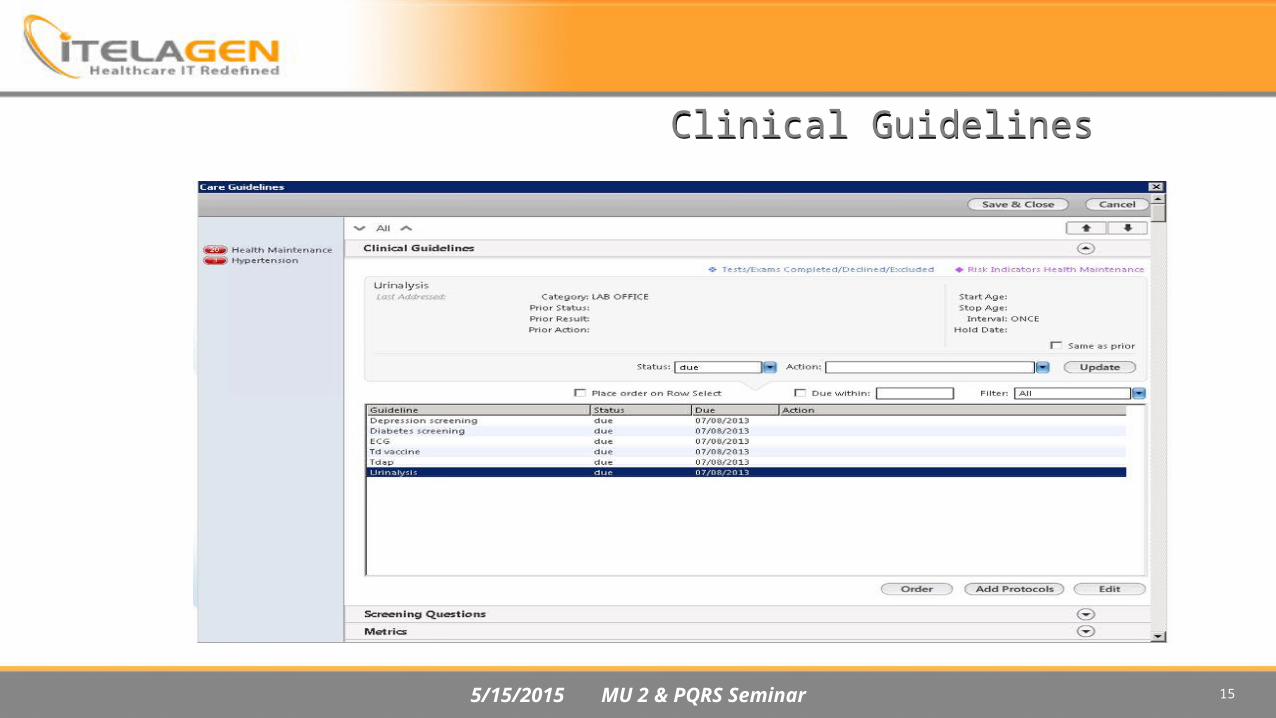
Clinical Decision SupportUse clinical decision support to improve performance on high-priority health conditions
Measure 1: • Implement five clinical decision support interventions related to four or more clinical quality measures at a
relevant point in patient care for the entire EHR reporting period. Absent four clinical quality measures related to an EP’s scope of practice or patient population, the clinical decision support interventions must be related to high-priority health conditions
Measure 2: • The EP has enabled and implemented the functionality for drug-drug and drug-allergy interaction checks for the
entire EHR reporting period
5/15/2015 MU 2 & PQRS Seminar 14
5/15/2015 MU 2 & PQRS Seminar 15
Clinical Guidelines
5/15/2015 MU 2 & PQRS Seminar 16
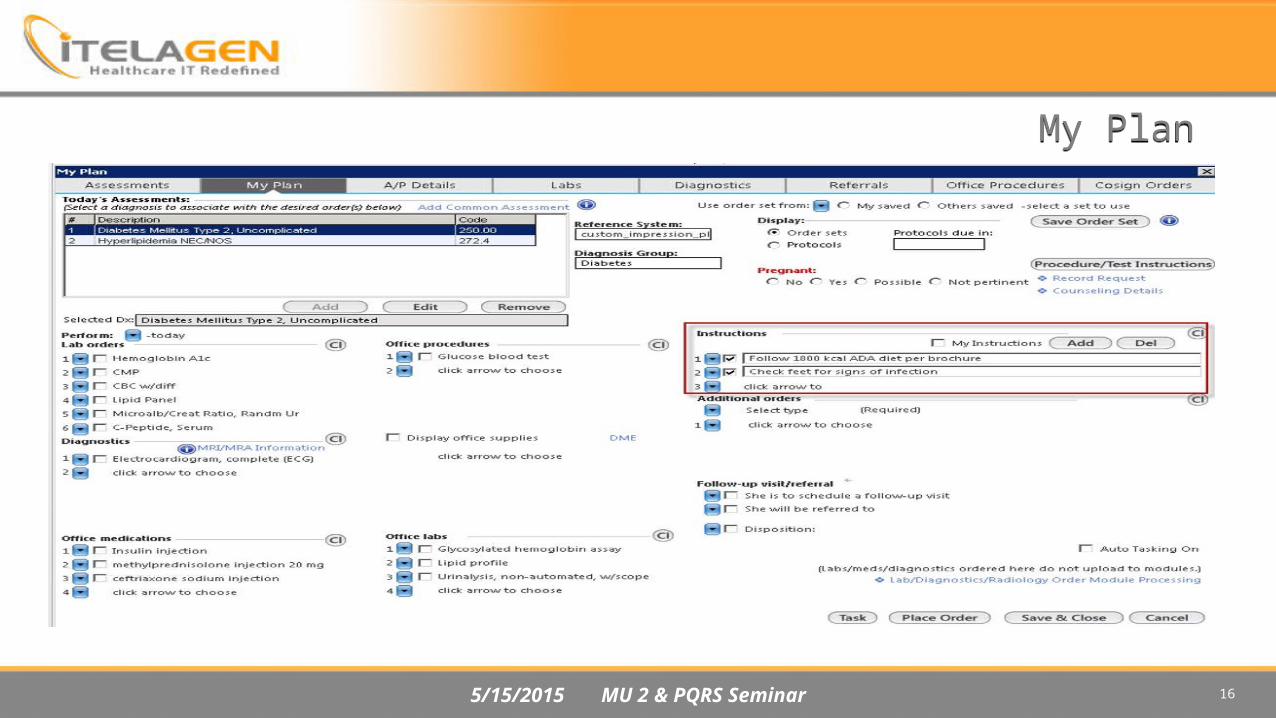
My Plan

5/15/2015 MU 2 & PQRS Seminar 17
Screening Tools

5/15/2015 MU 2 & PQRS Seminar 18
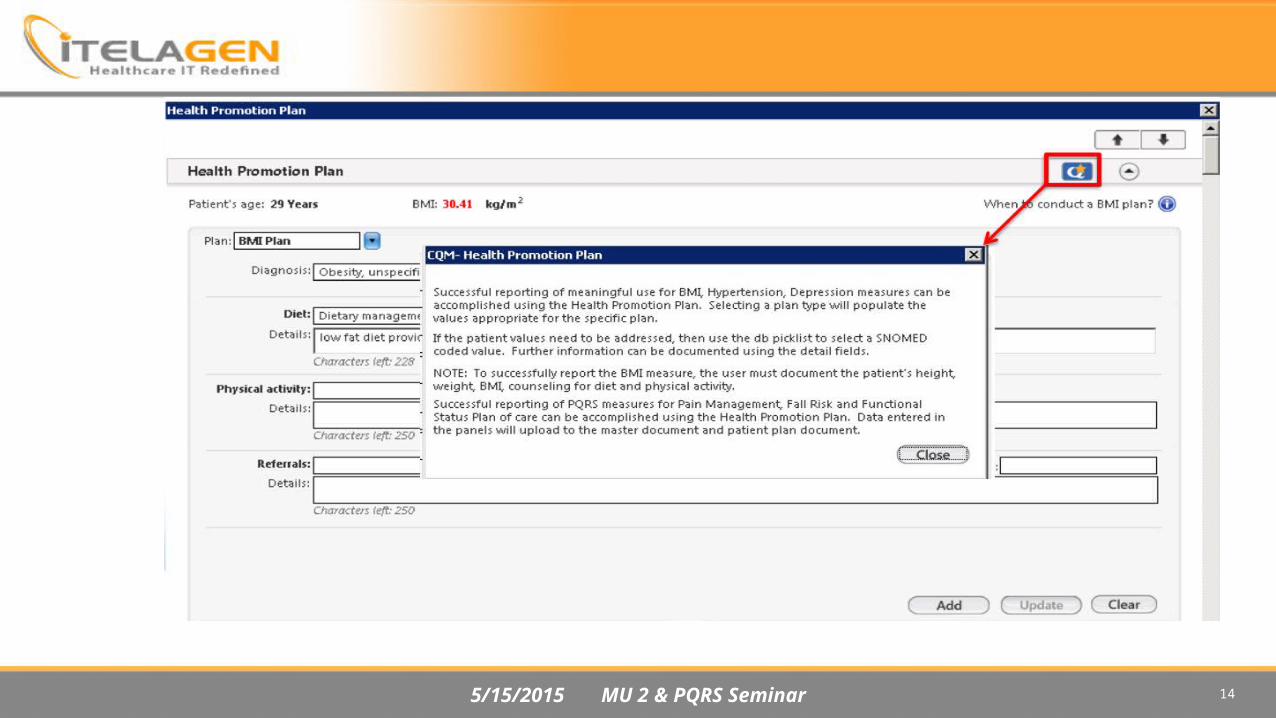
Patient EducationUse clinically relevant information from Certified EHR Technology to identify patient-specific education resources and provide those resources to the patient• Patient-specific education resources identified by Certified EHR Technology are provided to patients for more
than 10 percent of all unique patients with office visits seen by the EP during the EHR reporting period

5/15/2015 MU 2 & PQRS Seminar 19
Problem or Diagnosis List
5/15/2015 MU 2 & PQRS Seminar 20
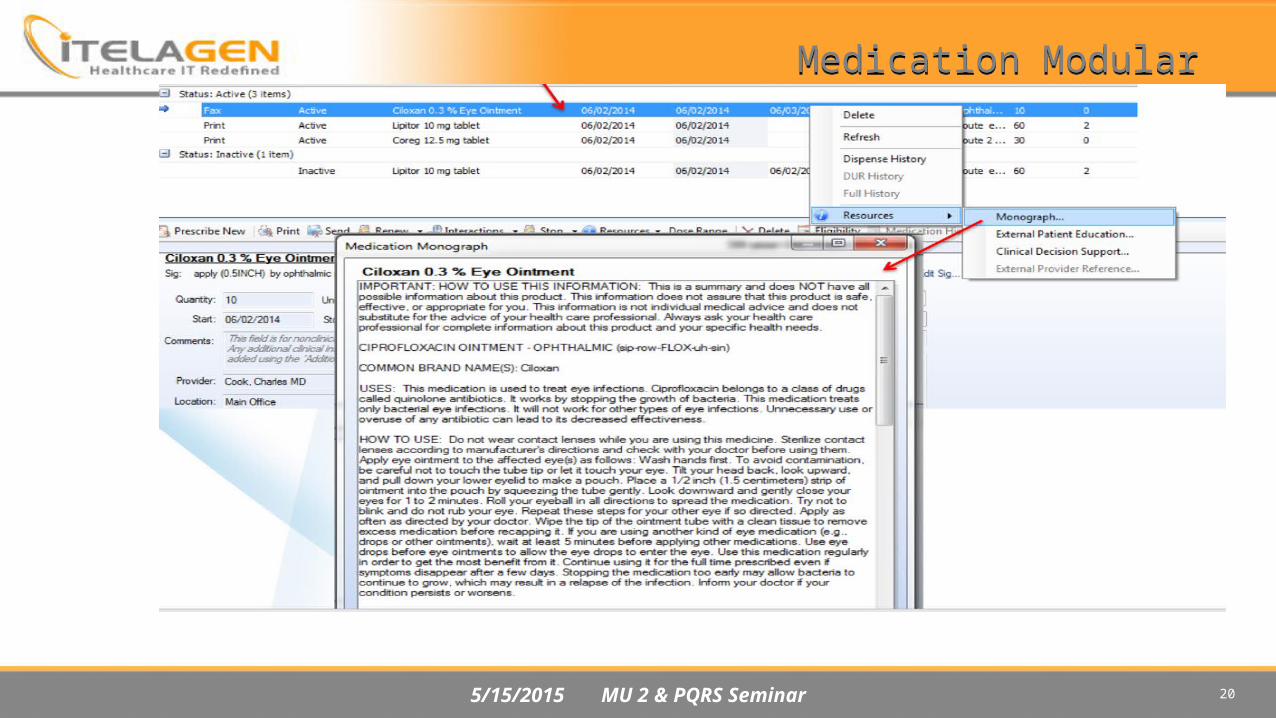
Medication Modular

5/15/2015 MU 2 & PQRS Seminar 21
5/15/2015 MU 2 & PQRS Seminar 22
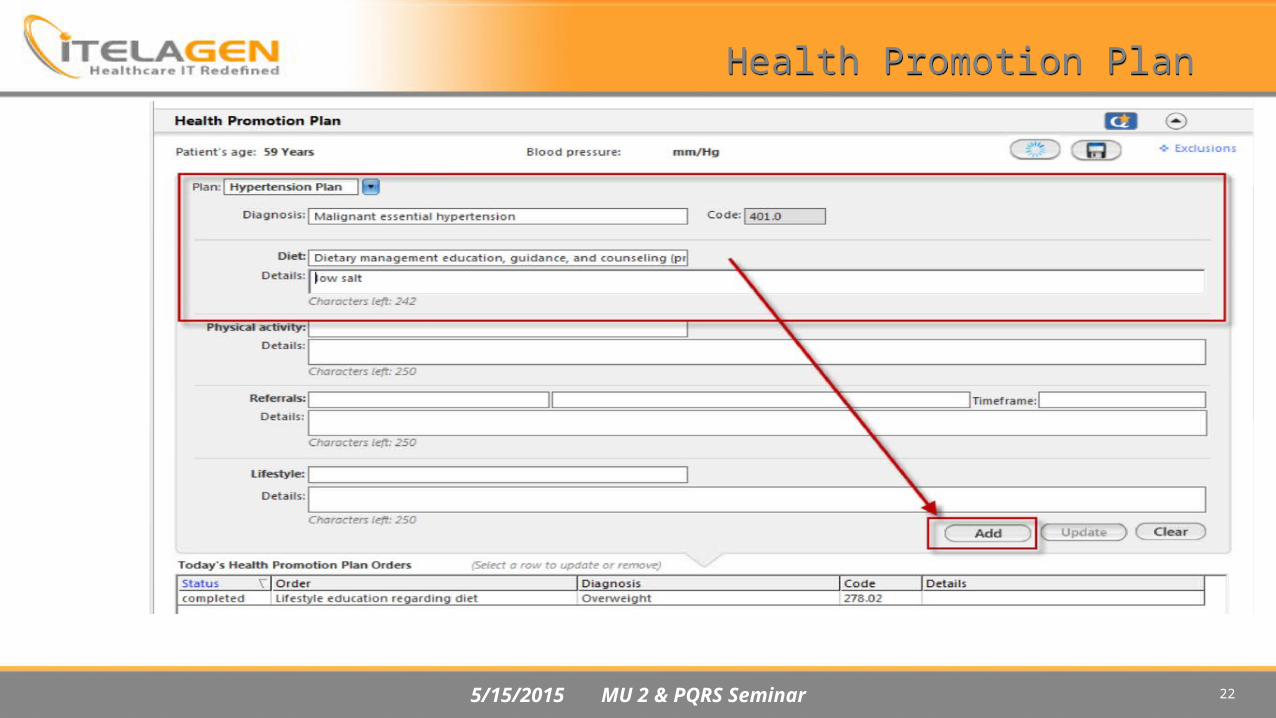
Health Promotion Plan

5/15/2015 MU 2 & PQRS Seminar 23
Advance Audit Tool

5/15/2015 MU 2 & PQRS Seminar 24
Medication ReconciliationThe EP who receives a patient from another setting of care or provider of care or believes an encounter is relevant should perform medication reconciliation• The EP who performs medication reconciliation for more than 50 percent of transitions of care in which the
patient is transitioned into the care of the EP• All Transition of Care, new patients, designated of an encounter with an existing patients with summary of
care record received or electronic C-CCD

5/15/2015 MU 2 & PQRS Seminar 25
Manual Reconciliation

5/15/2015 MU 2 & PQRS Seminar 26

5/15/2015 MU 2 & PQRS Seminar 27
Electronic Reconciliation

5/15/2015 MU 2 & PQRS Seminar 28

5/15/2015 MU 2 & PQRS Seminar 29

5/15/2015 MU 2 & PQRS Seminar 30
DEMO
5/15/2015 MU 2 & PQRS Seminar 31
Summary of Care RecordThe EP who transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide summary care record for each transition of care or referral
Measure 1: • The EP who transitions or refers their patient to another setting of care or provider of care provides summary of
care record for more than 50 percent of transitions of care and referrals – PHI LOG• Objective removed under 2015 proposed rule.
Measure 2: • The EP who transitions or refers their patient to another setting of care or provider of care provides a summary of
care record for more than 10 percent of such transitions and referrals either (a) electronically transmitted using CEHRT to a recipient or (b) where the recipient receives the summary of care record via exchange facilitated by an organization that is a NwHIN Exchange participant or in a manner that is consistent with the governance mechanism ONC establishes for the NwHIN
Measure 3:
An EP must satisfy one of the following criteria: • Conducts one or more successful electronic exchanges of a summary of care document, part of which is counted in
“measure 2” (for EPs the measure at §495.6(j)(14)(ii)(B) with a recipient who has EHR technology that was developed/designed by a different EHR
• Conducts one or more successful tests with the CMS-designated test EHR during the EHR reporting period• Objective removed under 2015 proposed rule.

5/15/2015 MU 2 & PQRS Seminar 32
PHI LOG

5/15/2015 MU 2 & PQRS Seminar 33

5/15/2015 MU 2 & PQRS Seminar 34
Referral Template

5/15/2015 MU 2 & PQRS Seminar 35
DEMO

5/15/2015 MU 2 & PQRS Seminar 36
2015 Proposed Rule for Meaningful UseReporting period modifications:• 2015 and 2016 all new providers just starting MU may select any 90 consecutive days.• All returning MU providers may select any 90 consecutive days in 2015 for MU.• In 2016 all returning MU providers would report for entire year.• In 2017 all providers (new and returning) would report for entire year.
All providers would report under ‘Modified Stage 2’ unless scheduled for Stage 1 in 2015, scheduled Stage 1 providers may use certain matching Stage 1 objectives. (CPOE, e-Rx)
Modified Stage 2 has 9 Core Objectives.
Menu Objective structure removed.
Stage 1 providers must successfully report on ‘1’ public health objective (unless all exclusions met)
Stage 2 providers must successfully report on ‘2’ public health objectives (unless exclusions met)

5/15/2015 MU 2 & PQRS Seminar 37
2015 Proposed Rule for Meaningful UseProposed reporting:
5/15/2015 MU 2 & PQRS Seminar 38
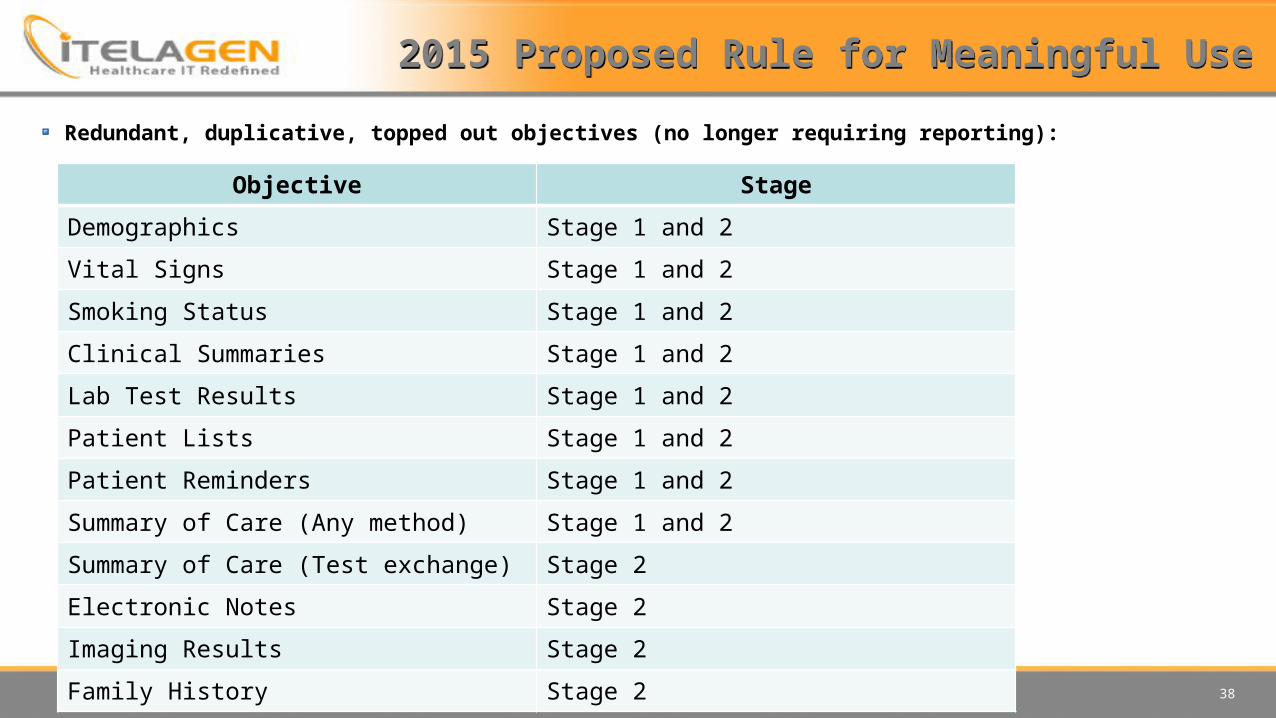
2015 Proposed Rule for Meaningful UseRedundant, duplicative, topped out objectives (no longer requiring reporting):
Objective StageDemographics Stage 1 and 2Vital Signs Stage 1 and 2Smoking Status Stage 1 and 2Clinical Summaries Stage 1 and 2Lab Test Results Stage 1 and 2Patient Lists Stage 1 and 2Patient Reminders Stage 1 and 2Summary of Care (Any method) Stage 1 and 2Summary of Care (Test exchange) Stage 2Electronic Notes Stage 2Imaging Results Stage 2Family History Stage 2
5/15/2015 MU 2 & PQRS Seminar 39
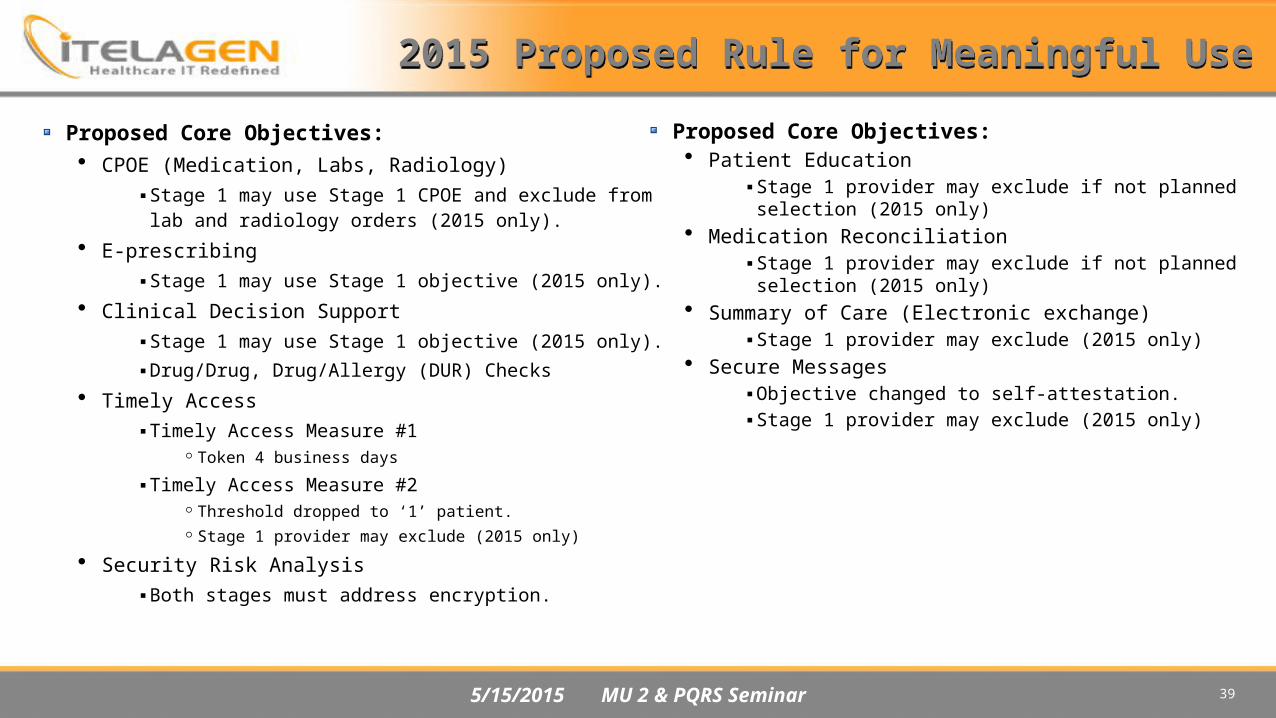
2015 Proposed Rule for Meaningful UseProposed Core Objectives:• CPOE (Medication, Labs, Radiology)
▪ Stage 1 may use Stage 1 CPOE and exclude from lab and radiology orders (2015 only).
• E-prescribing▪ Stage 1 may use Stage 1 objective (2015 only).
• Clinical Decision Support▪ Stage 1 may use Stage 1 objective (2015 only).▪ Drug/Drug, Drug/Allergy (DUR) Checks
• Timely Access▪ Timely Access Measure #1
Token 4 business days▪ Timely Access Measure #2
Threshold dropped to ‘1’ patient. Stage 1 provider may exclude (2015 only)
• Security Risk Analysis▪ Both stages must address encryption.
Proposed Core Objectives:• Patient Education
▪ Stage 1 provider may exclude if not planned selection (2015 only)
• Medication Reconciliation▪ Stage 1 provider may exclude if not planned
selection (2015 only)• Summary of Care (Electronic exchange)
▪ Stage 1 provider may exclude (2015 only)• Secure Messages
▪ Objective changed to self-attestation.▪ Stage 1 provider may exclude (2015 only)

5/15/2015 MU 2 & PQRS Seminar 40
2015 Proposed Rule for Meaningful Use
Public Health Objectives• Stage 1 provider must successfully report on ‘1’ objective (unless all exclusions met, 2015 only).• Stage 2 provider must successfully report on ‘2’ objectives (unless exclusions met and provider has less than 2
options)
Measure Times Measure Can CountImmunization Registry 1Syndromic Surveillance 1Case Reporting (new) 1Public Health Registry (cancer, etc.)
3
Clinical Data Registry Reporting (specialty registry)
3

5/15/2015 MU 2 & PQRS Seminar 41
Minimal products necessary to help demonstrate Stage 2 Meaningful Use if using only NextGen solutions:
• NextGen® Ambulatory EHR 5.8▪ e-Prescribing enabled ▪ NextGen Advanced Audit Utility
NextGen® KBM version 8.3 or higher
NextGen® Health Quality Measures (HQM)
Rosetta Interface Agent • Immunization registry interface • Syndromic reporting interface (if Menu Measure 1 selected) • Cancer Case interface (if Menu Measure 5 selected) • Specialized Registry interface (if Menu Measure 6 selected)
NextGen® Medical Summary Utility
NextGen® Patient Portal (powered by NextMD®) NextGen® Share

5/15/2015 MU 2 & PQRS Seminar 42
White Pages Manual
Nextgen Website: https://knowledge.nextgen.com/pe/action/forums/navigateresults
Download each white page
Use program to attach white page into 1 manual such as PDFil
Have a separate manual for CQM from Menu and Cores
5/15/2015 MU 2 & PQRS Seminar 43
The National Quality Strategy (NQS) In 2015, measures are classified according to the 6 NQS domains based on the NQS’s priorities. PQRS reporting options typically require an EP or PQRS group practice to report 9 or more measures covering at least 3 NQS domains, plus additional cross-cutting measures for EPs with billable face-to-face encounters for satisfactory reporting or participation to avoid the 2017 negative payment adjustment.
The Six NQS Domains: 1. Patient Safety 2. Person and Caregiver-Centered Experience and Outcomes 3. Communication and Care Coordination 4. Effective Clinical Care 5. Community/ Population Health 6. Efficiency and Cost Reduction

5/15/2015 MU 2 & PQRS Seminar 44
PQRS INDIVIDUAL EPs1. Report on at least 9 measures across at least 3 National Quality Strategy (NQS)
domains
2. Use a direct EHR product that is Certified EHR Technology (CEHRT) or EHR data submission vendor that is CEHRT
• If the EP’s CEHRT does not contain patient data for at least 9 measures across at least 3 domains, then the EP must report the measures for which there is Medicare patient data. An EP must report on at least 1 measure containing Medicare patient data.
Note for EHR Incentive Program participants: If an EP satisfactorily reports for 2015 PQRS using the electronic reporting option, (s)he will also satisfy the CQM component of the EHR Incentive program; however, EPs will still be required to meet the other Meaningful Use objectives through the Medicare EHR Incentive Program Registration and Attestation System.

5/15/2015 MU 2 & PQRS Seminar 45
2013 0.5% (performance year for 2015 penalty)
20140.5% (performance year for 2016 penalty)
2015 -1.5%
2016 -2%
2017 -2%
Medicare Physician Quality Reporting System Incentives and Penalties

46

5/15/2015 MU 2 & PQRS Seminar 47
Referencehttp://www.ama-assn.org/ama/pub/physician-resources/clinical-practice-improvement/clinical-quality/physician-quality-reporting-system.page?
2015 Physician Quality Reporting System (PQRS): Implementation Guide 1/15/2015 , CMS
Stage 1 vs. Stage 2 Comparison Table for Eligible Professionals , CMS
MU Core and menu objectives Manual, Nextgen
Nextgen E-Learning