12.palliative care and pain
TRANSCRIPT
283
12 Principles of palliative care 284
Presenting problems in palliative care 284Pain 284Breathlessness 289Cough 289Nausea and vomiting 289Gastrointestinal obstruction 290Weight loss and general weakness 290Anxiety and depression 290Delirium and terminal agitation 290
Palliative care and pain
D. Oxenham
Death and dying 290Talking about and planning towards dying 290Diagnosing dying 291Management 291Ethical issues at the end of life 291
Palliative care and Pain
12
284
symptoms as cancer, as well as psychological and family distress. The ‘palliative phase’ of these illnesses may be more difficult to identify because of periods of relative stability interspersed with acute episodes of severe illness. However, it is still possible to recognise those patients whose care may benefit from a palliative approach. The challenge is that symptom management needs to be delivered at the same time as treatment for acute exacerbations. This leads to difficult decisions as to the balance between symptom relief and aggressive management of the underlying disease. The starting point of need for palliative care in these conditions is the point at which consideration of comfort and individual values becomes important in decision-making, often alongside management of the underlying disease.
The third major trajectory is categorised by years of poor function and frailty before a relatively short terminal period; it is exemplified by dementia, but is also increasingly true for patients with many different chronic illnesses. As medical advances extend survival, this mode of dying is being experienced by increasing numbers of people. The main challenge lies in provid-ing nursing care and ensuring that plans are agreed for the time when medical intervention is no longer beneficial.
In a situation where death is inevitable and foresee-able, palliative care balances the ‘standard textbook’ approach with the wishes and values of the patient and a realistic assessment of the benefits of medical interven-tions. This often results in a greater focus on comfort, symptom control and support for patient and family, and may enable withdrawal of interventions that are ineffective or burdensome. Commonly, the outcome is less certain. In many cases, there is a substantial risk that the patient will die but there may be a small chance of improvement with further treatment. In these circum-stances, it is often (but not always) correct and helpful to share this information with the patient so that better decisions can be made about further care.
The principles of palliative care are being used increasingly in many different diseases so that death can be managed effectively and compassionately. Palliative management of the most common symptoms is dis-cussed in the next section.
PRESENTING PROBLEMS IN PALLIATIVE CARE
Pain
The International Association for the Study of Pain (IASP) has defined pain as ‘an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage’. It follows that each patient’s experience and expression of pain are different, and that severity of pain does not correlate with the degree of tissue damage. Effective pain treatment facilitates recovery from injury or surgery, aids rapid recovery of function, and may mini-mise chronic pain and disability. Unfortunately, the delivery of effective pain relief is often impeded by factors such as poor assessment and concerns about the use of opioid analgesia.
PRINCIPLES OF PALLIATIVE CARE
Palliative care is the active total care of patients with far advanced, rapidly progressive and ultimately fatal disease. Its focus is quality of life rather than cure, and it encompasses a distinct body of knowledge and skills that all good physicians must possess to allow them to care effectively for patients at the end of life. In palliative care, there is a fundamental change of emphasis in decision-making away from a focus on prolonging life towards decisions that balance comfort and the indi-vidual’s wishes with treatments that might prolong life. There is a growing recognition that the principles of, and some specific interventions developed in the palliative care of patients with cancer are equally applicable to other conditions. The principles of palliative care may therefore be applied not only to cancer but also to any chronic disease state.
Palliative care is often seen as a means of managing distress and symptoms in patients with cancer, where metastatic disease has been diagnosed and death is seen as inevitable. In other illnesses, the challenge is recognis-ing when patients have entered this phase of their illness, as there are fewer clear markers and the course of the illness is much more variable.
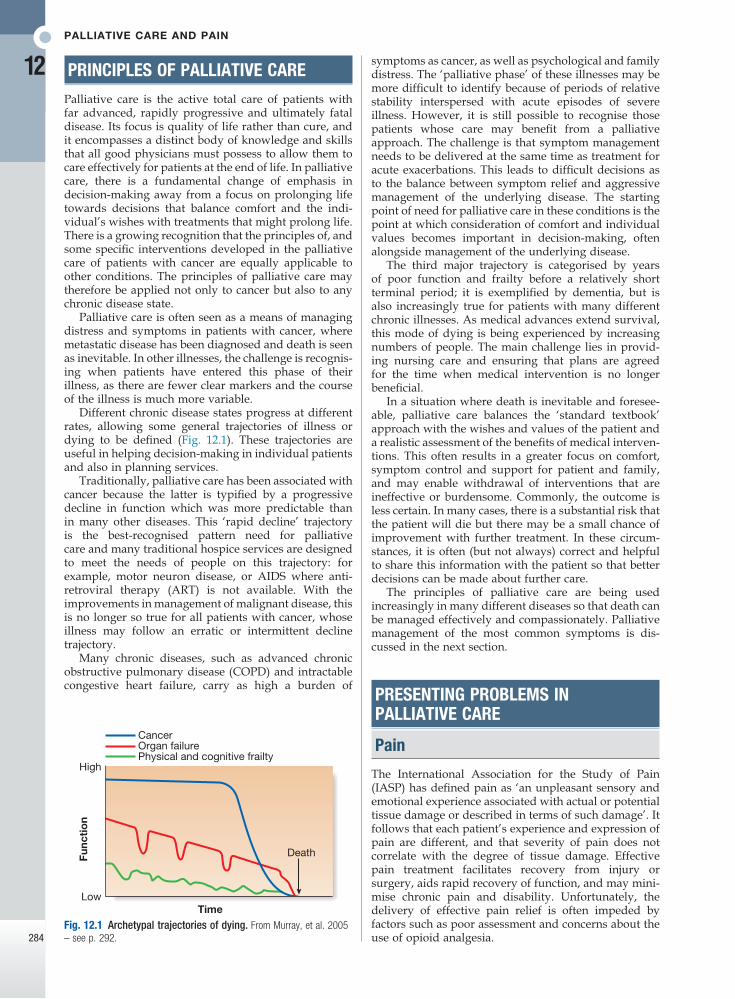
Different chronic disease states progress at different rates, allowing some general trajectories of illness or dying to be defined (Fig. 12.1). These trajectories are useful in helping decision-making in individual patients and also in planning services.
Traditionally, palliative care has been associated with cancer because the latter is typified by a progressive decline in function which was more predictable than in many other diseases. This ‘rapid decline’ trajectory is the best-recognised pattern need for palliative care and many traditional hospice services are designed to meet the needs of people on this trajectory: for example, motor neuron disease, or AIDS where anti-retroviral therapy (ART) is not available. With the improvements in management of malignant disease, this is no longer so true for all patients with cancer, whose illness may follow an erratic or intermittent decline trajectory.
Many chronic diseases, such as advanced chronic obstructive pulmonary disease (COPD) and intractable congestive heart failure, carry as high a burden of
Fig. 12.1 Archetypal trajectories of dying. From Murray, et al. 2005 – see p. 292.
High
Death
CancerOrgan failurePhysical and cognitive frailty
Func
tio
n
LowTime

Presenting problems in palliative care
12
285
as agitation and withdrawn posture, to assess levels of pain. Commonly used scales include Abbey and Dolorplus. Changes in behavioural rating pain scores can indicate whether drug measures have been successful.Regular recording of formal pain assessment and
patient-rated pain scores improves pain management and reduces the time taken to achieve pain control.
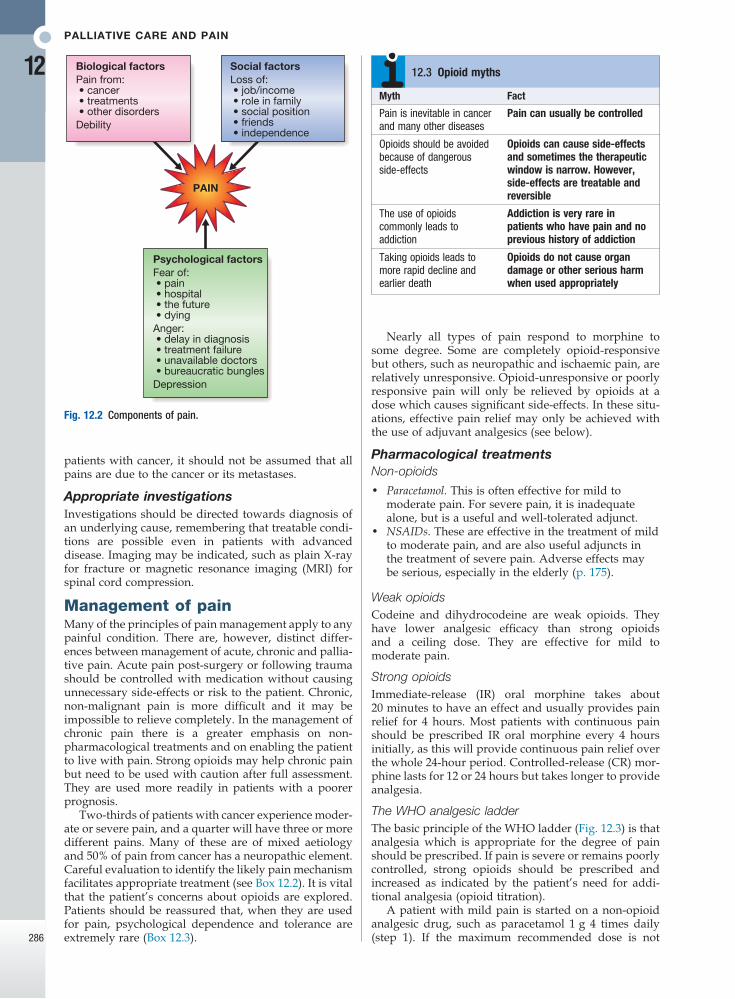
Psychological aspects of chronic painPerception of pain is influenced by many factors other than the painful stimulus, and pain cannot therefore be easily classified as wholly physical or psychogenic in any individual (Fig. 12.2). Patients who suffer chronic pain will be affected emotionally and, conversely, emo-tional distress can exacerbate physical pain (p. 240). Full assessment for symptoms of anxiety and depression is essential to effective pain management.
ExaminationThis should include careful assessment of the painful area, looking for signs of neuropathic pain (see Box 12.1) or bony tenderness suggestive of bone metastases. In
Pain classification and mechanismsPain can be classified into two types:• Nociceptive: due to direct stimulation of peripheral
nerve endings by a noxious stimulus such as trauma, burns or ischaemia.
• Neuropathic: due to dysfunction of the pain perception system within the peripheral or central nervous system as a result of injury, disease or surgical damage, such as continuing pain experienced from a limb which has been amputated (phantom limb pain). This should be identified early (Box 12.1) because it is more difficult to treat once established.The pain perception system (p. 1147) is not a simple
hard-wired circuit of nerves connecting tissue pain receptors to the brain, but a dynamic system in which a continuing pain stimulus can cause central changes that lead to an increase in pain perception. This plasticity (changeability) applies to all the peripheral and central components of the pain pathway. Early and appropriate treatment of pain reduces the potential for chronic unde-sirable changes to develop.
Assessment and measurement of painAccurate assessment of the patient is the first step in providing good analgesia.
History and measurement of painA full pain history should be taken, to establish its causes and the underlying diagnoses. Patients may have more than one pain; for example, bone and neuropathic pain may both arise from skeletal metastases (Box 12.2).
A diagram of the body on which the patient can mark the pain site can be helpful. When asked to score pain, patients consistently rate it higher than health profes-sionals and should, if able, always be asked to rate pain themselves. Methods include:• Verbal rating scale. Different verbal descriptions are
used to rate pain – ’no pain’, ‘mild pain’, ‘moderate pain’ and ‘severe pain’.
• Visual analogue scale. A question is used, such as ‘Over the past 24 hours, how would you rate your pain, if 0 is no pain and 10 is the worst pain you could imagine?’
• Behavioural rating scale. It can be particularly difficult to decide whether a patient with cognitive impairment is suffering pain. A variety of measures are available which use observed behaviours, such
Type of pain FeaturesManagement options
Bone pain Tender area over bone Possible pain on movement
Non-steroidal anti-inflammatory drugs (NSAIDs)BisphosphonatesRadiotherapy
Increased intracranial pressure
Headache, worse in the morning, associated with vomiting and occasionally confusion
CorticosteroidsRadiotherapyCodeine
Abdominal colic
Intermittent, severe, spasmodic, associated with nausea or vomiting
AntispasmodicsHyoscine butylbromide
Liver capsule pain
Right upper quadrant abdominal pain, often associated with tender enlarged liverResponds poorly to opioids
Corticosteroids
Neuropathic pain
See Box 12.1 Anticonvulsants:GabapentinPregabalinCarbamazepineAntidepressantsAmitriptylineDuloxetineKetamine
Ischaemic pain
Diffuse severe aching pain associated with evidence of poor perfusionResponds poorly to opioids
NSAIDsKetamine
Incident pain
Episodic pain usually related to movement or bowel spasm
Intermittent short-acting opioids Nerve block
12.2 Types of pain
• Burning, stabbing or pulsing pain• Spontaneous pain, without ongoing tissue damage• Pain in an area of sensory loss• Presence of a major neurological deficit• Pain in response to non-painful stimuli: ‘allodynia’• Increased pain in response to painful stimuli: ‘hyperalgesia’• Unpleasant abnormal sensations: ‘dysaesthesias’• Poor relief from opioids alone
12.1 Features of neuropathic pain
Palliative care and Pain
12
286
Nearly all types of pain respond to morphine to some degree. Some are completely opioid-responsive but others, such as neuropathic and ischaemic pain, are relatively unresponsive. Opioid-unresponsive or poorly responsive pain will only be relieved by opioids at a dose which causes significant side-effects. In these situ-ations, effective pain relief may only be achieved with the use of adjuvant analgesics (see below).
Pharmacological treatmentsNon-opioids
• Paracetamol. This is often effective for mild to moderate pain. For severe pain, it is inadequate alone, but is a useful and well-tolerated adjunct.
• NSAIDs. These are effective in the treatment of mild to moderate pain, and are also useful adjuncts in the treatment of severe pain. Adverse effects may be serious, especially in the elderly (p. 175).
Weak opioidsCodeine and dihydrocodeine are weak opioids. They have lower analgesic efficacy than strong opioids and a ceiling dose. They are effective for mild to moderate pain.
Strong opioidsImmediate-release (IR) oral morphine takes about 20 minutes to have an effect and usually provides pain relief for 4 hours. Most patients with continuous pain should be prescribed IR oral morphine every 4 hours initially, as this will provide continuous pain relief over the whole 24-hour period. Controlled-release (CR) mor-phine lasts for 12 or 24 hours but takes longer to provide analgesia.
The WHO analgesic ladderThe basic principle of the WHO ladder (Fig. 12.3) is that analgesia which is appropriate for the degree of pain should be prescribed. If pain is severe or remains poorly controlled, strong opioids should be prescribed and increased as indicated by the patient’s need for addi-tional analgesia (opioid titration).
A patient with mild pain is started on a non-opioid analgesic drug, such as paracetamol 1 g 4 times daily (step 1). If the maximum recommended dose is not
patients with cancer, it should not be assumed that all pains are due to the cancer or its metastases.
Appropriate investigationsInvestigations should be directed towards diagnosis of an underlying cause, remembering that treatable condi-tions are possible even in patients with advanced disease. Imaging may be indicated, such as plain X-ray for fracture or magnetic resonance imaging (MRI) for spinal cord compression.
Management of painMany of the principles of pain management apply to any painful condition. There are, however, distinct differ-ences between management of acute, chronic and pallia-tive pain. Acute pain post-surgery or following trauma should be controlled with medication without causing unnecessary side-effects or risk to the patient. Chronic, non-malignant pain is more difficult and it may be impossible to relieve completely. In the management of chronic pain there is a greater emphasis on non-pharmacological treatments and on enabling the patient to live with pain. Strong opioids may help chronic pain but need to be used with caution after full assessment. They are used more readily in patients with a poorer prognosis.
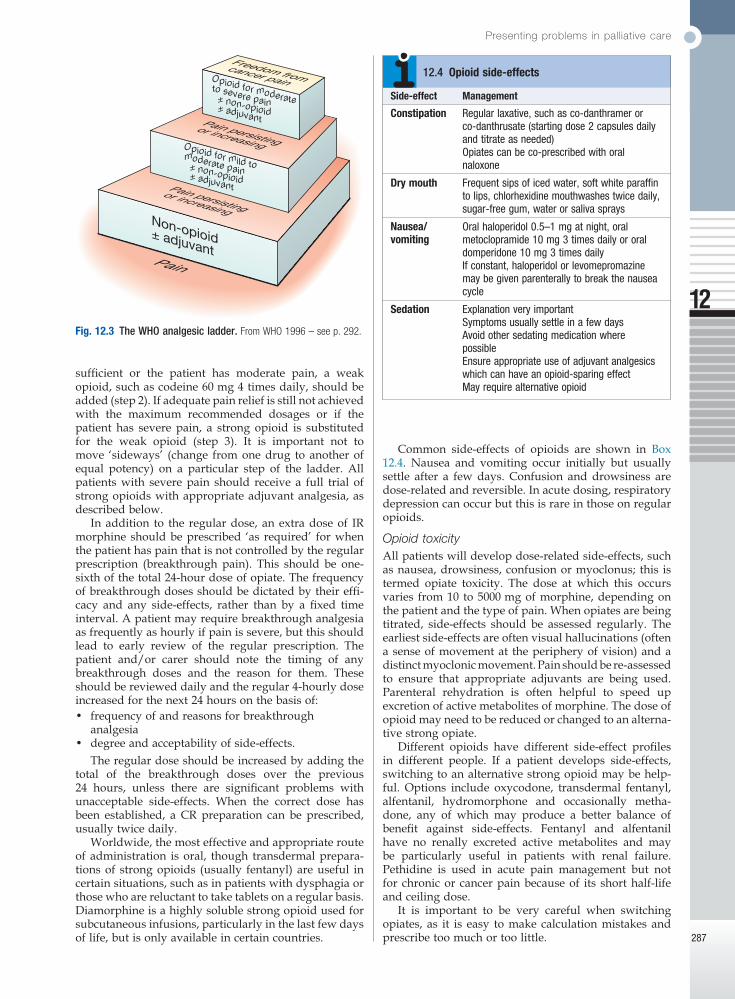
Two-thirds of patients with cancer experience moder-ate or severe pain, and a quarter will have three or more different pains. Many of these are of mixed aetiology and 50% of pain from cancer has a neuropathic element. Careful evaluation to identify the likely pain mechanism facilitates appropriate treatment (see Box 12.2). It is vital that the patient’s concerns about opioids are explored. Patients should be reassured that, when they are used for pain, psychological dependence and tolerance are extremely rare (Box 12.3).
Fig. 12.2 Components of pain.
PAIN
Psychological factorsFear of: • pain • hospital • the future • dyingAnger: • delay in diagnosis • treatment failure • unavailable doctors • bureaucratic bunglesDepression
Biological factorsPain from: • cancer • treatments • other disordersDebility
Social factorsLoss of: • job/income • role in family • social position • friends • independence
Myth Fact
Pain is inevitable in cancer and many other diseases
Pain can usually be controlled
Opioids should be avoided because of dangerous side-effects
Opioids can cause side-effects and sometimes the therapeutic window is narrow. However, side-effects are treatable and reversible
The use of opioids commonly leads to addiction
Addiction is very rare in patients who have pain and no previous history of addiction
Taking opioids leads to more rapid decline and earlier death
Opioids do not cause organ damage or other serious harm when used appropriately
12.3 Opioid myths
Presenting problems in palliative care
12
287
Common side-effects of opioids are shown in Box 12.4. Nausea and vomiting occur initially but usually settle after a few days. Confusion and drowsiness are dose-related and reversible. In acute dosing, respiratory depression can occur but this is rare in those on regular opioids.
Opioid toxicityAll patients will develop dose-related side-effects, such as nausea, drowsiness, confusion or myoclonus; this is termed opiate toxicity. The dose at which this occurs varies from 10 to 5000 mg of morphine, depending on the patient and the type of pain. When opiates are being titrated, side-effects should be assessed regularly. The earliest side-effects are often visual hallucinations (often a sense of movement at the periphery of vision) and a distinct myoclonic movement. Pain should be re-assessed to ensure that appropriate adjuvants are being used. Parenteral rehydration is often helpful to speed up excretion of active metabolites of morphine. The dose of opioid may need to be reduced or changed to an alterna-tive strong opiate.
Different opioids have different side-effect profiles in different people. If a patient develops side-effects, switching to an alternative strong opioid may be help-ful. Options include oxycodone, transdermal fentanyl, alfentanil, hydromorphone and occasionally metha-done, any of which may produce a better balance of benefit against side-effects. Fentanyl and alfentanil have no renally excreted active metabolites and may be particularly useful in patients with renal failure. Pethidine is used in acute pain management but not for chronic or cancer pain because of its short half-life and ceiling dose.
It is important to be very careful when switching opiates, as it is easy to make calculation mistakes and prescribe too much or too little.
sufficient or the patient has moderate pain, a weak opioid, such as codeine 60 mg 4 times daily, should be added (step 2). If adequate pain relief is still not achieved with the maximum recommended dosages or if the patient has severe pain, a strong opioid is substituted for the weak opioid (step 3). It is important not to move ‘sideways’ (change from one drug to another of equal potency) on a particular step of the ladder. All patients with severe pain should receive a full trial of strong opioids with appropriate adjuvant analgesia, as described below.
In addition to the regular dose, an extra dose of IR morphine should be prescribed ‘as required’ for when the patient has pain that is not controlled by the regular prescription (breakthrough pain). This should be one-sixth of the total 24-hour dose of opiate. The frequency of breakthrough doses should be dictated by their effi-cacy and any side-effects, rather than by a fixed time interval. A patient may require breakthrough analgesia as frequently as hourly if pain is severe, but this should lead to early review of the regular prescription. The patient and/or carer should note the timing of any breakthrough doses and the reason for them. These should be reviewed daily and the regular 4-hourly dose increased for the next 24 hours on the basis of:• frequency of and reasons for breakthrough
analgesia• degree and acceptability of side-effects.
The regular dose should be increased by adding the total of the breakthrough doses over the previous 24 hours, unless there are significant problems with unacceptable side-effects. When the correct dose has been established, a CR preparation can be prescribed, usually twice daily.
Worldwide, the most effective and appropriate route of administration is oral, though transdermal prepara-tions of strong opioids (usually fentanyl) are useful in certain situations, such as in patients with dysphagia or those who are reluctant to take tablets on a regular basis. Diamorphine is a highly soluble strong opioid used for subcutaneous infusions, particularly in the last few days of life, but is only available in certain countries.
Fig. 12.3 The WHO analgesic ladder. From WHO 1996 – see p. 292.
Opioid for moderateto severe pain ± non-opioid ± adjuvant
Opioid for mild tomoderate pain ± non-opioid ± adjuvant
Non-opioid± adjuvant
Pain persistingor increasing
Pain persistingor increasing
Freedom fromcancer pain
Pain
Side-effect Management
Constipation Regular laxative, such as co-danthramer or co-danthrusate (starting dose 2 capsules daily and titrate as needed)Opiates can be co-prescribed with oral naloxone
Dry mouth Frequent sips of iced water, soft white paraffin to lips, chlorhexidine mouthwashes twice daily, sugar-free gum, water or saliva sprays
Nausea/vomiting
Oral haloperidol 0.5–1 mg at night, oral metoclopramide 10 mg 3 times daily or oral domperidone 10 mg 3 times dailyIf constant, haloperidol or levomepromazine may be given parenterally to break the nausea cycle
Sedation Explanation very importantSymptoms usually settle in a few daysAvoid other sedating medication where possibleEnsure appropriate use of adjuvant analgesics which can have an opioid-sparing effectMay require alternative opioid
12.4 Opioid side-effects
Palliative care and Pain
12
288
Adjuvant analgesicsAn adjuvant analgesic is a drug with a primary indica-tion other than pain but which provides analgesia in some painful conditions and may enhance the effect of the primary analgesic. At each step of the WHO analge-sic ladder, an adjuvant analgesic should be considered, the choice depending on the type of pain (Boxes 12.5 and 12.6).
Non-pharmacological and complementary treatmentsRadiotherapyRadiotherapy can improve pain from bone metastases and may be considered for cancer in other sites (see Box 12.2).
PhysiotherapyThis helps to alleviate pain and restore function, through active mobilisation and specific physiotherapy tech-niques, such as spinal manipulation, massage, applica-tion of heat or cold, and exercise. Immediate application of cold with ice packs can reduce subsequent swelling and inflammation after a direct injury.
Psychological techniquesThese include simple relaxation, hypnosis, cognitive behavioural therapies and biofeedback (pp. 240–241), which train the patient to use coping strategies and behavioural techniques. This is often more relevant in chronic non-malignant pain than in cancer pain.
Fig. 12.4 Acupuncture.
‘Tricyclic antidepressants, a variety of anticonvulsants, and gabapentin are effective treatments for neuropathic pain.’
• Guideline 106. Scottish Intercollegiate Guidelines Network; 2008.
For further information: www.sign.ac.uk
12.5 Treatment of neuropathic pain
Stimulation therapiesAcupuncture (Fig. 12.4) has been used successfully in Eastern medicine for centuries. It causes release of endogenous analgesics (endorphins) within the spinal cord. It can be particularly effective in pain related to muscle spasm. Transcutaneous electrical nerve stimula-tion (TENS) may have a similar mechanism of action to acupuncture and can be used in both acute and chronic pain.
Herbal medicine and homeopathyThese are widely used for pain, but often with little evidence for efficacy (p. 15). Safety regulations for these treatments are limited, compared with conventional drugs, and the doctor should be wary of unrecognised side-effects which may result.
Drug Example Indications Side-effects*
NSAIDs Diclofenac Bone metastases, soft tissue infiltration, liver pain, inflammatory pain
Gastric irritation and bleeding, fluid retention, headache; caution in renal impairment
Corticosteroids Dexamethasone 8–16 mg per day, titrated to lowest dose that controls pain
Raised intracranial pressure, nerve compression, soft tissue infiltration, liver pain
Gastric irritation if used together with NSAID, fluid retention, confusion, Cushingoid appearance, candidiasis, hyperglycaemia
Anticonvulsants Evidence strongest for:GabapentinPregabalinDuloxetine
Neuropathic pain of any aetiology
Mild sedation, tremor, confusion
Tricyclic antidepressants
Amitriptyline Neuropathic pain of any aetiology
Sedation, dizziness, confusion, dry mouth, constipation, urinary retention; avoid in cardiac disease
NMDA blockers Ketamine Severe neuropathic pain (only under specialist supervision)
Confusion, anxiety, agitation, hypertension
(NMDA = N-methyl-D-aspartate)
12.6 Adjuvant analgesics
*In old age, all drugs can cause confusion.
Presenting problems in palliative care
12
289
Cough
Cough can be a troubling symptom in cancer and other illnesses such as motor neuron disease, cardiac failure and COPD. There are many possible causes (p. 654). Management should focus on treating the underlying condition if possible. If this fails to bring about the desired response, antitussives, such as codeine linctus, are sometimes effective, particularly for cough at night.
Nausea and vomiting
The presentation of nausea and vomiting differs, depending on the underlying cause, of which there are many (p. 853). Large-volume vomiting with little nausea is common in intestinal obstruction, whereas constant nausea with little or no vomiting is often due to meta-bolic abnormalities or drugs. Vomiting related to raised intracranial pressure is worse in the morning.
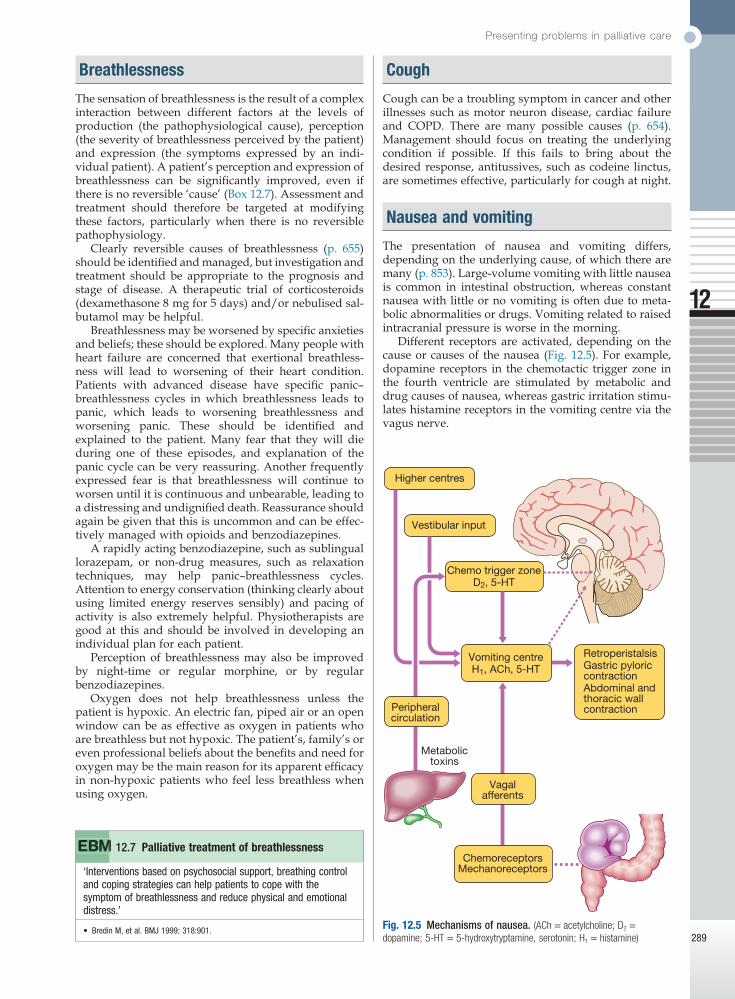
Different receptors are activated, depending on the cause or causes of the nausea (Fig. 12.5). For example, dopamine receptors in the chemotactic trigger zone in the fourth ventricle are stimulated by metabolic and drug causes of nausea, whereas gastric irritation stimu-lates histamine receptors in the vomiting centre via the vagus nerve.
Breathlessness
The sensation of breathlessness is the result of a complex interaction between different factors at the levels of production (the pathophysiological cause), perception (the severity of breathlessness perceived by the patient) and expression (the symptoms expressed by an indi-vidual patient). A patient’s perception and expression of breathlessness can be significantly improved, even if there is no reversible ‘cause’ (Box 12.7). Assessment and treatment should therefore be targeted at modifying these factors, particularly when there is no reversible pathophysiology.
Clearly reversible causes of breathlessness (p. 655) should be identified and managed, but investigation and treatment should be appropriate to the prognosis and stage of disease. A therapeutic trial of corticosteroids (dexamethasone 8 mg for 5 days) and/or nebulised sal-butamol may be helpful.
Breathlessness may be worsened by specific anxieties and beliefs; these should be explored. Many people with heart failure are concerned that exertional breathless-ness will lead to worsening of their heart condition. Patients with advanced disease have specific panic–breathlessness cycles in which breathlessness leads to panic, which leads to worsening breathlessness and worsening panic. These should be identified and explained to the patient. Many fear that they will die during one of these episodes, and explanation of the panic cycle can be very reassuring. Another frequently expressed fear is that breathlessness will continue to worsen until it is continuous and unbearable, leading to a distressing and undignified death. Reassurance should again be given that this is uncommon and can be effec-tively managed with opioids and benzodiazepines.
A rapidly acting benzodiazepine, such as sublingual lorazepam, or non-drug measures, such as relaxation techniques, may help panic–breathlessness cycles. Attention to energy conservation (thinking clearly about using limited energy reserves sensibly) and pacing of activity is also extremely helpful. Physiotherapists are good at this and should be involved in developing an individual plan for each patient.
Perception of breathlessness may also be improved by night-time or regular morphine, or by regular benzodiazepines.
Oxygen does not help breathlessness unless the patient is hypoxic. An electric fan, piped air or an open window can be as effective as oxygen in patients who are breathless but not hypoxic. The patient’s, family’s or even professional beliefs about the benefits and need for oxygen may be the main reason for its apparent efficacy in non-hypoxic patients who feel less breathless when using oxygen.
Fig. 12.5 Mechanisms of nausea. (ACh = acetylcholine; D2 = dopamine; 5-HT = 5-hydroxytryptamine, serotonin; H1 = histamine)
Higher centres
Vestibular input
Vomiting centreH1, ACh, 5-HT
Chemo trigger zoneD2, 5-HT
Vagalafferents
Metabolictoxins
ChemoreceptorsMechanoreceptors
RetroperistalsisGastric pyloriccontractionAbdominal andthoracic wallcontractionPeripheral
circulation
‘Interventions based on psychosocial support, breathing control and coping strategies can help patients to cope with the symptom of breathlessness and reduce physical and emotional distress.’
• Bredin M, et al. BMJ 1999; 318:901.
12.7 Palliative treatment of breathlessness
Palliative care and Pain
12
290
Anxiety and depression
Depression is common in palliative care but diagnosis is more difficult, as the physical symptoms of depression are similar to those of advanced disease. Anxiety and depression may still respond to treatment with a com-bination of drugs and psychotherapeutic approaches (p. 243). Citalopram and mirtazapine are better tolerated in patients with advanced disease. It should not be assumed that depression is an ‘understandable’ conse-quence of the patient’s situation.
Delirium and terminal agitation
Many patients become confused or agitated in the last days of life. It is important to identify and treat poten-tially reversible causes (pp. 173 and 280), unless the patient is too close to death for this to be feasible. Early diagnosis and effective management of delirium are extremely important. As in other palliative situations, it may not be possible to identify and treat the underlying cause, and the focus of management may be to ensure comfort. It is important to distinguish between behav-ioural change due to pain and that due to delirium, as opioids will improve one and worsen the other.
The management of delirium is detailed on page 174. It is important, even in palliative care to treat delirium with antipsychotic medicines such as haloperidol rather than regard it as distress or anxiety and use benzo-diazepines only.
DEATH AND DYING
Talking about and planning towards dying
There have been dramatic improvements in medical treatment and care of patients with cancer and other illnesses over recent years, but the inescapable fact remains that everyone will die at some time. Planning for death is not required for people who die suddenly but should be actively considered in patients with chronic diseases when the death is considered to be fore-seeable or inevitable. Doctors rarely know exactly when a patient will die but we are often aware that the risk of dying is increasing and that medical interventions are unlikely to prolong life or improve function. Many people wish their doctors to be honest about this situa-tion to allow them time to think ahead, make plans and address practical issues. A smaller number do not wish to discuss future deterioration or death; this avoidance of discussion should be respected.
For doctors, it is helpful to understand an individu-al’s wishes and values about medical interventions at this time, as this can help guide decisions about ceilings of intervention. Some interventions will not work in patients with far advanced disease. It is useful to distin-guish between those that will not work (a medical deci-sion) and those that do not confer sufficient benefit to be worthwhile (a decision that can only be reached with a patient’s involvement and consent). A common example
Reversible causes, such as hypercalcaemia and con-stipation, should be treated appropriately. Drug-induced causes should be considered and the offending drugs stopped if possible. As different classes of antiemetic drug act at different receptors, antiemetic therapy should be based on a careful assessment of the probable causes and a rational decision to use a particular class of drug (Box 12.8). The subcutaneous route is often required ini-tially to overcome gastric stasis and poor absorption of oral medicines.
Gastrointestinal obstruction
Gastrointestinal obstruction is a frequent complication of intra-abdominal cancer. Patients may have multiple levels of obstruction and symptoms may vary greatly in nature and severity. Surgical mortality is high in patients with advanced disease and obstruction should normally be managed without surgery.
The key to effective management is to address the presenting symptoms – colic, abdominal pain, nausea, vomiting, intestinal secretions – individually or in com-bination, using drugs which do not cause or worsen other symptoms. This can be problematic when a spe-cific treatment worsens another symptom. Cyclizine improves nausea and colic responds well to anticholin-ergic agents, such as hyoscine butylbromide, but both slow gut motility. Nausea will improve with metoclo-pramide, although this is contraindicated in the pres-ence of colic because of its prokinetic effect. There is some evidence that corticosteroids (dexamethasone 8 mg) can shorten the length of obstructive episodes. Somatostatin analogues, such as octreotide, will reduce intestinal secretions and therefore large-volume vomits. Occasionally, a nasogastric tube is required to reduce gaseous or fluid distension.
Weight loss and general weakness
Patients with cancer lose weight due to an alteration of metabolism by the tumour known as the cancer cachexia syndrome. NSAIDs and megestrol may be helpful in early-stage disease but are unlikely to be effective in advanced cancer. Corticosteroids can temporarily boost appetite and general well-being, but may cause false weight gain by promoting fluid retention. Their benefits need to be weighed against the risk of side-effects.
Area Receptors Drugs
Chemo trigger zone Dopamine2
5-HTHaloperidolMetoclopramide
Vomiting centre Histamine1
AcetylcholineCyclizineLevomepromazineHyoscine
Gut (gastric stasis) Metoclopramide
Gut distension (vagal stimulation)
Histamine1 Cyclizine
Gut (chemoreceptors) 5-HT Levomepromazine
12.8 Receptor site activity of antiemetic drugs
Death and dying
12
291
shift in management (Box 12.9). Symptom control, relief of distress and care for the family become the most important elements of care. Medication and investiga-tion are only justifiable if they contribute to these ends. When patients can no longer drink because they are dying, intravenous fluids are usually not necessary and may cause worsening of bronchial secretions. Medicines should always be prescribed for the relief of symptoms. For example, morphine or diamorphine may be used to control pain, levomepromazine to control nausea, haloperidol to treat confusion, diazepam or midazolam to treat distress, and hyoscine hydrobromide to reduce respiratory secretions. Side-effects, such as drowsiness, may be acceptable if the principal aim of relieving dis-tress is achieved. It is important to discuss and agree the aims of care with the patient’s family.
Ethical issues at the end of life
In Europe, between 25 and 50% of all deaths are associ-ated with some form of decision which may affect the length of a patient’s life. The most common form of deci-sion involves withdrawing or withholding further treat-ment: for example, not treating a chest infection in a patient who is clearly dying from advanced cancer. It is important to have a framework for considering such decisions (such as the four ethical principles: autonomy, beneficence, non-maleficence and justice, p. 10), which balances degrees of importance when there is conflict: for example, when a patient wishes to receive treatment which a doctor believes will be ineffective or which may cause harm. A decision has to be taken as to which principle is most important: whether it is better to respect a patient’s wishes, even if it causes harm, or to reduce the risk of harm but not accede to those wishes.
A futile treatment is one which has no chance of achieving worthwhile benefit: that is, the treatment cannot achieve a result that the patient would consider, now or in the future, to be worthwhile. Doctors are not required to institute futile treatments, such as resuscita-tion, in the event of cardiac arrest in a patient with ter-minal cancer.
Incapacity and advance directivesPatients’ wishes are very important in Western medical ethics, although other cultures emphasise the views of the family. If a patient is unable to express his or her view because of communication or cognitive impair-ment, that person lacks ‘capacity’. In order to decide what the patient would have wished, as much informa-tion as possible should be gained about any previously expressed wishes, along with the views of relatives and other health professionals.
An advance directive is a previously recorded, written document of a patient’s wishes (p. 171). It should carry the same weight in decision-making as a patient’s contemporaneously expressed wishes, but may not be sufficiently specific to be used in a particular clinical situation. The legal framework for decision-making varies in different countries.
HydrationDeciding whether to give intravenous fluids can be dif-ficult when a patient is very unwell and the prognosis
of this would be decisions about not attempting cardio-pulmonary resuscitation.
In general, people wish for a dignified and peaceful death and most prefer to die at home. Families also are grateful for the chance to prepare themselves for the death of a relative, by timely and gentle discussion with their doctor or other health professionals. Early discussion and effective planning improve the chances that an individual’s wishes will be achieved.
Diagnosing dying
When patients with cancer become bed-bound, semi-comatose, unable to take tablets and only able to take sips of water, with no reversible cause, they are likely to be dying and many will have died within 2 days. Patients with other conditions also reach a stage where death is predictable and imminent. Doctors are sometimes poor at recognising this, and should be alert to the views of other members of the multidisciplinary team. A clear decision that the patient is dying should be agreed and recorded.
Management
Once the conclusion has been reached that a patient is going to die in the next few days, there is a significant
Patient and family awareness
• Assess patient’s and family’s awareness of the situation• Ensure family understands plan of care
Medical interventions
• Stop non-essential medications that do not contribute to symptom control
• Stop inappropriate investigations and interventions, including routine observations
Resuscitation
• Complete Do Not Attempt Cardiopulmonary Resuscitation (DNACPR) form
• Deactivate implantable defibrillator
Symptom control
• Ensure availability of parenteral medication for symptom relief
Support for family
• Make sure you have contact details for family, that you know when they want to be contacted and that they are aware of the facilities available to them
Religious and spiritual needs
• Make sure any particular wishes are identified and followed
Ongoing assessment
• Family’s awareness of condition• Management of symptoms• Need for parenteral hydration
Care after death
• Make sure family know what they have to do• Notify other appropriate health professionals
12.9 How to manage a patient who is dying

Palliative care and Pain
12
292
in many others; public ethical and legal debate over this issue is likely to continue.
Further information and acknowledgements
Websiteswww.anaesthetist.com/ Information on pain physiology and
acute management of pain.www.helpthehospices.org.uk/clip/index.htm Useful online
tutorials on all aspects of palliative symptom control.www.palliativecareguidelines.scot.nhs.uk Regularly reviewed,
evidence-based clinical guidelines.www.palliativedrugs.co.uk Information for health professionals
about the use of drugs in palliative care. It highlights drugs given for unlicensed indications or by unlicensed routes, and the administration of multiple drugs by continuous subcutaneous infusion.
Figure acknowledgementsFig. 12.1 Reproduced from Murray SA, Kendall M, Boyd K,
et al. Illness trajectories and palliative care. BMJ 2005; 330:7498; reproduced with permission from the BMJ Publishing Group.
Fig. 12.3 WHO. Cancer pain relief. 2nd edn. Geneva: WHO; 1996.
is uncertain. If a patient is clearly dying and has a prog-nosis of a few days, rehydration may cause harm by increasing bronchial secretions, and will not benefit the patient by prolonging life. A patient with a major stroke, who is unable to swallow but expected to survive the event, will develop renal impairment and thirst if not given fluids and should be hydrated. Each decision should be individual and discussed with the patient’s family.
EuthanasiaIn the UK and Europe, between 3 and 6% of dying patients ask a doctor to end their life. Many of these requests are transient; some are associated with poor control of physical symptoms or a depressive illness. All expressions of a wish to die are an opportunity to help the patient discuss and address unresolved issues and problems.
Reversible causes, such as pain or depression, should be treated. Sometimes, patients may choose to discon-tinue life-prolonging treatments, such as diuretics or anticoagulation, following discussion and the provision of adequate alternative symptom control. However, there remain a small number of patients who have a sustained, competent wish to end their lives, despite good control of physical symptoms. Euthanasia is now permitted or legal in some countries but remains illegal