pain and symptom management in palliative care - … · effective pain and symptom management in...
TRANSCRIPT

Effective Pain and Symptom Management in Palliative Care
Phyllis A. Grauer, RPh, PharmD, CGP, CPE, Pain and Palliative Care Clinical Consultant, Independent Contractor, Plain City,
OH; and Bryce A. Jackman, RPh, BCNSP, Director of Pharmacy, CarePro Home Infusion, Cedar Rapids, IA

Disclosure Slide
Phyllis Grauer is a Pain and Palliative Care Clinical Consultant. The conflict of interest was resolved by peer review of slide content.
The speakers declare no financial disclosures.
Clinical trials and off‐label/investigational uses may be discussed during this presentation.
3/23/2014 2

CE Credit in Five Easy Steps!1. Scan your badge as you enter each session.2. Carry your Evaluation Packet to every session so you can add session evaluation forms to it.3. Track your hours on the “Statement of Session Attendance Form” as you go.4. At your last session, total the hours and sign both pages of your Statement of Session
Attendance Form. Keep the PINK copy for your records. Put the YELLOW and WHITE copies in your Evaluation Packet. Make sure a completed Session Evaluation Form is in your Evaluation Packet for each session
you attended.• Missing one? Extras are in a file near Registration.
5. Complete the General Attendance Evaluation Form located in your Evaluation Packet—and place it back in your envelope. Write your name on the outside of your Evaluation Packet envelope, seal it, and drop it in the
box near Registration. Applying for Pharmacy CPE? If you have not yet registered for an NABP e‐Profile ID, please
visit www.MyCPEmonitor.net to do so before submitting your packet. You must enter your NABP e‐Profile ID in order to receive CE credit this year!
3/23/2014 3

Objectives• Explain the conditions and diagnoses most likely to require
pain and symptom management in palliative care.
• List and describe the therapies most commonly administered for pain and symptom control.
• Describe the clinical considerations for compounding and administering single and multi‐drug pain control regimens.
• Describe the progression of treatment in patients moving from palliative to terminal/hospice care, and the implications this progression can have for medication
4

What is Palliative Care ?• Palliative care means patient and family‐centered care
that optimizes quality of life by anticipating, preventing and treating suffering.
• Palliative care throughout the continuum of illness involves addressing physical, intellectual, emotional, social and spiritual needs and to facilitate patient autonomy, access to information and choice.
5National Consensus Project for Quality Palliative Care (2013). Clinical Practice Guidelines for Quality Palliative Care, Third Edition. Pittsburgh, PA http://www.nationalconsensusproject.org.

What is Palliative Care ?• The following features characterize palliative care philosophy and delivery:– Care is provided and services are coordinated by an
interdisciplinary team– Patients, families, palliative and non‐palliative health care
providers collaborate and communicate about care needs– Services are available concurrently with or independent of
curative or life‐prolonging care– Patient and family hopes for peace and dignity are supported
throughout the course of illness, during the dying process, and after death
6National Consensus Project for Quality Palliative Care (2013). Clinical Practice Guidelines for Quality Palliative Care, Third Edition. Pittsburgh, PA http://www.nationalconsensusproject.org.

Life‐Limiting DiseaseFocus: curative/restorative treatment
Palliative CareFocus: symptom management, whole person care
Hospice Care< 6 month prognosis
Living
with
Risk
Factors
Life
Closure
Imminent
Death
Death &
Bereavem
ent
Palliative Care Continuum7Palliative Care Consultant 3rd Ed

Common ConditionsAdults:• Amyotrophic lateral sclerosis• Cancer• Dementia• Diabetes• Heart disease• HIV/AIDS• Kidney failure• Liver failure• Lung disease • Multiple sclerosis• Stroke
Children:• Birth defects• Heart defects• Certain cancers (leukemia,
brain & neurological cancers, bone cancers & lymphoma
• Cystic fibrosis• Muscular dystrophy• Cerebral palsy• Sickle cell anemia• Spina bifida• Liver disease• Kidney disease
8

JLynn ”Handbook for Mortals” 9

Common Symptoms• Pain• Nausea/vomiting• Anxiety/agitation• Depression• Dyspnea• Constipation
• Delirium• Sedation• Fatigue• Anorexia• Terminal secretions
10Paolini Symptoms Management at the End of Life JAOA Vol 101 No 10 Oct 2001

LD: 41‐yr‐old female• Ovarian cancer with metastases to colon, celiac plexus and lymph nodes
• Admitted to the palliative care team for management of pain + vomiting
• Current medications– Oxycodone 160mg po BID– Ondansetron 8mg q8h– Senna S 4 tablets BID
11

NociceptivePain
Somatic Visceral
NeuropathicPain
Peripherally Generated
Centrally Generated
Functional
Types of Pain
Nociceptive Pain •Normal processing of stimuli• Usually responds to non‐opioid and/or opioid analgesics
Neuropathic Pain •Abnormal processing of sensory input • Treatment usually includes adjuvants
12

Class and Generic Name (Brand Name)
Phenanthrenes
Morphine (various)
Codeine (various)
Hydrocodone (combination)
Hydromorphone (Dilaudid, various)
Oxycodone (various)
Oxymorphone (Numorphan, Opana)
Phenylpiperidines
Meperidine (Demerol, various)
Fentanyl (Sublimaze, Duragesic, Actiq, Onsolis, Fentora, various)
Diphenylheptanes
Methadone (Dolophine, various)
Opioid Agonist
13

Opioids EquivalencyDrug IV Dose PO Dose
Codeine 120 mg 200 mg
Fentanyl 100 mcg
Hydrocodone 30 mg
Hydromorphone 1.5 mg 7.5 mg
Methadone** Consult Specialist
Morphine 10 mg 30 mg
Oxycodone 20-30 mg
** Also works on NMDA receptor 14

Choosing an Opioid in Organ FailurePreferred Consider Avoid
Hepatic Failure
HydromorphoneMorphine
Methadone
OxycodoneFentanyl
CodeineHydrocodone
Tramadol
Renal Failure
FentanylMethadoneOxycodone
HydromorphoneHydrocodone
MorphineCodeineTramadol
Hepato-renal
Syndrome
HydromorphoneMethadone
FentanylOxycodone
MorphineCodeineTramadol
Hydrocodone
15

Common Opioid Adverse Effects• Constipation
– senna +/‐ docusate, bisacodyl, methylnaltrexone
• Nausea / vomiting–↓ dose– prochlorperazine, haloperidol, metoclopramide
• Dry mouth–↓ dose– Sugar‐free sour hard candy
• Sedation–↓ dose–methylphenidate
• Sweats–↓ dose
16

Less Common Opioid Adverse Effects
– Pruritus / urticaria (morphine is the worst)
• Rotate opioid
– Respiratory depression
• ↓ dose
– Bad dreams / hallucinations
• ↓ dose• Rotate opioid
– Dysphoria / delirium• Rotate opioid
– Myoclonus / seizures• Rotate opioid
17

Neuropathic Pain – Adjuvants
• Treatment Options–Tricyclic Antidepressants
• Nortriptyline, desipramine –Avoid Amitriptyline
–Antiepileptic Drugs• Gabapentin, pregabalin
18

LD: Colicky abdominal pain + shooting pain across her back• Rates pain at 20/10• Switched to hydromorphone (HM) 1mg/hr + 0.5mg q30min IV
• Dexamethasone 8mg IV BID• Ondansetron 8mg q8h changed to IV• Metoclopramide 10mg q6h IV
• What about using the subcutaneous route?
19
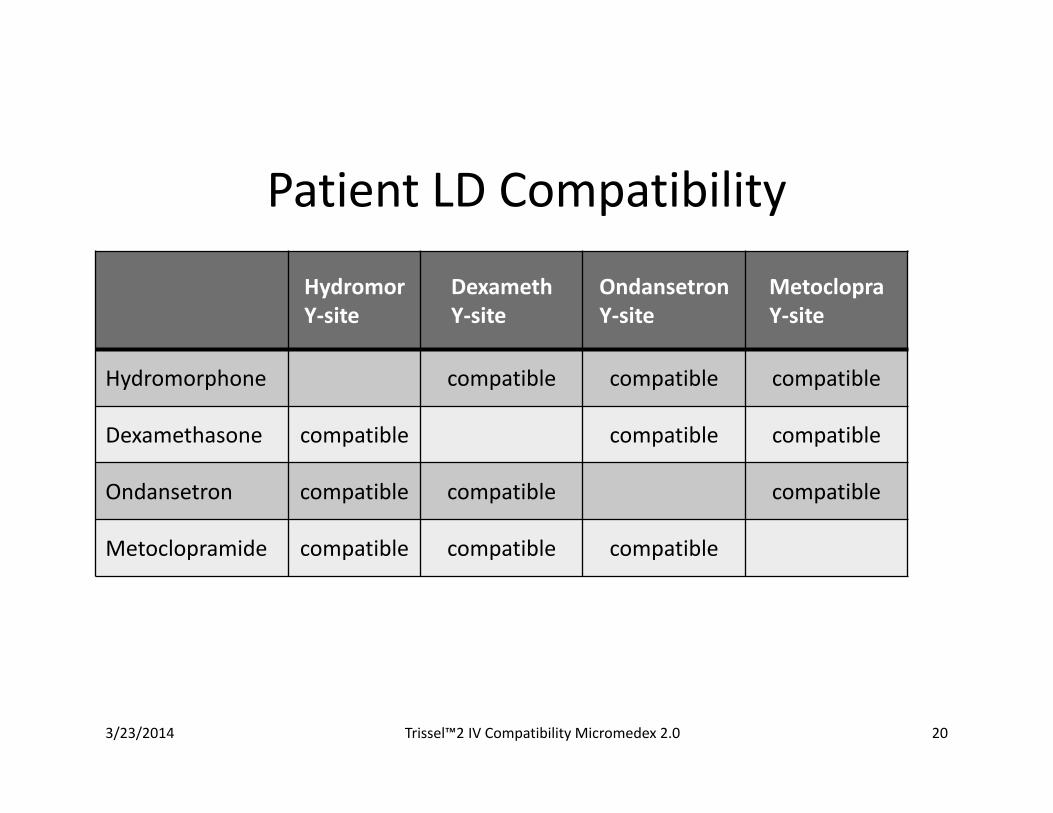
Patient LD Compatibility
HydromorY‐site
DexamethY‐site
OndansetronY‐site
MetoclopraY‐site
Hydromorphone compatible compatible compatible
Dexamethasone compatible compatible compatible
Ondansetron compatible compatible compatible
Metoclopramide compatible compatible compatible
3/23/2014 Trissel™2 IV Compatibility Micromedex 2.0 20

Routes of Administration
IV SubcutaneousInfusion
SubcutaneousInjection
Hydromorphone Yes Yes Yes
Dexamethasone Yes Yes Yes
Ondansetron Yes Yes Yes
Metoclopramide Yes Yes Yes
3/23/2014 Trissel™2 IV Compatibility Micromedex 2.0 21

Challenges of Multiple Drug Admin• For IV route, assuring there is adequate y‐site
compatibility information
• Issue of additional bolus dose if single lumen catheter, followed by potential delay in analgesia while catheter and extension refill
• For continuous subcutaneous, multiple infusion pumps and adequate infusion sites
• Consider soft‐set for patient comfort
• Consider multiple lead subcutaneous infusion sets for larger infusion volumes.
22

Soft Type Subcutaneous Sets
23

Multi‐lead subcutaneous set
24

Pumps

OpioidsDrug IV/SC Dose- Opioid
NaiveOnset (Min)
Peak(Min)
Duration(Hours)
Fentanyl(Sublimaze)
1-3 mcg/kg (25-75 mcg)May repeat in 2-3 min
1-4 3-5 0.5-1
Hydromorphone(Dilaudid)
0.01-0.02 mg/kg (0.5-2 mg)May repeat in 5-10 min
5-10 10-20 2-6
Morphine0.05-0.1 mg/kg (2-10mg)May repeat in 5-10 min
5-10 10-20 2-6
Methadone(Dolophone)
0.05-0.1 mg/kg (2.5-10mg) every 6 hours
2-4 hrs
4-6 hrs 20-30
McPherson, M.L. Demystifying Opioid Conversion Calculations: a guide for effective dosing. Bethesda MD: ASHP. 2009 26

LD: Pain Escalation • Within 4 days, hydromorphone increased to 16mg/hr + 8‐10 PRN doses (8mg q30 min prn ( ≈ 450mg IV/24 hr)
• Lethargic but still complains of excruciating pain
• Last bowel movement 5 days ago• Vomit has fecal odor• Pain service recommends epidural pain management
27
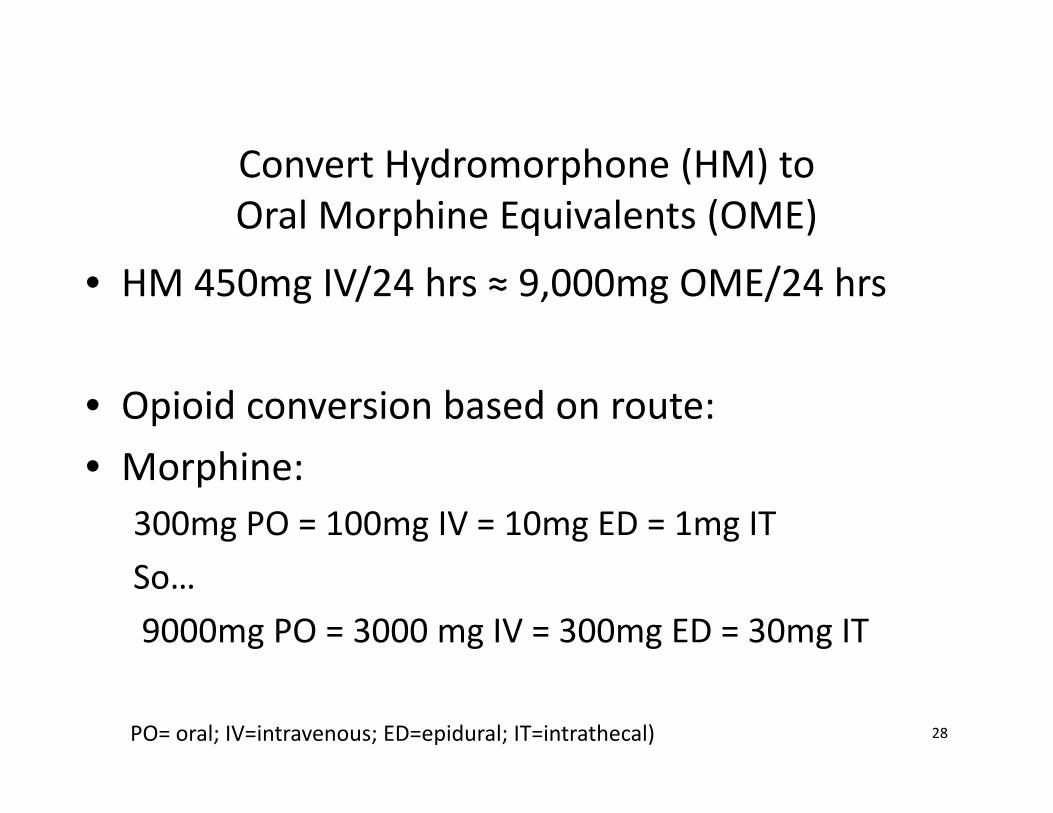
Convert Hydromorphone (HM) to Oral Morphine Equivalents (OME)
• HM 450mg IV/24 hrs ≈ 9,000mg OME/24 hrs
• Opioid conversion based on route:• Morphine:
300mg PO = 100mg IV = 10mg ED = 1mg ITSo…9000mg PO = 3000 mg IV = 300mg ED = 30mg IT
28PO= oral; IV=intravenous; ED=epidural; IT=intrathecal)

29
Opioid Choice for Epidural/ Intrathecal
Lipophilic
Hydrophilic
SufentanilBuprenorphineFentanylMethadoneHydromorphoneHydrocodoneOxycodoneMorphineCodeine
http://updates.pain‐topics.org/2012/02/new‐views‐on‐opioid‐equivalency.html

Epidural Adjuvants• Local anesthetics
–Lidocaine (4mg/ml IV, ED)
–Bupivacaine (0.25‐0.75% ED)
–Ropivacaine (0.2‐0.5% 5‐100ml/hr ED)
• Alpha2‐Adrenergic Agonist
–Clonidine (30‐40 mcg/hour ED)30Lexi‐Comp OnlineTM , Lexi‐Drugs OnlineTM , Hudson, Ohio: Lexi‐Comp, Inc.; 1/27/2014

Intrathecal Adjuvants• Calcium Channel Blocker N Type
– Ziconotide• Titrate by≤2.4 mcg/day (0.1 mcg/hour) at intervals ≤2‐3 times/week to a maximum dose of 19.2 mcg/day (0.8 mcg/hour) by day 21
• Average dose at day 21: 6.9 mcg/day (0.29 mcg/hour) IT.
31Lexi‐Comp OnlineTM , Lexi‐Drugs OnlineTM , Hudson, Ohio: Lexi‐Comp, Inc.; 1/27/2014

Epidural Compatibility and Stability
• Combination of morphine 50mg/mL, bupivacaine 24mg/ml and clonidine 2mg/mL in NS – little to no loss of drug over 90‐day study period
• Combination of fentanyl 35 mcg/mL, bupivacaine 1mg/mL and clonidine 9 mcg/mL – 28 day refrigerated, followed by 24 days room temperature
32Trissel™2 IV Compatibility Micromedex 2.0
Epidural Compatibility and Stability
• Combination of hydromorphone, or fentanyl or morphine and bupivacaine stable at multiple concentrations for extended periods of time.
33Trissel™2 IV Compatibility Micromedex 2.0

Epidural Administration Guidelines• Agreement with prescriber of what to do if temporary epidural catheter dislodges after hours
• Have naloxone available in the home, our protocol is if RR<8/min or patient is obtunded then administer 0.1mg(0.25ml) and contact prescriber
• Label infusion device with “Epidural Infusion” to avoid possible confusion if patient presents to ER unannounced
34

Opioid‐Induced Neurotoxicity• Signs:
– Rapidly escalating dose requirement
– Hyperalgesia/allodynia
– Pain “doesn’t make sense;” not consistent with recent pattern or known disease
– Myoclonus – twitching of large muscle groups
– Delirium
– Hallucinations/Seizures
35Pasero, C, and M McCaffery. "Opioid‐induced Hyperalgesia." Journal of Perianesthesia Nursing 27.1 (2012): 46‐50

Probability of opioid induced neurotoxicity by drug:Morphine > Hydromorphone >Oxycodone>Fentanyl >Methadone
Treatment:• Rotate to structurally dissimilar drug
– Methadone → Fentanyl → Oxycodone
• Hydration• Benzodiazepines for myoclonus
36
Treatment of Neurotoxicity

Methadone Pharmacology
Opioids NMDA Monoamines
•μ ‐ agonist•δ – agonist
•Blocking NMDA receptor prevents:
•Central sensitization•Cross tolerance•Hyperalgesia•Wind‐up•Opioid tolerance
•Inhibits reuptake of•5‐HT•NE
•Like TCAs
• Most effective opioid for neuropathic pain
Chhabra, S Bull J.Methadone American Journal of Hospice and Palliative Medicine, Volume 25, issue 2 (April 2008): 146‐150 37
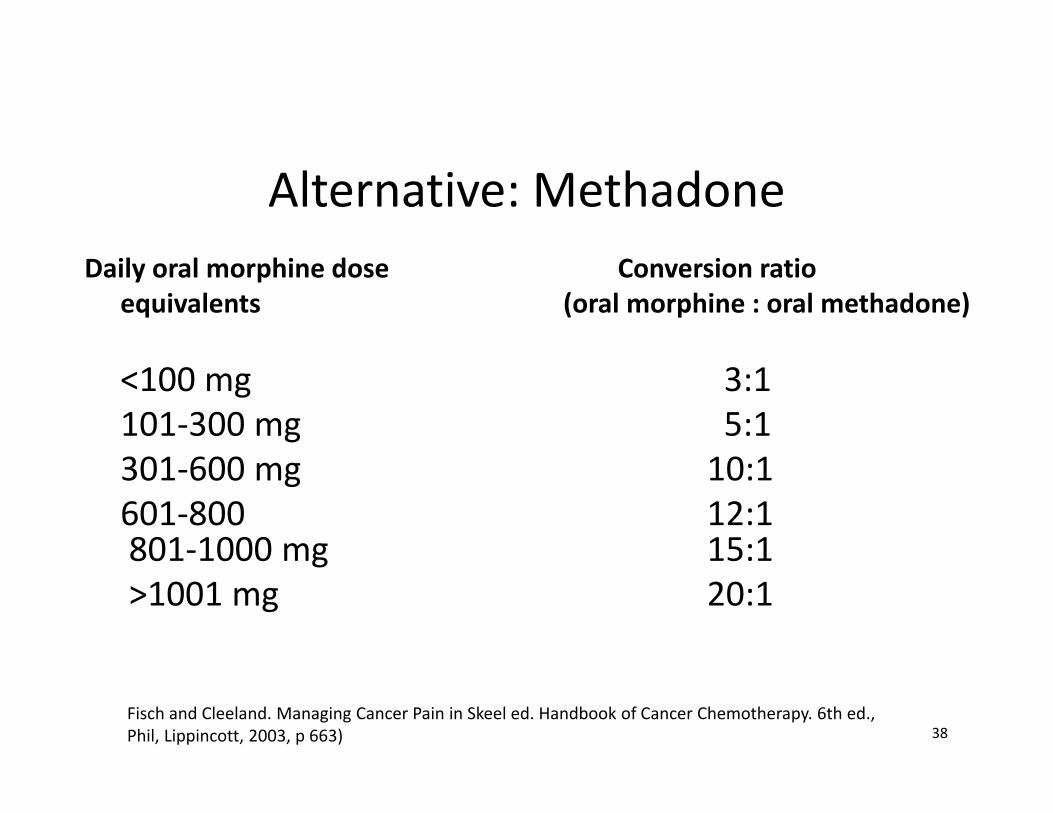
Alternative: MethadoneDaily oral morphine dose Conversion ratio
equivalents (oral morphine : oral methadone)
<100 mg 3:1 101‐300 mg 5:1301‐600 mg 10:1601‐800 12:1801‐1000 mg 15:1>1001 mg 20:1
38Fisch and Cleeland. Managing Cancer Pain in Skeel ed. Handbook of Cancer Chemotherapy. 6th ed., Phil, Lippincott, 2003, p 663)

• Dissociative anesthetic, NMDA antagonist• Refractory pain, neuropathic pain, hyperalgesia, allodynia– Resets central sensitization
• IV, PO, PR, SC, intranasal, transdermal• Dosing: varies per study
– Oral/SL : 5‐25mg po/sl q6‐8h– IV infusion: 0.05‐0.1mg/kg/hr
• Side Effects: nausea, sedation and hallucinations, dysphoria
Ketamine
Ketamine Use in Palliative Care Fast Facts #132 http://www.eperc.mcw.edu/EPERC/FastFactsIndex/ff_132.htm 39

Bowel Obstruction• Blockage of the bowel which causes a delay in the flow of intestinal contents
• Causes– Constipation/impaction, tumor mass, adhesions, severe ascites
• Symptoms– Nausea/vomiting, abdominal pain, colic/cramping
– Constipation, diarrhea, bloating, early satiety, anorexia
40

Bowel ObstructionPartial obstruction:• Metoclopramide
– Improve gastric motility• Haloperidol
– Decrease nausea sensation• Steroids
– Inflammatory response• Laxatives
– Prevent constipation– Vaseline® balls to facilitate disimpaction
41Alder, 2005; Jatoi et al, 2004

Bowel ObstructionFull obstruction:• Anticholinergics
– Slow hypermotility, dry secretions– Hyoscyamine (Levsin, Hyo‐max), Glycopyrrolate (Robinul)
• Octreotide (Sandostatin)– Inhibit secretion of numerous hormones & neurotransmitters which affect gastric function, decrease peristalsis
– 50‐100mg SQ q8h
42Alder, 2005; Jatoi et al, 2004; Ripamonti et al, 2004

Hypodermoclysis: Subcutaneous Fluid Administration• Indications
– Mild to moderate dehydration in adults
• Geriatric patients• Palliative Care
– Intravenous access difficult or impractical
– Patient unable to take PO • Nausea or vomiting• Intestinal obstruction• CVA
• Contraindications• Not indicated in pediatric patients
• Clotting disorder• Pulmonary edema• Large volume fluids required
– Severe dehydration or shock
– Severe electrolyte disturbance
43Am Fam Physician. 2001 Nov 1;64(9):1575‐1579

Hypodermoclysis & HyaluronidaseEnhances subcutaneous fluid absorption
• Lyses interstitial barrier for 24 to 48 hours
• Not necessary to prevent edema
• May cause discomfort and local reaction
• Dose– Hyaluronidase 150 Units per Liter fluid
– Inject 75 Units at each clysis site
• Ambulatory patients
– Abdomen– Upper chest (above the Breast)
– Over intercostal space– Scapula area
• Bed‐bound patients– Thighs– Abdomen– Outer upper arm
44

Hypodermocylsis Administration• Catheter site change q 72 hrs• Max volume 1.5L/site/24 hours• Limit of volume 75 ml/hr• Often takes ~20ml/hr to keep site patent• Use isotonic solution or electrolyte containing
hypotonic solution to prevent cardiovascular collapse• Hypertonic or electrolyte free solution has been
reported to cause CV collapse
45ASHP Palliative Pharmacy Care, Strickland 2009

Hyaluronidase
• Difficult to administer at home• Limited stability information, 24 hours in solution
• Most of our past patients have utilized multi‐site subcutaneous sets as discussed previously to help with administration of IV fluids
46

Delirium in Terminal Patients
Can be hyper‐ or hypoactive or mixed Cancer Patients 87% during course of disease
Reversible 49% of palliative care patients
Terminal Delirium 88% of dying patients
47LeGrand, SB. "Delirium in Palliative Medicine: a Review." Journal of Pain and Symptom Management. 44.4 (2012): 583‐94

Potentially Reversible Causes of Delirium Urinary retention Constipation Hypoxemia Infection Metabolic abnormalities ↑ or ↓ sodium ↑ calcium Altered blood glucose
Dehydration Drug side effects
Fatigue, sleep deprivation, altered circadian rhythms
Severe anemia Nutritional deficiencies Thiamine, folate, B12
Drug and alcohol withdrawal
Pain (especially uncontrolled)
48

Treatment of Delirium If appropriate, treat reversible causes
Reduce, eliminate or change drugs that may be contributing to delirium
Use antipsychotic drugs to treat confusion
Add benzodiazepines only if needed for anxiety and/or restlessness
49

Treatment of Delirium Pharmacologic interventions Neuroleptics*
• Haloperidol, clorpromazine• Quetiapine, olanzepine, risperidone chlorpromazine
Avoid using benzodiazepines unless in combination with neuroleptic Paradoxical worsening of delirium and anxiety
* Unlabeled use 50

Cardiac Failure• CT: 59 yr‐old‐male with hyperlipidemia HF, HTN• Optimized on all cardiac medications• Multiple hospitalizations• Has been in an outpatient heart failure clinic receiving intermittent dobutamine
• Now on continuous infusion dobutamine • Referred to hospice for heart disease• Desires to remain on dobutamine to make closure
51
Dobutmaine Administration• Dobutamine 1 and 4 mg/mL in D5W 9‐day medium risk refrigerated stability
• Suggest back‐up pump in the home in case primary pump fails
• Always ensure that available supply of medication includes not less than 2 containers of medication to prevent possible interruption of therapy
• Alternatively milrinone is used for this indication: 400, 600, 800 mcg/mL in D5W 9‐day medium‐risk refrigerated stability
52Bing, Extended Stability for Parenteral Drugs 5th ed.

Other Consideration in HF end of life• If patient had ICD (Implantable Cardioverter Defibrillator)– Make sure palliative care team knows so can discuss with cardiologist plan for deactivation
– If no plan for deactivation, make sure nursing staff has magnet available to disable cardioverter function to prevent unwanted shocks at end of life
– Magnet will not deactivate pacing in case of bradycardia, but will deactivate shocks in case of ventricular tachyarrhythmia
53Implantable Cardioverter Defibrillator at end of life, Medical College of Wisconsin Fast Facts#112, Harrington, MD et.al.
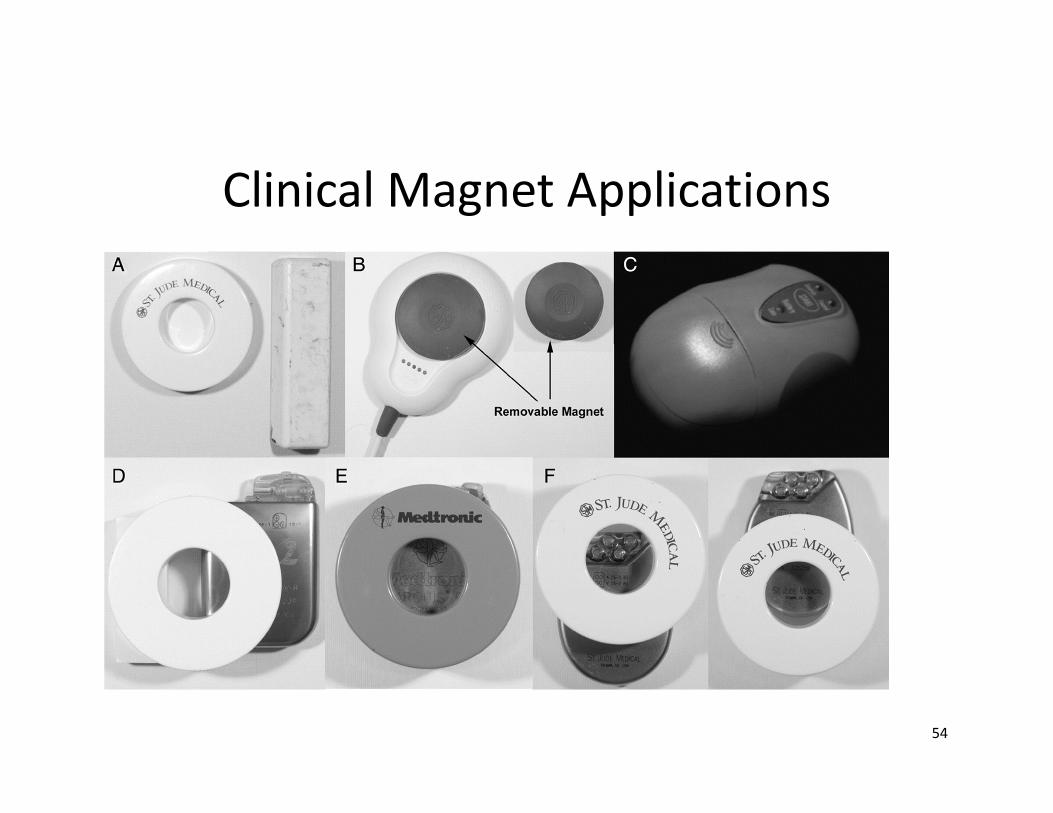
Clinical Magnet Applications
54

Pulmonary Hypertension• RS: 68‐yr‐old male with COPD, pulmonary fibrosis, pulmonary hypertension
• In ICU for progression of pulmonary hypertension
• On continuous infusion of epoprostenol • Receiving palliative care • Patient wants to go home with hospice
55
Pulmonary Hypertension• Prostaglandins:
– Very short‐acting given IV or inhaled very frequent or continuously• epoprostenol (Flolan), treprostinil (Remodulin, Tyvaso), iloprost (Ventavis)
• Phosphodiesterase type 5 inhibitors:– somewhat less effective than the prostaglandins – PO one to three times per day
• sildenafil (Revatio, Viagra), tadalafil (Adcirca, Cialis)
• Endothelium antagonists: – PO one to two times per day.
• bosentan (Tracleer) , ambrisentan (Letairis)
56Lexi‐Comp OnlineTM , Lexi‐Drugs OnlineTM , Hudson, Ohio: Lexi‐Comp, Inc.; 1/27/2014

DyspneaManagement of breathlessness (based on patient report) Opioids*
Low‐dose, immediate release Morphine 5‐ 20 mg PO/SL or 2‐5 IV/SC q 1h prn Hydromorphone 0.5mg IV/SC q1h prn Oxycodone 5‐20 mg PO/SL q 1h prn
To break dyspnea/ anxiety cycle Add anxiolytics
Low‐dose ATC + breakthrough Lorazepam 0.5‐2 mg po/sl/IV/sc q4‐8h
Non‐pharmacologic interventions Oxygen‐ only if hypoxic or palliative (per patient)
* Unlabeled use
57Kamal, Arif H, et al. "Dyspnea Review For The Palliative Care Professional: Treatment Goals And Therapeutic Options." Journal Of Palliative Medicine 15.1 (2012): 106‐114. MEDLINE with Full Text. Web. 31 Jan. 2014

Drug IV Dose Onset (Min)
Peak(Min)
Duration(Hours)
Lorazepam0.02-0.05 mg/kg slow IVP0.5-2 mgMay repeat 5-10 mins
2-10 15-60 6-8 hours
Midazolam0.05 mg/kg slow IVP0.5-5 mgMay repeat 3-5 mins
1-5 5-10 2-6 hoursActive metabolites
Diazepam0.1 mg/kg slow IVP (2-5 mins)2-10 mg May repeat 5-10 mins
1-5 15-30 VariableActive metabolites
1 mg lorazepam = 2-2.5 mg midazolam
Anxiety: Benzodiazepines
Lexi‐Comp OnlineTM , Lexi‐Drugs OnlineTM , Hudson, Ohio: Lexi‐Comp, Inc.; 1/27/2014 58

Epoprostenol Administration• Short stability requires patient and or caregiver with a back up able to mix at any time
• Always carry an extra dose and related supplies in case of emergency
• Back up pump required as infusion can not be interrupted
• Limited distribution products as they require special intensive follow up in the home setting to prevent problems associated with administration
59

Benzodiazepines Administration• Lorazepam: polyolefin or glass only!
– 0.1mg/mL in D5W or NS 7 days refrigerated– 1mg/mL in NS 9 day medium risk refrigerated stability
• Midazolam: PVC or polyolefin, more stable– 0.5 mg/mL in D5W or NS 9 day medium risk ref– 1mg/mL in NS 9 day medium risk ref
• Diazepam: not recommended for extended infusions due to variable stability in solution
60Bing, Extended Stability for Parenteral Drugs 5th ed.

Ethics of Pain/Symptom Management
INTENTSymptom management
VERSUS
Palliative sedationVERSUS
Euthanasia
61

Ethics: Potential Barriers
• Legal misconceptions and/or legal concerns about escalation of opioids and other palliative medications are very common
• Intent of therapy is relief of symptoms • Communication with family (and other health care providers) must stress this goal
Chest 2009;135:1360-962

Palliative/Respite Sedation RARELY needed
• Criteria: terminal care when symptoms are refractory to all available treatments
• Often requires an ethics consult• Medications:
– Midazolam or Lorazepam– Chlorpromazine– Phenobarbital
63

Benzodiazepine Administration
• Lorazepam: Limited stability in glass or PAB containers???
• Midazolam better stability information, wider range of concentrations for dose titration
64
