1 observations from the antiviral information management system (aims) database jeffry florian,...
TRANSCRIPT

1
Observations from the Antiviral Information Management System
(AIMS) Database
Jeffry Florian, Ph.D.
CDER/OTS/OCP
Division of Pharmacometrics, Reviewer
The opinions and information in this presentation are those of the author, and do not represent the views and/or policies of the U.S. Food and Drug Administration.

2
Outline
• Overview of the Antiviral Information Management System (AIMS)
• Observations and analyses from AIMS– EOP2– NDA– Trial design
• Future project considerations with the database

3
A system to archive data and assist analysis for new anti-HCV agents is needed to inform dose selection.
Project started in 2008 – Critical Path Initiative Dr. Gobburu and Dr. Jadhav
With more than forty new anti-HCV drugs in the pipeline, we must keep pace with development.
BOTTLENECK: Lack of available database & data
standards
40+ HCV drugs in
development
Systematic archival of data and analysis will help leverage prior knowledge in this emerging therapeutic area.
Modeling and simulation can help inform dosing and trial design issues for efficient development.

4
AnalysisData
AIMS Database Standards
AIMS database relies on : (1) Database standards, (2) Data requests (3) Internal analysis codes, and (4) Shared experience
Mean viral load :
1a
1b
log 1
0 H
CV
RN
A
time (weeks)
Modeling codes and analyses
Fra
ctio
n ac
hiev
ing
SV
RTime (weeks)
0 12 24 48
1.0
0.5
0
Modeling codes and analyses

5
Implementation of the relational database structure, data templates and controlled terms requires forward thinking and planning.
DRUG
DM
EX
PC
LB
VS
CM
MB
EP
STUDY
Analysis data specific for HCV
Raw data in abbreviated CDISC format
AIMS DatabaseRelationship Diagram:
Relational structure supports efficient queries
DRUG
STUDY DM
CM EX
PC
MB
VS
LBEP
Sponsors will receive a data template and a list of controlled terms to guide data submission.
Templates: definitions and examples for all data fields.
Controlled Terms: specific listing of acceptable inputs for each data field to ensure identical formatting for all sponsors.
demographics
endpoints lab measures
vital signs
concomitant meds exposure
pharmacokinetics
virology
6
The available information depends on the active and willing collaboration of sponsors developing HCV drugs
Original information request was issued in July 2010 to all companies with an active HCV IND
Voluntary data submission of completed trials according to the provided data standard.
Request data at the time of End-of-Phase 2, End-of-Phase 2A, or other key early development meetings
New data request issued whenever a sponsor submits a new IND

7
Every day is like drinking from a fire hose
http://www.phdcomics.com/comics/archive.php?comicid=820

8
The AIMS database contains demographic, PK, virologic, and treatment data from previous, recent, and ongoing trials.
Legacy data were converted using internal resources to include in the database.
Recent Phase III trials were submitted according to AIMS standard.
Many EOP2 meetings have accompanying AIMS datasets Multiple treatment regimens (PR, PR+DAA) and
durations were included in the dataset.
9 drug developmentprograms
29 studies 10K+ subjects

9
The AIMS database assists reviewers in analyses across all HCV submissions
Use archived HCV data to generate research hypotheses across multiple studies and drugs.
Archive data from sponsors without additional formatting.
Generate analysis datasets, plots and reports using automated scripts.
Archive analysis results (data, models, plots, reports).
Access historic data to inform decisions about new submissions.
10
Outline
• Overview of the Antiviral Information Management System (AIMS)
• Observations and analyses from AIMS– EOP2– NDA– Trial design
• Future project considerations with the database
11
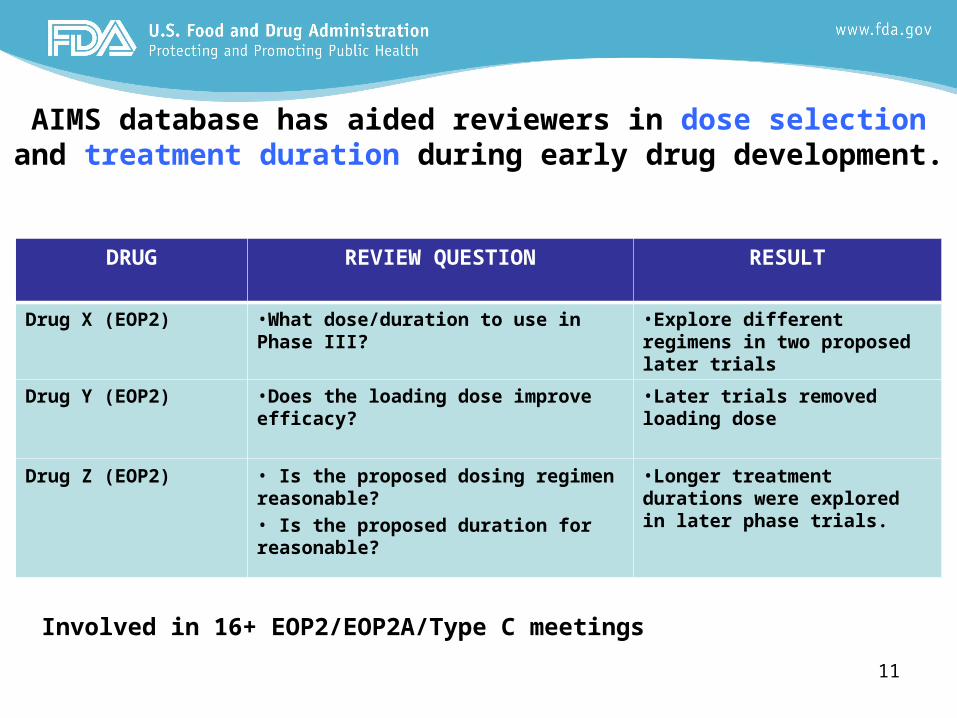
AIMS database has aided reviewers in dose selection and treatment duration during early drug development.
DRUG REVIEW QUESTION RESULT
Drug X (EOP2) •What dose/duration to use in Phase III? •Explore different regimens in two proposed later trials
Drug Y (EOP2) •Does the loading dose improve efficacy?
•Later trials removed loading dose
Drug Z (EOP2) • Is the proposed dosing regimen reasonable?• Is the proposed duration for reasonable?
•Longer treatment durations were explored in later phase trials.
Involved in 16+ EOP2/EOP2A/Type C meetings

12
Sponsors are submitting materials to support and justify doses, treatment durations, and patient population
A majority of EOP2 submission packages are accompanied by modeling and simulation results Supportive analyses for regimen(s) selected for registrational trials Viral kinetic modeling including resistance and viral subtypes Predictions of SVR using studied and/or exploratory regimens Exposure-response safety analyses for key signals identified in Phase II
AIMS datasets have been provided for ~50% of early phase meetings Data conversion and standardization is time consuming
not commonly performed until later in drug development
Sponsors provide datasets for modeling and simulation whenever available

13
General observations over multiple EOP2 submissions
As regimens are becoming better (↑SVR, ↓treatment duration), the need for earlier assessments increases
Intrinsic patient factors remain important for treatment outcome (e.g., IL28B, cirrhosis, baseline HCV RNA)
Genotype subtype is becoming more important (ref: Dr. Harrington)
P/R-regimens: time to HCV RNA not detected remains predictive of response The impact of shortening treatment duration may require even
earlier metrics (eRVR or even ‘Week 1’VR)
IFN-free regimens: antiviral activity ≠ SVR Predictive factors based on viral kinetics remain to be identified Much easier to identify when something is not optimal

14
Outline
• Overview of the Antiviral Information Management System (AIMS)
• Observations and analyses from AIMS– EOP2– NDA– Trial design
• Future project considerations with the database

15
Two new HCV therapies characterized by drastically different drug development programs
REGISTRATIONAL TRIAL DESIGNS
BOCEPREVIR TELAPREVIR
Lead-in Phase YES NO
Response Guided Therapy
All trials Only treatment-naïve patients
Treatment-experienced trial
Excludes null responders
Include relapsers, partial responders, and null
responders

16
“Bridging” Observations Through Interferon Responsiveness
• Similar response with first or second round of P/R treatment– Data for previously treated subjects are “bridged”
with data from untreated subjects
• Previously treated subjects are represented within untreated subjects
• P/R treatment for HCV is unlike HIV treatment which frequently leads to resistance and does not yield similar virologic response on subsequent courses of treatment

17
Similar Virologic Response at Week 4 with First or Second PR treatment (pooled analysis)
untreated
untreated
untreated
untreated
previously P/R treated
previously P/R treated
previously P/R treated
untreated
untreated
untreated
untreated
previously P/R treated
previously P/R treated
previously P/R treated
1416
597
507
548
468
219
112
Liu et al. CID 2012

18
Standardized datasets facilitated similar analyses and led to novel dosing recommendations.
EXAMPLE REVIEW QUESTIONS RESULT
Telaprevir •Pivotal trials did not evaluate shorter treatment durations in relapse patients
• Additional study deemed unnecessary.•Shorter treatment duration included in label for prior relapsers
Boceprevir •Prior null responders not included in Phase III•Different regimens for treatment-naïve (TN) and treatment-experienced (TE) trials
•Evidence of effectiveness for prior null responders•Dosing recommendations for TN late responders
A successful trial in TE subjects can serve as evidence of effectiveness to support dosing and approval in TN subjects.

19
Outline
• Overview of the Antiviral Information Management System (AIMS)
• Observations and analyses from AIMS– EOP2– NDA– Trial design
• Future project considerations with the database

20
SVR24 was the surrogate endpoint used in original Peg-IFN/RBV and recent DAA+Peg-IFN/RBV trials
TREATMENT
Follow-up Wk 24
8 240
TREATMENT
16 4032 48 60 72 WEEK
Follow-up Wk 24
Endpoint is assessed 24 weeks after the end of treatment
Follow-up duration may be as long as treatment
60-70%
30-40%
SVR12 (HCV not detected at 12 weeks post treatment) is evidence of effectiveness in Phase II Can a similar assessment be used in Phase III?

2121
Concordance was observed between SVR12 and SVR24 for all Peg-IFN/RBV and DAA+Peg-IFN/RBV treatments
SVR 24 Assessment
‘Y’ ‘N’
SVR12 Assessment
‘Y’ 5428 93
‘N’ 56 4617Sensitivity:
99%Specificity:
98.0%
PPV: 98%
NPV: 99%
SVR 24 Assessment
‘Y’ ‘N’
SVR4Assessment
‘Y’ 4239 412
‘N’ 53 3002
PPV:91.1%
NPV:98.2%
Sensitivity:98.7%
Specificity:87.7%
• ~2% of patients with SVR12 relapse by SVR24 assessment (false positive)
• Less agreement between SVR4 and SVR24
• SVR4 may be useful for guiding dose selection

22
Sensitivity analyses support that SVR12 and SVR24 are concordant for Peg-IFN/RBV containing regimens
Overall 2%
SVR 24 Assessment PPI
SVR 12 ‘Y’ (P/R Arms - all) 98.1%
SVR 12 ‘Y’ (DAA Arms) 98.8%
RGT (DAA Arms) 98.9%
No RGT (DAA Arms) 98.8%
• No matter how the analysis was performed 1-3% of patients relapse between SVR12 and SVR24

23
The analysis of SVR12/SVR24 for genotype 1 subjects motivated similar analyses for other populations and different regimens
Pediatrics Genotype 2/3
Subsequent application of the same analysis demonstrated concordance for
IFN-free regimens: Additional data is required Provide all available SVR12 and SVR24 data from drug
development program and discuss (all regimens)

24
Outline
• Overview of the Antiviral Information Management System (AIMS)
• Observations and analyses from AIMS– EOP2– NDA– Trial design
• Future project considerations with the database

eDISH (Evaluation of Drug-Induced Serious Hepatotoxicity) – FDA reviewer tool
• eDISH is a tool developed to assist reviewers in analyzing/explaining DILI in an IND/NDA
http://www.fda.gov/downloads/Drugs/ScienceResearch/ResearchAreas/ucm076777.pdf
• Compatible with AIMS datasets submitted by sponsors

26
eDISH (Evaluation of Drug-Induced Serious Hepatotoxicity) – FDA reviewer tool (cont.)
• eDISH includes time plots of key laboratory values
http://www.fda.gov/downloads/Drugs/ScienceResearch/ResearchAreas/ucm076777.pdf
• Data is linked to individual patient narratives• May assist in the safety analyses for IFN-free regimens

27
Conclusions• Sponsors are submitting datasets for AIMS
• These datasets are assisting in the review of submissions at EOP2 meetings
• Information from these submissions has provided insight regarding subsequent HCV trial design
• Future projects will continue to be evaluated as additional data becomes available

28
Acknowledgements• Critical Path Initiative and ORISE
– Lauren Neal– Jianmeng Chen
• OCP (Division of Clinical Pharmacology IV)
– John Lazor– Kellie Reynolds– Sarah Robertson– Vikram Arya– Stanley Au– Ruben Ayala– Shirley Seo– Jenny Zheng
• OCP (Division of Pharmacometrics)– Joga Gobburu– Pravin Jadhav– Yaning Wang– Ying Chen
• Division of Antiviral Products– Debra Birnkrant– Jeff Murray– Many supportive medical reviewers
and project managers• DAVP Clinical Virology Team
– Patrick Harrington– Jules O’Rear– Lisa Naeger
• NCTR– Steve Hodge – Edward Bearden
• OTS– Chuck Cooper
• Office of Biometrics– Ted Guo
• Many subjects, investigators, and sponsors who have provided data
29
Questions