1 gena c. peyton and jeremy harris, sutter health office of the general counsel and kat todd,...
TRANSCRIPT
1
Gena C. Peyton and Jeremy Harris, Sutter Health Office of the General Counsel
and
Kat Todd, Schuering Zimmerman & Doyle, LLP
Lengthy Difficult Patient Discharges From the Acute
Care SettingIssues, Pitfalls and Strategies

Overview
• The complex setting
• Pitfalls and strategies for common issues
2
Capacity
ResourcesBehaviors
3
The Complex Setting
Nature of services
Expectations
Laws and
Regs

4
Common Issues

5
Capacity

Patient Lacks Medical Decision-Making Capacity
6
Required for decision making – either to accept or reject medical care
Physicians assess capacity•Best case – advance directive or
verbal appointment•Worst case – court, county
involvement
Transfer/discharge require consent in most cases as part of discharge planning process
Conservatorships
7
• Prob. Code: Typically used for individuals suffering from dementia or other “organic” disorder affecting capacity
Probate
• LPS Act (Welfare & Institutions Code § 5350):
• Typically used for individuals gravely disabled as a result of mental disorder or impairment by chronic alcoholism
LPS

8
Patient Lacks Medical Decision-Making Capacity
Secure perimeter required /
Involuntary placement
and no conservator
Yes
Psychiatric Condition – not
Organic
Public Guardian – LPS
Conservatorship
Organic (dementia, anoxic brain injury,
etc)
Public Guardian – Probate
Conservatorship
Developmental disability (existed prior to age 18)
Regional Office – Lanterman
Developmental Disability Services
NoAuthorized Surrogate
decision-maker or next of kin involved?
Yes
Work with appropriate decision-maker(s) for discharge placement
and needs
NoPublic Guardian –
Probate Conservatorship

When the Individual Appointed Conservator Won’t Act
9
•Prob. Code § 2102: Conservators are subject to the regulation and control of the court in the performance of the duties of the office.
•Prob. Code § 2359(a): Upon petition of the guardian or conservator or ward or conservatee or other interested person, the court may authorize and instruct the guardian or conservator or approve and confirm the acts of the guardian or conservator.

When the Public Guardian Won’t Apply For Conservatorship
10
Limited ability to compel a county conservator to conserve an individual.
Prob. Code § 2920: The public guardian shall apply for appointment if:
• there is an imminent threat to the person’s health or safety or the person’s estate or
• the court so orders.

When the Public Guardian Won’t Apply for Conservatorship
11
Prob. Code § 2920, cont:
The court may make an order on behalf of any county resident who appears to require a guardian or conservator, if it appears that there is no one else who is qualified and willing to act, and if that appointment appears to be in the best interests of the person.
• LPS Act: Kaplan v. Superior Court (1989) 216 Cal.App.3d 1354

When the Family or County Won’t Act
12
Consider Petition for Authorization of Medical Care Without Conservator:
• Prob. Code § 3200: Request court authorization for medical care, including a transfer to another facility, when patient lacks capacity and there is no surrogate

Acquired Traumatic Brain Injured Patients
13
“Acquired traumatic brain injury” is an injury that is sustained after birth from an external force to the brain or any of its parts, resulting in cognitive, psychological, neurological, or anatomical changes in brain functions.”
[Welf. & Inst. Code §4354(a)]

Acquired Traumatic Brain Injured Patients
14
Welfare and Institutions Code § 4353:
“The Legislature finds and declares all of the following:
a)There is a large population of persons who have suffered traumatic head injuries resulting in significant functional impairment.
b)Approximately 80% of these injuries have occurred as a direct result of motor vehicle accidents.
Acquired Traumatic Brain Injured Patients
15
c)There is a lack of awareness of the problems associated with head injury resulting in a significant lack of services for persons with head injuries…
d)Although there are currently a number of different programs attempting to meet the needs of the persons with head injuries, there is no clearly defined ultimate responsibility vested in any single state agency. Nothing in this section shall be construed to mandate services for persons with acquired traumatic injury through county and city programs.”
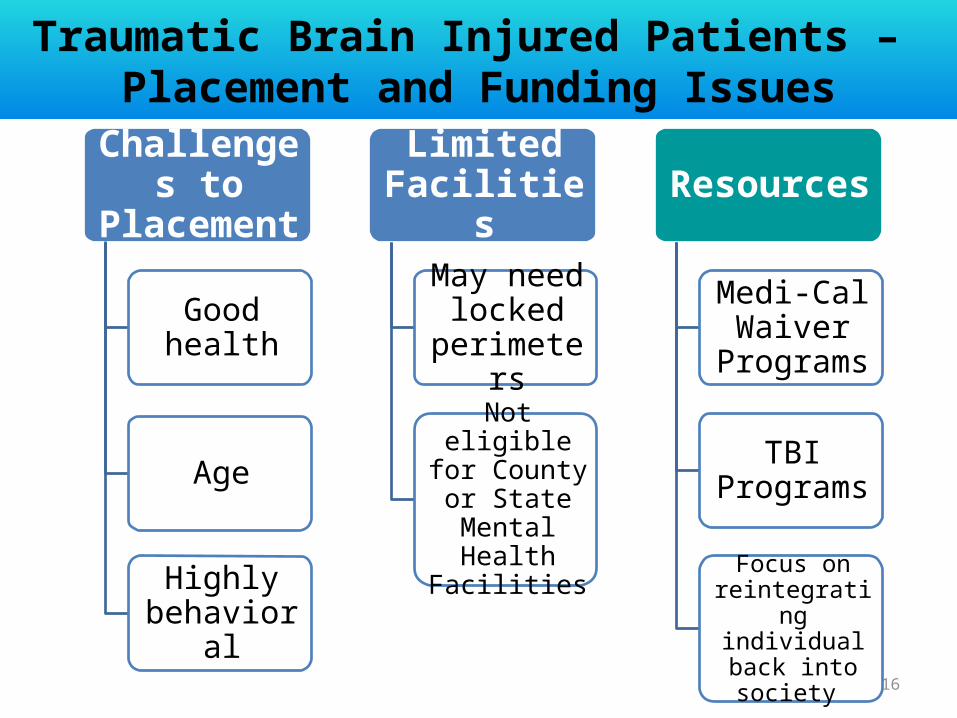
Traumatic Brain Injured Patients – Placement and Funding Issues
16
Challenges to Placement
Good health
Age
Highly behavioral
Limited Facilities
May need locked
perimeters
Not eligible for County or State Mental
Health Facilities
Resources
Medi-Cal Waiver
Programs
TBI Programs
Focus on reintegrating
individual back into society

17
Resources
18
Resources
Resource Issues
Homelessness
Medical Special Needs
Non-Medical Special Needs
When helping isn’t helpful…
19
“The SNF will take the patient if we agree to pay for the first three months at 150% of Medicare rate.”
(And, the SNF contracts with the hospital’s outpatient lab for its patients – 90% of which are Medicare/Medi-Cal patients.)

When helping isn’t helpful…
20
The federal anti-kickback statute makes it a criminal offense to knowingly and willfully offer, pay, solicit, or receive any remuneration to induce or reward referrals of items or services payable by a federal health care program.

When helping isn’t helpful…
21
“Remuneration” includes transfers of items or services for free or for other than fair market value.

When helping isn’t helpful…
22
“The Medicare patient says he will only go home if the hospital pays to install a wheelchair ramp and remodel his bathroom to make it easier for him to enter the shower.”
(The patient has the same conditions and abilities as he did before admission, has plenty of money and thinks it is the hospital’s responsibility “if they want [him] to leave”.)
When helping isn’t helpful…
23
Beneficiary inducement: Federal civil monetary penalties are assessed against any person who gives something of value to a Medicare or state healthcare program (including Medicaid) beneficiary that the benefactor knows or should know is likely to influence the beneficiary’s selection of a particular provider, practitioner, or supplier of any item or service for which payment may be made, in whole or in part, by Medicare or a state health care program including Medicaid.

When CAN We Help?
24
The Health Care and Education Reconciliation Act of 2010 amended the Patient Protection and Affordable Care Act’s definition of “remuneration” by adding a new exception for any other remuneration which promotes access to care and poses a low risk of harm to patient and Federal health care programs as designated under regulations.
When CAN We Help?
25
The OIG proposes updating the definition of “remuneration” in the inducement Civil Monetary Penalty regulations at 42 CFR §1003 by adding statutory exceptions for:
• certain remuneration that poses a low risk of harm and promotes access to care and
• certain remuneration to financially needy individuals.
But still…
26
The answer is hardly ever black and white

When CAN We Help?
27
SSA §1128A(A)(5) “Remuneration” Exception Criteria
1. The item or service is not advertised or solicited.
2. The item or service is not tied to the provision of other services reimbursed in whole or in part by Medicare or Medi-Cal.

When CAN We Help?
28
Criteria, cont.
3. There is a reasonable connection between the items or services and the medical care of the individual.
4. It is determined in good faith that the individual is in financial need.
29
Resources
Resource IssuesHomelessness
Communicate with available community resources; motel
Medical Special NeedsIdentify ResourcesAssist in paperwork
Facilitate outside sourcesUtilize checklist to avoid penalties
Non-Medical Special Needs

30
Behaviors
31
Behaviors
Patient
Family or surrogateStaff

Behavior Issues
Patient has capacity – refusing placement
Uninvolved or non-compliant surrogate decision-maker
32
Behaviors

33
Process Framework
1. Establish care team
2. Early identification and process trigger
3. Consistency
4. Documentation
34
Response Process

Establish Care Team
35
Response Process
• Attending MD • Physician Leadership as needed• Nursing• Social Work & Case Management• Risk• Security • Psych (as appropriate)• ED (as appropriate)• Outside social worker or case worker • CMO or Administration

Identification and Triggers
36
Response Process
• Potential/actual complex condition
• Change from home to care setting
• Disabling/life limiting condition
• Multiple specialty care needs
• High cost medications/outpatient needs
• History/repeat admissions
• Whole team needs on the same page to what care is rendered and the schedule of that care
• Behavioral issues discussed and unified approach developed when addressing or caring for the patient
• Directive care – patient must be informed of and consent to care, but team should address patient with treatment plan that maximize patient’s wellbeing and lessens opportunities for conflict
• Focus patient on recovery and desire to be as independent as possible
37
Response Process
Consistency
Documentation
38
Response Process
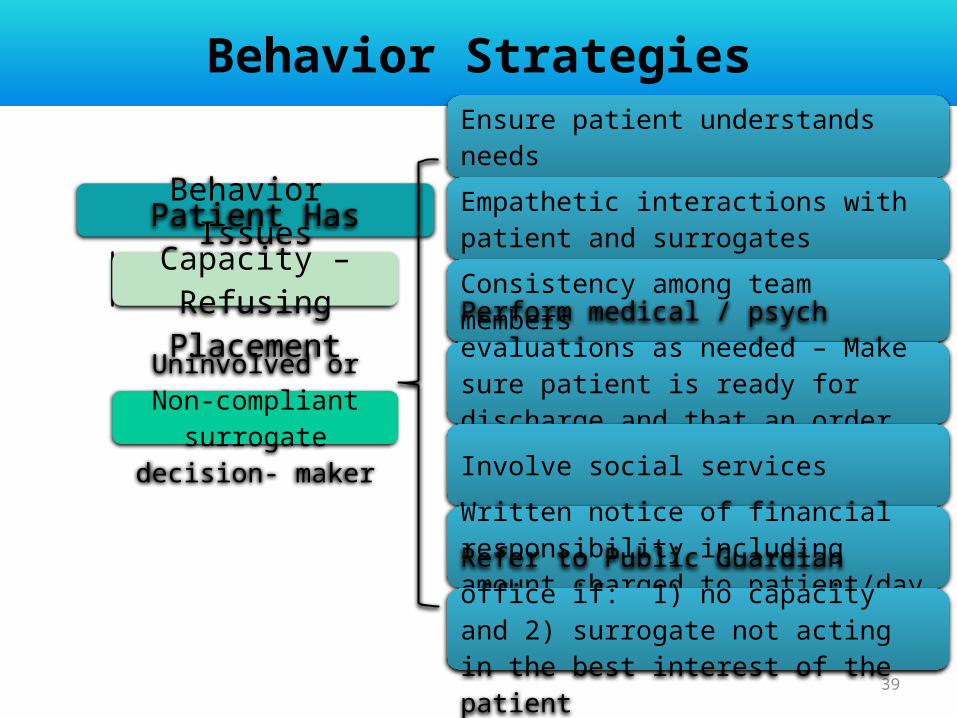
Behavior IssuesPatient Has
Capacity – Refusing
Placement
Uninvolved or Non-compliant surrogate
decision- maker
39
Behavior Strategies
Ensure patient understands needs
Empathetic interactions with patient and surrogates
Consistency among team members
Perform medical / psych evaluations as needed – Make sure patient is ready for discharge and that an order is written
Involve social services
Written notice of financial responsibility including amount charged to patient/day
Refer to Public Guardian office if: 1) no capacity and 2) surrogate not acting in the best interest of the patient
• Begin discharge planning/process at admission – or at least at earliest trigger
• Medicare certification for discharge (appeal rights)• Medi-Cal – reduces payment, but no real intervention
with the patient• If patient is stable for discharge, does not need medical
care, discuss reduction in services• Security escort out of hospital – depends on whether
the patient is ambulatory, needs continued care• Develop good relationship with your ambulance
services• Consider a contract with a cab or alternative service for
hospital paid transport 40
Behavior Strategies

41
Questions?