04. thyroid tumors
TRANSCRIPT

THYROID GLAND
TUMORSFahad zakwan
MD52014

introduction• Cancer is a group of many related diseases. All cancers
begin in cells, the body's basic unit of life. Cells make up tissues, and tissues make up the organs of the body.• Normally, cells grow and divide to form new cells as the
body needs them. When cells grow old and die, new cells take their place.• Sometimes this orderly process goes wrong. New cells
form when the body does not need them, and old cells do not die when they should. These extra cells can form a mass of tissue called a growth or tumor. • Growths on the thyroid are usually called nodules.

Thyroid nodules can be benign or malignant:• Benign nodules are not cancer.
• Cells from benign nodules do not spread to other parts of the body. • They are usually not a threat to life. • Most thyroid nodules (more than 90 percent) are benign.
• Malignant nodules are cancer. • They are generally more serious and may sometimes be life
threatening. • Cancer cells can invade and damage nearby tissues and organs. • Also, cancer cells can break away from a malignant nodule and
enter the bloodstream or the lymphatic system. • That is how cancer spreads from the original cancer (primary
tumor) to form new tumors in other organs. The spread of cancer is called metastasis.

Benign thyroid tumors
Follicular Adenoma• Present clinically as solitary nodule, may secret thyroid
hormones. The distinction between a follicular adenoma & carcinoma must be based on histological examination, FNAC is not sufficient as the difference between them is in the invasion of pericapsular blood vessels & the capsule of the gland.
Papillary adenoma• Actually does not even exist and any papillary
architecture should be considered as papillary carcinoma and hence treated as such.

Thyroid adenoma
Malignant tumors of the thyroid
• Frequency of thyroid Ca is approximately 1% of all malignancies. • The incidence of cancer of the thyroid gland varies between populations from 0.5% to 10% worldwide. • Thyroid cancer is the commonest (90%) of all endocrine malignancy with the highest contribution to endocrine related cancer death.• Thyroid cancer comprises of heterogeneous tumors with variable biological behavior.

•The risk and frequency thyroid cancer increases with age, and female to male ratio is 2.5:1. •Majority of these tumors present as a thyroid mass or nodular goiter. •Therefore a thyroid nodule may be malignant and the risk of malignancy varies depending on the type or characteristic of the nodule. •Secondary tumors are usually blood borne from cancer of breast, colon & kidneys.

The following are the major types of thyroid cancer:• Papillary and follicular thyroid cancers account for 80 to 90
percent of all thyroid cancers. Both types begin in the follicular cells of the thyroid. Most papillary and follicular thyroid cancers tend to grow slowly. If they are detected early, most can be treated successfully.• Medullary thyroid cancer accounts for 5 to 10 percent of
thyroid cancer cases. It arises in C cells, not follicular cells. Medullary thyroid cancer is easier to control if it is found and treated before it spreads to other parts of the body.• Anaplastic thyroid cancer is the least common type of thyroid
cancer (only 1 to 2 percent of cases). It arises in the follicular cells. The cancer cells are highly abnormal and difficult to recognize. This type of cancer is usually very hard to control because the cancer cells tend to grow and spread very quickly.

• If thyroid cancer spreads (metastasizes) outside the thyroid, cancer cells are often found in nearby lymph nodes, nerves, or blood vessels. • If the cancer has reached these lymph nodes, cancer
cells may have also spread to other lymph nodes or to other organs, such as the lungs or bones.• When cancer spreads from its original place to another
part of the body, the new tumor has the same kind of abnormal cells and the same name as the primary tumor. • For example, if thyroid cancer spreads to the lungs, the
cancer cells in the lungs are thyroid cancer cells. The disease is metastatic thyroid cancer, not lung cancer. It is treated as thyroid cancer, not as lung cancer

Papillary carcinoma of the thyroid gland • The Incidence of papillary carcinoma of the thyroid is 3.7
per 100.000 of the population, and Female to male ratio is 2.5:1. • The major predisposing factor is external irradiation to the
neck in childhood. • They accounts for about 80% of thyroid cancers in
childhood and 60% in adults. • They are slow growing and uncapsulated tumors. • Tumor is histologically characterized by papillary
projections with pale empty nucleus (Opharn Annie – eyed nuclei) and calcified bodies called psammoma bodies.
• The tumor have variable size and are usually multifocal (multiple foci in the same lobe) about 20-80% and bilateral in about one third of cases. • These tumors have tendency to lymphatic involvement within the thyroid and to regional lymph nodes in 80%, however only 35% will be detectable clinically. • The good thing about papillary carcinoma is that survival is not adversely affected by lymphatic spread and therefore they have good prognosis when compared to the rest of thyroid cancers with mortality of about 11%.


Occult carcinoma•The term occult carcinoma describes small probably clinically undetectable papillary tumors usually less than 1.5cm in diameter which has involved and caused enlargement of cervical lymph node which in turn is clinically detectable. •They have excellent prognosis.
Follicular carcinoma of the thyroid • Endemic nodular goiter due to prolonged TSH stimulation predisposes to Follicular carcinoma. • These tumors accounts for about 20% of all thyroid cancers and are common in iodine deficiency regions. • They are TSH dependant and tend to be slow growing, unifocal and capsulated. • It is the invasion of the capsule and pericapsular vessels which demonstrates malignancy in these tumors.

•Follicular carcinoma have tendency to hematogenous metastasis to involve lungs, bones and kidney and hence poorer prognosis when compared to papillary type. •They do not have tendency to multicentricity and lymph node involvement are rare. •Hürthle-cell carcinoma is a cytological variant with Hurthle (oxyphil cells); it is associated with poor prognosis.


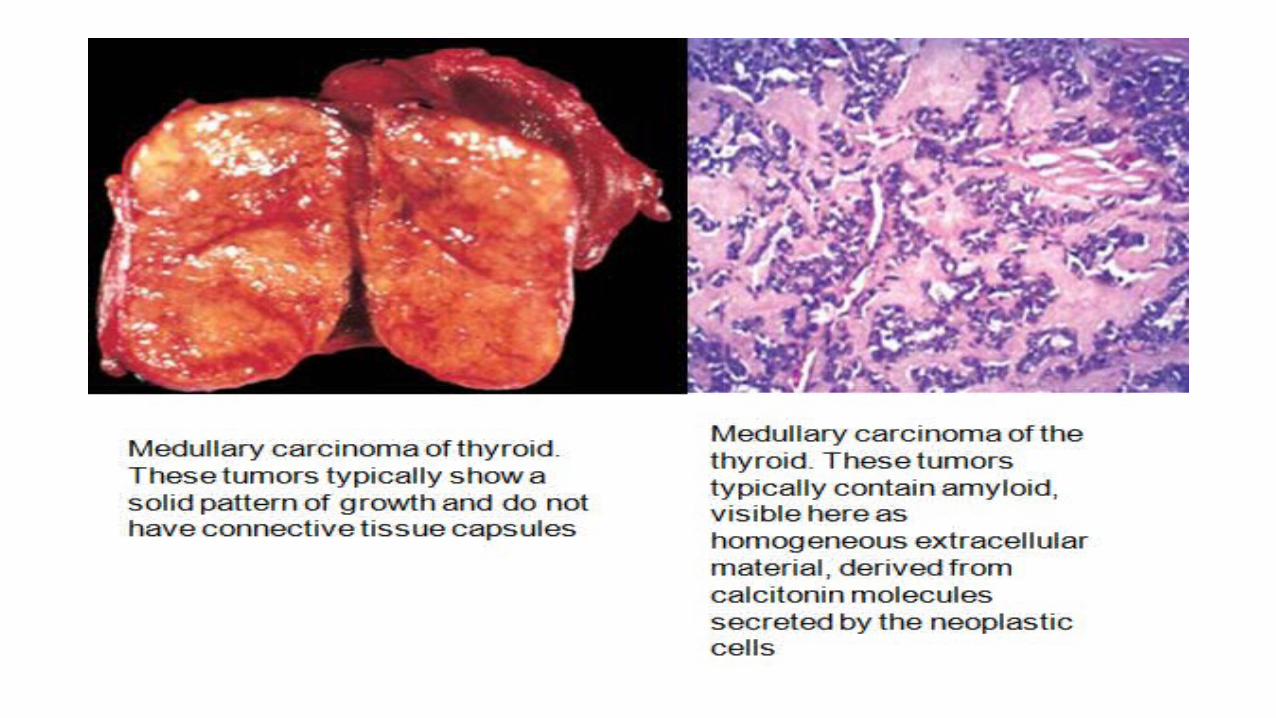
Medullary carcinoma of the thyroid gland• Originates in parafollicular (C cells), this tumor produces
calcitonin, but it can also secret other hormones such as corticotropin, serotonin, melanin and prostaglandins leading to paraneoplastic syndrome. • Because the tumor doesn’t arise from thyroid cells, it is
TSH independent. • The incidence is about of 6% of all thyroid cancers. • Medullary carcinoma may be familial (25%) which
affects children and young or sporadic (75%) which occurs at any age and sex.
• The tumor is usually unilateral and involves both regional lymph nodes in about 50% of patients and hematogenous metastases to the liver, lung, bone, and brain is common. • The overall survival of patients with medullary carcinoma is 65% at 10 years, and the poor prognostic factors include • advanced age, • advanced stage, • prior neck surgery, • associated-MEN.

Anaplastic carcinoma of the thyroid gland• This is a poorly differentiated tumor. • The incidence of anaplastic carcinoma of the thyroid is 13%, • it is a disease of old and female to male ratio is 1:1.5. • Microscopically it is composed of Spindle cell either small or
large cell type. • It is an aggressive tumor with extrathyroidal extension and
tends to spread by direct infiltration to adjacent structures leading to tracheal obstruction, perforation, recurrent laryngeal nerve infiltration with hoarseness, or esophageal obstruction. • It can also spread through regional lymphatics or blood spread. • It has the poorest prognosis of all thyroid cancers. • Most patients die within 1 to 2 years.

Lymphoma of the thyroid gland
• It a rare entity of the thyroid cancer, usually follows autoimmune Hashimoto’s thyroiditis. • It more common in females and tend occur in adulthood (60 years) and of Non Hodgkin type. • Thyroid lymphoma may be associated with hypothyroidism in 30-40%. • It grows fast, however the prognosis is favorable because it is usually confined to the thyroid which is accessible to chemotherapy and radiation

Investigations in thyroid neoplasia• Thyroid function test will exclude hyperthyroidism. • Fine Needle Aspiration Cytology (FNAC) is essential to establish malignancy. It is should always be done in thyroid neoplasia. • Lobectomy and histological examination • Lobectomy is the surgical removal one lobe of the thyroid gland, usually with ithsmusectomy. This should be done to all nodules with follicular pattern on FNAC.

• Thyroid scan • This is done in cases with intermediate cytological results. Cold
nodules are likely to be malignant, while hot nodules have very little likelihood of being malignant.• Chest X –rays • The chest X-ray is very important to rule out retrosternal
extension and lung metastasis. On the other hand thoracic inlet X-rays are necessary to establish tracheal compression and deviation.• Bone X-rays and bone scan• These two investigatations should be requested when bone
metastasis is suspected. This will establish bone metastasis especially follicular and medullary carcinoma of the thyroid. The former tend to cause osteolytic lesion and the later tend to form osteoblastic lesion on bone X-rays. Bone metastases are usually hot on bone scan.

•Abdominal ultrasound• Abdominal ultrasound is an important investigation to
exclude liver metastasis.
•Computed Tomography scan • CT scan of the neck, chest and abdomen can also
establish the extent of the tumor, especially in large tumors. In this way the nature of surgical intervention can be contemplated.
• Indirect Laryngoscopy• Indirect laryngoscopy is an important investigation. It is
advised in patient with hoarse voice to establish base line findings.

Causes and risk factors•No one knows the exact causes of thyroid cancer•Research has shown that people with certain risk factors are more likely than others to develop thyroid cancer•The following risk factors are associated with an increased chance of developing thyroid cancer:

Radiation.
• People exposed to high levels of radiation are much more likely than others to develop papillary or follicular thyroid cancer.• One important source of radiation exposure is treatment
with x-rays. • Another source of radiation is radioactive fallout. This
includes fallout from atomic weapons testing, nuclear power plant accidents and releases from atomic weapons production plants. • Such radioactive fallout contains radioactive iodine (I-
131). People, who were exposed to one or more sources of I-131, especially if they were children at the time of their exposure, may have an increased risk for thyroid diseases

Family history. • Medullary thyroid cancer can be caused by a change, or
alteration, in a gene called RET. The altered RET gene can be passed from parent to child. Nearly everyone with the altered RET gene will develop medullary thyroid cancer. • A blood test can detect an altered RET gene. If the
abnormal gene is found in a person with medullary thyroid cancer, the doctor may suggest that family members be tested. For those found to carry the altered RET gene, the doctor may recommend frequent lab tests or surgery to remove the thyroid before cancer develops. • A small number of people with a family history of goiter
or certain precancerous polyps in the colon are at risk for developing papillary thyroid cancer.

Being female.•Women are two to three times more likely than men to develop thyroid cancer.
Age.•Most patients with thyroid cancer are more than 40 years old. People with anaplastic thyroid cancer are usually more than 65 years old.
Race.•White people are more likely than African Americans to be diagnosed with thyroid cancer.

Not enough iodine in the diet.•The thyroid needs iodine to make thyroid hormone. • In the United States, iodine is added to salt to protect people from thyroid problems. Thyroid cancer seems to be less common in the United States than in countries where iodine is not part of the diet.

Symptoms of thyroid cancer
• Early thyroid cancer often does not cause symptoms. But as the cancer grows, symptoms may include:• A lump, or nodule, in the front of the neck near the Adam's
apple;• Hoarseness or difficulty speaking in a normal voice;• Swollen lymph nodes, especially in the neck;• Difficulty swallowing or breathing; or• Pain in the throat or neck.
• These symptoms are not sure signs of thyroid cancer. • An infection, a benign goiter, or another problem also
could cause these symptoms.

Staging of thyroid cancerTNM staging for differentiated thyroid carcinoma
• T Primary Tumor • TX Primary cannot be assessed • T0 No evidence of primary tumor• T1 Limited to thyroid 1cm or less• T2 Limited to thyroid 1cm less than 4cm• T3 Limited to thyroid more than 4cm• T4 Beyond thyroid capsule

•N Regional lymph node•Nx Regional lymph node cannot be assessed•N0 No regional lymph node metastasis•N1 Regional lymph node metastasis
•M Metastasis •Mx Cannot be assessed •M0 No metastasis •M1 Metastasis present

Clinical Staging
Stage Under 45years Over 45 years
I Any T, any N, M0 T1, N0, M0
II Any T, any N, M1 T2,N0,M0 or T3,N0,M0
III T4,No,M0 or Any T,N1,M0
IV Any T, Any N, M1
Only patients over 45 years have stage III and IV

Treatment of thyroid cancer• The choice on the procedure depends on type, differentiation
and stage at presentation; patients are generally regarded as low risk or high risk;
Low Risk• Female patients aged less than 50 years and male less than 40
years.• Patients with Papillary Ca, Follicular Ca (cytological suspicious),
tumor less than 1.5 to 2 cm, confined to one lobe, and without metastases.• Surgical intervention for low risk thyroid cancer is Lobectomy or
Near total thryoidectomy. • There is higher recurrence rate with lobectomy although the
overall survival between patients who undergo total near total thyroidectomy is not significant to those with lobectomy.

High Risk• Female patients aged more than 50 years and male
patients more than 40 years.• larger, bilateral tumors or metastases.• patients with Papillary Ca (extrathyroidal), Follicular Ca
(widely invasive) and Medullary Ca are considered as high risk. • Surgical intervention for high risk patients is usually total
thyroidectomy or near total thyroidectomy with neck lymphnode excision (central) or Modified radical neck dissection. • This is followed by postoperative thyroxine 100Umg/day to
suppress TSH in patients with thyroid hormone dependant thyroid cancers (papillary and follicular cancer)

•Note that medullary carcinoma is neither TSH dependant nor radioiodine sensitive. • Suppression of TSH reduces risk of recurrence and also improves survival. • Radioactive iodine I131 can also be used post operative to ablate all metastatic cells or tumor cells left during surgery. • A period of hypothyroidism is achieved by stopping thyroxin for a month to increase tumor cells sensitivity to radioactive iodine.

•For poorly differentiated (anaplastic) carcinoma of the thyroid; surgery (total thyroidectomy) can be tried if the patient presents early, this should be followed by chemoradiation. •In advanced cases chemoradiation is the mainstay of treatment.

Prognostic indicators in patients with differentiated thyroid carcinoma
• 10 years survival for middle-aged adults is about 80 to 95%, • 5 to 20% have local or regional recurrences while 10 to
15% have distant metastases. • The main survival determinants include; • age more than 45 years, • growth or type of tumor (pathology, differentiation), and
extent (micro vs. widely invasive), • size of the tumor less or more than 1.5cm • presence of metastasis and • completeness of surgical removal.

Thank you!!