as of june 1, sis data was available for 277 adults (initial sample drawn was 200 + 25) as of june...
TRANSCRIPT

As of June 1, SIS data was available for 277 adults (initial sample drawn was 200 + 25)
As of June 9, SIS data was available for 30 children and youth, ages 5 – 15 (initial sample drawn was 30)
Initial analyses consisted of: ◦ Sorting the data by the SIS Support Needs Index (SNI) ◦ Reviewing Overall Service Plan detail available in
Therap for 35 of the 277 adults◦ Examining the data for patterns related to exceptional
medical and behavioral needs◦ Looking for similarities and differences that might
relate to break-points in the SIS – SNI continuum
As verified by the Overall Service Plans for the adults we reviewed, the SIS – SNI differentiates between at least 3, possibly 4, levels of need:◦ Exceptional support needs and/or Higher support
needs (SNIs as high as 126)◦ Medium support needs (may be from ~ 80 to ~
100)◦ Lower support needs (SNIs as low as 55)
ICFs-MR were not listed as a service option for people with scores below 105, although Family Supports, TCLF, SLA, MSLA, and ISLA were service options above 105

Data from the supplemental measures was received shortly before this meeting (on Tuesday) and requires additional analysis
Specific funding levels for the primary residential and day programs for each individual needs to be obtained from DDD◦ This will help us determine whether it is possible
to establish a tiered funding structure that can be used flexible to purchase services, by selecting the appropriate staffing level from the standardized rate tables
Because of the absence of normative data, additional study of the children and youth data will be required
We may want to wait until the end of June for additional SIS completions before fully analyzing the data from the Child SIS

Phone conference held on May 14th with two veteran DDD Program Managers
Questions included:◦ Who chairs the IDT / person centered planning
meeting?◦ What is the general order of the IDT meeting?◦ How are the supports & services prioritized? ◦ What guidelines exist for what you can authorize
vs. what you need additional approvals to authorize?
◦ What is the current process for service authorization?
Generally, the service provider’s Program Coordinator chairs the IDT meeting, except in traditional self-directed supports or in the absence of a Program Coordinator, when Program Manager does it
The Overall Service Plan (OSP) is documented by the Program Manager; the Person Centered Service Plan (PCSP) is documented by the Program Coordinator◦ The OSP details what DHS pays for, plus generic services
(DD waiver / State Plan)◦ The PCSP lists goals, objectives, supports, medical, rights
issues, risk assessment, and financial info◦ All plan documentation is moving to Therap

For adults, all meetings are run pretty much the same way: ◦ First, do introductions, ◦ Then review confidentiality, ◦ Review progress from the previous year’s plan
(review outcomes), ◦ Go through the provider’s assessment results, ◦ Update medical status / appts, goals – see if they
still want those or have new ones, ◦ Review services to see if they are still appropriate), ◦ Review the risk assessment & rights documentation, ◦ Sign releases of information

For children, the Program Coordinator:◦ Talks with the parent(s) about what child is doing -as
part of the “present level”, they try to get the last dates for medical & dental visits, etc.
◦ Asks for the challenges that still exist; and ◦ Updates the risk assessment
Services are not prioritized. It’s expected that if it’s on the plan, the provider will get it done
If it is contracted service, in which a provider is granted a set number of hours of service, providers may indicate a reason a support or service cannot be done related to funding / authorized hours

For adults, the Program Manager (PM) authorizes services in the plan IF nothing changes◦ PM has to get a review for additional services
above what is currently authorized or services that are requested at higher levels
◦ If the person is in day services, all added services require Program Administrator (PA) review
For children, there is a statewide application that the PA has to authorize and a criteria for determining how much support is authorized◦ The application spells out these limits

Program Managers would be granted access to SIS Online, to enable them to review an individual’s assessment prior to the team meeting◦ The review process would involve:
Checking notes made by the SIS interviewer Looking for areas in which the individual needs support that
are not currently being addressed in the Overall Service Plan and its components
Determining which tier (Exceptional / Higher, Medium, or Lower) the individual is in and if it is on the borderline, whether any factors from the Risk Assessment would move the individual into a higher tier
More emphasis might be placed on using Essential Lifestyle Planning (Smull) or other person-centered planning methods, to “think outside the box”
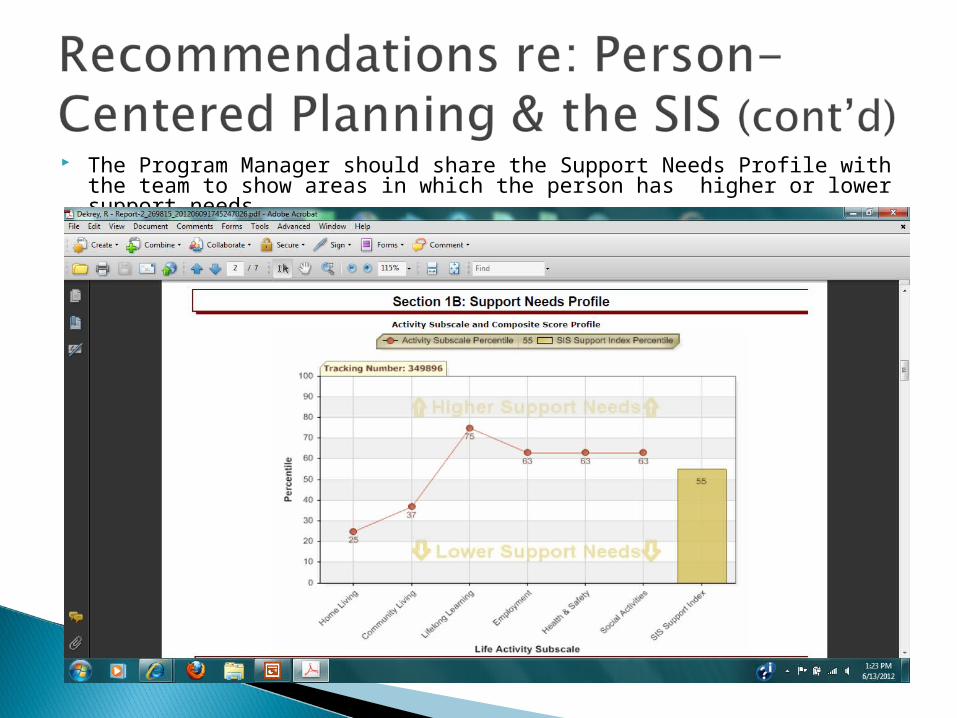
The Program Manager should share the Support Needs Profile with the team to show areas in which the person has higher or lower support needs
The Program Manager, who is responsible for authorizing services, would review service options available on the rate table and other options, to see how the identified needs could be met in the most cost-effective manner:◦ What has been tried in the past? How do other people
in the community usually address similar needs?◦ Does the individual, family, or any other team member
have an idea on how to meet this need? ◦ Could adaptations in people, environment, or
equipment help the individual `meet this need?◦ What informal resources (family, friends, and
volunteers) might be able to help?◦ What other community resources could be sought?

Does the current ratio of Program Managers to individuals served promote the right amount of external accountability?
Will discontinuing the use of the PAR free up more time for Program Managers for meeting preparation and QA?
Can Program Coordinators find creative approaches that would free up resources to be used to address the quality indicators (self determination and community integration)?