ª 2017 by the american college of cardiology …the gold standard to objectively assess func-tional...
TRANSCRIPT

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 7 0 , N O . 1 3 , 2 0 1 7
ª 2 0 1 7 B Y T H E A M E R I C A N CO L L E G E O F C A R D I O L O G Y F O U N DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 8 . 0 1 2
THE PRESENT AND FUTURE
STATE-OF-THE-ART REVIEW
Cardiopulmonary Exercise TestingWhat Is its Value?
Marco Guazzi, MD, PHD,a Francesco Bandera, MD, PHD,a Cemal Ozemek, PHD,b David Systrom, MD,c,d
Ross Arena, PHDb
ABSTRACT
Fro
Mi
Sci
Me
Ce
rel
Ma
Compared with traditional exercise tests, cardiopulmonary exercise testing (CPET) provides a thorough assessment of
exercise integrative physiology involving the pulmonary, cardiovascular, muscular, and cellular oxidative systems. Due to
the prognostic ability of key variables, CPET applications in cardiology have grown impressively to include all forms of
exercise intolerance, with a predominant focus on heart failure with reduced or with preserved ejection fraction. As
impaired cardiac output and peripheral oxygen diffusion are the main determinants of the abnormal functional response
in cardiac patients, invasive CPET has gained new popularity, especially for diagnosing early heart failure with preserved
ejection fraction and exercise-induced pulmonary hypertension. The most impactful advance has recently come from the
introduction of CPET combined with echocardiography or CPET imaging, which provides basic information regarding
cardiac and valve morphology and function. This review highlights modern CPET use as a single or combined test that
allows the pathophysiological bases of exercise limitation to be translated, quite easily, into clinical practice.
(J Am Coll Cardiol 2017;70:1618–36) © 2017 by the American College of Cardiology Foundation.
I n cardiopulmonary disorders, exercise intoler-ance is a major clinical feature from early stages,and becomes a source of symptoms and the
reason for referral to a physician. Exercise limitationis one of the most disabling problems experiencedby patients with heart failure (HF) (1). Its quantifica-tion may be approximated by several methods, but athorough analysis of the organ systems and pathwaysinvolved in the impaired physiological response isobtained by exercise gas exchange analysis withcardiopulmonary exercise testing (CPET). Thistechnique enables the clinician to scrutinize reasonsfor dyspnea and fatigue to precisely differentiatecardiac from pulmonary disorders, optimize thedecision-making process and outcome prediction,and objectively determine targets for therapies (2).Furthermore, CPET has become a reproducible (3)and safe technique (4).
m the aUniversity of Milan, Cardiology University Department, Heart Fai
lanese, Milan, Italy; bDepartment of Physical Therapy, Department of K
ences, University of Illinois at Chicago, Chicago, Illinois; cDivision of Pu
dicine, Brigham and Women’s Hospital and Harvard Medical School, B
nter, Brigham and Women’s Hospital, Boston, Massachusetts. The auth
evant to the contents of this paper to disclose.
nuscript received August 1, 2017; accepted August 2, 2017.
Despite this attractive evidence base and the clinicalpotential of CPET, the question put forth in the title ofthe present review (i.e., what is the value of CPET), isnot trivial, and the definitive response requiresmentioning a few historical notes and passages.
The idea of a CPET application in cardiology wasintroduced in the early 1980s byWeber et al. (5), whosework allowed the landmark classification of patientswith HF with reduced ejection fraction (HFrEF) basedon peak oxygen consumption (VO2), from A (peak VO2
> 20 ml $ kg�1 $ min�1) to D (peak VO2 < 10 ml $ kg�1 $
min�1) through B (peak VO2<20 to>15ml $kg�1 $min�1)and C (peak VO2 < 15 and 10 ml $ kg�1 $ min�1).
A few years later, Mancini et al. (6), in their seminal1991 paper, demonstrated that VO2 measured at peakexercise stratifies the risk of cardiovascular (CV) deathat 1 year in ambulatory patients with advanced HF.These remarkable findings were subsequently
lure Unit, IRCCS Policlinico San Donato, San Donato
inesiology and Nutrition, College of Applied Health
lmonary and Critical Care Medicine, Department of
oston, Massachusetts; and the dHeart and Vascular
ors have reported that they have no relationships

AB BR E V I A T I O N S
AND ACRONYM S
CaO2 = arterial oxygen content
CO = cardiac output
CPET = cardiopulmonary
exercise testing
CvO2 = venous oxygen content
EOV = exercise oscillatory
ventilation
HF = heart failure
HFpEF = heart failure with
preserved ejection fraction
HFrEF = heart failure with
reduced ejection fraction
PETCO2 = end-tidal pressure of
carbon dioxide
PETO2 = end-tidal pressure
of oxygen
tau = time constant
VCO2 = volume of carbon
dioxide released
VD = dead space
VE = ventilation
VO2 = peak oxygen
consumption
tidal volume
J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1619
validated and reproduced by several laboratories (7,8).This solid evidence perhaps led to a quite paradoxicalstatic vision of CPET applications for a long period (i.e.,until the 2000s), with a single parametric approachfocused just on advanced HF.
In the last 15 years, the utility of CPET has beenincreasingly recognized by both extending medical in-terest to the physiological bases of many variables thatwere previously under-recognized and by aligning evi-dence for a multivariable approach, including primarilyabnormalities in ventilation and its control (1). In HF, thecombined use of variables has led to the generation ofalgorithms (9) and risk scores (10–12) covering the entireset of HF stages. This process has been witnessed andvalidated by a significant number of official documentsand statements definitively (1,2,13) entering exercise gasexchange variables as study endpoint in the assessmentof the effects of emerging pharmacological therapies(14,15) and in interventional trials (16,17). Along with themain developments in HF, the role of routine CPET incardiology has been extended to specific patient pop-ulations, including those with suspected ischemic heartdisease (18), congenital heart defects (19), valve diseases(20), hypertrophic cardiomyopathy (21), suspected orconfirmed pulmonary arterial hypertension (PAH) (22),and left-sided pulmonary hypertension (PH) (23).
In this paper, the modern key applications of CPETin CV diseases, with primary emphasis on HF, arediscussed, starting from the principles that precipi-tate reduced exercise performance and impairedventilation, and highlighting the most recent de-velopments on combining exercise invasive hemo-dynamic and stress echocardiography with gasexchange evaluation. The large body of evidence onthe established pathophysiological clinical and prog-nostic impact of CPET-derived variables will beemphasized, making a continuum of value fromphysiological bases to their translation into thepractical applications. Accordingly, CPET is hereproposed as a technique that may provide significantand synergistic advancements in the process ofprecision medicine and phenotyping.
GAS EXCHANGE ANALYSES AND
THE PRINCIPAL BASES FOR
EXERCISE LIMITATION IN HF
OXYGEN TRANSPORT AND USE. The body underphysical stress behaves as a perfect machine that in-tegrates and harmonizes the functional responses ofmultiple organs and pathways. In this process, thedelivery of oxygen (O2) to mitochondria is essential toperform at aerobic capacity (24). Optimal O2 deliverydepends on a set of elegant biological interactions
between the functional components of the O2
transport chain, which requires oxygenationof the blood in the lung (alveolar diffusion),normal O2-carrying capacity of the bloodby adequate cardiac output (CO), yieldingto its redistribution to working muscles(delivery or convection) and adequate O2
release, diffusion from capillaries to cells,and tissue extraction from the blood(Central Illustration).
HF represents the typical condition wheremost of these pathways exhibit a maladaptiveresponse, impeding attainment of maximalVO2 because of the reduction in muscle O2
supply simultaneous with increasing de-mands for O2. Maximal performance istherefore defined by VO2 at peak exercise,conventionally measured as the VO2 averagedover a 20- to 30-s period at maximal effort,pending attainment of a respiratory exchangeratio (RER) >1.15 (1).
Measuring peak VO2 and, especially, thepercentage predicted, normalized to age-,sex-, and weight-based normative values, isthe gold standard to objectively assess func-tional limitations in cardiac patients (1).
What are the major pathophysiological reasons fora low peak VO2 in cardiac patients? These can bedescribed by analyzing the framework of the Fickprinciple (i.e., VO2 ¼ CO � [CaO2 � CvO2], where CO iscardiac output [stroke volume � heart rate], CaO2 isarterial oxygen content, CvO2 is venous oxygen con-tent, and [CaO2 � CvO2] is the arteriovenous [a-v]difference in O2).
On the basis of this equation, delivery or convec-tion and extraction are the 2 physiological processesthat convey O2 use through cellular pathways.O2 delivery is not only described by CO distribution,but is also the O2 content and the mechanismsinvolved in O2 dissociation from hemoglobin (Hb).O2 content is 1.34 (which corresponds to the ml of O2
carried by each gram of Hb) � O2 saturation � Hbconcentration.
Extraction is the net result of the chain of O2
transport and use, and depends on the ability of O2 todiffuse from capillaries to cells and on mitochondriafunction.
Normal, healthy adults can increase VO2 up to6-fold during exercise. The relative contributionof Fick’s equation determinants to VO2 changes isapproximately 1.2-, 2.5-, and 2.5-fold for strokevolume, heart rate, and CaO2 � CvO2, respectively.
Landmark pioneering studies (5,25) performed inpatients with HFrEF first demonstrated that low peak
VT =

CENTRAL ILLUSTRATION Determinants of the O2 Transport and Utilization Chain Framed on the Fick Principle
Guazzi, M. et al. J Am Coll Cardiol. 2017;70(13):1618–36.
Optimal O2 delivery depends on the optimal biological interaction between functional components of the O2 transport chain. This requires oxygenation of the blood in
the lung (alveolar diffusion), normal O2 carrying capacity of the blood by adequate CO; CO redistribution to working muscles (delivery or convection), and efficient O2
release, diffusion from capillaries to cells, and tissue extraction from the blood. The arteriovenous O2 difference reflects the extraction of O2 from mitochondria by
muscle cells. ATP ¼ adenosine triphosphate; CaO2 � CvO2 ¼ the arteriovenous difference in oxygen; CO ¼ cardiac output; Hb ¼ hemoglobin; HFpEF ¼ heart failure
with preserved ejection fraction; HFrEF ¼ heart failure with reduced ejection fraction; O2 ¼ oxygen; VO2 ¼ peak oxygen consumption.
Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1620
VO2 is tightly related to a limited CO increase andquite reasonably preserved peripheral O2 use. Whendata were stratified according to functional impair-ment, even Weber class D patients, despite having noincrease in CO, were still able to maintain theirCaO2 � CvO2 difference within the lower-normalrange (12 to 16 ml/dl). The underlying pathophysi-ology needs, of course, to be complemented with theconcept that along with reduced CO, several patientswith HF may have anemia and a lower O2 concen-tration, thus further impairing O2 delivery andchallenging the a-v O2 difference, irrespective of theability to efficiently extract O2 (1).
Intriguingly, observations have suggested thatiron deficiency in nonanemic patients with HF isresponsible for worse exercise performance andexercise gas exchange phenotypes (26). Theseobservations have been confirmed over time byseveral studies proving that in HFrEF, the capability
to extract O2 remains preserved thanks to an “opti-mized” peripheral blood flow redistribution and highmitochondrial activity (27–29), and that the cause ofan inadequate increase in CO is predominant, eventhough likely not exclusive. An additional set ofremarkable works aimed at assessing how much animpaired O2 diffusion may be involved in the lowaerobic performance (30), on the basis of Fick’s lawof diffusion: VO2 ¼ D � K � (PaO2 � PvO2), where D isequal to the O2 diffusive capacity (D), K is a constant,which is the ratio between arterial and venous O2
partial pressure (which is approximately 2), and(PaO2 � PvO2) is the capillary mitochondrial differ-ence, assuming an intracellular partial pressure of O2
close to 0.The relation of delivery or convection (Fick prin-
ciple) and diffusion (Fick’s law) can be represented ona diagram relating VO2 and PvO2, which are commonto both equations (Figure 1A).

FIGURE 1 The Relationship Between O2 Diffusion and Convection
3500
3000
2500 Peak
Peak
A
E
Controlpeak VO2
Fick law lines
Fick principle lines
C
D
B
30 W 30 W 30 W
RestRestCONVECTION
CONVECTION: VO2 = Q x [CaO2 – CvO2]
DIFFUSION
DIFFUSION: VO2 = D x k x PvO2
VO2 peak
2000
1500
1000
500
001009080706050403020100 2
Controls HFpEF HFrEF
4 6 8 10CvO2 in ml/dl
VO2 i
n m
l/min
Leg
VO2 (
ml/m
in)
Muscle Venous PO2 (Torr)
4000
A B C
3000
2000
1000
0
Oxyg
en C
onsu
mpt
ion
ml/m
in
Muscle Venous PO2, mm Hg12 14 16 18
(A) Scheme of the 2 relationships of delivery or convection (Fick principle) and diffusion (Fick’s law) in the diagram relating VO2 and in venous O2 pressure, which are
common to both equations (30). (B) Relative impairment of convection versus diffusion by 2 different exercise modalities, incremental test at maximum (A and B)
versus local isolated knee extension (C and D) (28). (C) VO2 and PvO2 relationship in a group of patients with HFrEF, HFpEF, and controls, showing a limitation in either
diffusion and convection (33). CaO2 ¼ arterial oxygen content; CvO2 ¼ venous oxygen content; D ¼ the O2 diffusive capacity; HFpEF ¼ heart failure with preserved
ejection fraction; HFrEF ¼ heart failure with reduced ejection fraction; K ¼ a constant (the ratio between arterial and venous O2 partial pressure, which is
approximately 2); O2 ¼ oxygen; PO2 ¼ oxygen pressure; PVO2 ¼ venous oxygen pressure; Q ¼ cardiac output; VO2 ¼ peak oxygen consumption.
J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1621
As proposed by Wagner (30), the diagram relatesVO2 to the muscle-venous PO2 from rest to peakexercise, with the lines of convection and diffusioncrossing the axes and intercepts, and whose slopevaries according to the muscle-venous PO2, with anupper and leftward shift representing the best diffu-sion, whereas the point of intersection between the 2lines represents the VO2 max (i.e., the resultant ofconvection and diffusion).
In a set of elegant, controlled experiments per-formed in HFrEF (28), the relative impairment ofconvection versus diffusion was assessed by testingthe same patients with 2 different exercise modal-ities: an incremental test at maximal exercise (needfor CO increase, central challenge) versus a localisolated knee extension (need for increase in O2
extraction, peripheral challenge) (Figure 1B). Theseexperiments were paralleled by the analysis of mus-cle fiber type, mitochondria volume, and thecapillary-to-fiber ratio.
Interestingly, skeletal muscle and mitochondriacontributed minimally to O2 limitation, in agreementwith the concept that mitochondrial oxidativecapacity largely exceeds O2 delivery at peak VO2 (31).Rather, patients with HF, compared with controls,exhibited an attenuation of convective and diffusivecomponents of O2 transport, both during maximalexercise and knee extension.
How do these concepts adapt to HF with preservedejection fraction (HFpEF) syndrome? Whereas some
pathophysiology overlaps between the 2 HF pheno-types, there is more uncertainty and unequivocaldefinition on the O2 transport/utilization-limitingsteps involved in the functional response of patientswith HFpEF. These patients are elderly and anemic ina high rate of cases, and exhibit a decreased totalcirculating red blood cell volume in 9 of 10 patientsaffected by Hb-based anemia, thus presenting withimpaired blood O2 carrying capacity (32). In addition,they may show a defect in O2 diffusion and lower(a-v) O2 (Figure 1C) (33).COMPLEMENTARY CPET-DERIVED MEASURES OF
AEROBIC EFFICIENCY. Although peak VO2 describesthe net limitation in exercise capacity, an even morecomprehensive idea of aerobic efficiency is obtainedby measuring the VO2 at the first ventilatory threshold(VT). VO2 at first VT reflects the metabolic conditionabove which blood lactate and pH start to increase anddecrease, respectively, generating isocapnic compen-satory acidotic buffering by bicarbonate (HCO3
�).There are 3 CPET-derived methods for detecting VO2 atthe first VT: the V-slope (i.e., the point at which theincremental volume of carbon dioxide [CO2] released[VCO2] becomes higher, as compared with VO2, due tothe additional CO2 produced by lactic acid buffering);the end-tidal CO2 (PETCO2) versus the end-tidal O2
(PETO2) method (when a divergent kinetic point of thesevariables occurs with PETO2 progressively increasingand the PETCO2 slightly decreasing) and the minuteventilation (VE)/VO2 versus VE/VCO2 ratio change in
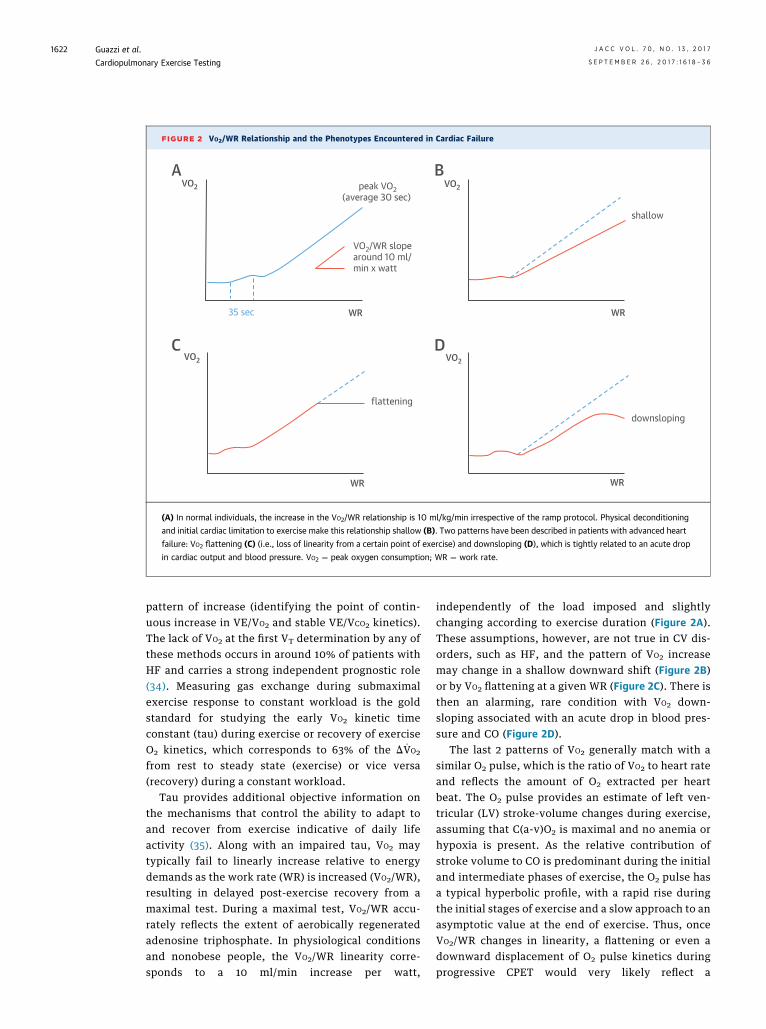
FIGURE 2 VO2/WR Relationship and the Phenotypes Encountered in Cardiac Failure
VO2
BA
DC
WR
shallow
VO2
WR
downsloping
35 sec
VO2/WR slopearound 10 ml/min x watt
WR
peak VO2(average 30 sec)
VO2
WR
flattening
VO2
(A) In normal individuals, the increase in the VO2/WR relationship is 10 ml/kg/min irrespective of the ramp protocol. Physical deconditioning
and initial cardiac limitation to exercise make this relationship shallow (B). Two patterns have been described in patients with advanced heart
failure: VO2 flattening (C) (i.e., loss of linearity from a certain point of exercise) and downsloping (D), which is tightly related to an acute drop
in cardiac output and blood pressure. VO2 ¼ peak oxygen consumption; WR ¼ work rate.
Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1622
pattern of increase (identifying the point of contin-uous increase in VE/VO2 and stable VE/VCO2 kinetics).The lack of VO2 at the first VT determination by any ofthese methods occurs in around 10% of patients withHF and carries a strong independent prognostic role(34). Measuring gas exchange during submaximalexercise response to constant workload is the goldstandard for studying the early VO2 kinetic timeconstant (tau) during exercise or recovery of exerciseO2 kinetics, which corresponds to 63% of the D _VO2
from rest to steady state (exercise) or vice versa(recovery) during a constant workload.
Tau provides additional objective information onthe mechanisms that control the ability to adapt toand recover from exercise indicative of daily lifeactivity (35). Along with an impaired tau, VO2 maytypically fail to linearly increase relative to energydemands as the work rate (WR) is increased (VO2/WR),resulting in delayed post-exercise recovery from amaximal test. During a maximal test, VO2/WR accu-rately reflects the extent of aerobically regeneratedadenosine triphosphate. In physiological conditionsand nonobese people, the VO2/WR linearity corre-sponds to a 10 ml/min increase per watt,
independently of the load imposed and slightlychanging according to exercise duration (Figure 2A).These assumptions, however, are not true in CV dis-orders, such as HF, and the pattern of VO2 increasemay change in a shallow downward shift (Figure 2B)or by VO2 flattening at a given WR (Figure 2C). There isthen an alarming, rare condition with VO2 down-sloping associated with an acute drop in blood pres-sure and CO (Figure 2D).
The last 2 patterns of VO2 generally match with asimilar O2 pulse, which is the ratio of VO2 to heart rateand reflects the amount of O2 extracted per heartbeat. The O2 pulse provides an estimate of left ven-tricular (LV) stroke-volume changes during exercise,assuming that C(a-v)O2 is maximal and no anemia orhypoxia is present. As the relative contribution ofstroke volume to CO is predominant during the initialand intermediate phases of exercise, the O2 pulse hasa typical hyperbolic profile, with a rapid rise duringthe initial stages of exercise and a slow approach to anasymptotic value at the end of exercise. Thus, onceVO2/WR changes in linearity, a flattening or even adownward displacement of O2 pulse kinetics duringprogressive CPET would very likely reflect a

J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1623
cardiogenic, rather than a peripheral vascular perfu-sion/extraction, limitation to exercise performance.Finally, the addition of systolic blood pressure to thepeak VO2, as circulatory power, has been proposedas having the potential to better investigate thecirculatory impairment (36).VENTILATORY EFFICIENCY AND LUNG MECHANICS.
Cardiac patients may exhibit a lung mechanical–related mechanism of exercise limitation, which istightly related to restrictive physiology due tocongestion and physical interaction between theheart and the lung (37). However, detection of lungmechanical dysfunction is often overlooked becausepatients with HF often display a normal breathingreserve, which is described by the relationshipbetween exercise VE and maximal breathing capacity,as estimated by resting maximal voluntary ventila-tion. Values <15% suggest a ventilatory limitation,and may help to discriminate between patients withHF and those with comorbid chronic obstructivepulmonary disease (COPD) (38).
The impaired breathing reserve would, however,be insensitive to mechanical ventilatory constraintscaused by differences in lung mechanics during ex-ercise compared to the maximal voluntary ventilationmaneuver. For this reason, the most recent consensusdocuments have introduced the use of flow-volumeloops as standard for the assessment of mechanicalVE limitation in cardiac versus lung disorders (2).Indeed, flow-volume loops supplement basic breath-ing mechanics information by identification of expi-ratory airflow limitation and changes in operationallung volumes during exercise.
Assessment of VE efficiency during CPET perhapsprovides the most relevant clues for addressing thepathophysiological changes behind the impairedexercise performance in HFrEF and HFpEF, especiallywhen associated with PH and right ventricular (RV)dysfunction (39,40). Similar reasoning may, in part,be applied to cases of post-embolic or idiopathic PAH.
An inefficient VE typically translates into anabnormal rate of increase in the slope of VE increaseversus VCO2 production. This relationship shows anear-linear increasing pattern that is determined by 3factors: the amount of CO2 produced; the physiolog-ical dead space/tidal volume ratio (VD/VT); and thearterial carbon dioxide partial pressure (PaCO2). Thisrelationship can be explained using the modifiedalveolar equation:
VE ¼ 863 � VCO2/(PaCO2 � [1 � VD/VT])For low and moderate intensities of work, the VE
response is tightly regulated by the PaCO2. At higherwork intensities, VE is affected by the increasedamount of VT over VD and the development of lactic
acidosis and proton (Hþ) production from theprevailing anaerobic metabolism, which furtherincreases CO2 release and the consequent amount ofVE. In HF, 3 different orders of mechanisms mediatean impaired VE requirement for a given CO2 produc-tion: increased waste ventilation (41,42); earlyoccurrence of decompensated acidosis (41,43); andabnormal chemoreflex and/or metaboreflex control(44). Recent findings obtained in HFpEF document aprimary role of increased VD/VT in causing a steepVE/VCO2 slope (45). In cases of a comorbid conditionwith COPD or COPD in isolation, high VD/VT mayprevail as a functional gas exchange abnormalitysustaining dyspnea sensation and hyperpnea (46).
The oxygen-uptake efficiency slope (OUES) is anunderused variable that reflects the global (pulmo-nary, CV, and skeletal muscle) functional impairmentby combining VO2 and VE/VCO2 slope. OUES is calcu-lated on the logarithmic transformation of VE data inliters/min (plotted on the x-axis), creating a linearrelationship with VO2 (plotted on the y-axis, whereVO2 ¼ log10 [VE þ b]). Given the tight linear relation-ship the OUES creates between VE and VO2
throughout a progressive exercise test (47), thiscalculation requires only submaximal effort.
Finally, an additional VE pattern at CPET evalua-tion, which is typically unmasked by gas exchangeanalysis, is an exercise oscillatory ventilatory (EOV)pattern (Figure 3) and consists of a cyclic fluctuationof VE and expired gas kinetics of variable amplitude,frequency, and duration detectable in up to 30% ofsymptomatic patients with HF (48). The source of thisventilatory abnormality is still controversial, but itsominous clinical and prognostic significance is clear(49,50). At variance with PAH, this pattern seemstypical of HF and pulmonary interstitial congestion,and a delayed circulatory transit time may explain theobserved differences (51).
APPLICATIONS OF CPET IN
CLINICAL PRACTICE
EVIDENCE INPREVENTIVEMEDICINEANDREHABILITATION
PROGRAMS. Application of CPET to primary andsecondary prevention is challenging. Interestingly, arole for CPET-derived data in detecting abnormal gasexchange pattern phenotypes has been just recentlyexplored in the general population at CV risk.An example is the European Exercise (EURO-EX)population-based trial, whose preliminary data havehighlighted some cases of EOV, typically occurring inthe phenotype of elderly diabetic women (52).
Overall, despite a wealth of persuasive evidenceand numerous statements supporting the utility of

FIGURE 3 9-Plot CPET Report of a Case of HFrEF With EOV
Time (sec)
VE (L
/min
) 0 100 200 300
0
20
40
60
80
Time (sec)0 100 200 300
0.0
0.5
1.0
1.5
0.0
0.5
1.0
1.5
VO2 (L/min)
HR (b
pm)
0.0 0.4 0.8 1.20
20
40
60
80
100
120
VCO2
VE (L
/min
)
0.0 0.4 0.8 1.20
20
40
60
80
Time (sec)
VE/V
O 2
VE/VCO2
0 100 200 3000
2
4
6
8
10
0
20
40
60
80
100
Time (sec)
HR (b
eats
/min
)
VO2 /HR
0 50 100 150 200 25060
70
80
90
100
0.0
0.1
0.2
0.3
0.4
0.5
VE (L/min)
V T (L) RR
0 20 40 60 800.0
0.5
1.0
1.5
2.0
0
20
40
60
Time (sec)
P ETO 2 (
mm
Hg)
PET CO
2 (mm
Hg)
0 100 200 30080
100
120
140
0
10
20
30
40
Work
VO2 (
mL/
min
)
VCO 2 (
L/m
in) VO
2 (L/min)
0 10 20 30 400.0
0.5
1.0
1.5
EOV is a specific VE abnormal phenotype occurring in approximately 30% of patients with mid-to-late manifestations of chronic heart failure, characterized by
cyclic fluctuation of VE and expired gas kinetics of variable amplitude, frequency, and duration. Because oscillatory manifestations may occur even in normal
subjects, criteria for an abnormal definition are an oscillatory pattern at rest that persists for $60% of the exercise test at an amplitude of $15% of the average
resting value (2). CPET ¼ cardiopulmonary exercise testing; EOV ¼ exercise oscillatory ventilation; HR ¼ heart rate; PETCO2 ¼ partial pressure of end-tidal carbon
dioxide; PETO2 ¼ partial pressure of end-tidal oxygen; RR ¼ respiratory rate; VCO2 ¼ volume of carbon dioxide released; VE ¼ ventilation; VO2 ¼ peak oxygen
consumption; VT ¼ tidal volume.
Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1624
CPET in prevention and in early HF stages, practi-tioners have not generally adopted a portfolio ofvariables that provides a 3-dimensional view ofcardiorespiratory fitness with diagnostic and prog-nostic applicability, and an effective means to eval-uate therapeutic benefits.
In the realm of patient care, exercise testingwithout the simultaneous collection of expired gaseshas seemingly taken on a static role, with the singular
(but not exclusive) purpose of evaluating signs andsymptoms of coronary insufficiency (53). However,despite observations pointing out the high sensitivityand specificity of gas exchange analysis in detectingsuspected myocardial ischemia (53,54), few of themrecognize a CPET role.
Implementation of rehabilitation and exercisetraining (ET) programs is a Class I (55) to IIa (56) guide-line recommendation. In this context, implementation

J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1625
of CPET is 3-fold: 1) to plan correct exercise intensitylevel or domain; 2) to assess benefits of exerciseprescription by monitoring gas exchange variables andtheir related phenotypes; and 3) to identify subjectswho, despite adherence to the program, are non- or poorresponders to this multilevel intervention.
Although guidelines recommend the application ofobjective exercise prescriptions using CPET data (57),it is commonplace for programs without CPET capa-bilities or with limited resources to establish exerciseintensity on the basis of resting heart rate (e.g.,exercising heart rate threshold set 20 or 30 beats/minabove the resting heart rate). This simple method hasbeen criticized and demonstrated to be inadequate bymany. For example, Reed et al. (58) reported that only26% and 38% of participants were exercising at therecommended exercise intensity of 40% to 60% ofheart rate reserve (confirmed by CPET) when usingresting heart rate þ 20 and 30 beats/min, respectively.Patients exercising at 30 beats/min or above theirresting heart rates experienced significantly greaterincreases in 6-min walk distances comparedwith patients exercising at 20 to 29 beats/minabove resting heart rate, suggesting that the imple-mentation of CPET as a standard tool in cardiacrehabilitation programs can really help to optimizehealth-related outcomes.
Accordingly, the recent joint European Associationfor Cardiovascular Prevention & Rehabilitation(EACPR)/American Association of Cardiovascular andPulmonary Rehabilitation Statement provideddirections on the identification of ET intensitydomains by using constant WR exercise tests, lookingat the different kinetic responses to VO2 (57), which,although it may be impractical in most cases, remainsthe most accurate physiology-based approach. Briefly,VO2 kinetics during a constant WR exercise reflect 3phases of adaptation of the organ systems and factorsinvolved in the alveolar-to-cell O2 coupling. The 3phases are identified as: phase I, or cardiodynamic,during which the increase in VO2 is mediated by theimmediate increase in CO and pulmonary blood flow atthe start of exercise; phase II, or cell respiration,reflecting the decreased O2 content (muscle extrac-tion) and increased venous CO2 content secondary toincreased cell respiration, as well as a further increasein CO; and phase III, or the eventual steady-statephase, during which an equilibrium is reached be-tween O2 extraction and the CO2 production rate. If theWR is above the subject’s first VT, the rate of increaseduring phase III is not steady and correlates tightlywith the magnitude of lactate increase.
This background applies and allows for the preciseidentification of 4 exercise training domains whose
intensity is based on the physiology of O2 uptakekinetics: light to moderate; moderate to high;high to severe; and severe to extreme. The light-to-moderate– and moderate-to-high–intensity programsare performed by continuous exercise, a conditionthat is not sustainable for high-to-severe and severe-to-extreme protocols, requiring an interval exerciseapproach. Intensity domains of light to moderateencompass the corresponding WR that engenders aVO2 steady-state value below the corresponding firstVT. During this constant workload range and in thisdomain, a VO2 steady state is attained relativelyrapidly following the onset of exercise, and lactate isnot produced. For this reason, exercise can be verywell tolerated and is generally sustainable for longperiods of time (30 to 40 min) with only a mild senseof fatigue and breathlessness. The moderate-to-high–intensity domain corresponds to workloads betweenthe first and second VTs.
An improvement in functional capacity is the mostimmediate and objective result of an effective ETprogram. Although functional capacity is governed byan integrated response of multiple organ systems thatare wholly or partly involved in this response, benefitsof ET interventions are generally quantified as changesin VO2. The physiological background behind exercisecapacity response and the progressive familiarizationof the cardiac rehabilitation personnel with the gasexchange analysis technique points, however, to astep forward that is a more in-depth analysis andcomprehensive interpretation of exercise interventiontrials. Indeed, attention to the determinants of exer-cise improvement that may add to peak VO2, andpotentially result in even more remarkable demon-stration of efficacy, seems quite timely.
One example of this reasoning is the unexplored,but perhaps intriguing, question of how much ET mayimprove VO2 kinetics (tau and VO2/WR linearity),rather than peak VO2. Specifically, looking at favor-able modifications that ET may induce in patterns ofVO2/WR (i.e., shallow, typical of deconditioned car-diac patients, flattening, or downsloping associatedwith acute drop in blood pressure and CO) (Figure 2).Thus, an analysis of the effects of different exercisetraining programs may be of value when consideringthe potential to modify these abnormal patterns, evenwhen changes in peak VO2 per se are not remarkable.DIAGNOSTIC ROLE OF CPET IN HF. As the severity ofCV disease advances, the role of CPET in the diag-nostic setting of HF is not completely recognized. The2013 American College of Cardiology (ACC)/AmericanHeart Association (AHA) guidelines for the manage-ment of HF highlight the subjective nature of the ACCFoundation/AHA stages of HF and the New York

Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1626
Heart Association functional classification system.These are primarily based on patient interviews per-taining to the “severity and triggers of dyspnea andfatigue, presence of chest pain, exercise capacity aswell as physical and sexual activity” (59), and arethen followed by objective procedures for character-ization of LV structure/function and evaluation ofdiagnostic blood markers. Despite evidence of CPETas a strong predictor of future HF development, itsconsideration as a primary diagnostic tool iscautioned, mainly due to the manifestations commonto other chronic conditions (e.g., PAH, congenitalheart defects, and interstitial lung disease) (60).However, it seems more appropriate to use CPETvariables to guide the diagnosis of secondary patho-physiological consequences of HF, irrespective ofetiology. Assessment of exercise ventilatory patternsis particularly attractive in identifying left-sided PHdue to its physiological link with ventilation-perfusion matching. Identification of left-sided PH isparticularly important, given that it is prevalent inroughly 30% to 50% patients with overt HF andcarries a poor prognosis (61). The VE/VCO2 slope, thePETCO2, and the presence of EOV hold a high level ofprognostic utility (9). In a study of parallel evaluationof pulmonary pressure, a VE/VCO2 slope of </$36 wasfound to be the strongest predictor (odds ratio [OR]:12.1; p < 0.001) of a pulmonary artery pressure(PAP) $40 mm Hg, followed by peak exercise PETCO2
(</$36 mm Hg; OR: 3.8; p < 0.001), and presence ofEOV (OR: 3.2; p < 0.001) in patients with HFrEF. Morecompelling was the greater predictive utility whenall measures were considered together (OR: 16.7;p < 0.001) (9). There have been significantly fewerstudies evaluating the relationship between diseaseseverity and CPET variables in patients with HFpEF,although most recent observations have shed newlight on VE efficiency (45,62). Considering that theVE/VCO2 relationship possesses prognostic value atsubmaximal levels of effort, this observation in-creases the feasibility of implementing CPET forprognostic purposes, particularly in an elderly popu-lation that is likely not accustomed to exercise or maybe hesitant to provide maximal effort.
Collectively, the aforementioned CPET indexesshould not be thought of as markers to identifyspecific pathophysiological conditions associatedwith HF, but rather for use of objective CPET data tohelp guide characterization of the HF disease state,which is staged, in part, by subjective determinants.Interpreting CPET outcomes in this manner helpsconfirming HF and identifying secondary issues andmay provide a clear objective in deciding the bestcourse of patient treatment.
MONITORING THERAPEUTIC EFFICACY WITH CPET. TheACC/AHA stages of HF provide a comprehensiveoutline of patient characteristics that define the stageof HF, as well as respective therapies and their asso-ciated goals. Many, if not all, therapeutic goals aim tomitigate HF-related symptoms (e.g., dyspnea at restand/or upon exertion, fatigue), reduce hospitalreadmission rates, and improve survival. The acuteefficacy of a number of therapeutic regimens aretypically verified by standard follow-up visits thatassess the patient’s resting blood pressure, weight,blood markers, and patient-reported changes insymptom severity/presence. This system of patientmanagement is generally considered to be adequatein most clinical settings, and therefore leaves manypractitioners with a lack of clarity as to the addedvalue of CPET. However, an important considerationis that follow-up visit examinations are done at rest,thus providing no information on symptoms andon hemodynamic measures during physical exertion(when symptoms typically become evident).Furthermore, the main aim of any intervention is toimprove prognosis, limit morbidity, and increase thequantity of years a patient is able to live a higherquality of life, all of which are markers associatedwith high peak VO2 values and lower VE/VCO2 slopes.
Furthermore, the current ACC/AHA guidelinesrecognize the therapeutic benefits of various phar-macological interventions to improve cardiorespira-tory fitness. Angiotensin-converting enzyme (ACE)inhibitors or angiotensin II receptor blockers (ARBs)significantly improve peak VO2 on their own and haveled to greater enhancements when taken together(63). These improvements also translate to reductionsin the VE/VCO2 slope with ACE inhibitor therapy;however, there are conflicting outcomes with ARBtherapy (64). The effects of b-blockers on exerciseperformance have been extensively studied, andCPET application has garnered relevant information,in terms of influence of different types of b-blockerson gas exchange (65). Moreover, decreases in PAP,with concomitant decreases in the VE/VCO2 slope (66)and some reversal of EOV (67), have been demon-strated with sildenafil therapy in patients withHFrEF. By contrast, CPET outcomes in response toACE inhibitor, ARB, or sildenafil therapy in patientswith HFpEF have not been as favorable (68–70). Thesame seems to be true for ivabradine (71).
Given the associated improvements in key prog-nostic CPET variables with the initiation of pharma-cological therapy in certain patient populations, itmay be interesting to explore the feasibility oftitrating medications based on CPET “responders” or“nonresponders” in future clinical trials. Peak VO2 is

J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1627
an endpoint in trials of cardiac resynchronizationtherapy, LV assist device implantation, and valvesurgical or percutaneous treatments, even thoughCPET-derived variables are not standardized criteriafor these indications (2).
The frequency at which a patient should performCPET evaluation to monitor the effectiveness ofinterventions is not well-defined. Certainly, in clini-cally stable patients, CPET should be considered at2- to 4-year intervals, whereas in patients with signsand symptoms, the test should occur in a time framethat has been reported to cause significant improve-ments in the variable of interest (2).PROGNOSTIC UTILITY OF CPET. Among the exten-sive list of criteria for determining candidates fortransplantation, CPET variables are recognized tohelp refine the selection process. At time of Manciniet al.’s investigation (6), demonstrating a higher1-year survival rate in HF patients with peak VO2
>14 ml $ kg�1 $ min�1 compared with patients withpeak VO2 #14 ml$kg�1$min�1, and a similar 1-yearsurvival rate of transplanted patients compared withthose above the 14 ml$kg�1$min�1 threshold,b-blocker therapy was not part of routine clinicalmanagement of patients with HF, as it became in theearly 2000s. Despite the marginal effects ofb-blockers on peak VO2, survival rates were signifi-cantly improved, and therefore prompted reconsid-eration of Mancini et al.’s proposed cutoff fortransplantation. Consequently, a threshold of10 ml$kg�1$min�1 was proposed to be the optimalprognostic threshold for transplantation consider-ation for b-blocked patients with HFrEF (72). Inaddition to these landmark studies, a continuingwealth of evidence has fortified the prognosticstrength of peak VO2, so much so that the Interna-tional Society for Heart Lung Transplantation pro-vides a Class I, Level of Evidence: B recommendationfor inclusion of maximal CPET (RER > 1.05) to guidetransplant listing, with peak VO2 #14 ml$kg�1$min�1
(Class I, Level of Evidence: B) in the absence of ab-blocker and a peak VO2 #12 ml$kg�1$min�1 (Class I,Level of Evidence: B) in its presence (73). However, anequally impressive and convincing body of publishedreports identifies ventilatory efficiency (e.g., theVE/VCO2 slope and EOV) as a more powerful prog-nostic index than peak VO2 (74). Despite the growingbody of evidence highlighting the greater prognosticutility of the VE/VCO2 slope, current ACC/AHA guide-lines recognize peak VO2 as the sole CPET outcome fortransplant consideration. Similarly, the InternationalSociety for Heart Lung Transplantation recommendedthat the VE/VCO2 slope be reserved (slope >35; ClassIIb, Level of Evidence: C) for CPET performances with
a submaximal effort (RER <1.05). Both sets of rec-ommendations are also similar in that they recom-mend the use of one of the CPET parameters, eventhough there is strong evidence for the increaseddiscriminatory power of the VE/VCO2 slope and othervariables considered together (2,10,75).Mult iparametr i c CPET data table . It is evidentthat across the years, there has been a surge of CPETvariables, making it difficult for clinicians to identifyand interpret measures of interest. To ameliorate thisconcern, early efforts by Wasserman (24) (Figure 3)provided 9 visually friendly panel plots incorporatingthe CPET variables of interest in a single-page report.A potential disadvantage of this method, however,was the lack of guidance or references to variablethresholds pertinent to CPET clinical application.Accordingly, Arena et al. (76) developed an earlyiteration of the figures by proposing color-codedinterpretive tables applied to different diseases. Anexample is shown in Table 1 (for HF), where the list ofCPET variables (the VE/VCO2 slope, peak VO2, EOV,resting PETCO2) was separated into primary (e.g., theVE/VCO2 slope and peak VO2) and secondary (e.g., EOVand resting PETCO2) CPET measures of interest, alongwith respective categories of risk. Furthermore,instructions were provided to help with guiding theinterpretation of multivariable CPET results. Thisapproach took valuable initial steps towardcondensing a large amount of CPET-related informa-tion into a single table that could be used by cliniciansin patient management. Many modifications weremade and subsequently integrated and presented inthe 2012 EACPR/AHA Scientific Statement (1). Thecolor-coded tables now provide striking visual cluesto facilitate the interpretation of CPET. Normal re-sponses are identified in green, whereas intensifyingabnormalities are highlighted in yellow, orange, andred. Expanded clinical recommendations for theoverall severity of the patient’s condition are pro-vided, based on the frequency of color occurrence inthe table. Of note, the decision to include therespective CPET variables in the outcome tables wasbased on the available evidence, summarized inTable 2, for the predictive application of each measureindependently, but more importantly, collectivelyacross populations. Moreover, these tables weredeveloped with the objective of being applicable andrelevant to the qualifications for CPET (e.g., prog-nosis, therapeutic efficacy, and diagnosis) in orderto promote their use. As such, the AHA, and EACPRhave made an effort to increase the visibility of amultivariable paradigm that implements visual cluesto trigger appropriate actions. Because no studieshave yet tested the feasibility of this model’s

TABLE 1 Clinical Stratification for Patients With HF
Primary CPET Variables
VE/VCO2 Slope Peak VO2 EOV PETCO2
Ventilatory Class I
VE/VCO2 slope <30.0
Ventilatory Class A
Peak VO2 >20.0 ml$kg�1$min�1
Not Present Resting PETCO2
$33.0 mm Hg3–8 mm Hg increase during ET
Ventilatory Class II
VE/VCO2 slope 30.0–35.9
Ventilatory Class B
Peak VO2 ¼ 16.0–20.0 ml$kg�1$min�1
Ventilatory Class III
VE/VCO2 slope 36.0–44.9
Ventilatory Class C
Peak VO2 ¼ 10.0–15.9 ml$kg�1$min�1
Present Resting PETCO2
<33.0 mm Hg<3 mm Hg increase during ET
Ventilatory Class IV
VE/VCO2 slope $45.0
Ventilatory Class D
Peak <10.0 ml$kg�1$min�1
Standard ET Variables
Hemodynamics ECG HRR
Rise in systolic BP during ET No sustained arrhythmias, ectopic foci, and/or ST-segmentchanges during ET and/or in recovery
>12 beats at 1 min recovery
Flat systolic BP response during ET Altered rhythm, ectopic foci, and or ST-segment changes duringET and/or in recovery: did not lead to test termination
#12 beats at 1 min recovery
Drop in systolic BP during ET Altered rhythm, ectopic foci, and/or ST-segment changes duringET and/or in recovery: led to test termination
Patient Reason for Test Termination
Lower extremity muscle fatigue Angina Dyspnea
Interpretation
� All variables in green: excellent prognosis in the next 1–4 years ($90% event-free)B Maintain medical management and retest in 4 years
� Greater number of CPET and standard ET variables in red/yellow/orange indicative of progressively worse prognosis.B All CPET variables in red: risk for major adverse event extremely high in next 1–4 years (>50%)
� Greater number of CPET and standard ET variables in red/yellow/orange indicative of increasing HF disease severity.B All CPET variables in red: expected significantly diminished cardiac output, elevated neurohormones, higher potential for secondary PH.
� Greater number of CPET and standard ET variables in red/yellow/orange warrants strong consideration of more aggressive medicalmanagement and surgical options.
Example of a color-coded table for clinical stratification that applies to patients with either HFrEF or HFpEF. A list of evidence-based CPET variables (the VE/VCO2 slope, peak VO2,EOV, resting PETCO2) are separated into primary (e.g., the VE/VCO2 slope and peak VO2) and secondary (e.g., EOV and resting PETCO2) measures of interest, along with respectivecolor-code categorizations of risk (2).
BP ¼ blood pressure; CPET ¼ cardiopulmonary exercise testing; ECG ¼ electrocardiogram; EOV ¼ exercise oscillatory ventilation; ET ¼ exercise testing; HF ¼ heart failure;HFrEF ¼ heart failure with reduced ejection fraction; HFpEF ¼ heart failure with preserved ejection fraction; HRR ¼ heart rate recovery; PETCO2 ¼ partial pressure of end-tidalcarbon dioxide; PH ¼ pulmonary hypertension; VE/VCO2 ¼ minute ventilation/carbon dioxide production; VO2 ¼ oxygen consumption.
Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1628
implementation in a clinical setting, as well as itseffect on patient management, future studies areencouraged to do so.
REAPPRAISAL OF INVASIVE CPET
Invasive CPET (iCPET) allows better characterizationof the hemodynamic reasons for exercise limitations,precisely dissecting central and peripheral mecha-nisms. As this approach has the potential to accu-rately phenotype cardiopulmonary disorders, it hasbeen reappraised since its initial use in early 1980s asa routine approach in more laboratories (77).Measuring pulmonary hemodynamics, LV fillingpressures, Fick CO, and a-v difference in O2, becomeessential in cases of unexplained exercise-induceddyspnea (78) and in the evaluation of exercise-induced PH of either idiopathic or secondary origin (79).
A recent analysis documented that iCPET allowsto considerably shorten the time lag from manifes-tations of unexplained exercise-induced dyspnea toan organ-specific diagnosis. Conditions that can beultimately diagnosed with iCPET are HFpEF, mito-chondrial myopathy, and confirmation of decondi-tioning (78).
Pulmonary hemodynamic measurements duringexercise, especially of PAP and pulmonary arterialwedge pressure (PAWP), have incremental prognosticvalue compared with evaluation at rest (79).
Borlaug et al. (80) first reported the potential todiagnose HFpEF in symptomatic euvolemic patientswith normal levels of B-type natriuretic peptide andwithout clear signs and symptoms of HF at rest. Inone-half of cases, looking at the PAWP and end-diastolic LV pressure increase, the observed increasein PAWP during exercise was diagnostic for HFpEF.

TABLE 2 Class Recommendation and Level of Evidence for CPET Applications in HF
ClassificationLevel ofEvidence
Prognostic Recommendations
CPET should be performed in patients with HFrEF beingconsidered for heart transplantation or mechanical deviceimplantation. However, CPET provides robust prognosticinformation in all patients with HFrEF and therefore is alsorecommended in those not being considered for end-stagesurgical management.
Class I A
Primary CPET variables, including the VE/VCO2 slope, peak VO2,and EOV, are strong predictors of adverse events. Theresponse of these 3 CPET variables is recommended to formthe basis of the prognostic assessment in patients withHFrEF. A combination of a VE/VCO2 slope $45.0, peakVO2 #10 ml$kg�1$min�1, and the presence of EOV carries aparticularly poor prognosis.
Secondary CPET variables, including PETCO2, O2 pulse, systolicblood pressure, and the ECG response to exercise, areadditional predictors of adverse events and can be usefulduring the prognostic assessment in patients with HFrEF. Aresting PETCO2 <33 mm Hg, a rise in PETCO2 <3 mm Hg duringexercise, a drop in systolic blood pressure during exercise,and/or ECG abnormalities warranting termination of exerciseindicate a worse prognosis.
Class IIa B
Prognostic value in patients with HFpEF is showing initialpromise, in particular, the VE/VCO2 slope, peak VO2, and EOV.These variables can be useful in providing prognosticinformation also in patients with HFpEF.
Class IIa B
Use of a multivariate model composed of key CPET variables andthresholds, as illustrated in Figure 4, can be useful inimproving prognostic resolution in patients with HFrEF incomparison with variables assessed independently.
Class IIa B
Recommendations for Gauging Therapeutic Efficacy
Primary CPET variables, including the VE/VCO2 slope and peakVO2, are responsive to numerous pharmacological, surgical,and exercise interventions in patients with HFrEF. As such,assessment of the change in the VE/VCO2 slope and peak VO2
is recommended when gauging therapeutic efficacy inpatients with HFrEF in both clinical and research settings.
Class I A
Reversal of EOV also may occur with pharmacological andexercise interventions in patients with HFrEF. Therefore,assessing for reversal of EOV as a gauge of therapeuticefficacy can be useful in both clinical and research settings.
Class IIa B
Primary CPET variables, including the VE/VCO2 slope and peakVO2, may be responsive to pharmacological, surgical, andexercise interventions in patients with HFpEF. As such, theVE/VCO2 slope and peak VO2 can be useful as core variableswhen gauging therapeutic efficacy in patients with HFpEF inboth clinical and research settings.
Class IIa C
Diagnostic Recommendations
CPET variables reflecting ventilatory efficiency, including theVE/VCO2 slope, EOV, and PETCO2 at rest and during exercise,may be considered in detecting left-sided PH in patients withHFrEF and HFpEF. If all 3 of these variables are in theirrespective red zones, as illustrated in Table 1, the suspicionthat the patient has left-sided PH may be reasonable. Aprimary indication of CPET for diagnostic purposes cannot berecommended at this time. Diagnostic assessments may beconsidered in patients with HF and suspicion of PH.
Class IIb B
Abbreviations as in Table 1.
J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1629
These data were reproduced by others, showingthat in patients with normal biventricular function, anincreased mean PCWP >20 mm Hg at peak exercise, inthe absence of elevations in pulmonary vascularresistance, suggests exercise-induced HFpEF (81).Patients with early stages of PAH and still normalcardiopulmonary hemodynamics at rest demonstrateincreased mean PAP >30 mm Hg and pulmonaryvascular resistance >80 to 120 dyne $ s $ cm5 oniCPET (82).
Exertional intolerance may be associated with pre-load–dependent limitations to stroke volume and CO(83). In this patient population, failure to augmentright atrial pressure on exercise is observed despiteabnormally decreased CO. Finally, impaired systemicO2 extraction indicates left-to-right shunting or amitochondrial myopathy. An algorithm for diag-nosing these conditions was recently proposed byHuang et al. (78).
Accurate assessment of the pressure-flow relation-ship during exercise by plotting mean PAP versus COprovides robust indication of abnormalities in RV topulmonary circulation coupling (79). A mean PAP/COrelationship >3 mm Hg/l/min is reflective of a PHresponse, which combines with an elevated VE/VCO2
slope (39). Evenmore, occurrence of RV-to-pulmonarycirculation (PC) uncoupling is responsible for adelayed VO2 on kinetics during early exercise (84).
The most relevant limitations to this approach areits invasive nature and technical inaccuracies inobtaining reliable pulmonary hemodynamic tracingsduring high respiratory frequencies, despite aver-aging of repeated measures.
CPET IMAGING: A NEW FRONTIER
CPET imaging is a quite recent and valuable testingmodality, which is receiving attention for its potentialto combine exercise physiological data with noninva-sive recordings of cardiac function by measures ofchamber volumes and geometry, valvular status, andsystolic and diastolic function, including the evalua-tion of left atrium (LA) function (85). In addition, theassessment of cardiac “functional reserve” by CPETimaging is greatly improved by the study of the path-ophysiological response of the pulmonary circulationto exercise, whose clinical implications appear com-plementary to and synergistic with the informationobtained with iCPET (86,87). A typical example of thisconcept is the identification of a basic role of RV topulmonary circulation uncoupling in determining theflattening of the DVO2/DWR relationship (88).
On a methodological basis, there is not yet stan-dardization, but the semirecumbent position is
suggested for a better Doppler evaluation of param-eters that are strictly dependent on workload (i.e.,systolic pulmonary pressure, transvalvular gradients,LV outflow gradients) and decline quickly during thefirst seconds of recovery. Feasibility is strictlydependent on the acoustic window and its variability

Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1630
during exercise caused by breath, body motion, andheart movements.
Incremental ramps at low increasing workload (8 to15 W/min) are preferable for fully acquiring imagesevery 2 min. Loop storage of adequate duration (3 to 5beats) is required in order to perform the averagingof measures, especially for Doppler parameters,accounting for physiological respiratory variations.Figure 4 summarizes the main parameters providedby CPET imaging, pointing out their applications tospecific cardiac diseases, with some illustrative casesof HFrEF, HFpEF, mitral valve insufficiency, andhypertrophic cardiomyopathy.HF WITH REDUCED EJECTION FRACTION. There aremultiple applications of CPET imaging in HF. First, agood discrimination between circulatory ratherdeconditioning limitation is signaled by the inabilityto reach an exercise stroke volume >50 ml/m2 (89).The importance of measuring CO reserve (90,91) inparallel with LV compliance and filling pressures iswell-established (92). Furthermore, estimation of O2
peripheral extraction by CPET imaging using theechocardiographic-derived Fick equation is an im-mediate method to explore the role of the periphery(90). Assessment of functional mitral regurgitation(MR) is of basic relevance as a marker of severity andadverse outcome (93), which, in early stages, may bedetectable just during exercise (20). Exercise-inducedMR determines the same extent of exercise limitationobserved in patients with severe MR at rest. DynamicPH is a further limiting mechanism, also induced byMR, and is associated with specific ventilatory phe-notypes of gas exchange, such as EOV (20). Inadvanced HFrEF, assessment of exercise-induced RVcontractile reserve may be investigated by CPETimaging. In a study of 97 patients with advancedHFrEF, RV exercise contractile reserve and RV-to-PCcoupling response to maximal exercise wereanalyzed through the relationships of systolic pul-monary arterial pressure (sPAP) to tricuspid annularpeak systolic excursion (TAPSE) and sPAP to CO usingstress echocardiography and CPET. Categorizationinto 3 groups based on TAPSE at rest$16 mm (group A,n ¼ 60) and patients with TAPSE at rest <16 mm,who were further divided into 2 subgroups (group B,n ¼ 19; group C, TAPSE <15.5 mm, n ¼ 18) according towhether their respective median TAPSE was higher orlower than 15.5 mm at peak exercise. Group B, atvariance with group C, showed an upward shift of theTAPSE versus sPAP relationship and some degree offavorable coupling adaptation during exercise. Thus,severely impaired RV function at rest may still beassociated with the capacity to improve RV-to-PCcoupling during exertion in a proportion of the
patients with HFrEF (87). Interestingly, the worstRV-to-PC coupling pattern was associated with thehighest rate of exercise ventilation inefficiency. Thisanalysis appears useful for unmasking different rightheart phenotypes not detectable with rest evaluation.
Most recent findings suggest that impaired LAdynamics, estimated by LA strain response duringmaximal exercise and during the recovery phase,plays a central hemodynamic role in triggering RV toPC uncoupling and ventilatory inefficiency, especiallywhen LV systolic function is reduced (85).HF WITH PRESERVED EJECTION FRACTION. HFpEFis a syndrome whose diagnostic process and limitedtherapeutic options remain major challenges (94).The expanding body of published reports on CPETimaging in this syndrome is based on several points:to uncover unexplained dyspnea and suspectedHFpEF; to confirm HFpEF diagnosis in subjects notmeeting the criteria required at rest; and to stratifyCV risk once a true diagnosis is established.
Recently, the American Society of Echocardiogra-phy/European Association of Cardiovascular Imagingrecommendations on diastolic function evaluationadvocated the use of the exercise E/e0 ratio to detectdiastolic dysfunction (95) and, for the past severalyears, changes in E/e0 were taken as a reference tointerpret unexplained dyspnea and suspected HFpEF(96,97). In a study by Nedelikovic et al. (98), per-formed in 87 patients with dyspnea unexplained byexercise and hypertension, gas exchange and Doppleranalysis led to the ultimate diagnosis of HFpEF in theminority of patients presenting with a combinationof E/e0 >15 at peak exercise, along with an elevatedVE/VCO2 slope.
A parallel number of observations have focused onhow exercise E/e0 may add to the clinical follow-up ofestablished HFpEF, especially looking at the associ-ated changes in pulmonary pressure during effort(99,100). Interestingly, CPET imaging with immedi-ately post-exercise echocardiographic assessment hasdocumented that in about 1 of 3 patients with HFpEF,exercise elevation of LV filling pressure (E/e0
EXE >13)can be absent, but associated with reduced contrac-tile reserve and ventriculoarterial coupling, as well aswith a mild degree of functional impairment (101).However, a similar approach has shown that peakE/e0 >15 occurred in 9% of hypertensive patientswith exertional dyspnea and normal resting LVfunction, being associated with lower peak VO2 andsignificantly impaired ventilator efficiency (higherVE/VCO2), compared with patients with normalexercise E/e0 (98).
The intrinsic value of exercise echocardiographyhas been recently confirmed in an elegant

FIGURE 4 Example of CPET Imaging Applied to Different Cardiac Diseases
The figure shows the semirecumbent approach (center), allowing for simultaneous echocardiography and expired-gas analysis. The yellow table on the right lists the
main parameters provided by exercise echocardiography; the disease-specific tables indicate prognostic parameters to collect during the test. The blue table on the
left lists the main CPET parameters; the “red flags” table (left) points out CPET pathological patterns with prognostic impact. The 4 panels in blue depict cases of iCPET
with the main CPET (left blue frame) and echocardiographic (right red frames) findings. (Upper left) A case of HFrEF due to post-ischemic LV dysfunction with a very
abnormal functional phenotype; CPET frames show pronounced exercise oscillatory ventilation and severe impairment of ventilatory efficiency; echocardiographic
frames show end-diastolic and end-systolic apical 4-chamber views with apical aneurysmatic evolution and severely reduced ejection fraction, transmitral pulsed wave
Doppler, and annular TDI displaying grade III diastolic dysfunction and transtricuspid continuous wave Doppler demonstrating severe pulmonary hypertension at rest
and during exercise. (Upper right) A case of HCM with preserved functional phenotype, despite the evidence of severe left ventricular outflow obstruction; CPET
frames show normal ventilatory response; echocardiographic frames show left ventricular outflow tract continuous wave Doppler demonstrating severe rest dynamic
obstruction, enhanced by the Valsalva maneuver and by post-exercise period (when afterload is decreasing, but adrenergic inotropic drive is still present). (Bottom
right) A case of HFpEF with typical abnormal functional phenotype characterized by chronotropic incompetence; CPET frames show the flattening of the DVO2/DWR
relationship, expression of blunted cardiac output during exercise, and the reduced chronotropic response related to VO2 consumption; echocardiographic frames show
transmitral pulsed wave Doppler and annular TDI displaying rest grade II diastolic dysfunction with worsening during exercise, transtricuspid continuous wave
Doppler demonstrating a borderline rest gradient with a severe exercise-induced increase, and left ventricular outflow tract pulsed wave Doppler evidencing a slight
increase of flow during exercise, consistent with abnormal stroke volume reserve. (Bottom left) A case of moderate left ventricular systolic dysfunction characterized by
exercise-induced mitral regurgitation with mild exercise oscillatory ventilation. CPET frames show mild exercise oscillatory ventilation with preserved ventilatory
efficiency; echocardiographic frames show rest and exercise midsystolic color Doppler apical 4-chamber views with severe exercise-induced mitral regurgitation and
transtricuspid continuous wave Doppler demonstrating normal rest gradient with abnormal exercise-induced increase, reflecting dynamic pulmonary hypertension.
AT ¼ anaerobic threshold; AVA ¼ aortic valve area; CO2 ¼ carbon dioxide; EDA ¼ end-diastolic area; EDV ¼ end-diastolic volume; ERO ¼ effective regurgitant orifice;
ESA ¼ end-systolic area; ESV ¼ end-systolic volume; EXE ¼ exercise; FAC ¼ fractional area change; GLS ¼ global longitudinal strain; HCM ¼ hypertrophic cardio-
myopathy; iCPET ¼ invasive cardiopulmonary exercise testing; iEDV ¼ indexed end-diastolic volume; iESV ¼ indexed end-systolic volume; LVEF ¼ left ventricular
ejection fraction; MPG ¼ mean pressure gradient; MG ¼ mean gradient; MR ¼ mitral regurgitation; PG ¼ peak gradient; RegVol ¼ mitral regurgitant volume;
RER ¼ respiratory exchange ratio; RV ¼ right ventricular; SPAP ¼ systolic pulmonary artery pressure; SV ¼ systolic volume; TAPSE ¼ tricuspid annular plane systolic
excursion; TDI ¼ tissue Doppler imaging; WMSI ¼ wall motion score index; other abbreviations as in Figures 1 to 3.
J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1631

Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1632
simultaneous invasive and echocardiographic studyreporting increased sensitivity, but compromisedspecificity of guideline-recommended use of theexercise E/e0 ratio (77), proposing a screening role ofexercise echocardiography aimed at ruling out thepresence of HF.
VALVULAR DISEASES. Exercise echocardiography isextensively used for the evaluation of valvular dis-eases, as recently stated in the European Associationof Cardiovascular Imaging/American Society ofEchocardiography recommendations (95). Specificprotocols and target parameters have been estab-lished according to the valve disease and the clinicalquestion (102). The main goal of physical stress is tomeasure the “valve reserve” (i.e., the entity ofexercise-induced worsening of valve disease) and thedirect pathophysiological consequences (i.e.,exercise-induced PH, LV transient systolic dysfunc-tion, increase in transvalvular gradients). The mainindication for testing patients with valvular disease isan unclear clinical presentation. Considering theadvanced age of people with valvular disease andtheir high prevalence of dyspnea (103), it is quitecommon to experience some difficulties in under-standing the origin of self-reported dyspnea. In thedecision process for surgical treatment, what appearspivotal is the recognition of how much symptoms arerelated to the valve disease or reflective of otherconditions, in order to optimize surgical timing. Ofnote, CPET imaging was recently used in patientswith rheumatic mitral stenosis, providing evidencethat functional limitation has a complex origin.Restrictive lung function, chronotropic incompe-tence, limited stroke volume reserve, and peripheralfactors equally contributed to reduce ability to exer-cise (104). Interestingly, patients with attenuatedfunctional responses showed the expected exercise-induced PH; however, this was not the mainlimiting factor. A similar combined approach has beenused in functional MR to demonstrate that exercise-induced severe MR limits patients with HFrEF,mainly causing exercise PH. The rationale for usingCPET imaging in valvular disease is strong; however,systematic data are still lacking and future in-vestigations are desirable for defining surgical risk,especially in the assessment of complex conditions,such as paradoxical low-flow–low-gradient severeaortic stenosis (105).
HYPERTROPHIC CARDIOMYOPATHY. Hypertrophiccardiomyopathy (HCM) is commonly associated withexercise intolerance, and CPET analysis is helpful forimproving prognostic stratification (106). Mechanismsunderlying abnormal gas exchange during exercise
can differ according to the predominant echocardio-graphic phenotype (107). CPET imaging allows theidentification of LV outflow obstruction and diastolicdysfunction assessment during exercise, as well asobjective measurement of functional limitations.In 156 patients with HCM evaluated with both CPETand noninvasive hemodynamic assessment, a highprevalence of exercise intolerance and ventilatoryinefficiency has been reported (108). Impaired peakVO2 (<80% of predicted) was associated with peakcardiac index, age, male sex, and RV end-diastolicarea, whereas ventilatory inefficiency (VE/VCO2 >34)was related to E/e0 and to indexed LA volume. Bothfunctional parameters were predictive of increasedrisk of major events in the short-term follow-up.
The role of diastolic dysfunction as a limiting factorof functional response has been reinforced by a recentpaper using iCPET imaging in 197 patients with HCM(109). Multivariate analysis showed that LV obstruc-tion, LA dilation, and especially rest or latentdiastolic dysfunction were the main determinants ofexercise intolerance.
According to the European guidelines (110), CPEThas a Class IIa indication in patients with HCM,irrespective of symptoms reported, and a Class Iaindication when consistent symptoms are present.Simultaneous exercise echocardiography has theadvantage of evaluating LV outflow tract obstructionand weighing all potential causes of exercise intoler-ance, such as diastolic dysfunction, dynamic MR, andPH. An additive value of CPET imaging has beensuggested for monitoring therapeutic response toseptal reduction, looking at the linearity of the DVO2/DWR relationship, which can be flattened in case ofsevere obstruction and normalize after septal reduc-tion (111).SUSPECTED OR CONFIRMED PH. CPET imaging andexercise echocardiography have independent, spe-cific roles in the diagnostic work-up, functionalevaluation, and clinical management of patients withconfirmed PH, irrespective of disease origin (95).Nonetheless, the combination of both tests in asingle-step evaluation has the advantage of confirm-ing suspected PH, making an early diagnosis, identi-fying secondary causes of PH, and improving overallpatient characterization. Systolic pulmonary pressureduring exercise is one of the most important variablesto collect during exercise echocardiography in severalclinical settings because it reflects the main mecha-nism of effort intolerance. Nonetheless, in thecontext of Group 1 or PAH, the role of exercise echo-cardiography in the diagnostic work-up is stilldebated and it is not recommended for diagnosis andclinical purposes (112).

J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1633
The role of CPET imaging has been validated inseveral conditions for determining exercise-inducedPH, however no prospective studies have tested theincremental value of this combined approach in thediagnostic work-up of PAH.
CONCLUSIONS
CPET now has a definitive place in the armamen-tarium of the practicing clinician for the evaluation ofcardiopulmonary disorders, primarily HF. It providesa thorough assessment of the integrative multiorganphysiological response to exercise. A revival of
invasive CPET and introduction of CPET imaging havenow extended the amount of pathophysiologicaland clinical information, providing new insights insystemic and pulmonary hemodynamics, along withdirect knowledge of cardiac, valve, and functionaldata.
ADDRESS FOR CORRESPONDENCE: Dr. Marco Guazzi,University of Milano, Department of Biomedical Sciencesfor Health, Heart Failure Unit, University CardiologyDepartment, IRCCS Policlinico San Donato, Piazza E.Malan 2, 20097 San Donato Milanese, Milan, Italy.E-mail: [email protected].
RE F E RENCE S
1. Guazzi M, Adams V, Conraads V, et al. EACPR/AHA Scientific Statement. Clinical recommenda-tions for cardiopulmonary exercise testing dataassessment in specific patient populations. Circu-lation 2012;126:2261–74.
2. Guazzi M, Arena R, Halle M, Piepoli MF, Myers J,Lavie CJ. 2016 focused update: clinical recom-mendations for cardiopulmonary exercise testingdata assessment in specific patient populations.Circulation 2016;133:e694–711.
3. Barron A, Dhutia N, Mayet J, Hughes AD,Francis DP, Wensel R. Test-retest repeatability ofcardiopulmonary exercise test variables in patientswith cardiac or respiratory disease. Eur J PrevCardiol 2014;21:445–53.
4. Skalski J, Allison TG, Miller TD. The safety ofcardiopulmonary exercise testing in a populationwith high-risk cardiovascular diseases. Circulation2012;126:2465–72.
5. Weber KT, Kinasewitz GT, Janicki JS,Fishman AP. Oxygen utilization and ventilationduring exercise in patients with chronic cardiacfailure. Circulation 1982;65:1213–23.
6. Mancini DM, Eisen H, Kussmaul W, Mull R,Edmunds LH Jr., Wilson JR. Value of peak exerciseoxygen consumption for optimal timing of cardiactransplantation in ambulatory patients with heartfailure. Circulation 1991;83:778–86.
7. Osada N, Chaitman BR, Miller LW, et al.Cardiopulmonary exercise testing identifies lowrisk patients with heart failure and severelyimpaired exercise capacity considered forheart transplantation. J Am Coll Cardiol 1998;31:577–82.
8. Chomsky DB, Lang CC, Rayos GH, et al.Hemodynamic exercise testing. A valuable tool inthe selection of cardiac transplantation candi-dates. Circulation 1996;94:3176–83.
9. Lim HS, Theodosiou M. Exercise ventilatoryparameters for the diagnosis of reactive pulmo-nary hypertension in patients with heart failure.J Card Fail 2014;20:650–7.
10. Agostoni P, Corrà U, Cattadori G, et al., MECKIScore Research Group. Metabolic exercise testdata combined with cardiac and kidney indexes,the MECKI score: a multiparametric approach to
heart failure prognosis. Int J Cardiol 2013;167:2710–8.
11. Levy WC, Aaronson KD, Dardas TF, Williams P,Haythe J, Mancini D. Prognostic impact of theaddition of peak oxygen consumption to theSeattle Heart Failure Model in a transplant referralpopulation. J Heart Lung Transplant 2012;31:817–24.
12. Lund LH, Aaronson KD, Mancini DM. Validationof peak exercise oxygen consumption and theHeart Failure Survival Score for serial risk stratifi-cation in advanced heart failure. Am J Cardiol2005;95:734–41.
13. Balady GJ, Arena R, Sietsema K, et al., Councilon Epidemiology and Prevention, Council onPeripheral Vascular Disease, InterdisciplinaryCouncil on Quality of Care and OutcomesResearch, American Heart Association Exercise,Cardiac Rehabilitation, and Prevention Committeeof the Council on Clinical Cardiology. Clinician’sguide to cardiopulmonary exercise testing inadults: a scientific statement from the AmericanHeart Association. Circulation 2010;122:191–225.
14. Redfield MM, Chen HH, Borlaug BA, et al.,RELAX Trial. Effect of phosphodiesterase-5 inhi-bition on exercise capacity and clinical status inheart failure with preserved ejection fraction: arandomized clinical trial. JAMA 2013;309:1268–77.
15. Zamani P, Rawat D, Shiva-Kumar P, et al.Effect of inorganic nitrate on exercise capacity inheart failure with preserved ejection fraction.Circulation 2015;131:371–80; discussion 380.
16. Swank AM, Horton J, Fleg JL, et al. Modestincrease in peak VO2 is related to better clinicaloutcomes in chronic heart failure patients: resultsfrom heart failure and a controlled trial to inves-tigate outcomes of exercise training. Circ HeartFail 2012;5:579–85.
17. Dunlay SM, Allison TG, Pereira NL. Changes incardiopulmonary exercise testing parametersfollowing continuous flow left ventricular assistdevice implantation and heart transplantation.J Card Fail 2014;20:548–54.
18. Chaudhry S, Kumar N, Behbahani H, et al.Abnormal heart-rate response during cardiopul-monary exercise testing identifies cardiacdysfunction in symptomatic patients with
non-obstructive coronary artery disease. Int JCardiol 2017;228:114–21.
19. Barber NJ, Ako EO, Kowalik GT, et al. Magneticresonance-augmented cardiopulmonary exercisetesting: comprehensively assessing exerciseintolerance in children with cardiovascular disease.Circ Cardiovasc Imaging 2016;9:e005282.
20. Bandera F, Generati G, Pellegrino M, et al.Mitral regurgitation in heart failure: insights fromCPET combined with exercise echocardiography.Eur Heart J Cardiovasc Imaging 2017;18:296–303.
21. Coats CJ, Rantell K, Bartnik A, et al. Cardio-pulmonary exercise testing and prognosis inhypertrophic cardiomyopathy. Circ Heart Fail2015;8:1022–31.
22. Charalampopoulos A, Gibbs JS, Davies RJ,et al. Exercise physiological responses to drugtreatments in chronic thromboembolic pulmonaryhypertension. J Appl Physiol (1985) 2016;121:623–8.
23. Guazzi M, Cahalin LP, Arena R. Cardiopulmo-nary exercise testing as a diagnostic tool for thedetection of left-sided pulmonary hypertension inheart failure. J Card Fail 2013;19:461–7.
24. Wasserman K. Coupling of external to cellularrespiration during exercise: the wisdom of thebody revisited. Am J Physiol 1994;266:E519–39.
25. Sullivan MJ, Knight JD, Higginbotham MB,Cobb FR. Relation between central and peripheralhemodynamics during exercise in patients withchronic heart failure. Muscle blood flow is reducedwith maintenance of arterial perfusion pressure.Circulation 1989;80:769–81.
26. Okonko DO, Mandal AK, Missouris CG, Poole-Wilson PA. Disordered iron homeostasis in chronicheart failure: prevalence, predictors, and relationto anemia, exercise capacity, and survival. J AmColl Cardiol 2011;58:1241–51.
27. Agostoni P, Wasserman K, Perego GB, et al.Oxygen transport to muscle during exercise inchronic congestive heart failure secondary toidiopathic dilated cardiomyopathy. Am J Cardiol1997;79:1120–4.
28. Esposito F, Mathieu-Costello O, Shabetai R,Wagner PD, Richardson RS. Limited maximalexercise capacity in patients with chronic heart
Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1634
failure: partitioning the contributors. J Am CollCardiol 2010;55:1945–54.
29. Stringer WW, Hansen JE, Wasserman K. Car-diac output estimated noninvasively from oxygenuptake during exercise. J Appl Physiol (1985)1997;82:908–12.
30. Wagner PD. Muscle O2 transport and O2
dependent control of metabolism. Med Sci SportsExerc 1995;27:47–53.
31. Boushel R, Gnaiger E, Calbet JA, et al. Musclemitochondrial capacity exceeds maximal oxygendelivery in humans. Mitochondrion 2011;11:303–7.
32. Abramov D, Cohen RS, Katz SD, Mancini D,Maurer MS. Comparison of blood volume charac-teristics in anemic patients with low versuspreserved left ventricular ejection fractions. Am JCardiol 2008;102:1069–72.
33. Dhakal BP, Malhotra R, Murphy RM, et al.Mechanisms of exercise intolerance in heart failurewith preserved ejection fraction: the role ofabnormal peripheral oxygen extraction. Circ HeartFail 2015;8:286–94.
34. Agostoni P, Corrà U, Cattadori G, et al., MECKIScore Research Group. Prognostic value of inde-terminable anaerobic threshold in heart failure.Circ Heart Fail 2013;6:977–87.
35. Poole DC, Hirai DM, Copp SW, Musch TI.Muscle oxygen transport and utilization in heartfailure: implications for exercise (in)tolerance. AmJ Physiol Heart Circ Physiol 2012;302:H1050–63.
36. Cohen-Solal A, Tabet JY, Logeart D,Bourgoin P, Tokmakova M, Dahan M. A non-invasively determined surrogate of cardiac power(’circulatory power’) at peak exercise is a powerfulprognostic factor in chronic heart failure. EurHeart J 2002;23:806–14.
37. Agostoni P, Pellegrino R, Conca C, Rodarte JR,Brusasco V. Exercise hyperpnea in chronic heartfailure: relationships to lung stiffness and expira-tory flow limitation. J Appl Physiol (1985) 2002;92:1409–16.
38. Barron A, Francis DP, Mayet J, et al. Oxygenuptake efficiency slope and breathing reserve, notanaerobic threshold, discriminate betweenpatients with cardiovascular disease over chronicobstructive pulmonary disease. J Am Coll CardiolHF 2016;4:252–61.
39. Lewis GD, Murphy RM, Shah RV, et al. Pul-monary vascular response patterns during exercisein left ventricular systolic dysfunction predict ex-ercise capacity and outcomes. Circ Heart Fail 2011;4:276–85.
40. Guazzi M, Dixon D, Labate V, et al. RV con-tractile function and its coupling to pulmonarycirculation in heart failure with preserved ejectionfraction: stratification of clinical phenotypes andoutcomes. J Am Coll Cardiol Img 2017 Apr 7[E-pub ahead of print].
41. Guazzi M, Reina G, Tumminello G, Guazzi MD.Exercise ventilation inefficiency and cardiovascularmortality in heart failure: the critical independentprognostic value of the arterial CO2 partial pres-sure. Eur Heart J 2005;26:472–80.
42. Kee K, Stuart-Andrews C, Ellis MJ, et al.Increased dead space ventilation mediates
reduced exercise capacity in systolic heart failure.Am J Respir Crit Care Med 2016;193:1292–300.
43. Hachamovitch R, Brown HV, Rubin SA. Respi-ratory and circulatory analysis of CO2 outputduring exercise in chronic heart failure. Circulation1991;84:605–12.
44. Olson TP, Joyner MJ, Johnson BD. Influence oflocomotor muscle metaboreceptor stimulation onthe ventilatory response to exercise in heartfailure. Circ Heart Fail 2010;3:212–9.
45. Van Iterson EH, Johnson BD, Borlaug BA,Olson TP. Physiologic dead space and arterialcarbon dioxide contribution to exercise ventilatoryinefficiency in patients with reduced or preservedejection fraction. Eur J Heart Fail 2017. In press.
46. Elbehairy AF, Ciavaglia CE, Webb KA, et al.,Canadian Respiratory Research Network. Pulmo-nary gas exchange abnormalities in mild chronicobstructive pulmonary disease. Implications fordyspnea and exercise intolerance. Am J Respir CritCare Med 2015;191:1384–94.
47. Van Laethem C, Bartunek J, Goethals M,Nellens P, Andries E, Vanderheyden M. Oxygenuptake efficiency slope, a new submaximalparameter in evaluating exercise capacity inchronic heart failure patients. Am Heart J 2005;149:175–80.
48. Guazzi M. Treating exercise oscillatory venti-lation in heart failure: the detail that may matter.Eur Respir J 2012;40:1075–7.
49. Guazzi M, Raimondo R, Vicenzi M, et al.Exercise oscillatory ventilation may predict suddencardiac death in heart failure patients. J Am CollCardiol 2007;50:299–308.
50. Sun XG, Hansen JE, Beshai JF, Wasserman K.Oscillatory breathing and exercise gas exchangeabnormalities prognosticate early mortality andmorbidity in heart failure. J Am Coll Cardiol 2010;55:1814–23.
51. Vicenzi M, Deboeck G, Faoro V, Loison J,Vachiery JL, Naeije R. Exercise oscillatory ventila-tion in heart failure and in pulmonary arterialhypertension. Int J Cardiol 2016;202:736–40.
52. Guazzi M, Arena R, Pellegrino M, et al. Preva-lence and characterization of exercise oscillatoryventilation in apparently healthy individuals atvariable risk for cardiovascular disease: a sub-analysis of the EURO-EX trial. Eur J Prev Cardiol2016;23:328–34.
53. Belardinelli R, Lacalaprice F, Carle F, et al.Exercise-induced myocardial ischaemia detectedby cardiopulmonary exercise testing. Eur Heart J2003;24:1304–13.
54. Popovic D, Martic D, Djordjevic T, et al.Oxygen consumption and carbon-dioxide recoverykinetics in the prediction of coronary artery dis-ease severity and outcome. Int J Cardiol 2017 Jun28 [E-pub ahead of print].
55. Balady GJ, Ades PA, Bittner VA, et al. Referral,enrollment, and delivery of cardiac rehabilitation/secondary prevention programs at clinical centersand beyond: a presidential advisory from theAmerican Heart Association. Circulation 2011;124:2951–60.
56. Ponikowski P, Voors AA, Anker SD, et al. 2016ESC guidelines for the diagnosis and treatment of
acute and chronic heart failure: the Task Force forthe diagnosis and treatment of acute and chronicheart failure of the European Society of Cardiology(ESC). Eur J Heart Fail 2016;18:891–975.
57. Mezzani A, Hamm LF, Jones AM, et al. Aerobicexercise intensity assessment and prescription incardiac rehabilitation: a joint position statement ofthe European Association for CardiovascularPrevention and Rehabilitation, the AmericanAssociation of Cardiovascular and PulmonaryRehabilitation and the Canadian Association ofCardiac Rehabilitation. Eur J Prev Cardiol 2013;20:442–67.
58. Reed JL, Blais AZ, Keast ML, Pipe AL, Reid RD.Performance of fixed heart rate increment targetsof 20 vs 30 beats per minute for exercise reha-bilitation prescription in outpatients with heartfailure. Can J Cardiol 2017;33:777–84.
59. Yancy CW, Jessup M, Bozkurt B, et al. 2013ACCF/AHA guideline for the management of heartfailure: a report of the American College ofCardiology Foundation/American Heart Associa-tion Task Force on Practice Guidelines. J Am CollCardiol 2013;62:e147–239.
60. Arena R, Guazzi M, Cahalin LP, Myers J.Revisiting cardiopulmonary exercise testingapplications in heart failure: aligning evidencewith clinical practice. Exerc Sport Sci Rev 2014;42:153–60.
61. Guazzi M, Naeije R. Pulmonary hypertension inheart failure: pathophysiology, pathobiology, andemerging clinical perspectives. J Am Coll Cardiol2017;69:1718–34.
62. Klaassen SHC, Liu LCY, Hummel YM, et al.Clinical and hemodynamic correlates and prog-nostic value of VE/VCO2 slope in patients withheart failure with preserved ejection fraction andpulmonary hypertension. J Card Fail 2017 Jul 20[E-pub ahead of print].
63. Bhatia V, Bhatia R, Mathew B. Angiotensinreceptor blockers in congestive heart failure:evidence, concerns, and controversies. Cardiol Rev2005;13:297–303.
64. Guazzi M, Arena R. The impact of pharmaco-therapy on the cardiopulmonary exercise testresponse in patients with heart failure: a minireview. Curr Vasc Pharmacol 2009;7:557–69.
65. Agostoni P, Apostolo A, Cattadori G, et al.Effects of beta-blockers on ventilation efficiencyin heart failure. Am Heart J 2010;159:1067–73.
66. Guazzi M, Myers J, Peberdy MA, Bensimhon D,Chase P, Arena R. Ventilatory efficiency anddyspnea on exertion improvements are related toreduced pulmonary pressure in heart failurepatients receiving sildenafil. Int J Cardiol 2010;144:410–2.
67. Guazzi M, Vicenzi M, Arena R. Phosphodies-terase 5 inhibition with sildenafil reverses exerciseoscillatory breathing in chronic heart failure: along-term cardiopulmonary exercise testingplacebo-controlled study. Eur J Heart Fail 2012;14:82–90.
68. Hussain I, Mohammed SF, Forfia PR, et al.Impaired right ventricular-pulmonary arterialcoupling and effect of sildenafil in heart failurewith preserved ejection fraction: an ancillaryanalysis from the Phosphodiesterase-5 Inhibition

J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7 Guazzi et al.S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6 Cardiopulmonary Exercise Testing
1635
to Improve Clinical Status And Exercise Capacity inDiastolic Heart Failure (RELAX) trial. Circ Heart Fail2016;9:e002729.
69. Kitzman DW, Hundley WG, Brubaker PH, et al.A randomized double-blind trial of enalapril inolder patients with heart failure and preservedejection fraction: effects on exercise tolerance andarterial distensibility. Circ Heart Fail 2010;3:477–85.
70. Parthasarathy HK, Pieske B, Weisskopf M,et al. A randomized, double-blind, placebo-controlled study to determine the effects ofvalsartan on exercise time in patients with symp-tomatic heart failure with preserved ejectionfraction. Eur J Heart Fail 2009;11:980–9.
71. Pal N, Sivaswamy N, Mahmod M, et al. Effectof selective heart rate slowing in heart failure withpreserved ejection fraction. Circulation 2015;132:1719–25.
72. O’Neill JO, Young JB, Pothier CE, Lauer MS.Peak oxygen consumption as a predictor of deathin patients with heart failure receiving beta-blockers. Circulation 2005;111:2313–8.
73. Mehra MR, Canter CE, Hannan MM, et al.,International Society for Heart Lung Trans-plantation (ISHLT) Infectious Diseases, Pediatricand Heart Failure and Transplantation Councils.The 2016 International Society for Heart LungTransplantation listing criteria for heart trans-plantation: a 10-year update. J Heart LungTransplant 2016;35:1–23.
74. Arena R, Myers J, Abella J, et al. Developmentof a ventilatory classification system in patientswith heart failure. Circulation 2007;115:2410–7.
75. Guazzi M, Boracchi P, Arena R, et al. Devel-opment of a cardiopulmonary exercise prognosticscore for optimizing risk stratification in heartfailure: the (P)e(R)i(O)dic (B)reathing during(E)xercise (PROBE) study. J Card Fail 2010;16:799–805.
76. Arena R, Myers J, Guazzi M. Cardiopulmonaryexercise testing is a core assessment for patientswith heart failure. Congest Heart Fail 2011;17:115–9.
77. Obokata M, Kane GC, Reddy YN, Olson TP,Melenovsky V, Borlaug BA. Role of diastolic stresstesting in the evaluation for heart failure withpreserved ejection fraction: a simultaneousinvasive-echocardiographic study. Circulation2017;135:825–38.
78. Huang W, Resch S, Oliveira RK, Cockrill BA,Systrom DM, Waxman AB. Invasive cardiopulmo-nary exercise testing in the evaluation of unex-plained dyspnea: insights from a multidisciplinarydyspnea center. Eur J Prev Cardiol 2017;24:1190–9.
79. Lewis GD, Bossone E, Naeije R, et al. Pulmo-nary vascular hemodynamic response to exercisein cardiopulmonary diseases. Circulation 2013;128:1470–9.
80. Borlaug BA, Nishimura RA, Sorajja P, Lam CS,Redfield MM. Exercise hemodynamics enhancediagnosis of early heart failure with preservedejection fraction. Circ Heart Fail 2010;3:588–95.
81. Dorfs S, Zeh W, Hochholzer W, et al. Pulmo-nary capillary wedge pressure during exercise and
long-term mortality in patients with suspectedheart failure with preserved ejection fraction. EurHeart J 2014;35:3103–12.
82. Berry NC, Manyoo A, Oldham WM, et al.Protocol for exercise hemodynamic assessment:performing an invasive cardiopulmonary exercisetest in clinical practice. Pulm Circ 2015;5:610–8.
83. Fu Q, Vangundy TB, Galbreath MM, et al.Cardiac origins of the postural orthostatic tachy-cardia syndrome. J Am Coll Cardiol 2010;55:2858–68.
84. Chatterjee NA, Murphy RM, Malhotra R, et al.Prolonged mean VO2 response time in systolicheart failure: an indicator of impaired rightventricular-pulmonary vascular function. CircHeart Fail 2013;6:499–507.
85. Sugimoto T, Bandera F, Generati G,Alfonzetti E, Bussadori C, Guazzi M. Left atrialfunction dynamics during exercise in heart failure:pathophysiological implications on the right heartand exercise ventilation inefficiency. J Am CollCardiol Img 2016 Dec 12 [E-pub ahead of print].
86. Claessen G, La Gerche A. Pulmonary vascularfunction during exercise: progressing towardroutine clinical use. Circ Cardiovasc Imaging 2017;10:006326.
87. Guazzi M, Villani S, Generati G, et al. Rightventricular contractile reserve and pulmonarycirculation uncoupling during exercise challenge inheart failure: pathophysiology and clinical phe-notypes. J Am Coll Cardiol HF 2016;4:625–35.
88. Bandera F, Generati G, Pellegrino M, et al.Role of right ventricle and dynamic pulmonaryhypertension on determining DVO2/DWork Rateflattening: insights from cardiopulmonary exercisetest combined with exercise echocardiography.Circ Heart Fail 2014;7:782–90.
89. Rozenbaum Z, Khoury S, Aviram G, et al.Discriminating circulatory problems from decon-ditioning: echocardiographic and cardiopulmonaryexercise test analysis. Chest 2017;151:431–40.
90. Shimiaie J, Sherez J, Aviram G, et al.Determinants of effort intolerance in patients withheart failure: combined echocardiography andcardiopulmonary stress protocol. J Am Coll CardiolHF 2015;3:803–14.
91. Hummel YM, Bugatti S, Damman K, et al.Functional and hemodynamic cardiac de-terminants of exercise capacity in patients withsystolic heart failure. Am J Cardiol 2012;110:1336–41.
92. Podolec P, Rubís P, Tomkiewicz-Pajak L,Kope�c G, Tracz W. Usefulness of the evaluation ofleft ventricular diastolic function changes duringstress echocardiography in predicting exercisecapacity in patients with ischemic heart failure.J Am Soc Echocardiogr 2008;21:834–40.
93. Grigioni F, Enriquez-Sarano M, Zehr KJ,Bailey KR, Tajik AJ. Ischemic mitral regurgitation:long-term outcome and prognostic implicationswith quantitative Doppler assessment. Circulation2001;103:1759–64.
94. Borlaug BA. Is HFpEF one disease or many?J Am Coll Cardiol 2016;67:671–3.
95. Lancellotti P, Pellikka PA, Budts W, et al. Theclinical use of stress echocardiography in non-
ischaemic heart disease: recommendations fromthe European Association of CardiovascularImaging and the American Society of Echocardi-ography. Eur Heart J Cardiovasc Imaging 2016;17:1191–229.
96. Meluzin J, Sitar J, Kristek J, et al. The roleof exercise echocardiography in the diagnosticsof heart failure with normal left ventricularejection fraction. Eur J Echocardiogr 2011;12:591–602.
97. Ha JW, Oh JK, Pellikka PA, et al. Diastolicstress echocardiography: a novel noninvasivediagnostic test for diastolic dysfunction using su-pine bicycle exercise Doppler echocardiography.J Am Soc Echocardiogr 2005;18:63–8.
98. Nedeljkovic I, Banovic M, Stepanovic J, et al.The combined exercise stress echocardiographyand cardiopulmonary exercise test for identifica-tion of masked heart failure with preserved ejec-tion fraction in patients with hypertension. Eur JPrev Cardiol 2016;23:71–7.
99. Donal E, Lund LH, Oger E, et al., KaRenInvestigators. Value of exercise echocardiographyin heart failure with preserved ejection fraction: asubstudy from the KaRen study. Eur Heart JCardiovasc Imaging 2016;17:106–13.
100. Shim CY, Kim SA, Choi D, et al. Clinicaloutcomes of exercise-induced pulmonary hyper-tension in subjects with preserved left ventricularejection fraction: implication of an increase in leftventricular filling pressure during exercise. Heart2011;97:1417–24.
101. Kosmala W, Rojek A, Przewlocka-Kosmala M,Mysiak A, Karolko B, Marwick TH. Contributions ofnondiastolic factors to exercise intolerance inheart failure with preserved ejection fraction. J AmColl Cardiol 2016;67:659–70.
102. Garbi M, Chambers J, Vannan MA,Lancellotti P. Valve stress echocardiography: apractical guide for referral, procedure, reporting,and clinical implementation of results from theHAVEC Group. J Am Coll Cardiol Img 2015;8:724–36.
103. Pedersen F, Mehlsen J, Raymond I, Atar D,Skjoldborg US, Hildebrandt PR. Evaluation ofdyspnoea in a sample of elderly subjects recruitedfrom general practice. Int J Clin Pract 2007;61:1481–91.
104. Laufer-Perl M, Gura Y, Shimiaie J, et al.Mechanisms of effort intolerance in patients withrheumatic mitral stenosis: combined echocardi-ography and cardiopulmonary stress protocol.J Am Coll Cardiol Img 2017;10:622–33.
105. Bandera F, Generati G, Pellegrino M, et al.Paradoxical low flow/low gradient aortic stenosis:can cardiopulmonary exercise test help in identi-fying it? Int J Cardiol 2016;203:37–9.
106. Magri D, Limongelli G, Re F, et al. Cardio-pulmonary exercise test and sudden cardiac deathrisk in hypertrophic cardiomyopathy. Heart 2016;102:602–9.
107. Maron BJ, Maron MS. Hypertrophic cardio-myopathy. Lancet 2013;381:242–55.
108. Finocchiaro G, Haddad F, Knowles JW,et al. Cardiopulmonary responses and prognosisin hypertrophic cardiomyopathy: a potential role

Guazzi et al. J A C C V O L . 7 0 , N O . 1 3 , 2 0 1 7
Cardiopulmonary Exercise Testing S E P T E M B E R 2 6 , 2 0 1 7 : 1 6 1 8 – 3 6
1636
for comprehensive noninvasive hemodynamicassessment. J Am Coll Cardiol HF 2015;3:408–18.
109. Re F, Zachara E, Avella A, et al. Dissectingfunctional impairment in hypertrophic cardiomy-opathy by dynamic assessment of diastolicreserve and outflow obstruction: a combinedcardiopulmonary-echocardiographic study. Int JCardiol 2017;227:743–50.
110. Elliott PM, Anastasakis A, Borger MA, et al.2014 ESC guidelines on diagnosis and management
of hypertrophic cardiomyopathy: the Task Force forthe Diagnosis and Management of HypertrophicCardiomyopathy of the European Society of Cardi-ology (ESC). Eur Heart J 2014;35:2733–79.
111. Bandera F, Generati G, Pellegrino M, Secchi F,Menicanti L, Guazzi M. Exercise gas exchangeanalysis in obstructive hypertrophic cardiomyop-athy before and after myectomy (cardiopulmonaryexercise test combined with exercise-echocardiography in HCM). Int J Cardiol 2015;178:282–3.
112. Galiè N, Humbert M, Vachiery JL, et al. 2015ESC/ERS guidelines for the diagnosis andtreatment of pulmonary hypertension: the JointTask Force for the Diagnosis and Treatment ofPulmonary Hypertension of the European Societyof Cardiology (ESC) and the European RespiratorySociety (ERS). Eur Heart J 2016;37:67–119.
KEY WORDS exercise, gas exchangeanalysis, heart failure, oxygen consumption