zsuzsanna arányi dept. of neurology semmelweis university
TRANSCRIPT

Zsuzsanna ArányiDept. of Neurology
Semmelweis University
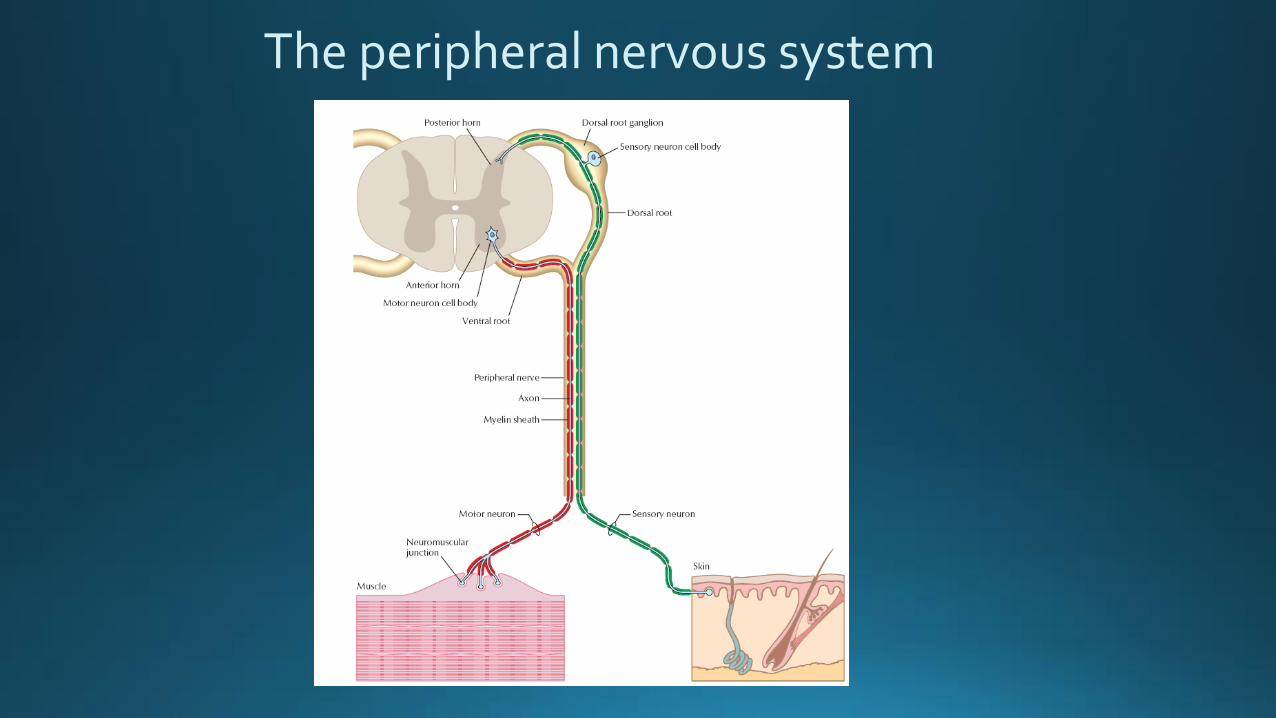
The peripheral nervous system

The peripheral nerve

Anatomy of the peripheral nerve
Elements of the peripheral nerve:– Axons and Schwann cells– Connective tissue elements– Blood vessels

Internal structure of the peripheral nerve
– Axons are organized into fascicles
– Fascicles are organized into fasciclegroups
– Continuous interchange of axonsbetween the fascicles: plexiformstructure
The ratio of fascicles versus connective tissue elements ranges between 25 and 75%

Internal architecture of peripheral nerves
▪ Plexiform structure
▪ Fibers to a specifictarget run together fromproximal to distal
▪ Plexiform structure is less evident distally

Myelin sheath and nerve conduction
Saltatory conduction of a myelinated nerve fiber
Myelin sheath:▪ Provides insulation to the nerve fiber▪ Increases fiber diameter▪ Allows for saltatory conduction▪ Dramatic increase of conduction velocity
▪ Myelinated fibers: 35-75 m/s▪ Unmyelinated fibers: 1-5 m/s
Node of Ranvier
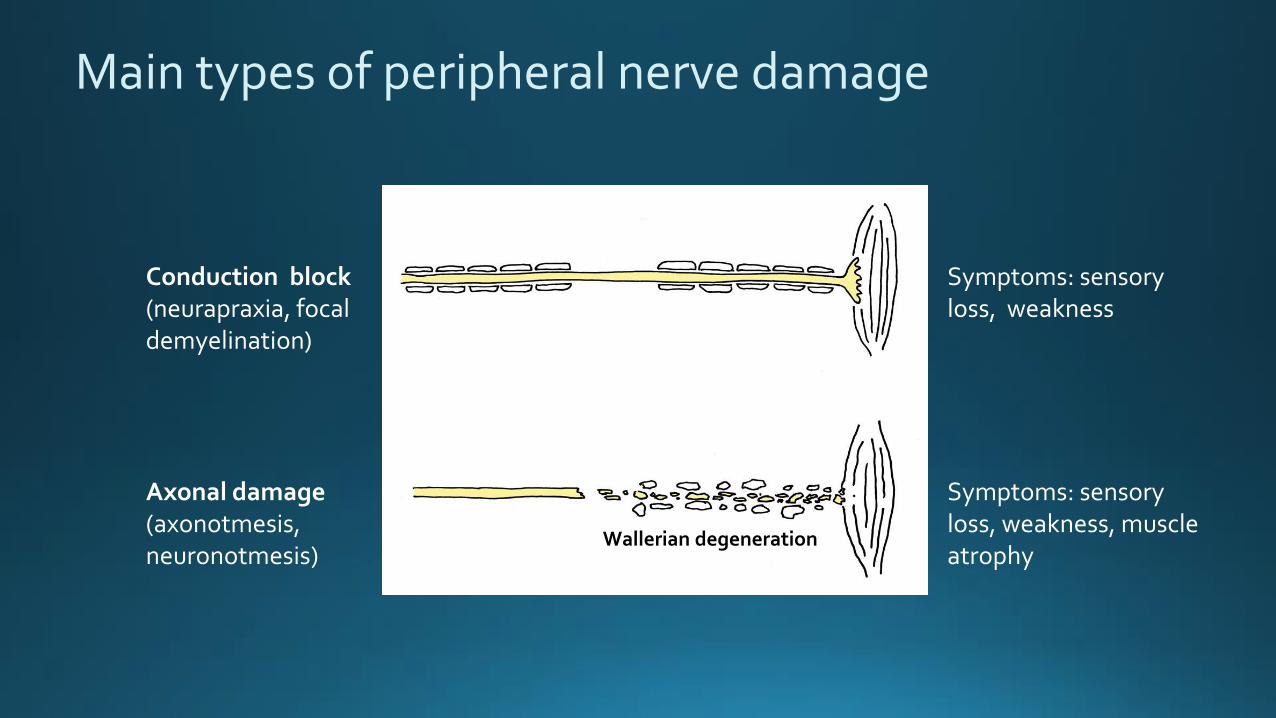
Main types of peripheral nerve damage
Conduction block(neurapraxia, focaldemyelination)
Axonal damage(axonotmesis,neuronotmesis)
Symptoms: sensoryloss, weakness
Symptoms: sensoryloss, weakness, muscleatrophy
Wallerian degeneration

Connective tissue elements of the peripheral nerve
– Mesoneurium - paraneurium
– Epineurium
– Perineurium
– Interfascicular fat
– Endoneurium
– Basal lamina

EpineuriumOuter layer surrounding the whole nerve (outerepineurium) and separating the fascicles / fascicle groups (inner epineurium)
Az ideg proximo-distalis tengelye
– Mainly consists of collagen fibers
– Wavy collagen fibers are diagonally organisedwith respect to the longitudinal axis of thenerve
– Contains elastin fibers as well
– Few cellular components
Relatively resistant to stretch!
outer
inner
group

Perineurium
Layer sorrounding individual fascicles
– Mainly consists of cellular components
– 8-18 alternating concentric layers of cellularlaminae and connective tissue (longitudinalcollagen)
– Tight junctions between flat, polygonal cells
Barrier function: blood-nerve barrier
Less resistant against resistant

Endoneurium
Layer surrounding individual axons (axon + Schwanncells + basal lamina)
Consists of two layers of collagen:
– Outer, longitudinally oriented layer
– Inner, looser layer connected to the basal lamina
Endoneural tubes (axons and Schwann cells removed)
Important role in axon regeneration

Basal lamina
Extracellular matrix surrounding the axon + Schwanncell complex
Non-myelinated axons
Crucial role in axon regeneration: guides theregenerating axon
– Produced by Schwann cells
– Matrix structure: laminin 2 + collagen IV polymers
– Non –myelinated axons: the basal laimnaproduced by one Schwann cell surrounds severalaxons

„Bands of Fontana”
Bands of Fontana: dark circular shadows seenon normal nerves under the microscope
– Cause: optical phenomenon caused by theundulating, spiral course of the axons
– Disappears under stretch
Peripheral nerves resist some degree of stretch
(15-20%?) without damage
„Elasticity” of nerves:
– Undulating, spiral course of axons
– Connective tissue elements, elasticity of the epineurium
Before stretch
Under stretch

Main types of peripheral nerve damage
Conduction block(neurapraxia, focaldemyelination)
Axonal damage(axonotmesis,neuronotmesis)
Symptom: loss of sensation, muscle weakness
Symptom: loss of sensation, muscle weakness and atrophy
Waller-f. degeneration

Symptoms and signs of peripheral nerve damage
Sensory fibers: sensory loss in the innervation area of theaffected nerve
Motor fibers: weakness / wasting of the muscles innervatedby the affected nerve
Autonomic: loss of sweating, dry skin, vasodilatation

Localization within the peripheral nervous system
Root / spinal segment?
Plexus?
Peripheral nerve?
Peripheral nerve – at what levelis the nerve damaged?

Localization within the peripheral nervous system
Root / spinal segment?
Plexus?
Peripheral nerve?
Peripheral nerve – at what levelis the nerve damaged?
Distribution of weakness / muscle atrophy and sensory loss
Requires mainly anatomicalknowledge

1. dorsal interosseous (FDI) brachioradial muscle
Check contraction (change in bulk) of the muscle tested: other muscleswith the same function may mask weakness of the muscle tested
Physical examination of muscle power▪ Spontaneous movements, gait▪ Contraction against resistance of the examiner
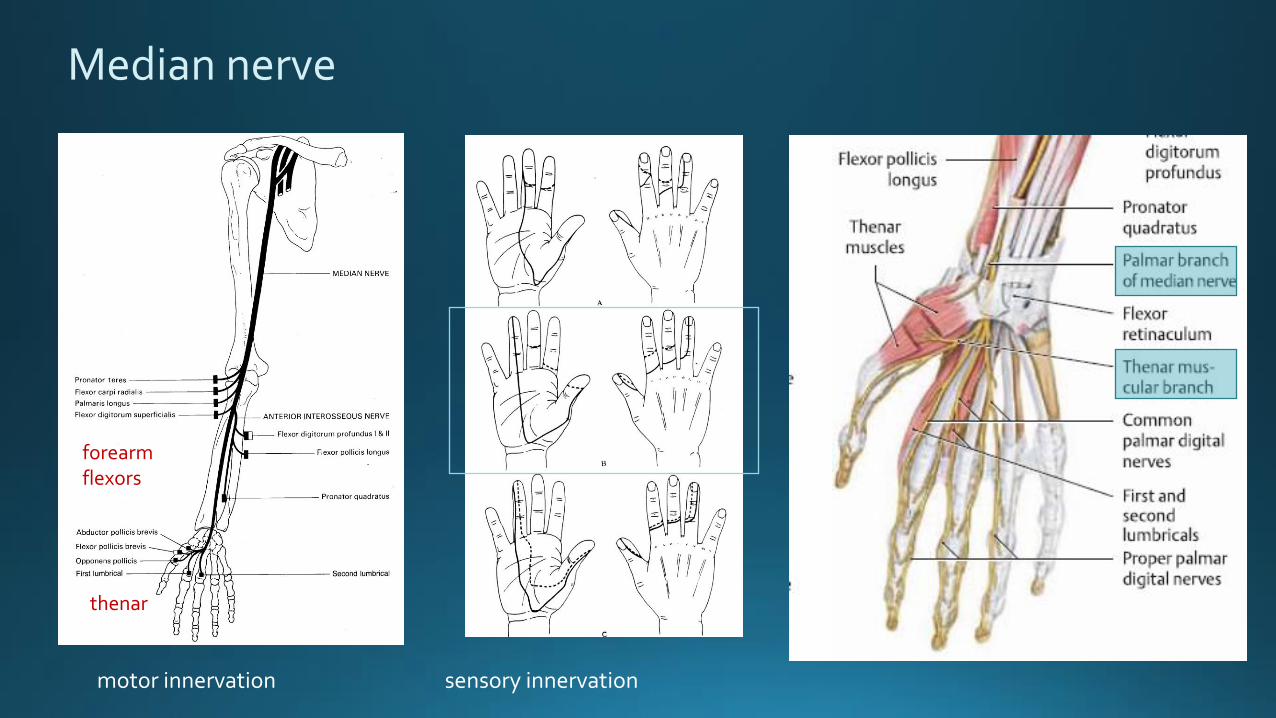
Median nerve
forearm flexors
thenar
motor innervation sensory innervation

Level of lesion within a peripheral nerve
Median nerve
▪ Motor and sensory branches branching distal tothe lesion are affected
▪ Innervation area proximal to the lesion is normal
▪ All muscles supplied by the given nerve shouldbe tested

Distal median nerve damage: carpal tunnel syndrome
Causes:▪ idiopathic▪ overuse (housewife, athletes, carpenters)▪ change of tunnel anatomy (arthritis, edema, fractures, etc.)▪ diabetes

Carpal tunnel syndrome
thenar atrophy
Loss of sensation: 1-4th fingers; superficial palmar branch (skin above the thenar) spared
Motor deficit: thenar; finger flexion spared

RadLun
Cap
PL
Flexorín
Thenar
Dist Prox
PQ
Normal median nerve in the carpal tunnel in longitudinal section
Carpal tunnel syndrome: nerve ultrasound

Rad
Lun
Flexor tendon
Median nerve in the carpal tunnel
CSA: 23.6 mm2 CSA: 6 mm2 CSA: 23.5 mm2
longitudinal
axial
Palm Carpal tunnel Wrist
Normal CSA: < 13 mm2

Video: from proximal to distal at the wrist
Carpal tunnel syndrome

Proximal median nerve lesion
▪ All muscles supplied by the median nerve are weak:‘oath hand’ when making a fist
▪ Loss of sensation in the whole innervation area
Median nerve lesion on the upper arm

Proximal median nerve lesion
▪ Loss of flexion in the distal phalanx of 1-2. fingers: FPL, FDP2 and PQ weakness
▪ No sensory loss
Anterior interosseous nerve (AIN) lesion

Pitfalls in the localization of focal nerve lesions
Fascicular lesion: proximal selective involvement of onenerve fascicle▪ clinically the lesion appears more distal
Length-dependent damage of axons▪ distal symptoms are more pronounced

PThu
PTuln
Brach
DistProx
Segmental enlargement of the AIN fascicle within the median nerve atthe elbow
PTPT
PT: pronator teres muscle
PTPT
axial
longitudinal
Sudden onset of AIN lesion (inflammatory neuropathy): selective involvement of AIN fascicle within themedian nerve at the elbow

Video: axial scanning of the median nerve at the elbow from distal to proximal
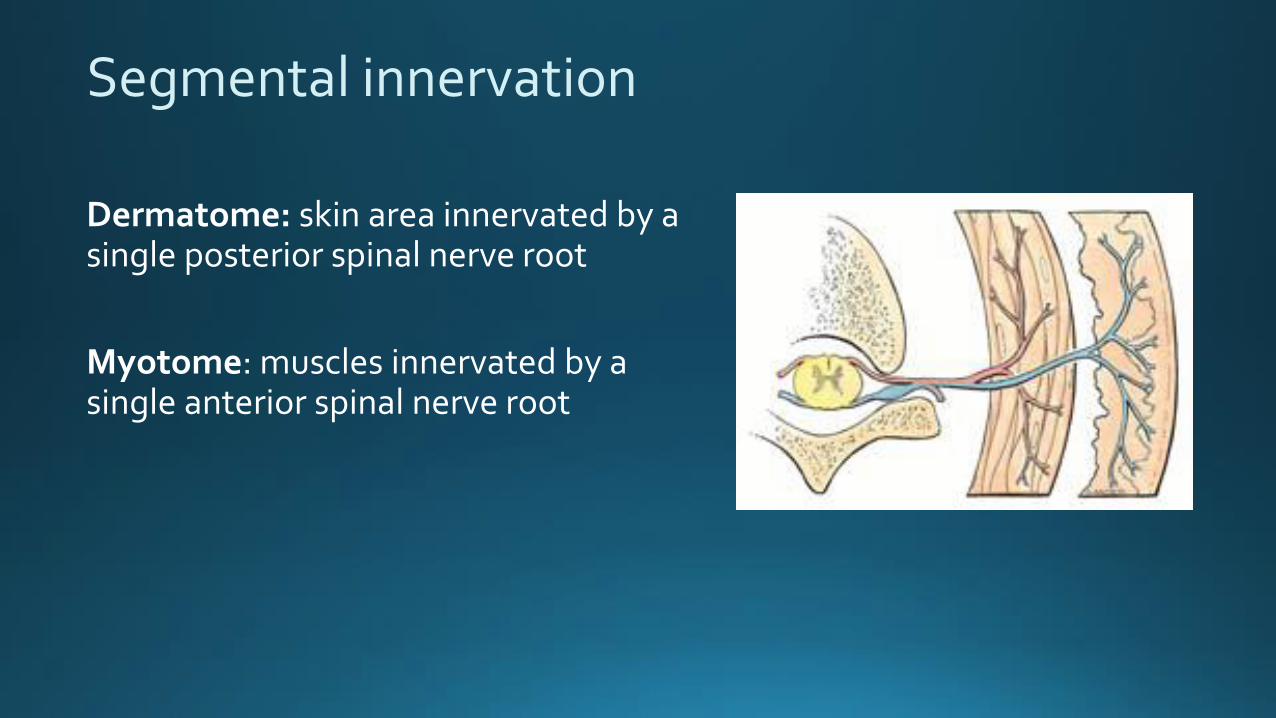
Segmental innervation
Dermatome: skin area innervated by a single posterior spinal nerve root
Myotome: muscles innervated by a single anterior spinal nerve root

Sensory innervation
Dermatomes Peripheral nerves

Myotomes

Segmental versus peripheral nerve damage
C8-Th1 segmental damage (e.g. spinal nerve root compression by discalherniation) versus ulnar nerve damage (e.g. cubital tunnel syndrome)
❑ Weakness and atrophy of smallhand muscles
❑ The atrophy of the first dorsalinterosseus muscle is the most conspicuous
❑ Claw hand
❑ Sensory loss on the 4-5th finger

Segmental versus peripheral nerve damage
C8-Th1 segmental damage (e.g. spinal nerve root compression by discalherniation) versus ulnar nerve damage (e.g. cubital tunnel syndrome)

Segmental versus peripheral nerve damage
C8-Th1 segmental damage versus Ulnar nerve damage
❑ Weakness / atrophy of ulnar innervatedsmall hand muscles: C8-Th1
❑ Sensory loss on the 4-5th finger
❑ Weakness / atrophy of ulnar innervatedsmall hand muscles: C8-Th1
❑ Sensory loss on the 4-5th finger (half of 4th finger)
❑ Weakness / atrophy of the thenar:median nerve – Th1
❑ Weakness / atrophy of extensorindicis proprius muscle:radial nerve – C8
❑ Sensory loss on the medial aspect of the forearm – Th1

Segmental versus peripheral nerve damage
L5 segmental damage (e.g. root compression caused by discal herniation) versus common peroneal nerve damage (e.g. compression at the fibular head)
❑ Weakness of dorsiflexion of the foot and toes(foot drop)
❑ Weakness of foot pronation
❑ Sensory loss: foot, great toe, lower leg

Segmental versus peripheral nerve damage
L5 segmental damage versus Common peroneal nerve damage
❑ Weakness / atrophy of peronealnerve innervated leg muscles(extensor and peroneal musclegroups: L5)
❑ Sensory loss: hallux (lower leg)
❑ Weakness / atrophy of peroneal nerveinnervated leg muscles (extensor and peroneal muscle groups:
❑ Sensory loss: dorsum of the foot, lateral aspect of the leg
❑ Weakness of tibial posterior muscle(supination of the foot): posteriortibial nerve, L5
❑ Weakness of gluteus medius muscle(hip abduction): superior glutealnerve, L5

L5 indicator muscle: extensor hallucis longus (90% L5)

Thank you for your attention!