zosteriform lichen planus: an unusual clinical variant · clinical •purple polygonal pruritic...
TRANSCRIPT

A S H VI N G A R L A P A T I , D . O .P R O G R A M D I R E C T O R : S T A N L E Y S K O P I T , D O , M S E , F A O C D
L A R K I N C O M M U N I T Y H O S P I T A L / N S U - C O M
A O C D M I D Y E A R M E E T I N G
A P R I L 2 3 - 2 6 2 0 1 5
ZOSTERIFORM LICHEN PLANUS: AN UNUSUAL
CLINICAL VARIANT

DISCLOSURES
No Financial Relations
with
Commercial Interests

OBJECTIVES
• Case presentation
• Introduction
• Epidemiology
• Clinical
• Pathogenesis
• Differential Diagnosis
• Histopathology
• Treatment and Prognosis

CASE PRESENTATION
• 52-year-old woman w/ six-week history of a pruritic
eruption on her right leg
• PMHX: Discoid Lupus Erythematosus (DLE). No prior
hx of herpes zoster
• No significant family or medication history
• Hepatitis C serology was negative

PHYSICAL EXAMINATION
• Purple pruritic papules and plaques with an
overlying white scale present on her right thigh
• The lesions were arranged in a linear pattern in the
L1, L2, and L3 dermatomal distribution
• A lacy white patch was seen on her left buccal
mucosa
• There was no scalp or nail involvement



DIAGNOSIS
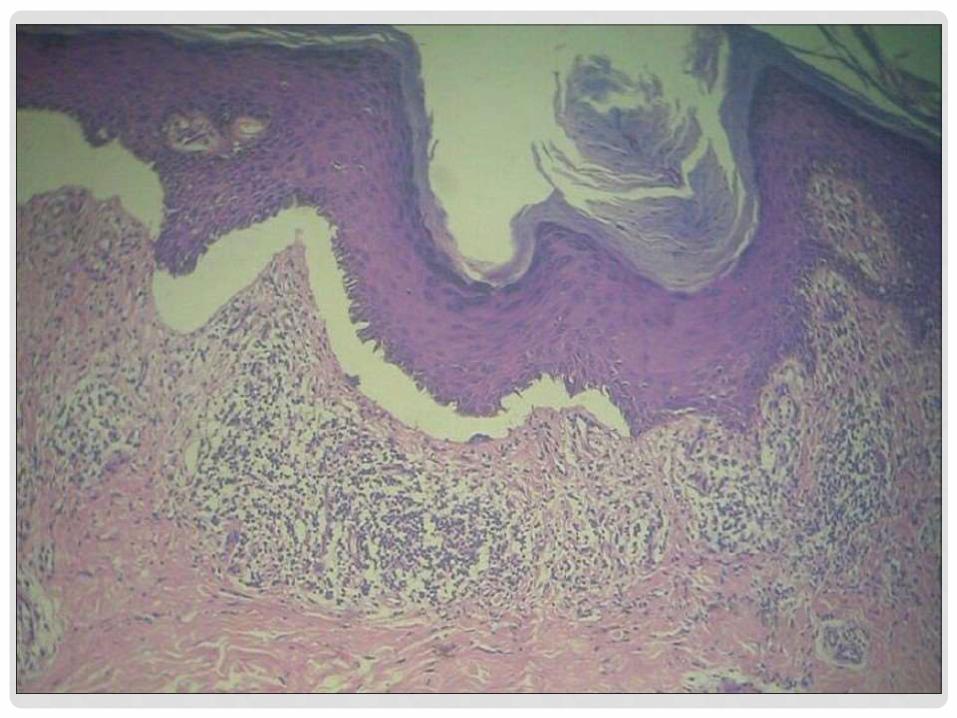
• Histopathology: Wedge shaped hypergranulosis,
acanthosis, saw-tooth rete ridges, and a lichenoid
infiltrate
• A diagnosis of Zosteriform Lichen Planus was made
based on the clinical and pathological correlation


TREATMENT
• Intramuscular injection of Kenalog 40mg
• Tacrolimus ointment 0.1%, which was applied to the
cutaneous and oral lesions twice daily

INTRODUCTION
• Lichen Planus(LP): Papulosquamous skin disorder
with several morphological variants.
• Zosteriform LP may arise:
De novo
At sites of trauma (koebnerization)
Wolf’s isotopic response at the site of healed zoster
• Zosteriform type is an uncommon variant of lichen
planus with dermatomal or zonal distribution.

EPIDEMIOLOGY
• Prevalence of LP is 0.22% to 5% worldwide
• Average age of onset is 50 years old
• No racial predilection
• Females slightly more affected often than males
• The mucous membranes are affected in 65% of cases
• Oral LP: Wickham's striae may develop into squamous cell carcinoma(SCC) in 0.2% of cases
• Zosteriform LP is an atypical presentation of linear LP. Linear LP accounts for less than 1% of cases

CLINICAL
• Purple polygonal pruritic flat-topped papule and plaques. May have wickham's striae on papules
• Over 20 variants of lichen planus
• Linear LP refers to lichen planus with a unilateral linear distribution
• Can present in segmental distribution corresponding to a dermatome referred to as zosteriform lichen planus
• Zosteriform lichen planus: Wolf’s isotopic response at areas of healed zoster
Secondary to Koebnerization from trauma
De novo eruption on previously normal skin

PATHOGENESIS
• Lesions arranged in band several centimeters wide
and run along the course of a peripheral cutaneous
nerve and its branches
Triggered by neural factors
Suggested that the lesions in zosteriform LP actually follow
the Lines of Blaschko rather than an actual dermatome
Blaschkoid lines are invisible lines in the skin that are
believed to trace the migration of embryonic cells
Some believe that true zosteriform LP only occurs if lesions
develop at sites of healed herpes zoster

DIFFERENTIAL DIAGNOSIS
• Linear psoriasis
• Lichen striatus
• Linear epidermal nevus
• Linear darier’s disease
• Inflammatory linear verrucous epidermal
nevus(ILVEN)
• Lichen simplex chronicus
• Lichenoid drug eruption
• Lichenoid mycosis fungoides

HISTOPATHOLOGY
• Band-like lymphohistiocytic infiltrate at the dermal-epidermal junction(DEJ) and upper dermis. Wedge-shaped hypergranulosis and acanthosis with saw-toothed rete ridges
Wickham’s Striae seen in areas of hypergranulosis
• Max Joseph Spaces: Vacuolar degeneration at the basal layer leading to focal subepidermal clefts
• Civatte Bodies: Eosinophilic remnants of anucleateapoptotic basal cells found in the dermis
• Squamatization: Maturation and flattening basal layer cells


DIRECT IMMUNOFLUORESCENCE
• Direct Immunofluorescence(DIF):
Shaggy fibrin, cytoid bodies, and deposition of IgM immunoglobulins at the DEJ
Can distinguish LP from hypertrophic lupus erythematosus
(continuous granular band of IgG, IgM, IgA, and C3 at the
DEJ on DIF)

TREATMENT AND PROGNOSIS
• Treatments aimed to induce remission and relieve
associated pruritus
• First line therapy:
High potency topical steroids
• Systemic corticosteroids can be used as a second
line treatment or in those with more extensive
disease

TREATMENT AND PROGNOSIS
• Alternative treaments include
Immunosuppressive agents
Cyclosporine
Methotrexate
Azathioprine
Dapsone
Topical Tacrolimus
Narrow-band Ultraviolet B phototherapy. Psoralen plus ultraviolet A (PUVA)
Enoxaprarin Sodium
Oral Metronidazole

TREATMENT AND PROGNOSIS
• Treatment of pruritus• Oral antihistamines
• Diphenhydramine • Hydroxyzine
• Topical antipruritic agents • Menthol• Camphor• Pramoxine • Doxepin
• Prognosis: • Often resolves over average period of 18 months
• Approximately 20% of patients will have a second occurrence.In a subset of patients, the disease may persist for many years.
• Oral LP more therapy resistant, and close follow up advised given increased risk for SCC

REFERENCES
• 1. Pai K, Pai S. Zosteriform Lichen Planus: Case report of a rare variant of lichen planus. Our Dermatol Online. 2013; 4(2): 183-184.
• 2. Turel A, Ozturkcan 5, Sahin MT, TUrkdogan P. Wolf's isotopic response: a case of zosteriform lichen planus.J Dermatol 2002; 29: 339-42.
• 3. Scully C, Beyli M, Ferreiro MC, et al. Update on oral lichen planus: etiopathogenesis and management. Crit Rev Oral Biol Med 1998;9:86-122.
• 4. Boyd AS, Neldner KH. Lichen planus. J Am Acad Dermatol. 1991 Oct; 25(4): 593-619
• 5. Happle R: Zosteriform’ Lichen planus: Is it Zosteriform?Dermatology. 1996;192:385-6.
• 6. Turel A, Ozturkcan S, Ozturkcan S, Sahin MT: Wolf’s isotopic response: a case of zosteriform lichen planus. J Dermatol.2002;29:339-42.
• 7. Braun RP, Barua D, Masouye I: Zosteriform lichen planus after herpes zoster. Dermatology. 1998;197:87-8.
• 8. Perry D, Fazel N. Zosteriform lichen planus. Dermatology Online Journal 2006 Sep 8;12: (5): 3
• 9. Elston, Dirk M., and Tammie Ferringer. “Interface Dermatitis.” Dermatopathology. Edinburgh: Saunders/Elsevier, 2009. 135-139. Print.
• 10. Taneja A, Taylor CR. Narrow-band UVB for lichen planus treatment. Int J Dermatol. 2002 May;41(5):282-3.
• 11. Sugerman PB, Savage NW. Oral lichen planus: Causes, diagnosis and management. Australian Dental Journal 2002;47:(4):290-297.
• 12. James WD, Berger TG, Elston DM, eds. Andrews' Diseases of the Skin: Clinical Dermatology. 11th ed. Philadelphia, Pa: Saunders Elsevier; 2011:chap 12, Lichen Planus and Related Conditions; p. 213-218.