zoonoses: emerging rickettsial diseases
TRANSCRIPT

The science you expect.The people you know.
Zoonoses: Emerging Rickettsial Diseases
Sharon Altmann, PhD, RBP (ABSA), CBSP (ABSA)

Learning Objectives
Review the major groups of rickettsioses and their clinical manifestations
Identify risk factors for rickettsial infection
Understand the considerations for rickettsial diagnostics and treatments
2

3
Rickettsioses and Their Clinical Manifestations

What Are Rickettsia?• Members of the Alphaproteobacteria
order Rickettsiales• Obligate endosymbionts of eukaryotic
cells• Gram negative bacilli• Primarily transmitted by arthropod
vectors• Laboratory acquired infections
associated with aerosols, accidental parenteral inoculation
• One report of nosocomial A. phagocytophilum transmission from China (Zhang et al. JAMA. 2008;300(19):2263-2270)
• Anaplasmosis and ehrlichiosis have been contracted though contaminated blood transfusion products or solid organ transplant
Spotted Fever Group•Rickettsia rickettsia (Rocky Mountain Spotted Fever, RMSF)•R. parkeri (R. parkeri rickettsiosis)•R. conorii (Mediterranean spotted fever)•R. africae (African tick bite fever)
Typhus Group•R. prowazekii (epidemic typhus)•R. typhi (murine typhus)
Transitional Group•R. akari (rickettsialpox)•R. felis (flea-borne spotted fever)
Scrub Typhus Group•Orientia tsutsugamushi•Candidatus Orientia chuto•Candidatus Orientia chiloensis
Anaplasma Group•Anaplasma phagocytophilum (Anaplasmosis, formerly human granulocytic ehrlichiosis (HGE))
Ehrlichia Group•Ehrlichia chaffeensis•E. ewingii•E. muris eauclarensis
4

Transmission Vectors
Spotted Fever Group, Anaplasmas, Ehrlichias• Hard body (ixodid) tick bites
Typhus Group• R. prowazekii: bites from infected body lice (Pediculous humanus humanus) or ectoparasites from infected
flying squirrels; inhalation or accidental mucosal or parenteral inoculation of body louse feces• R. typhi: accidental mucosal or parenteral inoculation of rat flea (Xenopsylla cheopsis)
Transitional Group• R. akari: accidental mucosal or parenteral inoculation of mouse mite (Liponyssoides sanguineus) feces• R. felis: bites from cat fleas (Ctenocephalides felis)
Scrub Typhus Group• Trombiculid mite larvae (chigger) bites
5

U.S. Geographical Distribution
6
Reported incidence rate per 1,000,000 persons per year, by county, 2000-2013
Spotted fever rickettsiosis, including Rocky Mountain Spotted Fever
Ehrlichia chafeensis ehrlichiosis Anaplasmosis
Biggs HM et al. MMWR Recomm Rep. 2016;65(No. RR-2):1–44.

Vector (And Pathogen) Distribution Is Changing• Gulf Coast tick (Ambylomma maculatum) reported in Illinois for
the first time during surveys in 2013 and 2019– 8 of 14 screened specimens were positive for R. parkeri (Phillips et al. J Parasitol. 2020;106(1):9-13)
• Asian longhorned tick (Haemaphysalis longicornis) first confirmed in the U.S. in 2017, with archived samples suggesting introduction in 2010 or earlier; confirmed in 14 states as of August 2020.
• Shown to carry at least 30 human pathogens naturally, including seven spotted fever group rickettsiae, three species of Ehrlichia, and seven species of Anaplasma (Zhao et al. Lancet Planet Health. 2020;4(8):e320-e329)
• Shown experimentally to support R. rickettsia infection (Stanley et al. J Med Entomol. 2020;57(5):1635-1639)
• Murine typhus is re-emerging in areas of Texas where it was previously eradicated (Ruiz et al. Emerg Infect Dis. 2020;26(5):1044-1046)
• Lone Start tick (A. americanum), a key vector for Ehrlichiaspecies, has markedly increased its range in the last 70 years (Monzón et al. Genome Biol Evol. 2016:8(5):1351-1360).
7
Historical and current expanded distribution of A. americanum. From Monzón et al. Genome Biol Evol. 2016:8(5):1351-1360

Clinical Manifestations- Tick-borne Rickettsioses
8
Adapted from Biggs et al. MMWR Recomm Rep. 2016;65(No. RR-2):1-44.
RMSF maculopapular rash, late-stage petechial purpuric rash, and late-stage gangrene of the digits.
Photos/CDC
R. parkeri rickettsiosis eschars and vesiculopapular rash. Photos/CDC
Disease Incubation period
Common initial signs and symptoms Cutaneous signs Common laboratory findings Severe disease
Estimated case-fatality
rateRocky Mountain spotted fever
3–12 days Fever, headache, chills, malaise, myalgia, nausea, vomiting, abdominal pain, photophobia, anorexia
Maculopapular rash approximately 2–4 days after fever onset in most, might become petechial and involve palms and soles
Thrombocytopenia, slightly increased hepatic transaminase levels, normal or slightly increased white blood cell count with increased immature neutrophils, hyponatremia
Meningoencephalitis, acute renal failure, ARDS, cutaneous necrosis, shock, arrhythmia, seizure, focal neurologic deficits, fulminant vasculitis, sudden transient hearing loss
5%–10% (treated),
25% (untreated)
Rickettsia parkeri rickettsiosis
2–10 days Fever, myalgia, headache Eschar, sparse maculopapular or vesiculopapular rash that might involve palms and soles
Mild thrombocytopenia, mild leukopenia, increased hepatic transaminase levels
Vasculitis —*
Ehrlichia chaffeensis ehrlichiosis (human monocytic ehrlichiosis)
5–14 days Fever, headache, malaise, myalgia, nausea, diarrhea, vomiting
Rash in approximately 30% of adults and 60% of children, variable rash pattern that might involve palms and soles, appears a median of 5 days after illness onset
Leukopenia, thrombocytopenia, increased hepatic transaminase levels, hyponatremia, anemia
Anemia, ARDS, DIC-like coagulopathies, central nervous system involvement, renal failure
1% (treated), 3%
(untreated)
Ehrlichiaewingii ehrlichiosis
—† Fever, headache, malaise, myalgia
Rash rare Leukopenia, thrombocytopenia, increased hepatic transaminase levels
—*
Ehrlichia muris-like agent ehrlichiosis
—† Fever, headache, malaise, myalgia
Rash in approximately 12%
Thrombocytopenia, lymphopenia, leukopenia, increased hepatic transaminase levels, anemia
—*
Human anaplasmosis(human granulocytic anaplasmosis)
5–14 days Fever, headache, malaise, myalgia, chills
Rash rare, in <10% Thrombocytopenia, leukopenia, mild anemia, increased hepatic transaminase levels, increased numbers of immature neutrophils
ARDS, peripheral neuropathies, DIC-like coagulopathies, hemorrhagic manifestations, rhabdomyolysis, pancreatitis, acute renal failure, secondary opportunistic infections
<%1 (treated), 1% (untreated)
*No known deaths. †Not documented.
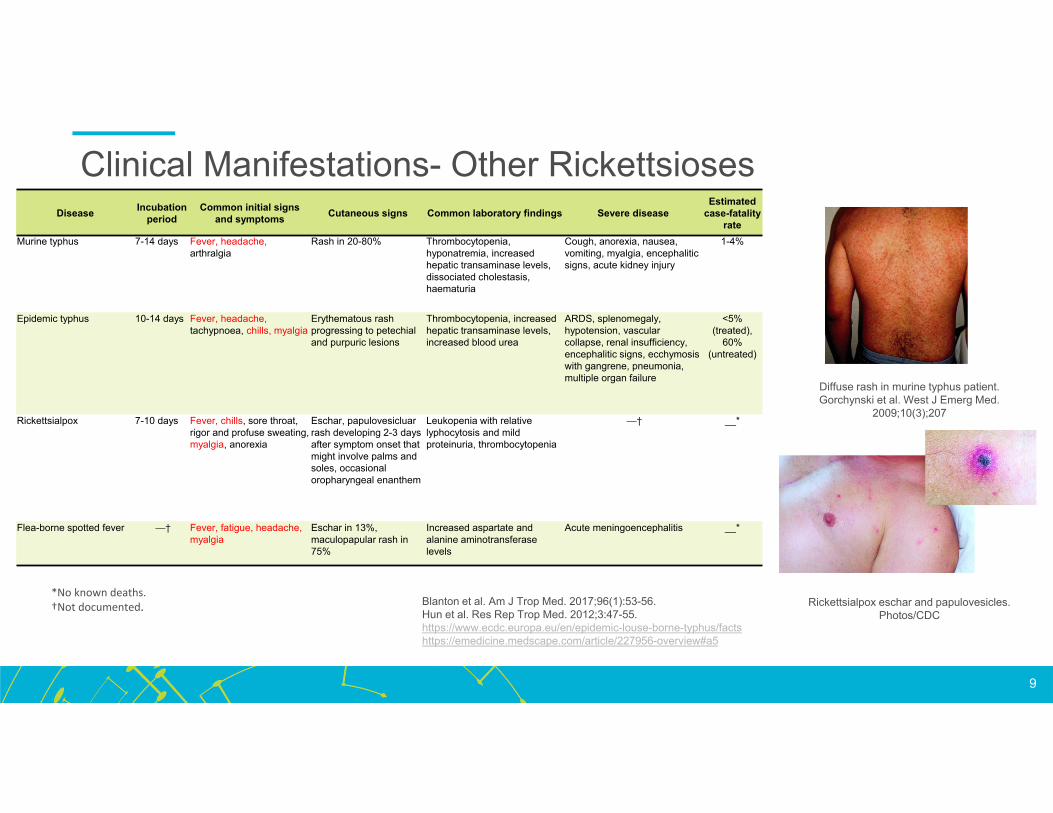
Clinical Manifestations- Other Rickettsioses
9
*No known deaths.†Not documented. Blanton et al. Am J Trop Med. 2017;96(1):53-56.
Hun et al. Res Rep Trop Med. 2012;3:47-55.https://www.ecdc.europa.eu/en/epidemic-louse-borne-typhus/factshttps://emedicine.medscape.com/article/227956-overview#a5
Diffuse rash in murine typhus patient.Gorchynski et al. West J Emerg Med.
2009;10(3);207
Rickettsialpox eschar and papulovesicles. Photos/CDC
Disease Incubation period
Common initial signs and symptoms Cutaneous signs Common laboratory findings Severe disease
Estimated case-fatality
rateMurine typhus 7-14 days Fever, headache,
arthralgiaRash in 20-80% Thrombocytopenia,
hyponatremia, increased hepatic transaminase levels, dissociated cholestasis, haematuria
Cough, anorexia, nausea, vomiting, myalgia, encephalitic signs, acute kidney injury
1-4%
Epidemic typhus 10-14 days Fever, headache, tachypnoea, chills, myalgia
Erythematous rash progressing to petechial and purpuric lesions
Thrombocytopenia, increased hepatic transaminase levels, increased blood urea
ARDS, splenomegaly, hypotension, vascular collapse, renal insufficiency, encephalitic signs, ecchymosis with gangrene, pneumonia, multiple organ failure
<5% (treated),
60% (untreated)
Rickettsialpox 7-10 days Fever, chills, sore throat, rigor and profuse sweating, myalgia, anorexia
Eschar, papulovesicluar rash developing 2-3 days after symptom onset that might involve palms and soles, occasional oropharyngeal enanthem
Leukopenia with relative lyphocytosis and mild proteinuria, thrombocytopenia
—† __*
Flea-borne spotted fever —† Fever, fatigue, headache, myalgia
Eschar in 13%, maculopapular rash in 75%
Increased aspartate and alanine aminotransferase levels
Acute meningoencephalitis __*

10
Risk Factors for Rickettsial Infection
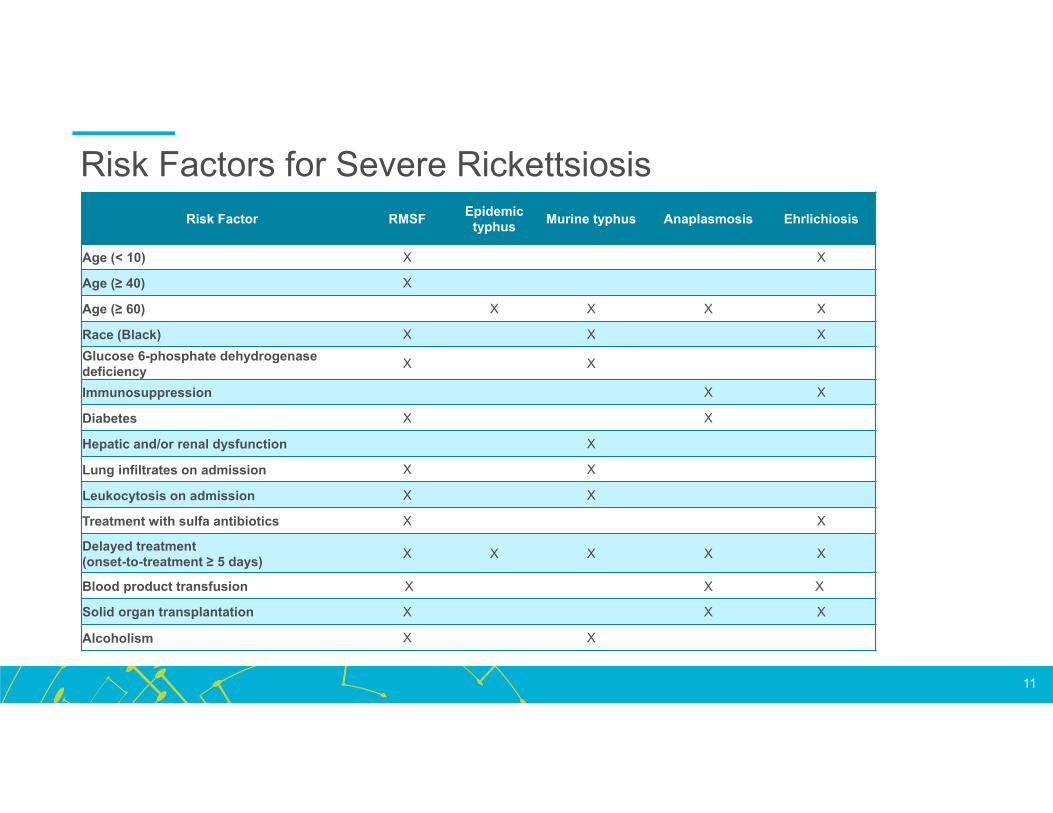
Risk Factors for Severe RickettsiosisRisk Factor RMSF Epidemic
typhus Murine typhus Anaplasmosis Ehrlichiosis
Age (< 10) X X
Age (≥ 40) X
Age (≥ 60) X X X X
Race (Black) X X XGlucose 6-phosphate dehydrogenase deficiency X X
Immunosuppression X X
Diabetes X X
Hepatic and/or renal dysfunction X
Lung infiltrates on admission X X
Leukocytosis on admission X X
Treatment with sulfa antibiotics X X
Delayed treatment (onset-to-treatment ≥ 5 days) X X X X X
Blood product transfusion X X X
Solid organ transplantation X X X
Alcoholism X X
11

Environmental And Behavioral Risk Factors For Exposure• Occupational or recreational exposure
to brushy or wooded areas with tall grasses or shrubs
• Lack of use of appropriate tick repellents
• Lack of appropriate clothing worn in high-risk areas
• Exposure to animals and birds (wild, livestock, and/or peridomestic)
• International travel• Exposure to individuals living with
poor sanitation and hygiene availability
Examples of at-risk populations:
12
• Hunters • Surveyors
• Outdoor enthusiasts • Pet / livestock owners
• Utility workers • Agricultural workers
• Veterinarians / animal
control
• Scientists / students
involved in fieldwork
• International travelers • Unhomed individuals
• Those working or living in
refugee / detention camps
• Those working with or near
unhomed populations
• Forestry / park workers • Military personnel

13
Considerations for Diagnostics and Treatment

Diagnostic Challenges• Poor awareness of vector exposure• Poor public awareness of their risks of
vector-transmitted diseases• Review of responses to the 2009, 2011, and
2012 HealthStyles surveys found 13.9% of respondents from New England and 20.8% from the Mid-Atlantic reported that no tickborne diseases were present in their area (Hook et al.2015. Ticks Tick Borne Dis;6(4)-483-488).
• Initial symptoms nonspecific• Characteristic rashes often develop after
initial clinical visit• Characteristic rashes under-identified in
patients with darker skin• For epidemic typhus, late relapse can
occur months or years after the initial infection, with a similar but milder clinical presentation (Brill-Zinsser disease)
14
Select differential diagnoses for tickborne rickettsioses. From Biggs HM et al. MMWR Recomm Rep. 2016;65(No. RR-2):1–44.
Select differential diagnoses for typhus group rickettsioses. From https://emedicine.medscape.com/article/231374-differential

Diagnostic RecommendationsAssay Pathogen Specimen Pros Cons
CultureSpotted fever group, Typhus group, Anaplasmas, Ehrlichias
Whole blood; punch biopsy of eschar or rash; autopsy specimens
Microbiological reference standard
Requires biosafety level 3 facility; may require ≥ 10 days; effectiveness decreases after first week of illness, commencement of therapy
Nucleic acid detection (polymerase chain reaction (PCR))
Spotted fever group, Anaplasmas, Ehrlichias
Whole blood; serum; eschar swab; punch biopsy; autopsy specimens
Increasingly common; easier differentiation between pathogens; short turnaround time; no specialized facilities required
Most sensitive when performed on eschar biopsy; most sensitive within first week of illness and before/within 48 hours of commencing therapy
Blood smear Anaplasmas, Ehrlichias Whole blood Rapid
Low sensitivity; requires specialized stains; requires experienced microscopist to read
Indirect immunofluorescentassay (IFA)
Spotted fever group, Typhus group, Anaplasmas, Ehrlichias
Serum
Current referencestandard; short turnaround time; effective independent of commencement of therapy
Antibodies generally absent during first week of illness; confirmation requires fourfold or greater increase in titer between acute and convalescent serum specimens; antibodies usually specific to genus rather than species
ImmunohistochemistrySpotted fever group, Typhus group, Anaplasmas, Ehrlichias
Punch biopsy (spotted fever group); autopsy specimens; formalin-fixed tissue
Effective with spotted fever eschars and rash lesions; effective post-mortem
Availability restricted to reference centers or research laboratories
15

Treatment Challenges• Treatment is less effective at preventing severe complications and death
when started ≥ 5 days after the onset of symptoms • Case fatality rate for untreated RMSF is 20-25%, with most deaths within 7-9 days of
symptom onset• Case fatality rate for untreated epidemic typhus can be up to 60%
• Diagnostic tests are not typically helpful for making a timely diagnosis of rickettsial disease
• Laboratory findings often remain within normal ranges until disease is severe• Microbiological reference standard test (organism culture) can take 10 or more days
to complete• IFA requires at least 2 weeks (need paired acute and convalescent sera, 2-4 weeks
apart)• Sensitivity of PCR assays vary by species, specimen type, time since onset of
symptoms, and whether treatment has been started
16
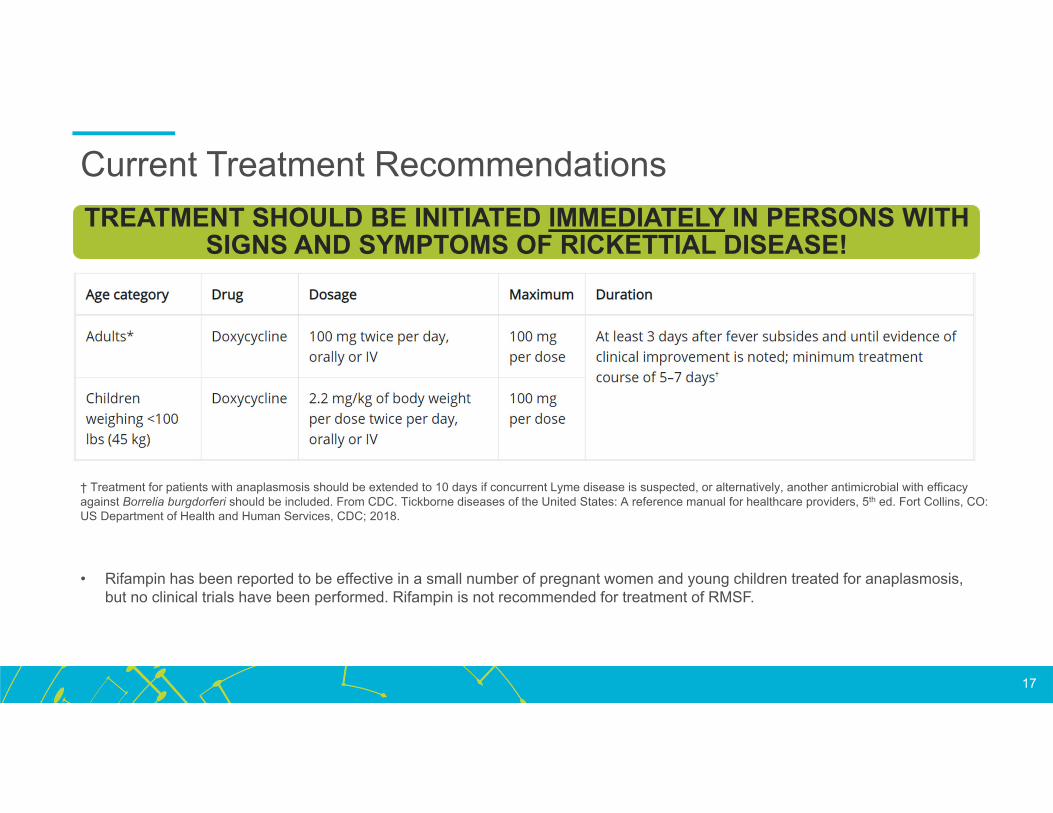
Current Treatment Recommendations
17
TREATMENT SHOULD BE INITIATED IMMEDIATELY IN PERSONS WITH SIGNS AND SYMPTOMS OF RICKETTIAL DISEASE!
• Rifampin has been reported to be effective in a small number of pregnant women and young children treated for anaplasmosis, but no clinical trials have been performed. Rifampin is not recommended for treatment of RMSF.
† Treatment for patients with anaplasmosis should be extended to 10 days if concurrent Lyme disease is suspected, or alternatively, another antimicrobial with efficacy against Borrelia burgdorferi should be included. From CDC. Tickborne diseases of the United States: A reference manual for healthcare providers, 5th ed. Fort Collins, CO: US Department of Health and Human Services, CDC; 2018.

National Reporting Requirements• Spotted fever group rickettsioses (including RMSF), ehrlichioses, and anaplasmosis are nationally notifiable
in the U.S.• State or local health departments should be notified of potential cases of tickborne disease• Health department should be able to help obtain confirmatory laboratory testing• Health department staff may contact the healthcare provider and patient for information to determine the surveillance
case definition.
• Typhus group rickettsioses are no longer nationally notifiable, although murine typhus is reportable in at least 14 states, including DE, MA, NH, OH, and PA. However…
• R. prowazekii is listed as a Health and Human Services Select Agent under 42 CFR Part 73. Clinical or diagnostic specimens used for diagnosis are considered exempt from the requirements within the regulation provided:
• The specimens are secured against theft, loss, or release during the period of time between the identification of R. prowazekii and the transfer or destruction of the specimens; and
• Any theft, loss, or release of the specimens is reported; and• Unless otherwise directed by the HHS Secretary, the specimens collected from the positive patient are transferred to a
registered entity or destroyed on-site by a recognized sterilization or inactivation process within 7 calendar days of the conclusion of patient care; and
• The laboratory notifies the specimen provider, CDC, and other appropriate authorities of the identification of R. prowazekii by telephone, fax, or email, and must submit an APHIS/CDC Form 4 to CDC within 7 calendar days of identification.
18

Select References1. Zhang L, Liu Y, Ni D, et al. Nosocomial Transmission of Human Granulocytic Anaplasmosis in China. JAMA. 2008;300(19):2263-2270.
https://jamanetwork.com/journals/jama/fullarticle/182918. Accessed September 10, 2020.
2. Biggs HM, Behravesh CB, Bradley KK, et al. Diagnosis and management of tickborne rickettsial diseases: Rocky mountain spotted fever and other spotted fever group rickettsioses, ehrlichioses, and anaplasmosis - United States a practical guide for health care and public health professionals. MMWR Recomm Rep. 2016;65(No. RR-2):1-44. doi:10.15585/mmwr.rr6502a1
3. Phillips VC, Zieman EA, Kim C-H, Stone CM, Tuten HC, Jiménez FA. Documentation of the Expansion of the Gulf Coast Tick ( Amblyomma maculatum) and Rickettsia parkeri : First Report in Illinois. J Parasitol. 2020;106(1):13. doi:10.1645/19-118
4. Zhao L, Li J, Cui X, et al. Distribution of Haemaphysalis longicornis and associated pathogens: analysis of pooled data from a China field survey and global published data. Lancet Planet Heal. 2020;4(8):e320-e329. doi:10.1016/S2542-5196(20)30145-5
5. Stanley HM, Ford SL, Snellgrove AN, et al. The Ability of the Invasive Asian Longhorned Tick Haemaphysalis longicornis (Acari: Ixodidae) to Acquire and Transmit Rickettsia rickettsii(Rickettsiales: Rickettsiaceae), the Agent of Rocky Mountain Spotted Fever, Under Laboratory Conditions. J Med Entomol. 2020;57(5):1635-1639. doi:10.1093/jme/tjaa076
6. Ruiz K, Valcin R, Keiser P, Blanton LS. Rise in murine typhus in Galveston County, Texas, USA, 2018. Emerg Infect Dis. 2020;26(5):1044-1046. doi:10.3201/eid2605.191505
7. Monzón JD, Atkinson EG, Henn BM, Benach JL. Population and evolutionary genomics of amblyomma americanum, an expanding arthropod disease vector. Genome Biol Evol. 2016;8(5):1351-1360. doi:10.1093/gbe/evw080
8. Blanton LS. The Rickettsioses: A Practical Update. Infect Dis Clin North Am. 2019;33(1):213-229. doi:10.1016/j.idc.2018.10.010
9. Hun L, Troyo A. An update on the detection and treatment of RIckettsia felis. Res Rep Trop Med. 2012;3:47-55. doi:10.2147/RRTM.S24753
10. Facts about epidemic louse-borne typhus. https://www.ecdc.europa.eu/en/epidemic-louse-borne-typhus/facts. Accessed September 11, 2020.
11. Typhus: Background, Pathophysiology, Epidemiology. https://emedicine.medscape.com/article/231374-overview. Accessed September 11, 2020.
12. Rickettsialpox: Background, Pathophysiology, Epidemiology. https://emedicine.medscape.com/article/227956-overview#a5. Accessed September 11, 2020.
13. Hook SA, Nelson CA, Mead PS. U.S. public’s experience with ticks and tick-borne diseases: Results from national HealthStyles surveys. Ticks Tick Borne Dis. 2015;6(4):483-488. doi:10.1016/j.ttbdis.2015.03.017
14. CDC. Tickborne Diseases of the United States: A Reference Manual for Healthcare Providers. 5th ed. Fort Collins, CO: US Department of Health and Human Services, CDC; 2018. https://www.cdc.gov/ticks/tickbornediseases/TickborneDiseases-P.pdf. Accessed September 8, 2020.
19
