zoonoses
DESCRIPTION
Zoonoses. Epidemiology of diseases transmitted from animals to humans. What are zoonoses?. Diseases that are transmitted from animals to humans. Bacillus anthracis Brucellosis Crimean-Congo hemorrhagic fever Rabies Hanta Virus Toxoplasmosis Campylobacter. Farm Animals Cattle Swine - PowerPoint PPT PresentationTRANSCRIPT

Zoonoses
Epidemiology of diseases transmitted from animals to
humans
What are zoonoses?
Diseases that are transmitted from animals to humans

Bacillus anthracis Brucellosis Crimean-Congo hemorrhagic fever Rabies Hanta Virus Toxoplasmosis Campylobacter

What kind of animals transmit zoonoses?
Farm Animals
Cattle Swine Goats Cats & dogs Poultry
Wild Animals
Ticks Squirrels Raccoons Mice/rodents others

Farmers more susceptible to contracting zoonoses
1. More likely to share air and space with animals
2. More contact with domestic and wild animals

How are disease transmitted?
Every day contact with animals Transporting By-products (feces/urine) Scratches or bites From milk and milking Contaminated soils Contaminated meats

Common Zoonoses
Campylobacter
Common CarriersCattle
Sheep
Pigs
Dogs
Rodents
Poultry

Campylobacter
Transmission
Contaminated food or animals
Clinical presentation
Stomach ache Nausea Headache Diarrhea

Cat-Scratch Disease
Common carriers
Cats
Dogs

Cat-Scratch DiseaseBartonella henselae
Transmission
Scratches and puncture wounds from infected animals
Clinical presentation
Fever Skin papule Swollen lymph nodes

Salmonella
Common carriers
Cattle
Cats
Dogs
Horses
Poultry

Salmonella
TransmissionDirect contact with
animal or feces
Contaminated food
Clinical Presentation Chills Fever Headache Diarrhea Vomiting

Encephalitis
Common carriers
Horses
Rodents

Encephalitis
Transmission
Mosquito bites Tick bites
Clinical presentation
Lethargy Fever Headache Disorientation

Rabies
Common Carriers
CatsDogs
RaccoonsSkunks
BatsFoxes

Rabies
Transmission
Animal Bite
Contact with infected tissue, fluids or feces
Clinical presentation Fever Headache Agitation Confusion Seizures Excessive salivation

Toxoplasmosis
Common carriers
Cats
Sheep

Toxoplasmosis
Transmission
Ingestion of infected meats
Fecal contaminated soil
Clinical Presentation
Fever Swollen nodes Abortion Still-birth Mental retardation

Scabies
Common Carriers
Dogs
Raccoons

Scabies
Transmission
Direct contact with infected animals
Clinical presentation
Itching skin lesions

Prevention and Control

Assure an uncontaminated water supply
Add chlorination to water Connect to water supply Appropriate disposal of wastes

Prevent food contamination
1. Avoid unpasturized milk2. Wash hands3. Disinfect kitchen surfaces4. Wash raw fruits and vegetables5. Don’t defrost meats on the counter6. Use separate utensils for raw/cooked meat

Always drink pasteurized milk!

Protect pets from getting & transmitting diseases
Vaccinate cats and dogs against rabies Do not keep wild animals as pets Do not allow pets to drink from toilet Clean pet’s living area 1x/week Clean litter box daily

Pregnant women should not clean litter
boxes

Prevent tick bites
Wear repellent Wear appropriate clothing
Long-sleeved shirt Tuck pant legs into socks
Check yourself and pets after being in a tick-infested area

Treat animal scratches and bites seriously
Wash area with soap and water Apply anti-bacterial medication Bandage wound Consider medical attention
Most Zoonoses are preventable if cautionary
measures are taken!!

Food-borne and Water-borne Diseases
Epidemiology of diseases spread by food and water

Definition
Food-borne illness – two or more cases of a similar illness resulting from the ingestion of a common food
Water-borne illness – an illness that occurs after consumption or use of water intended for drinking or as illness associated with recreational water such as swimming pools, whirlpools, hot tubs, spas, water parks, and naturally occurring fresh and marine surface waters

Epidemiology - Food-borne
In the U.S. per year
76 million illness
325,000 hospitalizations
5000 deaths - most unknown pathogens Three known pathogens cause 1500 deaths
Salmonella
Listeria
Toxoplasma

Epidemiology - Food-borne
Cholera only bacterial food-borne illness that must be reported internationally
Hepatitis A only viral food-borne illness that is reported
Globally only 1-10% of food-borne illness incidences are reported.

Epidemiology - Food-borne
List of most common bacterial food-borne illness, listed in order of occurrence
1) Campylobacter
2) Salmonella
3) Shigella
4) E. Coli

Epidemiology - Food-borne List of most common viral food-borne illness
1) Norwalk virus
2) Astroviruses
3) Rotaviruses
4) Enteric adenoviruses 23,000,000 incidences per year in the U.S Spread person to person via fecal-oral route Infectious at low doses; foods act as transfer
media only
Diagnosis
Important to the history is the exact time of exposure which can help narrow down the causative agent

History
History of two or more people within a household becoming ill at the same time more likely food-borne vs. two people becoming ill within 24-36h.

History
Identify food handling practices
a) length of preparation before
consumption
b) cooking time and reheating
c) possible cross contamination
d) people with poor hygiene

History
Identify activities that increase risk of exposure
restaurants
day care centers
street-vended food or raw seafood
overseas travel
camping-ingestion of lake/stream water Check to see if patient is on antibiotics or
medications that reduce gastric acidity

Physical Examination
Determine hydration statusPresence of blood in the stoolExclude other diarrheal illness

Diagnostic Tests
Blood cultures – suspect bateremia Gram stain - identifies campylobacter with
66-99% sensitivity Fecal leukocytes - if positive = higher culture
yield Ova and parasites - done in the ER

Diagnostic Tests
Stool cultures only if pt
1) febrile
2) bloody diarrhea
3) severe abdominal pain
4) clinically severe or persistent
5) significant historical risk factors for
food-borne illness

Bacillus anthracis
Incubation period – 2d-weeks Signs and symptoms – nausea, vomiting,
bloody diarrhea, abdominal pain Duration – weeks Food Source – contaminated meat Lab testing – blood
Bacillus cereus
Enterotoxin Incubation period – 1-6h Signs and symptoms – sudden fever, nausea,
vomiting, may have diarrhea Duration – 24h Food Source – rice, meat Lab testing – none Treatment – supportive only

Brucella spp.
Incubation period – 7-21d Signs and symptoms – fever, chills, headache,
myalgias, arthralgias, bloody diarrhea Duration – weeks Food Source – raw milk, goat cheese, meats Lab testing – blood, serology

Clostridium botulinum
Adults, children Incubation period – 12-72h Signs and symptoms – vomiting, diarrhea, diplopia,
dysphagia, descending muscle weakness Duration – variable, can end in death Food Source – improperly canned foods, fermented fish,
garlic, herb-infused oils, baked potato in foil, foods kept in a warm oven for hours
Lab testing – stool, serum, and food assayed for toxin at CDC or state labs
Treatment – botulinum antitoxin

Clostridium botulinum
Infants Incubation period – 3-30d Signs and symptoms – lethargy, poor feeding,
hypotonia Duration – variable Food Source – honey, home-canned foods Lab testing – stool, serum, and food assayed for
toxin at CDC or state lab Treatment – botulinum immune globulin

Campylobacter
Incubation period – 2-5d Signs and symptoms – bloody or watery diarrhea,
cramps, fever Duration – 2-10d Food Source – Poultry, milk, water Lab testing – special stool culture

Clostridium perfringens
Incubation period – 8-16h Signs and symptoms – watery diarrhea, nausea,
cramps Duration – 24-48h Food Source – meat, poultry, gravy, dried or
precooked foods Lab testing – quantitative culture of stool Treatment – supportive only

Enterohemorrhagic E. coli
Incubation period – 1-8d Signs and symptoms – bloody diarrhea, abdominal
pain, vomiting Duration – 5-10d Food Source – undercooked meat, unpasteurized
dairy products, milk, raw fruit and vegetables, salami, contaminated water, salad dressing, yogurt, acidic foods
Lab testing – specific stool culture Treatment – supportive only

Enterotoxigenic E. coli (traveler’s diarrhea)
Incubation period – 1-3d Signs and symptoms – watery diarrhea, vomiting,
cramps Duration – 3-10d Food Source – fecal contamination of food Lab testing – specific stool culture

Salmonella spp.
Incubation period – 1-3d Signs and symptoms – diarrhea, fever, cramps, vomiting, s.
typhi and paratyphi cause chills, myalgia, headache, with rare diarrhea
Duration – 4-7d Food Source – eggs, poultry, unpasteurized milk or juice, raw
fruits and vegetables, street venders, fecal water contamination Lab testing – stool cultures Necessitates typhoid immunization for travelers
Shigella spp.
Incubation period – 24-48h Signs and symptoms – bloody diarrhea, fever,
cramps Duration – 4-7d Food Source – fecal food or water contamination,
person-person spread by fecal-oral contamination
Lab testing – stool cultures
S. Aureus
Incubation period – 1-6h Signs and symptoms – sudden severe nausea,
vomiting, diarrhea Duration – 24-48h Food Source – unrefrigerated meats, potato
and egg salad, cream pastries Lab testing – none Treatment – supportive only

Vibrio cholerae
Incubation period – 24-72h Signs and symptoms – severe watery diarrhea
and vomiting Duration – 3-7d death from dehydration Food Source – contaminated water, fish, shellfish,
street vendors Lab testing – specific stool cultures
Yersinia spp.
Incubation period – 24-48h Signs and symptoms – mimics appendicitis, can
have a rash Duration – 1-3 weeks Food Source – undercooked pork, unpasteurized
milk, contaminated water Lab testing – specific stool or blood cultures

Epidemiology of diseases spread by arthropod vectors

Vector-borne Disease Mortality Distribution
WHO, 2005
Majority of Vector-borne Disease (VBD) burden borne by developing countries
High amount in Africa

Vector-borne Disease What is VBD? Types of VBD transmission:
Human-vector-human
(Anthroponotic Infections)
Vector
Humans
Humans
Vector
MalariaDengueYellow fever
Animal-vector-human
(Zoonotic Infections)
Vector Vector
Animals
AnimalsHumans Lyme disease
Hantaviral diseaseMost arboviral diseases (e.g., WNV)

Vector-borne Diseases of Concern
Disease Pathogen Vector Transmission
Protozoan
Malaria Plasmodium falciparum, vivax, ovale, malariae
Anopheles spp. Mosquitoes Anthroponotic
Leishmaniasis * Leishmania spp. Lutzomyia & Phlebotomus spp. Sandflies
Zoonotic
Trypanosomiasis * Trypanosoma brucei gambiense, rhodesiense
Glossina spp. (tsetse fly)
Zoonotic
Chagas disease * Trypanosoma cruzi Triatomine spp. Zoonotic
* WHO neglected tropical disease Hill et al., 2005
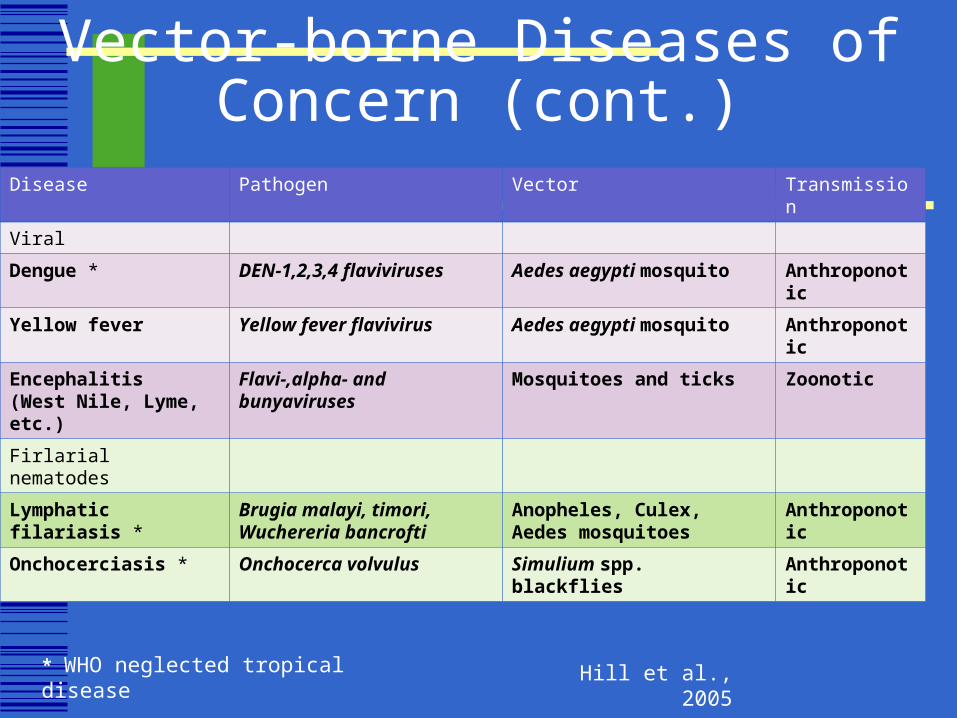
Vector-borne Diseases of Concern (cont.)
Disease Pathogen Vector Transmission
Viral
Dengue * DEN-1,2,3,4 flaviviruses Aedes aegypti mosquito Anthroponotic
Yellow fever Yellow fever flavivirus Aedes aegypti mosquito Anthroponotic
Encephalitis(West Nile, Lyme, etc.)
Flavi-,alpha- and bunyaviruses
Mosquitoes and ticks Zoonotic
Firlarial nematodes
Lymphatic filariasis * Brugia malayi, timori, Wuchereria bancrofti
Anopheles, Culex, Aedes mosquitoes
Anthroponotic
Onchocerciasis * Onchocerca volvulus Simulium spp. blackflies Anthroponotic
* WHO neglected tropical disease Hill et al., 2005

Vector-borne Disease Dynamics
Susceptible population
• Migration (forced)
•Vector environment
Vector•Survival, lifespan
•Reproduction/breeding patterns
•Biting behavior
Pathogen
•Survival
•Transmission
•Replication in host
Pathophysiologic pathways
Individual/population
Health
Genetic/constitutional
factors
Individual riskfactors
Social relationships
Living conditionsLivelihoods
Institutions (including medical
care)
Social and economic
policies
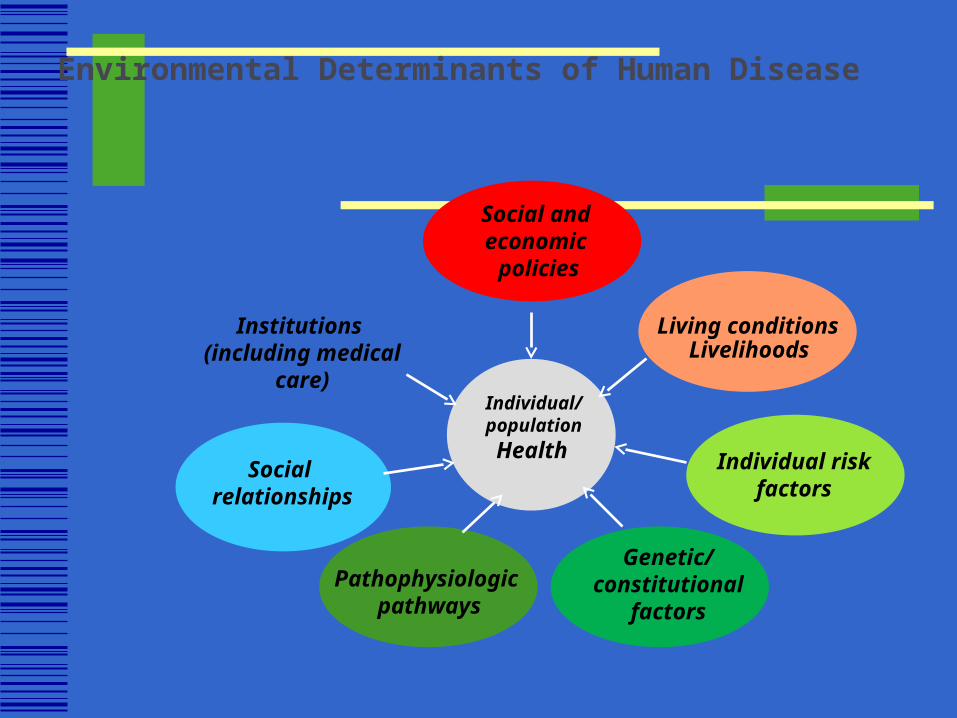
Environmental Determinants of Human Disease

Pathophysiologic pathways
Individual/populationHealth
Genetic/constitutional
factors
Individual riskfactors
Social relationships
Living conditionsLivelihoods
Institutions (including medical
care)
Social and economic
policies
Climate?
Environmental Determinants of Human Disease (cont.)

Case Study I: Malaria

40% world population at risk 500 million severely ill Climate sensitive disease1
No transmission where mosquitoes cannot survive
Anopheles: optimal adult development 28-32ºC
P falciparum transmission: 16-33ºC
Highland malaria2
Areas on the edges of endemic regions
Global warming El Niño3
Outbreaks
Estimated incidence of clinical malaria episodes (WHO)
1 Khasnis and Nettleman 2005; 2 Patz and Olson 2006; 3 Haines and Patz, 2004
McDonald et al., 1957
Case Study I: Malaria (cont.)

WHO, 2008b
Malaria Transmission Map

Case Study 2: Lyme Disease

Stafford, 2007
Transmission Cycle of Lyme Disease
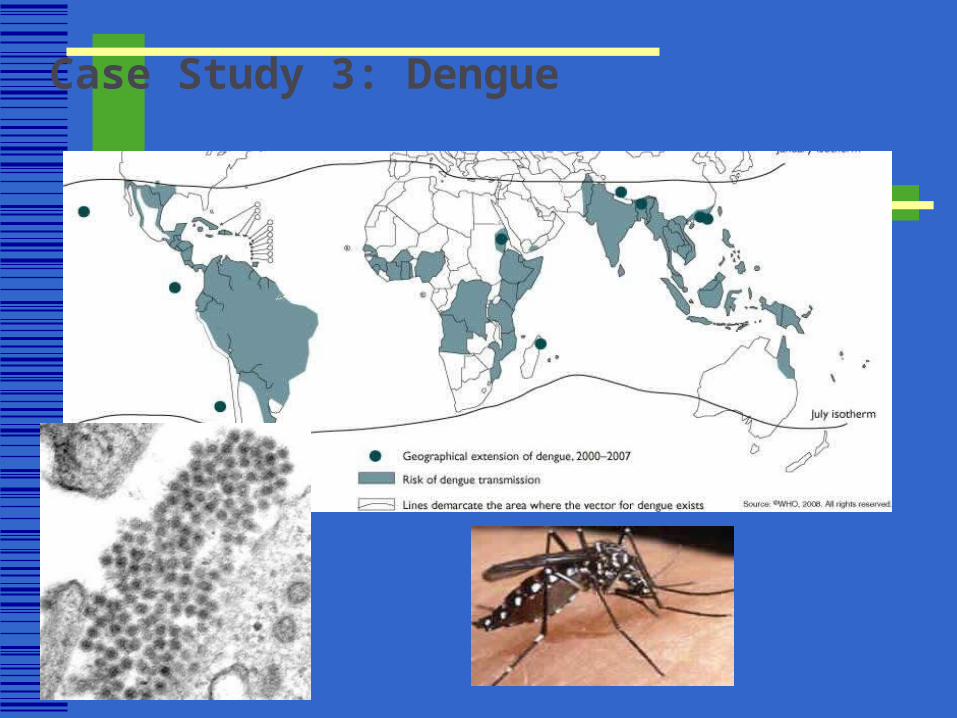
Case Study 3: Dengue

Whitehead et al., 2007
Transmission Cycle of Dengue

T. b. gambienseT. b. gambiense
T. b. rhodesiense
T. b. rhodesiense
Case Study 4: African Trypanosomiasis

Trypanosomiasis Trypanosomosis, spread
by tsetse flies, imposes a huge burden on African people and livestock
Many aspects of the vectors’ life cycles are sensitive to climate, and spatial distributions can be predicted using satellite-derived proxies for climate variables
Source: David Rogers, Oxford
Case Study 4: African Trypanosomiasis (cont.)

IMMUNIZATION
active passive

Active immunization
Inactivated virus Live attenuated virus Bacterial protein or polysaccharides
These immunogens are carried out BEFORE exposure to a disease

Passive immunization
Pooled immune globulins that contain specified amounts of antibody used for individuals who have recently been or may soon be exposed to a disease

Differences
Passive immunization can never have a life-long protective effect.
Active immunization towards most of the diseases have a life-long protective effect.
(5-20 years)

Differences
Passive immunization: protective effect starts immediately
Active immunization: protective effect starts a few weeks later

Differences
In passive immunization there is a greater possibility for the hypersensitity reactions to occur than there is in active immunization
Therefore epinephrine, corticosteroids, antihistaminics must be at hand.

Post-infection immunity
Immunity towards certain diseases can also be achieved by acquiring the disease
Measles, Hep.A have life-long post-infection immunity

Herd immunity
Used for the immunity of the whole population.
At least 70% of the population must be immune.

Variables of herd immunity
characteristics of organism ıts mode of transmission period of infectivity ıncubation time size of the population duration of artificial or post-infection
immunity

Active immunizing agents
Tetanus bacterial toxoid i.m. Diphteria bacterial toxoid i.m. Rubella live attenuated virus s.c. Measles live attenuated virus s.c. Mumps live attenuated virus s.c.

Active immunizing agents
Poliomyelitis inactivated virus oral or i.m. Rabies HDCV i.m. Hepatitis B recombinant DNA i.m.

Passive immunizing agents(Human immunoglobulin)
Tetanus management of wounds Rabies post exposure prophylaxis of animal
bites Measles prevention or modification of
disease before likely exposure or after contact (not used in the control of epidemics)

Passive immunizing agents(Human immunoglobulin
Hepatitis A modification of disease of househod contacts (not used in the control of epidemics)
Antivenin for snake, spider, or scorpion bite.

Tetanus prophylaxis in wound management
For clean wounds tetanus toxoid (active immunization) is indicated unless the patient has received two or more doses of toxoid within five years
For unclean or deep wounds in addition to toxoid 250 units of TIG (passive immunization)should be administered at separate sites

Rabies
Postexposure prophylaxis always includes both passive and active immunization except for persons who have previously been actively been immunized
RIG (20iu/kg) i.m. And around the bite HDCV (Human Diploid Cell Vaccine) on
days 1,3,7,14 and 28

COLD CHAIN IN VACCINATION
Vaccines should be at certain temperatures at the Ministry of Health, Health Directorate of the Province, Health Institutions and the Mobile Health team
Vaccines should be transported at certain temperatures
Vaccines should never be kept above 80 C even at the mobile team

CONDITIONS FOR KEEPING VACCINES AT A REFRIGERATOR AT PRIMARY HEALTH ARE LEVEL :
one health personnel should be the responsible person for this refrigerator
nothing but only vaccines and related water should be kept in this refrigerator
there should be a thermometer inside the refrigerator the responsible person must check the temperature 2
times a day and mark it on a chart sticked to the door of the refrigerator

no vaccine shouldbe kept inside the door of the refrigerator
space should be kept in between the vaccines for cold air circulation
a virus vaccine should not touch a piece of ice refrigerator should be kept at a distance of at
least 20 cm from the wall refrigerator should be placed away from the
sunlight