zambia - institute for health metrics and evaluation · 2 full country evaluation 2014 findings...
TRANSCRIPT
2 Full Country Evaluation 2014
Findings from the 2014 Gavi Full Country EvaluationZAMBIA
UNIVERSIDADEE D U A R D OM O N D L A N E
UNIVERSIDADEE D U A R D OM O N D L A N E
24, rue Salomon de Rothschild - 92288 Suresnes - FRANCETél. : +33 (0)1 57 32 87 00 / Fax : +33 (0)1 57 32 87 87Web : www.carrenoir.com
GAVIGAI_14_6999_LogoBlancQuad_GB30/07/2014
ÉQUIVALENCE QUADRICHROMIE
CYAN 40 % JAUNE 100 %
CYAN 100 % MAGENTA 50 %
CYAN 80 %
Ce �chier est un document d’exécution créé sur Illustrator version CS5.
RÉSERVE BLANCHE

3Full Country Evaluation 2014
This brief presents findings for Zambia from the 2014 Gavi Full Country Evaluation (FCE) Annual Dissemination Report. It was prepared by the Institute for Health Metrics and Evaluation (IHME) at the University of Washington in collaboration with members of the Gavi FCE Team: the University of Zambia (UNZA), Zambia; the Infectious Diseases Research Collaboration (IDRC), Uganda; University of Eduardo Mondlane (UEM), Mozam-bique; Health Alliance International (HAI), Mozambique; International Centre for Diar-rhoeal Disease Research, Bangladesh (icddr,b); and PATH, USA. This work is intended to inform evidence-based improvements for immunization delivery in Zambia, partner FCE countries, and more broadly, in low-income countries, with a focus on Gavi funding.
The contents of this publication may not be reproduced in whole or in part without per-mission from the Gavi Full Country Evaluation Team.
Citation: Citation: Gavi Full Country Evaluation Team. Zambia: Findings from the 2014 Gavi Full Country Evaluation. Seattle, WA: IHME, 2015.
Institute for Health Metrics and Evaluation 2301 Fifth Ave., Suite 600 Seattle, WA 98121 USA
Telephone: +1-206-897-2800 Fax: +1-206-897-2899 Email: [email protected]
www.healthdata.org
University of Zambia, Department of Economics School of Humanities & Social Sciences Great East Road Campus Lusaka Zambia
Telephone: +260-21-1-290475 Fax: +260-21-1-290475 Email: Felix Masiye, PhD, MSc [email protected]
www.unza.zm
Copyright ©2015 Gavi Full Country Evaluation Team
Gavi Secretariat Monitoring & Evaluation 2, Chemin des Mines, 1202 Geneva Switzerland
Telephone: 00 41 22 9096542 Fax: 00 41 22 9096551 Email: Abdallah Bchir [email protected]
www.gavi.org

1 Full Country Evaluation 2014
Coverage rates have been highly variable among districts since 2000. The full 2014 Annual Dissemination Report pro-vides district-level maps for 2000 and 2013 for all antigens.
• Diphtheria, pertussis, tetanus vaccine (DPT3). Coverage increased in a majority of districts between 2000 and 2013, but in both periods there are large within-country inequal-ities in coverage. By 2013, DPT3 coverage exceeded 80% in approximately half of districts, while in about 10% of districts coverage was below 65% (Figure 1).
• Fully vaccinated child (received Bacillus Calmette-Guérin [BCG] vaccine, three doses of oral polio vaccine [OPV3], three doses of DPT, and measles vaccine). Nearly 40% of districts experienced increases between 2000 and 2013. Full vaccination coverage was even more variable than coverage of DPT3 in 2013, with a handful of districts below 20% and the best-performing district at 99% (Figure 2).
0%
20%
40%
60%
80%
100%2000 2013
0%
20%
40%
60%
80%
100%20132000
Figure 1: District-level DPT3 coverage, using small area analysis techniques Figure 2: District-level fully vaccinated child coverage, using small area analysis techniques
Assessment of progress, successes, and challenges• CollectedandrevieweddocumentsrelevanttoGavi
funding, operational plans and budgets, guidelines, and planning and reporting.
• Conductedbriefinterviewstoconfirmfactualinformation.• ObservedChildHealthTechnicalWorkingGroup(TWG)
meetings, Expanded Program on Immunization (EPI) TWGmeetings,InteragencyCoordinatingCommittee(ICC)meetings,HealthSystemsStrenthening(HSS) proposalinceptionworkshop,post-trainingevaluationof rotavirus vaccine Training of Trainers (TOT), and the pneumococcal conjugate vaccine (PCV)/rotavirus vaccine Post-IntroductionEvaluation(PIE)debriefing.
Key informant interviews• Conducted32interviewsatthenationalanddistrictlevelsandwithstakeholdersfromtheMinistryofCommunityDevelopment,MotherandChildHealth(MCDMCH)andpartner organizations.
• ConductednineinterviewswiththeGaviSecretariatandVaccine Alliance partners.
Health facilities survey• PreliminaryanalysisofstratifiedrandomsampleofZambian
health facilities.
Analysis of administrative data on vaccine coverage• AnalysisofHealthManagementInformationSystem
data collected from health facility survey.
Small area analysis • Compiledandanalyzedallavailablesurveyandcensus
data sources.
Inequality analysis • Compiledandanalyzedallavailablesurveydatasources
of household wealth and vaccination coverage.
Summary of 2014 evaluation activities
ANALYSISof immunization coverage, child mortality, and inequality
2Full Country Evaluation 2014
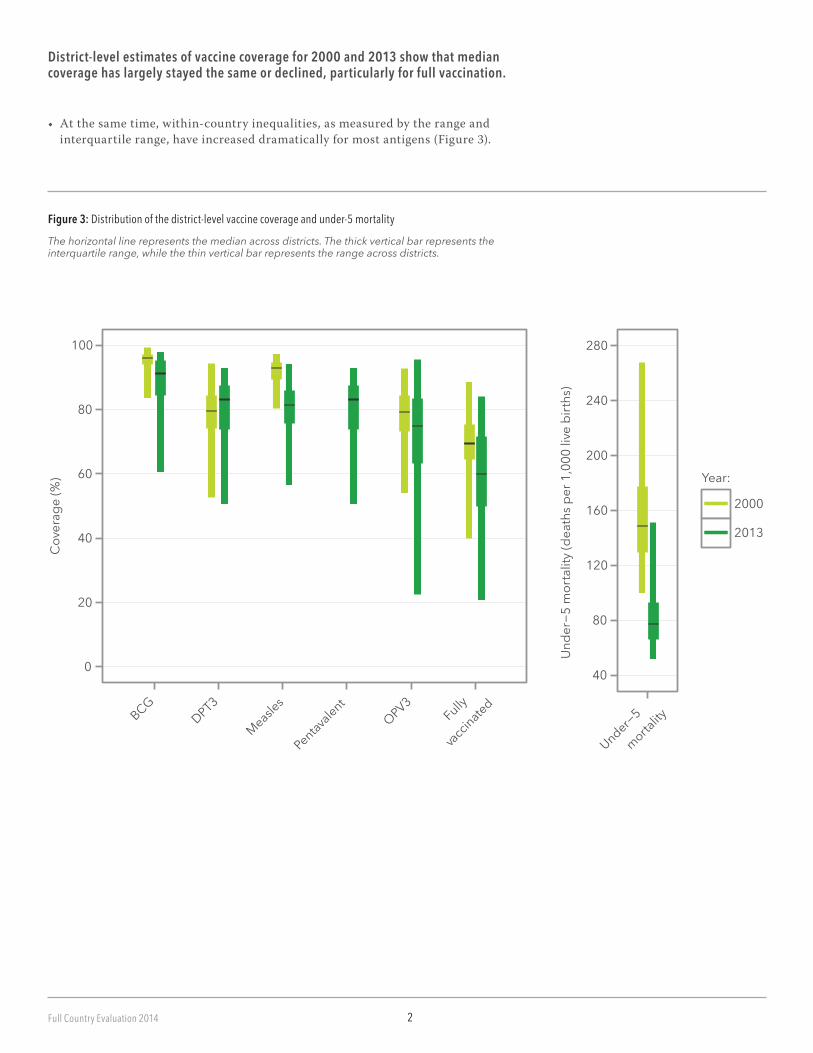
Figure 3: Distribution of the district-level vaccine coverage and under-5 mortality
District-level estimates of vaccine coverage for 2000 and 2013 show that median coverage has largely stayed the same or declined, particularly for full vaccination.
• Atthesametime,within-countryinequalities,asmeasuredbytherangeandinterquartile range, have increased dramatically for most antigens (Figure 3).
0
20
40
60
80
100
BCGDPT3
Measles
Pentavalent
OPV3Fully
vacci
nated
Cov
erag
e (%
)
40
80
120
160
200
240
280
Under−5
morta
lity
Und
er−5
mor
talit
y (d
eath
s per
1,0
00 li
ve b
irths
)
Year:
2000
2013
The horizontal line represents the median across districts. The thick vertical bar represents the interquartile range, while the thin vertical bar represents the range across districts.
3 Full Country Evaluation 2014
�
�
�
�
�
��
�
�
�
�
��
�
�
0.9
1.0
1.1
1.2
1.3
1.4
1.5
1989 1991 1993 1995 1997 1999 2001 2003 2005 2007
Year
Cov
erag
e ra
tio Group
�
�
Sex
Wealth
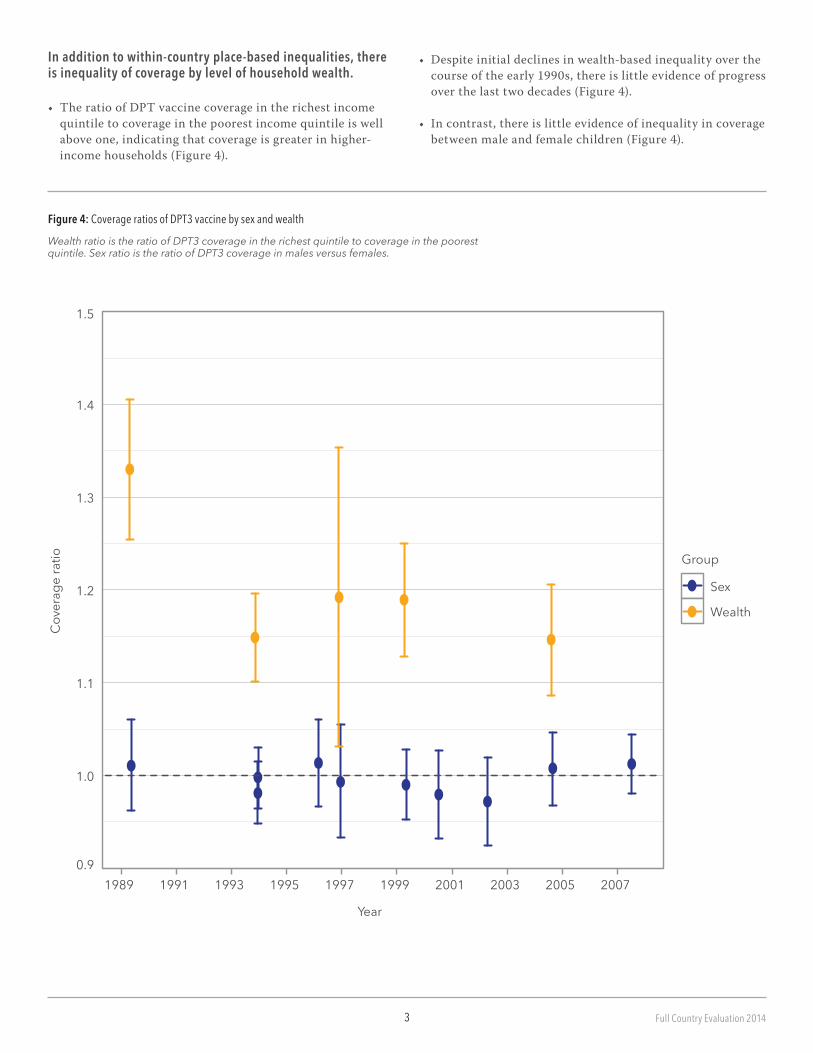
Figure 4: Coverage ratios of DPT3 vaccine by sex and wealth
Wealth ratio is the ratio of DPT3 coverage in the richest quintile to coverage in the poorest quintile. Sex ratio is the ratio of DPT3 coverage in males versus females.
In addition to within-country place-based inequalities, there is inequality of coverage by level of household wealth.
• TheratioofDPTvaccinecoverageintherichestincomequintile to coverage in the poorest income quintile is well above one, indicating that coverage is greater in higher- income households (Figure 4).
•Despiteinitialdeclinesinwealth-basedinequalityoverthecourse of the early 1990s, there is little evidence of progress over the last two decades (Figure 4).
•Incontrast,thereislittleevidenceofinequalityincoveragebetween male and female children (Figure 4).
4Full Country Evaluation 2014
40
80
120
160
200
240
2802000 2013
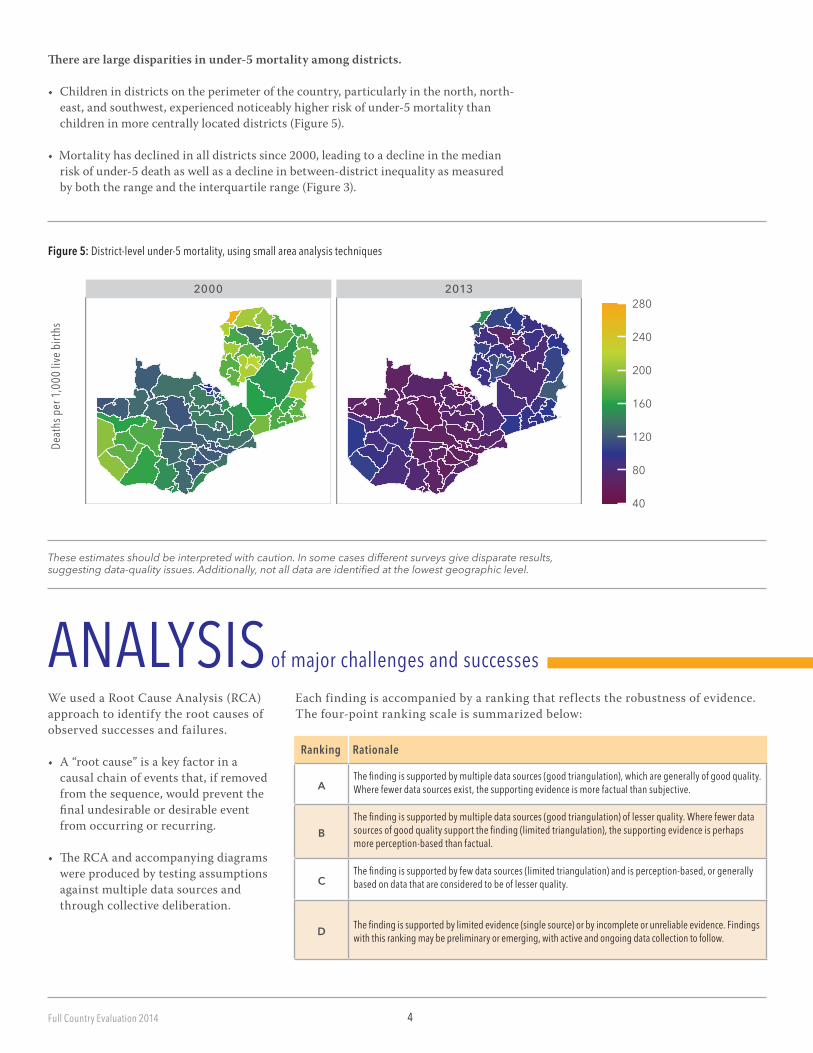
Figure 5: District-level under-5 mortality, using small area analysis techniques
There are large disparities in under-5 mortality among districts.
• Childrenindistrictsontheperimeterofthecountry,particularlyinthenorth,north-east,andsouthwest,experiencednoticeablyhigherriskofunder-5mortalitythanchildren in more centrally located districts (Figure 5).
•Mortalityhasdeclinedinalldistrictssince2000,leadingtoadeclineinthemedianriskofunder-5deathaswellasadeclineinbetween-districtinequalityasmeasuredby both the range and the interquartile range (Figure 3).
These estimates should be interpreted with caution. In some cases different surveys give disparate results, suggesting data-quality issues. Additionally, not all data are identified at the lowest geographic level.
Deat
hs p
er 1,
000 l
ive bi
rths
WeusedaRootCauseAnalysis(RCA)approach to identify the root causes of observed successes and failures.
• A“rootcause”isakeyfactorinacausal chain of events that, if removed from the sequence, would prevent the finalundesirableordesirableeventfrom occurring or recurring.
• TheRCAandaccompanyingdiagramswere produced by testing assumptions against multiple data sources and through collective deliberation.
Eachfindingisaccompaniedbyarankingthatreflectstherobustnessofevidence.Thefour-pointrankingscaleissummarizedbelow:
Ranking Rationale
ANALYSIS of major challenges and successes
AThe finding is supported by multiple data sources (good triangulation), which are generally of good quality. Where fewer data sources exist, the supporting evidence is more factual than subjective.
BThe finding is supported by multiple data sources (good triangulation) of lesser quality. Where fewer data sources of good quality support the finding (limited triangulation), the supporting evidence is perhaps more perception-based than factual.
CThe finding is supported by few data sources (limited triangulation) and is perception-based, or generally based on data that are considered to be of lesser quality.
D The finding is supported by limited evidence (single source) or by incomplete or unreliable evidence. Findings with this ranking may be preliminary or emerging, with active and ongoing data collection to follow.
5 Full Country Evaluation 2014
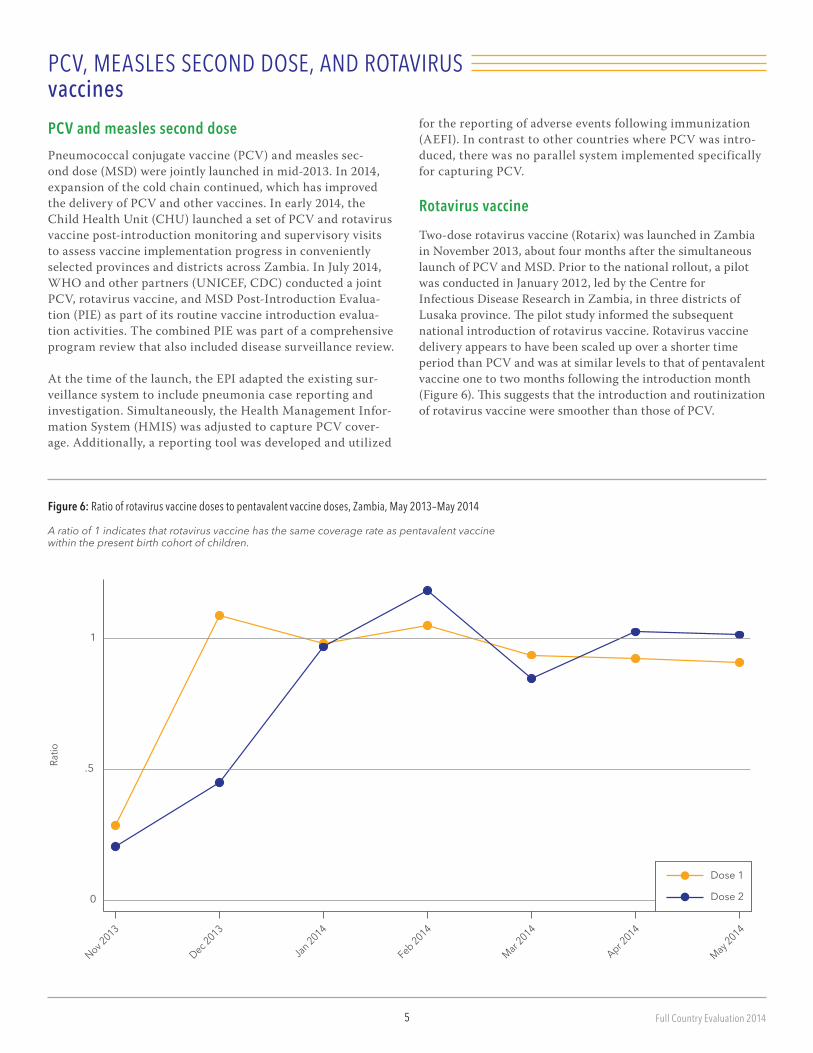
Figure 6: Ratio of rotavirus vaccine doses to pentavalent vaccine doses, Zambia, May 2013–May 2014
A ratio of 1 indicates that rotavirus vaccine has the same coverage rate as pentavalent vaccine within the present birth cohort of children.
PCV, MEASLES SECOND DOSE, AND ROTAVIRUS vaccines
PCV and measles second dosePneumococcal conjugate vaccine (PCV) and measles sec-onddose(MSD)werejointlylaunchedinmid-2013.In2014,expansion of the cold chain continued, which has improved the delivery of PCV and other vaccines. In early 2014, the ChildHealthUnit(CHU)launchedasetofPCVandrotavirusvaccine post-introduction monitoring and supervisory visits to assess vaccine implementation progress in conveniently selectedprovincesanddistrictsacrossZambia.InJuly2014,WHOandotherpartners(UNICEF,CDC)conductedajointPCV,rotavirusvaccine,andMSDPost-IntroductionEvalua-tion (PIE) as part of its routine vaccine introduction evalua-tion activities. The combined PIE was part of a comprehensive program review that also included disease surveillance review.
At the time of the launch, the EPI adapted the existing sur-veillance system to include pneumonia case reporting and investigation.Simultaneously,theHealthManagementInfor-mationSystem(HMIS)wasadjustedtocapturePCVcover-age. Additionally, a reporting tool was developed and utilized
0
.5
1
Ratio
Nov 2013
Dec 2013
Jan 2014
Feb 2014
Mar 2014
Apr 2014
May 2014
Dose 1
Dose 2
for the reporting of adverse events following immunization (AEFI). In contrast to other countries where PCV was intro-duced, there was no parallel system implemented specifically for capturing PCV.
Rotavirus vaccineTwo-doserotavirusvaccine(Rotarix)waslaunchedinZambiain November 2013, about four months after the simultaneous launchofPCVandMSD.Priortothenationalrollout,apilotwasconductedinJanuary2012,ledbytheCentrefor InfectiousDiseaseResearchinZambia,inthreedistrictsofLusakaprovince.Thepilotstudyinformedthesubsequentnational introduction of rotavirus vaccine. Rotavirus vaccine delivery appears to have been scaled up over a shorter time period than PCV and was at similar levels to that of pentavalent vaccine one to two months following the introduction month (Figure6).Thissuggeststhattheintroductionandroutinizationof rotavirus vaccine were smoother than those of PCV.
6Full Country Evaluation 2014
RECOMMENDATIONS1.InZambia,substantiallong-terminvestmentand
multi-sectorial involvement are required to develop more accurate estimates of target populations for measuring vaccine coverage and determining vaccine supply. In the nearerterm,theEPIprogramwithappropriatestakehold-ers,includingdistricts,CentralStatisticalOffice(CSO),andpartnerssuchasWHOandUNICEF,shouldidentifysolutions to mitigate the effect of inaccurate denominators leadingtovaccinestock-outs.
Root cause
Challenge
Consequence
Response
Success
Context
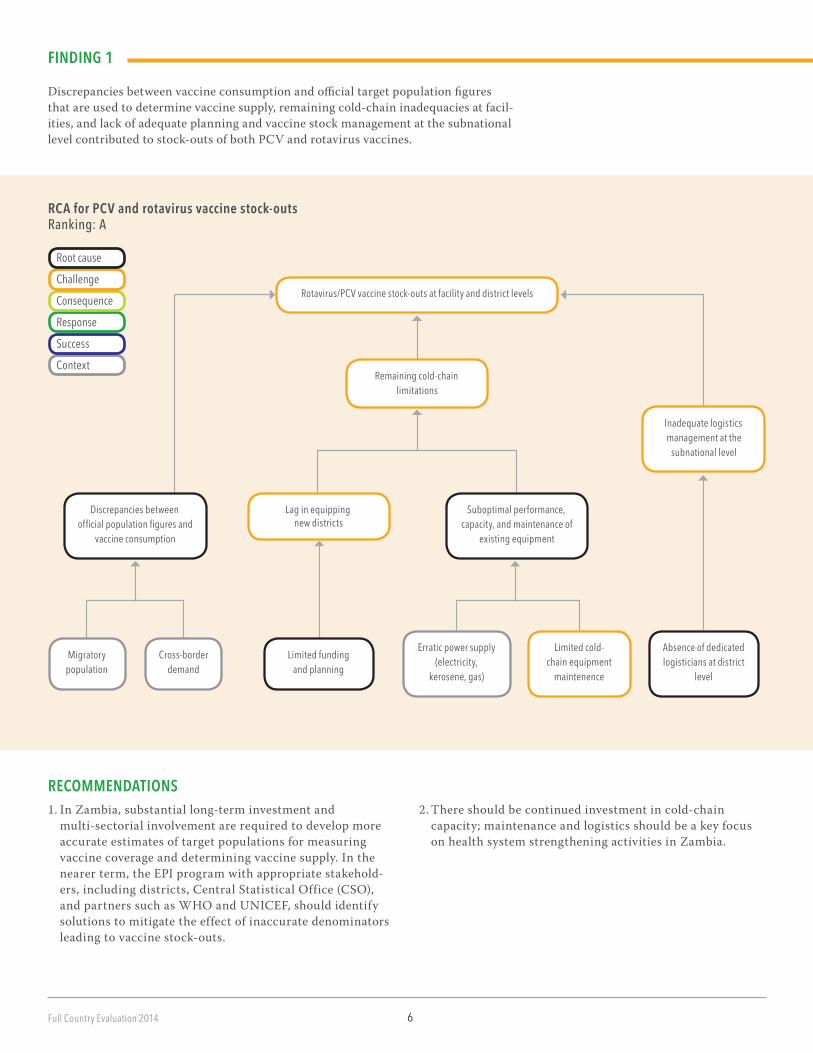
RCA for PCV and rotavirus vaccine stock-outs Ranking: A
FINDING 1
Discrepanciesbetweenvaccineconsumptionandofficialtargetpopulationfiguresthat are used to determine vaccine supply, remaining cold-chain inadequacies at facil-ities,andlackofadequateplanningandvaccinestockmanagementatthesubnationallevelcontributedtostock-outsofbothPCVandrotavirusvaccines.
2. There should be continued investment in cold-chain capacity;maintenanceandlogisticsshouldbeakeyfocusonhealthsystemstrengtheningactivitiesinZambia.
Rotavirus/PCV vaccine stock-outs at facility and district levels
Inadequate logistics management at the
subnational level
Discrepancies between official population figures and
vaccine consumption
Limited funding and planning
Absence of dedicated logisticians at district
level
Lag in equipping new districts
Suboptimal performance, capacity, and maintenance of
existing equipment
Remaining cold-chain limitations
Erratic power supply (electricity,
kerosene, gas)
Limited cold-chain equipment
maintenence
Migratory population
Cross-border demand

7 Full Country Evaluation 2014
RECOMMENDATIONDataqualityisakeyfocusofthelatestHSSsupportstream.Consistent with this focus and the findings of the evaluation, theupcomingapplicationforHSSinZambiashouldincludesubstantial investments to address the issue of data quality, including ensuring availability of forms and tools, as well as training to ensure accurate reporting.
FINDING 2
Ongoinglimitationsofthevaccinesurveillancesystem,includinglackoftoolsandformsatfacilitylevels,inaccuratedenominators,insufficienthealthworkertrain-ing,andincompletereporting,limittheabilityoftheEPIprogramtotracktherollout of PCV and rotavirus vaccine in terms of vaccine coverage, adverse events, and other indicators.
RCA for vaccine data quality challenges Ranking: A
Root cause
Challenge
Consequence
Response
Success
Context
Vaccine data quality challenges
Internally migrating populations
Border-crossing populations
Insufficiently trained health
workers
Unavailability of official reporting forms and vaccination cards
Health workers unwilling to report
Discrepancies between official population figures and vaccine
consumption patterns
Incomplete reporting and suboptimal response rate in
administrative system
Inaccurate vaccine coverage data
Inadequate adverse event following immunization (AEFI) reporting mechanisms
8Full Country Evaluation 2014
RECOMMENDATION
EPI programs, country-partners, and Gavi should ensure that learning experiences are maximized for new vaccine introductions. Learning from previous introductions should be based on robust post-launch monitoring and evalua-tion, including post-introduction evaluations. This should also include sufficient time between introductions to allow
Root cause
Challenge
Consequence
Response
Success
Context
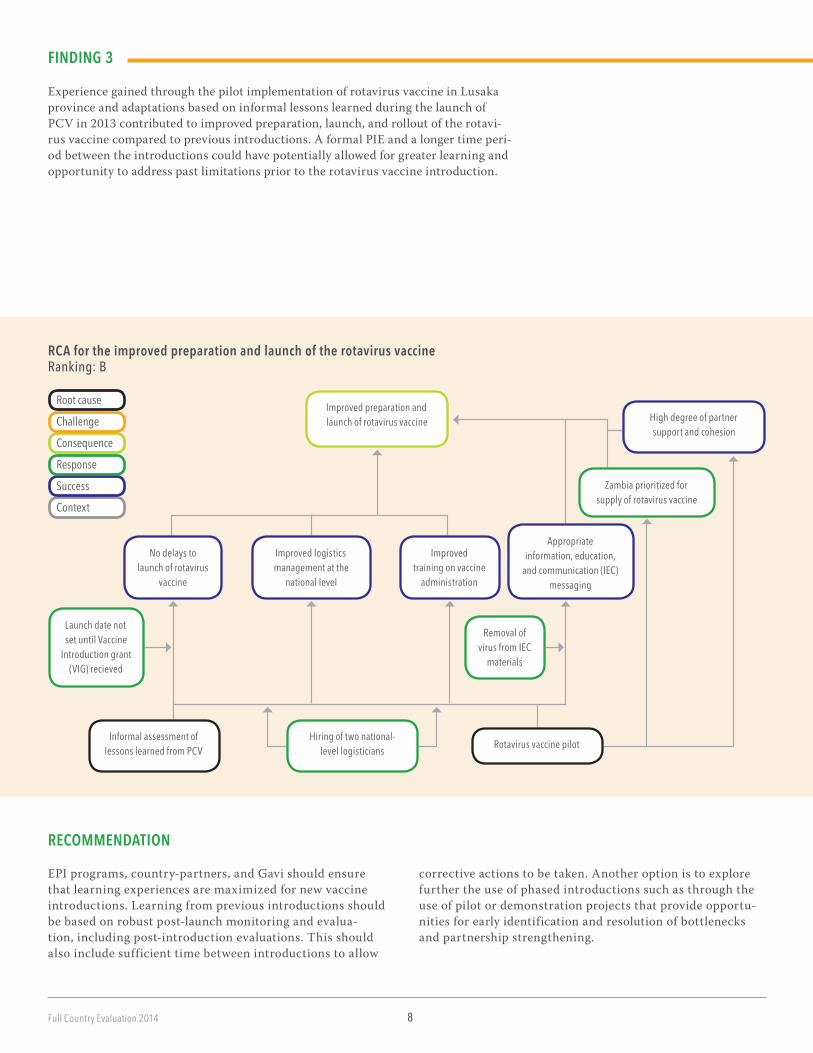
RCA for the improved preparation and launch of the rotavirus vaccine Ranking: B
FINDING 3
ExperiencegainedthroughthepilotimplementationofrotavirusvaccineinLusakaprovince and adaptations based on informal lessons learned during the launch of PCV in 2013 contributed to improved preparation, launch, and rollout of the rotavi-rus vaccine compared to previous introductions. A formal PIE and a longer time peri-od between the introductions could have potentially allowed for greater learning and opportunity to address past limitations prior to the rotavirus vaccine introduction.
correctiveactionstobetaken.Anotheroptionistoexplorefurther the use of phased introductions such as through the use of pilot or demonstration projects that provide opportu-nitiesforearlyidentificationandresolutionofbottlenecksand partnership strengthening.
Improved preparation and launch of rotavirus vaccine
Zambia prioritized for supply of rotavirus vaccine
Improved training on vaccine
administration
Launch date not set until Vaccine
Introduction grant (VIG) recieved
Informal assessment of lessons learned from PCV
Hiring of two national-level logisticians
No delays to launch of rotavirus
vaccine
High degree of partner support and cohesion
Appropriate information, education,
and communication (IEC) messaging
Improved logistics management at the
national level
Removal of virus from IEC
materials
Rotavirus vaccine pilot

9 Full Country Evaluation 2014
Delayed application
Unclear writing roles and responsibilities
Late recruitment of consultant
Coordination and communication challenges
between partners
Roles and responsibilities for HSS structured differently than for New Vaccine Support (NVS)
Orientation and training by WHO of stakeholders in
HSS application process
Ongoing adaptation to ministerial realignment
RECOMMENDATION
MCDMCHshouldidentifyadedicatedpointpersonwithinthe Department of Planning and Information to coordinate theapplicationoftheHSSgrantinZambia.
CASH-BASED SUPPORT: Health System Strengthening
ThegovernmentofZambiabegantoimplementtheinitialHealthSystemStrengthening(HSS)grantprogramin2008.However,theprogramcouldnotbecompletedduetothefreezing of funds following alleged financial irregularity in theMinistryofHealth.Later,thegovernmentofZambiawasgiven the option to either reprogram the grant for the undis-bursed funds or submit an application for a new grant. The government opted to submit a new application. An Expres-sionofInterest(EOI)toapplyforGaviHSSsupportwassub-sequentlysubmittedinMay2014.ThegovernmenthadaimedtosubmittheapplicationintheSeptember2014application
Root cause
Challenge
Consequence
Response
Success
Context
RCA for the delayed application for HSSRanking: C
window.However,thisdatewasnotmet,andtheapplicationwas expected to be submitted in the first quarter of 2015.
FINDING 1Coordination challenges stemming from the different part-nershipstructureforHSScomparedtonewvaccineintro-ductions,limitedexperiencewiththenewHSSapplicationprocess, and multiple competing priorities led to a revision of thetimelinefortheHSSapplicationsubmissionfromSep-tember2014toJanuary2015.
Competing priorities for the government of Zambia and other
stakeholders
Limited experience in HSS application process
10Full Country Evaluation 2014
UPCOMING areas of evaluation
CROSS-STREAM findings for Zambia
Inactivated polio vaccine
ThegovernmentofZambiathroughMCDMCHsubmittedanEOI for IPV to the Interagency Coordinating Committee for endorsementinMay2014.Afteritwasapproved,asmallteamrepresentingMCDMCH,WHO,andUNICEFbeganprepar-ing the full IPV proposal. Technical support was provided by WHOandUNICEFinSeptember2014,througharegionalworkshopforthedevelopmentofIPVapplications.ThefullapplicationwassubmittedinSeptember2014.TherevisionoftheComprehensiveMulti-yearPlanwasfinalizedinearlySeptember2014andincludedtheintroductionofIPVin2015.
Vaccine data qualityData-quality issues affected the availability of vaccines.
• ThevolumeofvaccinesreceivedbythegovernmentofZambiaandtheallocationofthesevaccinestodistrictsandfacilitiesisbasedonofficialCentralStatisticalOffice(CSO)figuresofvaccine-eligiblechildren.
• DuetopatternsofseasonalmigrationofpopulationswithinandintoZambia,vaccineconsumptiondiffersfromCSOfig-ures, with health facilities experiencing higher vaccine demand than the allocated amount. Combined with transportation challenges,vaccineswerestocked-outinthefacilities.
Data-quality issues affected the accurate surveillance of vaccine coverage and adverse events following immunization (AEFI).
• Dataqualityofvaccineadministrationwassuboptimaldueeither to absent or incomplete reporting or absence of official formsforvaccineandAEFIsinasignificantproportionofhealth facilities.
• Dataonvaccineadministrationweremissingforcertainperi-odsintheHealthManagementInformationSystem(HMIS)at many facilities.
• SomefacilitiesdidnothaveasysteminplacetoreportAEFIs,orhealthworkersavoidedreportingthemforfearofbeingthe cause behind the adverse event.
• HSSprovidesanopportunitytoaddressthesevaccinedata-qualitychallenges,includingstrengtheningHMISthroughsystem expansion, training, data management, and analysis.
The Full Country Evaluation will investigate the IPV decision and application development process in the near future, following up on these key issues:
• TheinfluenceoftheGovernmentofZambia,globalstake-holders,andinternationalstakeholdersinthisapplication.
• TheinfluenceofthetimeandresourcesdevotedtoIPVonthepreparationoftheHSSproposal,giventhatthecoreteam was the same for both applications.
• Theextentofstakeholderconsultationinproposaldevelopment.
Human resourcesHealth worker shortages, in terms of both quantity and skill level, affect not only the EPI, but the entire health system. • Atthenationallevel,limitedprogramstaffatMCDMCHmustmanagehighworkloadswithmanycompetingpriorities.
• Atthesubnationallevel,theabsenceoflogisticianscontrib-utedtogapsinlogisticsmanagement.However,thehiringoftwo national-level logisticians with support from the Centre forInfectiousDiseaseResearchinZambia(CIDRZ)easedtheburdenoflogisticsmanagementonotherstaffandimprovedlogistics management generally at the national level.
• BuildingcapacityofhealthworkersthroughtrainingmaybeanareaofinvestmentforHSS.
Cold chainZambia has achieved accelerated expansion of the cold chain in the past two years with significant partner support.
• TheJapanInternationalCooperationAgency(JICA)andCIDRZwereinstrumentalinprovidingfundsforthepro-curement and installation of cold chain equipment at both the national and subnational levels.
Despite improvements, there are severe, persistent challenges in many districts’ cold chains, which have incapac-itated the effective management of vaccine stocks in general.
• Erraticpowersupply,lackoftimelymaintenanceservices,and the absence of vaccine storage equipment in many facili-tiescontributedtothefailuretostockvaccinesinmanyfacil-ities and the interruption of immunization service delivery.

11 Full Country Evaluation 2014
The challenges surrounding the cold chain are critical bottle-necks in health system delivery in the HSS application that is under development and are likely to be an area of further investment.
• Vaccineintroductiongrantsdidnotproveenoughtosolvethecold-chainproblems;asuccessfulapplicationforHSSwillprovide an opportunity for the improvement of cold-chain capacity in the country.
Partnership
Clarity in roles and responsibilities of partners in the prepa-ration and launch of rotavirus vaccine was crucial to the smooth launch and roll out of the vaccine.
• Thisstrongpartnershipmaybeduetothelearningandexpe-rience from partnership in the pilot of the rotavirus vaccine, or tothestrongleadershiproleCIDRZplayedintheimplementa-tionandinsupportingMCDMCHinpreparingfortherollout.
CONCLUSIONS
Lack of clarity about the roles and responsibilities of partners in developing the HSS application delayed the development and submission of an HSS application.
• ThoughrelevantpartnershipdevelopedaroadmapfortheHSSapplication,weakcoordinationandcommunicationbetween partners contributed to delays in development and submission.
The value of Gavi partnership at the country level is a key theme for evaluation.
• Partnershiphasarecognizedcontributioninthecontextof the new vaccine- and cash-based streams of support and willbeakeyareaforfurtherinvestigation,especiallyinthecontextoftheongoingHSSapplicationdevelopment.
In 2013, Zambia expanded its vaccination program substan-tially with support from Gavi.
• ThegovernmentofZambiahasnowintroducedthreenewvaccineswithsupportfromGavi:PCV,MSD,androtavirusvaccines.
• BothPCVandrotavirusvaccinewereroutinizedfairlyquicklyfollowingtheirrespectivenationallaunches.Thescale-up of rotavirus was notably faster than that of PCV.
• Atthesubnationallevel,PCVandrotavirusvaccineswerewell-received and integrated into the local immunization programs, and their delivery benefits from annual govern-ment planning and budgeting.
Gavi support is generally well aligned with Zambia’s priori-ties, which are described in the national health strategic plan and the Comprehensive Multi-Year Plan (cMYP), and contrib-ute to Zambia’s priority of accelerating reductions in child mortality.
• ThecMYPwasrevisedtoincludeIPVjustpriortotheapplication for Gavi support.
• PneumoniaanddiarrheaareleadingcausesofchilddeathsinZambia;theintroductionandroutinizationofPCVandrotavirusvaccinearelikelycontributingtothecountry’sefforts toward reducing child mortality.
Gavi support to Zambia is implemented with a network of local partners.
• Allplanningandimplementationactivitieswere undertakenwithsupportfromcountrypartners.
• Gavi’ssupportplayedacatalyticroleinsecuringsupportfrom local donors to support the cold chain and other com-ponentsoftheEPI:
SupportfromJICAandCIDRZforthecoldchainiswelldocumented.
National logistics planning and management were boosted by the addition of two national-level logisticians basedatCHU,oneofwhomwasfundedbyCIDRZ.
The FCE suggests that there was a stronger and broader partnership around the rotavirus vaccine introduction compared to previous introductions.
A number of challenges in the EPI remain, and fully reaching the target population is constrained by persistent deficien-cies of the immunization system.
• Monitoringanddemandforecastingarehamperedbydata-quality issues.
• Althoughthecoldchainwasexpandedaroundtheintro-duction of PCV and rotavirus vaccine, it remains inad-equate at the subnational level and is compounded by breakdownsinthecoldchain.

12Full Country Evaluation 2014
• Thereisalackoftrainedlogisticiansatthesubnationallevel to manage logistics planning and management.
• Thereisanoverallshortageofstafftodeliverimmuniza-tions, especially in rural areas.
• ThevaccineintroductiongrantprovidedbyGaviremainsinadequate to cover all these deficiencies, and these are all keyareasoffocusthatwerecommendforhealthsystemstrengthening activities, especially given the upcoming HSSapplication.
There is limited use of monitoring and evaluation tools to inform policy and program performance.
• ThereislittleregularfeedbackfromthesurveillanceunitsituatedattheUniversityTeachingHospitaltotheplan-ningdepartmentintheMCDMCH.
• DuringtheTechnicalWorkingGroupmeetings,thereislowemphasis on accessing regular reports to facilitate monitor-ing of program performance to inform program implemen-tation, indicating the perception of low data quality.
• Thisisanimportantareaforfutureinvestment.
POSITIVE AND NEGATIVE unintended consequences of Gavi support in ZambiaNew vaccine support stimulated local donors to provide funding to the EPI.
• Fundingforcold-chainexpansion,supportforsurveillancefor diarrheal diseases, and national-level training were examples of this support.
There was not enough time to perform a formal evaluation of the PCV/MSD introduction to inform the introduction of rotavi-rus vaccine and to implement solutions for evaluation- identified deficiencies.
• TheintroductionofseveralnewvaccinesbyZambiawiththe support of Gavi over a short time period was a notable achievement and will contribute to averted burden of vaccine-preventable disease.
• However,therewasinsufficienttimetoformallyevaluatethePCV/MSDintroduction,solessonsfromthisexperiencedid not inform the introduction of rotavirus vaccine or lend to the implementation of solutions for evaluation-identified deficiencies.
Prioritization of activities related to the new vaccine applica-tion, introduction, and routinization process likely contribut-ed to delays in the HSS process.
• ThedevelopmentoftheIPVapplicationtookpriorityovertheHSSapplicationandwasfinalizedandsubmitted,whiletheHSSapplicationwasdeferredtoalaterdate.
• Consequently,criticalinvestmentstostrengthentheimmunization programs and facilitate smoother introduc-tions were delayed.
• Itisimportantthatambitiousprogrammaticgoalsandplans are balanced with effective technical capacity and implementation.

Full Country Evaluation 2014
TIMELINE of major immunization events in Zambia20
1220
1320
14
Ministerial realignment, Ministry of Community Development, Mother and Child Health (MCDMCH) created
Gavi approved New Vaccine Support (NVS) for rotavirus vaccine
PCV arrived in Zambia central stores
Training of Trainers implemented; PCV shipping to districts began
Social mobilization for PCV launched
National launch of PCV
Training of Trainers
National launch of rotavirus vaccine
Post-launch monitoring and supervisory visits
Post-Introduction Evaluation
Decision to postpone application to 2015 window
Draft HSS proposal presented to stakeholders by consultant from Malawi
The internal appraisal notes an Effective Vaccine Management Assessment (EVMA) planned
Revision of Comprehensive Multi-year Plan (cMYP) finalized, which included the introduction of IPV in 2015; IPV application submitted
Rapid assessment of stocks, vaccine management, and cold-chain status
HSS orientation workshop and proposal to make new application by Technical Working Group (TWG)
Decision to make new application in 2014 endorsed by Interagency Coordinating Committee (ICC); Expression of Interest (EOI) for HSS submitted to Gavi
Through MCDMCH, Zambia submitted an EOI for IPV to the ICC for endorsement
Post-launch monitoring and supervisory visits
Post-Introduction Evaluation
PCV Vaccine Introduction Grant (VIG) arrived in country (disbursed to UNICEF and WHO)
JAN
FEB
MAR
APR
MAY
JUN
JUL
AUG
SEPT
OCT
NOV
DEC
JAN
FEB
MAR
APR
MAY
JUN
JUL
AUG
SEPT
OCT
NOV
DEC
JAN
FEB
MAR
APR
MAY
JUN
JUL
AUG
SEPT
OCT
NOV
DEC
Streams of support evaluated in 2014
Implementation of pneumococcal conjugate vaccine (PCV)
Rotavirus vaccine
Cash-based support through Health System Strengthening (HSS)
Inactivated polio vaccine (IPV)
Not vaccine-specific
NVS for PCV was approved by Gavi on Septem-ber 26, 2011. The proposal was submitted on June 11, 2011. NVS for rotavirus vaccine was ap-proved by Gavi on April 12, 2012; the application was submitted November 15, 2011. ISS support was approved by Gavi on April 21, 2009. HSS support was approved on August 1, 2007; the application was submitted in May 2007. EVMA occurred in July 2011.
