zachariah influenza -...
TRANSCRIPT
3/2/2014
1
Joseph K. Zachariah D.O.
Private Practice in Infectious Disease – Hospital Based
Banner Baywood Hospital, MESA ,AZ
Founder & Director: Travelhealthadvisor.com
(Interactive Web based Medical Recommendations for Overseas Travel)
“Just as the day is light and night is dark ;
Winter brings us the malady, they call the flu”
Unknown
Please ladies ; this is not my good side !
3/2/2014
2
Impact of Seasonal Influenza in the US
35 – 50 million cases / year
200,000 hospital admissions / year
3000 – 40,000 deaths /year
31 million outpatient doctor visits / year
3.1 million hospital days/ year
$10.4 billion in medical costs/ year
$16.3 billion in lost earnings / years
Vaccine 2007:25; 5086-5096
JAMA 2004: 292(11) 1333-40
Please ladies ; this is not my good side !
Please ladies ; this is not my good side !
3/2/2014
3
Impact of Seasonal Influenza in the US
Estimate of age adjusted Mortality
Age Number Rate
<19 124/yr 0.2/100,000
19-64 2385/yr 1.5/100,000
> 65 21,098/yr 66.1/100,000
Deaths among people over 65 years of age – 89% of all influenza
associated deaths
MMWR 2010:59(33)1057-62
Please ladies ; this is not my good side !
Influenza Virus Composition : 2013-2014
N=36,619 Respiratory Specimens
Influenza A – 97%
H1N1 - 96%
H3N2 - 3.7%
3/2/2014
4
.
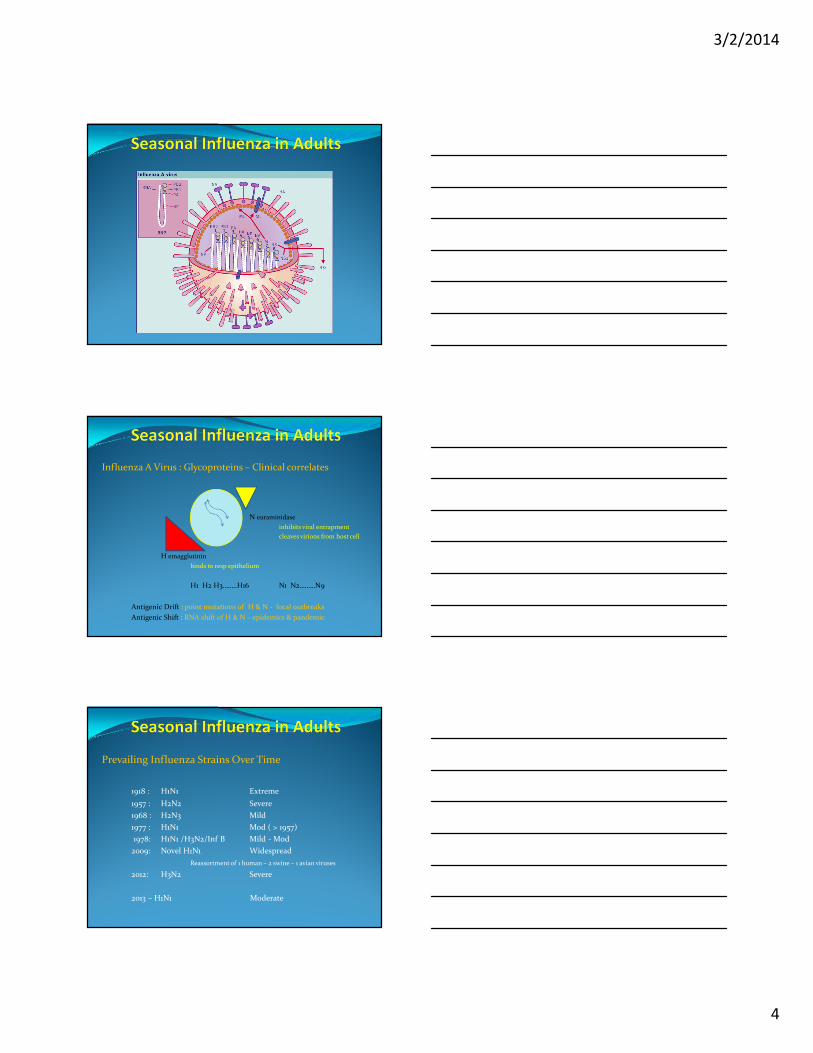
Influenza A Virus : Glycoproteins – Clinical correlates
N euraminidase
inhibits viral entrapment
cleaves virions from host cell
H emagglutinin
binds to resp epithelium
H1 H2 H3……..H16 N1 N2………N9
Antigenic Drift : point mutations of H & N - local outbreaks
Antigenic Shift : RNA shift of H & N – epidemics & pandemic
Prevailing Influenza Strains Over Time
1918 : H1N1 Extreme
1957 : H2N2 Severe
1968 : H2N3 Mild
1977 : H1N1 Mod ( > 1957)
1978: H1N1 /H3N2/Inf B Mild - Mod
2009: Novel H1N1 Widespread
Reassortment of 1 human – 2 swine – 1 avian viruses
2012: H3N2 Severe
2013 – H1N1 Moderate

3/2/2014
5
Influenza Viral Characteristics -2013-14
R – Oseltamivir Zanamivir
h1n1 0.8% 0
h3n2 0 0
Infl B 0 0
cdc.gov/flu/week – 3/2/2013
Time Course of Influenza
Abrupt Onset
Peaks in 2-3 weeks
Lasts for 2-3 months
Earliest Indicators
Febrile Respiratory Illness in Children
Attack Rates : 10 -20 % of general population
50% in selected populations
Number of Febrile Respiratory Illnesses Studied from Selected Primary-Care Facilities and Number Positive for Influenza A Viruses According to Week, Houston, 1975–76.
Glezen WP et al. N Engl J Med 1978;298:587-592.

3/2/2014
6
Transmission
Large Particle Droplets - > 5 micron / 6 foot radius
Coughing
Sneezing*
Talking
Contaminated surfaces - 2 to 8 hours
Possibly Small droplets – Remain in air for extended periods
Trans ocular entry
Brankston G,Lancet Inf Dis ;2007:257
Blachere FM,CID;2009:48:438
Wong BC,CID:2010;51:1176
Noti JD,CID;2012:54:1569
Incubation:
Average : 2 days ( 1-4 days)
Secondary attack rate : 25% among household
Onset of ILI in household : 3-4 days
Killingley B, JID;2012:205:35
Cowling BJ, NEJM;2010:362:2175
Duration of Viral Shedding in Secretions
Onset : 24 hours before clinical symptoms
Peak : 48 -72 hours after clinical symptoms
Duration : 5 days
Cleared : From day 7 on ( symptoms may last 10 days)
Longer duration of shedding : children , elderly, chronic illness
F Currant, Am J Epid 2008;167:775
3/2/2014
7
Clinical Symptoms & Findings
Symptoms – Abrupt onset
Headache, myalgias, malaise, dry cough, sore-throat, nasal drainageExam
Hot & flushed, febrile, hyperemia of pharynx, mild cervical nodes
Cough 5.4 OR (3.8-7.7 ci)
Fever 3.8 OR ( 2.8-5.0 ci)
Malaise 2.6 OR ( 2.2-3.1 ci)
Chills 2.6 2.6 ( 2.0-3.3 ci)
Sneezing <<<< less likely to be influenza
Call SA, JAMA 2005;293:987
Laboratory Testing
TEST TIME COMMENTS
Rapid Antigen Tests 15 -30 min Low Sensitivity 50-65%
Immunofluorescence 2-4 hours* Mod Sensitivity 65-80%
RT-PCR 2-6 hours * High Sensitivity /High Specificity
Viral Culture 3-10 days Mod Sensitivity/High Specificity
Serology ( Antibody) ** Not useful in acute setting
Specimen: Nasopharyngeal wash > NP swab>Pharyngeal swab
Timing: 24-48 hours of illness
Concentration: Earlier in illness – higher viral load
.
3/2/2014
8
Test and Treat or Should You Just Treat ??
Pretest Probability
If > 30 -40% : Just treat if symptoms are suggestive
If it is flu season in your state or county and symptoms are classic
Interpretation
True (+) : Positive screening test during Peak Influenza Season
False (-) : Negative screening test during Peak Influenza Season
“A Doctor can cure the flu in fourteen days
Leave it alone and it goes away in two weeks”
Unknown
Treatment - Neuraminidase Inhibitors
Oseltamivir
Decreases duration of illness by 24 hours
May decrease LRI needing antibiotics
May decrease hospitalizations
May decrease mortality
Need to treat within 24 -36 hours of symptoms
Dose : 75mg bid x 5 days ( 150 mg )
Capsule,Powder or Solution
Side effects : ? Delerium in children ( <<<)
3/2/2014
9
Treatment – Neuraminidase Inhibitor
Zanamivir
Decreases duration of illness
by 1.3 days in < 65 years
by 2 days in > 65 years
Decreases LRI needing antibiotics
Need to initiate therapy within 36 hours of symptoms
Inhalation : 10 mg bid x 5days
Intranasal : 6.4 mg qd x 5days
Side effects : Bronchospasm
Treatment – Neuraminidase Inhibitors
Pregnancy : category C
Risk of Influenza is greater than risk of medication
Treat with oseltamivir
Treat fever ( risk of neural tube defects-siezure-cp)
Treatment : Targeted groups
Residents of SNF / group homes
Age > 65
Pregnant / 2 weeks post partum
COPD
CHF / CAD
Diabetes Mellitus
Hemoglobinopathies
HIV with cd4 <200
Transplant patients
Inflammatory Bowel Disease
Immunosuppressive Medications
Neurologic Conditions that impair Respiratory function
BMI > 35
Splenectomy
3/2/2014
10
Treatment :
Any one presenting within 48 hours of illness
Those presenting after 48 hours of illness
with prior risk factors
requiring hospitalization
Vaccine Effectiveness in Healthy Adults
N = 849
Age : 18 – 64 years
Vaccine group
Upper Respiratory Illness < 25% p 0.001
Sick leave < 43% p 0.001
Doctor Visits < 44% p 0.004
NEJM 1995:333(14) 889-893
Vaccinations - How effective are influenza vaccines?
Need for Antigenic Match – Belongia EA, JID 2009;199:159
2004-05 Ag Match 5% 10% effective
2006-07 Ag Match 91% 52% effective
Endpoint Measured – Osterholm MI, Lancet ID 2012;12:36
Serology 70-90% effective
Lab confirmed Influenza 59% effective
Effectiveness of 2012-13 vaccine – ` cdc.gov/3/1/2014
Lab confirmed Influenza 62% effective
52% effective > 65 yr
,
3/2/2014
11
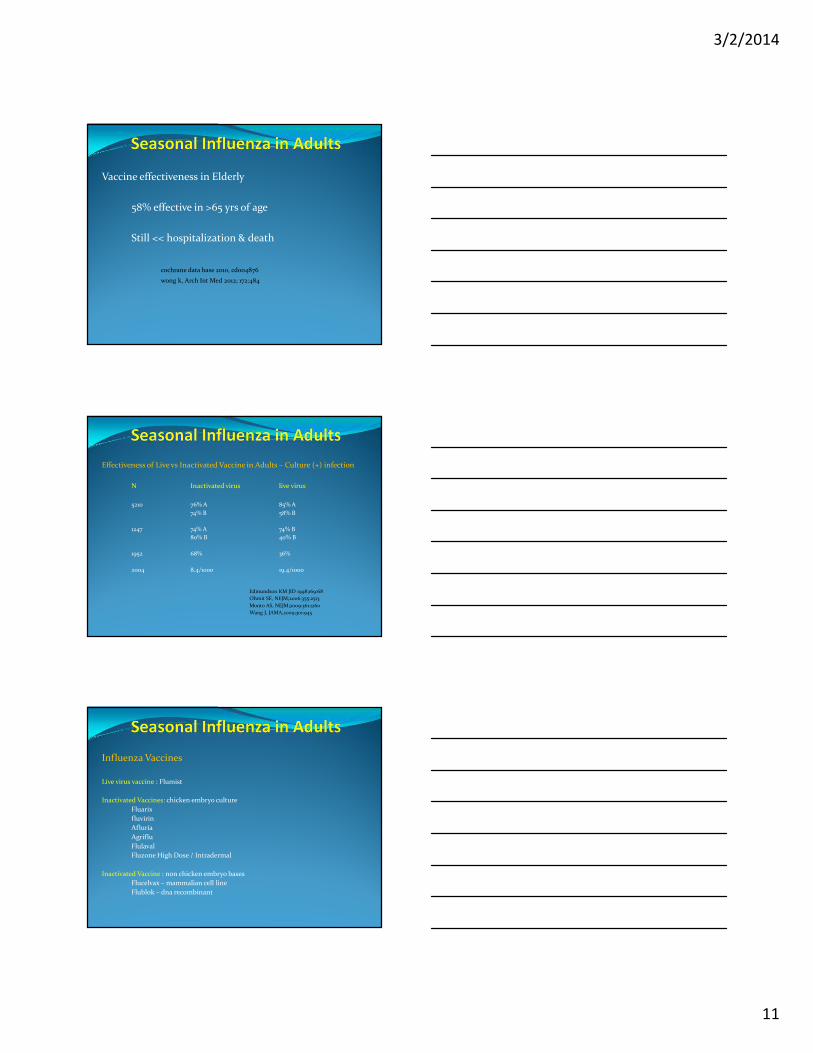
Vaccine effectiveness in Elderly
58% effective in >65 yrs of age
Still << hospitalization & death
cochrane data base 2010, cd004876
wong k, Arch Int Med 2012; 172:484
Effectiveness of Live vs Inactivated Vaccine in Adults – Culture (+) infection
N Inactivated virus live virus
5210 76% A 85% A
74% B 58% B
1247 74% A 74% B
80% B 40% B
1952 68% 36%
2004 8.4/1000 19.4/1000
Edmundson KM JID 1998;169:68
Ohmit SE, NEJM;2006:355:2513
Monto AS, NEJM;2009:361:1260
Wang J, JAMA,2009;301:945
Influenza Vaccines
Live virus vaccine : Flumist
Inactivated Vaccines: chicken embryo culture
Fluarix
fluvirin
Afluria
Agriflu
Flulaval
Fluzone High Dose / Intradermal
Inactivated Vaccine : non chicken embryo bases
Flucelvax – mammalian cell line
Flublok – dna recombinant
3/2/2014
12
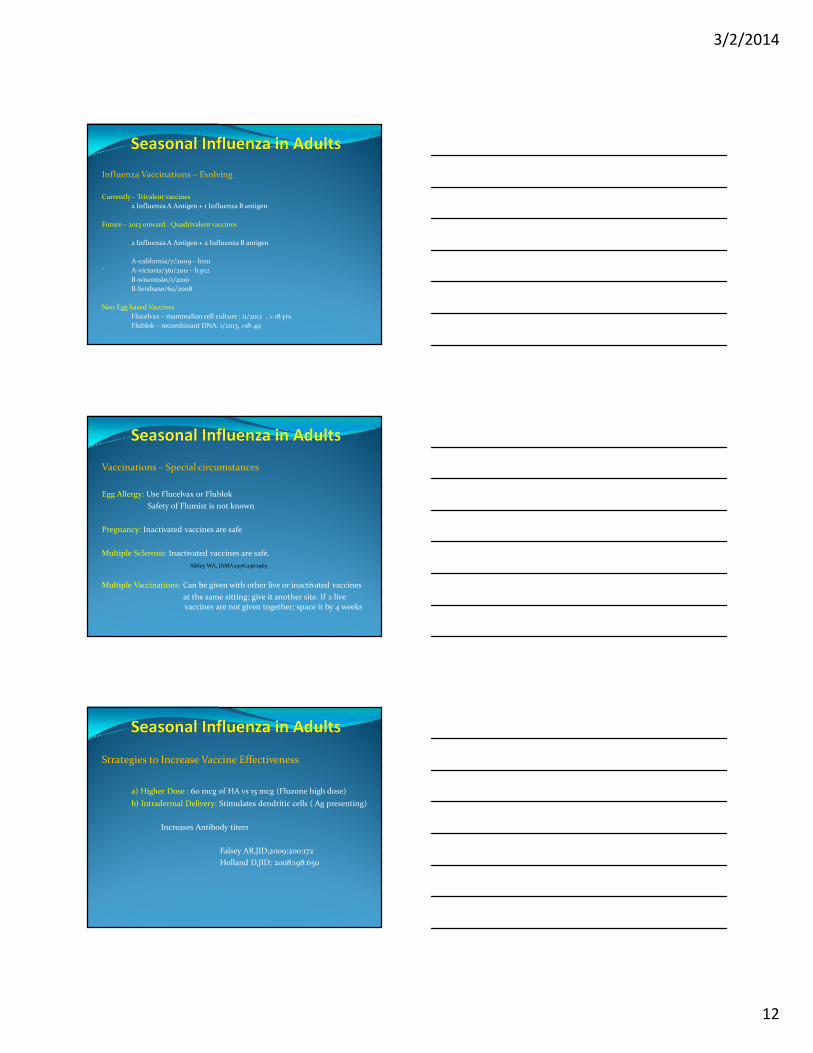
Influenza Vaccinations – Evolving
Currently – Trivalent vaccines
2 Influenza A Antigen + 1 Influenza B antigen
Future – 2013 onward : Quadrivalent vaccines
2 Influenza A Antigen + 2 Influenza B antigen
A-california/7/2009 – h1n1
` A-victoria/361/2011 – h3n2
B-wisconsin/1/2010
B-brisbane/60/2008
Non Egg based Vaccines
Flucelvax – mammalian cell culture : 11/2012 , > 18 yrs
Flublok – recombinant DNA: 1/2013, >18-49
Vaccinations – Special circumstances
Egg Allergy: Use Flucelvax or Flublok
Safety of Flumist is not known
Pregnancy: Inactivated vaccines are safe
Multiple Sclerosis: Inactivated vaccines are safe.
Sibley WA, JAMA:1976;236:1965
Multiple Vaccinations: Can be given with other live or inactivated vaccines
at the same sitting; give it another site. If 2 live vaccines are not given together; space it by 4 weeks
Strategies to Increase Vaccine Effectiveness
a) Higher Dose : 60 mcg of HA vs 15 mcg (Fluzone high dose)
b) Intradermal Delivery: Stimulates dendritic cells ( Ag presenting)
Increases Antibody titers
Falsey AR,JID;2009:200:172
Holland D,JID; 2008:198:650
3/2/2014
13
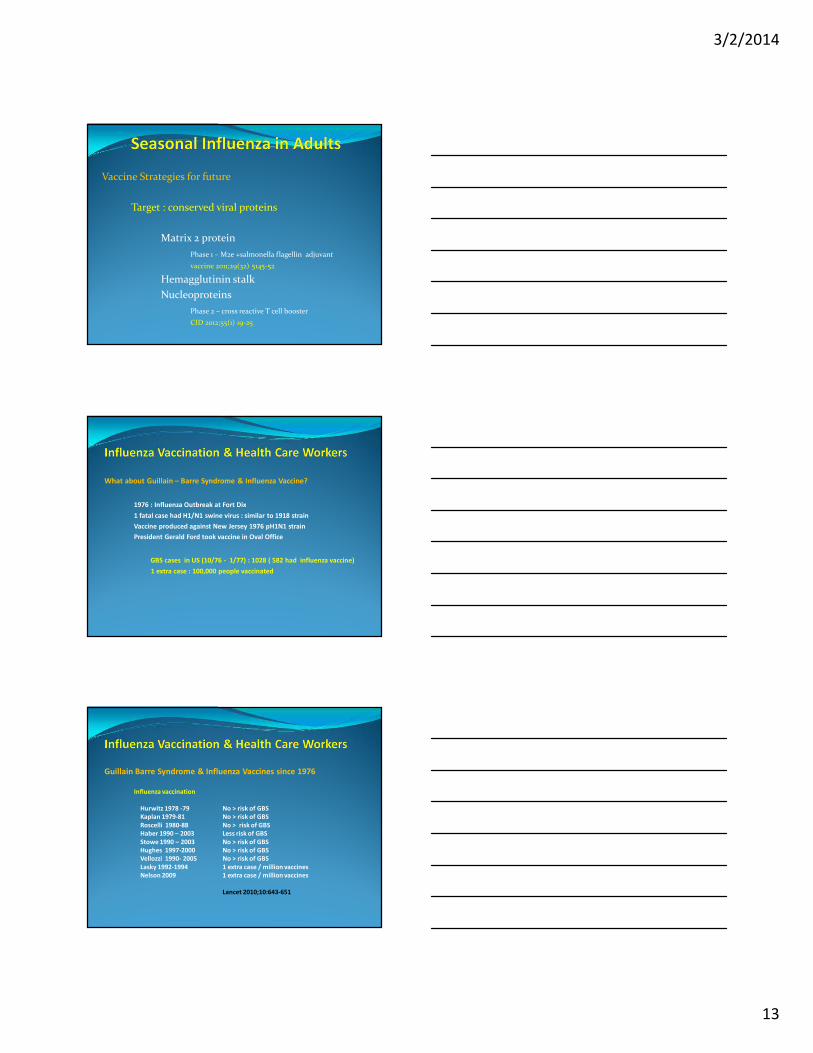
Vaccine Strategies for future
Target : conserved viral proteins
Matrix 2 protein
Phase 1 – M2e +salmonella flagellin adjuvant
vaccine 2011;29(32) 5145-52
Hemagglutinin stalk
Nucleoproteins
Phase 2 – cross reactive T cell booster
CID 2012;55(1) 19-25
What about Guillain – Barre Syndrome & Influenza Vaccine?
1976 : Influenza Outbreak at Fort Dix
1 fatal case had H1/N1 swine virus : similar to 1918 strain
Vaccine produced against New Jersey 1976 pH1N1 strain
President Gerald Ford took vaccine in Oval Office
GBS cases in US (10/76 - 1/77) : 1028 ( 582 had influenza vaccine)
1 extra case : 100,000 people vaccinated
Guillain Barre Syndrome & Influenza Vaccines since 1976
Influenza vaccination
Hurwitz 1978 -79 No > risk of GBS
Kaplan 1979-81 No > risk of GBS
Roscelli 1980-88 No > risk of GBS
Haber 1990 – 2003 Less risk of GBS
Stowe 1990 – 2003 No > risk of GBS
Hughes 1997-2000 No > risk of GBS
Vellozzi 1990- 2005 No > risk of GBS
Lasky 1992-1994 1 extra case / million vaccines
Nelson 2009 1 extra case / million vaccines
Lancet 2010;10:643-651
3/2/2014
14
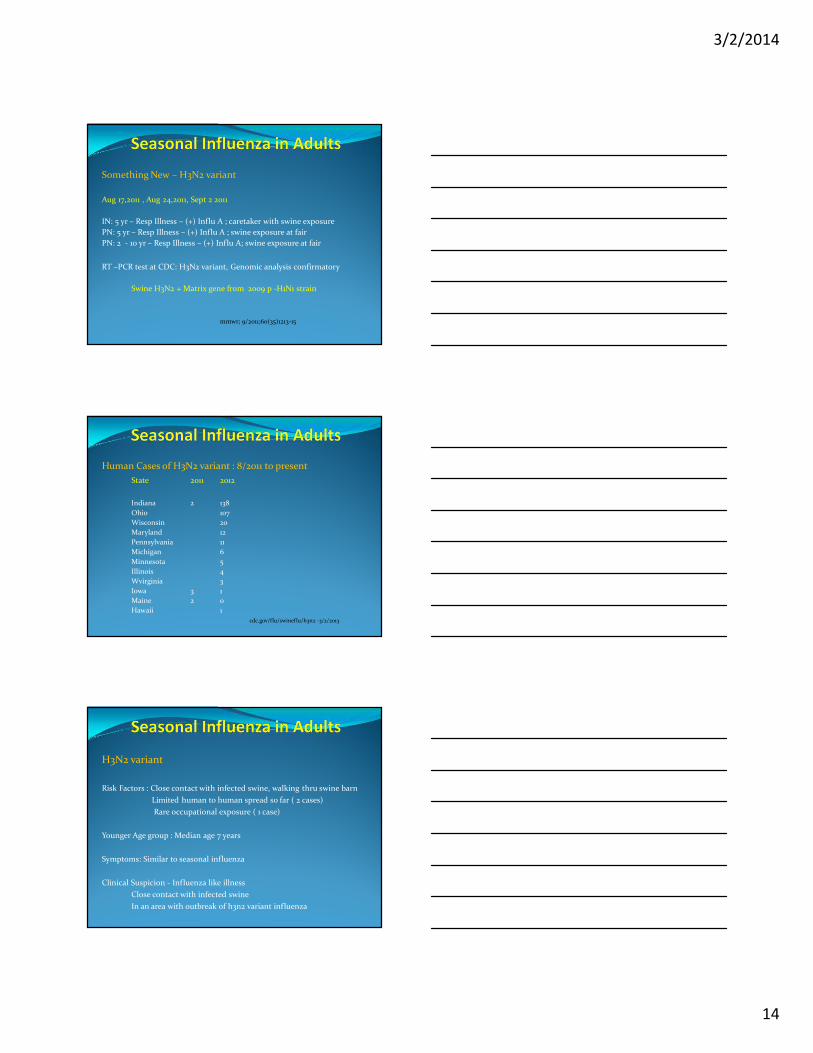
Something New – H3N2 variant
Aug 17,2011 , Aug 24,2011, Sept 2 2011
IN: 5 yr – Resp Illness – (+) Influ A ; caretaker with swine exposure
PN: 5 yr – Resp Illness – (+) Influ A ; swine exposure at fair
PN: 2 - 10 yr – Resp Illness – (+) Influ A; swine exposure at fair
RT –PCR test at CDC: H3N2 variant, Genomic analysis confirmatory
Swine H3N2 + Matrix gene from 2009 p -H1N1 strain
mmwr; 9/2011;60(35)1213-15
Human Cases of H3N2 variant : 8/2011 to present
State 2011 2012
Indiana 2 138
Ohio 107
Wisconsin 20
Maryland 12
Pennsylvania 11
Michigan 6
Minnesota 5
Illinois 4
Wvirginia 3
Iowa 3 1
Maine 2 0
Hawaii 1
cdc.gov/flu/swineflu/h3n2 -3/2/2013
H3N2 variant
Risk Factors : Close contact with infected swine, walking thru swine barn
Limited human to human spread so far ( 2 cases)
Rare occupational exposure ( 1 case)
Younger Age group : Median age 7 years
Symptoms: Similar to seasonal influenza
Clinical Suspicion - Influenza like illness
Close contact with infected swine
In an area with outbreak of h3n2 variant influenza
3/2/2014
15
H3N2 Variant
Laboratory detection
4 rapid tests: directigen/sofia/veritor/expect
CDC flu – r RT – PCR – Dx Panel
Treatment : oseltamivir or zanamivir
Vaccine : current vaccine is not preventive
This can’t be happening again ? More blood draw?
Oh no ! It is happening again !!

3/2/2014
16
Influenza A H7/N9
Avian Influenza A h7/N9
N=132Deaths : 30%Age: 4 – 87
Isolated in live bird markets - chickens, ducks, pigeons ,quail
Hemagglutinin structure is associated with low virulence in bird
First time H7/N9 has infected Humans
1st case outside china - malaysia 2/2014
Avian Influenza A H7/N9
Combination of 3 different avian influenza viruses
Affinity to alpha 2-6 receptors : ability to infect humans
Prior H7 infections were associated with conjunctivitis
Testing : RT – PCR is available through CDC & WHO
Treatment: Neuraminidase Inhibitors appear to be sensitive
Index of Suspicion : Traveler’s from China
3/2/2014
17
Please ladies ; this is not my good side !
Avian Influenza H5N1
N= 600 cases ( 2003-2014)
Mortality – 60%
1st case in North America – 1/8//2014 : Toronto
Risk – Close contact with sick or dead poultry, visiting live
Poultry markets, prolonged exposure to sick individuals
Endemic in Poultry- Bangladesh, China,Egypt,India,Indonesia, Vietnam
Index of Suspicion : Traveler’s from China
Role of Pigs
3/2/2014
18
Incidence of Influenza in HCW’s
Setting : 4 acute care hospitals - Glasgow
Year: 1993-94 ; OPD incidence 0.2 %
N = 518 HCW’s ( 90% involved in patient care)
Incidence - 120/ 518 (23%)
Asymptomatic – 59%
Sick leave – 35%
Physician Diagnosis – 18%
BMJ 1996:313;1241-42
Characteristics of Viral Shedding
Setting: US Air Force Academy
Year: 2009-2010
Samples: Nasal washings analyzed by RT-PCR
N = 167
Temp < 37.8 31/106 29%
Asymptomatic 11/58 19%
7 days post ILI 7/29 24%
Am Journ Prev Med
2010:38;121-6
Nosocomial Influenza Outbreak
Setting : Univ of Manitoba HSC, Geriatric unit
Year: Dec 1 – 20, 1989
N = 16/34 patients, 17/51 HCW’s
No shared Rooms during 1st 7 days of outbreak
9/16 HCW’s became ill first
Peak of outbreaks
Dec 1 9 HCW’s
Dec 9,10 8 patients
Dec 14 > 7 HCW’s
Vaccine Status of HCW’s 14%
Can Journal of Inf Dis
1993:4(1) 52-56
3/2/2014
19
Evidence for Nosocomial Influenza
Setting Duration #Patients
Neuro 30 days 77
NICU 7 days 3
Medical 7 days 9
Pediatric 30 days 12
NICU 7 days 8
Medical 30 days 28
Transplant 5 days 4
MICU 7 days 3
BMT 7 days 7
NICU 5 days 4
Rehab 30 days 19
Medical 30 days 10
Lancet Inf Dis 2002:2;145-55
Correlation of HCW Vaccinations & Nosocomial Influenza
Setting: Univ of Virginia Health Systems
Period: 1987-88 & 1999-2000
1987-88 1999-2000
HCW vaccination rate 4% 67%
Nosocomial Influenza 32% 0%
HCW with influenza 42% 9%
Inf Control & Hosp Epid 2004:25;923-928
HCW Vaccination Rates and Effects on Patient Mortality
Setting: 44 Long term care homes in UK
22 – vaccine intervention & 22 control group
Period : 2003-04
N = 2604 patients, 1703 HCW’s
Influenza Season
Vaccine group Control group P values
HCW vaccine rate 48% 5.9%
Death 140 203 0.002
ILI 142 300 0.004
OPD Doctor visits 125 247 0.002
Hospitalizations 4 23 0.009
BMJ Dec 1 , 2006:581354.55
3/2/2014
20
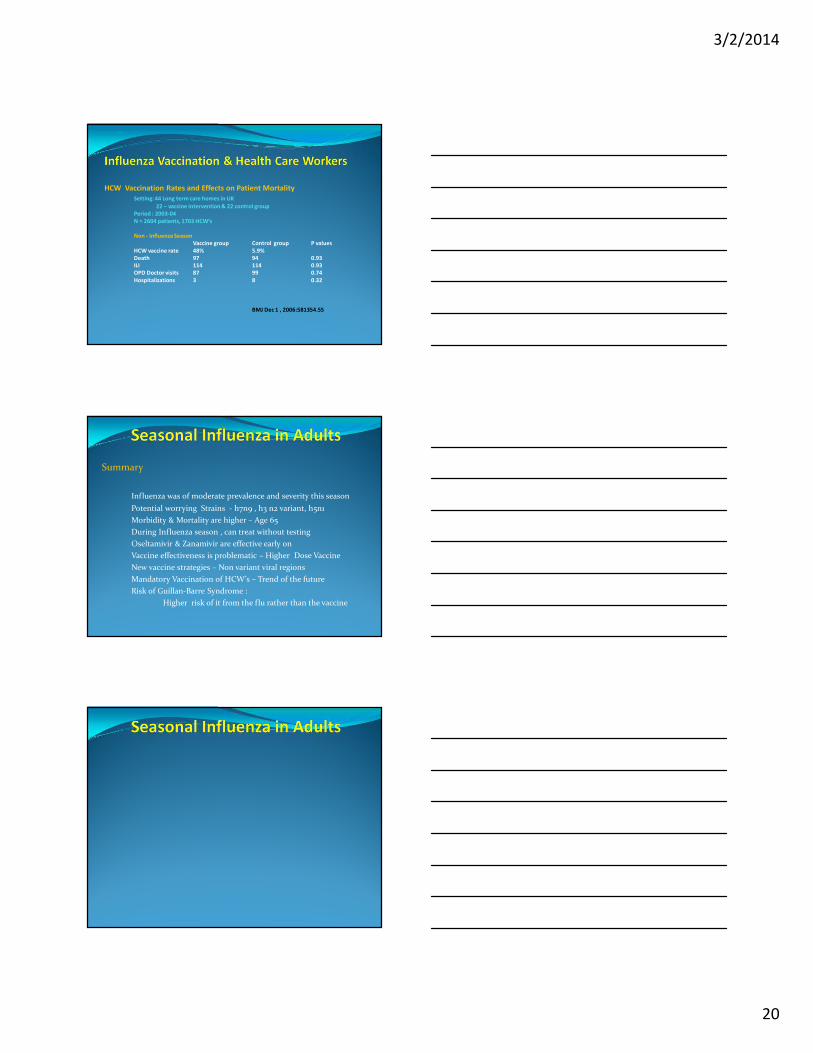
HCW Vaccination Rates and Effects on Patient Mortality
Setting: 44 Long term care homes in UK
22 – vaccine intervention & 22 control group
Period : 2003-04
N = 2604 patients, 1703 HCW’s
Non - Influenza Season
Vaccine group Control group P values
HCW vaccine rate 48% 5.9%
Death 97 94 0.93
ILI 114 114 0.93
OPD Doctor visits 87 99 0.74
Hospitalizations 3 8 0.32
BMJ Dec 1 , 2006:581354.55
Summary
Influenza was of moderate prevalence and severity this season
Potential worrying Strains - h7n9 , h3 n2 variant, h5n1
Morbidity & Mortality are higher – Age 65
During Influenza season , can treat without testing
Oseltamivir & Zanamivir are effective early on
Vaccine effectiveness is problematic – Higher Dose Vaccine
New vaccine strategies – Non variant viral regions
Mandatory Vaccination of HCW’s – Trend of the future
Risk of Guillan-Barre Syndrome :
Higher risk of it from the flu rather than the vaccine

3/2/2014
21