‘you must be the change you want to see in the world’ - m k gandhi ‘you have to dream before...
TRANSCRIPT
‘You must be the change you want to see in the world’
- M K Gandhi
‘You have to dream before your dreams can come true’
- APJ Abdul Kalam
Table of Contents
• The Gap in Cancer Care in Developing Nations • Cancer Care in Eastern India• The I-Care Project• How far have we come?• Going Forward• Participation
Our Starting Point :The Gap in Cancer Care in Developing Nations
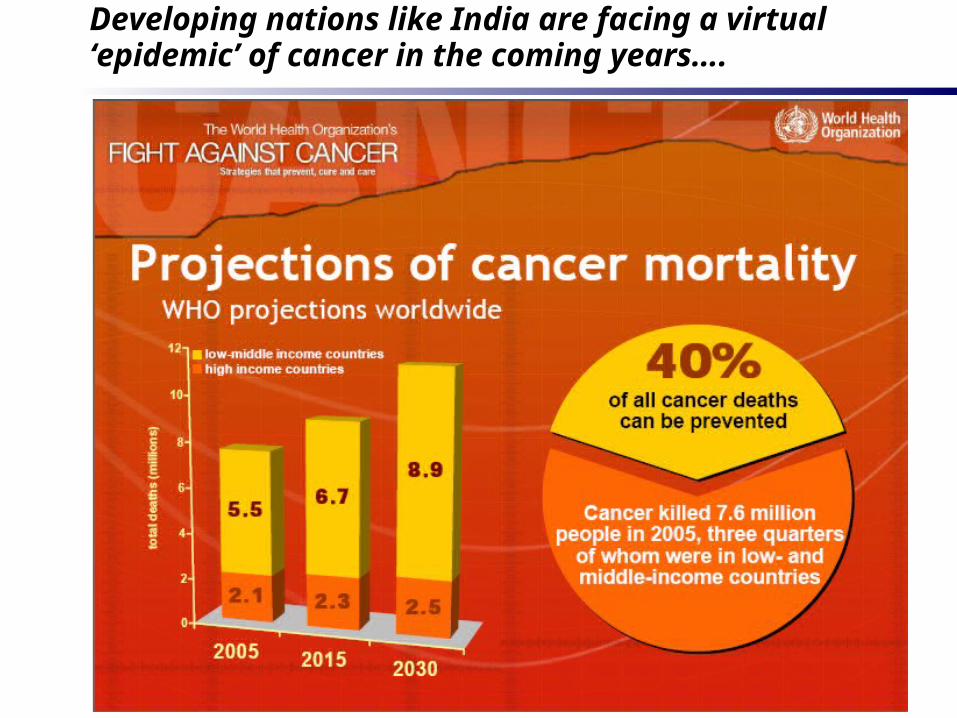
Developing nations like India are facing a virtual ‘epidemic’ of cancer in the coming years….
Developing nations like India are facing a virtual ‘epidemic’ of cancer in the coming years (Contd.)….
• ‘Number of new cancer cases in Asia is set to increase from 3.5 million in 2002 to 8.1 million by 2020’ - Lancet Asia Medical Forum
• ‘It is estimated that by 2020 there will be 15 millions cancer cases a year, the majority of them in developing countries…cancer control planning needs to be tailored to meet a country’s specific requirements and resources’ – IAEA Conference, Spotlight on Asia Pacific
90
4029
79
45
9
27
36
6
20
1
22
3
22
24
12
10
97
134
70
23
12
5
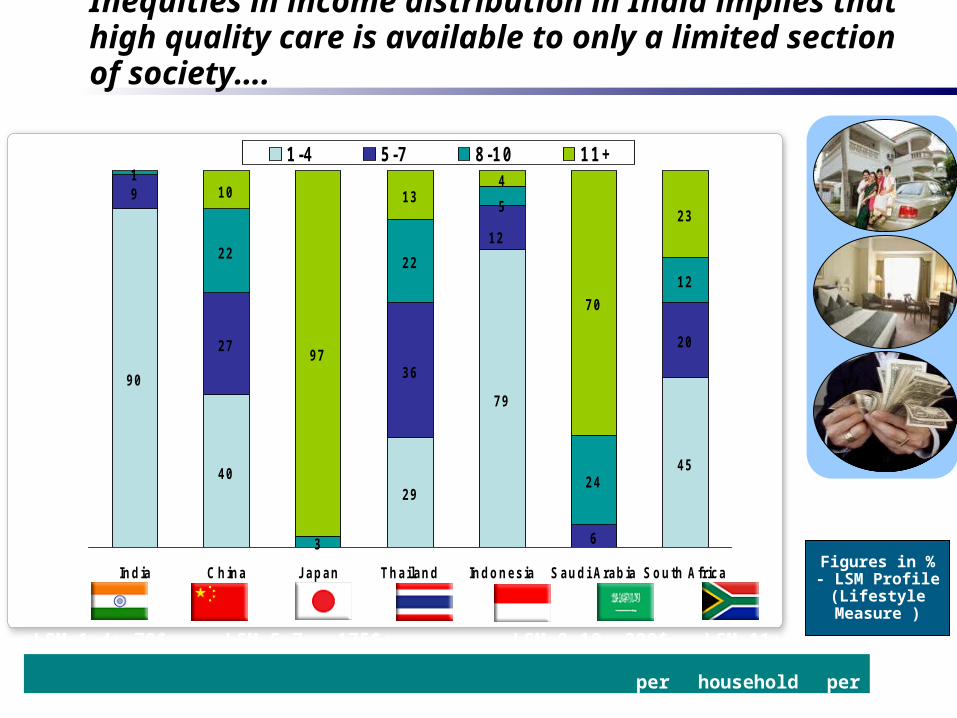
India China Japan Thailand Indonesia Saudi Arabia South Africa
1 -4 5 -7 8 -1 0 1 1 +
LSM 1-4: 70$; LSM 5-7 : 175$; LSM 8-10: 300$ LSM 11+ 500$ + per household per month
Figures in % - LSM Profile
(Lifestyle Measure )
Inequities in income distribution in India implies that high quality care is available to only a limited section of society….
Therefore, cancer care in India is still available for a limited section of society…
• Cancer initiatives are led by large corporate-funded hospitals that cater to higher-income sections of society
• Government hospitals lack adequate funding and limited infrastructure to cater to the middle or lower income patients, quality of care is poor
• Absence of large scale health insurance cover implies large sections of society (rural, urban poor) do not have access to treatment
• Awareness of cancer remains low – perceptions that cancer is ‘communicable’ still remain
• Cancer detection remains the biggest hurdle – WHO projects that 40% of cancer deaths can be prevented through early detection
• Palliative or hospice care remains significantly absent, with terminal patients left out of the ambit of organized cancer care
Recent innovations in India has seen the advent of ‘game changing’ models of patient care…
• The Aravind Eye Care System– Started off to build awareness that a simple cataract operation can restore eyesight– Set up as a non-profit organization under a charitable trust– Built on model of high productivity for doctors and operation theatres, with post-op care
in the hands of trained nurses and paramedics– Developed own lens for cataract operations, significantly cheaper than the market-ready
varieties– Built on innovation models of care - outreach program, rural eye clinics, trained village-
based doctors, etc. – All patients treated for free, after-care is charged as per service desired– 2 million patients treated since inception, in a self-sustaining operating model – Supported by affiliations with John Hopkins University, USA, the Royal College of
Ophthalmology UK and the Bill and Melinda Gates Foundation
• Models like the Aravind Eye Care System demonstrate that innovative models of care in developing nations like India can bridge the gap in cancer care between the rising incidences and the limitations of ‘traditional’ models of care

Cancer Care in Eastern India
In Eastern India, the cancer care scenario mirrors the realities for India as a whole…
On the demand side….– The National Cancer Registry puts the minimum incidence in the Kolkata Center at 49.2
per 100,000 for males and 56.2 per 100,000 for females– Across India, minimum cancer incidence is estimated to be about 36.2 per 100,000 across
both rural and urban populations – With a population of 80 million, West Bengal would have a conservative estimate of
30,000 cases – factoring in the other eastern states, the cancer incidence for Eastern India would be close to 50,000
– This ties in with the patient statistics released by the Tata Memorial Hospital in Mumbai which states that "over 24 per cent of the 2 to 3-lakh patients attended to by the hospital annually, are from the eastern and the north-eastern region” - which again puts the number at 55,000
On the supply side….– The Chittaranjan Cancer Hospital (200 beds) and the Thakurpukur Cancer Care Welfare
Home (250 beds) are the dedicated cancer care establishments in the city– The sum of these establishments are not adequate to cater to even the economically well-off
patients, as demonstrated by the number of people seeking treatment outside West Bengal– Current plans for the proposed Tata hospital in Kolkata and similar ventures focus again on
a limited section of society that is able to pay for expensive treatment options– This leaves a large part of society outside the reach of treatment, uncared for and untreated– The new Chittaranjan National Cancer Institute (CNCI) is in planning stage

The I-Care Project
www.i-careonline.org
The mandate for the I-Care Project is therefore to develop a new model of cancer care based on the following…
• A venture led by professionals
• Focused on delivering innovative cancer care to a larger section of society
• A philanthropy-based business model
• With strong operational planning balancing investment in technology with fiscal discipline
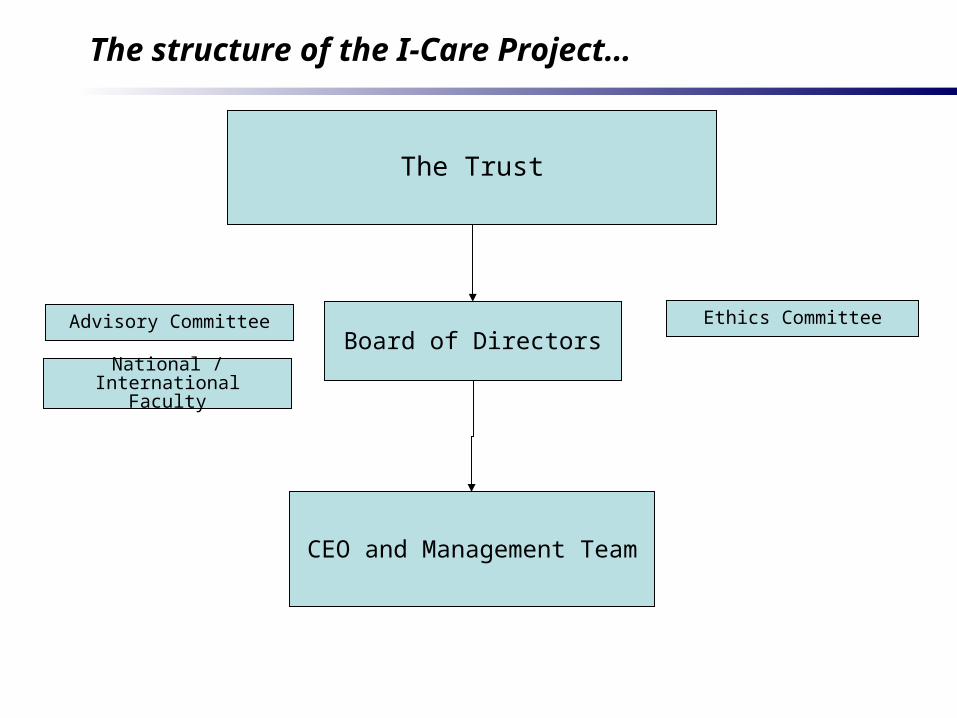
The structure of the I-Care Project…
The Trust
Board of Directors
CEO and Management Team
Advisory Committee Ethics Committee
National / International Faculty
A Philanthropy-based model…..
• Why Philanthropy?– Model of corporate-funded and commercially profitable projects do not reach
all segments of society and the model of care is not inclusive
– Great institutions in India and USA have been built on a philanthropic model
– Philanthropy does not have to be without profit – all these institutions are self-sustaining and growing/developing entities
– The aim is to be financially self-sufficient, when fully operational
• Economics of Philanthropy for I-Care– Profits non-taxable, re-invested into the institution (profit is not the aim)
– Low cost care for an significant percentage of beds (up to 40%)
– Offering customized care options, since cancer care cannot be ‘packaged’
– Investing in peripheral human resource development through the Hub and Spoke model
– Develop a model of cancer care which can be replicated to reach larger patient populations in low income countries
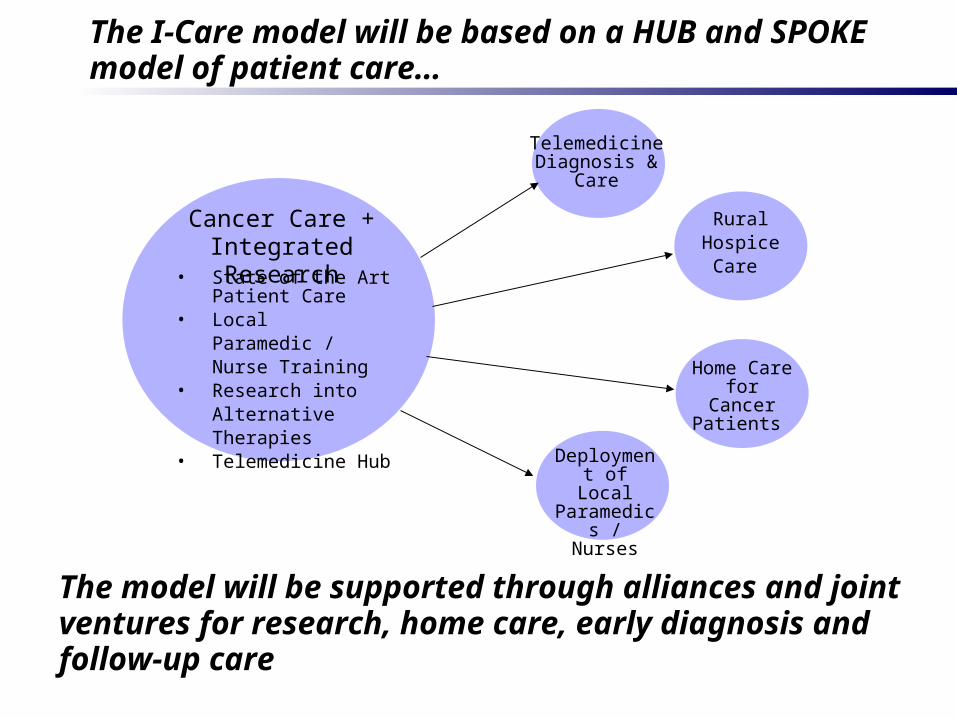
The I-Care model will be based on a HUB and SPOKE model of patient care…
Cancer Care + Integrated Research• State of the Art
Patient Care• Local Paramedic /
Nurse Training• Research into
Alternative Therapies• Telemedicine Hub
Telemedicine Diagnosis &
Care
RuralHospice
Care
Deployment of Local
Paramedics / Nurses
The model will be supported through alliances and joint ventures for research, home care, early diagnosis and follow-up care
Home Care for Cancer Patients
A focus on research…
• At the I-Care project, research would constitute an integral part of the treatment of cancer, not in advanced areas but in more pragmatic context
• Research in the context of a developing country has a more basic function involving – accurate patient data recording,
– maintaining transparency and accountability,
– conducting program evaluation
– researching alternative medicine with scientific controls
• In addition, our research activities would consist of the following:– The subsidized treatment of poorer patients using research grants with consent
along with legal and ethical controls
– Developing and maintaining an academic focus to the institution for teaching from basic to post postgraduate levels
– To develop an approach and attitude of caring for poorer patients
– To keep abreast with developments in cancer care worldwide
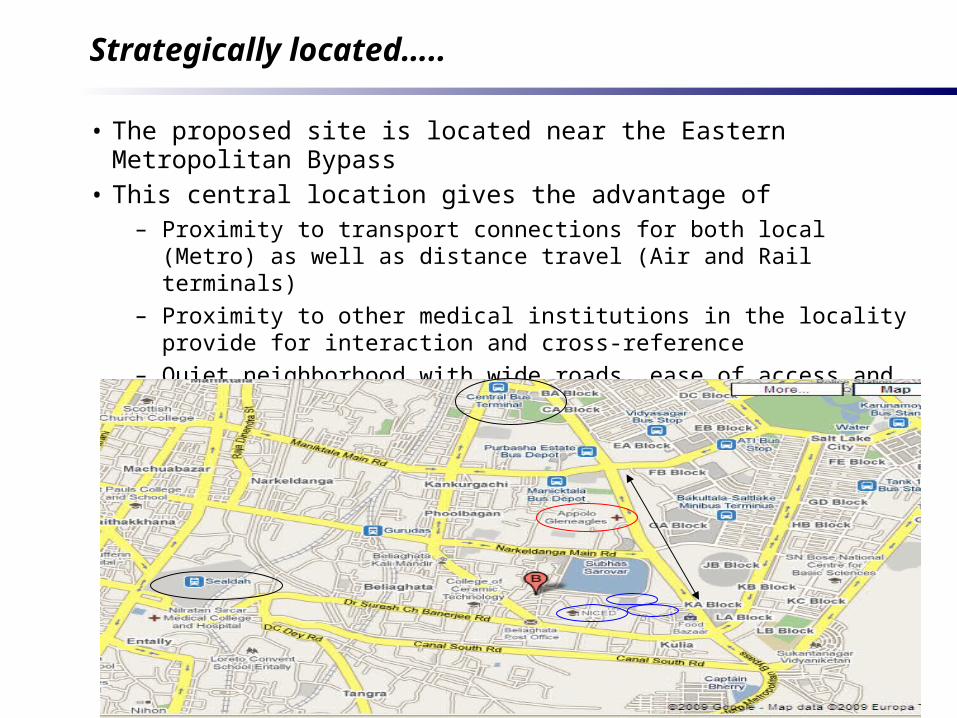
Strategically located…..
• The proposed site is located near the Eastern Metropolitan Bypass • This central location gives the advantage of
– Proximity to transport connections for both local (Metro) as well as distance travel (Air and Rail terminals)
– Proximity to other medical institutions in the locality provide for interaction and cross-reference
– Quiet neighborhood with wide roads, ease of access and fully developed land in terms of water, electricity and other amenities
How Far Have we Come ?
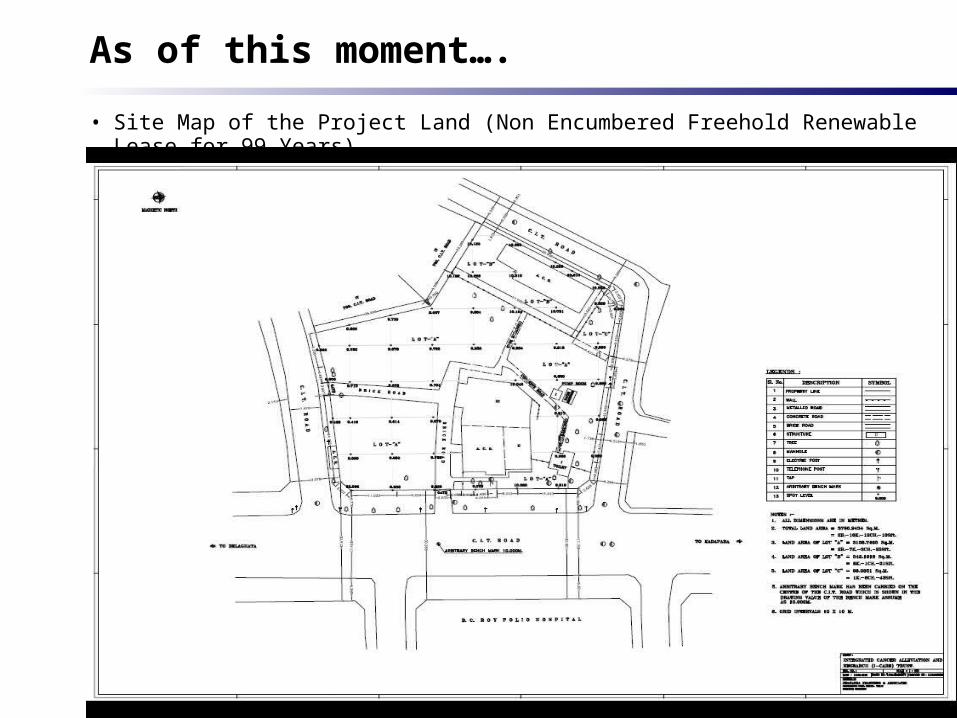
As of this moment….
• Site Map of the Project Land (Non Encumbered Freehold Renewable Lease for 99 Years)
In this meeting we seek to….
• Create awareness – about the state of cancer care in India and the widening gap which the I-Care project wishes to bridge
• Discuss our ideas with you – solicit your opinion on our project in an interactive forum
• Invite you to be a partner in our journey, in the form of– Financial Support– Technical and Professional Advise– Organizational Liaison with relevant entities

Thank You for your Time!