xience side branch access stent for treatment of bifurcation coronary disease: a review of...
TRANSCRIPT

C©2012, Wiley Periodicals, Inc.DOI: 10.1111/j.1540-8183.2012.00736.x
ORIGINAL INVESTIGATION
Xience Side Branch Access Stent for Treatment of Bifurcation CoronaryDisease: A Review of Preclinical Data
DAVID G. RIZIK, M.D., F.A.C.C., F.S.C.A.I.,1 JAMES B. HERMILLER, M.D., F.A.C.C., F.S.C.A.I.,2
KEVIN J. KLASSEN, M.D., F.A.C.C, 1 and MAULIK SHAH, M.D.1
From the 1Scottsdale Heart Group, Scottsdale Healthcare Hospital, Scottsdale, Arizona; and 2St. Vincent Heart Center of Indiana,Indianapolis, Indiana
The Xience Side Branch Access (SBA) stent is an everolimus-eluting stent designed specifically for branchingcoronary geometry, providing wire access into the side branch (SB) regardless of the planned treatment strategy.The stent is delivered via a low-profile, dual-lumen, and single-tip catheter. A single inflation deploys the stent inthe main branch (MB) and opens a portal into the SB. It is through this portal opening, allowing wire access intothe SB, that this device differentiates itself from certain other dedicated bifurcation devices currently in variousstages of development and testing. The Xience SBA stent was compared with a standard Multi-Link Vision R© stentusing a provisional T-stenting strategy in an ovine beating heart model. The Xience SBA stent tended to be deployedwith less mean contrast usage (21.05 vs. 43.23 mL; P = 0.09), shorter fluoroscopy time (2.55 vs. 4.52 minute; P =0.12), and lower rates of guidewire entanglement (16% vs. 100%) compared with the workhorse stent. As a result,the total procedure time with the Xience SBA stent was significantly shorter than that with the standard stent (5.46vs. 8.65 minute; P = 0.01). The Xience SBA stent was also evaluated by four recently trained interventionalists whohad no previous experience with the device. Using a perfused synthetic heart model, SB access time was reducedby 54%, average fluoroscopy time was reduced by 46%, and average contrast usage was lowered by 39% with theXience SBA compared with the standard stent. Initial experience in the ovine model suggests that the Xience SBAstent is also amenable for use in distal left main coronary artery disease, regardless of whether it is deployed in theleft ascending coronary artery or left circumflex artery and the portal opened in the opposing vessel. On the basisof these experimental results, the Xience SBA stent is an easy to use and versatile device for the purpose of SBaccess and potentially for the treatment of bifurcation coronary artery lesions. (J Interven Cardiol 2012;∗∗:1–7)
Introduction
Coronary bifurcation lesions, which have been iden-tified in approximately 10–15% of diagnostic catheter-izations,1–3 are associated with higher rates of pro-cedural complications, restenosis, intermediate-termstent thrombosis, and target vessel revascularization(TVR) compared with percutaneous revascularizationof nonbifurcated lesions.4–6 Numerous strategies havebeen proposed for treating bifurcation disease rang-ing from a single main branch (MB) stent with sidebranch (SB) balloon angioplasty to various two-stent
Address for reprints: David G. Rizik, MD, Scottsdale HealthcareHospital, 10101 North 92th Street, Suite 101, Scottsdale, AZ 85258.Fax: (480) 860–1580; e-mail: [email protected]
techniques.7,8 Although consensus for an optimal strat-egy remains elusive, many interventional cardiologistsconsider provisional T stenting as the current standardfor the treatment of bifurcation coronary artery disease.In provisional T stenting, a stent is first placed in theMB and then the SB is evaluated for flow limitationsand degree of stenosis, thereby preserving options forSB treatment by balloon angioplasty or placement of asecond stent.9,10 In several recent meta-analyses, provi-sional T stenting was shown to produce outcomes thatwere at least comparable to those achieved with morecomplex two-stent strategies.11–13 However, more re-cent randomized data are conflicting.14
Currently available stents, whether bare metal ordrug-eluting iterations, were designed for use in sin-gle tubular vessels and not in the complex branching
Vol. 00, No. 0, 2012 Journal of Interventional Cardiology 1

RIZIK, ET AL.
Figure 1. Xience side branch access (SBA)stent. The upper panel shows the positionof the joining mandrel, allowing for singletip, low profile delivery. The bottom panelshows the fully expanded appearance of theXience SBA stent.
geometries found in bifurcation lesions.15 Accordingly,conventional stents are not ideal for treating bifurcationdisease, but rather may be limited by several factors in-cluding SB ostial gaps, MB stent overlap, stent distor-tion, and procedural complications such as guidewireentanglement.7 Analyses by coronary angiography andintravascular ultrasound indicate that consistent cov-erage of the SB ostium is necessary for successfultreatment of bifurcation disease and for preventingmajor adverse cardiac events.4,16 Given the limita-tions of conventional stents, multiple devices are underdevelopment specifically for bifurcation disease.17,18
Although each differs in concept and design, they canbe broadly classified into four groups: dedicated MBdevices, dedicated SB devices, true bifurcation devicesin which a “limb” of metal is deployed in both the par-ent and daughter vessel, and MB devices with an SBaccess port. The latter group includes those devicesoffering primary stent coverage of the MB while pre-serving access to the SB, and consequently may bebest suited for a provisional T-stenting strategy. Us-ing a device in this side branch access (SBA) group,the operator retains the ability to employ a numberof treatment options, from simple SB preservation toboth one- and two-stent strategies. Included in this lastgroup is the Abbott Vascular Xience Side Branch Ac-cess stent (Abbott Vascular, Redwood City, CA, USA),which is commonly referred to as the Xience SBAstent.
Xience SBA Stent. The Xience SBA stent isan everolimus-eluting stent that uses the drug, poly-
mer, and scaffolding technology of the XIENCETM
V Everolimus-Eluting Coronary Stent System. Thecobalt chromium stent is composed of 0.0034-inchstruts and coated with a biocompatible fluoropolymerthat releases everolimus at a controlled rate. The stentis delivered via a 7 French dual-lumen catheter con-taining an MB balloon attached to the rapid-exchangelumen and an SB balloon attached to the over-the-wire(OTW) lumen (Fig. 1). The stent is crimped on bothballoons to allow the SB balloon to exit through a por-tal opening located in the center of the stent. Proximalto the balloons, the two lumens converge into a singlecommon inflation lumen that can be pressurized witha single inflation device. Of note, the catheter containsa unique joining mandrel that holds the MB and SBtips together to avoid guidewire entanglement beforestent placement. The joining mandrel exits from theSB balloon tip and immediately enters a pocket along-side the extended MB balloon tip. This configurationeffectively joins the two tips together thereby allowingeasy single-tip delivery over only one wire. The deviceis engineered to self-rotate into proper alignment at theSB, thereby adding to its ease of use and predictability.The catheter is advanced to a point just proximal tothe target bifurcation, and then the joining mandrel isunlocked (retracted) at the proximal adapter hub andwithdrawn from the OTW lumen. A new wire is thenintroduced into the OTW lumen and placed into theSB. The system is then advanced into the bifurcation,and single kissing balloon inflation is used to deploy theMB stent and open a portal into the SB. This minimizes
2 Journal of Interventional Cardiology Vol. 00, No. 0, 2012

XIENCE SBA STENT FOR BIFURCATION DISEASE
any plaque shifting from the MB or carina into the SBostium that can occur during deployment of a conven-tional stent in the MB.19
Historically, Xience SBA is based on its predeces-sor, the bare metal Multi-Link Frontier coronary bi-furcation stent system (Guidant Corp., Santa Clara,CA, USA) that is commercially available in Europe.The Frontier stent registry published in 2005 included105 patients with coronary bifurcation lesions.5 Al-though the bare metal Frontier catheter was deployedsuccessfully at a high rate and with few acute proce-dural complications, it was associated with a 6-monthrestensosis rate of 44.8%, including MB and SB in-segment restenosis of 29.9% and 29.1%, respectively.The Xience SBA stent is intended to address severalissues: it releases everolimus to minimize restenosisfollowing successful device implantation, and it allowsthe provisional T-stenting strategy. However, it is alsointended to retain the versatility for other treatmentoptions including an upfront two-stent methodology.
The Xience SBA was compared with a standardMulti-Link Vision R© coronary stent system (AbbottVascular, Abbott Park, IL, USA) using a provisionalT-stenting strategy in a perfused synthetic model of thecoronary vasculature with SB angulations of 30◦, 50◦,70◦, and 90◦.20 The Xience SBA was deployed in thesame total time as the standard stents in the provisionalT-stent approach; however, the time to stent deploy-ment in the MB was shorter with the Xience SBA, andas a result, total contrast usage and fluoroscopy timewere lower. In addition, the Xience SBA was associ-ated with lower rates of guidewire entanglement, lessdistal protrusion of the SB stent into the MB, and lessproximal protrusion compared with the standard stents.Significant gaps in coverage of the SB ostium were notseen with either the Xience SBA or the standard stents.
Methods
Deployment of the Xience SBA Stent in the OvineBeating Heart. The Xience SBA stent and Multi-Link Vision stent were compared using a provisionalT-stenting strategy in a nonatherosclerotic ovine coro-nary artery model. Four healthy sheep were used in thestudy, with each animal receiving at least one of eachstent type. In total, six Xience SBA stents and six Multi-Link Vision R© stents were implanted. Animal care wasconducted in accordance with the guidelines of theUS Department of Agriculture through the Animal
Welfare Act. All devices used in the implant procedurewere sterilized before use. The animals were fasted forat least 36 hours before the procedure, and receivedclopidogrel 150 mg PO and aspirin 325 mg PO on theday before the procedure (day 1) and on the day ofthe procedure (day 0). Nifedipine 30 mg PO was givenin the afternoon of day 1 and in the morning of day0. The animals were anesthetized with bupreorphine(0.1–0.5 mg/kg intramuscularly) and then an appropri-ately sized sheath for vascular access was placed in thecarotid artery. Heparin was administered to maintainan activated clotting time ≥250 seconds, and nitro-glycerin 200 µg intraluminally was given as needed tocontrol arterial vasospasm.
Initial angiography was performed to select thedesired vasculature for stent implantation, and then thestent diameter (either 2.5 mm × 18 mm or 3.0 mm ×18 mm) was matched to the appropriate vessel size toachieve a target overstretch of 10%. A guidewire wasadvanced through the guiding catheter into the targetMB, and then the delivery system was advanced overthe guidewire until the stent reached the target vessel.The Xience SBA stent was deployed by ballooninflation as described earlier after guidewire access tothe SB was achieved. For the Multi-Link Vision stent,a guidewire was advanced into the SB through a cellin the stent wall, and then a balloon was advancedto the SB ostium and deployed with final kissingpostdilation. SB stenting was not performed after theplacement of either device. After deployment, thedelivery device was withdrawn and a final angiogramwas obtained. The animals were humanely euthanizedafter the last stent was placed, and then the heart wasexcised and flushed of blood. Faxitron images wereobtained to evaluate stent apposition and possiblestent deformation.
Left Main Deployment in the Ovine BeatingHeart. The feasibility of left main deployment of theXience SBA stent was explored in the ovine beatingheart model. In each of eight healthy sheep, the XienceSBA stent (3.0 mm × 18 mm) was deployed in theleft main vessel with either the left anterior descend-ing coronary artery (LAD) or left circumflex coronaryartery (LCX) designated as the MB, and the opposingvessel designated as the SB. Following deployment, aMulti-Link Vision stent (either 2.5 mm × 18 mm or3.0 mm × 18 mm) was placed in the designated SB.Coronary angiography was performed after theprocedure to evaluate for evidence of stent migra-tion, SB patency, and distal flow characteristics.
Vol. 00, No. 0, 2012 Journal of Interventional Cardiology 3
RIZIK, ET AL.
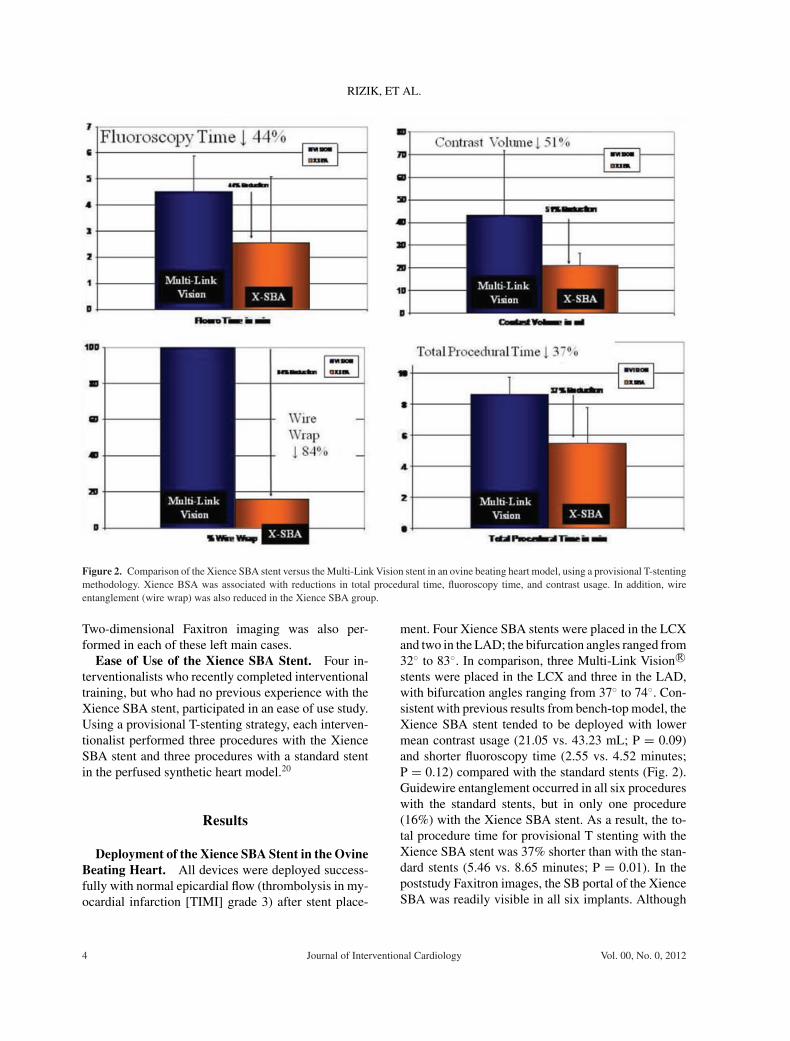
Figure 2. Comparison of the Xience SBA stent versus the Multi-Link Vision stent in an ovine beating heart model, using a provisional T-stentingmethodology. Xience BSA was associated with reductions in total procedural time, fluoroscopy time, and contrast usage. In addition, wireentanglement (wire wrap) was also reduced in the Xience SBA group.
Two-dimensional Faxitron imaging was also per-formed in each of these left main cases.
Ease of Use of the Xience SBA Stent. Four in-terventionalists who recently completed interventionaltraining, but who had no previous experience with theXience SBA stent, participated in an ease of use study.Using a provisional T-stenting strategy, each interven-tionalist performed three procedures with the XienceSBA stent and three procedures with a standard stentin the perfused synthetic heart model.20
Results
Deployment of the Xience SBA Stent in the OvineBeating Heart. All devices were deployed success-fully with normal epicardial flow (thrombolysis in my-ocardial infarction [TIMI] grade 3) after stent place-
ment. Four Xience SBA stents were placed in the LCXand two in the LAD; the bifurcation angles ranged from32◦ to 83◦. In comparison, three Multi-Link Vision R©stents were placed in the LCX and three in the LAD,with bifurcation angles ranging from 37◦ to 74◦. Con-sistent with previous results from bench-top model, theXience SBA stent tended to be deployed with lowermean contrast usage (21.05 vs. 43.23 mL; P = 0.09)and shorter fluoroscopy time (2.55 vs. 4.52 minutes;P = 0.12) compared with the standard stents (Fig. 2).Guidewire entanglement occurred in all six procedureswith the standard stents, but in only one procedure(16%) with the Xience SBA stent. As a result, the to-tal procedure time for provisional T stenting with theXience SBA stent was 37% shorter than with the stan-dard stents (5.46 vs. 8.65 minutes; P = 0.01). In thepoststudy Faxitron images, the SB portal of the XienceSBA was readily visible in all six implants. Although
4 Journal of Interventional Cardiology Vol. 00, No. 0, 2012
XIENCE SBA STENT FOR BIFURCATION DISEASE
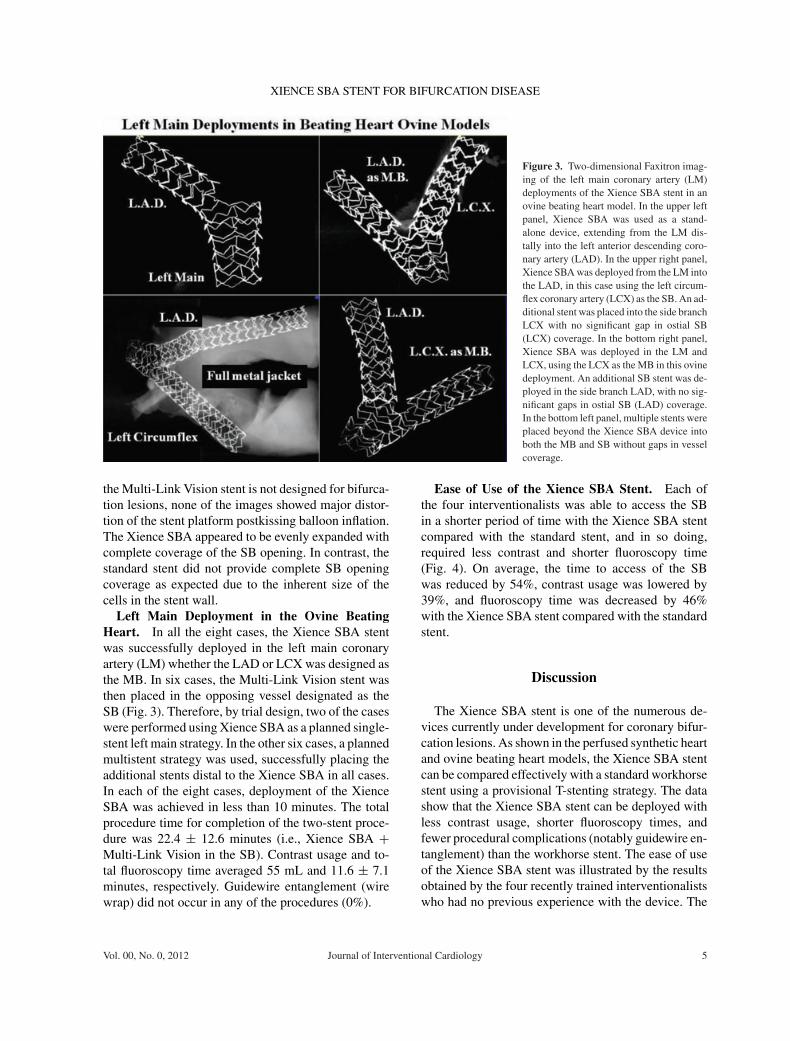
Figure 3. Two-dimensional Faxitron imag-ing of the left main coronary artery (LM)deployments of the Xience SBA stent in anovine beating heart model. In the upper leftpanel, Xience SBA was used as a stand-alone device, extending from the LM dis-tally into the left anterior descending coro-nary artery (LAD). In the upper right panel,Xience SBA was deployed from the LM intothe LAD, in this case using the left circum-flex coronary artery (LCX) as the SB. An ad-ditional stent was placed into the side branchLCX with no significant gap in ostial SB(LCX) coverage. In the bottom right panel,Xience SBA was deployed in the LM andLCX, using the LCX as the MB in this ovinedeployment. An additional SB stent was de-ployed in the side branch LAD, with no sig-nificant gaps in ostial SB (LAD) coverage.In the bottom left panel, multiple stents wereplaced beyond the Xience SBA device intoboth the MB and SB without gaps in vesselcoverage.
the Multi-Link Vision stent is not designed for bifurca-tion lesions, none of the images showed major distor-tion of the stent platform postkissing balloon inflation.The Xience SBA appeared to be evenly expanded withcomplete coverage of the SB opening. In contrast, thestandard stent did not provide complete SB openingcoverage as expected due to the inherent size of thecells in the stent wall.
Left Main Deployment in the Ovine BeatingHeart. In all the eight cases, the Xience SBA stentwas successfully deployed in the left main coronaryartery (LM) whether the LAD or LCX was designed asthe MB. In six cases, the Multi-Link Vision stent wasthen placed in the opposing vessel designated as theSB (Fig. 3). Therefore, by trial design, two of the caseswere performed using Xience SBA as a planned single-stent left main strategy. In the other six cases, a plannedmultistent strategy was used, successfully placing theadditional stents distal to the Xience SBA in all cases.In each of the eight cases, deployment of the XienceSBA was achieved in less than 10 minutes. The totalprocedure time for completion of the two-stent proce-dure was 22.4 ± 12.6 minutes (i.e., Xience SBA +Multi-Link Vision in the SB). Contrast usage and to-tal fluoroscopy time averaged 55 mL and 11.6 ± 7.1minutes, respectively. Guidewire entanglement (wirewrap) did not occur in any of the procedures (0%).
Ease of Use of the Xience SBA Stent. Each ofthe four interventionalists was able to access the SBin a shorter period of time with the Xience SBA stentcompared with the standard stent, and in so doing,required less contrast and shorter fluoroscopy time(Fig. 4). On average, the time to access of the SBwas reduced by 54%, contrast usage was lowered by39%, and fluoroscopy time was decreased by 46%with the Xience SBA stent compared with the standardstent.
Discussion
The Xience SBA stent is one of the numerous de-vices currently under development for coronary bifur-cation lesions. As shown in the perfused synthetic heartand ovine beating heart models, the Xience SBA stentcan be compared effectively with a standard workhorsestent using a provisional T-stenting strategy. The datashow that the Xience SBA stent can be deployed withless contrast usage, shorter fluoroscopy times, andfewer procedural complications (notably guidewire en-tanglement) than the workhorse stent. The ease of useof the Xience SBA stent was illustrated by the resultsobtained by the four recently trained interventionalistswho had no previous experience with the device. The
Vol. 00, No. 0, 2012 Journal of Interventional Cardiology 5

RIZIK, ET AL.
Figure 4. Ease of use of study comparing the Xience SBA stent and the Multi-Link Vision stent in a perfused synthetic heart model by fourrecently trained interventional cardiologists. The figure shows the mean time to SB access, mean contrast usage, and mean fluoroscopy time forthree procedures with the Xience SBA stent and three procedures with the standard Vision stent.
same treatment approach used in these experimentalstudies should be appropriate for clinical evaluation ofdevices that are deployed in the MB.
Our initial experience suggests that the Xience SBAis also amenable for use in distal LM disease. Coro-nary artery bypass grafting is the standard therapy forpatients with LM disease, but percutaneous coronaryintervention has emerged as a potential alternative dueto advances in drug-eluting stent technology and oper-ator experience. Both approaches have been reported toyield comparable long-term outcomes in patients withunprotected left main disease, although higher TVRrates were found with stenting, even when drug-elutingstents were used.21–23 The presence of distal lesions onbifurcation of the LM into the LAD and LCX addsto the complexity of percutaneous intervention, andis usually addressed by a provisional T-stenting strat-egy. In the French Left Main Taxus Registry, a provi-sional T-stenting approach was used in 92% of patientswith distal LM lesions, with SB stenting in 43% of the
cases.24 For the entire registry cohort, the 2-year majoradverse cardiac events (MACE) rate was 5.4%, but itwas tripled in those with a T-shaped bifurcation lesion.Acceptable outcomes have also been reported with pro-visional T stenting in other registries of patients withunprotected distal left main disease.25,26
Clearly the emphasis of treating bifurcation lesionsshould remain on achieving durable MB patency when-ever MB disease is present. That said, as it relatesto the potential for developing dedicated bifurcationdevices, simplicity of use and broad applicability toa wide variety of branching coronary geometries arekey. Specifically, adoption of any catheter-based deviceneeds to be easy to use, particularly by intermediate-level operators, and they must be broadly applicableto the heterogeneous pool of bifurcations. With grow-ing emphasis on the percutaneous treatment of morecomplex lesion subsets, the preclinical experience withXience SBA has emphasized feasibility of use in LMdisease.
6 Journal of Interventional Cardiology Vol. 00, No. 0, 2012

XIENCE SBA STENT FOR BIFURCATION DISEASE
Until recently, the consensus of treating bifurca-tion lesions focused on provisional SB methodologyas the preferred strategy. However, this notion maybe challenged in the light of recently published datashowing lower restenosis and TVR rates with dou-ble kissing crush compared with provisional stentingtechniques in patients with coronary bifurcation le-sions.14 Therefore, it seems reasonable to suggest thatdevices offering the greatest versatility are likely to en-joy the greatest adoption, regardless of whether a one-stent, two-stent, or provisional SB-stenting strategy isused.
Acknowledgement: This study and the other preclinical studiescited in this manuscript were carried out with a research grant pro-vided by Abbott Vascular of Santa Clara, CA, USA.
References
1. Al Suwaidi J, Yeh W, Cohen HA, et al. Immediate and one-year outcome in patients with coronary bifurcation lesionsin the modern era (NHLBI dynamic registry). Am J Cardiol2001;87:1139–1144.
2. Garot P, Lefevre T, Savage M, et al. Nine-month outcome ofpatients treated by percutaneous coronary interventions for bi-furcation lesions in the recent era. A report from the Preventionof Restenosis with Tranilast and its Outcomes (PRESTO) trial.J Am Coll Cardiol 2005;46:606–612.
3. Bezerra H, Perin E, Berger P, et al. Outcomes of unselected re-cipients of sirolimus-eluting stents: The Cypher stent U.S. post-marketing surveillance registry. J Invasive Cardiol 2010;22:48–55.
4. Colombo A, Moses JW, Morice MC, et al. Random-ized study to evaluate sirolimus-eluting stents implantedat coronary bifurcation lesions. Circulation 2004;109:1244–1249.
5. Lefevre T, Ormiston J, Guagliumi G, et al. The FRONTIERstent registry. Safety and feasibility of a novel dedicated stentfor the treatment of bifurcation coronary artery lesions. J AmColl Cardiol 2005;46:592–598.
6. Kim YH, Park DW, Lee SW, et al. Long-term safety and ef-fectiveness of unprotected left main coronary stenting withdrug-eluting stents compared with bare metal stents. Circula-tion 2009;120:400–407.
7. Rizik DG, Klassen KJ, Hermiller JB. Bifurcation coronaryartery disease: Current techniques and future directions (part1). J Invasive Cardiol 2008;20:82–90.
8. Louvard Y, Lefevre T, Morice M-C. Percutaneous coro-nary intervention for bifurcation coronary disease. Heart2004;90:713–722.
9. Brunel P, Lefevre T, Darremont O, et al. Provisional T-stentingand kissing balloon in the treatment of coronary bifurcationlesions: Results from the French multicenter “TULIPE” study.Catheter Cardiovasc Interv 2006;68:67–73.
10. Ferenc M, Gick M, Kienzle R-P, et al. Randomized trial onroutine vs. provisional T-stenting in the treatment of de novocoronary bifurcation lesions. Eur Heart J 2008;29:2859–2867.
11. Hakeem A, Khan FM, Bhatti S, et al. Provisional vs. com-plex stenting strategy for coronary bifurcation lesions: Meta-analysis of randomized trials. J Invasive Cardiol 2009;21:589–595.
12. Zhang F, Dong L, Ge J. Simple versus complex stenting strategyfor coronary artery bifurcation lesions in the drug-eluting stentera: A meta-analysis of randomised trials. Heart 2009;95:1676–1681.
13. Athappan G, Ponniah T, Jeyaseeian L. True coronary bi-furcation lesions: Meta-analysis and review of literature. JCardiovasc Med 2010;11:103–110.
14. Chen SL, Santoso T, Zhang JJ, et al. A randomizedclinical study comparing double kissing crush with pro-visional stenting for treatment of coronary bifurcationlesions. Results from the DKCRUSH-II (Double KissingCrush versus Provisional Stenting Technique for Treatmentof Coronary Bifurcation Lesions) trial. J Am Coll Cardiol2011;57:914–920.
15. Hermiller JB. Contemporary bifurcation treatment strate-gies: The role of currently available slotted tube stents. RevCardiovasc Med 2010;11(Suppl 1):S17–S26.
16. Costa RA, Mintz GS, Carlier SG, et al. Bifurcation coronarylesions treated with the “crush” technique. An intravascularultrasound analysis. J Am Coll Cardiol 2005;46:599–605.
17. Rizik DG, Klassen KJ, Hermiller JB. Bifurcation coronaryartery disease: Current techniques and future directions (part2). J Invasive Cardiol 2008;20:135–141.
18. Rizik DG, Klassen KJ. Dedicated bifurcation devices. RevCardiovasc Med 2010;11(Suppl 1):S27–S37.
19. Koo BK, Waseda K, Kang HJ, et al. Anatomic and functionalevaluation of bifurcation lesions undergoing percutaneouscoronary intervention. Circ Cardiovasc Interv 2010;3:113–119.
20. Rizik DG, Klag JM, Tenaglia A, et al. Evaluation of a bifur-cation drug-eluting stent system versus provisional T-stentingin a perfused synthetic coronary artery model. J Interv Cardiol2009;22:537–546.
21. Seung KB, Park D-W, Kim Y-H, et al. Stents versus coronary-artery bypass grafting for left main coronary artery disease. NEng J Med 2008;358:1781–1792.
22. Buszman PE, Kiesz SR, Bochenek A, et al. Acute and lateoutcomes of unprotected left main stenting in comparison withsurgical revascularization. J Am Coll Cardiol 2008;51:538–545.
23. Park DW, Kim YH, Yun SC, et al. Long-term outcomes afterstenting versus coronary artery bypass grafting for unprotectedleft main coronary artery disease: 10-year results of bare-metalstents and 5-year results of drug-eluting stents from the ASAN-MAIN (ASAN Medical Center-Left MAIN Revascularization)Registry. J Am Coll Cardiol 2010;56:1366–1375.
24. Vaquerizo B, Lefevre T, Darremont O, et al. Unprotected leftmain stenting in the real world. Two-year outcomes of theFrench Left Main Taxus Registry. Circulation 2009;119:2349–2356.
25. Carrie D, Eltchaninoff H, Lefevre T, et al. Twelve month clini-cal and angiographic outcome after stenting of unprotected leftmain coronary artery stenosis with paclitaxel-eluting stents—results of the multicentre FRIEND registry. EuroIntervention2009;4:449–456.
26. De Luca L, Altamura L, Corvo P, et al. Long-term outcome ofprovisional side-branch T-stenting for the treatment of unpro-tected distal left main coronary artery disease. Catheter Car-diovasc Interv 2011;77:765–772.
Vol. 00, No. 0, 2012 Journal of Interventional Cardiology 7