world health organization 1 august 2008 infectious diseases in a globalized world: risks to our...
TRANSCRIPT
World Health Organization
1August 2008
Infectious diseases in a globalized world: risks to Infectious diseases in a globalized world: risks to our public health securityour public health security
World Health Organization
2August 2008
Cryptosporidiosis
Lyme Borreliosis
Reston virus
Venezuelan Equine Encephalitis
Dengue haemhorrhagic fever
Cholera
E.coli O157
West Nile Fever
Typhoid
Diphtheria
E.coli O157
EchinococcosisLassa feverYellow fever
Ebola haemorrhagic fever
O’nyong-nyong fever
Human Monkeypox
Cholera 0139
Dengue haemhorrhagic fever
Influenza A(H5N1)
Cholera
RVF/VHF
nvCJD
Ross River virusHendra virus
BSE
Multidrug resistant Salmonella
E.coli non-O157
West Nile Virus
Malaria
Nipah Virus
Reston Virus
Legionnaire’s Disease
Buruli ulcer
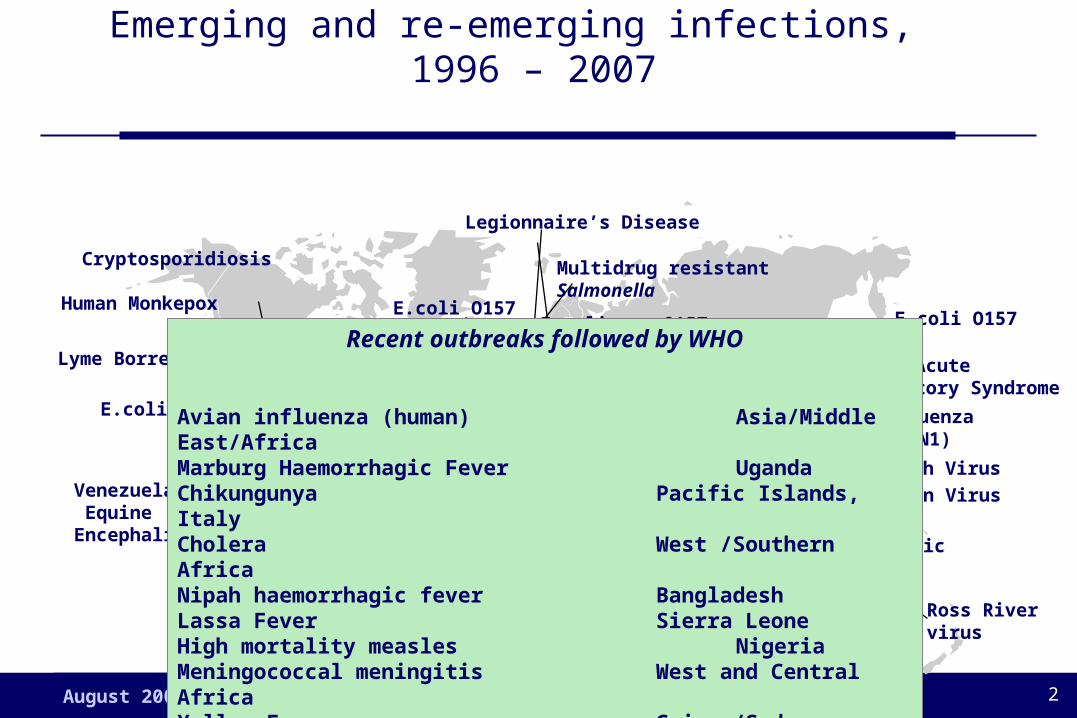
Emerging and re-emerging infections, 1996 – 2007
Severe Acute Respiratory Syndrome (SARS)
Human Monkepox
Marburghaemorrhagic fever
E.coli O157
Recent outbreaks followed by WHO
Avian influenza (human) Asia/Middle East/AfricaMarburg Haemorrhagic Fever UgandaChikungunya Pacific Islands, ItalyCholera West /Southern AfricaNipah haemorrhagic fever BangladeshLassa Fever Sierra LeoneHigh mortality measles NigeriaMeningococcal meningitis West and Central AfricaYellow Fever Guinea/SudanPoliomyelitis DRC/Bangladesh
World Health Organization
3August 2008
Points for discussionPoints for discussion
What do we know about emerging infections?– Resilience/dynamism
– Relationship with animals
– Persons at greatest risk
– Other

World Health Organization
4August 2008
Breaches in species barrier: selected emerging Breaches in species barrier: selected emerging infections in humans identified since 1976 infections in humans identified since 1976
Infection Original Yearhost reported(confirmed/hypothesized)
Ebola virus Bats 1976
HIV-1 Primates 1981
E. coli O157:H7 Cattle 1982
Borrelia burgdorferi Rodents 1982
HIV-2 Primate 1986
Hendra virus Bats 1994
BSE/vCJD Cattle 1996
Australian lyssavirus Bats 1996
H5N1 influenza A Chickens 1997
Nipah virus Bats 1999
SARS coronavirus Palm civets 2003 adapted from Woolhouse et al. (2005)
World Health Organization
5August 2008
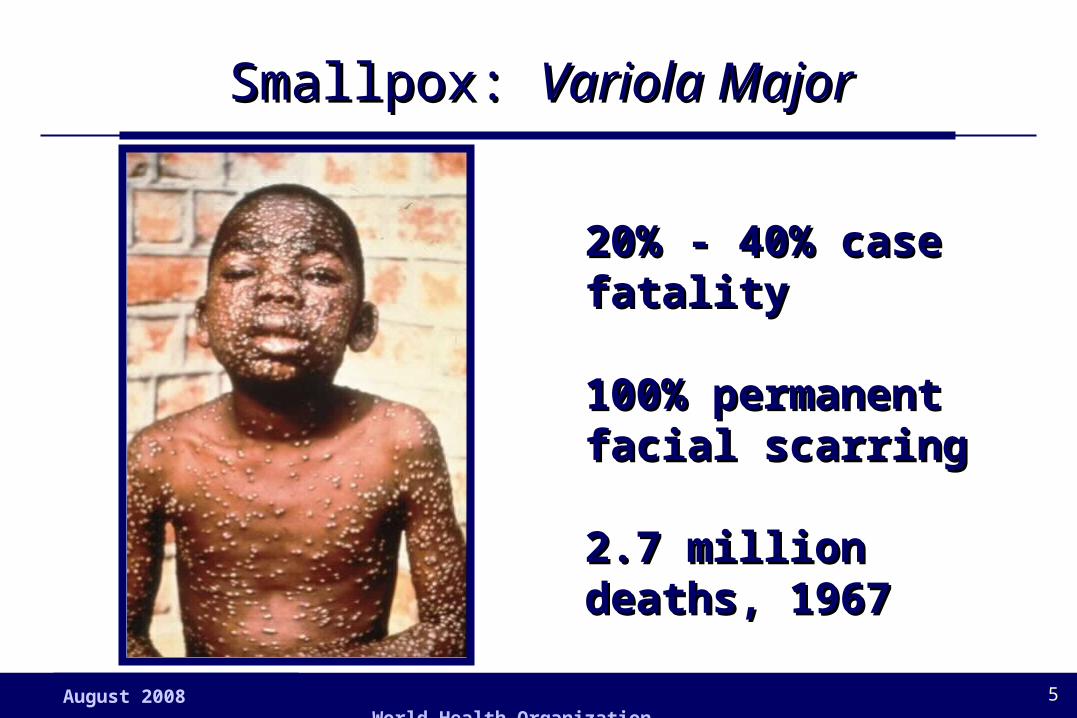
Smallpox: Smallpox: Variola MajorVariola Major
20% - 40% case 20% - 40% case fatalityfatality
100% permanent 100% permanent facial scarringfacial scarring
2.7 million deaths, 2.7 million deaths, 19671967

World Health Organization
6August 2008
Smallpox Eradication:Certified 1980

World Health Organization
7August 2008
Persons living with HIV infection, 2006: >40 million
3 million deaths during 200320 million deaths since 1981
1984: smallpox vaccination in HIV-infected adult was
AIDS defining event with generalized vaccinia/death

World Health Organization
8August 2008
Source: WHO/CDC
0
2
4
6
8
10
12
14
16
7-
Mar
13-
Mar
19-
Mar
25-
Mar
31-
Mar
6-
Apr
12-
Apr
18-
Apr
24-
Apr
30-
Apr
6-
May
12-
May
18-
May
24-
May
30-
May
5-
Jun
11-
Jun
17-
Jun
Non health care workers
Health care workers
Ebola Haemorrhagic Fever by mode of transmission, Kikwit Zaire, 1995

World Health Organization
9August 2008
SARS, chain of human-to- human SARS, chain of human-to- human transmission, Singapore 2003 transmission, Singapore 2003

World Health Organization
10August 2008
International travellers, 1950 - 2006International travellers, 1950 - 2006
Source: WHO/World Tourism Organization
International airline passengers (millions)
1000
800
600
400
200
01950 1960 1970 1980 1990 2000
1200
1400
Increased to over 2 billion international travellers in 2006

World Health Organization
11August 2008
Outbreak of leptospirosis (N = 33) among 312 Outbreak of leptospirosis (N = 33) among 312 participants, Eco Challenge 2000, Malaysiaparticipants, Eco Challenge 2000, Malaysia
Eco Challenge
Eco Challenge
US: 10
Canada: 4
Brazil: 1
Uruguay: 1 Australia: 4
France: 4UK: 9

World Health Organization
12August 2008
Doctorfrom
Guangdong
Doctorfrom
Guangdong
CanadaCanada
Hotel MHong Kong
IrelandIreland
USAUSA
New YorkNew York
SingaporeSingapore
Viet NamViet Nam
BangkokBangkok
B
I
K
F G
ED
C
JH
A
Germany1 HCW +
2
Germany1 HCW +
2
Source: WHO/CDC
SARS: international spread from Hong Kong,SARS: international spread from Hong Kong, 21 February – 12 March, 2003 21 February – 12 March, 2003
Hong KongHong Kong
+ 219 health care workers

World Health Organization
13August 2008
Countries in which airport malaria has been Countries in which airport malaria has been reported, 1969 – August 2003reported, 1969 – August 2003
USA: 1USA: 1 Switzerland: 1Switzerland: 1
Australia: 1Australia: 1
Belgium: 1Belgium: 1
Germany: 1Germany: 1
United Kingdom: 7United Kingdom: 7
France: 3France: 3
Israel: 1Israel: 1
Luxembourg: 2Luxembourg: 2

World Health Organization
14August 2008
West Nile Virus in the United States, 2005West Nile Virus in the United States, 2005
Genetic sequencing compatible with
One-time introduction in late 1990s

World Health Organization
15August 2008
Increased world trade in agricultural Increased world trade in agricultural products/animals, 1950 - 2006products/animals, 1950 - 2006
19500
40
80
120
160 export of agricultural products by volume
1960 1970 1980 1990 2000
Source: WTO, 2000
World trade in agricultural products has increased 5-fold since 1950
World Health Organization
16August 2008
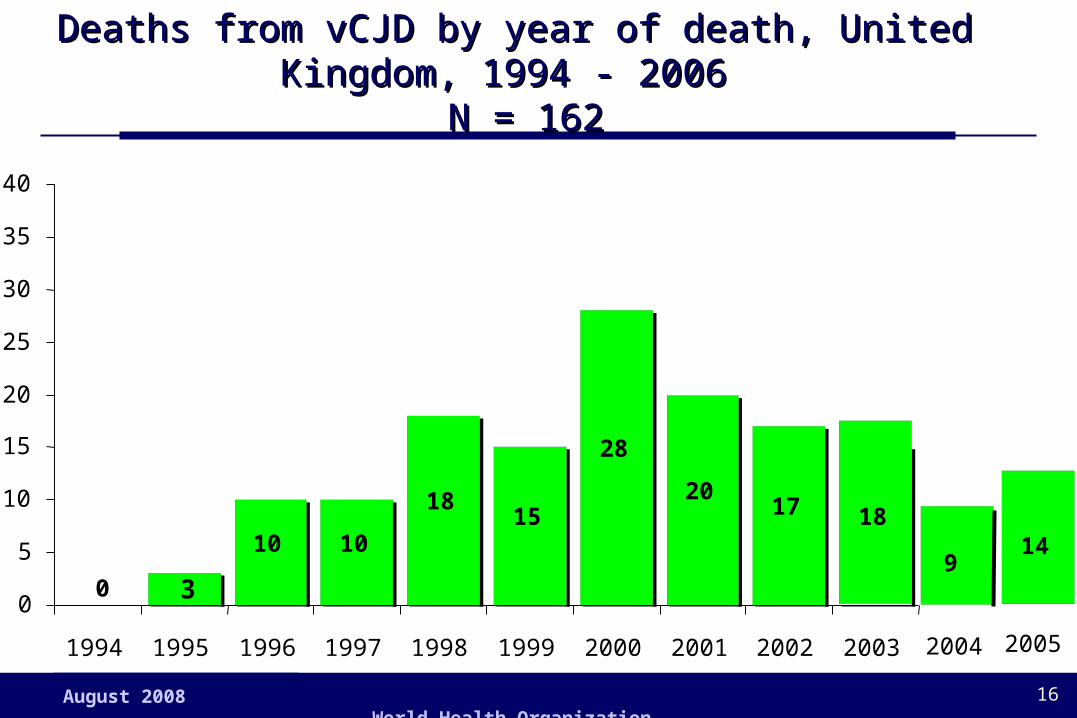
Deaths from vCJD by year of death, United Kingdom, Deaths from vCJD by year of death, United Kingdom, 1994 - 2006 1994 - 2006
N = 162 N = 162
10 1015
28
2017 18
18
0
5
10
15
20
25
30
35
40
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003
0 39
14
2004 2005
World Health Organization
17August 2008
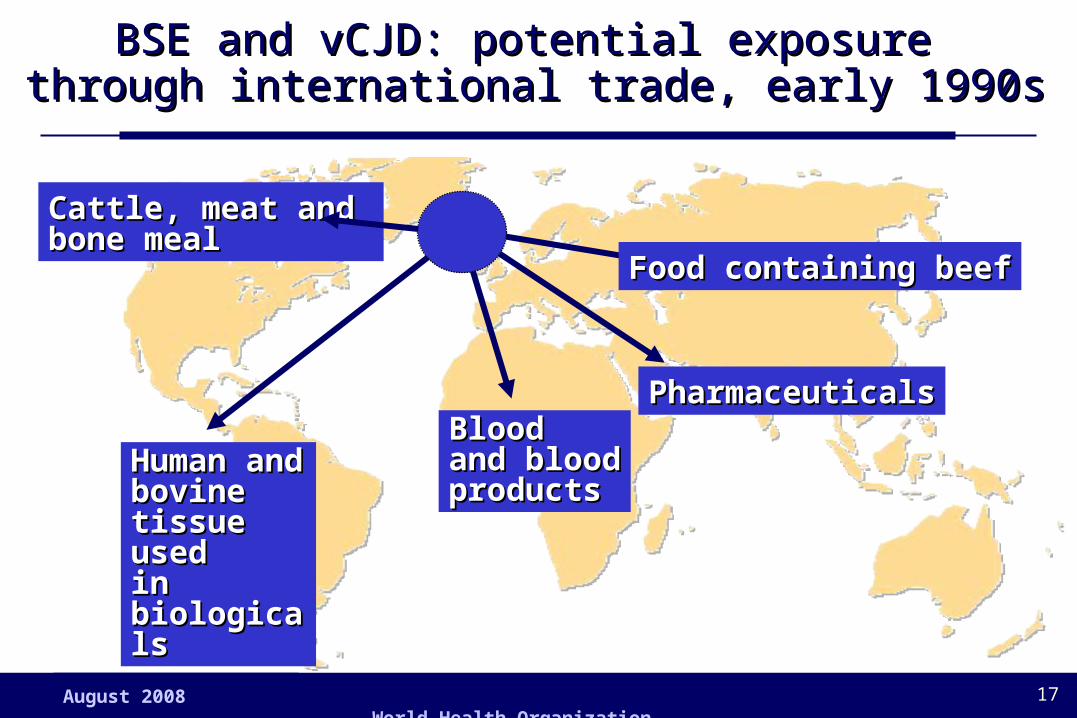
BSE and vCJD: potential exposure BSE and vCJD: potential exposure through international trade, early 1990sthrough international trade, early 1990s
Food containing beefFood containing beef
PharmaceuticalsPharmaceuticalsBlood Blood and bloodand bloodproductsproducts
Cattle, mCattle, meat and eat and bone mealbone meal
Human and Human and bovinebovinetissue used tissue used in biologicalsin biologicals

World Health Organization
18August 2008
PharmaceuticalsPharmaceuticalsBlood Blood and bloodand bloodproductsproducts
Meat and Meat and bone mealbone meal
Human and Human and bovinebovinetissue used tissue used in biologicalsin biologicals
vCJD: vCJD: ggeographieographic distribution of human c distribution of human infectionsinfections

World Health Organization
19August 2008
Rift Valley Fever, humans, Yemen, Rift Valley Fever, humans, Yemen, September 2000September 2000
0
20
40
60
80
September 1-30, 2000
Number of cases
World Health Organization
20August 2008
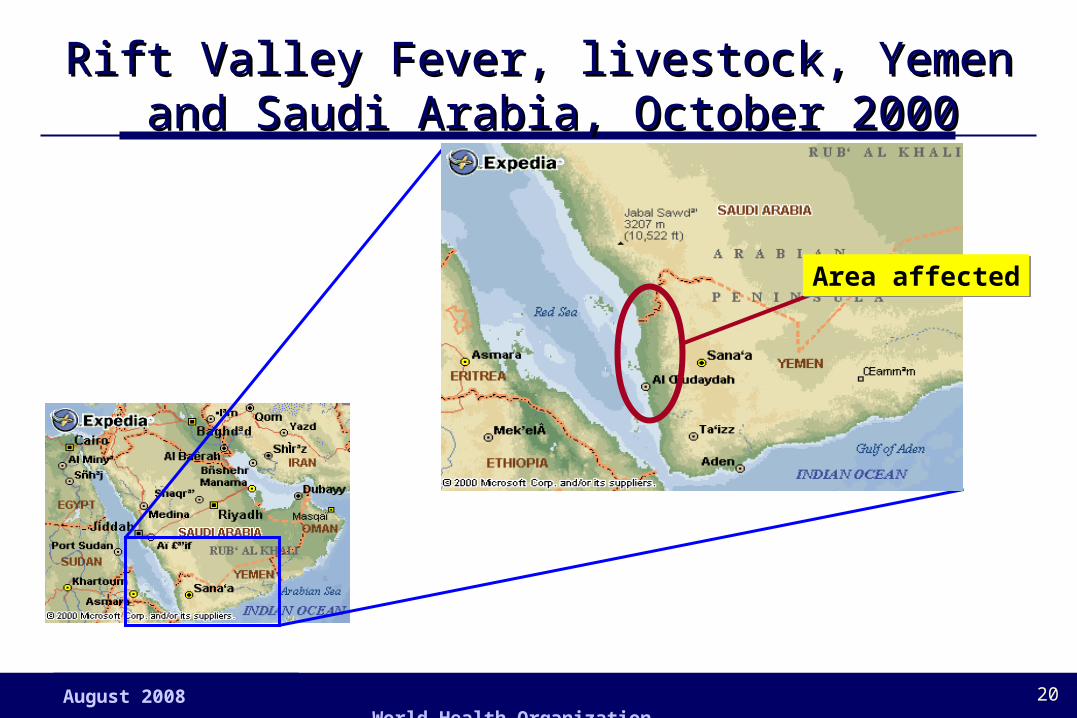
Rift Valley Fever, livestock, Yemen Rift Valley Fever, livestock, Yemen and Saudi Arabia, October 2000and Saudi Arabia, October 2000
Area affectedArea affected

World Health Organization
21August 2008
El Nino-associated flooding, East Africa, 1998El Nino-associated flooding, East Africa, 1998
Animal vaccination suspended early 1990s
Flooding forced humans and animals to close proximity
Increased mosquito breeding sites

World Health Organization
22August 2008
Highly pathogenic H5N1 influenza virus in smuggled Thai eagles, Belgium, 2005
Source: Van Borm, et al, Emerging Infectious Diseases Vol. 11, No. 5, May 2005

World Health Organization
23August 2008
Points for discussionPoints for discussion
What can be done to prevent the international spread of infectious diseases?
What measures have been taken by governments in the past?
Have any of these measures been effective?

World Health Organization
24August 2008
Concern about public health security throughout Concern about public health security throughout the agesthe ages
1374 Venice Quarantine for Plague
1851 Paris 1st International Sanitary Conference
1947 Geneva WHO Epidemiological Information Service
1951 Geneva International Sanitary Regulations
1969 Geneva International Health Regulations
World Health Organization
25August 2008
“…ensure the maximum security against the international spread
of disease with a minimum
interferencewith world traffic.”
International Health Regulations purpose International Health Regulations purpose 19691969

June 2007 World Health Organization 26
Content of International Health Regulations 1969: requirements
NotificationNotification to WHO: cholera, plague or yellow to WHO: cholera, plague or yellow fever – reports only accepted from countries fever – reports only accepted from countries where event is occurringwhere event is occurring
Health Organization at borders:Health Organization at borders: ports, airports ports, airports and frontier posts adequately equipped to and frontier posts adequately equipped to prevent vector proliferation prevent vector proliferation
Health Measures:Health Measures: describe maximum measures describe maximum measures that a country may require to protect against that a country may require to protect against cholera, plague and yellow fever (e.g. yellow cholera, plague and yellow fever (e.g. yellow fever vaccination card)fever vaccination card)
World Health Organization
27August 2008
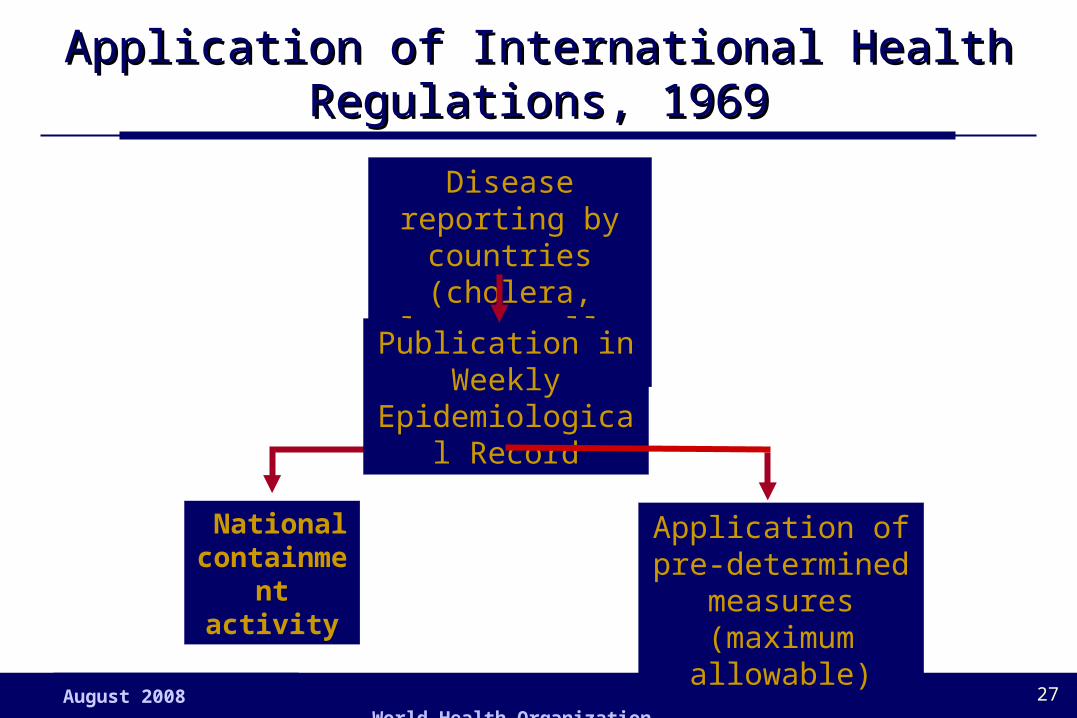
Application of International Health Application of International Health Regulations, 1969Regulations, 1969
National containment
activity
Disease reporting by countries (cholera,
plague, yellow fever)
Publication in Weekly Epidemiological Record
Application of pre-determined measures (maximum allowable)
World Health Organization
28August 2008
Points for discussionPoints for discussion
Do you think the International Health Regulations are an effective means of dealing with the international spread of infectious diseases?
If yes, why?
If no, why?

World Health Organization
29August 2008
Direct economic impact, selected infectious disease outbreaks, 1990-2003
Asia – SARSUS$ 30 billion
2003
UK - BSE US$ 39 billion
1990-1998
Tanzania - CholeraUS$ 36 million
1998
India - PlagueUS$ 1.7 billion
1995
Peru - CholeraUS$ 770 million
1991
Malaysia- Nipah Pig destruction
1999
Hong Kong - influenza A(H5N1) Poultry destruction
1997
US E. coli 0157Food recall/destruction
Periodic

World Health Organization
30August 2008
Cryptosporidiosis
Lyme Borreliosis
Reston virus
Venezuelan Equine Encephalitis
Dengue haemhorrhagic fever
Cholera
E.coli O157
West Nile Fever
Typhoid
Diphtheria
E.coli O157
EchinococcosisLassa feverYellow fever
Ebola haemorrhagic fever
O’nyong-nyong fever
Human Monkeypox
Cholera 0139
Dengue haemhorrhagic fever
Influenza A(H5N1)
Cholera
RVF/VHF
nvCJD
Ross River virusHendra virus
BSE
Multidrug resistant Salmonella
E.coli non-O157
West Nile Virus
Malaria
Nipah Virus
Reston Virus
Legionnaire’s Disease
Buruli ulcer
Emerging and re-emerging infections: 1996 - 2007
Severe Acute Respiratory Syndrome (SARS)
Human Monkepox
Marburghaemorrhagic fever

World Health Organization
31August 2008
Global outbreaks, the challenge: Global outbreaks, the challenge: latelate reporting and response reporting and response
0
10
20
30
40
50
60
70
80
90
1 4 7 10 13 16 19 22 25 28 31 34 37 40
Delayed response
DAY
CA
SE
S
Lost opportunity for control/risk of international spread
Late reporting
First case

World Health Organization
32August 2008
010
2030
4050
6070
8090
1 4 7 10 13 16 19 22 25 28 31 34 37 40
Rapid response
CA
SE
S
Early reporting Potential cases prevented/
international spread prevented
DAY
Global outbreaks, the solution: Global outbreaks, the solution: earlyearly reporting and response reporting and response

World Health Organization
33August 2008
Points for discussionPoints for discussion
What would you do next?

World Health Organization
34August 2008
Vision for revision of the International Health Vision for revision of the International Health Regulations, 1996Regulations, 1996
A world on the alert and able to detect and collectively respond to international infectious disease threats within 24 hours using the most up to date means of global communication and collaboration

World Health Organization
35August 2008
Global Public Health Intelligence Network, Global Public Health Intelligence Network, CanadaCanada

World Health Organization
36August 2008
Outbreak Verification & Response Outbreak Verification & Response Afghanistan, February 1999Afghanistan, February 1999
16 February16 February 19 February19 February 24 February 24 February 1 March 1 March
GPHIN report of highly fatal respiratory
disease
WHO/local teampreliminary investigation
WHO collaborative
team
Investigation completedDiagnosis confirmed

World Health Organization
37August 2008
Information sources, public health risks reported Information sources, public health risks reported to WHO, 2003to WHO, 2003
0%
10%
20%
30%
40%
50%
60%
70%
AFR
O
EMR
O
EUR
O
AM
RO
SEA
RO
WPR
O
WR
s
NG
Os
PRO
MED
Oth
ers
GPH
IN
Countries ( 23% of reports)
WHO Alert & Response Network ( 77% of reports)

World Health Organization
38August 2008
OperationaliOperationalizing the IHR in the 21zing the IHR in the 21stst century: p century: partnership artnership for global alert and response to infectious diseasesfor global alert and response to infectious diseases
Electronic Discussion sitesMedia
NGOs
MilitaryLaboratoryNetworks
WHO Collaborating Centres/Laboratories Epidemiology and
Surveillance Networks
WHO Regional & Country Offices
Countries/National Disease Control
Centres
UNSister Agencies
FORMALFORMAL
GPHIN
INFORMALINFORMAL

World Health Organization
39August 2008
Request for GOARN support: terms of Request for GOARN support: terms of referencereference
World Health Organization
40August 2008
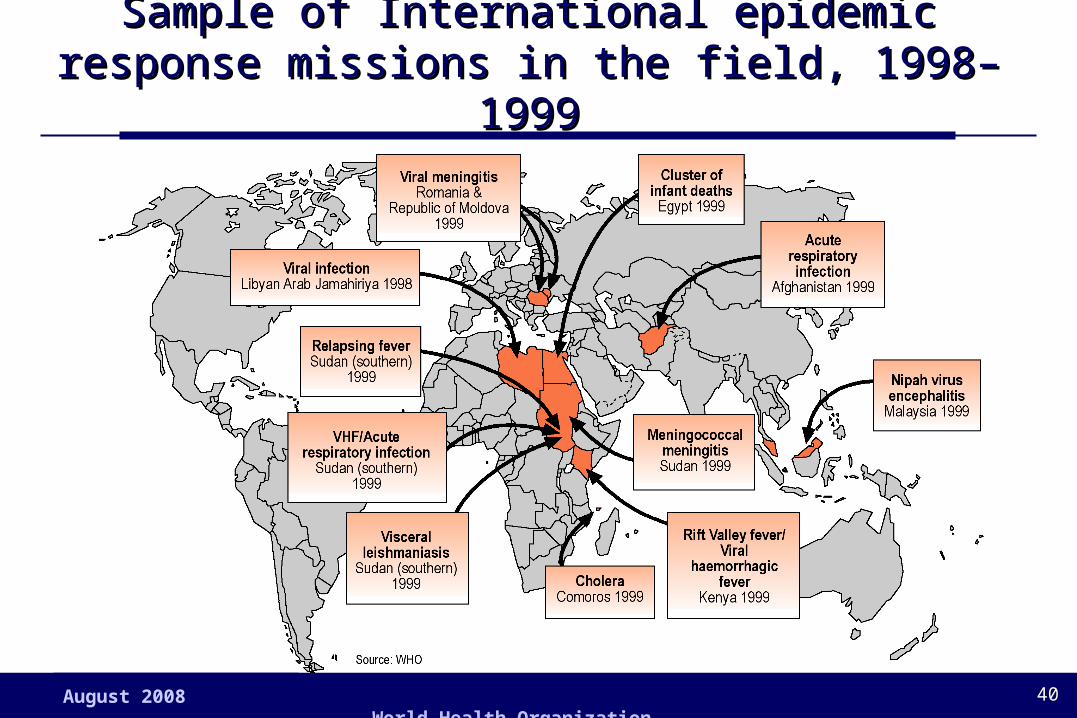
Sample of International epidemic response Sample of International epidemic response missions in the field, 1998–1999missions in the field, 1998–1999

World Health Organization
41August 2008
Global outbreak alert and response network: Global outbreak alert and response network: surveillance network partners in Asiasurveillance network partners in Asia
Mekong Basin Disease Surveillance (MBDS)
ASEAN
APEC
SEAMIC
SEANET
EIDIOR
Flu Net
GPHIN
Pacific Public HealthSurveillance
Network (PPHSN)
+ Red Cross, other NGOs

World Health Organization
42August 2008
Reports of respiratory infection, China, Reports of respiratory infection, China, 2002–20032002–2003
16 November, 2002 – Guangdong : outbreak of respiratory illness/government
recommending isolation of anyone with symptoms (GPHIN)
– official government report of normal influenza B activity, 7 Dec. 2002
11 February, 2003– Guangdong: outbreak of atypical pneumonia among health workers
(GPHIN)
– official government report of atypical pneumonia outbreak with 305 cases and 5 deaths, influenza virus not isolated, 14 Feb. 2003

World Health Organization
43August 2008
26 February– Hanoi: 48-year-old business man with high fever (> 38 ºC),
atypical pneumonia and respiratory failure with history of previous travel to China and Hong Kong (WHO country office)
4–5 March– Hong Kong and Hanoi: 77 medical staff (Hong Kong) plus 7
(Hanoi) reported with atypical pneumonia, not influenza (WHO team/liaison)
Intensified surveillance for respiratory Intensified surveillance for respiratory infections, Asia, 2002–2003infections, Asia, 2002–2003

World Health Organization
44August 2008
Global Alert: Severe Acute Respiratory Global Alert: Severe Acute Respiratory Syndrome (SARS)Syndrome (SARS)
12 March: First global alert – Described atypical pneumonia in Viet Nam and Hong Kong
14 March
– 4 persons Ontario, 3 persons in Singapore, with severe atypical pneumonia fitting description of 12 March alert reported to WHO
15 March
– Medical doctor with atypical pneumonia fitting description of 12 March reported by Ministry of Health, Singapore on return flight from New York
World Health Organization
45August 2008
Situation on 15 March, 2003Situation on 15 March, 2003
Atypical pneumonia with rapid progression to respiratory failure, none yet recovered
Health workers appeared to be at greatest risk
Unidentified cause, presumed to be an infectious agent
Antibiotics and antivirals did not appear effective
Spreading internationally within Asia and to Europe and North America
World Health Organization
46August 2008
Points for discussionPoints for discussion
What would you do next?

World Health Organization
47August 2008
Global Outbreak Containment: Decision 15 Global Outbreak Containment: Decision 15 March, 2003 March, 2003
World Health Organization issues emergency travel advisory
15 March 2003 | GENEVA -- During the past week, WHO has received reports of more than 150 new suspected cases of Severe Acute Respiratory Syndrome (SARS), an atypical pneumonia for which cause has not yet been determined. Reports to date have been received from Canada, China, Hong Kong Special Administrative Region of China, Indonesia, Philippines, Singapore, Thailand, and Viet Nam. Early today, an ill passenger and companions who travelled from New York, United States, and who landed in Frankfurt, Germany were removed from their flight and taken to hospital isolation.
Due to the spread of SARS to several countries in a short period of time, the World Health Organization today has issued emergency guidance for travelers and airlines.
“This syndrome, SARS, is now a worldwide health threat,” said Dr. Gro Harlem Brundtland, Director General of the World Health Organization. “The world needs to work together to find its cause, cure the sick, and stop its spread.”
There is presently no recommendation for people to restrict travel to any destination. However in response to enquiries from governments, airlines, physicians and travelers, WHO is now offering guidance for travelers, airline crew and airlines. The exact nature of the infection is still under investigation and this guidance is based on the early information available to WHO.
TRAVELLERS INCLUDING AIRLINE CREW: All travelers should be aware of main symptoms and signs of SARS which include:
high fever (>38oC)
AND
one or more respiratory symptoms including cough, shortness of breath, difficulty breathing
AND
one or more of the following:
close contact* with a person who has been diagnosed with SARS
recent history of travel to areas reporting cases of SARS.

World Health Organization
48August 2008
Global Outbreak Alert and Response Network 115 experts from 26 institutions in 17 countries field teams sent to 5 countries
Strategies that increased power of epidemic Strategies that increased power of epidemic control: global partnershipscontrol: global partnerships

World Health Organization
49August 2008
Probable SARS transmission, flight CA112, Probable SARS transmission, flight CA112, March 2006 March 2006
World Health Organization
50August 2008
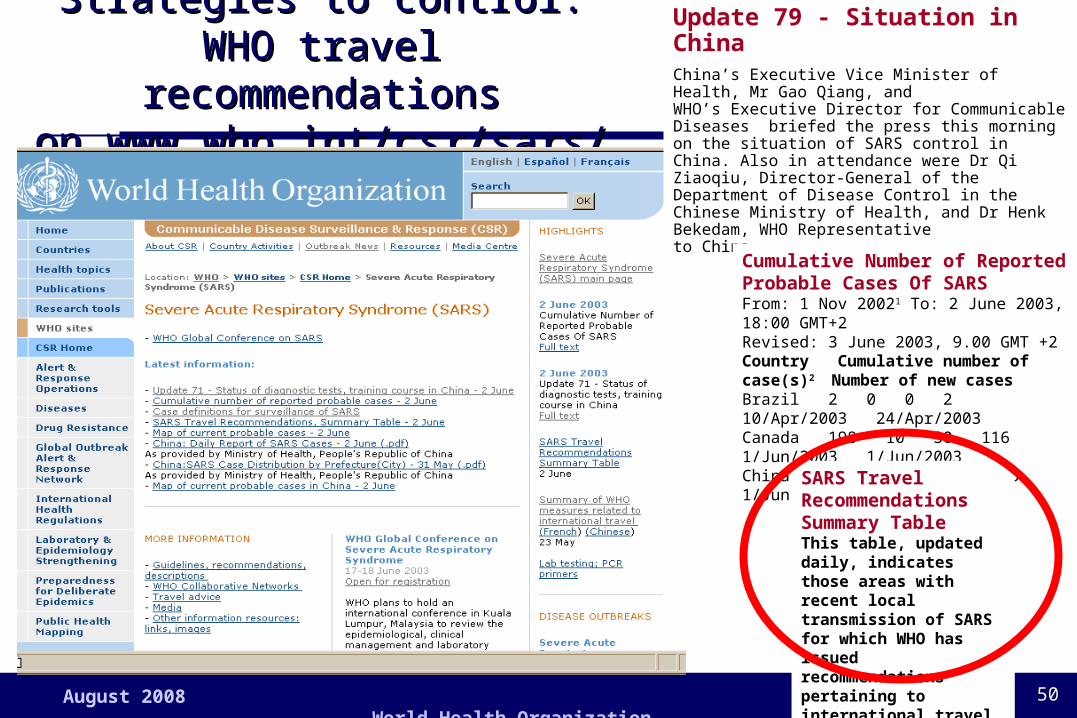
Strategies to control: WHO Strategies to control: WHO travel recommendationstravel recommendationson www.who.int/csr/sars/on www.who.int/csr/sars/
Update 79 - Situation in China China’s Executive Vice Minister of Health, Mr Gao Qiang, and WHO’s Executive Director for Communicable Diseases briefed the press this morning on the situation of SARS control in China. Also in attendance were Dr Qi Ziaoqiu, Director-General of the Department of Disease Control in the Chinese Ministry of Health, and Dr Henk Bekedam, WHO Representative to China.
Cumulative Number of Reported Probable Cases Of SARSFrom: 1 Nov 20021 To: 2 June 2003, 18:00 GMT+2 Revised: 3 June 2003, 9.00 GMT +2Country Cumulative number of case(s)2 Number of new cases Brazil 2 0 0 2 10/Apr/2003 24/Apr/2003 Canada 198 10 30 116 1/Jun/2003 1/Jun/2003 China 5328 2 334 3495 1/Jun/2003 2/Jun/2003
SARS Travel Recommendations Summary TableThis table, updated daily, indicates those areas with recent local transmission of SARS for which WHO has issued recommendations pertaining to international travel.

World Health Organization
51August 2008
Probable cases of SARS by date of onset Probable cases of SARS by date of onset worldwide, 1 March – 27 June 2003worldwide, 1 March – 27 June 2003

World Health Organization
52August 2008
SARS Epidemic curve, China, SARS Epidemic curve, China, 2002 - 20032002 - 2003

World Health Organization
53August 2008
Passenger movement, Hong Kong International Passenger movement, Hong Kong International Airport, March-July 2003Airport, March-July 2003
WHO lifted travel advisory WHO travel advisory
0
20 000
40 000
60 000
80 000
100 000
120 000
3/16
3/20
3/24
3/28 4/1
4/5
4/9
4/13
4/17
4/21
4/25
4/29 5/3
5/7
5/11
5/15
5/19
5/23
5/27
5/31 6/4
6/8
6/12
6/16
6/20
6/24
6/28 7/2
Num
ber o
f pas
seng
er
Total
23 May2 April
14 670
102 165
65 255

World Health Organization
54August 2008
The cost of SARS: initial estimates for six month The cost of SARS: initial estimates for six month outbreaks, Asian Development Bank, 2003outbreaks, Asian Development Bank, 2003
76543210 US$ billion
Hong Kong
China, mainland
Taiwan
South Korea
Indonesia
Singapore
Thailand
Malaysia
PhilippinesUS$ billionUS$ billion
4%
0.5%
1.9%
0.5%
1.4%
2.3%
1.6%
1.5%
0.8%
% of GDP
As of 30 September, 2003, SARS had decreased Asia’s combined GDP by US$18 billion and cost nearly US$60 billion in lost demand and revenues

World Health Organization
55August 2008
Points for discussionPoints for discussion
How would you ensure that the new way of working during the SARS outbreak remains a permanent way of responding to infectious diseases with international spread?

World Health Organization
56August 2008
New norms for reporting and responding to New norms for reporting and responding to infectious diseases established, 2003infectious diseases established, 2003
Reporting of infectious diseases from other sources accepted by WHO Member States
All infectious diseases with potential for international spread to be reported
Revised International Health Regulations to serve as a formal framework for pro-active international surveillance and response to all public health emergencies of international concern
Severe acute respiratory syndrome (SARS)

World Health Organization
57August 2008
International Health Regulations 2005
From three diseases to all public health threats
From passive to pro-active using real time surveillance/evidence
From control at borders to detection and containment at source

World Health Organization
58August 2008
Requirements, International Health Requirements, International Health Regulations (2005)Regulations (2005)
• Strengthened national core capacity for surveillance and control including at border posts
• Mandatory reporting of possible public health emergency of international importance, and of four specific diseases: SARS, smallpox, avian influenza and polio
• Collective, pro-active global collaboration for prevention, alert and response to international public health emergencies
• Monitoring of implementation by the World Health Assembly

World Health Organization
59August 2008
Decision making and response and the revised Decision making and response and the revised International Health RegulationsInternational Health Regulations
National containment
of public health risk
Public health risk reporting by countries
National containment
of public health risk
NO YES
Public health risk reporting from WHO Alert & Response Network
Collaborative risk-based public health measures identified and managed
pro-actively by WHO
Decision-tree analysis to determine if of urgent international public health importance

World Health Organization
60August 2008
Points for discussionPoints for discussion
Do the revised International Health Regulations meet the vision for their revision?
If not, tell what more could be done
What are some major infectious disease threat today that would fall under the Revised Regulations?

World Health Organization
61August 2008
Defining Health SecurityDefining Health Security
Individual Health Security:
Access of persons to health care and to medicines/vaccines and other health goods; removal of obstacles to good health
Public Health Security:
Activities required to minimize vulnerability to public health events that endanger the health of populations
Global Public Health Security:
Collective activities required to protect the public health of populations living across geographical regions and international boundaries