world bank documentdocuments.worldbank.org/curated/en/... · rpms sars shcp sinave sisveflu spsh ss...
TRANSCRIPT
Document of
The World Bank
Report No: NCO00001902
NOTE ON CANCELLED OPERATION
ON A
LOAN
IN THE AMOUNT OF US$491 MILLION
TO THE
UNITED MEXICAN STATES
FOR AN
INFLUENZA PREVENTION AND CONTROL PROJECT
November 22, 2011
Human Development Sector Management Unit
Mexico and Colombia Country Management Unit
Latin America and the Caribbean Region
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

i
CURRENCY EQUIVALENTS
(Exchange Rate Effective June 1, 2011)
Currency Unit = MXN
1 MXN = US$0.086
US$ 1.00 = MXN 11.668
FISCAL YEAR
January 1 – December 31
ABBREVIATIONS AND ACRONYMS
ACC Applicable anticorruption clauses
AHIF Avian and Human Influenza Facility Grant for the Influenza A/H1N1
Prevention
AIDS Acquired Immune Deficiency Syndrome
BIRMEX Laboratories of Biologics and Reagents of Mexico- Laboratorios de
Biológicos y Reactivos de México
BP Bank Procedure
CENAVECE National Center for Epidemiological Surveillance and Disease Control -
Centro Nacional de Vigilancia Epidemiológica y Control de Enfermedades
CENSIA National Center for Child and Adolescent Health - Centro Nacional para la
Salud de la Infancia y la Adolescencia
CNPHI Canadian Network for Public Health Intelligence
CPS Country Partnership Strategy
DGAE Adjunct Directorate of Epidemiology - Dirección General Adjunta de
Epidemiología
DGAPP Adjunct Directorate of Preventative Programs - Dirección General Adjunta de
Programas Preventivos
FY
GAC
GDP
GoM
GPAI
HDI
HIV
OP
PDO
RPMs
SARS
SHCP
SINAVE
SISVEFLU
SPSH
SS
UPPH
Fiscal Year
Governance and Anti-corruption
Gross Domestic Product
Government of Mexico
Global Program for Avian and Human Influenza Preparedness
Human Development Index
Human Immunodeficiency Virus
Operational Policy
Project Development Objective
Regional Procurement Managers
Severe Acute Respiratory Syndrome
Federal Secretariat of Finance - Secretaría de Hacienda y Crédito Público
National System for Epidemiological Surveillance - Sistema Nacional de
Vigilancia Epidemiológica
Epidemiological Surveillance System for Influenza-Sistema de Vigilancia
Epidemiológica de Influenza
Social Protection System in Health-Sistema de Protección Social en Salud,
SPSS
Federal Secretariat of Health - Secretaría de Salud
Under-Secretariat for Prevention and Promotion in Health- Subsecretaría de
Prevención y Promoción

ii
Vice President: Pamela Cox
Country Director: Gloria Grandolini
Sector Manager: Joana Godinho
Project Team Leader: Christoph Kurowski
NCO Team Leader: Claudia Macias

iii
UNITED MEXICAN STATES
Influenza Prevention and Control Project
CONTENTS
Data Sheet
A. Basic Information ................................................................................. Error! Bookmark not defined. B. Key Dates .............................................................................................. Error! Bookmark not defined.
C. Ratings Summary ................................................................................. Error! Bookmark not defined. D. Sector and Theme Codes ....................................................................... Error! Bookmark not defined. E. Bank Staff .............................................................................................. Error! Bookmark not defined.
F. Ratings of Project Performance in ISRs (if available).......................... Error! Bookmark not defined.
1. Context, Project Development Objectives, and Design ...................................................................... 1
2. Post-Approval Experience and Reasons for Cancellation ................................................................... 8 3. Assessment of Bank Performance ..................................................................................................... 12 4. Assessment of Borrower Performance .............................................................................................. 14
5. Lessons Learned ................................................................................................................................ 15
Annex 1. Bank Lending and Implementation Support/Supervision Processes ......................................... 17 Annex 2. List of Supporting Documents .................................................................................................. 19 MAP IBRD 33447R .................................................................................................................................. 20

1
1. Context, Project Development Objectives, and Design
1. Country Background. As Mexico neared the end of the annual influenza season in early
2009, health officials had noticed an unusual increase in patients presenting flu-like symptoms.
Testing revealed that a new strain of influenza A/H1N1 was responsible for the infections. By
mid-June, the spread of A/H1N1 around the world had led the WHO to declare a Phase 6
Pandemic Alert, which according to that agency was an indication that “a global pandemic is
underway” and that “actions should shift from preparedness to response”. By the time the
negotiations of a proposed loan in the amount of US$491 million to the United Mexican States
(the Borrower) in support of the Influenza Prevention and Control Project (the Project) were
being concluded in September 2009, there had been more than 52,000 laboratorial-confirmed
cases causing the death of more than 350 people in Mexico. Health care providers had reported
more than 175,000 clinical cases, according to which the Bank estimated that the total number of
infections exceeded 347,000.
2. At the same time, in 2009, Mexico was expected to experience its sharpest economic
contraction since the 1994-95 peso crisis: the Secretaría de Hacienda y Crédito Público (SHCP,
the Ministry of Finance and Public Credit) had in August projected that GDP would decline 6.8
percent, a sharp drop from the moderate growth of the previous four years. The cause of this
contraction was the global financial crisis that had precipitated a sharp drop in the demand for
Mexico’s exports. In addition, the global financial crisis had affected Mexico’s economy
through lower oil prices, capital flight (and consequent credit contraction) and a decline in
remittances (with resultant reduction in consumer demand). The economic contraction had
contributed to a large projected budget deficit for 2009, at the time projected to reach 2.1 percent
of GDP that circumscribed the Government’s ability to direct resources toward its response to
the A/H1N1 influenza outbreak that was affecting its population.
3. Reciprocally, the A/H1N1 epidemic was further weakening fiscal and macroeconomic
prospects. Direct public expenditures on the response to the first wave of A/H1N1 were
estimated by the Government to have exceeded US$600 million, and the macroeconomic impact
of the epidemic was estimated by the Government and the Bank to range from 0.3 to 0.8 percent
of GDP. The A/H1N1 epidemic was affecting the economy through lost revenues due to reduced
demand from social distancing, particularly in the retail sector, as well as through a severe drop
in tourism revenue. Further, the economic downturn was expected to result in an increase in
poverty, thereby creating conditions that could facilitate the spread of the A/H1N1 virus.
4. Adding to the Government’s concerns was the fact that epidemiologists, based on the
patterns of past influenza pandemics, expected that a second wave of A/H1N1 would affect
Mexico during the winter, and that by then the virus could have mutated into a more virulent
strain.
5. At the same time, the A/H1N1 epidemic and the economic contraction threatened human
development and specifically health outcomes in Mexico, many of which were already
incommensurate with the country’s income level. While Mexico’s overall Human Development
Index (HDI) was close to that of countries with similar levels of GDP per capita, some outcomes
were closer to those much poorer countries. Infant mortality, at 28 per 1000 live births, was

2
above the expected level for a country with Mexico’s per capita GDP. Further, human
development outcomes varied widely across Mexico’s federal entities (31 states and the Federal
District). For purposes of illustration, Mexico’s HDI ranked 52nd
among countries in the world,
while that of the State of Chiapas, would, if it were a country, result in a rank of 107th
in the
world.
6. Sector Background. Mexico’s health system was not ideally positioned to confront the
twin challenges of the epidemic and the recession. The Government was spending about 2.9
percent of GDP in health, well below the regional average of 3.6 percent for countries in the
Latin American and Caribbean region. Partly as a consequence of this, more than half of all
health expenditures were out-of-pocket. Social health insurance programs and national health
services operate in parallel with decentralized state-level health service provision; this
fragmentation was problematic because it constrained effective planning and sector-wide
coordination.
7. Conceived at the outset of the current administration, the Government’s National
Epidemiological Surveillance System (SINAVE) Plan 2007-2012 and its National Health Sector
Program 2007-2012, together focused, inter alia, on improving the epidemiological surveillance
and strengthening the response capacity of health services. The Government’s five-year plan for
SINAVE and the health sector emphasized the need for strengthening preparedness for disease
epidemics. The Bank was already supporting several pillars of the Government’s National
Health Sector Program through several ongoing and proposed operations (see Rationale for Bank
Involvement, below), but not directly in the area of health surveillance. The proposed Project
would complement and expand upon the Bank’s support to Mexico’s health sector, by supporting
the country in addressing the A/H1N1 epidemic and, in parallel, improving health surveillance.
8. Rationale for Bank Involvement. The rationale for the Bank’s involvement was strong.
At the Bank and IMF Spring Meetings in April 2009, Mexico’s Minister of Finance and Public
Credit and the Bank’s President agreed upon a package of assistance to help close the gap
between the costs of controlling the first wave of influenza A/H1N1, improving detection,
expanding its response capacity and the budget resources available that included the
reprogramming of an ongoing operation, preparing a new loan to support the Government’s
efforts, and securing grant funding under the Avian and Human Influenza Facility (AHIF). The
Bank responded initially by reprogramming US$25.7 million from the then ongoing Third Basic
Health Care Project to reimburse expenditures on laboratory equipment, laboratory supplies,
anti-viral medicines and medical supplies.1 Assistance under the AHIF was to support state
health systems in promoting preventive behaviors. The Project was expected to supplement
these resources.
1 In April 2009, the Bank agreed to restructure Third Basic Health Care Project, Project ID P066321 to allow the
then remaining loan funds (approximately US$25 million remaining in the Designated Account) as an immediate
financial assistance to purchase vaccines, pharmaceuticals and medical equipment and supplies. The second order
project restructuring was agreed and the Federal Ministry of Health presented the respective procurement plan that
would require higher management approval since the procurement involved retroactive financing of goods
purchased under direct contracting. In the end, the Bank did not approve procurement by direct contracting, and the
Bank worked with the Federal Ministry of Health to identify expenditures under the Project that would be eligible
for financing under the Loan, which had been fully disbursed by its Closing Date. Assistance under the emergency
restructuring of this project was also not utilized for the A/H1N1 response.
3
9. At the same time, the Bank had a long history of providing assistance to Mexico’s health
sector. Starting with the First Basic Health Care Project in the late 1980s, the Bank had
supported expanding the reach and improving the quality of health services, ensuring the
financial sustainability of social health insurance programs, expanding non-contributory health
insurance coverage of the poor, and developing institutional capacity in the health sector.
Following the implementation of three successive health projects, the Bank was, at the time,
working with the Government on the preparation of a project in support of the Government’s
non-contributory health insurance program, Seguro Popular, that provides universal health
coverage to Mexico’s population. The Bank had also engaged in extensive analytical work and
advisory services on health care issues in tandem with implementation support and project
preparation.
10. The Bank also had extensive experience in supporting Governments throughout the world
in preparing for and responding to influenza epidemics, in controlling infectious disease, and in
strengthening national epidemiological surveillance systems. This experience included that
acquired through the Global Program on Avian Influenza, the response to the SARS epidemic
and HIV/AIDS, especially in Latin America, and strengthening national epidemiological
surveillance systems also in Latin America.
11. The flexible design of the World Bank Group’s Country Partnership Strategy (CPS)
2008-2013 discussed by the Bank’s Board on April 8, 2008 facilitated a timely and effective
response to Mexico’s changing development needs in the face of the deteriorating global
financial and economic environment. The Project was consistent with the objectives and
principles of engagement of the CPS that included flexibility, fast response and selectivity in
addressing developing challenges. The Project, processed as an emergency response in
accordance with OP/BP 8.00, demonstrated the Bank’s flexibility and fast response capacity to
Mexico’s changing financing and development needs, and was closely aligned with two of the
development challenges identified in the CPS, namely sustainable growth through investment in
human capital and strengthening institutions.
12. The Project was consistent with OP/BP 8.00 since it would provide resources that the
Government needed to preserve human capital, restore economic activity, and prepare and
mitigate the effects of potential future health emergencies. By strengthening the Government’s
ability to monitor and control influenza epidemics, the Project was expected to support these
eligible objectives defined in OP 8.00. Alternative sources of financing had been considered,
including from the Bank’s Global Program for Avian and Human Influenza Preparedness
(GPAI), but given the magnitude of the resources that Mexico would require, the Bank opted for
preparing a stand-alone project that would be considered directly by its Board of Directors.
13. Development Objectives. The development objective of the Project was to strengthen the
capacity of the Mexican health system to monitor the spread of influenza viruses and to control
epidemic waves. The capacity to monitor the spread of influenza viruses rested on the
robustness of the SINAVE, the improvement of which entailed developing SINAVE’s
information technology system, upgrading Mexico’s national reference laboratory, training staff,
and strengthening data analysis, research and evidence-based public health decision making.
4
The capacity to control influenza epidemic waves depended on the infrastructure to effectively
distribute medicines, vaccines and medical supplies and the strategic reserves thereof.
Project Components. The Project comprised two components, as described below.
14. Component I: Strengthening the capacity to monitor the spread of influenza viruses
(US$64 million). The objective of this first component was to strengthen the capacity of the
Mexican health system to monitor influenza activity. The Project was expected to accomplish
this by: (a) strengthening the management and technical quality of the SINAVE through
developing SINAVE’s information technology system and upgrading the Borrower’s national
reference laboratory for epidemiological surveillance, including construction and equipping; (b)
ensuring the quality, relevance and timeliness of epidemiologic information through
organizational reforms in the Secretaría de Salud (the Borrower’s Federal Secretariat of Health,
SS) including the establishment of a central analysis unit and mobile units, setting up
epidemiological research programs to assess the relevance and deepen the understanding of
information collected, and certifying SINAVE according to international standards; and (c)
improving SINAVE’s human resource capacity through training its staff in new processes,
management schemes and bio-security in laboratories, applying new information technologies
and platforms, carrying out knowledge events promoting a culture of analysis, research and
dissemination of information for policy-making.
15. Component II: Strengthening the capacity to control epidemic waves of influenza
viruses (US$426 million). The objective of this second component was to strengthen the
capacity of the Mexican health system to control influenza epidemic waves. The Project
expected to accomplish this by strengthening the infrastructure to effectively distribute
medicines, vaccines and medical supplies, replenishing and expanding the country’s strategic
reserves thereof. In particular, the Government planned to vaccinate more than 20 million
Mexicans against A/H1N1 in the winter of 2009, as soon as the vaccine became available. The
proposed loan would reimburse the Government for the expenditures it had incurred during the
first wave of influenza A/H1N1 for the purchase of medicines, vaccines and medical supplies on
or after April 23, 2009, once it met the eligibility criteria under each of the Project components.
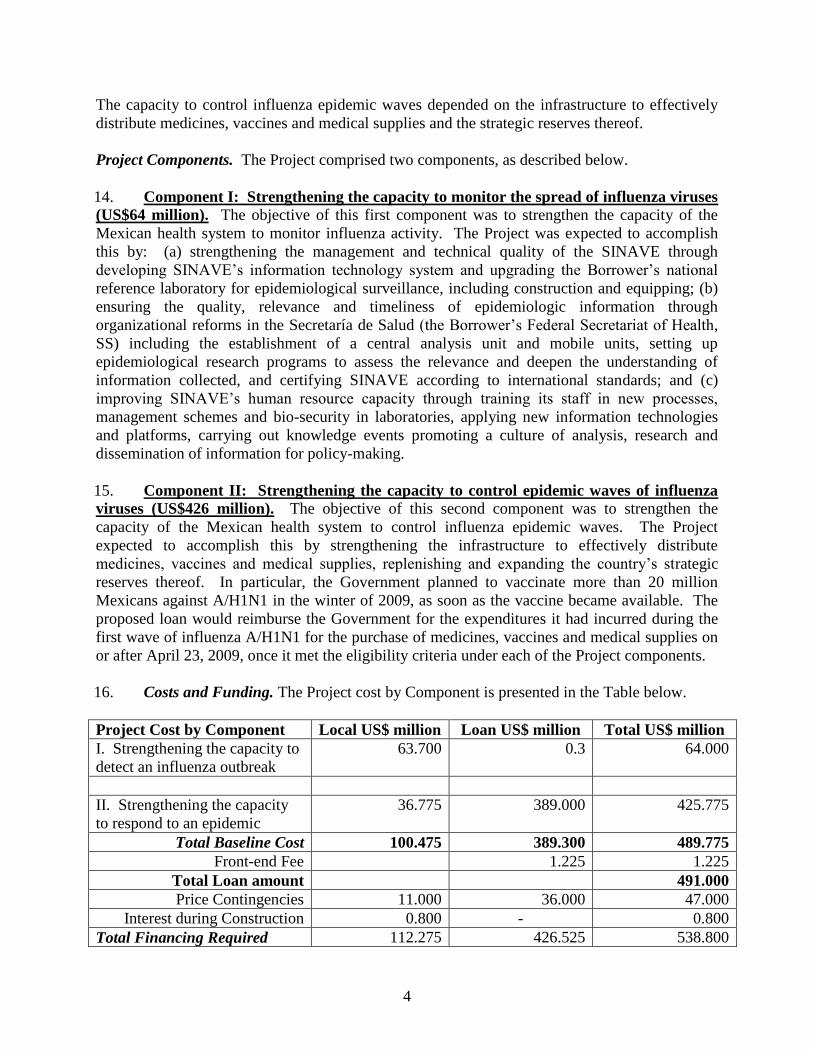
16. Costs and Funding. The Project cost by Component is presented in the Table below.
Project Cost by Component Local US$ million Loan US$ million Total US$ million
I. Strengthening the capacity to
detect an influenza outbreak
63.700 0.3 64.000
II. Strengthening the capacity
to respond to an epidemic
36.775 389.000 425.775
Total Baseline Cost 100.475 389.300 489.775
Front-end Fee 1.225 1.225
Total Loan amount 491.000
Price Contingencies 11.000 36.000 47.000
Interest during Construction 0.800 - 0.800
Total Financing Required 112.275 426.525 538.800

5
17. Implementation Arrangements. The Project would have been coordinated and
implemented using organizational structures and staff of the Federal Secretariat of Health (SS),
specifically through organizational units under the Under-Secretariat for Prevention and
Promotion in Health (UPPH), including the National Center for Epidemiological Surveillance
and Disease Control (CENAVECE), the National Center for Child and Adolescent Health
(CENSIA) and the Directorate of Operations. Within CENAVECE, the Adjunct Directorate for
Epidemiology (DGAE) and the Adjunct Directorate for Preventive Programs (DGAPP) would
have had important roles. The DGAE would have served as the Project Coordination Unit and
have led the implementation of the Project’s Component I. In close collaboration with DGAE,
DGAPP and CENSIA would have led the implementation of the Project’s Component II.
Although not formally incorporated as an implementing agency under the Project, BIRMEX, a
financially autonomous public limited company registered in Mexico, was the only agency
responsible for purchasing and delivering A/H1N1 vaccines, which were at the time in limited
supply, for the Government.2
18. The Directorate of Operations was to have supported DGAE, DGAPP and CENSIA in all
fiduciary tasks, including preparing and updating the Project’s Operational Manual and
procurement plans, carrying out the procurement of goods, works and services, preparing ex-post
procurement reviews, non-audited Interim Financial Reports, Project Financial Statements and
Statements of Expenditures, Records and Summary Sheets and preparing for Project audits. On
fiduciary matters, all units and in particular the Directorate of Operations would have been
supported by Nacional Financiera, a public financial agent with ample experience in supporting
the implementation of Bank-financed projects.
19. The Project was to have been implemented at the national level, including the central
acquisition of all works, goods and services. Yet, the impact of the Project was to depend on
complementary activities carried out by federal entities. For this, DGAE was to ensure that
project activities were incorporated into Cooperation Agreements that were routinely entered
into by the Federal Secretariat of Health with each of the federal entities. These Cooperation
Agreements were to include, inter alia, the federal entities’ obligations to carry out
complementary activities, for the distribution of medicines and vaccines and to comply with the
Project’s safeguard requirements.
20. Eligible expenditures financed by the Federal Secretariat of Health with resources from
the National Budget were to be reimbursed by the Bank on the basis of supporting documents.
Eligible expenditures paid by the Government between April 23, 2009 (the date the new
influenza strain had been identified) and the date of loan signing could have been reimbursed up
to an amount not exceeding 40 percent of the loan amount.
21. Risk Analysis. The Emergency Project Paper, in its section on Project Risks and
Mitigating Measures, identified four key risks (although it provided no risk ratings), and
corresponding mitigating measures, as follows:
2 The contracts with BIRMEX provided the Government not only with access to large amounts of influenza vaccines
despite the global shortage, but also provided these vaccines at prices below those offered by competitors and the
Pan American Health Organization
6
i. Mexico could face challenges in preparing for a second wave of the A/H1N1 influenza
epidemic in particular, its response capacity could be insufficient to control a second
wave. Global production of the A/H1N1 vaccine (when it was developed) was expected
to be insufficient to meet global demand in the short-term, the national vaccination
program might not have the capacity to vaccinate large groups of the population, and
Mexico’s stock of anti-viral drugs would likely be insufficient to respond to a second
wave with an attack rate of more than one percent. The Government was taking steps to
mitigate this risk, including: the strategic reserve of vaccines was being stocked to
inoculate more than 20 million people; Mexico in partnership with a leading
pharmaceutical company was developing domestic vaccine production capacity that
would start in the Spring of 2011 and through that partnership, had preferential access to
20 million doses of an A/H1N1 vaccine as soon as they became available; and the
Government with financing under the Loan would invest heavily in strengthening the
country’s cold chain as the most likely bottleneck for further scaling up of its vaccination
program (that in any given year had the capacity to vaccinate close to 20 million against
seasonal influenza).
ii. The A/H1N1 vaccine that was being developed could be expected to cause adverse health
events more frequently and of more severe nature than anticipated and tolerable. This
risk for a new vaccine was considered to be higher than that of a well-established vaccine
since it would only have been tested in clinical trials with some of the potential target
population. The risk of intolerable side effects would be mitigated by close monitoring
of adverse health event and changes to vaccination protocols, if necessary. Mexico was
considered to have a comprehensive system for the surveillance of vaccine associated
events, and staff of health facilities participating in vaccination campaigns had been
trained to notify adverse events and investigate causalities.
iii. Implementation capacity constraints could hamper the timely execution of Project
activities and investment in information technology might not be sustainable. This
encompassed three main risks that had been foreseen: that human resource capacity at
the UPPH were already taxed with responding to the epidemic, and would likely have
limited time and resources to manage the Project, that large investments in information
technology required corresponding investments in maintenance capacity and also that
these information technology investments would call for a challenging cultural shift
toward real-time analysis and effective dissemination of epidemiological intelligence.
These risks were considered to be mitigated by the planned upgrading and staffing of the
DGAE into a General Directorate, the hiring of fiduciary specialists into the Directorate
of Operations together with possible support from other units, the probable out-sourcing
of information technology support services, including the possibility of leasing rather
than purchasing hardware, and significant training of SINAVE staff to support the
cultural change.
iv. Reductions in fiscal space expected as a consequence of the economic crisis could reduce
the Government’s budget for the Project’s activities. The severe economic downturn was
expected to produce a sharp contraction in fiscal space and force difficult trade-offs. The
Government had taken steps to mitigate this risk: the President publicly committed
7
himself to some of the Project’s objectives and intervened personally to reduce planned
budget cuts to the Federal Secretariat of Health’s’ budget, the Federal Secretariat of
Finance (SHCP) and the Federal Secretariat of Health had begun talks about additional
budgetary allocations for A/H1N1 preparedness and response in 2009, and the
Government considered drawing resources from the Trust Fund for Catastrophic Health
Expenditures.
22. In addition, the Project’s financial management residual risk was considered to be
Modest, with the only financial management risk rated Substantial being that related to Entity
risk; while the Federal Secretariat of Health had implemented several Bank-financed projects,
the Project’s Project Coordination Unit had not. The Project’s Procurement risk was considered
to be Substantial, based mostly on the risk posed by the lack of experience of staff in the
Directorate of Operations in carrying out procurement processes in accordance with Bank
Guidelines, compounded by the emergency nature of the Project.
23. Quality at Entry. The Project responded to the high-level request by the Government
and the agreement at the highest level in the Bank to support Mexico in addressing the A/H1N1
influenza epidemic (see Rationale for Bank Involvement). This high-level agreement put
pressure on both the Government and the Bank’s teams to deliver the agreed assistance in view
of the visibility it had generated. The request came less than one and a half months from the
outset of the new strain of the influenza in Mexico. Project preparation benefitted from an in-
depth knowledge of Mexico’s health sector developed over the course of over twenty years of
financial and technical support and a strong policy dialogue with Government authorities on
sector-related strategy and issues. As a result of this, the activities to be supported under the
Project would have been reinforced by related Bank operations, ongoing and under preparation.
They would not be carried out in a vacuum, but rather as part of a comprehensive plan to
strengthen the capacity of Mexico’s heath system to respond to the immediate A/H1N1 challenge
that the system faced, and in the process to leave in place a stronger capacity of monitoring and
controlling epidemic waves. The Project was also prepared within a package of emergency
support that included in addition the restructuring of an ongoing project3 and the securing of
grant funding under the Avian and Human Influenza Facility.
24. The Project was prepared expeditiously—in less than two months--under OP/BP 8.00 and
included emergency recovery and activities aimed at preparedness and mitigation, through
improved surveillance. Loan negotiations began in July 2009, but continued on until October
2009. This delay in concluding negotiations reflected the lengthy discussions between the SHCP
and the Federal Secretariat of Health regarding the amount of resources the latter could absorb
and its need for additional budgetary allocations in order to implement the Project, especially
since external financing is normally not incremental to an executing agency’s budget in Mexico.
Before loan negotiations, the Bank had anticipated that the non-incremental financing and high
transaction costs (i.e., complying with Bank fiduciary and other requirements) could lead to
incentive issues with the Federal Secretariat of Health and had already explored the possibilities
for providing assistance through alternative lending instruments, under the then recently Board-
approved changes to the Avian and Human Influenza Facility (AHIF) financing facility,
including the Development Policy Lending with Catastrophe Deferred Drawdown Option (CAT
3 Third Basic Health Care Project, Project ID No. P066321

8
DDO). However, after considerable internal discussion, the team was advised to follow a
Specific Investment Loan option, in accordance with OP/BP 8.00, and agreed to include
financing of additional staff within the Federal Secretariat of Health to coordinate activities and
ensure compliance with the Bank’s fiduciary requirements, which the Federal Secretariat of
Health accepted in end-2009.
25. The Catastrophe Deferred Draw Down option was not considered because financing
available through this scheme was more in the realm of longer term recovery and reconstruction
needs, whereas the Project was designed to cover a shorter term emergency program for
containing the epidemic (with some longer term surveillance activities) and not for economic
recovery.
2. Post-Approval Experience and Reasons for Cancellation
26. The US$491 million Loan for the Project was approved by the Bank’s Board on
November 24, 2009 and signed on November 30, 2009. After three extensions of the original
February 26, 2010 effectiveness deadline, the Loan lapsed without becoming effective on
February 28, 2011.4 The factors that, combined, and to a greater or lesser extent led to this
outcome included: (i) the lack of incentive for Federal Secretariat of Health to utilize the loan in
view of its lack of incremental financing, (ii) problems in utilizing retroactive finance according
to Bank policies, (iii) a lack of consensus for moving forward with a loan restructuring, and (iv)
a milder than expected course of the A/H1N1 epidemic that translated into reduced budgetary
allocations to the Federal Secretariat of Health. Despite the problems with the Bank’s loan, the
Federal Secretariat of Health made in the period following approval until now significant
progress towards the Project’s objectives, with continued technical and advisory support from
the Bank.
27. Lack of Incentive to Utilize the Loan. Mexico’s budget reality is such that external
finance is generally not incremental to the executing agencies. Therefore, the proceeds of the
Bank’s loan were to accrue to the country’s budget through SHCP that had pre-financed
expenditures for the purchase of the anti-virals and vaccines, and for the expenditures that
Federal Secretariat of Health incurred and would incur for the implementation of activities under
Component I under its normal budget allocation. However, the external financing had important
implications to the Federal Secretariat of Health in terms of its need to comply with the Project’s
fiduciary requirements even though the financing associated with the Project would produce no
incrementality to its budget. Although an important counter-balance to this was the technical
implementation support that the Federal Secretariat of Health was to receive from the Bank
under the Project, overall there was little incentive of the Federal Secretariat of Health to
implement the Project with Bank financing. Negotiations were affected by the lengthy
discussions between SHCP and Federal Secretariat of Health as to the overall project cost, with
Federal Secretariat of Health requesting that at least some of the external finance be provided in
the form of incremental finance to the agency. For the same reason, this lack of incentive to the
SS later affected the decision to move ahead with a loan restructuring.
4 The three extensions were as follows: a six-month extension until August 31, 2010, followed by a three-month
extension until November 30, 2010, followed by a final three-month extension until February 28, 2011.

9
28. Problems in Utilizing Retroactive Finance. In line with OP/BP 8.00, the Loan had
provisions to reimburse the Government for up to US$196.4 million (or 40 percent of the loan
amount) for eligible expenditures incurred since the outbreak of the new A/H1N1 influenza virus
on April 23, 2009 under expedited Bank procurement procedures. Nevertheless, despite the
emergency, the Government was not able to obtain retroactive financing of the goods
(particularly vaccines and anti-viral medicines) that were procured and delivered prior to the
signing of the Loan Agreement. Loan signing only took place about seven months after the
outbreak of A/H1N1, and by the time the Government had incurred already a significant amount
of retroactive expenditures. The considerable delays towards effectiveness, caused mostly by the
need for internal clearances described below, only made the problems in utilizing retroactive
finance more important in the final outcome.
29. The Task Team requested internal clearances for the direct contracting for the purchase
of the anti-virals and the A/H1N1 influenza and seasonal influenza vaccines in the amount of
approximately US$150 million. The direct contracting for the purchase of anti-virals was
authorized but would have required a restructuring to include the supplier, BIRMEX, a
financially autonomous public limited company in Mexico as an implementing agency under the
Project (and not contracted as an independent provider). Authorization for retroactively
reimbursing amounts for both purchases was subject to the retrofitting of each of the contracts
with primary suppliers with anticorruption clauses as required by the Bank’s anticorruption
guidelines. However, in accordance with Mexico’s legal framework, it was not possible for the
Government to retrofit vaccine and anti-viral medicine contracts to comply with the Bank’s
guidelines. While the Government of Mexico during negotiations had in general concurred to
retrofit the contract with suppliers of anti-viral medicines and A/H1N1 vaccines, upon
consultation with the Federal Secretariat of Health’s Legal Department, the Government
concluded that Bank conditions for retroactive financing could not be reconciled with federal
legislation and regulation. More specifically, any amendment of closed contracts to introduce
additional language (including language consistent with the anti-corruption guidelines) would be
inconsistent with internal regulations.
30. Possible Project Restructuring. With this constraint in utilizing retroactive financing
(that represented such a large amount of the Loan), the Government and the Bank began
discussing the possibility of a project restructuring that would include additional activities aimed
at strengthening Mexico’s efforts to monitor the spread of influenza viruses and controlling
epidemic waves, consistent with the Project’s Development Objectives (PDO). The Bank began
preparing a Level One Restructuring that would respond to the Government’s request to expand
the scope of the Project to capture epidemic response outcomes. The PDOs, as approved focused
the Project merely on capacity. The proposed Restructuring would expand the scope of the
Project’s second objective to respond, not only control, epidemic waves, by introducing a third
project component that would entail: (a) an expansion of the scope of the Project’s Indigenous
People Plan to ensure that indigenous people benefitted from the response; (b) the introduction of
the national Commission of Social Protection in Health as one of the Project’s implementing
agencies; (c) the adoption of the premium of the Popular Health Insurance as a new category of
eligible expenditures to finance the delivery of services during the epidemic (with expenditures
incurred between April 23, 2009 and loan signing to be considered as retroactive finance, subject

10
to the cap of 40 percent of the loan amount); and (d) adjustments to the financial management
and disbursement arrangements to reflect the new arrangements for this new component.
31. As background, the response to the epidemic had been financed by and large through the
Social Protection System in Health (SPSH). From January to October 2009, the SPSH provided
41.5 million consultations for its beneficiaries, 25.9 percent more than were registered in the
same period of the previous year, while affiliating 4.2 million new beneficiaries. Service
delivery, through the use of mobile health units and the establishment of temporary clinics, was
complemented by communications campaigns promoting the use of health services by
individuals with influenza symptoms but discouraging the use of health services for non-urgent
matters. Given the increase in health service delivery and the effect of communication
campaigns during the peak of the epidemic, the Government estimates that at least 30 percent of
consultations provided to beneficiaries of the SPSH’s Popular Health Insurance during 2009 and
the first half of 2010 were related to influenza5. As part of the proposed Restructuring, the
Project’s results and monitoring framework, its institutional arrangements, the Environmental
Action Plan and the Indigenous Peoples Plan would be adjusted to conform to a restructured
project. The proposal for a Project Restructuring never moved forward, in part due to the lack of
incentive to the Federal Secretariat of Health, even though both the Federal Secretariat of
Finance and the Federal Secretariat of Health recognized that it would address the disbursement
issues that had thus far affected the Project and Loan.
32. Milder than expected A/H1N1 Epidemic. The Mexican Congress did not authorize the
proposed 2010 budget for vaccines and medicines, thereby declining to maintain funding that
had become available during the course of the epidemic in 2009. Then, by mid-July 2010,
having caused more than 72,500 laboratory-confirmed infections and the death of more than
1,300 people in Mexico, infection trends of the A/H1N1 virus were confirmed to be on a decline,
which in turn led the SHCP to allocate a significantly smaller budget for project activities to be
carried out in 2010. In August of the same year, the World Health Organization reviewed global
A/H1N1 epidemic trends calling for a shift in focus towards “post-pandemic period” strategies.
The nature of the Project, given this turn-around in the epidemic, shifted from one of emergency
response to one of only strengthening longer-term capacity and ability to respond to future
emergencies. Although the Federal Secretariat of Health remained fully committed to the
Project’s objectives, especially to its Component I that aimed to strengthen Mexico’s
epidemiological surveillance capacity (with or without restructuring), and to a proposed Project
Restructuring, it required incremental budgetary resources from the Bank’s Loan to produce the
expected outcomes. Given the nature of external financing in Mexico, however, the Bank’s
disbursements would not be incremental to the Federal Secretariat of Health’s budget, and the SS
would have to implement the Project with a significantly reduced budget allocation.
33. Progress Towards Project Objectives. Despite the absence of disbursements from the
Bank’s Loan, the Federal Secretariat of Health made significant progress towards the PDOs, as
5 The Popular Health Insurance is a key pillar of Mexico’s Social Protection System in Health serving people
without contributory social security. The Bank is financing the Popular Health Insurance under the Project in
Support to the Social Protection System in Health Loan (Loan 7860-ME)
11
measured by the Project’s Outcome Indicators and Intermediate Outcome Indicators, through
December 31, 2010.6 These results were as follows:
34. The SINAVE performance index7 and the SISVEFLU index8 were indicators selected to
measure progress towards the first PDO, that is: strengthen the capacity of the Mexican health
system to monitor the spread of influenza viruses. The SINAVE performance index improved
from a baseline of 79.8 in December 2008 to 81.5 in December 2010 (against a target of 83.0 by
December 2011). Similarly, the SISVEFLU index improved from a baseline of 49.0 in
December 2008 to 61.0 in December 2010 (against a target of 65.0 by December 2011). These
improvements were made possible through progress towards the achievement of intermediate
outcomes under the Project, including:
Establishment of a central Epidemiological Analysis Unit, improving the quality of
epidemiological information produced by the SINAVE. This Unit developed a number
of knowledge products for policy decision-making including the analysis of case studies
of the first A/H1N1 epidemic wave;
Carrying out an evaluation of the SINAVE information technology platform.
Findings of this evaluation, together with lessons learned from an analysis of the
implementation of the Canadian epidemiological surveillance system guided the
development of a plan to upgrade the SINAVE platform;
Strengthening the capacity of sentinel health facilities and administrative health units
through the provision of equipment and training of staff. By December 31, 2010, 47
percent of state jurisdiction epidemiological offices were fully equipped and connected to
the new information technology platform (against a baseline of zero and a target of 80
percent by June 30, 2012), and 31 percent of sentinel health facilities had their staff
trained in the use of the new information technology platform (against a baseline of zero
and a target of 80 percent by June 30, 2012).
35. Progress towards the Project’s second PDO, that is, to strengthen the capacity of the
Mexican health system to control epidemic waves of influenza, was to be measured by two
6 In part, this is because Bank financing and disbursements in Mexico are not incremental to the implementing
agency. The Federal Secretariat of Health had budgetary allocations approved by SHCP, and would implement the
Project using those allocations. Bank disbursements were to reimburse the Treasury for previously-allocated
amounts. 7 The SINAVE index comprises measures for three of it four sub-systems, including nine different elements, as
follows: (1) the system for the weekly notification of reportable diseases; (2) the sentinel health facility surveillance
system; (3) the surveillance system for acute flaccid paralysis; (4) the surveillance system for acute febrile illness;
(5) the surveillance system for HIV/AIDS; (6) the surveillance system for diabetes; (7) the surveillance system for
neural tube defects; (8) the registry system for malignant neoplasms, and (9) the surveillance system for addictions.
Examples of indicators for these elements include: the percentage of medical centers reporting cases in a timely
manner, the number of consecutive weeks of reporting, the number of notified cases of specific diseases among
children, the percentage of samples drawn according to standards and percentage of probable cases tested in a timely
manner. Data for these indicators is provided by health facilities, sentinel sites and laboratories across the country
and consolidated by the SINAVE at the federal level. 8 The SISVEFLU index comprises measures for the timeliness and quality of sample processing, and the use and the
representativeness of generated information. Specific measures include: timely notification of probable cases,
timely investigation of cases, adequacy of sample collection, timeliness of shipment of samples, concordance of
samples, compliance with case identification goals and follow-up of diagnosed and notified cases. Data for this
index is provided by the national laboratory network and consolidated annually by the federal “Caminando a la
Excelencia” program.
12
outcome indicators: (1) percentage of population vaccinated against influenza A/H1N1, and (2)
number of antiviral treatments stockpiles. The Project was able to exceed the targets for both of
these indicators. By December 2010, 24 percent of the population had been vaccinated against
A/H1N1 (against a baseline of zero and a target of 15 percent by June 30, 2012), and the
Government purchased more than 2.150 million treatments of antiviral medicines to replenish
and expand the country’s strategic reserves (against a baseline stockpile of 1.2 million in October
2009 and a target of 2.150 million by June 30, 2012). This was possible, in part, through efforts
to update equipment necessary for the correct functioning of the cold chain for the proper
distribution of vaccines.
36. The Government, however, postponed the construction of Mexico’s national reference
laboratory, instead allocating limited resources to activities that had an immediate impact on the
control of the A/H1N1 epidemic.
3. Assessment of Bank Performance
Rating: Moderately Satisfactory
37. The Bank’s Performance is rated Moderately Satisfactory. The Project was prepared
expeditiously, within the framework of emergency assistance, in accordance with OP/BP 8.00,
that included the Project, a first order restructuring of the now completed Third Basic Health
Care Project, and a grant, approved by the Avian and Human Influenza Facility that would
ensure the successful production and dissemination of messages on influenza-related behavior
change. The Bank’s team was country-based, very experienced, and had a thorough knowledge
of Mexico’s health sector and a very active and productive engagement and policy dialogue with
sector authorities developed over years of preparation and supervision of new and ongoing
operations, as well as through an active program of non-lending, analytical and advisory
services. It brought this experience and dialogue, together with the Bank’s broader lessons of
experience with emergency responses in health to bear in assisting the Government first in
putting its emergency response in place, and, concurrently, in delivering and integrated package
of assistance, consistent with the CPS and with the Bank’s then ongoing assistance program in
health. The Project’s focus not only on emergency finance of needed inputs, but also on
preparedness and mitigation of future health emergencies through strengthening Mexico’s
epidemiological surveillance capacity was commendable. Realizing that the incentive issues
surrounding non-incremental finance could come to affect the negotiation and implementation of
the Project, the team actively explored the use of alternative instruments that would get around
possible problems.
38. The Bank’s team was persistent in trying to help the Government in getting the Loan
effective and disbursing, and worked closely with the SS through continuous dialogue to support
the activities the agency was carrying out. Despite repeated efforts to find a solution to the
impasse with regard to the financing of retroactive expenditures for vaccines and anti-virals, it
became clear in November 2009 that this would not be possible. The Bank then opted for
working with the Government to prepare a first order Project Restructuring that would allow the
Loan to finance Mexico’s emergency response efforts in an alternative manner. However, with
the A/H1N1 epidemic no longer on the radar screen, and consequently reduced budgetary

13
allocations to the Federal Secretariat of Health (and the non-incremental nature of Bank finance
to executing agencies in Mexico) the processing of the by then fully developed Restructuring
proposal never moved forward.
Bank performance in providing technical assistance during the epidemic outbreak
39. The Bank carried out an assessment of the performance of the Mexican epidemiological
surveillance system (SINAVE), identifying areas in which the Canadian Network for Public
Health Intelligence (CNPHI) could serve as a model to help improve SINAVE’s performance,
and to develop a strategy for developing or adapting technology. The Bank also supported the
GoM through a US$1.7 million Avian and Human Influenza (AHIF) grant, in the development of
a national education communication campaign for influenza prevention and comprehensive risk
communication strategies at the local level. The Bank supported a number of decisions and
actions taken by the GoM that contributed effectively to contain the epidemic.
Bank performance on project processing
40. The Project was processed expeditiously - in less than two months- under OP/BP 8.00.
The Project was consistent with the policy, but emergency purchases under the Project were
treated by the Bank as regular purchases typical of SIL operations. The loan provided for
retroactive financing, up to 40% for goods that had been procured under the Borrower’s
emergency procurement procedures. However, Bank policy on Fraud and Corruption requires
that bidders, suppliers and contractors under Bank-financed contracts include the applicable
anticorruption clauses (ACC). This required the Government to retrofit contracts that had been
executed months earlier, many of them just a few days after the epidemic outbreak started. As
this contravened Mexican legislation, the Government was not able to do so because it
contravened Mexican legislation and internal regulations.
41. As mandated by the Bank procedural guidelines for rapid response to crisis and
emergencies, in emergency situations, procurement actions need to be facilitated through higher
levels of delegation to the Borrower and, within the Bank, through the delegation by RPMs
(Regional Procurement Managers) of higher levels of approval authority to Bank Procurement
Specialists on task teams to allow for the use of direct contracting, shopping, and simpler
procurement methods for the delivery of urgently needed services and goods. However, in the
case of this Project, the procurement delegation prerogative was not in effect due to the loan
amount and the contracts amount that needed to be cleared to allow the Government to access to
retroactive financing.
42. Since the emergency started in April 2009, the Bank had anticipated that the non-
incremental financing and high transaction costs (i.e., complying with Bank fiduciary and other
requirements) could lead to incentive issues with the Federal Secretariat of Health and explored
the possibilities for providing assistance through alternative lending instruments, under the then
recently Board-approved changes to the Avian and Human Influenza Facility (AHIF) financing
facility, including the Development Policy Lending with Catastrophe Deferred Drawdown
Option (CAT DDO). However, after considerable internal discussion, the team was advised to
follow a Specific Investment Loan option, in accordance with OP/BP 8.00. Finally, despite the
14
fact that the Project was prepared in less than two months, the lengthy negotiations (3 months)
affected project processing. The considerable delays towards effectiveness, caused mostly by the
need for internal procurement clearances, made retroactive finance impossible. It also made the
Government to lose interest in the loan.
4. Assessment of Borrower Performance Rating: Moderately Satisfactory
43. The Borrower’s Performance is rated Moderately Satisfactory. The Government’s
response to the A/H1N1 outbreak was swift, as was its request to the Bank for assistance. The
SHCP allocated resources needed to pre-finance needed medicines and vaccines, when they
became available, using their internal procurement procedures, and established arrangements for
purchase of vaccines, which in any event were streamlined given proprietary rights and the
global shortage of A/H1N1 vaccines at the time. The highest level of Government intervened
initially to preclude budget cuts to the Federal Secretariat of Health, despite a severe economic
downturn that had reduced the Government’s fiscal space. This support for sustained budget
allocations fell somewhat, however, once the epidemic lost steam. The Federal Secretariat of
Health, as the main implementing agency, carried out the Project within its allocated budget. In
so doing, it remained fully committed to the Project’s objectives. When it became clear that it
would not be possible to utilize loan resources, either as originally approved or as it could have
been restructured neither the Federal Secretariat of Finance nor the Federal Secretariat of Health
wanted to request the Loan’s cancellation, and the Loan was left to lapse.
Government performance during the epidemic outbreak
44. A number of decisions and actions taken by the GoM contributed to attenuate the
magnitude and the rate of disease spread. Such actions allowed saving valuable time to
understand the virulence and transmission features of the virus and to distribute medical
countermeasures in health care facilities. Although quick and effective action was taken, Mexico
needed to strengthen the epidemiologic surveillance system, including the public health
laboratories and information tools. The project was envisaged as a means to achieving this. Since
the approval of the Project in November, 2009, progress towards achieving project objectives
was considerable. The GoM implemented a number of actions which have strengthened its
capacity to monitor effectively, distribute vaccines, medicines and medical supplies as well as
expanding the country’s strategic reserves of these medical supplies.
Government performance in project processing
45. The Project was affected by the enduring discussions between the Ministry of Finance
(SHCP) and the Federal Ministry of Health throughout the whole project preparation and
processing. Despite the enthusiasm regarding the Project Development Objectives, and
especially to its Component I, there were doubts on the part of the Federal Secretariat of Health
with regard to committing to a Bank loan in the absence of confirmation of additional budgetary
allocations for the Federal Secretariat of Health. The lack of clarity around this issue resulted in
lengthy loan negotiations, which lasted from July to October 2009. During this period, the
discussions were mainly centered on the amount of resources that the Federal Secretariat of

15
Health could absorb and its need for additional budgetary allocations to implement the project.
The discussions were further complicated in November 2009, shortly after the project was
approved, when it became clear that that financing of retroactive expenditures for vaccines and
anti-virals would not be possible. In January 2010 when the Mexican Congress refused to
maintain funding for vaccines and medicines that had become available during the course of the
epidemic in 2009, the Government interest in the project decreased significantly. This complex
process explains the three project effectiveness extensions. Finally, following the decline in
infection rates confirmed in mid-July 2010, the Government allowed the third deadline to lapse
on February 28, 2011.
46. The Government was not willing to proceed with the proposed restructuring, although it
could have provided a straightforward manner of disbursing retroactive finance against an easy
to disburse category of expenditures: eligible federal social contributions to the premium of the
Popular Health Insurance to cover the costs of medical services provided during the influenza
epidemic. While there may not have been any incentive for the Federal Secretariat of Health in
the restructuring, it would have provided an alternative for disbursement to the Government that
was most definitely within its program of emergency response to the A/H1N1 epidemic. But, a
restructuring along these lines would have required bringing another implementing agency on
board, and, by that time the epidemic had subsided and, more importantly, the Bank’s then
recently approved loan for the Project in Support of the Social Protection System in Health
(Loan 7860-ME) had become effective and begun disbursing, thereby providing finance for the
premiums of the Popular Health Insurance (Seguro Popular).
5. Lessons Learned
47. The Project, its design and implementation experience offer a couple of lessons that are
relevant to the design of Bank-financed emergency operations, especially those related to
epidemics.
48. Non-incremental financing incentives. In Mexico, external financing is generally not
incremental for sector agencies. This has important implications for executing agencies and their
willingness to comply with the often-extensive requirements of Bank-financed projects.
Although the strong technical implementation support that those agencies receive under Bank-
financed projects is welcome, the Bank should reassess the value added of a non-additional loan
in middle income countries such as Mexico, which nevertheless comes with Bank fiduciary and
safeguard requirements on the sectors.
49. GAC policy and its application under emergency situations. Although GAC measures
aim to limit exposure to fraud and corruption risks and manage reputational risks of the Bank and
the Borrower, these limit the flexibility of quickly prepared and disbursed operations. There is
room for improvement in the way the Bank engages with countries on GAC issues in general,
but particularly in emergency situations.
50. Consistency of emergency policies (OP/BP 8.00) with other fiduciary policies. Even
though OP/BP 8.0 operational guiding principles have been developed bearing in mind the need
to respond with speed, simplicity and flexibility in emergency situations, the policy is not fully

16
aligned with other fiduciary policies and guidelines, such as GAC and procurement. Therefore,
policies may benefit from reassessment in terms of their compatibility; and task teams will
benefit from more explicit guidance on the application of emergency policies, especially when
dealing with health emergencies.
51. Efficacy of the emergency instrument in health emergencies. In public health
emergencies it is difficult to predict the course of the emergency or the damage caused in terms
of human lives and health. Other instruments, such as a DPL or a CAT-DDO, may provide a
better option for responding to client needs in view of the fiduciary requirements related to the
emergency purchases.
52. Different Nature of Emergencies requires different responses. The Bank supports
different borrowers in responding to very different types of emergencies under OP/BP 8.00. The
unique element of this Project was the lack of information of the A/H1N1 Influenza, followed by
the lack of predictability of the eventual outcome of the epidemic. As compared to emergencies
relating to natural disasters that typically consist of more predictable and quantifiable damages
and losses, the emergency supported by the Project was a dynamic one. There was an outbreak of
a previously unknown virus that spread rapidly, and the World Health Organization had declared
a Phase 6 Pandemic Alert, indicating that a global pandemic was underway. Expectations were
that Mexico would experience a second wave of A/H1N1 in the winter, and that by then the virus
would have mutated into a more virulent strain.
53. Implications for the Bank in responding to public health emergencies. There are a
number of aspects that the Bank needs to consider when responding to public health
emergencies. First, the preparation of pandemic-related operations requires even greater urgency
in response, since the emergency is ongoing and possibly expanding exponentially. Second, the
preparation of these operations faces much greater uncertainty than that of other emergency
responses. Finally, since there is greater uncertainty of the emergency’s outcome, the Project
and the achievement of its PDOs face greater risks, especially those related to the longer-term
preparedness and mitigation. In the case of this Project, when the infection trends of the
A/H1N1 Influenza were, thankfully, confirmed to be on a decline, activities for improved
epidemiological surveillance continued, but with less budgetary support. The difficulty in
finding an easy solution also would seem to imply that these operations pose a higher
reputational risk to the Bank.

17
ANNEXES
Annex 1. Bank Lending and Implementation Support/Supervision Processes
(a) Task Team members
Names Title Unit Responsibility/Specialty
Lending (from Task Team in Emergency Project Paper Data Sheet)
Christoph Kurowski Senior Health Specialist LCSHD Task Team Leader
Claudia Macias
Senior Operations Officer LCSHH NCO Task Team Leader
Maria E. Castro-Munoz
Senior Social Development
SpecialistConsultant
LCSSO
Marta Elena Molares-
Halberg,
Lead Counsel LEGLA
Francis V. Fragano
Senior Environmental
Specialist
LCSDE
Manuel Antonio Vargas
Madrigal
Senior Financial
Management Specialist
LCSFM
Dmitri Gourfinkel,
Financial Management
Analyst
LCSFM
Snezana B. Mitrovic, Lead Procurement Specialist LCSPT
Jose M. Martinez
Senior Procurement
Specialist
LCSPT
Jean-Jacques Verdeaux
Senior Procurement
Specialist
LCSPT
Tomas Socias
Senior Procurement
Specialist
LCSPT
Gabriel Penaloza Procurement Analyst LCSPT
Silvia Moran-Porche Procurement Assistant LCSPT
Judith Marcano Williams Program Assistant LCSHD
Manuela Villar Uribe Consultant LCSHD
Christina Novinskey Consultant LCSHD
Dorothy Kronick Consultant LCSHD
Abelardo Octavio Cerecedo Consultant LCSHD

18
(c) Staff Time and Cost (from SAP) [all fields are pre-populated by the system]
Stage of Project Cycle
Staff Time and Cost (Bank Budget Only)
No. of staff weeks US$ thousands
(incl. travel and consultants costs)
and consultants) Lending (by FY)
FY09 5.38 15,419.82
FY10 31.21 103,834.75
TOTAL 36.59 119,254.57
Supervision/NCO (by FY)
FY10 16.54 84,629.92
FY11 23.32 68,004.19
TOTAL 39.86 152,634.11
Supervision (from Task Team Members in all archived ISRs, if available)
Christoph Kurowski Senior Health Specialist LCSHD Task Team Leader
Claudia Macias Senior Operations Officer LCSHH NCO Task Team Leader
Snezana B. Mitrovic Lead Procurement Specialist LCSPT
Tomas Socias
Senior Procurement
Specialist
LCSPT
Jean-Jacques Verdeaux
Senior Procurement
Specialist
LCSPT
Gabriel Penaloza Procurement Analyst LCSPT
Silvia Moran-Porche Procurement Assistant LCSPT
Dmitri Gourfinkel
Financial Management
Analyst
LCSFM
Manuela Villar Uribe Consultant LCSHD
Ietza Bojorquez Consultant LCSHD
Marcos Gonzalez-Marron Consultant LCSHD
Suzana Nagele de Campos
Abbott
Consultant ECSHD
Maria E. Castro-Munoz Consultant LCSSO

19
Annex 2. List of Supporting Documents
1. Project Concept Note, June 17,2009]
2. Emergency Project Paper, Report No. 49367-MX, November 4, 2009
3. Implementation Status Reports, Numbers 1-3
4. OPCS Case Recommendation and Review Report

20
MAP IBRD 33447R