world bank document research working paper 5846 tall claims mortality selection and the height of...
TRANSCRIPT
Policy Research Working Paper 5846
Tall Claims
Mortality Selection and the Height of Children
Harold AldermanMichael LokshinSergiy Radyakin
The World BankDevelopment Research GroupHuman Development and Public Services TeamOctober 2011
WPS5846P
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
edP
ublic
Dis
clos
ure
Aut
horiz
ed

Produced by the Research Support Team
Abstract
The Policy Research Working Paper Series disseminates the findings of work in progress to encourage the exchange of ideas about development issues. An objective of the series is to get the findings out quickly, even if the presentations are less than fully polished. The papers carry the names of the authors and should be cited accordingly. The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors. They do not necessarily represent the views of the International Bank for Reconstruction and Development/World Bank and its affiliated organizations, or those of the Executive Directors of the World Bank or the governments they represent.
Policy Research Working Paper 5846
Data from three rounds of nationally representative health surveys in India are used to assess the impact of selective mortality on children’s anthropometrics. The nutritional status of the child population was simulated under the counterfactual scenario that all children who died in the first three years of life were alive at the time of measurement. The simulations demonstrate that the difference in anthropometrics due to selective mortality would be large only if there were very large
This paper is a product of the Human Development and Public Services Team, Development Research Group. It is part of a larger effort by the World Bank to provide open access to its research and make a contribution to development policy discussions around the world. Policy Research Working Papers are also posted on the Web at http://econ.worldbank.org. The author may be contacted at [email protected].
differences in anthropometrics between the children who died and those who survived. Differences of this size are not substantiated by the research on the degree of association between mortality and malnutrition. The study shows that although mortality risk is higher among malnourished children, selective mortality has only a minor impact on the measured nutritional status of children or on that status distinguished by gender.

TALL CLAIMS:
MORTALITY SELECTION AND THE HEIGHT OF CHILDREN
Harold Alderman, Michael Lokshin and Sergiy Radyakin*
Keywords: Mortality, nutrition, children, India
JEL: J12, I32, O12
* Harold Alderman, World Bank, 1818 H Street, NW, Washington DC, 20433, MSN MC3-306;
[email protected]. Michael Lokshin, World Bank, 1818 H Street, NW, Washington DC, 20433,
MSN MC3-306; Sergiy Radyakin, World Bank, 1818 H Street, NW, Washington DC, 20433, MSN MC3-
306. The authors are grateful to Jishnu Das, Monica Das Gupta, and Adam Wagstaff for comments on an
earlier draft. The findings, interpretations and conclusions of this paper are those of the authors and should
not be attributed to the World Bank, its Executive Directors, or the countries they represent.

2
I. Introduction
Anthropometric status is often used as an indicator of welfare (Steckel 1995, 2009).
Many people also consider adequate nutrition to be of intrinsic value—a good in its own
right. Others have emphasized its instrumental role in productivity and economic growth
(Fogel 2004; Alderman, Behrman, and Hoddinott 2005). But regardless of whether
nutritional status is used to explain welfare or to understand growth, it may be important
to determine whether trends or differences in anthropometric measures of nutritional
status in population groups1 are a reflection of trends and differences in another key
indicator of welfare, mortality.
For example, Deaton (2007) explores the relationship of income and adult height
and speculates on explanations for a positive relationship between mortality and height in
Africa. This relationship, which contrasts with that found for all other countries pooled in
a separate regression, is observed even after accounting for country specific effects. One
possible reason for this association is that in Africa mortality selection dominates the
what Deaton refers to as ―scarring― – a reduction in adult height because of disease and
malnutrition in childhood, Mortality selection is, of course, an extreme form of sample
attrition, widely recognized as a potential source of bias in economic analysis (Fitzgerald,
Gottschalk, and Moffitt 1998). The well documented association of malnutrition and
mortality (see, for example, Victora and others 2008) may truncate the lower tail of the
height distribution, and this may be sufficient to offset the negative association of child
mortality with the causes of malnutrition.
While Deaton‘s study is an attempt to explain the pattern of heights in Africa, the
concern that selection may mask patterns of health is more general. For example, in a
review dominated by evidence from developed countries Almond and Currie (2009),
write: ―Finally, Bozzoli, Deaton, and Quintana-Domeque [2009] highlight that in
developing countries, high average mortality rates cause the selection effect of early
childhood mortality to overwhelm the ‘scarring’ effect. Thus, the positive relationship
between early childhood health and subsequent human capital may be absent in analyses
that do not account for selective attrition in high mortality settings―. Almond and Currie,
however, do not offer functional definition for ‗high‘. Results of studies on nutrition may
be called into question when mortality is high. For example, Maccini and Yang (2009)
worry about the possible bias in their estimates of heights that might come from selective
mortality (though they offer a simple argument that this is not a concern for Indonesia).
Our paper is partially motivated by the view that the legitimate concern for extreme
mortality environments might be taken out of their range of validity.
1 While anthropometry does not cover all aspects of nutrition – many micronutrient deficiencies do not
manifest in changes in weight or height – it is a commonly tracked measure. Unless otherwise stated, this
paper implies anthropometric measures of nutritional status when discussing nutrition and malnutrition.

3
Steckel (2009) suggests that this impact of mortality on the height of survivors
can be tested through simulations. The current paper is in keeping with this strategy.
Although it does not simulate the effect of sample truncation on nutritional status across
countries, it does employ simulations at the individual level that can indicate whether
selective mortality might mask improvements in nutritional status over time in a country
where mortality rates have been declining rapidly or whether truncation might bias
comparisons across genders. Three rounds of nationally representative health survey data
from India are used to simulate the nutritional status of the child population under the
polar counterfactual that all children who died in the first three years of life are alive at
the time of measurement.
The objective of this study is similar to that of studies by Boerma et al (1992), Pitt
(1997) and Dancer, Rammohan, and Smith (2008), although the approach differs.
Boerma et al. use data from longitudinal studies and retrospective data from cross-
sectional studies in 17 countries to analyze the effect of selective survival on children‘s
anthropometric measures. Their study concludes that selective survival has only a
marginal effect on the comparisons of anthropometric outcomes across geographic areas,
subpopulation and time. Pitt recognizes that children who fail to survive through
childhood are not a random draw from a population and furthermore that fertility itself is
a choice. He addresses this by simultaneously estimating the probability of these two
events along with nutritional status and finds that although fertility and mortality are
statistically significant determinates of nutrition there is no behaviorally significant bias
in the parameters if this selection is ignored. Dancer, Rammohan, and Smith use a
selection correction to estimate models of nutritional status and find that survival is
positively associated with nutritional status. That is, they find that scarring, to use
Deaton‘s terminology, is more prevalent in the sample than is selection.
Similarly, a paper by Gorgens et al. (2007) finds evidence that extremely high
mortality rates during the 1959-196 famine in China impacts trends in adult height in
rural areas, but the affect of the estimated selection is relatively small. At the same time,
no significant mortality bias was found for urban population in China. Bozzoli, Deaton
and Quintana-Domeque (2009) also demonstrate that the selection could have a
significant positive impact on adult height at very high mortality rates2. A recent paper
by Moradi (2010) estimates the size of the selection affect of survival in Gambia and
finds it to be too small to account for the tall adult heights observed in Sub-Saharan
Africa.
2 The paper presents several specifications of the regression of adult height on pre-adult mortality rates and
mortality rates squared. The coefficients on the linear mortality rates are negative and those on quadratic
mortality rates are positive and significant. The estimated inflection rate after which higher pre-adult
mortality rates have a positive effect on adult height varies by specification, but for all specifications this
rate is outside of the data range (i.e. at or above pre-adult 250 deaths per 1000).

4
The current study confirms that even when mortality risk is higher among
malnourished children, this has only a minor impact on the measured nutritional status of
the child population or on that status by gender with evidence from a country with high
rates of malnutrition and moderately high mortality. We show this, first, by illustrating
the degree to which the nutrition results reported in various surveys form India would
have changed had mortality rates differed. While our initial simulations impute results
using global evidence on the relationship of nutrition and risk of mortality we also bolster
these simulations with additional simulations based on the estimated hazard of mortality
from survey data.
The paper is organized as follows: The next section describes the data and
presents some descriptive statistics. Section II outlines the theoretical framework and the
empirical strategy. Section III discusses the main results, and section IV presents some
implications of the findings.
II. Data and Descriptive Statistics
This analysis uses data from three waves of India‘s National Family Health Survey
(NFHS; 1992/93, 1998/99 and 2005/06), a survey of representative households in states
and territories covering some 99 percent of the population3 and similar in structure to
demographic and health surveys conducted in several other countries. The NFHS follows
the pattern of a standard Demographic and Health Survey. The main sample of NFHS
contains information on 45,279 children in 33,032 households from the 1992/93 round,
30,984 children in 26,056 household from the 1998/99 round, and 48,679 children in
33,968 households from the 2005/06 round.4
Because the NFHS does not collect information on household income or
consumption, a household wealth index was constructed from the data on household
assets using the method based on principal components (see, for example, Filmer and
Pritchett 2001; Rutstein and Johnson 2004).
The NFHS provides height and weight data for children under age 48 months in
1992/93, under age 36 months in 1998/99, and under age 60 months in 2005/06. The
NFHS contains no anthropometric information for deceased children at the time of their
death. For comparability between NFHS rounds, the sample was restricted to children
under age 36 months. The analysis focuses on the age-adjusted measure of height-for-
3
Kashmir, Sikkim, and some remote territories were not covered in NFHS-1. Detailed information on
NFHS methodology and sample design is available at www.nfhsindia.org/. The data are available from
MEASURE DHS, Macro International Inc. at www.measuredhs.com. 4 The number of observations in the 1998/99 round is smaller, as it collected height and weight information
only for the last two children under age 3 of ever-married women who were interviewed. In the 1992/93
round, measurements of height were not collected in Andhra Pradesh, Himachal Pradesh, Madhya Pradesh,
Tamil Nadu, and West Bengal.

5
age, which reflects children‘s development relative to a reference population of well-
nourished children (WHO 2006).5
Because children‘s weight at birth influences their health and prospects for
survival (Rosenzweig and Shultz 1982), a key variable for this study is the data on
children‘s weight at birth in the survey. The NFHS collects information on weight at birth
in addition to weight at the time of the survey and asks mothers to categorize the weight
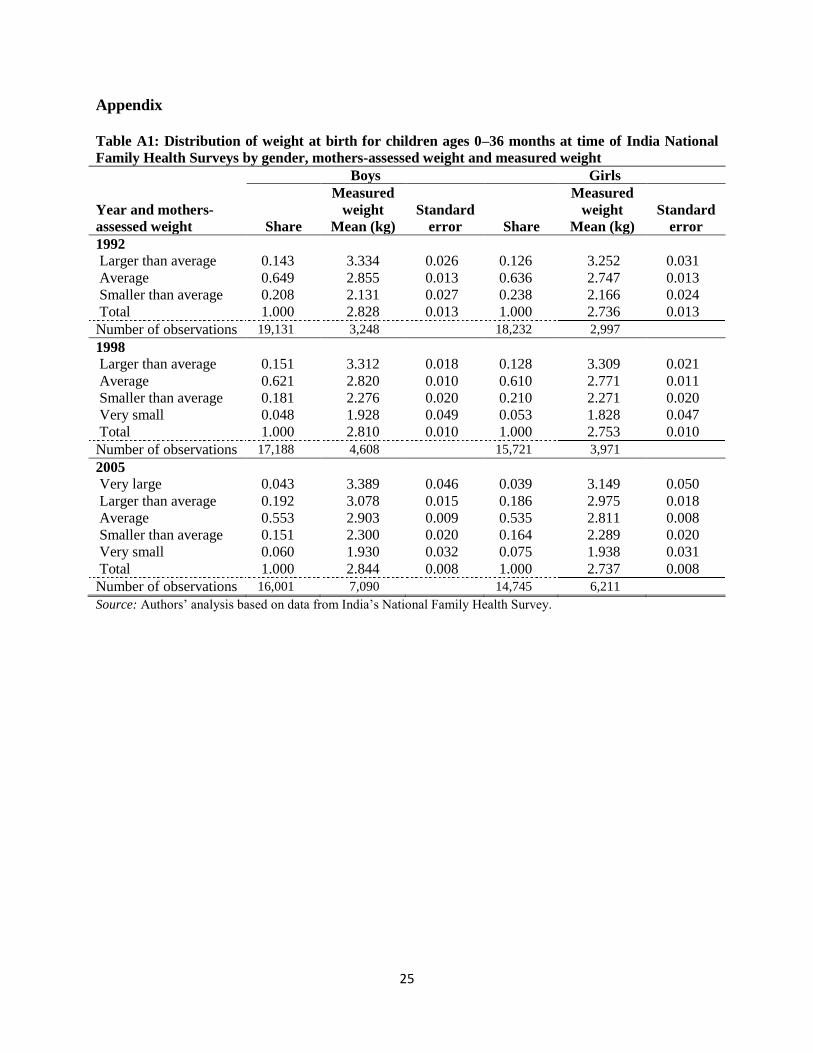
of their children at birth as large, average, or small.6 The sample of children with weight
measured at birth is much smaller than the sample of children whose weight was assessed
by their mother (table A1 in the appendix). The study relies mainly on these subjective
assessments as a proxy for health endowments at birth. The weight of about 20–25
percent of children was lower than average according to their mothers‘ assessments (see
table A1), a figure not out of keeping with the rate of low birth weight children in India.
The data show that average height-for-age has risen over time for both boys and
girls, with z-scores rising from –1.91 in 1992 to –1.55 in 2005 for boys and from –1.86 to
–1.53 for girls. Correspondingly, stunting declined from 72 percent of boys and 70
percent of girls in 1995 to 65 percent for both sexes by 2005. Despite these
improvements, malnutrition remains prevalent in India.
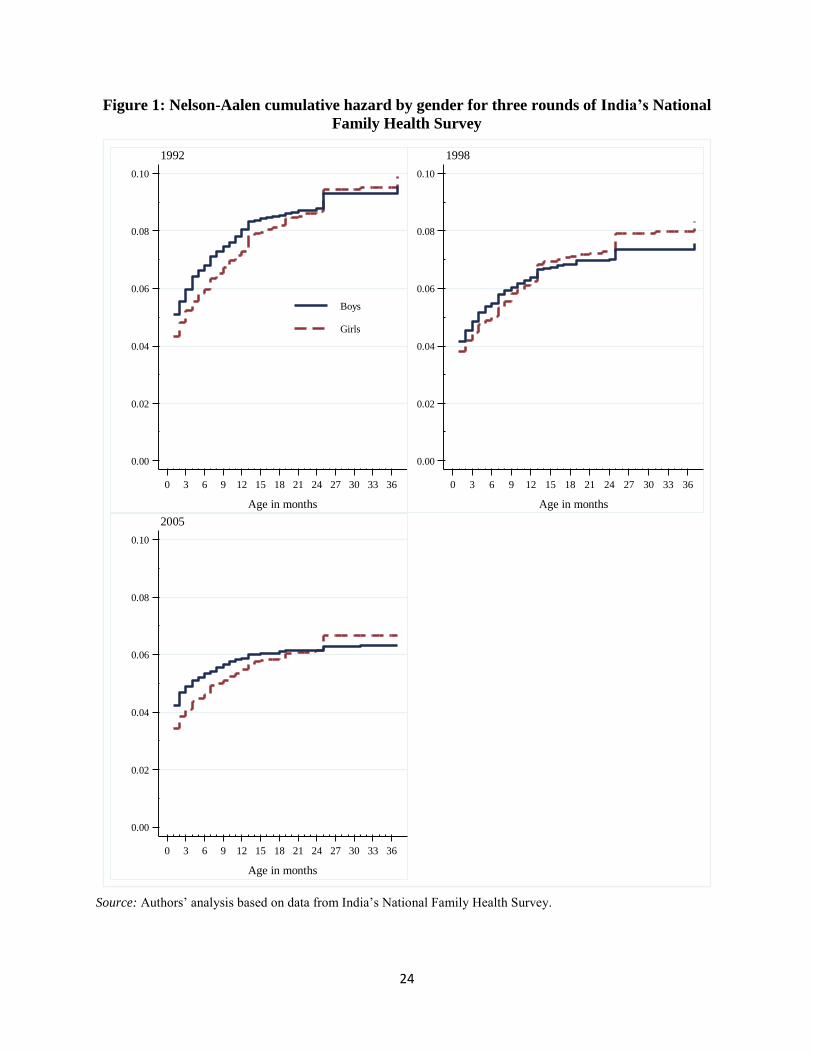
Deaths around the time of birth (neonatal) are high in all rounds of the NFHS
(table 1). Boys accounted for about 56 percent of all deaths in the immediate postnatal
period. However, beyond age 6 months, the share of deaths is higher for girls than for
boys. A plot of the cumulative mortality hazard by gender for the three rounds of the
NFHS again shows that more than half the deaths in children under age 36 months occur
in the first month after birth, with little change over the years. It also shows a higher
mortality risk for boys than for girls in the early months of life (figure 1), followed by a
reversal in later months. This switch in mortality patterns results in almost identical total
mortality rates for boys and girls ages 0–36 months.
5 A report by Nutrition Foundation of India concluded that the World Health Organization (WHO) standard
was generally applicable to Indian children (IIPS 2000). The nutritional status of children calculated in this
way is compared with the nutritional status of an international reference population recommended by the
WHO (Dibley and others 1987). The use of this reference group is based on the empirical finding that well-
nourished children in all population groups for which data exist follow similar growth patterns (Martorell
and Habicht 1986). Across rounds of the NFHS, about 10 percent of eligible children were not measured,
either because the children were not at home or because their mothers refused to allow the measurements
(Lokshin, Das Gupta, and Ivaschenko 2005). 6 There is a good correspondence between the measured weight and the weight at birth assessed by the
mothers. For example, in 1992, only about 3 percent of children who were assessed as large at birth had
measured weight in the lowest quintile of the weight distribution. Seidman and others (1987) show that
about 75 percent of self-reported birth weights were accurate within 100 grams. A study by Adegboyea and
Heitmannb (2008) that uses a weight categorization similar to NFHS concludes that maternal assessment of
a child‘s weight at birth ―seems to be sufficiently accurate for clinical and epidemiological use.‖

6
III. Quantifying the Impact of Selective Mortality on Nutritional Indicators
The magnitude of the influence of selective mortality on nutritional status of a population
depends on child mortality level, prevalence of malnutrition among living children, and
prevalence of malnutrition among deceased children (Boerma et al. 1992). Our
population – all children – consists of living and deceased children. Taking a height-for-
age z-score as a measure of malnutrition, the average height-for-age z-score for all
children Zall can be expressed as:
(1) (1 )all s d d dZ Z P Z P ,
where Zs and Zd are average z-scores for survivors and deceased children,
correspondingly, and Pd is the proportion of dead children. The change in the z-score had
deceased children survived is then:
(2)
Assuming that at least some deaths are related to malnutrition (Zd < Zs) the inclusion of
dead children in the sample results in lower average z-scores (Zall < Zs). Δ is larger the
higher is child mortality and the larger is the difference in the average z-scores of living
and deceased children.
The analysis starts with simple simulations illustrating empirically the magnitude
of the potential influence of selective mortality and then moves on to simulations based
on a proportional hazard model.
Simulations Illustrating the Magnitude of Potential Impact of Selective Mortality
What would be the observed height-for-age for all Indian children ages 0–36 months had
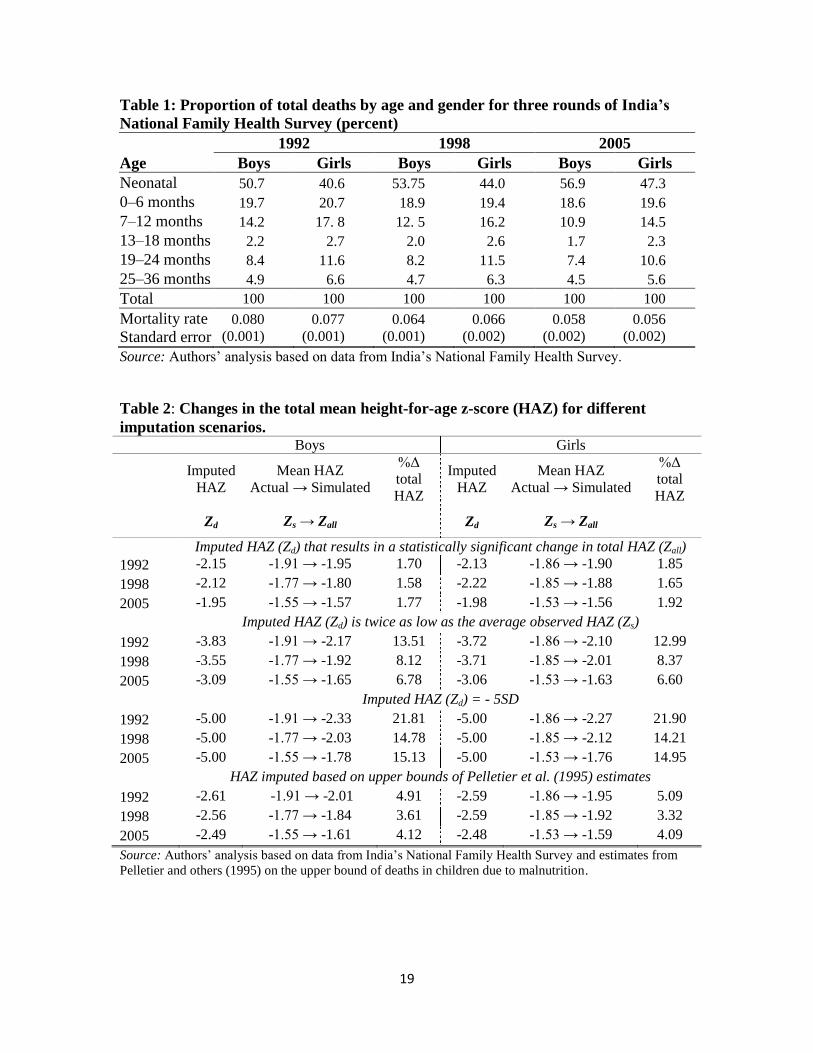
the children who died before age 36 months survived? Table 2 presents the simulated
changes in the average height-for-age z-score for different imputation scenarios for three
rounds of NFHS.
The first set of results demonstrates how large the difference in z-scores between
children who died before age 36 months (Zd) and those who survived (Zs) should for Δ in
(2) to be statistically significant. In 1992, 7.7 percent of boys and 8.0 percent of girls died
before age 36 months. The average height-for-age z-score of surviving children (Zs) was
–1.91 with a standard error of 0.016 for boys and –1.86 with a standard error of 0.017 for
girls. The first row of table 2 shows, that imputing a z-score of -2.5 for dead boys results
in the statistically significant changes in overall z-score (Zall) from the actual -1.91 to -
1.95. For girls, the impact of selective mortality would be statistically significant had the
currently deceased girls survived and their average z-score were -2.3.

7
If the average height-for-age of children who died was twice as far below the age
and gender reference mean as that of children who survived (–3.83 rather than –1.91), the
height-for-age z-score for the total sample would rise from –1.91(Zs) to –2.17(Zall), or by
13.5 percent. If a height-for-age z-score of –5.0 (the lower bound recommended as the
cut-off for outliers; WHO 1995) is imputed to a sample of children who died, the overall
z-score would rise from –1.91 to –2.32, or by 21.8 percent. Similar tendencies are
observed for the 1998 and 2005 samples.
The impact of the imputations for height-for-age on the total sample is
proportional to the mortality rates. For example, the imputation of a height-for-age z-
score twice as low as the average to the sample of girls who died before age 36 months
results in a 13.0 percent change in the overall mean z-score in 1992 but only a 8.4 percent
change in 1998 and a 6.6 percent change in 2005, reflecting the decline in girls‘ mortality
rates from 0.077 in 1992 to 0.056 in 2005.
But not all deaths before age 36 months were caused by malnutrition. The next
simulation is based on the results from the literature that estimates the contribution of
malnutrition to child mortality. Puffer and Serrano (1973) found that malnutrition was an
underlying cause in 54 percent of deaths for children ages 2–4 years. Pelletier (1994)
explored 28 prospective datasets and found that the population-attributable risk of
mortality associated with anthropometric deficits varied from 17 percent to 74 percent in
eight studies for Asia and Africa. Pelletier and others (1994) applied to prospective
surveys in Ethiopia, Guatemala, India, and Malawi a new methodology for determining
the association of malnutrition and mortality by the severity of malnutrition. They
demonstrated that 42–57 percent of deaths of children ages 6–59 months were associated
with malnutrition‘s potentiating effects on infectious disease, 76–89 percent of them
attributable to mild to moderate malnutrition. Analysis of data for 53 developing
countries for the 1980s found that about 56 percent of child deaths were associated with
malnutrition. The proportion is close to 67 percent for India, with 73–74 percent of it
attributable to mild to moderate malnutrition (Pelletier and others 1995).
While this approach is based on weight for age and not height-for-age, it makes a
good starting point for a simulation of imputed height-for-age, based on the assumption
that 67 percent of deaths in children up to age 36 months in India were related to
malnutrition (the upper bound for that association; see bottom panel of table 2). The
height-for-age of living children by gender in a particular year was used to impute the
average height-for-age of children whose deaths were not associated with malnutrition.
Of deaths among children related to malnutrition, 70 percent were assumed to have
occurred among children with moderate to mild malnutrition, and an average height to

8
age z-score of –2.5 was imputed to them. For the rest of the sample of children who had
died, an average height to age z-score of –4 was imputed7.
Even though these imputations are based on the upper bound estimates of Pelletier
and others (1995), they result in only modest changes in the overall mean. The largest
changes are observed for the 1992 sample because mortality rates are highest in that year
(see bottom panel of table 2). Had all the children who died survived, the total mean
height-for-age z-score for boys would change from –1.91 to –2.01, a 4.9 percent change.
The impact of imputations is smaller for 1998, at 3.6 percent and 2005, at 4.1 percent.
For girls, the imputations change the total mean from –1.86 to –1.95 in 1992, a 5.1
percent change, and by 3.3 percent for 1998 and 4.09 percent for 2005. The change in
height-for-age z-score is slightly larger in percentage terms in 2005 than in 1998
(although the absolute value of the change is smaller) in keeping with the lower mortality
rate.
Recent studies by Pelletier and Frongillo (2003) and Black and other (2008)
indicate that globally among children younger than 36 months the proportion of deaths
associated with malnutrition declined to 37 percent in the late 1990s and early 2000s
because of the effect of expanded coverage of immunizations, oral rehydration therapy,
antibiotics, and other child survival interventions. Imputations of height-for-age z-scores
corrected for contemporaneous mortality selection based on these estimates would yield
smaller and statistically insignificant changes in the total mean for the 1998 and 2005
NFHS samples. While these more modest associations are not illustrated in table 2, the
simulations that are shown demonstrate that the selectivity mortality would only have a
large impact on observed anthropometrics if there were very large differences in
anthropometrics between the children who died and those who survived. Current research
on the association between mortality and malnutrition does not substantiate such large
differences.
Simulations Based on a Proportional Hazard Model
The simulations discussed in the previous section were based on imputations of a few
categories of height-for-age data to the children in the sample who had died. It is more
realistic to assume that children‘s anthropometrics and survival depend on their
individual characteristics, prenatal conditions, health of the mother, and those of their
household (Wolpin 1997). To approximate this, children who died were matched with
children who survived past the age of 36 months using the estimated survival hazard as a
matching score. The anthropometric scores of children who survived were then imputed
7 Boerma et al (1992) demonstrate that the differences in malnutrition between the children who died after
the measurement and who survived a specified time period in longitudinal studies in Indian states of Tamil
Nadu and Punjab were relatively small: height-for-age z-scores of 60 percent of dead children were lower
than -2 SD from the mean compared to 50 percent among survivors.

9
to the children who had died, and the impact of these imputations on the average height-
for-age z-score of the total sample was estimated.
The estimation uses a standard theoretical framework of household utility
maximization that incorporates the production function of a child‘s health (Behrman and
Deolalikar 1988). Household utility is a function of the consumption and leisure of
household members and the quality (health) and quantity of their children. A household
maximizes its utility subject to budget constraints and the restrictions imposed by the
health production function. The household demand for child health at time t depends on a
set of exogenous characteristics of the child and its mother, household, and community,
as well as some unobserved factors captured by the random error term it (Thomas,
Strauss, and Henriques 1991). This relation can be expressed, in linear form, as:
(3) it it itH X
where vectoriX combines the child‘s, mother‘s, household‘s, and community‘s
characteristics, and β is a vector of parameters.
The child‘s health can be linked to mortality through the stochastic rule for
observing death (Sickles and Taubman 1997). The mortality state for child i at time t is
defined as:
(4)
*1
0
it it itM if H H
otherwise
where *
itH is a child- and time-specific mortality threshold that can be interpreted as a
shock whose arrival time follows a Poisson distribution. The probability that a shock *
itH
occurs during the period ( , )t t is 0( ) ( )P h t o . Then the hazard of dying during
this period is:
(5) 0( ) ( )[1 ( )]i ith t h t F H
where h0(t) is the baseline hazard and F(Hit) is the health distribution function. The
survival function is then:
(6) 0( | ) exp{ ( )[1 ( )] }.i i itS t x h t F H t
Assumptions about the distribution of the health shocks that are standard in the
literature on mortality can be used to estimate the survival function using the Weibull
proportion hazard model, such that:
(7)
1 1
1
( ) exp{ } exp{ }
( | ) exp{ exp( ) }
i it i
i i
h t t H t x
and
S t x t x t
10
where θ is an unknown parameter.
To control for the unobserved heterogeneity in children‘s health (frailty), a
parameter is introduced that represents the effect of unobserved factors on survival. This
effect is not directly estimated from data but is assumed to have unit mean and variance
αi that is estimated (see Vaupel, Manton, and Stallard 1979; Lancaster 1979; Hougaard
1995). In the presence of such unobserved heterogeneity, survival function (7) becomes:
(8) ( | , ) { ( | )} i
i i iS t x S t x .
The unconditional survival function is obtained by integrating out the
unobservable factor by assuming a distribution for α. If the unobserved factor is inverse-
Gaussian-distributed,8 the survival function of the Weibull proportional hazard model (8)
becomes:
(9) 1/21 [1 2 ln( ( ))]
( | , ) exp{ }i
S tS t x
.
The parameters of equation (9) are estimated using the maximum likelihood algorithm.
Once these parameters are obtained, dead and surviving children can be matched on the
estimated hazard as a matching score, and this matching can be used to impute a height-
for-age z-score for children who died. The matching approach used here is analogous to
the approach used in propensity score matching (see Rubin 1973, 1979; Rosenbaum and
Rubin 1983), but the hazard function is a different functional form than commonly used
for propensity score matching. It was chosen for its ability to account for censoring and
truncation, making it the preferred model for estimating survival.9 The overall conclusion
is robust to an estimation of survival based on a probit regression (results not reported in
tables), the functional form more commonly employed in propensity score matching.
IV. Results
The explanatory variables used in proportional hazard estimation (equation 7) include the
child‘s sex, birth order, and weight at birth; the mother‘s age, educational attainment,
employment status, and other characteristics; household size, socio-demographic
8 For the inverse-Gaussian frailty distribution, the relative variability of frailties among surviving children
decreases with age, which could be a more realistic assumption for modeling child mortality; Gamma
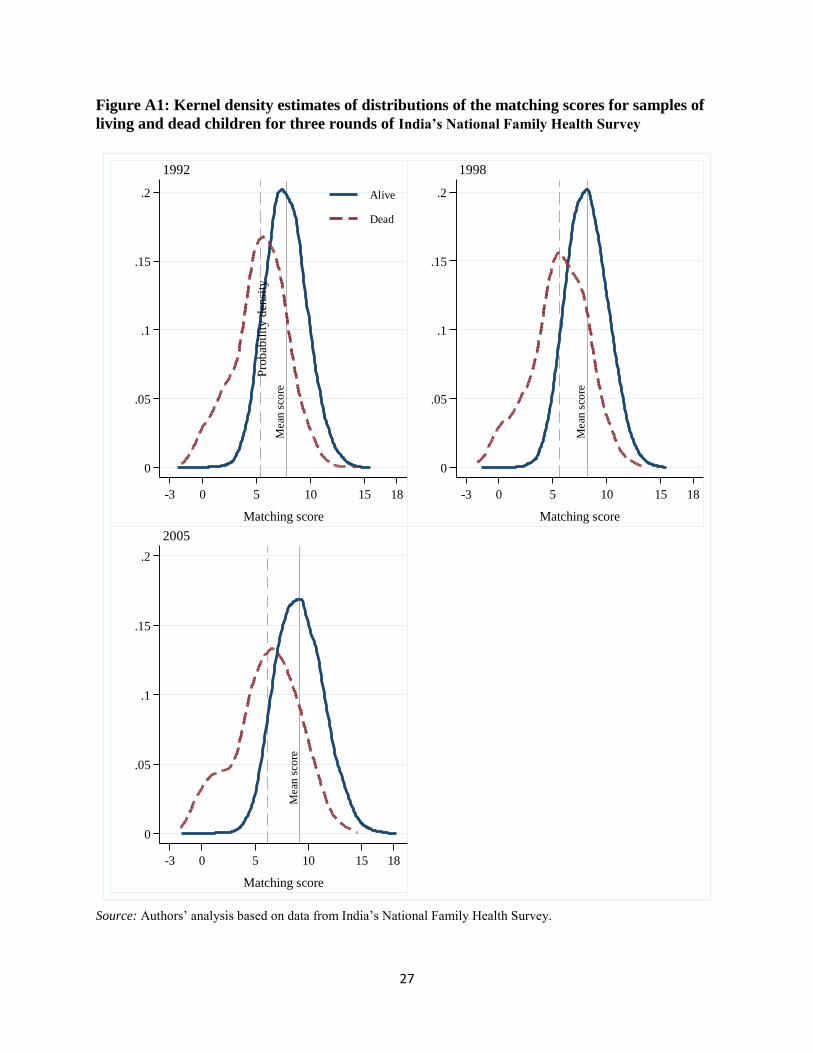
frailty distribution assumes constant variability of frailty with age (Gutierrez 2002). 9 Samples of dead and surviving children were matched using a nearest neighbor algorithm with the
restriction that observations in both samples are on a common support in terms of the matching score
(Heckman, LaLonde, and Smith 1999). The probability density functions of matching scores for dead and
surviving children are shown in figure A1 in the appendix. An alternative, and probably more intuitive, way
to run these simulations would be to model children‘s height for age z-scores as a function of their
characteristics and to impute height for age z-scores to the dead children using out-of-sample prediction.
The approach here is similar to that because the out-of-sample prediction could be interpreted as a case of
matching. The advantages of the current approach are the use of a more flexible function form for the
matching and the ability of the hazard model to deal better with attrition issues.

11
composition, wealth index, religion, and caste; and the availability of community services
and infrastructure. The descriptive statistics for these variables are presented in table 3.
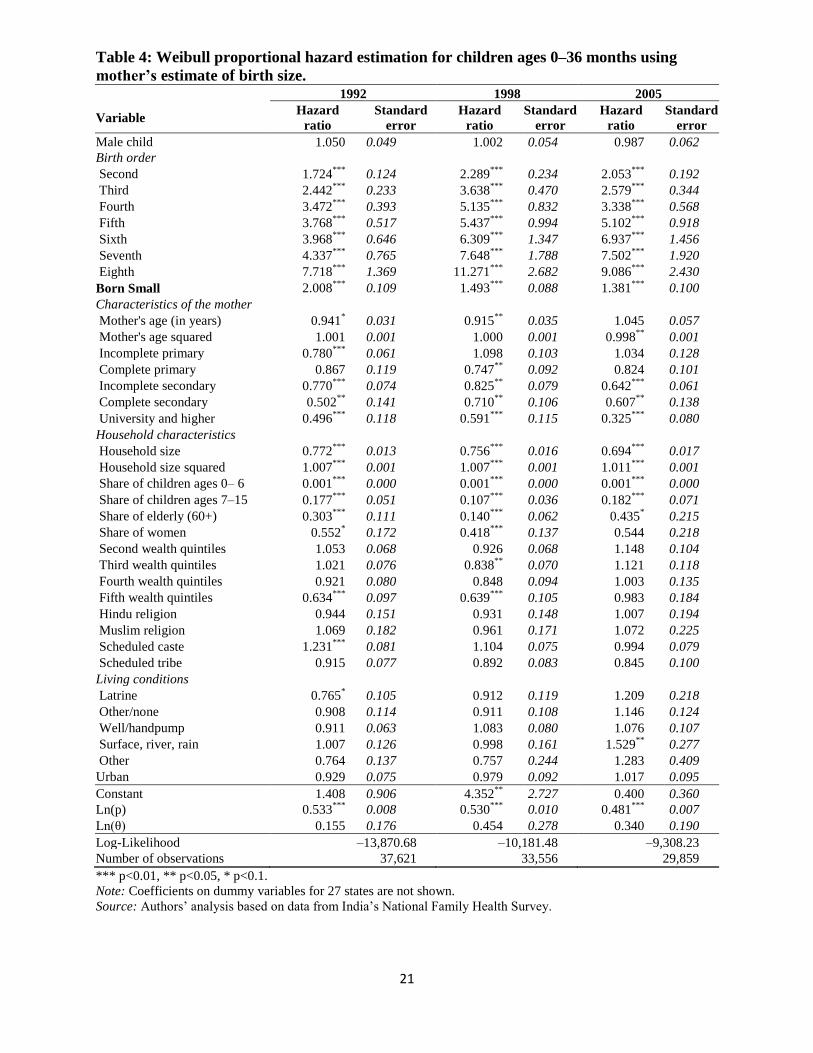
Tables 4 and 5 show the coefficients of the Weibull proportional hazard
estimation for children younger than age 36 months using three rounds of the NFHS.10
Table 4 includes the child‘s weight at birth estimated by the mother; Table 5 uses weight
measured at birth. The weight at birth is one of the important factors affecting neo-natal
child mortality that combines the unobserved information about pre-natal conditions and
shocks experienced by the mother and her child (i.e., Claeson, et al. 2000). The results of
the two estimations are not directly comparable as one is a categorical variable (mother‘s
assessment of weight at birth) and the other is a continuous variable (measured weight),
but the implications are similar11
. The remainder of the discussion focuses on the
estimations based on the specification using mother-assessed weight at birth because the
sample sizes are much larger.
The estimated hazard odds ratios on the control variables in the estimations of
proportional hazard models reveal the expected relationship between child mortality and
characteristics of the child, mother, and household. A child‘s gender has no effect on
mortality hazard: mortality rates for boys are higher than for girls in the six months after
birth and lower after that. A higher birth order has a negative impact on survival
probabilities (Miller et al. 1992). Weight at birth, whether assessed by the mother or
measured at birth, is a strong predictor of mortality. Children whose mother‘s assessed
their weight as small (with an odds ratio greater than 1 on the dummy variable reported in
table 4) and children with low measured weight (with odds ratios less than one on the
continuous measured weight variables in table 6) are significantly less likely to survive
than are children who weigh more at birth.
Children living in the wealthiest households and with better educated mothers
have better prospects for survival than do children from poor households and with less
educated mothers. In an inverted U-shaped relationship, children‘s survival improves
with the mother‘s age till about age 40 and declines thereafter.
10
The specification with Weibull distribution is selected based on the comparison of Akaike (1974)
information criterion values for specifications with exponential, Weibull, Gompertz, log-normal, log-
logistic, and general gamma distributions. 11
Note that the interpretation of the numbers presented in tables 5 and 6 are different from the standard
interpretation of the regression coefficients. The odds ratios are always positive; odds ratios that are less
than one indicate that an increase in a particular factor reduces the probability of an event, while odds ratios
greater than 1 mean that a particular factor increases the probability of an event. Correspondingly, the t-
tests of the odds ratio test the null hypothesis of odds ratios being equal to 1. For comparability, we re-
estimated the hazard model shown in Table 5 with the continuous variable on weight at birth categorized as
a binary indicator equal to 1 for children with weight at birth < 2,500 grams. The odds ratio for this dummy
is less than 1 and significant, but the effect of being born with low weight is smaller compared to
coefficient in Table 5. One explanation for this could be that children whose weight was measured at birth
come from the wealthier families with better access to post-natal health care.

12
Table 6 presents the simulated impact of the matched imputations of height-for-
age z-scores for all children ages 0–36 month who did not survive till the age of 36
months. The average z-score is higher for children with measured weight at birth than for
children with mother-assessed weights at birth reflecting wealth differences.
In 1992, the average height-for-age z-score for boys who survived past age 36
months was –1.913. When the matched z-score estimates are imputed to children who
died before age 36 months, the overall average height-for-age z-score becomes –1.936;
the difference of –0.023 is not statistically significantly different from 0. Similar
differences are observed for other years. In all years, for both boys and girls, the
imputations have no significant impact on the overall anthropometric indices. In all cases,
the average imputed height-for-age z-score in the simulations based on the survival
model is smaller than the imputed z-score that would result in a statistically significant
change in the overall height-for-age z-score as shown in first panel of table 212
. These
results resonate with other studies that use longitudinal data from surviving and non-
surviving children and find a modest amount of selection via child mortality on height-
for-age z-scores i.e., Boerma et al (1992), Moradi (2010)13
.
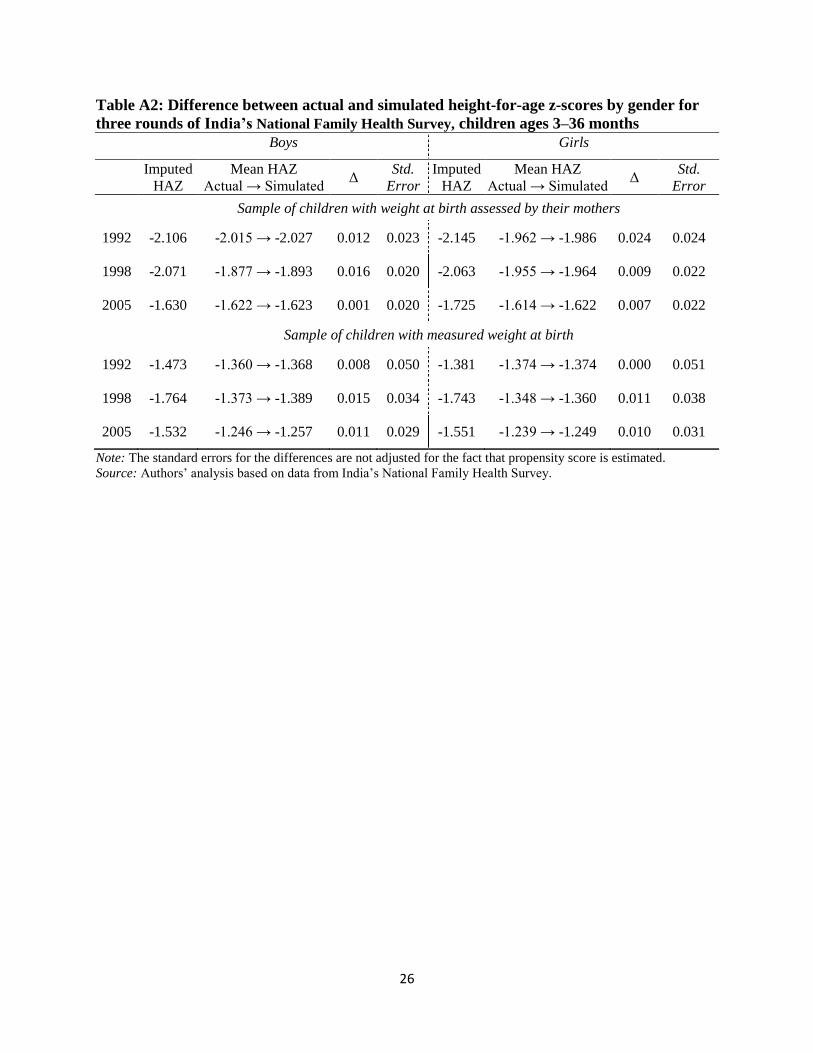
The effect of the change in mortality on gender patterns of height-for-age z-scores
was also simulated using the results of hazard function estimations. This simulation
closes the gender gap in mortality in the age 3–36 month group by artificially increasing
the mortality among boys14
. The simulation assumes that 144 of the boys in the sample
with the lowest probabilities of survival did not survive and thus did not contribute to the
observed height-for-age z-scores. The simulation of this increase in boys‘ mortality on
the data from 1992 of NFHS demonstrates a 0.12 percent increase in the height-for-age z-
score. This clearly has a negligible impact on the difference in nutritional status between
boys and girls.
Finally, taking our model a step further, we simulate the health outcomes of
Indian children if the mortality rates in India were as high as one of the highest rates
current in Africa. In this simulation we change the surviving status of living children with
lowest probabilities of survival to reach the mortality rate of 15 percent for both boys and
12
Table A2 in Appendix presents the simulated impact of the matched imputations of height-for-age z-
scores for children ages 3–36 months who did not survive till the age of 36 months. Neonatal mortality was
excluded in the hazard estimates as it could have a different set of correlates, but the results are not
particularly sensitive to the exclusion of this age group. 13
Our empirical model fails to account for the possible selection bias due to high levels of maternal
mortality in India (e.g., Ronsmans and Graham 2006). Correction of this bias would increase the gap in
anthropometric outcomes between the deceased and living children. Unfortunately, the nature of IFHS
sample makes it difficult to look on the relationship of maternal mortality and children health outcomes. 14
In principle, one could, simulate a more desirable decrease in girls‘ mortality to close this gap, but it is
more direct to use the estimates from boys actually in the sample then to make projections for girls who
would otherwise have been in the sample.

13
girls.15
The results of the simulation (table 7) show only minor changes in the aggregate
height-for-age z-scores when the mortality rates are increased from 5 – 8 percent (table 1)
to 15 percent. The changes are statistically significant for the samples of boys and girls in
1998 and for the sample of boys in 2005, but even in these cases the magnitudes of the
changes have not exceeded 3 percent.
V. Conclusion
This paper used data from three rounds of a nationally representative health survey in
India to assess the magnitude of the bias in children‘s anthropometrics due to selective
mortality. The nutritional status of the child population was simulated under the
counterfactual scenario that all children who had died in the first three years of life were
alive at the time of measurement. These simulations imputed various values of height-
for-age z-scores to the sample of dead children. The simple simulations, with imputed z-
scores that are independent of the child‘s characteristics, show that, at the rates of child
mortality prevailing in India in 1992–2005, the selective mortality could have only a
moderate impact on overall anthropometric measures. The imputations based on the
literature on the association between child mortality and nutrition result in only a 5
percent difference between the counterfactual and the actual height-for-age z-scores.
The simulations based on the hazard model that takes into account differences in
mortality and anthropometrics related to child characteristics are consistent with the
observation that malnourished children are less likely to survive and thus to contribute to
anthropomorphic measurements. However, the results also show that with the current low
(and declining) mortality rates by historical standards, improved survival rates have an
insignificant impact on overall height-for-age z-scores. The changes in mortality between
1992 and 2005 imply that some malnourished children who would previously have died
instead survived and are measured in the 2005 survey. To the degree that selective
mortality affects overall malnutrition levels or rates, the reductions in child mortality
mask some of the improvement in nutrition. However, the results of this study suggest
that progress on the fourth Millennium Development Goal to reduce child mortality only
lightly obscures the results for the target for the first Millennium Development Goal to
reduce malnutrition and hunger.16
Similarly, the findings imply that differences in mortality are unlikely to explain
gender differences in anthropometrics—or their absence. While the NFHS data do not
15
This rate corresponds to the high mortality rate of 14.2 percent observed among boys in Cote d‘Ivoire in
1998. The rate for Cote D‘Ivoire was the highest mortality rate from 30 DHS of African countries
reviewed. 16 This target is measured in terms of underweight rather than height for age. Underweight is somewhat
easier to measure in a survey covering young children, though height for age is a clearer indicator of
cumulative health. While underweight rates and stunting rates often differ, trends in the two tend to move
together.

14
show a marked gender pattern in overall mortality of children 0–36 months, deaths are
higher for girls after the neonatal period. Nevertheless, the imputations here have no
significant impact on relative nutritional status. While the results reported here are from
India over a two decade period, in a more general sense, it appears that selective
mortality is unlikely to be of significant magnitude in most countries to have a large
impact on trends in populations or subpopulations.
15
References
Adegboye, A., and B. Heitmannb. 2008 ―Accuracy and correlates of maternal recall of
birth weight and gestational age.‖ International Journal of Obstetrics and
Gynaecology 115 (7): 866–93
Alderman, H., Behrman, J. and J. Hoddinott. 2005. ―Nutrition, malnutrition, and
economic growth.‖ In Health and economic growth: findings and policy
implications, ed. Guillem López-Casasnovas, Berta Rivera, and Luis Currais.
Cambridge, Mass: MIT Press.
Almond, D. and J. Currie (2010) ―Human Capital Development before Age Five,‖ NBER
Working Paper Series, Working Paper #15827
Behrman, J., and A. Deolalikar (1988) ―Health and nutrition.‖ In Handbook of
development economics, Vol. 1, ed. H. Chenery and T. Srinivasan. Amsterdam:
North Holland.
Black, R., L. Allen, Z. Bhutta, L. Caulfi, M. Onis, M. Ezzati, C. Mathers, and J. Rivera.
2008. ―Maternal and child undernutrition: global and regional exposures and
health consequences.‖ Lancet 371: 243–60.
Boerma, J., Sommerfelt, E., and G. Bicego. 1992. ―Child Anthropometry in Cross-
Sectional Surveys in Developing Countries: an Assessment of the Survivor Bias,‖
American Journal of Epidemiology, Vol. 135(4): 438–49
Bozzoli, C., Deaton, A., and C. Quintanta-Domeque. 2007. ―Adult Height and Childhood
Mortality.‖ Demography, Vol. 46(4): 647–69
Claeson, M., Bos, E., Mawji, T. and I. Pathmanathan (2000) ―Reducing child mortality in
India in the new millennium.‖ Bulletin of the World Health Organization, Vol.
78: 1192-1199
Dancer, D., Rammohan, A., and M. Smith. 2008. ―Infant mortality and child nutrition in
Bangladesh.‖ Health Economics 17: 1015–35.
Deaton, A. 2007. ―Height, health and development.‖ Proceeding of the National
Academy of Science 104 (33): 13232–37.
Dibley, M., J. Goldsby, N. Staehling, and F. Trowbridge. 1987. ―Development of
normalized curves for the international growth reference: historical and technical
considerations.‖ American Journal of Clinical Nutrition 46: 736–48.
Filmer, D. and L. Pritchett. 2001. ―Estimating wealth effects without expenditure data—
or tears: an application to educational enrollments in states of India.‖
Demography 38 (1): 115–32.
Fitzgerald, J., P. Gottschalk, and R. Moffitt. 1998. ―An analysis of sample attrition in
panel data.‖ Journal of Human Resources 33: 251–99.
Fogel, Robert W. 2004. ―Health, nutrition, and economic growth.‖ Economic
Development & Cultural Change 52 (3): 643–58.
16
Gørgens, T., Meng, X. and R. Vaithianathan. 2007. ―Stunting and Selection Effects of
Famine: A Case Study of the Great Chinese Famine.‖ IZA Discussion Paper No.
2543. Institute for the Study of Labor, Bonn, Germany.
Gutierrez, R. 2002. ―Parametric frailty and shared frailty survival models.‖ Stata Journal
2 (1): 22–44.
Heckman, J., R. LaLonde, and J. Smith. 1999. ―The economics and econometrics of
active labor market programs.‖ In Handbook of labor economics, Vol.III, ed. O.
Ashenfelter and D. Card. Amsterdam: Elsevier.
Hougaard, P. 1995. ―Frailty models for survival data.‖ Lifetime Data Analysis 1: 255–73
Lancaster, T. 1979. ―Econometric methods for the duration of unemployment.‖
Econometrica, 47: 939–56
Lokshin, M., Das Gupta, M., and O. Ivaschenko. 2005. ―An assessment of India's
Integrated Child Development Services Nutrition Program.‖ Development and
Change 36 (4): 613–40.
Maccini, Sharon and Dean Yang (2009). Under the Weather: Health, Schooling, and
Economic Consequences of Early-Life Rainfall. American Economic Review. June
99 (3), 1006-26.
Martorell, R. and J. Habicht. 1986. ―Growth in early childhood in developing countries.‖
In Falkner, F. and J. Tanner (eds): Human Growth. Volume 3. Methodology.
Ecological, Genetic, and Nutritional Effects on Growth. Second Edition. New
York: Plenum, pp. 241-262.
Miller, J., Trussel, J., Pebley, A., and B. Vaughan. 1992. ―Birth spacing and child
mortality in Bangladesh and the Philippines.‖ Demography 29: 305–18.
Moradi, A. 2010. ―Selective mortality or growth after childhood? What really is Key to
understand the Puzzlingly Tall Adult Heights in Sub-Saharan Africa". CSAE
WPS 2010-17
Pelletier, D. 1994. ―Relationship between child anthropometry and the mortality in
developing countries: implications for policy programs and future research.‖
Journal of Nutrition, 124 (10): 2047S–81S.
Pelletier, D., and E. Frognillo. 2003. ―Change in child survival are strongly associated
with changes in malnutrition in developing countries.‖ Journal of Nutrition 133:
107–19.
Pelletier, D., A. Frongillo, D. Schroeder, and J. Habicht. 1994. ―A methodology for
estimating the contribution of malnutrition to child mortality in developing
countries.‖ Journal of Nutrition 124 (10): 2106S–22S
Pelletier, D., E. Frognillo, D. Schroeder, and J. Habicht. 1995. ―The effects of
malnutrition on child mortality in developing countries.‖ Bulletin of the World
Health Organization 73 (4): 443–46.
Pitt, Mark. 1997. ―Estimating the determinants of child health when fertility and
mortality are selective.‖ Journal of Human Resources 32 (1): 129–58.
17
Puffer, R., and C. Serrano. 1973. Patterns of mortality in childhood. Scientific
Publication 262. Washington, DC: Pan American Health Organization.
Ronsmans, C., and W. Graham. 2006. ―Maternal mortality: who, when, where,
and why.‖ Lancet, Vol. 368: 1189-200
Rosenzweig, M., and T. Schultz. 1982. ―The behavior of mothers as inputs to child
health: the determinants of birth weight, gestation, and rate of fetal growth.‖ In
Economic aspects of health ed. V. Fuchs. Chicago: University of Chicago Press,
Chicago.
Rosenbaum, P., and D. Rubin. 1983. ―The central role of the propensity score in
observational studies for causal effects.‖ Biometrika 70 (1): 41–55.
Rubin, D. 1973. ―Matching to remove bias in observational studies.‖ Biometrics 29: 159–
83.
________, 1979 ―Using multivariate matched sampling and regression adjustment to
control bias in observation studies.‖ Journal of the American Statistical
Association 74 (366): 318–28.
Rutstein, S., and K. Johnson. 2004. ―The DHS wealth index.‖ DHS Comparative Reports.
6., Calverton, Maryland: ORC Macro.
Seidman, D., P. Slater, P. Ever-Hadani, and R. Gale. 1987. ―Accuracy of mothers' recall
of birthweight and gestational age.‖ International Journal of Obstetrics &
Gynaecology 94 (8): 731–35.
Shrimpton R, C. Victora, M. de Onis, R. Costa Lima, M. Blössner, and G. Clugston.
2001. ―Worldwide timing of growth faltering: implications for nutritional
interventions.‖ Pediatrics 107: 75-81.
Sickles R., and P. Taubman. 1997. ―Mortality and morbidity among adults and elderly.‖
in Handbook of population and family economics, Vol. 1A, ed. M. Rosenzweig
and O. Stark. Amsterdam: North-Holland.
Steckel, Richard H. 1995. ―Stature and the standard of living.‖ Journal of Economic
Literature 33 (4): 1903–40.
———. 2009. ―Heights and human welfare: recent developments and new directions.”
Explorations in Economic History 46 (1): 1–23.
Thomas, D., J. Strauss, and M. Henriques. 1991. ―How does mother's education affect
child height?‖ Journal of Human Resources 26 (2): 183–211.
Victora, C., L. Adair, C. Fall, P. Hallal, R. Martorell, L. Richter, and H. Sachdev. 2008.
―Maternal and Child Undernutrition Study Group. Maternal and child
undernutrition: consequences for adult health and human capital.‖ Lancet 371
(9609): 302.
Victora, C, M. de Onis, P. Hallal, M. Blossner and R. Shrimpton. 2010. Worldwide
timing of Growth Faltering: Revisiting Implications for Interventions. Pediatrics.
125: 473-480..
Vaupel, J., K. Manton, and E. Stallard. 1979. ―The impact of heterogeneity in individual
frailty on the dynamics of mortality.‖ Demography 16: 439–54.

18
Wolpin, K. 1997. ―Determinants and consequences of the mortality and health of infants
and children.‖ In Handbook of population and family economics, Vol. 1A, ed. M.
Rosenzweig and O. Stark. Amsterdam: North-Holland.
WHO (World Health Organization). 1995. Physical status: the use and interpretation of
anthropometry. WHO technical report series 854. Geneva: World Health
Organization.
———. 2006. ―Child growth standards: length/height-for-age, weight-for-age, weight-
for-length, weight-for-height and body mass index-for-age: methods and
development.‖ Geneva: World Health Organization.
19
Table 1: Proportion of total deaths by age and gender for three rounds of India’s
National Family Health Survey (percent)
1992 1998 2005
Age Boys Girls Boys Girls Boys Girls
Neonatal 50.7 40.6 53.75 44.0 56.9 47.3
0–6 months 19.7 20.7 18.9 19.4 18.6 19.6
7–12 months 14.2 17. 8 12. 5 16.2 10.9 14.5
13–18 months 2.2 2.7 2.0 2.6 1.7 2.3
19–24 months 8.4 11.6 8.2 11.5 7.4 10.6
25–36 months 4.9 6.6 4.7 6.3 4.5 5.6
Total 100 100 100 100 100 100
Mortality rate
Standard error 0.080
(0.001)
0.077
(0.001)
0.064
(0.001)
0.066
(0.002)
0.058
(0.002)
0.056
(0.002)
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
Table 2: Changes in the total mean height-for-age z-score (HAZ) for different
imputation scenarios.
Boys Girls
Imputed
HAZ
Zd
Mean HAZ
Actual → Simulated
Zs → Zall
%Δ
total
HAZ
Imputed
HAZ
Zd
Mean HAZ
Actual → Simulated
Zs → Zall
%Δ
total
HAZ
Imputed HAZ (Zd) that results in a statistically significant change in total HAZ (Zall)
1992 -2.15 -1.91 → -1.95 1.70 -2.13 -1.86 → -1.90 1.85
1998 -2.12 -1.77 → -1.80 1.58 -2.22 -1.85 → -1.88 1.65
2005 -1.95 -1.55 → -1.57 1.77 -1.98 -1.53 → -1.56 1.92
Imputed HAZ (Zd) is twice as low as the average observed HAZ (Zs)
1992 -3.83 -1.91 → -2.17 13.51 -3.72 -1.86 → -2.10 12.99
1998 -3.55 -1.77 → -1.92 8.12 -3.71 -1.85 → -2.01 8.37
2005 -3.09 -1.55 → -1.65 6.78 -3.06 -1.53 → -1.63 6.60
Imputed HAZ (Zd) = - 5SD
1992 -5.00 -1.91 → -2.33 21.81 -5.00 -1.86 → -2.27 21.90
1998 -5.00 -1.77 → -2.03 14.78 -5.00 -1.85 → -2.12 14.21
2005 -5.00 -1.55 → -1.78 15.13 -5.00 -1.53 → -1.76 14.95
HAZ imputed based on upper bounds of Pelletier et al. (1995) estimates
1992 -2.61 -1.91 → -2.01 4.91 -2.59 -1.86 → -1.95 5.09
1998 -2.56 -1.77 → -1.84 3.61 -2.59 -1.85 → -1.92 3.32
2005 -2.49 -1.55 → -1.61 4.12 -2.48 -1.53 → -1.59 4.09
Source: Authors‘ analysis based on data from India‘s National Family Health Survey and estimates from
Pelletier and others (1995) on the upper bound of deaths in children due to malnutrition.
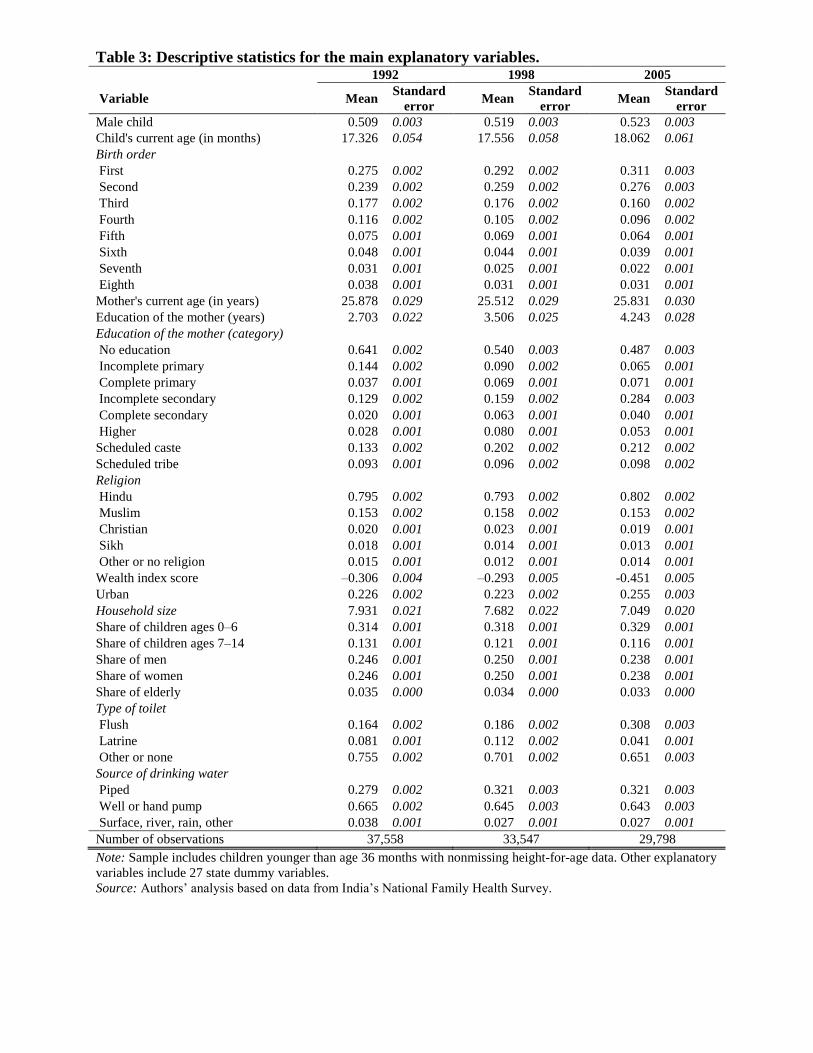
Table 3: Descriptive statistics for the main explanatory variables. 1992 1998 2005
Variable Mean Standard
error Mean
Standard
error Mean
Standard
error
Male child 0.509 0.003 0.519 0.003 0.523 0.003
Child's current age (in months) 17.326 0.054 17.556 0.058 18.062 0.061
Birth order
First 0.275 0.002 0.292 0.002 0.311 0.003
Second 0.239 0.002 0.259 0.002 0.276 0.003
Third 0.177 0.002 0.176 0.002 0.160 0.002
Fourth 0.116 0.002 0.105 0.002 0.096 0.002
Fifth 0.075 0.001 0.069 0.001 0.064 0.001
Sixth 0.048 0.001 0.044 0.001 0.039 0.001
Seventh 0.031 0.001 0.025 0.001 0.022 0.001
Eighth 0.038 0.001 0.031 0.001 0.031 0.001
Mother's current age (in years) 25.878 0.029 25.512 0.029 25.831 0.030
Education of the mother (years) 2.703 0.022 3.506 0.025 4.243 0.028
Education of the mother (category)
No education 0.641 0.002 0.540 0.003 0.487 0.003
Incomplete primary 0.144 0.002 0.090 0.002 0.065 0.001
Complete primary 0.037 0.001 0.069 0.001 0.071 0.001
Incomplete secondary 0.129 0.002 0.159 0.002 0.284 0.003
Complete secondary 0.020 0.001 0.063 0.001 0.040 0.001
Higher 0.028 0.001 0.080 0.001 0.053 0.001
Scheduled caste 0.133 0.002 0.202 0.002 0.212 0.002
Scheduled tribe 0.093 0.001 0.096 0.002 0.098 0.002
Religion
Hindu 0.795 0.002 0.793 0.002 0.802 0.002
Muslim 0.153 0.002 0.158 0.002 0.153 0.002
Christian 0.020 0.001 0.023 0.001 0.019 0.001
Sikh 0.018 0.001 0.014 0.001 0.013 0.001
Other or no religion 0.015 0.001 0.012 0.001 0.014 0.001
Wealth index score –0.306 0.004 –0.293 0.005 -0.451 0.005
Urban 0.226 0.002 0.223 0.002 0.255 0.003
Household size 7.931 0.021 7.682 0.022 7.049 0.020
Share of children ages 0–6 0.314 0.001 0.318 0.001 0.329 0.001
Share of children ages 7–14 0.131 0.001 0.121 0.001 0.116 0.001
Share of men 0.246 0.001 0.250 0.001 0.238 0.001
Share of women 0.246 0.001 0.250 0.001 0.238 0.001
Share of elderly 0.035 0.000 0.034 0.000 0.033 0.000
Type of toilet
Flush 0.164 0.002 0.186 0.002 0.308 0.003
Latrine 0.081 0.001 0.112 0.002 0.041 0.001
Other or none 0.755 0.002 0.701 0.002 0.651 0.003
Source of drinking water
Piped 0.279 0.002 0.321 0.003 0.321 0.003
Well or hand pump 0.665 0.002 0.645 0.003 0.643 0.003
Surface, river, rain, other 0.038 0.001 0.027 0.001 0.027 0.001
Number of observations 37,558 33,547 29,798
Note: Sample includes children younger than age 36 months with nonmissing height-for-age data. Other explanatory
variables include 27 state dummy variables.
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
21
Table 4: Weibull proportional hazard estimation for children ages 0–36 months using
mother’s estimate of birth size.
1992 1998 2005
Variable Hazard
ratio
Standard
error
Hazard
ratio
Standard
error
Hazard
ratio
Standard
error
Male child 1.050 0.049 1.002 0.054 0.987 0.062
Birth order
Second 1.724***
0.124 2.289***
0.234 2.053***
0.192
Third 2.442***
0.233 3.638***
0.470 2.579***
0.344
Fourth 3.472***
0.393 5.135***
0.832 3.338***
0.568
Fifth 3.768***
0.517 5.437***
0.994 5.102***
0.918
Sixth 3.968***
0.646 6.309***
1.347 6.937***
1.456
Seventh 4.337***
0.765 7.648***
1.788 7.502***
1.920
Eighth 7.718***
1.369 11.271***
2.682 9.086***
2.430
Born Small 2.008***
0.109 1.493***
0.088 1.381***
0.100
Characteristics of the mother
Mother's age (in years) 0.941* 0.031 0.915
** 0.035 1.045 0.057
Mother's age squared 1.001 0.001 1.000 0.001 0.998**
0.001
Incomplete primary 0.780***
0.061 1.098 0.103 1.034 0.128
Complete primary 0.867 0.119 0.747**
0.092 0.824 0.101
Incomplete secondary 0.770***
0.074 0.825**
0.079 0.642***
0.061
Complete secondary 0.502**
0.141 0.710**
0.106 0.607**
0.138
University and higher 0.496***
0.118 0.591***
0.115 0.325***
0.080
Household characteristics
Household size 0.772***
0.013 0.756***
0.016 0.694***
0.017
Household size squared 1.007***
0.001 1.007***
0.001 1.011***
0.001
Share of children ages 0– 6
years
0.001***
0.000 0.001***
0.000 0.001***
0.000
Share of children ages 7–15
years 0.177
*** 0.051 0.107
*** 0.036 0.182
*** 0.071
Share of elderly (60+) 0.303***
0.111 0.140***
0.062 0.435* 0.215
Share of women 0.552* 0.172 0.418
*** 0.137 0.544 0.218
Second wealth quintiles 1.053 0.068 0.926 0.068 1.148 0.104
Third wealth quintiles 1.021 0.076 0.838**
0.070 1.121 0.118
Fourth wealth quintiles 0.921 0.080 0.848 0.094 1.003 0.135
Fifth wealth quintiles 0.634***
0.097 0.639***
0.105 0.983 0.184
Hindu religion 0.944 0.151 0.931 0.148 1.007 0.194
Muslim religion 1.069 0.182 0.961 0.171 1.072 0.225
Scheduled caste 1.231***
0.081 1.104 0.075 0.994 0.079
Scheduled tribe 0.915 0.077 0.892 0.083 0.845 0.100
Living conditions
Latrine 0.765* 0.105 0.912 0.119 1.209 0.218
Other/none 0.908 0.114 0.911 0.108 1.146 0.124
Well/handpump 0.911 0.063 1.083 0.080 1.076 0.107
Surface, river, rain 1.007 0.126 0.998 0.161 1.529**
0.277
Other 0.764 0.137 0.757 0.244 1.283 0.409
Urban 0.929 0.075 0.979 0.092 1.017 0.095
Constant 1.408 0.906 4.352**
2.727 0.400 0.360
Ln(p) 0.533***
0.008 0.530***
0.010 0.481***
0.007
Ln(θ) 0.155 0.176 0.454 0.278 0.340 0.190
Log-Likelihood –13,870.68 –10,181.48 –9,308.23
Number of observations 37,621 33,556 29,859
*** p<0.01, ** p<0.05, * p<0.1.
Note: Coefficients on dummy variables for 27 states are not shown.
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.

22
Table 5: Weibull proportional hazard estimation for children ages 0–36 months using
recorded weights.
1992 1998 2005
Variable Hazard
ratio
Standard
error
Hazard
ratio
Standard
error
Hazard
ratio
Standard
error
Male child 1.588**
0.287 1.181 0.186 1.133 0.168
Birth order
Second 1.967***
0.479 4.476***
0.986 2.983***
0.547
Third 3.994***
1.287 4.205***
1.334 4.367***
1.212
Fourth 7.157***
3.013 4.286***
2.062 9.430***
3.451
Fifth 11.530***
6.806 10.650***
5.736 3.081* 1.946
Sixth 0.000***
0.000 5.201**
3.669 49.997***
26.524
Seventh 1.277 1.473 17.193***
11.702 30.526***
16.715
Eighth 16.028***
13.796 10.887**
12.939 1.214 1.539
Measured weight at birth 0.457***
0.068 0.533***
0.074 0.668***
0.098
Characteristics of the mother
Mother's age (in years) 0.905 0.107 0.905 0.103 1.293* 0.193
Mother's age squared 1.001 0.002 1.001 0.002 0.994**
0.003
Incomplete primary 0.930 0.238 0.821 0.190 1.047 0.257
Complete primary 1.358 0.426 0.533* 0.196 0.763 0.247
Incomplete secondary 0.642 0.182 0.461***
0.105 0.555***
0.104
Complete secondary 0.791 0.324 0.477**
0.141 0.469**
0.147
University and higher 0.512 0.210 0.317***
0.100 0.209***
0.078
Household characteristics
Household size 0.756***
0.046 0.668***
0.038 0.684***
0.042
Household size squared 1.006***
0.001 1.012***
0.002 1.010***
0.003
Share of children ages 0–6 years 0.001***
0.000 0.001***
0.000 0.001***
0.000
Share of children ages 7–15
years 0.063
*** 0.063 0.075
*** 0.070 0.022
*** 0.018
Share of elderly (60+) 0.637 0.741 0.078**
0.092 0.222* 0.194
Share of women 0.467 0.424 0.581 0.484 0.214**
0.150
Second wealth quintiles 0.694 0.320 0.787 0.250 1.147 0.327
Third wealth quintiles 0.653 0.289 0.884 0.271 1.628* 0.426
Fourth wealth quintiles 0.613 0.276 0.872 0.279 1.915**
0.542
Fifth wealth quintiles 0.399* 0.201 1.235 0.454 2.078
** 0.686
Hindu religion 0.835 0.221 1.194 0.348 0.846 0.234
Muslim religion 0.670 0.271 1.011 0.395 0.802 0.287
Scheduled caste 0.663 0.247 1.038 0.218 1.084 0.191
Scheduled tribe 0.426* 0.190 1.011 0.326 0.756 0.232
Living conditions
Latrine 0.819 0.243 0.981 0.280 0.957 0.358
Other/none 1.228 0.325 0.928 0.249 1.344 0.279
Well/handpump 0.938 0.177 0.916 0.158 1.351**
0.194
Surface, river, rain 1.301 0.686 1.154 0.697 1.043 0.559
Other 0.394 0.238 2.168* 0.990 1.342 0.837
Urban 1.546* 0.346 0.888 0.213 1.071 0.184
Constant 22.884* 39.678 55.530
** 100.703 0.339 0.744
Ln(p) 0.547***
0.027 0.517***
0.023 0.522***
0.018
Ln(θ) 0.001***
0.000 0.001***
0.000 0.001***
0.000
Log-Likelihood –1,011.30 –1,239.06 –1,791.04
Number of observations 6,228 8,555 12,755
***p<0.01, **p<0.05, *p<0.1.
Note: Coefficients on dummy variables for 27 states are not shown.
Source: Authors‘ analysis based on data from India‘s National Family Health Survey
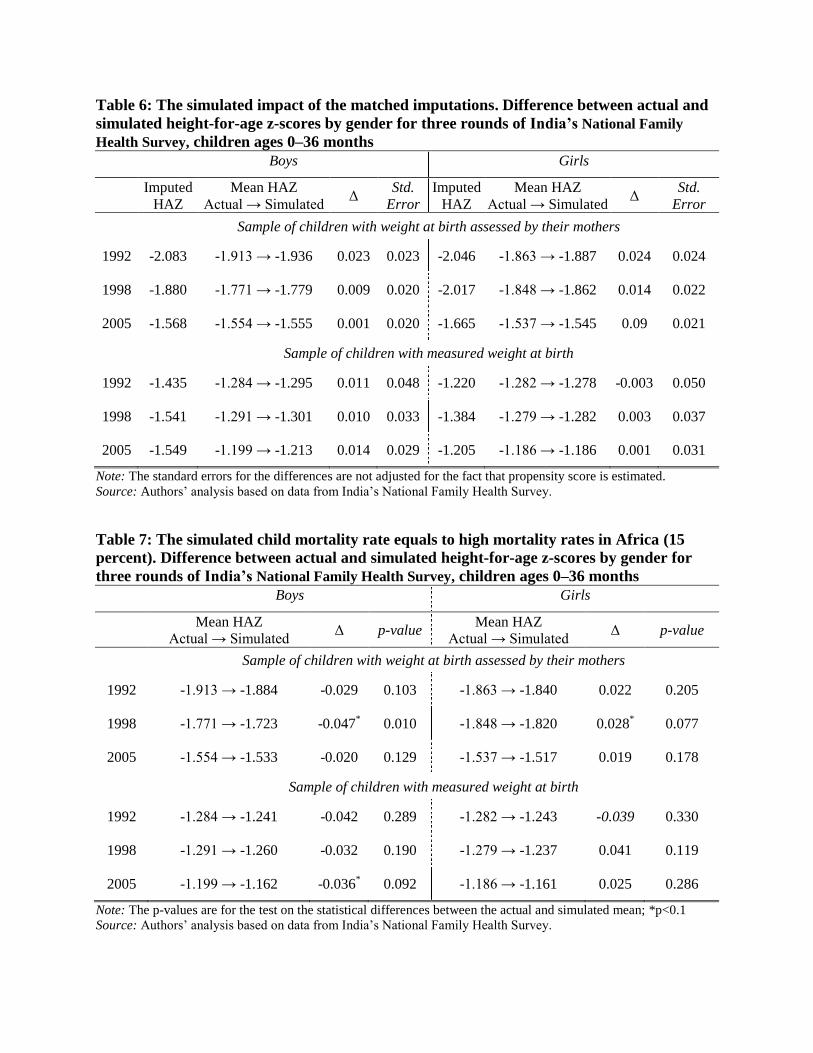
Table 6: The simulated impact of the matched imputations. Difference between actual and
simulated height-for-age z-scores by gender for three rounds of India’s National Family
Health Survey, children ages 0–36 months
Boys Girls
Imputed
HAZ
Mean HAZ
Actual → Simulated Δ
Std.
Error
Imputed
HAZ
Mean HAZ
Actual → Simulated Δ
Std.
Error
Sample of children with weight at birth assessed by their mothers
1992 -2.083 -1.913 → -1.936 0.023 0.023 -2.046 -1.863 → -1.887 0.024 0.024
1998 -1.880 -1.771 → -1.779 0.009 0.020 -2.017 -1.848 → -1.862 0.014 0.022
2005 -1.568 -1.554 → -1.555 0.001 0.020 -1.665 -1.537 → -1.545 0.09 0.021
Sample of children with measured weight at birth
1992 -1.435 -1.284 → -1.295 0.011 0.048 -1.220 -1.282 → -1.278 -0.003 0.050
1998 -1.541 -1.291 → -1.301 0.010 0.033 -1.384 -1.279 → -1.282 0.003 0.037
2005 -1.549 -1.199 → -1.213 0.014 0.029 -1.205 -1.186 → -1.186 0.001 0.031
Note: The standard errors for the differences are not adjusted for the fact that propensity score is estimated.
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
Table 7: The simulated child mortality rate equals to high mortality rates in Africa (15
percent). Difference between actual and simulated height-for-age z-scores by gender for
three rounds of India’s National Family Health Survey, children ages 0–36 months
Boys Girls
Mean HAZ
Actual → Simulated Δ p-value
Mean HAZ
Actual → Simulated Δ p-value
Sample of children with weight at birth assessed by their mothers
1992 -1.913 → -1.884 -0.029 0.103 -1.863 → -1.840 0.022 0.205
1998 -1.771 → -1.723 -0.047* 0.010 -1.848 → -1.820 0.028
* 0.077
2005 -1.554 → -1.533 -0.020 0.129 -1.537 → -1.517 0.019 0.178
Sample of children with measured weight at birth
1992 -1.284 → -1.241 -0.042 0.289 -1.282 → -1.243 -0.039 0.330
1998 -1.291 → -1.260 -0.032 0.190 -1.279 → -1.237 0.041 0.119
2005 -1.199 → -1.162 -0.036* 0.092 -1.186 → -1.161 0.025 0.286
Note: The p-values are for the test on the statistical differences between the actual and simulated mean; *p<0.1
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
24
Figure 1: Nelson-Aalen cumulative hazard by gender for three rounds of India’s National
Family Health Survey
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
0.00
0.02
0.04
0.06
0.08
0.10
Nel
son
-Aal
en c
um
ula
tiv
e h
azar
d
0 3 6 9 12 15 18 21 24 27 30 33 36
Age in months
Boys
Girls
1992
0.00
0.02
0.04
0.06
0.08
0.10
0 3 6 9 12 15 18 21 24 27 30 33 36
Age in months
1998
0.00
0.02
0.04
0.06
0.08
0.10
Nel
son
-Aal
en c
um
ula
tiv
e h
azar
d
0 3 6 9 12 15 18 21 24 27 30 33 36
Age in months
2005
25
Appendix
Table A1: Distribution of weight at birth for children ages 0–36 months at time of India National
Family Health Surveys by gender, mothers-assessed weight and measured weight
Boys Girls
Year and mothers-
assessed weight Share
Measured
weight
Mean (kg)
Standard
error Share
Measured
weight
Mean (kg)
Standard
error
1992
Larger than average 0.143 3.334 0.026 0.126 3.252 0.031
Average 0.649 2.855 0.013 0.636 2.747 0.013
Smaller than average 0.208 2.131 0.027 0.238 2.166 0.024
Total 1.000 2.828 0.013 1.000 2.736 0.013
Number of observations 19,131 3,248 18,232 2,997
1998
Larger than average 0.151 3.312 0.018 0.128 3.309 0.021
Average 0.621 2.820 0.010 0.610 2.771 0.011
Smaller than average 0.181 2.276 0.020 0.210 2.271 0.020
Very small 0.048 1.928 0.049 0.053 1.828 0.047
Total 1.000 2.810 0.010 1.000 2.753 0.010
Number of observations 17,188 4,608 15,721 3,971
2005
Very large 0.043 3.389 0.046 0.039 3.149 0.050
Larger than average 0.192 3.078 0.015 0.186 2.975 0.018
Average 0.553 2.903 0.009 0.535 2.811 0.008
Smaller than average 0.151 2.300 0.020 0.164 2.289 0.020
Very small 0.060 1.930 0.032 0.075 1.938 0.031
Total 1.000 2.844 0.008 1.000 2.737 0.008
Number of observations 16,001 7,090 14,745 6,211
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
26
Table A2: Difference between actual and simulated height-for-age z-scores by gender for
three rounds of India’s National Family Health Survey, children ages 3–36 months
Boys Girls
Imputed
HAZ
Mean HAZ
Actual → Simulated Δ
Std.
Error
Imputed
HAZ
Mean HAZ
Actual → Simulated Δ
Std.
Error
Sample of children with weight at birth assessed by their mothers
1992 -2.106 -2.015 → -2.027 0.012 0.023 -2.145 -1.962 → -1.986 0.024 0.024
1998 -2.071 -1.877 → -1.893 0.016 0.020 -2.063 -1.955 → -1.964 0.009 0.022
2005 -1.630 -1.622 → -1.623 0.001 0.020 -1.725 -1.614 → -1.622 0.007 0.022
Sample of children with measured weight at birth
1992 -1.473 -1.360 → -1.368 0.008 0.050 -1.381 -1.374 → -1.374 0.000 0.051
1998 -1.764 -1.373 → -1.389 0.015 0.034 -1.743 -1.348 → -1.360 0.011 0.038
2005 -1.532 -1.246 → -1.257 0.011 0.029 -1.551 -1.239 → -1.249 0.010 0.031
Note: The standard errors for the differences are not adjusted for the fact that propensity score is estimated.
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
27
Figure A1: Kernel density estimates of distributions of the matching scores for samples of
living and dead children for three rounds of India’s National Family Health Survey
Source: Authors‘ analysis based on data from India‘s National Family Health Survey.
Mean
sco
re
0
.05
.1
.15
.2
Pro
bab
ilit
y d
ensi
ty
-3 0 5 10 15 18
Matching score
Alive
Dead
1992
Mean
sco
re
0
.05
.1
.15
.2
Pro
bab
ilit
y d
ensi
ty
-3 0 5 10 15 18
Matching score
1998
Mean
sco
re
0
.05
.1
.15
.2
Pro
bab
ilit
y d
ensi
ty
-3 0 5 10 15 18
Matching score
2005