workshop 5 information technology ho shell 5_information...– pharmacy information system as first...
TRANSCRIPT

PRACTICE MODEL TRANSFORMATIONS:Achieving excellence through accountability and innovation
Information Technology‐Leading Versus Being Led in the New Information Era
Rita Shane, Pharm.D., FASHP, FCSHP
Cedars‐Sinai Medical Center
Los Angeles, CA
Christopher J. Urbanski, B.S.Pharm, M.S.
Indiana University Health
Indianapolis, IN
Objectives
• Discuss the importance of the pharmacy department’s role in leading the involvement of information technology in the institution’s medication‐use processes.
• Apply new ideas and ways to work closely with the IT department to assure the pharmacy department’s directdepartment to assure the pharmacy department s direct involvement in the medication‐use process.
• Analyze lessons learned from various scenarios of IT’s involvement in medication‐use processes
• Identify IT metrics to improve the medication use processes
• Identify the implications of meaningful use for pharmacy practice
Question
• What are the top 3 challenges you have experienced in implementing new information technology and automation? – Pharmacy information system
– Decentral or central automation
– Smart pumps
– Bar code dispensing
– Medication administration
– Other
6

Information Technology: Ideal (Future) State
• Clinical information systems and medication use technologies are integrated
• Medication information including updates (formulary changes, shortages) is communicated synchronously and transparently across systemsand transparently across systems
• Clinical decision support is relevant, timely and specific to patient care needs
• Workflows support safe, timely, efficient, effective medication use
• Pharmacists are involved in knowledge‐based vstransaction‐based activities
Information Technology Structure and Relationships
Information Technology
Medication Use Technologies
Automated Dispensing Machines
Robots, Carousels
Smart Pumps
Bar Code Dispensing
Clinical Information Systems
Pharmacy System
CPOE CDSS BCMA
Technology to Prevent Adverse Drug Events (ADEs)
Dispensing4%
Transcription6%
CarouselsRobots for Dispensing and IV CompoundingAutomated Dispensing Cabinets
Ordering56%
Administration34%
Source: Bates, et al. JAMA (1995) CPOEEMAR, Profiled Automated Dispensing Cabinets,BCMA, Smart Pumps
7

Information Technology: Under Construction
• Clinical information system may consist of multiple components (best of breeds) which may be interfaced with each other and with medication use technologies– Pharmacy information system may be separate from the computer prescriber order entry (CPOE) systemp p y ( ) y
• Organizational priorities for IT and automation implementation may not take into account implications for medication management and pharmacy
• Pharmacy staff maintain medication “libraries” across the various systems to ensure they are in synch
Information Technology: Under Construction
• Clinical decision support is limited to avoid alert fatigue
• Workflows are retrofitted to support the various systemsvarious systems
• Pharmacists are involved in numerous transactions related to processing orders which reduces time that can be allocated to patient care
Current challenges associated with information technology include
a. Multiple systems that require medication libraries to be in synch
b. Lack of clinical information system vendors
b f d d i i d i ic. Absence of drug‐drug interactions decision support
d. Lack of interface between pharmacy information system and automated dispensing cabinets
8

Cedars‐Sinai Medical Center
• 952 bed acute, tertiary care, non‐profit, teaching hospital• 2000 private attending physicians• 2000 nurses• Over 300 pharmacy staff• Traditional decentralized pharmacy services via 6 satellitesp y
– Integrated practice model: first dose dispensing, tech order entry, pharmacist verification
• 4 outpatient pharmacies• Home grown pharmacy information system from 1980‐
2009– Paper MAR (medication administration record)
Electronic Health Record Implementation Process
• Multidisciplinary process for vendor selection
• Implementation steps:
– Revenue Cycle
– Pharmacy Information System as first clinical go‐live– Pharmacy Information System as first clinical go‐live
• Pharmacy IT background
– Home grown system since 1980
– Not interfaced with automated dispensing machines
– Central robot for cart fill interfaced with legacy system
Electronic Health Record Implementation Process
34 Month Sprint –Jan 09‐present• Pharmacy information system • EMAR (electronic MAR)• Clinical documentation• Decentralized automation• Decentralized automation • Centralization of drug distribution from satellite‐based dispensing of doses until cart fill
• Housewide bar code medication administration*• Practice model redesign‐ongoing evolution• CPOE pilot 2011; rollout 2012
*except diagnostic/procedural areas and ED
9

Strategic Planning
• Core Principles
• Organizational Priorities
• Discipline‐Specific Priorities: RN, RX, MD, RT, O i i iCase Management, PT, OT, Dietitian, etc
• Medication Management Priorities
Core Principles
• One patient, one record (medical record)
• Leverage pharmacy expertise to meet the clinical needs of the patient is the priority
• One pharmacist touches all orders for a patient
• Processes must be designed to the highest standards for patientProcesses must be designed to the highest standards for patient safety, effectiveness, efficiency, reliability, and uniformity
• All health care providers physicians, pharmacists and nurses are responsible and accountable for the safety of the medication use process
• Checks and balances that assure safety and appropriateness are built into medication management process
Strategic Planning entails patient‐centered decision making
a. True
b. False
10

Strategic Planning
• Art of negotiation and compromise
– Being a part of the leadership project team
– Patient‐centered decision‐making
• Importance of multilingual leadership
Patient
IT
Pharmacy
Executive Mgmt
Nursing
Clinical Services Team*
Medical Staff
*Respiratory therapists, dietitians, PT/OT, case management staff
Multilingual Leadership
• Proactive
• Engaged in all aspects of technology planning
• What Pharmacy brings to the IT planning process
U d t di h t k h ld ’ d i d• Understanding each stakeholder’s domain and perspective
• Developing credible relationships
• When to compromise; when not to compromise
• How and when to communicate and educate
11

Medication Use and AutomationPHYSICIAN PHARMACY
CPOE
Rx Evaluation & Review
Robot
Carousel
ADC
Smart Pump
E‐MAR Documentation
Med CartTPN Pump
BCMA
High speed packager
Strategic Planning
• Change management
– Begins with oneself
• Human‐Technology Interfaces and Workflows
I f d di d d– Importance of understanding end‐to‐end workflows
– Anticipating unintended consequences
• Engaging pharmacy staff in redesign of medication use process
12

Technology ImplementationLessons Learned
• Important to ensure Pharmacy participates in planning at the organizational leadership level
• Participation provides opportunities for education:
A medication order is a sentence.• Ongoing communication and meetings are resource• Ongoing communication and meetings are resource‐
intensive but essential
• Resources are allocated based on understanding of pharmacy’s essential role in medication management
• Integrated systems create new linkages and new tensions between disciplines and within Pharmacy
• Patient centered focus drives decision‐making
• Tension is natural
• Compromise is inevitable
• Leadership is essential
Technology ImplementationLessons Learned
• Education is invaluable
• Persistence and timing are critical
Small Group Discussions #1Strategic Planning and Change Management
• Hospital R2D2 is in the process of implementing an electronic health record (EHR); first phase planned for sometime in 2012
• You are the pharmacy leader and you are very enthusiastic about the Pharmacy Practice Model Initiative and ensuring pharmacists practice at the top of their license at your organizations
• After much dialogue with colleagues reading AJHP at all hours of the• After much dialogue with colleagues, reading AJHP at all hours of the night, studying options at the Exhibit Hall at ASHP meetings and conducting site visits at other health‐system pharmacies, you and your pharmacy team have determined that you need to change your medication distribution system
• Your VP concurs with your decision and states that capital funding should not be a problem and advises you to put together a strategic plan to obtain approval from IT and Executive Management
13
See page 27 for enlarged view

Small Group Discussions #1Strategic Planning and Change Management
Objective: Develop a strategic plan for changing the medication distribution system in order to advance the practice model in your health system
• Elements of the Strategic Plan should include:– Rationale for change and process for communicating to IT and
Executive Management P d i li b f f Ph 1 f HER ( l i h l h– Proposed timeline‐before or after Phase 1 of HER (electronic health record)
– Stakeholder identification and engagement – Key implementation milestones– Key challenges and tactics to overcome them
• Scenarios1. Change from central robot to decentralized automated cabinets2. Changed from decentralized automated cabinets to central robot
Closing the Loop: Incorporating New Technologies into Medication ManagementMedication Management Workflows
Medication‐Use Process: Closing The Loop
Prescribe
Prepare/Procurement/
Dispense
AdministerMonitor
Storage
14
See page 27 for enlarged view

Which best describes your position with respect to closed‐loop medication systems?
a. I can define and we have this
b. I can define but we don’t have this
I thi k I d fi thic. I think I can define this
d. I’m not sure what this is
e. Other
What is a Closed‐Loop Control System?
• In a closed‐loop control system, a sensor monitors the system output and feeds the data to a controller which adjusts the control as necessary to maintain the desired systemas necessary to maintain the desired system output.
Wikipedia. Control theory. http://en.wikipedia.org/wiki/Control_theory#Closed‐loop_transfer_function (2011 Aug 20)
Closed‐Loop Diagram
Car’sspeed
Throttle position Engine
Monitor
Wikipedia. Control theory. http://en.wikipedia.org/wiki/Control_theory#Closed‐loop_transfer_function (2011 Aug 20)
15

What do we mean by a “Closed‐Loop Medication‐Use System”?
“The achievement of an outcome using information‐system support can come from a new expression of system control called a closed‐loop solution A closed‐loop solutionclosed loop solution. A closed loop solution offers online, real‐time control of information.”
Bill Felkey
Felkey BG. Health system informatics. Am J Health‐Syst Pharm. 1997; 54:274‐80
Closed‐Loop MedicationManagement System
A truly closed‐loop medication management system is designed to feed outcomes from medication processes back into the system to allow for future improvements and changes inallow for future improvements and changes in a patient’s course of care.
Closing the Loop in Medication Management. Microsoft Amalga Hospital Information System. April 2009.
Closed‐Loop Medication‐Use Control System: CPOE
Safe
EMRPrescriberOrderEntry
Safe medication therapy
Pharmacist/CDSS
16

Closed‐Loop Medication‐Use Control System: ADC Profile
Accurate Med
Order Verification EMR and ADC
Formulary
Med Profile
Interface
Closed‐Loop Medication‐Use Systems
• Eliminates a great many steps in the complex process, thereby significantly reducing the number of opportunities for mistakes.
• At one U.S. medical center, closing the loopAt one U.S. medical center, closing the loop meant reducing the number of steps in medication administration from 17 to 5, which decreased the rate of harm from ADEs from 3.5 per 1,000 to 0.52 per 1,000 patients
Closing the Loop in Medication Management. Microsoft Amalga Hospital Information System. April 2009.
Closed‐Loop Medication‐Use Systems
“The typical IT approach to implementing a new system involves automating existing processes. Using this approach, organizations achieve only 10% of the potential value fromachieve only 10% of the potential value from the new system.”
Small R, Kubej, J. Closed‐Loop Medication Management: The Big Payback. 2007; HIMSS Annual Conference and Exhibition
17
Optimizing Process Flow
StandardizeReduce Eliminate Reduce
MeasureStandardize the Process
Process Variation
Unnecessary Steps
Opportunity for Error
Measure Results
Adapted from: Small R, Kubej, J. Closed‐Loop Medication Management: The Big Payback. 2007; HIMSS Annual Conference and Exhibition
• "If you want to make enemies, try to change something."—Woodrow Wilson
• "Change is the law of life and those who look only to the past or present are certain to miss the future."—John F Kennedy
Change is Hard!
John F. Kennedy
• "Change is hard because people overestimate the value of what they have—and underestimate the value of what they may gain by giving that up."— James Belasco and Ralph StayerFlight of the Buffalo (1994)
Project Management – Process Redesign
• Design Milestone
– Current State Process Flow Diagram
• Necessary evil
• Need details step‐by‐stepNeed details step by step
• Verify with those who know
– Future State Process Flow Diagram
• What steps can be improved?
• Don’t just convert current state to electronic state
• How can the vendor help optimize the process?
18

What is your level of experience with creating process flow diagrams?
a. Expert.
b. Fairly experienced.
S h t i dc. Somewhat experienced.
d. Minimal experience.
e. No experience.
Sample Process Flow Diagram
Small Group Discussions #2: Unit‐Dose Process Flow Diagram
• US Global Health Hospitals and Clinics
– Initiated project for BCMA implementation
– Current table‐top oral solid packager does not apply a barcodeapply a barcode
– Will implement a new high‐speed oral solid packager as part of barcode infrastructure
– Unit‐dose distribution model is decentral cartlessmodel with ADCs (automated dispensing cabinets)
19
See page 28 for enlarged view
Current‐State Workflow
Unit-Dose Workflow Diagram
Pha
rmac
y W
areh
ouse
B
uyer
ehou
se
nici
an
Unit-dose med?
No
YesPharmacy
Warehouse Ordering and Receiving
Needs repackaging?
Stocked in warehouse
Yes
No
Stocked in warehouse
Pha
rmac
y C
ompo
undi
ng
Tec
hnic
ian
Pha
rmac
ist
Pha
rmac
y T
echn
icia
nW
are
Tec
h
Packaged with unit-dose table-top
packager
Order entry/verification
Label prints to send first doses or
stock ADC
Doses picked from dispensing area
Doses sent to floor or stocked in ADC
Small Group Discussions #2: Assignment
• Add high‐speed oral solid packager into workflow
• Identify steps that can be improved or eliminatedeliminated
• Be sure to close the loop – what is the sensor or monitor to provide system feedback?
• Are there ways to align with the IT department for support?
Information Technology (IT) Metrics
• Identify core set of metrics across key dimensions of pharmacy practice to support safe and effective medication use
20
See page 28 for enlarged view
See page 29 for enlarged view

IT Metrics
Dimension Metric
Operational Turnaround time‐MD order‐RN administration
Clinical # contraindicated drug‐drug interaction overrides/month
Medication Safety # prescribing errors intercepted/month# reversal agents administered toprevent an adverse drug event/month
Financial Drug cost/solid organ transplant by type of transplant
Workload # orders verified/hr/pharmacist in med‐surg vs oncology vs ICU
Real‐Time Metric Dashboards
Real‐Time Metric Dashboards
21

Real‐Time Metric Dashboards
Advancing the Pharmacy Practice Model
Innovation
CollaborationLeading the Technology
Small Group Discussions #3
• Develop core set of metrics for each dimension
22
See page 29 for enlarged view

IT Metrics
Dimension Metric
Operational
Clinical
Medication Safety
Financial
Workload
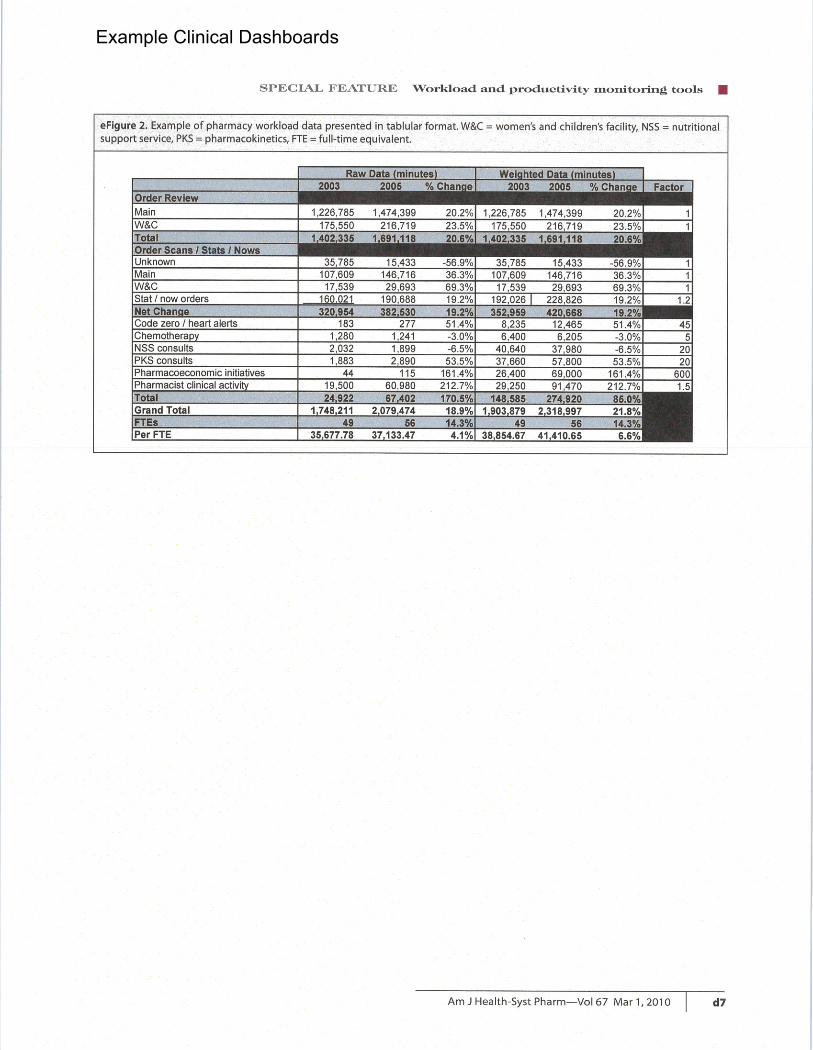
Dashboard Resources
• Bahl V et al. Developing dashboards to measure and manage inpatient pharmacy costs Am J Health Syst Pharm September 1, 2007 64:1859‐66; doi:10.2146/ajhp060596
• Rough SS et al. Effective use of workload and d ti it it i t l i h lth tproductivity monitoring tools in health‐system
pharmacy, part 2 Am J Health Syst Pharm March 1, 2010 67:380‐88; doi:10.2146/ajhp090217.p2
• Pedersen CA et al. ASHP national survey of pharmacy practice in hospital settings: Prescribing and transcribing—2010 Am J Health Syst Pharm April 15, 2011 68:669‐88; doi:10.2146/ajhp100711
Meaningful Use Highlights
• Initial standards and certification criteria for Electronic Health Record technology– Stage 1‐2011
– Incentives for early adoption:
• $7.2M over 4 years for hospital with 200,000 discharges; penalties for non‐compliance by 2015
• Improve Quality, Safety, Efficiency– CPOE
– Implement drug‐drug, drug‐allergy, drug‐formulary checks
– Active medication & allergy lists
– Implement drug formulary checks
https://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqSummary.pdf
23
See page 30 for enlarged view

What are the Requirements of Stage 1 Meaningful Use?
Hospitals must complete:
• 14 Core Objectives
Obj i f 10 f• 5 Objectives out of 10 from menu set
• 15 Clinical Quality Measures
https://www.cms.gov/EHRIncentivePrograms/Downloads/MU_Stage1_ReqSummary.pdf
Meaningful Use Highlights• Engage Patients and Families
– Provide patients with electronic copy of health information
• Improve Care Coordination– Performmedication reconciliation at relevant– Perform medication reconciliation at relevant encounters, transitions
• Clinical Quality Measures (CQM)– Core Measures
• Hypertension: Blood Pressure Measurement• Tobacco Use Assessment; Tobacco Cessation Intervention • Adult Weight Screening and Follow‐up
• Emergency Department (ED) Throughput –admitted patients Median time from ED arrival to ED departure for admitted patients
• Emergency Department Throughput –admitted patients –Admission decision time to ED departure time for admitted patients
Required Hospital Clinical Quality Measures
patients
• Ischemic stroke –Discharge on anti‐thrombotics
• Ischemic stroke –Anticoagulation for A‐fib/flutter
• Ischemic stroke –Thrombolytic therapy for patients arriving within 2 hours of symptom onset
www.cms.gov/ehrIncentivePrograms, accessed 8/28/11.
24

• Ischemic or hemorrhagic stroke –Antithrombotic therapy by day 2
• Ischemic stroke –Discharge on statins
• Ischemic or hemorrhagic stroke –Stroke education
• Ischemic or hemorrhagic stroke –Rehabilitation
Required Hospital Clinical Quality Measures
assessment
• VTE prophylaxis within 24 hours of arrival
• Intensive Care Unit VTE prophylaxis
• Anticoagulation overlap therapy
• Platelet monitoring on unfractionated heparin
• VTE discharge instructions
• Incidence of potentially preventable VTEwww.cms.gov/ehrIncentivePrograms, accessed 8/28/11.
The best approach to implementing a new
system involves automating existing processes.
a. True
b. False
Which of the following is not a strategy for optimizing process flow?
a. Eliminate unnecessary steps.
b. Estimate results.
c. Standardize the process.
d. Reduce process variation.
e. Reduce opportunity for error.
25

Real‐time pharmacy metric dashboards may include all of the following except:
a. Financial data.
b. Clinical workload.
c. Order queue volume.
d. Patient acuity score.
e. Prescription insurance plans.
PRACTICE MODEL TRANSFORMATIONS:Achieving excellence through accountability and innovation
Information Technology‐Leading Versus Being Led in the New Information Era
CE Session Code for this workshop:
L11xxx
26
Small Group Discussions #1Strategic Planning and Change Management
• Hospital R2D2 is in the process of implementing an electronic health record (EHR); first phase planned for sometime in 2012
• You are the pharmacy leader and you are very enthusiastic about the Pharmacy Practice Model Initiative and ensuring pharmacists practice at the top of their license at your organizations
• After much dialogue with colleagues, reading AJHP at all hours of the night, studying options at the Exhibit Hall at ASHP meetings and conducting site visits at other health‐system pharmacies, you and your pharmacy team have determined that you need to change your medication distribution system
• Your VP concurs with your decision and states that capital funding should not be a problem and advises you to put together a strategic plan to obtain approval from IT and Executive Management
Small Group Discussions #1Strategic Planning and Change Management
Objective: Develop a strategic plan for changing the medication distribution system in order to advance the practice model in your health systemhealth system
• Elements of the Strategic Plan should include:– Rationale for change and process for communicating to IT and
Executive Management – Proposed timeline‐before or after Phase 1 of HER (electronic health
record)– Stakeholder identification and engagement – Key implementation milestones
h ll d i h– Key challenges and tactics to overcome them
• Scenarios1. Change from central robot to decentralized automated cabinets2. Changed from decentralized automated cabinets to central robot
27

Small Group Discussions #2: Unit‐Dose Process Flow Diagram
• US Global Health Hospitals and Clinics
– Initiated project for BCMA implementation
– Current table‐top oral solid packager does not apply a barcode
– Will implement a new high‐speed oral solid packager as part of barcode infrastructure
– Unit‐dose distribution model is decentral cartlessmodel with ADCs (automated dispensing cabinets)
Current‐State Workflow
Unit-Dose Workflow Diagram
Pha
rmac
y W
are
hous
e B
uyer
Ph
arm
acy
Tec
hnic
ian
War
eho
use
Tec
hnic
ian
Unit-dose med?
No
YesPharmacy
Warehouse Ordering and Receiving
Needs repackaging?
Stocked in warehouse
Yes
No
Stocked in warehouse
Label prints to send first doses or
stock ADC
Doses picked from dispensing area
Doses sent to floor or stocked in ADC
Pha
rmac
y C
ompo
und
ing
Tec
hnic
ian
Pha
rmac
ist
Packaged with unit-dose table-top
packager
Order entry/verification
28

Small Group Discussions #2: Assignment
• Add high‐speed oral solid packager into kflworkflow
• Identify steps that can be improved or eliminated
• Be sure to close the loop – what is the sensor or monitor to provide system feedback?or monitor to provide system feedback?
• Are there ways to align with the IT department for support?
Small Group Discussions #3
• Develop core set of metrics for each di idimension
29

IT Metrics
Dimension Metric
Operational
Clinical
Medication Safety
Financial
Workload
30

Sixteenth Annual ASHP Conference
for Leaders in Health-System Pharmacy SELF-ASSESSMENT QUESTIONS 1. Current challenges associated with information technology include
a. Multiple systems that require medication libraries to be in synch. b. Lack of clinical information system vendors. c. Absence of drug-drug interactions decision support. d. Lack of interface between pharmacy information system and automated dispensing
cabinets. 2. Strategic Planning entails patient-centered decision making
a. True. b. False.
3. The best approach to implementing a new system involves automating existing processes.
a. True. b. False.
4. Which of the following is not a strategy for optimizing process flow?
a. Eliminate unnecessary steps. b. Estimate results. c. Standardize the process. d. Reduce process variation. e. Reduce opportunity for error.
5. Real-time pharmacy metric dashboards may include all of the following except:
a. Financial data. b. Clinical workload. c. Order queue volume. d. Patient acuity score. e. Prescription insurance plans.
31

Sixteenth Annual ASHP Conference
for Leaders in Health-System Pharmacy REFERENCES
Kelly WN, Rucker TD. Compelling features of a safe medication-use system. Am J Health-Syst Pharm. 2006; 63:1461-8
Felkey BG. Health system informatics. Am J Health-Syst Pharm. 1997; 54:274-80
Small R, Kubej, J. Closed-Loop Medication Management: The Big Payback. 2007; HIMSS Annual Conference and Exhibition.
Closing the Loop in Medication Management. Microsoft Amalga Hospital Information System. April 2009.
Wikipedia. Control theory. http://en.wikipedia.org/wiki/Control_theory#Closed-loop_transfer_function (2011 Aug 20).
Bahl V et al. Developing dashboards to measure and manage inpatient pharmacy costs. Am J Health Syst Pharm. September 1, 2007; 64:1859-66; doi:10.2146/ajhp060596.
Rough SS et al. Effective use of workload and productivity monitoring tools in health-system pharmacy, part 2 Am J Health Syst Pharm. March 1, 2010; 67:380-88; doi:10.2146/ajhp090217.p2.
Pedersen CA et al. ASHP national survey of pharmacy practice in hospital settings: Prescribing and transcribing—2010 Am J Health Syst Pharm. April 15, 2011; 68:669-88; doi:10.2146/ajhp100711.
32

Example Clinical Dashboards

Example Clinical Dashboards
Example Clinical Dashboards

Example Clinical Dashboards

1
Eligible Hospital and Critical Access Hospital (CAH) Attestation Worksheet for the Medicare Electronic Health Record (EHR) Incentive
Program
The Eligible Hospital and CAH Attestation Worksheet allows eligible hospitals and CAHs to log their meaningful use measures on this page to use as a reference when attesting for the Medicare EHR Incentive Program in the CMS system.
Numerator, denominator, and exclusion information for clinical quality measures (CQMs) must be reported directly from information generated by certified EHR technology and are not included in this worksheet. However, information for the remaining meaningful use core and menu set measures does not necessarily have to be entered directly from information generated by certified EHR technology. For each objective with a percentage-based measure, certified EHR technology must include the capability to electronically record the numerator and denominator and generate a report including the numerator, denominator, and resulting percentage for these measures. However, eligible hospitals and CAHs may use additional data to calculate numerators and denominators and to generate reports on all measures of the core and menu set meaningful use objectives except CQMs. In order to provide complete and accurate information for certain of these measures, eligible hospitals and CAHs may also have to include information from paper-based patient records or from records maintained in uncertified EHR technology.
Eligible hospitals and CAHs can enter their meaningful use criteria in the blue boxes. Each measure’s objective is included to help eligible hospitals and CAHs enter the correct criteria. Certain measures do not require a numerator and denominator, but rather a yes/no answer, and are marked as such. Measures with exclusions have the exclusion description listed in the measure information section.
Note: Claiming an exclusion for a specific measure qualifies as submission of that measure. If an eligible hospital or CAH claims an exclusion for which they qualify, indicate this in the Attestation System by clicking “yes” under the exclusion part of the measure question.
Eligible hospitals and CAHs must report on the following:
1. All 14 of the core measures; 2. 5 out of 10 of the menu measures; at least 1 public health measure must be selected
as part of the 5 3. All 15 of the clinical quality measures (CQMs)
Reporting Period: For an eligible hospital or critical access hospital, the reporting period must be at least 90 consecutive days within Federal Fiscal Year 2011 (October 1, 2010, through September 30, 2011).

2
Meaningful Use Core Measures - Eligible hospitals and CAHs must fill out all 14 core measures
# Measure Information Measure Values
1 Objective: Use computerized provider order entry (CPOE) for medication orders directly entered by any licensed healthcare professional who can enter orders into the medical record per state, local and professional guidelines. Measure: More than 30 percent of all unique patients with at least one medication in their medication list admitted to the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) have at least one medication order entered using CPOE Numerator: Number of patients in the denominator that have at least one medication order entered during CPOE Denominator: Number of unique patients with at least one medication in their medication list seen by the eligible hospital or CAH during the EHR reporting period
2 Objective: Implement drug-drug and drug-allergy interaction checks Measure: The eligible hospital or CAH has enabled the functionality for drug-drug and drug-allergy interaction checks for the entire EHR reporting period Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
3 Objective: Maintain an up-to-date problem list of current and active diagnoses Measure: More than 80 percent of all unique patients admitted to the eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) have at least one entry or an indication that no problems are known for the patient recorded as structured data Numerator: Number of patients in the denominator who have at least one entry or indication that no problems are known for the patient recorded as structured data in their problem list Denominator: Number of unique patients admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period
4 Objective: Maintain active medication list Measure: More than 80 percent of all unique patients admitted to the eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) have at least one entry (or an indication that the patient is not currently prescribed any medication) recorded as structured data Numerator: Number of patients in the denominator who have a medication (or an indication that the patient is not currently prescribed any medication) recorded as structured data Denominator: Number of unique patients admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period

3
# Measure Information Measure Values
5 Objective: Maintain active medication allergy list Measure: More than 80 percent of all unique patients admitted to the eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) have at least one entry (or an indication that the patient has no known medical allergies) recorded as structured data Numerator: Number of patients in the denominator who have at least one entry (or indication that the patient has no known medical allergies) recorded as structured data in their medication allergy list Denominator: Number of unique patients admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period
6 Objective: Record all of the following demographics: preferred language, gender, race, ethnicity, date of birth, and date and preliminary cause of death in the event of mortality in the eligible hospital or CAH Measure: More than 50 percent of all unique patients seen by the eligible hospital or CAH or admitted to the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) have demographics recorded as structured data Numerator: Number of patients in the denominator who have all of the elements of demographics (or a specific exclusion if the patient declined to provide one or more elements or if recording an element is contrary to state law) recorded as structured data Denominator: Number of unique patients admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period
7 Objective: Record and chart changes in vital signs: height, weight, blood pressure, calculate and display body mass index (BMI), plot and display growth charts for children 2-20 years, including BMI Measure: For more than 50 percent of all unique patients age 2 and over admitted to eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23), height, weight and blood pressure are recorded as structured data Numerator: Number of patients in the denominator who have at least one entry of their height, weight and blood pressure are recorded as structured data Denominator: Number of unique patients age 2 or over that are admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period
8 Objective: Record smoking status for patients 13 years or older Measure: More than 50 percent of all unique patients 13 years or older admitted to eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) have smoking status recorded as structured data Exclusion: An eligible hospital or CAH that sees no patients 13 years or older would be excluded from this requirement Does this exclusion apply to you? Yes NoNumerator: Number of patients in the denominator with smoking status recorded as structured data Denominator: Number of unique patients age 13 or over admitted to an eligible hospital or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR report period

4
# Measure Information Measure Values
9 Objective: Report hospital clinical quality measures to CMS or, in the case of Medicaid eligible hospitals, the States Measure: Provide aggregate numerator, denominator, and exclusions through attestation as discussed in section II(A)(3) of the final Rule Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
10 Objective: Implement one clinical decision support rule related to a high priority hospital condition with the ability to track compliance with that rule Measure: Implement one clinical decisions support rule Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
11 Objective: Provide patients with an electronic copy of their health information (including diagnostic test results, problem list, medication lists, medication allergies, discharge summary, procedures), upon request Measure: More than 50% of all patients of the inpatient or emergency department of the eligible hospital or CAH (POS 21 or 23) who request an electronic copy of their health information are provided it within 3 business days Exclusion: Any eligible hospital or CAH that has no requests from patients or their agents for an electronic copy of patient health information during the EHR reporting period would be excluded from this requirement Does this exclusion apply to you? Yes NoNumerator: Number of patients in the denominator who receive an electronic copy of their electronic health information within three business days Denominator: Number of patients who request an electronic copy of their electronic health information four business days prior to the end of the EHR reporting period
12 Objective: Provide patients with an electronic copy of their discharge instructions at the time of discharge, upon request Measure: More than 50% of all patients who are discharged from an eligible hospital or CAH’s inpatient department or emergency department (POS 21 or 23) and who request an electronic copy of their discharge instructions are provided it Exclusion: An eligible hospital or CAH that has no requests from patients or their agents for an electronic copy of the discharge instructions during the EHR reporting period would be excluded from this requirement Does this exclusion apply to you? Yes NoNumerator: The number of patients in the denominator who are provided an electronic copy of discharge instructions Denominator: Number of patients discharged from an eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) who request an electronic copy of their discharge instructions during the EHR reporting period

5
# Measure Information Measure Values
13 Objective: Capability to exchange key clinical information (for example, discharge summary, procedures, problem list, medication list, medication allergies, diagnostic test results), among providers of care and patient-authorized entities electronically Measure: Performed at least one test of certified EHR technology’s capacity to electronically exchange key clinical information Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
14 Objective: Protect electronic health information created or maintained by the certified EHR technology through the implementation of appropriate technical capabilities Measure: Conduct or review a security risk analysis in accordance with the requirements under 45 CFR 164.308(a)(1) and implement security updates as necessary and correct identified security deficiencies as part of its risk management process Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
Meaningful Use Menu Measures - Eligible hospitals and CAHs must fill out 5 out of 10 menu measures (at least 1 of these must be a public health measure, which are noted with an asterisk)
# Measure Information Measure Values
1* Objective: Capability to submit electronic data to immunization registries or immunization information systems and actual submission according to applicable law and practice Measure: Performed at least one test of certified EHR technology’s capacity to submit electronic data to immunization registries and follow up submission if the test is successful (unless none of the immunization registries to which the eligible hospital or CAH submits such information has the capacity to receive the information electronically) Exclusion 1: An eligible hospital or CAH that administers no immunizations during the EHR reporting period would be excluded from this requirement Exclusion 2: If there is no immunization registry that has the capacity to receive the information electronically, then the eligible hospital or CAH would be excluded from this requirement Note: This measure only requires a yes/no answer Does this exclusion 1 apply to you? Yes NoDoes this exclusion 2 apply to you? Yes NoNumerator: N/A
YES NODenominator: N/A

6
# Measure Information Measure Values
2* Objective: Capability to submit electronic data on reportable (as required by State or local law) lab results to public health agencies and actual submission according to applicable law and practice Measure: Performed at least one test of certified EHR technology’s capacity to provide electronic submission of reportable lab results to public health agencies and follow-up submission if the test is successful (unless none of the public health agencies to which an eligible hospital or CAH submits such information has the capacity to receive the information electronically) Exclusion: If no public health agency to which the eligible hospital or CAH submits such information has the capacity to receive the information electronically, then the eligible hospital or CAH would be excluded from this requirement Note: This measure only requires a yes/no answer Does this exclusion apply to you? Yes NoNumerator: N/A
YES NODenominator: N/A
3* Objective: Capability to submit electronic syndromic surveillance data to public health agencies and actual submission according to applicable law and practice Measure: Performed at least one test of certified EHR technology’s capacity to provide electronic syndromic surveillance data to public health agencies and follow-up submission if the test is successful (unless none of the public health agencies to which an eligible hospital or CAH submits such information has the capacity to receive the information electronically) Exclusion: If no public health agency to which the eligible hospital or CAH submits such information has the capacity to receive the information electronically, then the eligible hospital or CAH would be excluded from this requirement Note: This measure only requires a yes/no answer Does this exclusion apply to you? Yes NoNumerator: N/A
YES NODenominator: N/A
4 Objective: Implement drug formulary checks Measure: The eligible hospital or CAH has enabled this functionality and has access to at least one internal or external formulary for the entire EHR reporting period Note: This measure only requires a yes/no answer Numerator: N/A
YES NODenominator: N/A
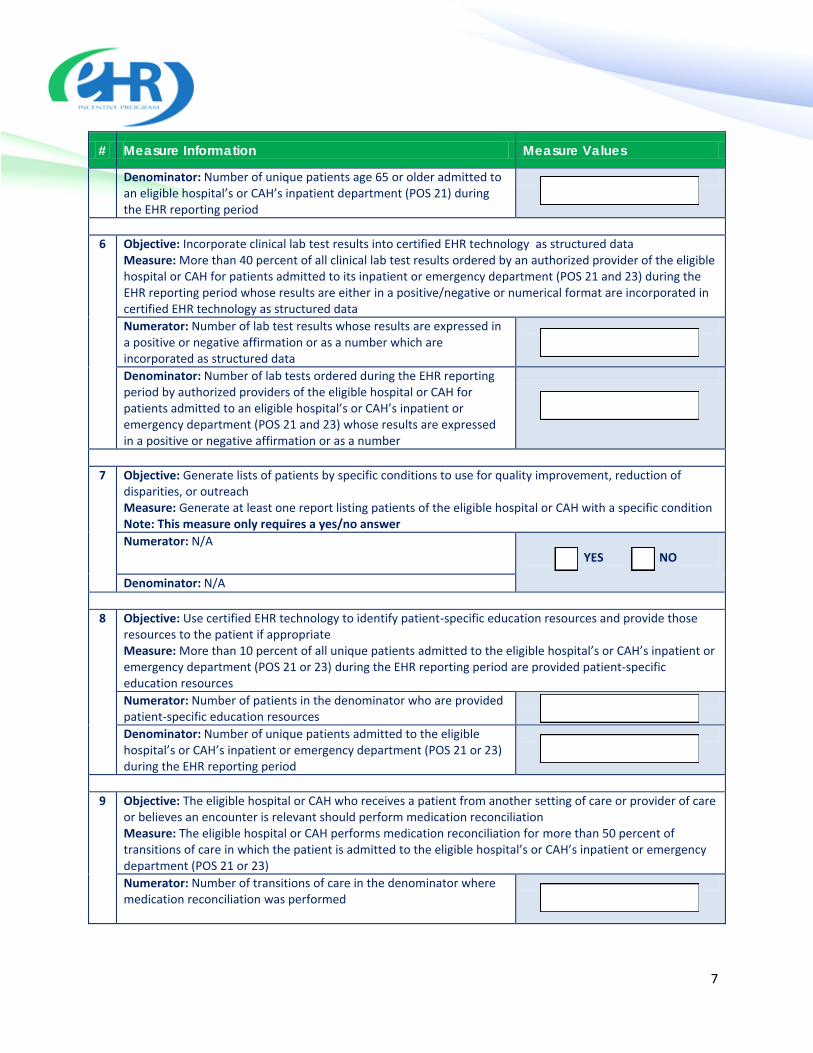
5 Objective: Record advance directives for patient 65 years old or older Measure: More than 50 percent of all unique patients 65 years old or older admitted to the eligible hospital’s or CAH’s inpatient (POS 21) have an indication of an advance directive status recorded as structured data Exclusion: An eligible hospital or CAH that admitted no patients age 65 years old or older during the EHR reporting period would be excluded from this requirement Does this exclusion apply to you? Yes NoNumerator: Number of patients in the denominator with an indication of an advanced directive entered using structured data
7
# Measure Information Measure Values
Denominator: Number of unique patients age 65 or older admitted to an eligible hospital’s or CAH’s inpatient department (POS 21) during the EHR reporting period
6 Objective: Incorporate clinical lab test results into certified EHR technology as structured data Measure: More than 40 percent of all clinical lab test results ordered by an authorized provider of the eligible hospital or CAH for patients admitted to its inpatient or emergency department (POS 21 and 23) during the EHR reporting period whose results are either in a positive/negative or numerical format are incorporated in certified EHR technology as structured data Numerator: Number of lab test results whose results are expressed in a positive or negative affirmation or as a number which are incorporated as structured data Denominator: Number of lab tests ordered during the EHR reporting period by authorized providers of the eligible hospital or CAH for patients admitted to an eligible hospital’s or CAH’s inpatient or emergency department (POS 21 and 23) whose results are expressed in a positive or negative affirmation or as a number
7 Objective: Generate lists of patients by specific conditions to use for quality improvement, reduction of disparities, or outreach Measure: Generate at least one report listing patients of the eligible hospital or CAH with a specific condition Note: This measure only requires a yes/no answer Numerator: N/A
YES NO
Denominator: N/A
8 Objective: Use certified EHR technology to identify patient-specific education resources and provide those resources to the patient if appropriate Measure: More than 10 percent of all unique patients admitted to the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR reporting period are provided patient-specific education resources Numerator: Number of patients in the denominator who are provided patient-specific education resources Denominator: Number of unique patients admitted to the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) during the EHR reporting period
9 Objective: The eligible hospital or CAH who receives a patient from another setting of care or provider of care or believes an encounter is relevant should perform medication reconciliation Measure: The eligible hospital or CAH performs medication reconciliation for more than 50 percent of transitions of care in which the patient is admitted to the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 or 23) Numerator: Number of transitions of care in the denominator where medication reconciliation was performed

8
# Measure Information Measure Values
Denominator: Number of transitions of care during the EHR reporting period for which the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 to 23) was the receiving party of the transition
10 Objective: The eligible hospital or CAH that transitions their patient to another setting of care or provider of care or refers their patient to another provider of care should provide summary care record for each transition of care or referral Measure: The eligible hospital or CAH that transitions or refers their patient to another setting of care or provider of care provides a summary of care record for more than 50 percent of transitions of care and referrals Numerator: Number of transitions of care and referrals in the denominator where a summary of care record was provided
Denominator: Number of transitions of care and referrals during the EHR reporting period for which the eligible hospital’s or CAH’s inpatient or emergency department (POS 21 to 23) was the transferring or referring provider