women’s health 1 dr pamela sides tuesday 22nd march 2011 dr pamela sides tuesday 22nd march 2011
TRANSCRIPT
Women’s Health 1
Women’s Health 1
Dr Pamela Sides
Tuesday 22nd March 2011
Dr Pamela Sides
Tuesday 22nd March 2011

Aims & PlanAims & Plan• To cover those parts of the curriculum
where you have the greatest needs
• 2.00 introductions and agenda setting
• 2.05 presentation -
pregnancy, menopause & hrt in general practice • 2.30 small groups to discuss cases
• 3.00 discussion about cases
• 3.25 any questions,plenary and feedback
• To cover those parts of the curriculum where you have the greatest needs
• 2.00 introductions and agenda setting
• 2.05 presentation -
pregnancy, menopause & hrt in general practice • 2.30 small groups to discuss cases
• 3.00 discussion about cases
• 3.25 any questions,plenary and feedback

PregnancyPregnancy
• Not covering antenatal care
• Pre conception• Fertility issues• The 1st appointment
• Post natal
• Not covering antenatal care
• Pre conception• Fertility issues• The 1st appointment
• Post natal

Pre Conception Counselling
Pre Conception Counselling
• Life Style• SmokingAlcohol Diet• Advice if under or over weight
• Consider illicit drugs• Consider exposure to harmful
substances in employment
• Life Style• SmokingAlcohol Diet• Advice if under or over weight
• Consider illicit drugs• Consider exposure to harmful
substances in employment

Pre Conception Counselling
Pre Conception Counselling
• Medical
• Regular medication• Mum’s (?Dad’s) medical history• Family history
• Immunisation - rubella, ?varicella, ?? Hep B
• Medical
• Regular medication• Mum’s (?Dad’s) medical history• Family history
• Immunisation - rubella, ?varicella, ?? Hep B

Pre Conception Counselling
Pre Conception Counselling
• Advice
• Folic acid - usually 400 micrograms until 12 weeks
• High risk PRESCRIBE 5mg
• Dietary - vit A, soft cheeses• o/c medication
• Discuss time expected to conceive & when they should return.
• Advice
• Folic acid - usually 400 micrograms until 12 weeks
• High risk PRESCRIBE 5mg
• Dietary - vit A, soft cheeses• o/c medication
• Discuss time expected to conceive & when they should return.

Pre Conception Counselling
Pre Conception Counselling
•ICE
• As if I need to remind you!
•ICE
• As if I need to remind you!

Fertility IssuesFertility Issues
• Ask• How long have they been trying• Previous pregnancies in this relationship or to either partner
• Consider • Health, pmh, medication,smoking, etoh, wt
• Relevant gynae history• Contraception - what & when stopped.• Lmp & menstrual cycle• Frequency of sex• Need to examine - smear, chlamydia, fibroids
• Ask• How long have they been trying• Previous pregnancies in this relationship or to either partner
• Consider • Health, pmh, medication,smoking, etoh, wt
• Relevant gynae history• Contraception - what & when stopped.• Lmp & menstrual cycle• Frequency of sex• Need to examine - smear, chlamydia, fibroids

Fertility IssuesFertility Issues
• Investigations• Her : fbc, tft, 21 day
progesterone?fsh/lh if irregular bleedingprolactin if need to exclude pituitary
problems
Him : semen count
• Investigations• Her : fbc, tft, 21 day
progesterone?fsh/lh if irregular bleedingprolactin if need to exclude pituitary
problems
Him : semen count

Fertility IssuesFertility Issues
• Refer - usually if > 1 year trying
• But also pre-conceptual advice as above.
• Refer - usually if > 1 year trying
• But also pre-conceptual advice as above.


1st Appointment1st Appointment
Back to preconception counselling. Refer to midwife as practice protocol
GOOD NEWS
Let her/them talk.
Yes
Make sure they are able to see someone who is.
No
Are you prepared to discuss the options?
BAD NEWS
Do you need to confirm?
Dr, I think I'm pregnant
Back to preconception counselling. Refer to midwife as practice protocol
GOOD NEWS
Let her/them talk.
Yes
Make sure they are able to see someone who is.
No
Are you prepared to discuss the options?
BAD NEWS
Do you need to confirm?
Dr, I think I'm pregnant
Referral for TerminationReferral for Termination
• Treat as fast track• Are you willing to sign the “blue
form”?
• Try to be up to date with optionseg - medical v surgical
May need a dating scan
• Treat as fast track• Are you willing to sign the “blue
form”?
• Try to be up to date with optionseg - medical v surgical
May need a dating scan


Post NatalPost Natal
• Her experience - the pregnancy,the birth & 1st few weeks
feeding, bleeding, sleeping, coping etc
• How is she? Physically? Emotionally?
• The future -pregnancies/contraception and probably plans for return to work.
• Her experience - the pregnancy,the birth & 1st few weeks
feeding, bleeding, sleeping, coping etc
• How is she? Physically? Emotionally?
• The future -pregnancies/contraception and probably plans for return to work.

Post NatalPost Natal
• ExaminationBP & Wt
? Abdo/pv. Check scar if C section
PV if still bleeding, concern about stitches ORshe wants/expects one.
Only cervical cytology -if it’s due and she’s not likely to return
• ExaminationBP & Wt
? Abdo/pv. Check scar if C section
PV if still bleeding, concern about stitches ORshe wants/expects one.
Only cervical cytology -if it’s due and she’s not likely to return


Menopause - diagnosis and managementMenopause - diagnosis and management
• By definition the menopause is the last period
• The climacteric covers the time leading up to the last period and the months or years afterwards when the woman is symptomatic
• The menopause can only be diagnosed retrospectively
(after 2yrs if <50. After 1 yr if > 50)
• Can we diagnose the climacteric and do we need to?
• By definition the menopause is the last period
• The climacteric covers the time leading up to the last period and the months or years afterwards when the woman is symptomatic
• The menopause can only be diagnosed retrospectively
(after 2yrs if <50. After 1 yr if > 50)
• Can we diagnose the climacteric and do we need to?

Menopause - diagnosisMenopause - diagnosis
• What investigations would you perform?
• Bloods ?hormones - fsh/lhfbc tft fbs lipids
• ?Bone density - in particular if early menopause (<45)
• What investigations would you perform?
• Bloods ?hormones - fsh/lhfbc tft fbs lipids
• ?Bone density - in particular if early menopause (<45)

Menopause - symptomsMenopause - symptoms
• Sweats/flushes• Dry vagina
• Mood changes• Aching joints• Memory loss• etc etc etc
• Sweats/flushes• Dry vagina
• Mood changes• Aching joints• Memory loss• etc etc etc

Menopause - ManagementMenopause - Management
• Reassure and inform. Offer leaflets and/or websites. Cover contraception
• Self help
• Discuss alternative therapies
• Prescribed medication
• Reassure and inform. Offer leaflets and/or websites. Cover contraception
• Self help
• Discuss alternative therapies
• Prescribed medication

Menopause - ManagementMenopause - Management
Self helpwww.menopausematters.co.uknhs directnumerous books
SWEATS - minimised by light clothing and especially consider temperature of bedroom
avoiding stress (!), cutting down alcohol, caffeine and spicy foodsand of course - stop smoking
VAGINAL DRYNESS - lubricants Replens, Senselle and Durex
OSTEOPOROSIS - weight bearing exercise and plenty of dietary calcium
Self helpwww.menopausematters.co.uknhs directnumerous books
SWEATS - minimised by light clothing and especially consider temperature of bedroom
avoiding stress (!), cutting down alcohol, caffeine and spicy foodsand of course - stop smoking
VAGINAL DRYNESS - lubricants Replens, Senselle and Durex
OSTEOPOROSIS - weight bearing exercise and plenty of dietary calcium

Menopause - ManagementMenopause - Management
Alternative Therapies
None are proven to be effective
Remember phytoestrogens may have adverse effects
Patients may have tried :Soya productsRed CloverBlack CohoshEvening PrimroseGinkgo BilobaSt John’s Wart
Alternative Therapies
None are proven to be effective
Remember phytoestrogens may have adverse effects
Patients may have tried :Soya productsRed CloverBlack CohoshEvening PrimroseGinkgo BilobaSt John’s Wart

Menopause - ManagementMenopause - Management
Prescribed Medicationusually for sweats & flushes
HRT
clonidineB blockersanti depressants - particularly ssri & snri? gabapentin
Also osteoporosis
calciumbisphosphonatesstrontium
Prescribed Medicationusually for sweats & flushes
HRT
clonidineB blockersanti depressants - particularly ssri & snri? gabapentin
Also osteoporosis
calciumbisphosphonatesstrontium

Hormone Replacement Therapy
Hormone Replacement Therapy
• Minimum dose
• Shortest time
• At least annual review
• Minimum dose
• Shortest time
• At least annual review

HRTHRT• Has she got a uterus?
If not : oestrogen only(caution if the hysterectomy was for endometriosis)
If she has : Oestrogen & progestagen
• Is she clearly > 1 yr post menopausalIf not : will need cyclical bleed (double script charge)
•If she is : probably try bleed free
• Oral? Patches? Gel? Vaginal?
• Has she got a uterus?If not : oestrogen only(caution if the hysterectomy was for endometriosis)
If she has : Oestrogen & progestagen
• Is she clearly > 1 yr post menopausalIf not : will need cyclical bleed (double script charge)
•If she is : probably try bleed free
• Oral? Patches? Gel? Vaginal?

HRTHRT
• Lots to choose from
• Appears confusing
• Get familiar with one preparation for each scenario
• If the 1st doesn’t work - change the progestogen
• cks.nhs.uk/menopause lists preparations & costs
• What follows is MY table - not necessarily a recommendation.
• Lots to choose from
• Appears confusing
• Get familiar with one preparation for each scenario
• If the 1st doesn’t work - change the progestogen
• cks.nhs.uk/menopause lists preparations & costs
• What follows is MY table - not necessarily a recommendation.

Pamela’s tableEstradiolPamela’s tableEstradiol
Progestogen ORAL Patches
Periods Bleed free
Oestogen only
Periods Bleed free Oestogen only
Norethisterone
Elleste duet1mg & 2mg
Elleste duet conti2mg(Kliovance)1mg
Elleste Solo1mg & 2mg
Evorel Sequi
Evorel conti
Evorel
Levonorgestrel
Nuvelle2mg
Climaval 1mg & 2mg
FemSeven Sequi
FemSeven Conti
Elleste solo MX
Dydrogesterone
Femoston1mg & 2mg
Femoston conti1mg
Zumenon1mg & 2mg
Femapak(patches & tablets)
FemSeven
Drospirenone Angeliq
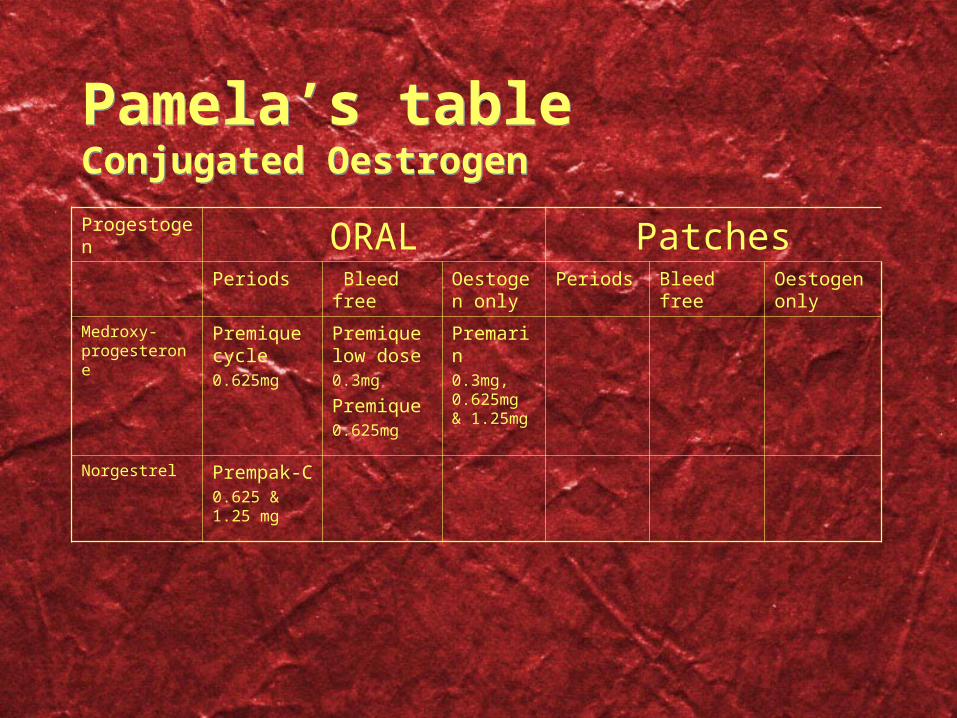
Pamela’s tableConjugated OestrogenPamela’s tableConjugated Oestrogen
Progestogen ORAL Patches
Periods Bleed free
Oestogen only
Periods Bleed free Oestogen only
Medroxy-progesterone
Premique cycle0.625mg
Premique low dose0.3mg
Premique0.625mg
Premarin0.3mg, 0.625mg & 1.25mg
Norgestrel Prempak-C0.625 & 1.25 mg

HRTother systemic preparationsHRTother systemic preparations
• Cyclo-progynova - tablet free week = flushes come back
• Tridestra - quarterly bleed
• Trisequens - lower level oestogen week 4
• Tibolone (Livial) - oestrogenic & progestogenic with weak androgenic activity. May improve libido.
• Oestrogel - apply measures of gel to arms or thighs. Oestrogen only
• Mirena coil - can be used to supply continuous progestogen.Needs changing after 4 years (not 5 as when contraceptive)
• Cyclo-progynova - tablet free week = flushes come back
• Tridestra - quarterly bleed
• Trisequens - lower level oestogen week 4
• Tibolone (Livial) - oestrogenic & progestogenic with weak androgenic activity. May improve libido.
• Oestrogel - apply measures of gel to arms or thighs. Oestrogen only
• Mirena coil - can be used to supply continuous progestogen.Needs changing after 4 years (not 5 as when contraceptive)

HRTlocal preparationsHRTlocal preparations
• Ostrogen only• RingPessary Cream Tablets• Estring -replace every 3 months. Max 2 years
• Ortho-gynest pessary or cream - daily then weekly
• Ovestin cream - daily then weekly
• Vagifem - daily then twice weekly
• Premarin - daily for 3 weeks, then week without
• All except ring need review at 3 - 6 months• Minimal absorption - but consider progestagen challenge
• Ostrogen only• RingPessary Cream Tablets• Estring -replace every 3 months. Max 2 years
• Ortho-gynest pessary or cream - daily then weekly
• Ovestin cream - daily then weekly
• Vagifem - daily then twice weekly
• Premarin - daily for 3 weeks, then week without
• All except ring need review at 3 - 6 months• Minimal absorption - but consider progestagen challenge

Menopause - ManagementMenopause - Management
Clonidine25 microgram tabs 2 bd, increasing to 3 bd
drowsiness, dry mouth, dizziness, nausea, sleeplessness.
Caution with pvd and depression
B blockersmay be worth trying if likely to be other benefits (^BP, anxiety)
SSRI & NSRIvenlafaxine at low dose or other ssri’s
Gabapentinusually start at 300 mg and increase dose slowly
Clonidine25 microgram tabs 2 bd, increasing to 3 bd
drowsiness, dry mouth, dizziness, nausea, sleeplessness.
Caution with pvd and depression
B blockersmay be worth trying if likely to be other benefits (^BP, anxiety)
SSRI & NSRIvenlafaxine at low dose or other ssri’s
Gabapentinusually start at 300 mg and increase dose slowly

• Any questions about the menopause or HRT?
• Any questions about the menopause or HRT?


Case 1Case 1
• Miss SG is aged 17 and attends complaining that she been bleeding for 5 weeks.
• She wants to start depo provera for contraception.
• She stopped microgynon 30 (coc) 3 months ago.• She had a normal withdrawal bleed, and then a period one month later.
• a) What would you cover in this consultation?• b) Would you request any investigations?• c) How would you manage her bleeding?• d) Can she have depo?
• Miss SG is aged 17 and attends complaining that she been bleeding for 5 weeks.
• She wants to start depo provera for contraception.
• She stopped microgynon 30 (coc) 3 months ago.• She had a normal withdrawal bleed, and then a period one month later.
• a) What would you cover in this consultation?• b) Would you request any investigations?• c) How would you manage her bleeding?• d) Can she have depo?

Case 2Case 2
• Mrs ST is aged 50 and complains her periods “are all over the place”
• She had a regular cycle (5-7/26) until about 1 yr ago.• This year her periods have been infrequent and very
heavy - described as “flooding”• She’s about to go away for a special holiday.
• a) Do you need any further information from her?• b) Would you carry out any investigations?• c) Can you help her for her holiday?
• Mrs ST is aged 50 and complains her periods “are all over the place”
• She had a regular cycle (5-7/26) until about 1 yr ago.• This year her periods have been infrequent and very
heavy - described as “flooding”• She’s about to go away for a special holiday.
• a) Do you need any further information from her?• b) Would you carry out any investigations?• c) Can you help her for her holiday?

Case 1Case 1
• a) full menstrual & sexual history. Risk of pregnancy. Any imb/pcb?
• b) probably fbc & pregnancy test
• c) norethisterone 5mg tds until bleeding stops
• d) I would prefer her to have 3 months of regular periods 1st.
• a) full menstrual & sexual history. Risk of pregnancy. Any imb/pcb?
• b) probably fbc & pregnancy test
• c) norethisterone 5mg tds until bleeding stops
• d) I would prefer her to have 3 months of regular periods 1st.

Case 2Case 2
• a) full menstrual history - in particular asking about imb/pcb
• b) probably examine her. CS if due. Bloodsmight need USG - depending on findings
• c) norethisterone 5mg tds starting 3 days before she goes, and continuing until she’s prepared to bleed.
• a) full menstrual history - in particular asking about imb/pcb
• b) probably examine her. CS if due. Bloodsmight need USG - depending on findings
• c) norethisterone 5mg tds starting 3 days before she goes, and continuing until she’s prepared to bleed.

Management of Menorrhagia
Management of Menorrhagia
reassure nsaid
tranexamic acid
(cyklokapron)500mgx2 tdswhile bleeding
etamsylate
(dicynene)500mg qdswhile bleeding
haemostatics
oralcoc
progestagens
systemicmirenadepo
hormones
investigate/examine
Primary Care
hormones endometrial ablation hysterectomy
investigate/examine
Secondary Care
Menorrhagia
reassure nsaid
tranexamic acid
(cyklokapron)500mgx2 tdswhile bleeding
etamsylate
(dicynene)500mg qdswhile bleeding
haemostatics
oralcoc
progestagens
systemicmirenadepo
hormones
investigate/examine
Primary Care
hormones endometrial ablation hysterectomy
investigate/examine
Secondary Care
Menorrhagia
Case 3Case 3
• Mrs LV is aged 44 and attends to report her last period was about 11 months ago. She has a high powered job which is being affected by her sweats and irritability. She comments that she’s not sleeping well, and is uncharacteristically weepy. Her question is “how far through the menopause am I?”
• a) what else do you need to know?• b) what investigations would you perform?• c) how would you answer her question?
• You can assume investigations suggest she is menopausal.
• d) how would you manager her?
• Mrs LV is aged 44 and attends to report her last period was about 11 months ago. She has a high powered job which is being affected by her sweats and irritability. She comments that she’s not sleeping well, and is uncharacteristically weepy. Her question is “how far through the menopause am I?”
• a) what else do you need to know?• b) what investigations would you perform?• c) how would you answer her question?
• You can assume investigations suggest she is menopausal.
• d) how would you manager her?

Case 3Case 3
• a) full medical & gynae history - including use of contraception
• b) PREGNANCY TEST plus bloods
• c) Impossible!
• d) she hasn’t come back - but I would be willing to prescribe HRT.
• Her bone density was fine in 2007.• Incidentally her cholesterol was >8 - so she will be chased
up.
• a) full medical & gynae history - including use of contraception
• b) PREGNANCY TEST plus bloods
• c) Impossible!
• d) she hasn’t come back - but I would be willing to prescribe HRT.
• Her bone density was fine in 2007.• Incidentally her cholesterol was >8 - so she will be chased
up.

Case 4Case 4
• Ms KS is aged 56. HRT was started 4 years ago when she hadn’t had a period for 6 months and was she was being disturbed by sweats/flushes.
• Elleste Duet 1mg has been prescribed with good symptom relief and cycle control.
• She had vv surgery 2 years ago - hrt was stopped pre op with recurrence of her sweats.
• She’s now keen to stop HRT because she’s concerned about the long term risks.
• a) How would you advise her?
• Ms KS is aged 56. HRT was started 4 years ago when she hadn’t had a period for 6 months and was she was being disturbed by sweats/flushes.
• Elleste Duet 1mg has been prescribed with good symptom relief and cycle control.
• She had vv surgery 2 years ago - hrt was stopped pre op with recurrence of her sweats.
• She’s now keen to stop HRT because she’s concerned about the long term risks.
• a) How would you advise her?

Case 4Case 4
• She’s already on a low dose preparation
• Prescribe oestrogen only - alternate days, then every 3rd day and slowly tailing off.
• Progestagen challenge at least 3 monthly.
• She’s already on a low dose preparation
• Prescribe oestrogen only - alternate days, then every 3rd day and slowly tailing off.
• Progestagen challenge at least 3 monthly.

Case 4Case 4Stopping HRTAdvise then to come off slowlyStep 1 move stepwise to lowest dose
Step 2 prescribe unopposed oestrogenadvise reducing frequency of tabletsor spacing patch changes further apart
They must report any unexpected bleedingChallenge with progestagen at least quarterlyClimanor 5mg (medroxyprogesterone) 2 daily 14 days (£3.27)
ORUtrogestran 200mg (progesterone) 1 daily 12 - 14 days (£5.70)
Think again if it takes longer than 6 months
Stopping HRTAdvise then to come off slowlyStep 1 move stepwise to lowest dose
Step 2 prescribe unopposed oestrogenadvise reducing frequency of tabletsor spacing patch changes further apart
They must report any unexpected bleedingChallenge with progestagen at least quarterlyClimanor 5mg (medroxyprogesterone) 2 daily 14 days (£3.27)
ORUtrogestran 200mg (progesterone) 1 daily 12 - 14 days (£5.70)
Think again if it takes longer than 6 months

Case 5Case 5
• Mrs JW is aged 65 and comes (with her husband) complaining about flushing++. She’s waking 7 or 8 times every night.
• HRT was prescribed in her early 50’s - and her memory is that it was wonderful. Review of her records shows she had to try several preparations (prempak, estracombi, tibolone & elleste).
• Breast cancer was diagnosed at routine mammography in 2005. She has responded well to treatment and has no evidence of metastatic disease. She is not currently taking any medication.
• a) what are her options?
• Mrs JW is aged 65 and comes (with her husband) complaining about flushing++. She’s waking 7 or 8 times every night.
• HRT was prescribed in her early 50’s - and her memory is that it was wonderful. Review of her records shows she had to try several preparations (prempak, estracombi, tibolone & elleste).
• Breast cancer was diagnosed at routine mammography in 2005. She has responded well to treatment and has no evidence of metastatic disease. She is not currently taking any medication.
• a) what are her options?

Case 5Case 5
• She agrees that re-starting HRT is not an option. Self help etc have not improved her symptoms.
• B blocker - no effect• Clonidine - some improvement, but abdo pain &
diarrhoea• Venlafaxine - “15% improvement” but she
doesn’t think the benefit outweighs the disadvantages of taking an antidepressant.
• What next?!!!!
• She agrees that re-starting HRT is not an option. Self help etc have not improved her symptoms.
• B blocker - no effect• Clonidine - some improvement, but abdo pain &
diarrhoea• Venlafaxine - “15% improvement” but she
doesn’t think the benefit outweighs the disadvantages of taking an antidepressant.
• What next?!!!!
Case 6Case 6
• Mrs PS is aged 75 and attends to report “bleeding down below”.
• She was last seen complaining about vaginal discomfort about a month previously, but had no bleeding at that time. She was thought to have either thrush or senile vaginitis. A swab was negative.
• Pmh - breast Ca 10 yrs previously, followed by tamoxifen for 5 years.
• a) how would you manage her?• b) what is the likely diagnosis?
• Mrs PS is aged 75 and attends to report “bleeding down below”.
• She was last seen complaining about vaginal discomfort about a month previously, but had no bleeding at that time. She was thought to have either thrush or senile vaginitis. A swab was negative.
• Pmh - breast Ca 10 yrs previously, followed by tamoxifen for 5 years.
• a) how would you manage her?• b) what is the likely diagnosis?

Case 6Case 6
• a) examine her - blood clearly coming from cervical osfast track referral - which would have been indicated even if the blood hadn’t been seen
• b) senile vaginitis v endometrial ca
• Actually had a large benign endometrial polyp.
• a) examine her - blood clearly coming from cervical osfast track referral - which would have been indicated even if the blood hadn’t been seen
• b) senile vaginitis v endometrial ca
• Actually had a large benign endometrial polyp.


Psychosexual ProblemsWhat & Who?
Psychosexual ProblemsWhat & Who?
• What• Reduced libido• Differing levels of desire• Failure to reach orgasm• Pain
• Who• New mums• Perimenopausal• Teenagers - unlikely to be their initial complaint except pain
• ?Widows
• What• Reduced libido• Differing levels of desire• Failure to reach orgasm• Pain
• Who• New mums• Perimenopausal• Teenagers - unlikely to be their initial complaint except pain
• ?Widows

Psychosexual ProblemsHow can you help in 10 minutesPsychosexual ProblemsHow can you help in 10 minutes
• Listen• Possibly examine - mainly for pain• Reassure • Provide information• Recommend self help• Be prepared to discuss medication• Refer
• Listen• Possibly examine - mainly for pain• Reassure • Provide information• Recommend self help• Be prepared to discuss medication• Refer

Psychosexual ProblemsSelf Help & Referral
Psychosexual ProblemsSelf Help & Referral
• Teenage magazines
• Healthy Sex Miriam Stoppard• Treat Yourself to Sex Brown & Faulder• Relate Guide to Sex Litvinoff
• Vaginal lubricants - Replens Sylk Durex
• relate.org.uk
• Refer to Relate
• Teenage magazines
• Healthy Sex Miriam Stoppard• Treat Yourself to Sex Brown & Faulder• Relate Guide to Sex Litvinoff
• Vaginal lubricants - Replens Sylk Durex
• relate.org.uk
• Refer to Relate

Psychosexual ProblemsPrescribing
Psychosexual ProblemsPrescribing
• Viagra etc - not licensed for women
• Livial
• Testosterone patch = Intrinsaonly in women who have had total hysterectomy
• Vaginal oestrogens for atrophic vaginitis
• Viagra etc - not licensed for women
• Livial
• Testosterone patch = Intrinsaonly in women who have had total hysterectomy
• Vaginal oestrogens for atrophic vaginitis