william j. ennis do,mba professor of clinical surgery chief … · william j. ennis do,mba ....
TRANSCRIPT

William J. Ennis DO,MBA Professor of Clinical Surgery
Chief Section Wound Healing and Tissue Repair University of Illinois Hospital and Health Sciences
System

I am speaking to you as an independent physician, no entity paid for my travel and I will not receive an honorarium for my presentation
Full time employed Professor of Surgery at the University of Illinois Hospital and Health Sciences System
I am currently not on any industry scientific advisory board or speaker’s bureau
I am a consultant to Accelecare wound centers, a management company in Bellevue WA

Field of wound care
1962, 1978, 1982, 1998

The Scope of the Problem
• 14 billion dollar global industry • US 2 billion dollar market, with a CAGR of 10% between
2010 and 2017 • 20% US population > 65 in 2020
– Elderly have more chronic disease states – Increased venous ulcerations – Increased peripheral arterial disease, amputations,
stroke, MI etc. • 8% US diabetic, 15% develop a diabetic foot ulcer • 67% US population is overweight • Increases in surgical procedures
The Scope of the problem • Chronic wounds lead to lost days of work,
decreased quality of life, depression • Acute wounds with substandard treatment can
transition into chronic wounds • Complications from surgical wounds can lead to
increased length of stay, higher healthcare costs and readmissions
• Pressure ulcers can impact the most vulnerable populations, the elderly and spinal cord injured patients

CER
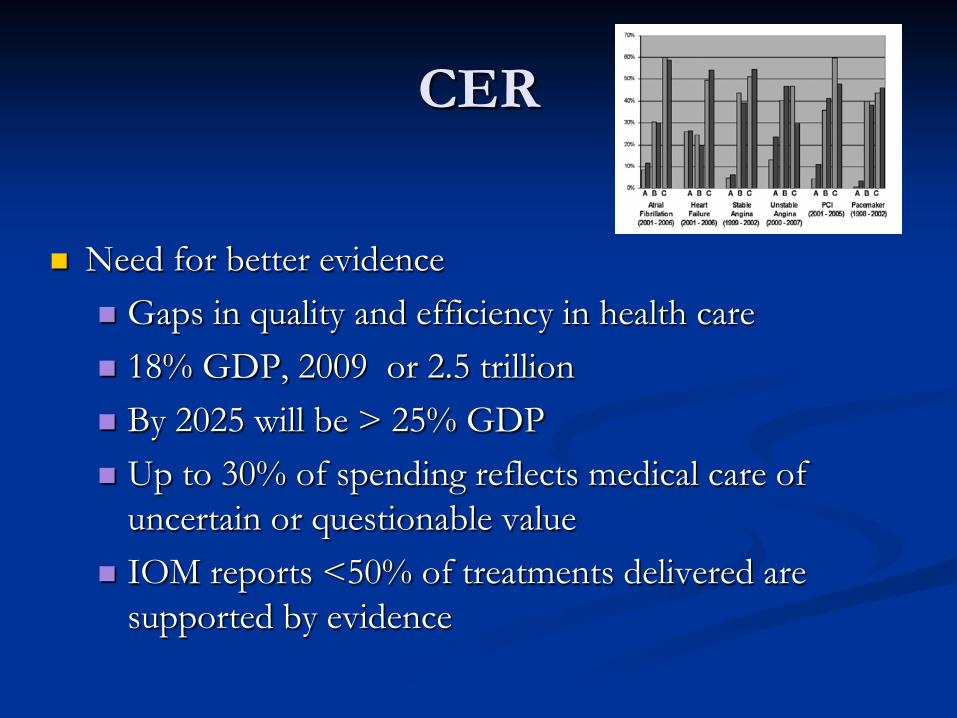
Need for better evidence Gaps in quality and efficiency in health care 18% GDP, 2009 or 2.5 trillion By 2025 will be > 25% GDP Up to 30% of spending reflects medical care of
uncertain or questionable value IOM reports <50% of treatments delivered are
supported by evidence

Wound care is Unique? Is it?
• Treatments take a long time • Treatments can span sites of care • Not all patients can be cured/healed • Access to care can be compromised • Nutritional issues • Psychological impact of disease on patient
and care providers • Costly therapy

Wound care is Unique? Is it? • Complex group of patients with a highly
prevalent condition that has a large economic impact on the healthcare industry
• Innovation can be slow based on regulatory pathways, product adoption, poorly defined endpoints,
• Clinical situations often require clinicians to use multiple agents at the same time or in sequence despite research based on each treatment utilized as a stand alone therapy

The last two slides could be used in a presentation
focused on
Oncology, Transplantation, Connective tissue disorders,
Spinal cord injury, etc.

Wound Care Patients
• Medically complex but unlike most other medical conditions, the wound is a manifestation of a collection of underlying co-morbid conditions. This potentially confounds the treatment directed at the wound surface and complicates research.
• Currently treatments are currently regulated based on their impact on complete healing
• A cancerous lesion might be treated with neo-adjuvant chemo to shrink the mass, followed by surgical excision, followed by radiation therapy
• Each therapeutic step would be assessed on its ability to achieve the desired outcome

Wound Care Patients • Standard of care
– Has been decided in wound care but wide variation exists within each subcategory
• Debridement- High powered venturi effect water based removal of full thickness slough is a debridement, use of a sterile 2mm curette is a debridement.
• Offloading, Moist environment, bioburden control, – Oncology- removal of colon and harvesting
nodes is fairly uniform – Need to agree upon SOC in all trials


Donaldson BMJ 2002
1 2 3
A ?
B
C ?
Declining effectiveness
Increasing cost
Problem Between 1999-2006 32/46 studies with economic outcomes ended up with results in box C1 So recommendations to approve due to increasing cost effectiveness but leads to overall increase in cost Problems with allocative efficiency

Can we predict who will heal? • How long should it take • What treatments should we use • In what order / In what setting • If they heal will it stay healed • Will/Can the patient adhere to protocol • What are the goals and objectives of the
patient and do they have access • Centers of Excellence • Economic alignment for total episode of
care

2008 Third Congress of the World Union of Wound Healing Societies, Toronto, Canada
Site of Care Outcomes Table 1. The Overall Healing Rate and the Mean and Median Time to Healing from
Two Sources Communit
y Hospital-Based Outpatient Clinic*
Tertiary care Hospital Outpatient Clinic
Number of Wounds 303 344 Wounds Healed 225 (74%) 252 (73%) Kaplan Meier derived mean time to healing 14± 1 12 ± 1
Kaplan Meier derived median time to healing 9 ± 1 9 ± 1
*Ref Ennis et al Ostomy/Wound Management 1998;44(11):22-39

CONSISTENCY

1995-1998 436 Patients / 580 Wounds Screened
-At Risk Population
2006-2009 1077 Patients / 2515 Wounds
Screened -At Risk Population
Consult Only 102 patients with 114 wounds
Active at Trial End 24 / 36
Consult Only 266 patients with 652 wounds
Active at Trial End 46 / 75
Study Population ITT 310 Patients / 431 Wounds (71.1%, 74.3% of screened)
Study Population ITT 763 Patients / 1788 Wounds (70.8%, 71.1% of screened)
Completely Healed Wounds 319 / 431 (74%)
Completely Healed Wounds 1388 / 1788 (77.6%)
Patients in which all wounds healed 214 / 310 (69%)
Patients in which all wounds healed 519 / 763 (68%)
Outcomes Single Hospital based outpatient wound clinic
(Patients / Wounds)
Reproducible over time


Issue # wound
Total wound
Total wound healed
% healed
NA 2515 1388 55.2
Active at completion 75 2440 1388 56.9
Consult only 652 1788 1388 77.6
d/c cv,fp,im,surg,plastic 42 1746 1388 79.5
Died 21 1725 1388 80.5
Lost to nh,another facility 48 1677 1388 82.8
Lost to f/u 82 1595 1388 87.0
Moved 4 1591 1388 87.2
Pt request 3 1588 1388 87.4

Solutions? • Think about the trial designs required for wound care
technologies of the near future – Registries, SOC, Use product/technology to achieve
specific physiological endpoints – Cell therapy, gene therapy, small molecular weight
proteins, systemic pharma based therapy, scaffoldings with active cytokines etc.
• Think about quality of healing, how important is total healing if it only lasts for 3 weeks?
• Non invasive diagnostic methods to assess quality of healing need to be developed
• Consider patient focused outcomes and include patient input in trial design of future innovations

Quality
Cost
Innovation
Access
Competing Paradigms



William J Ennis DO,MBA
Professor Clinical Surgery, Chief Section Wound Healing and Tissue Repair
University of Illinois Hospital and Health Sciences System
WHAT THE PATIENT SAYS ABOUT PATIENT CENTERED OUTCOMES SUMMIT JULY 25TH, 2012

PATIENT CENTERED OUTCOMES SUMMIT
