wie ich mit prostatakrebs umgehe stephen b. strum, md, facp medical oncologist stuttgart, germany...
TRANSCRIPT

Wie ich mit Prostatakrebs umgeheStephen B. Strum, MD, FACP
Medical Oncologist
Stuttgart, Germany11.05.2009

Active Objectified Surveillance & Other Strategies
Active Objectified Surveillance
• Patients with “insignificant” PC based on set clinical & pathological criteria
• Patients with significant age & co-morbidity factors
• Patients able to be monitored over time
• Determine thresholds relating to treatment intervention
• Patients who are reclassified as higher risk can be treated with cure
• Reduce psychological stress of living with untreated cancer

“Insignificant” Prostate Cancer
•Gleason score 6 or less•PSA 10 or less•Clinical stage T2a or less•Free to total PSA percent > 15%•Less than 3 cores involved•50% or less of any one core with
PC•PSA doubling time > 3 years

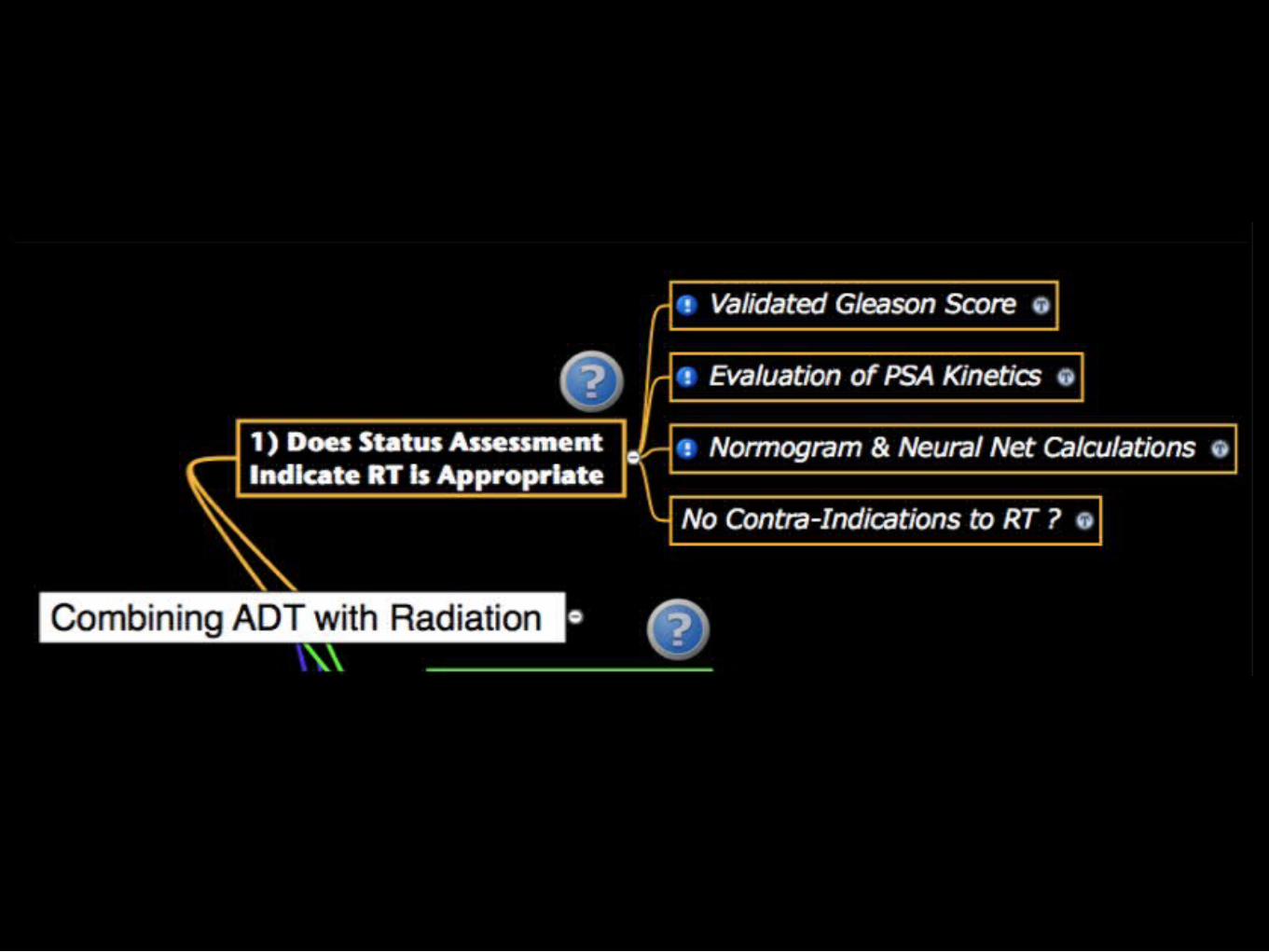
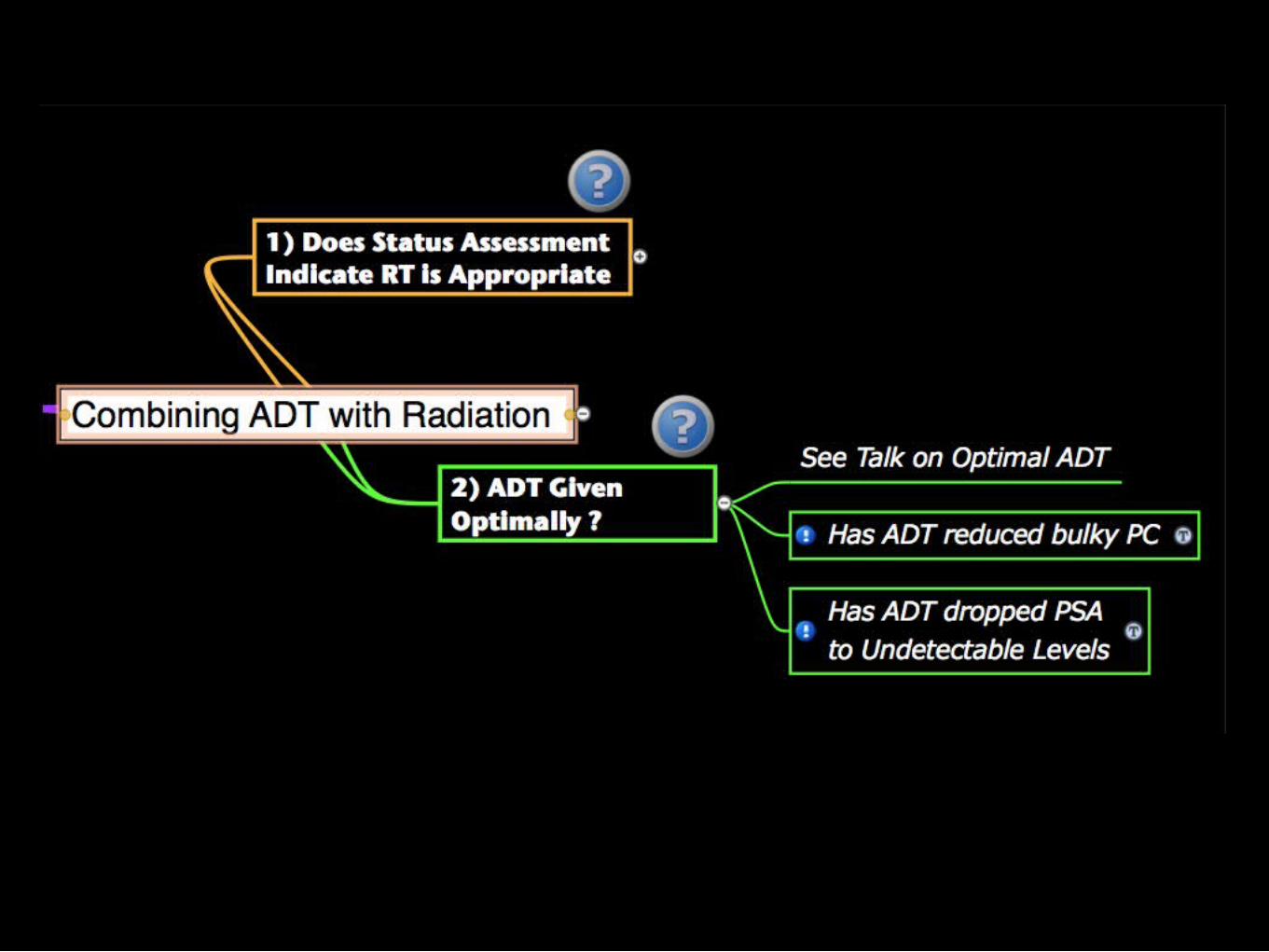
AOS (active objectified surveillance): Key Role of Status

7

Importance of Milieu in PC BehaviorA Key Ingredient in any Active Surveillance Strategy
Klotz L: Active surveillance with selective delayed intervention is the way to manage 'good-risk' prostate cancer. Nat Clin Pract Urol 2:136-42; 2005.
1.Study begun in 1995 involving 299 patients
2.Median PSADT 7 yrs with 42% having DT > 10 yrs
3.At 8 yrs, overall actuarial survival 85% with PC-specific survival of 99%
Key Findings


Optimal ADT (androgen deprivation therapy)
6 Ways to Optimize ADT
1) Block androgen access to the PC cell
2) Ensure significant lowering of Testosterone
3) Measure testosterone using accurate lab assay
4) Use US-PSA as biologic endpoint for ADT
5) Use measures that down-regulate (dR) sensitivity of the androgen receptor (AR)
6) Block bone-derived growth factors that are released due to excessive osteoclast activity (induced by androgen deprivation)


15

16

Are We Using the Optima Dose of Dutasteride ?
Dr. Mostaghel's group looked for gene changes in 75 men with localized PC. Twenty-five had
RP alone, 26 were given neoadjuvant dutasteride at 0.5 mg, and the remaining 24
received dutasteride, 3.5 mg orally per day for 4 months prior to RP.

ADT is about Androgen Availability
Huggins won Nobel Prize 43 years ago showing PC dependence on Androgens.
Testosterone assays inaccurate at low T levels: need to use LC/MS/MS based assays.
• PC growth is mediated by androgens.
• We call it Androgen Dependent PC (ADPC) or Androgen Independent PC (AIPC) or Castration Resistant PC (CRPC) but PC growth is androgen related.
• PC mets even synthesize their own androgens.
• Testosterone level (T) is a key Biological End Point.
• T not measured in 95% of men with PC.
• “Castration” threshold should be < 20 ng/dl.
• Further lowering of T may enhance response.
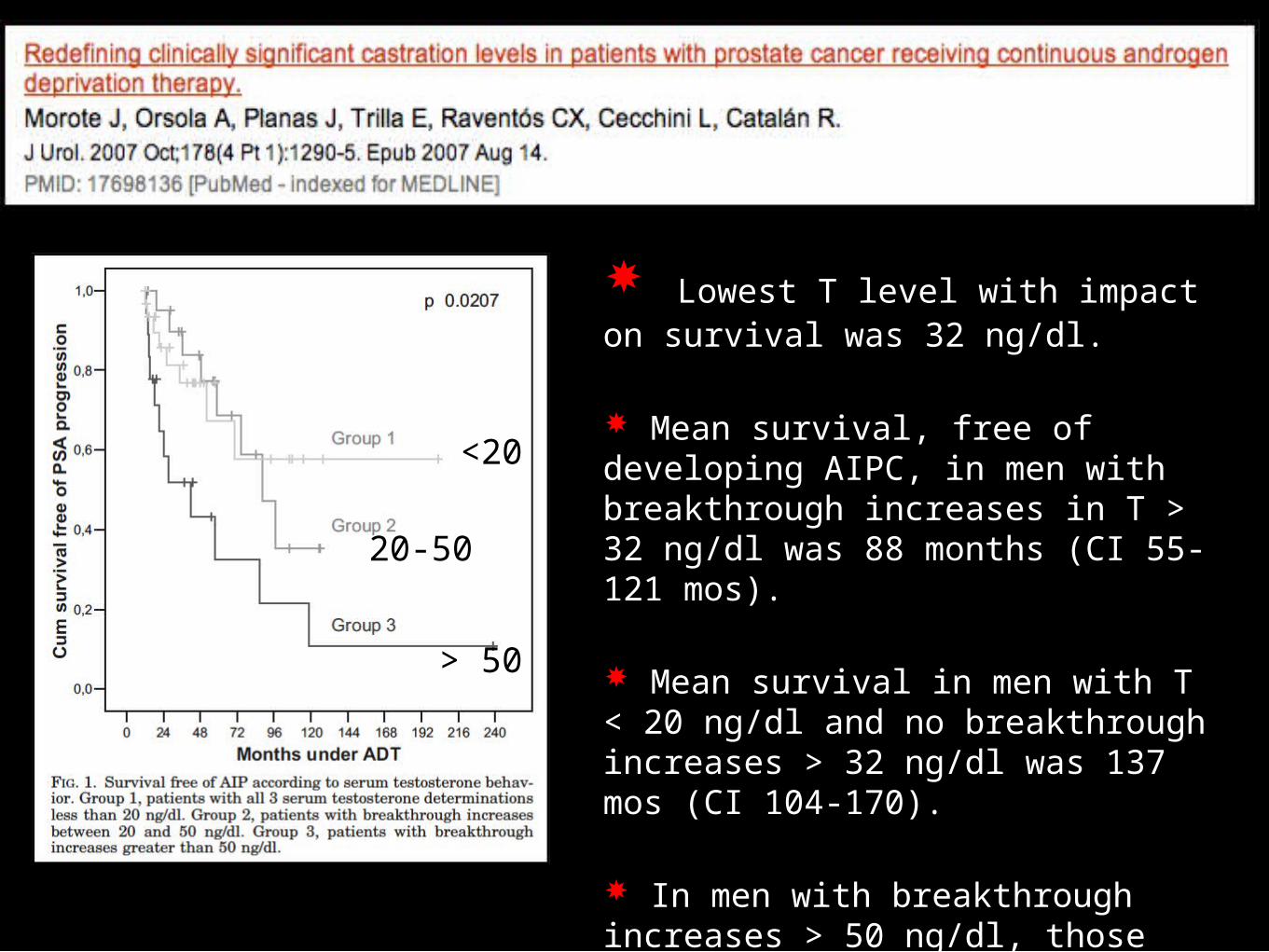
Lowest T level with impact on survival was 32 ng/dl.
Mean survival, free of developing AIPC, in men with breakthrough increases in T > 32 ng/dl was 88 months (CI 55-121 mos).
Mean survival in men with T < 20 ng/dl and no breakthrough increases > 32 ng/dl was 137 mos (CI 104-170).
In men with breakthrough increases > 50 ng/dl, those men with maximal ADT had a significantly longer survival free of AIPC.
<20
20-50
> 50
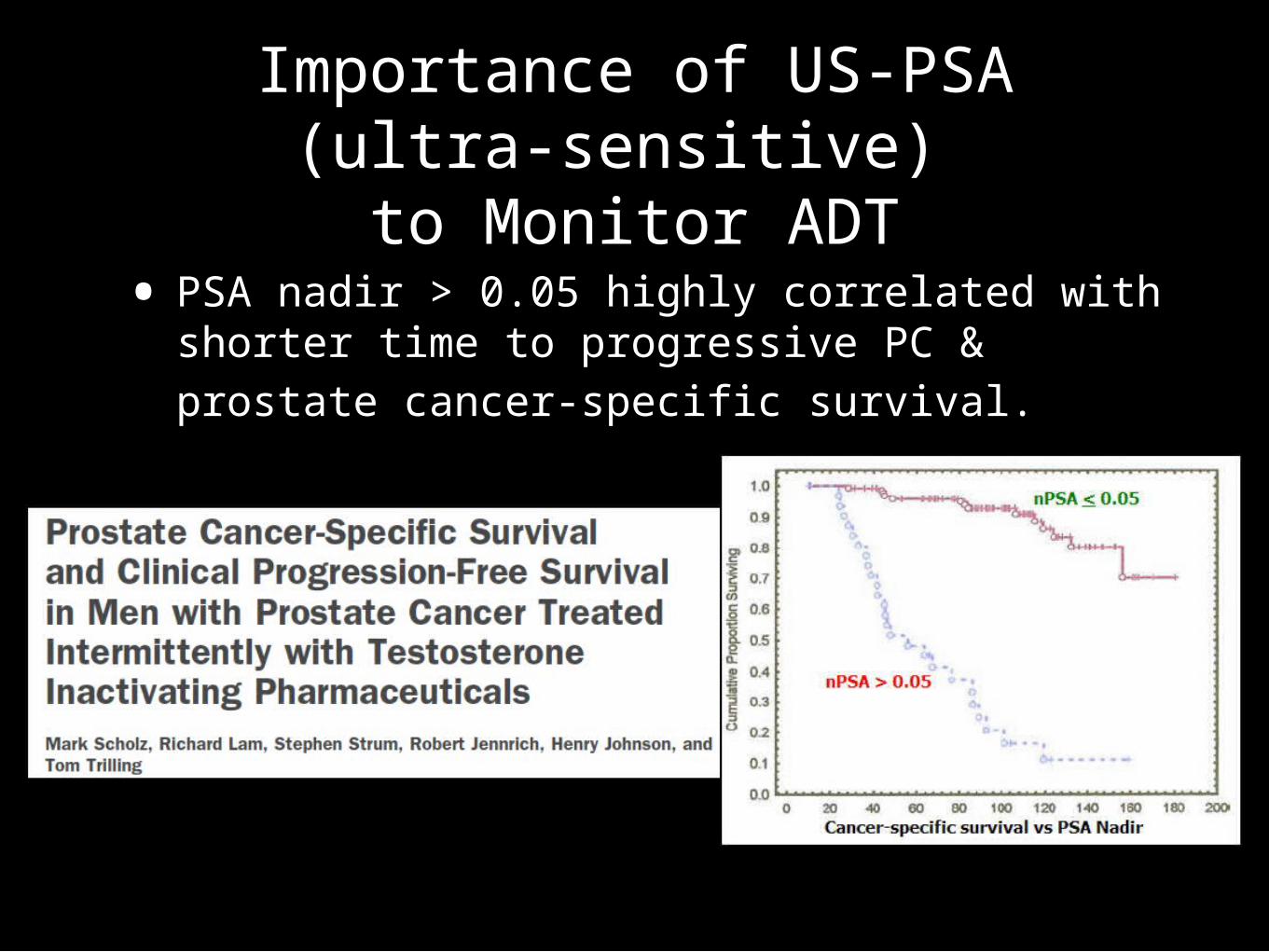
Importance of US-PSA (ultra-sensitive)
to Monitor ADT• PSA nadir > 0.05 highly correlated with
shorter time to progressive PC & prostate cancer-specific survival.
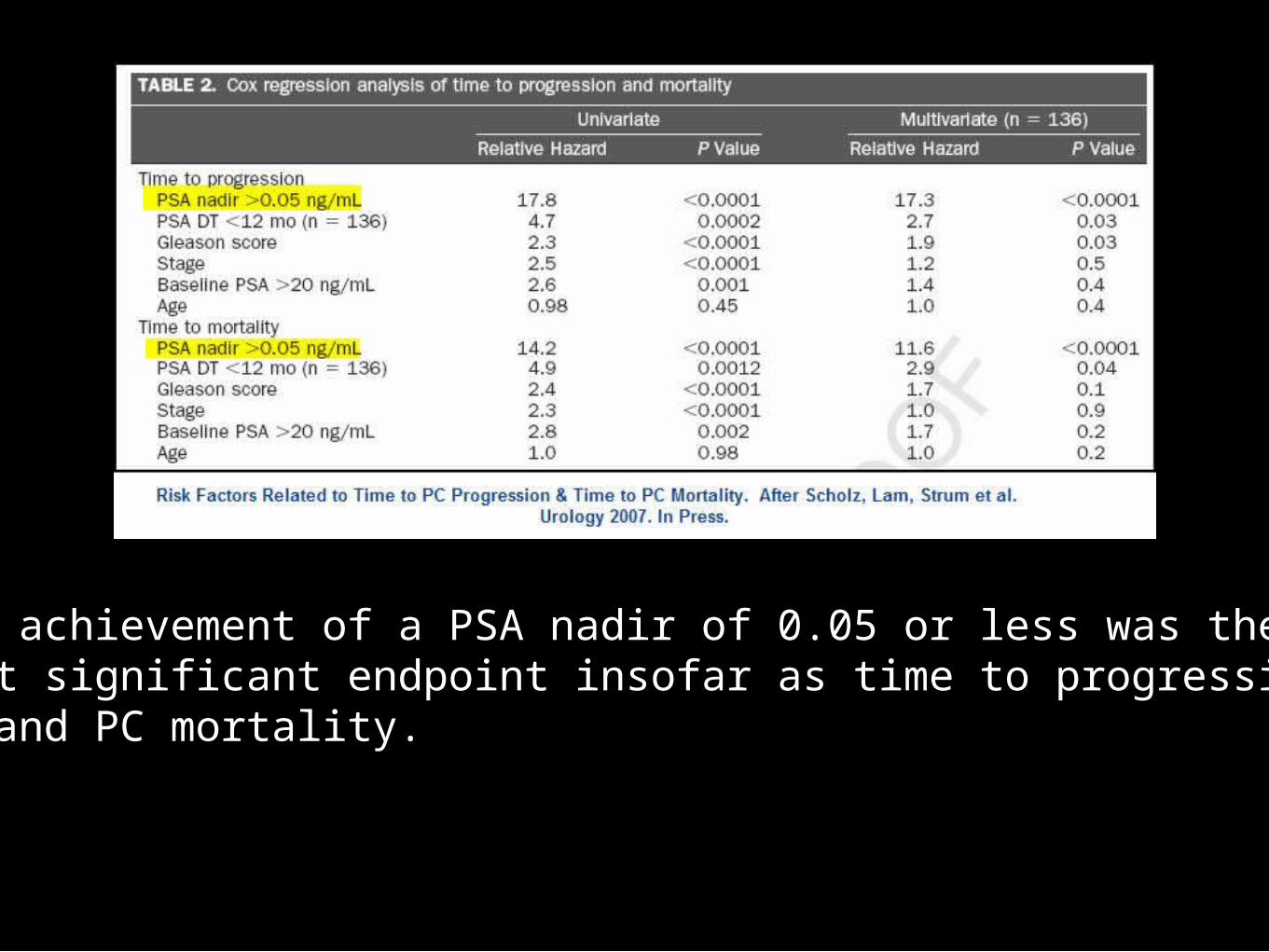
The achievement of a PSA nadir of 0.05 or less was the most significant endpoint insofar as time to progressivePC and PC mortality.

Androgen Receptor (AR) Related Dysfunction
• (1) Reduce AR sensitivity
• Prolactin Inhibitors
• 5AR inhibitors
• EGCG
• HSP inhibitors
• PPAR-G ligands
• DIM & POMx
• Silymarin
• Melatonin
• (2) Avoid Drugs Stimulating “Promiscuous” AR
• Avoid or use cautiously standard glucocorticoids such as prednisone & dexamethasone
• Use triamcinolone instead e.g. HDK with triamcinolone instead of Hydrocortisone (HC)
Androgen Receptor (AR) Related Dysfunction
• (3) Evaluate for ARM (androgen receptor mutation)– see http://www.prostate-cancer.org/education/andeprv/Strum_IADT.html
• Withdraw anti-androgen, progestin, estrogen to see if PSA or other marker is reduced.
• If possible ARM due to Casodex need 6 weeks to eliminate Casodex (bicalutamide) from body.
• (4) Avoid agents that stimulate ARM
• Steroidal anti-androgens such as CPA (cyproterone acetate)
• Progestins, in certain contexts.

•Androgen Deprivation Therapy (ADT) immediately induces bone resorption
• Orchiectomy Orchiectomy
• LHRH agonists (Lupron, Zoladex) LHRH agonists (Lupron, Zoladex)
• LHRH antagonists (Plenaxis)LHRH antagonists (Plenaxis)
• Anti-androgens, Ketoconazole, EstrogensAnti-androgens, Ketoconazole, Estrogens
• Androgen Receptor AntagonistsAndrogen Receptor Antagonists
Clarke NW, McClure J, & George NJR: The effects of orchidectomy on skeletal metabolism in metastatic prostate
cancer. Scand J Urol Nephrol 27: 475-483, 1993.

Lowering of Testosterone Lowering of Testosterone removesremoves an osteoclast an osteoclast inhibitor.inhibitor.
ADT (androgen deprivation ADT (androgen deprivation therapy) lowers Testosterone.therapy) lowers Testosterone.
Increased osteoclast function Increased osteoclast function leads to net bone loss due to leads to net bone loss due to excessive resorption.excessive resorption.
Testosterone Inhibits Osteoclast FormationTestosterone Inhibits Osteoclast Formation
Chen Q, Kaji H, Sugimoto T, et al: Chen Q, Kaji H, Sugimoto T, et al: Testosterone inhibits osteoclast formation Testosterone inhibits osteoclast formation stimulated by parathyroid hormone stimulated by parathyroid hormone through androgen receptor. FEBS Lett through androgen receptor. FEBS Lett 491:91-3, 2001. 491:91-3, 2001.
Graphic per Strum, A Primer on PC
All of Biology is a Two Edged Sword
• Part of optimizing ADT is recognition of the above statement.
• We need to start therapies to minimize the down-sides of any treatment we use, including ADT.
• A key focus should be to prevent osteoclast activation with release of bone-derived growth factors.
• Agents like bisphoshonates & Denosumab should be used early in the treatment of men with PC.

Monoclonal antibody to Receptor Activator of Nuclear Kappa Ligand (RANKL) Stops Bone Resorption & Decreases Skeletal-Related Events Better then Aredia or Zometa.
27
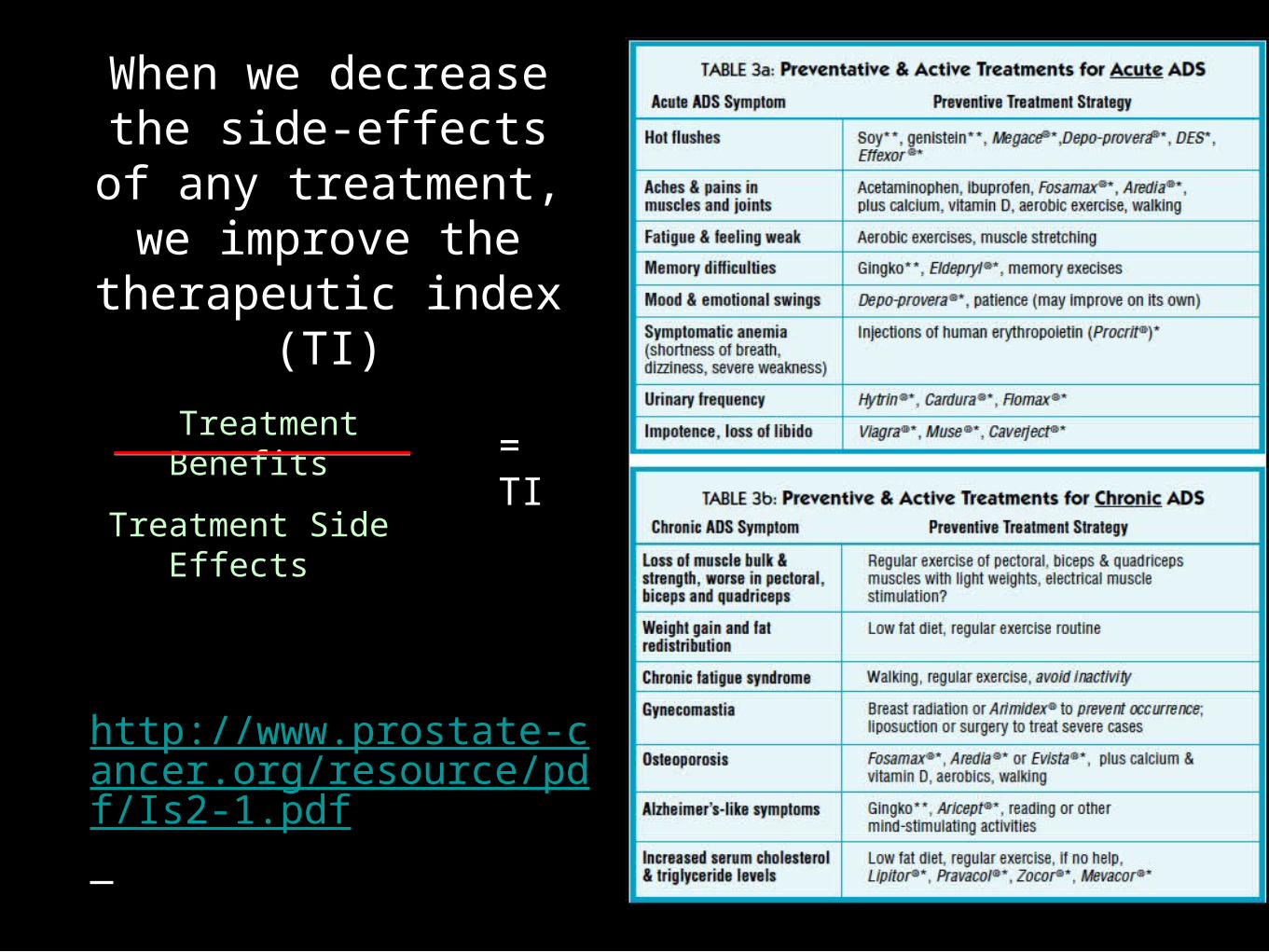
When we decrease the side-effects of any treatment, we
improve the therapeutic index (TI)
Treatment Benefits
Treatment Side Effects
= TI
http://www.prostate-cancer.org/resource/pdf/Is2-1.pdf