why we do what we do: serological testing - seabb · and antibody detection/titration and...
TRANSCRIPT

Serological Testing: Why we did what we did!
W. John Judd, FIBMS, MIBiol
Emeritus Professor
University of Michigan
What we did…
Provided blood and blood products in a timely, cost-efficient manner.
Implemented policies and procedures such that the product provided optimal clinical benefit to the recipient and did not cause adverse clinical effects or transmit disease
Assisted in the prevention and management of HDFN
Aided in the diagnosis of immune hemolysis

More specifically, what we did…
compatibility testing
prenatal/perinatal testing
immune hemolysis investigation
Performed blood group determination, and antibody detection/titration and identification as applied to:

Why we did some of the things we did…
We had to (compliance) To improve patient care To save money To use staff better To eliminate redundant testing Because we had always done it that way! To stay in front

What we had to do…
Donor Recipient Donor/Recipient
ABO/Rh requisition selection
antibodies identity crossmatch
disease sample issue
ABO/Rh ABO/Rh bedside
antibodies
records

Donor Testingtransfusion service
ABO confirm RBC type on all RBC units
Rh direct tests with anti-D on RBC units labeled Rh-
Antibodies not required
Infectious agents
not required except for platelets

ABO/Rh on RBC Units
Required by FDA and AABB Necessary for electronic crossmatch Done upon receipt from blood supplier Anti-A,B used to test units labeled group O IgM mAb anti-D used to test units labeled Rh-negative
About 100 mislabeled units/year reported to FDA
Protecting the Recipient
REQUISITION right patient right reason right product
IDENTIFICATION right patient
SAMPLE right name right ID # right blood in tube
TRANSFUSION right patient right reason right product
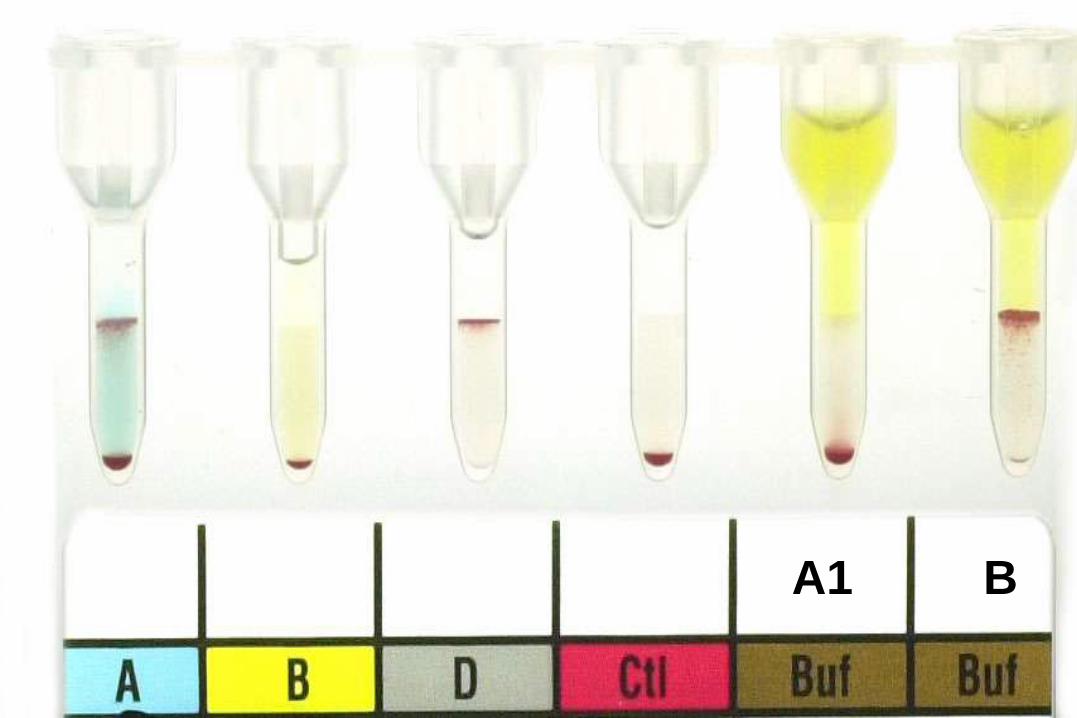
A1 B
Confirmation of Identity
Old Way verbal
verbal + visual
ID bracelet– patient unique
– SS number
– barcoded
New Way digitalized thumbprint
retinal scan
voice recognition

Because We Must!
Stoppered tube with firmly attached label– first and last name
– identification number
– date (time) of collection
Labeled at the bedside!
Obtained within 3 days of scheduled transfusion if patient transfused or pregnant in preceding 3 months
matches requisition

How did we do what we did?pretransfusion testing
ABO/Rh
Antibody detection
Crossmatch

ABO/Rh Typing Requirements
ABO RBCs with anti-A and –B
Serum/plasma with A1 and B RBCs
Concordance between serum and RBCs
Positive reactions must be >2+
Rh Direct tests with anti-D
Positive reactions must be >2+
Control to detect false-positives
No test for weak D

Why didn’t we…? Because….
Test patient RBCs with anti-A,B?
Rare A/B subgroups given group O RBCs
Test apparent Rh-
patient samples for weak D?
Weak D can result from partial D, requiring Rh- RBCs

Valid ABO/Rh Reactionstube tests
anti-A anti-BBiocloneanti-D
A1 RBCs B RBCs
0 0 >2+/0 >2+ >2+
>2+ 0 >2+/0 0 >2+
0 >2+ >2+/0 >2+ 0
>2+ >2+ 0* 0 0
* inert control required if positive

Weak Reactionswhy we care
Less the expected 3+ or 4+
May represent a false-positive test
Seen in newborns and in disease
May result from non-ABO-type specific transfusion
May indicate partial D phenotype

Increased workload from requirement to detect bacterial contamination in platelets
Positive sample identification
Standardized testing leading to better compliance with cGMP
Increased costs of traditional reagents
To stay in front
Why did we automate?

Valid ABO/Rh Reactionsautomated gel tests
anti-A anti-B anti-D Control A1 RBCs B RBCs
0 0 >3+/0 0 >1+ >1+
>2+ 0 >3+/0 0 0 >1+
0 >2+ >3+/0 0 >1+ 0
>2+ >2+ >3+/0 0 0 0

Why the change?
Gel not optimal for detection of anti-A and –B in plasma
Discrepancies between tube and gel Rh types were associated in 3/13 cases with DAR form of partial D

Antibody Detection
Room temperature
AlbuminLIS
37 C
Anti-IgG+C3
Autocontrol
37 C
Gel/LIS
Anti-IgG
in the past current

Approved Methodsantibody detection
serum:RBCs time AHG
SAL >2:1, 3-4% 30-60’ PS/IgG
ALB >2:1, 3-4% 15-30’ PS/IgG
LIS 2:2, 2% 10’-15’ PS/IgG
GEL 1:2, 0.8% 15’ IgG
PEG 2:1, 3-4% 15-30’ IgG
LIP 2:1, 1% 1’ IgG
SPA 1:1, 0.4% 15’ IgG

Why Gel?
LISA PEG GEL SPA
sensitivity 91.2% 96.8% 95.9% 99.1%
specificity 98.1% 97.8% 99.6% 90.1%
Reilly et al. Transfusion 1997;37(S):64
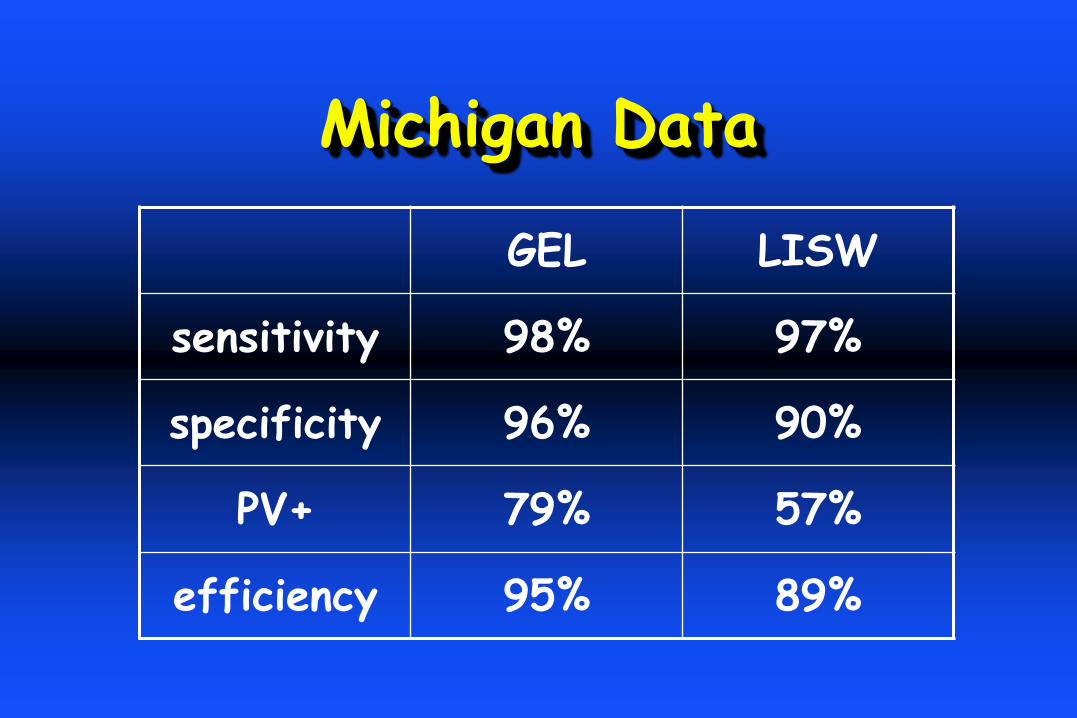
Michigan Data
GEL LISW
sensitivity 98% 97%
specificity 96% 90%
PV+ 79% 57%
efficiency 95% 89%

Anti Found by: anti-c
-E + -c LIS or Gel 32 39%
-E + -c Ficin-Gel 21 26%
-E alone LIS or Gel 29 35%
total anti-c any method 53 65%
82 R1R1 Patients with Anti-E
Gel in the RL
Eliminated testing that was not required.
What we did most of all…

Redundant Testing
RT incubation
Anti-C3 in AHG
3-cell-sample screen
IAT-crossmatch (negative screen)
DAT
37 C reading

No anti-C3 or RT?
Unwanted
Negatives
Unwanted
Positives
LIS RT-37-IgG+C3 0 1.41%
37-IgG+C3 0 0.61%
37-IgG 5* 0.1%
* All anti-Jk

Reagent RBCs
Two group O RBC samples that between them, carry C c D E e; K k; Fya Fyb; Jka Jkb; M N S s ; Lea
Leb and P1
R1R1 and R2R2, one Jk(a+b-)
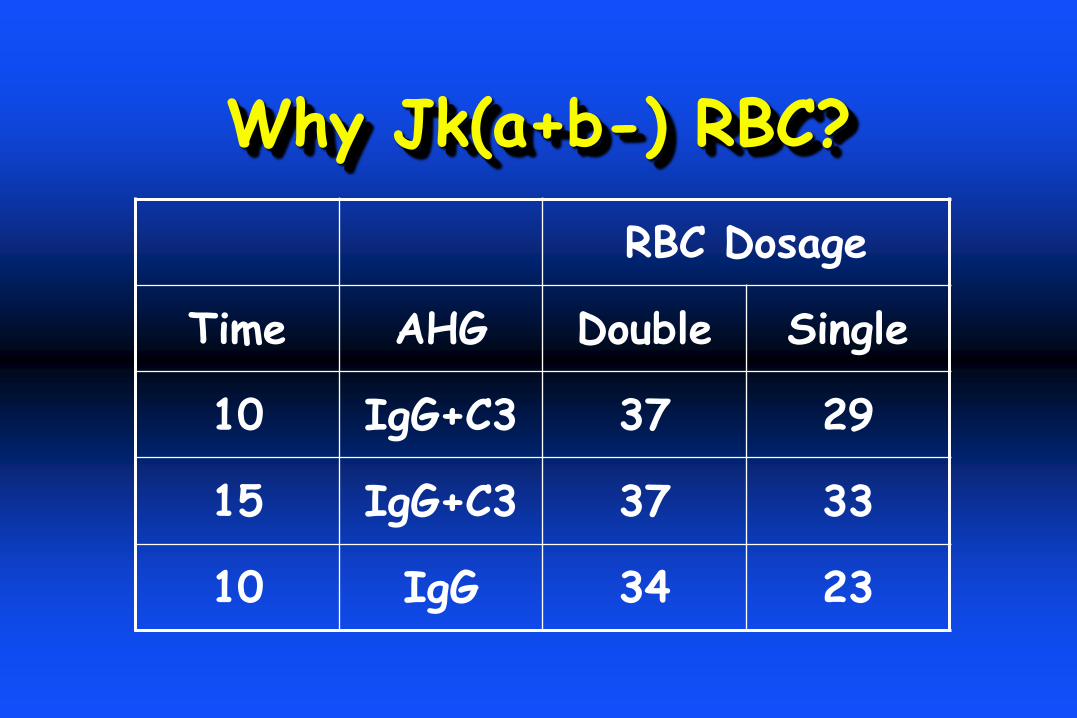
Why Jk(a+b-) RBC?
RBC Dosage
Time AHG Double Single
10 IgG+C3 37 29
15 IgG+C3 37 33
10 IgG 34 23

Antibodies found at X-Matchnegative screen
Year # Tests Method Wanted Unwanted†
1975-76 82,674 ALB 8(1) 201
1979-80 58,639 LIS 10(1) 85
1983-84 81,444 LIS 17(4) 114
222,730 35(6*) 400
* to low prevalence antigen; † anti-I, -HI. –M, etc

Seen only by X-Match
C 3 E 11 e 1 c 2
K 3 Jk 7 Cw 1 Fy 2
V 2 Jsa 2 Wra 1
Data used in support of IS-crossmatch and 2-cell-sample screen.

Why were antibodies only found at X-Match?
Dosage? Note: A rr sample will not have afforded detection of 11 -E and 3 -C
Better antigen expression on donor RBCs?
More caution applied to reading X-match?
Inconstant degree of agitation applied to tube tests

DAT/Autocontrol Study
Samples 65,049 -ve serum
IgG DAT+ 3570 3133
Evaluated: 778 489
transfusion 720 482
reactive serum 43 0
diagnostic 15 7

Findings
ELUATESnegative 518
auto 192
drug 7
passive 9
allo 52
BY EVALUATION3 Jka eluate
2 K1 eluate
1 Lua eluate
1 D serum-ficin
1 E serum-ficin
1 K serum K+k-RBCs
PV+ = 0.29%
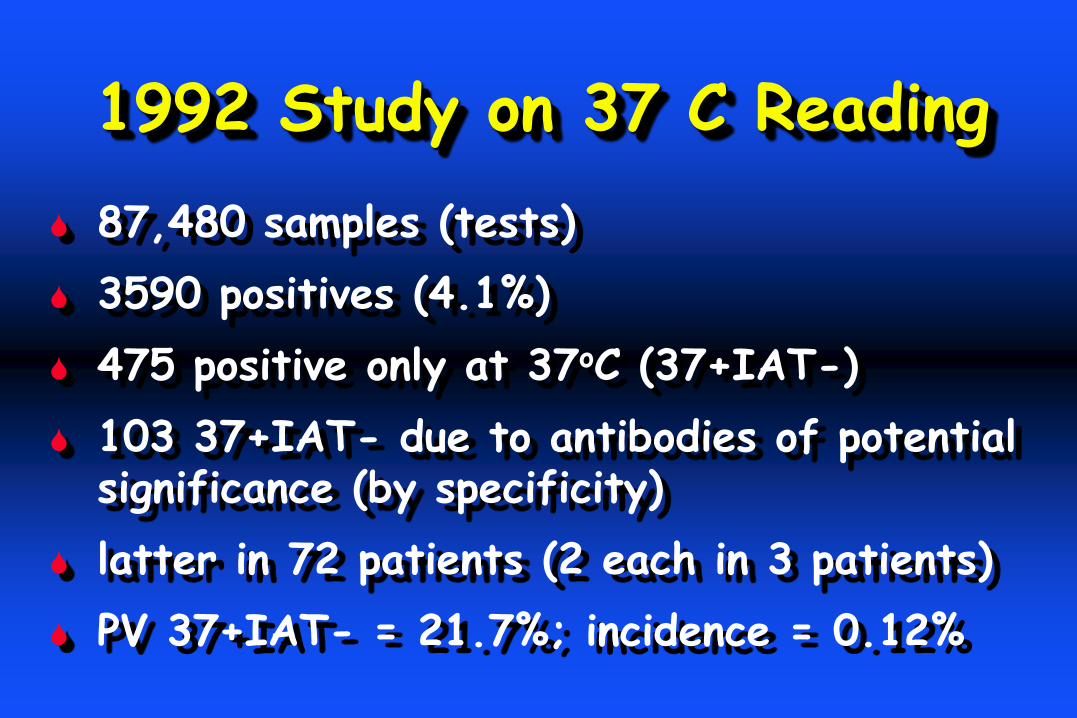
1992 Study on 37 C Reading
87,480 samples (tests)
3590 positives (4.1%)
475 positive only at 37oC (37+IAT-)
103 37+IAT- due to antibodies of potential significance (by specificity)
latter in 72 patients (2 each in 3 patients)
PV 37+IAT- = 21.7%; incidence = 0.12%

37 C Agglutinins
significance n specificity
harmless 196 I, HI, etc
dubious 176 MN, Le, P1, Lua
potential 103 E(63), D(4), C(1),
cE(3) K(27), Jk(5)
87,480 samples

RBC Exposurepatients (n = 75)
transfusion E C cE D K Jka
< 4 months 32 2 1 20 2
> 1 year 9 1 1 1 1
none known 3 1 1
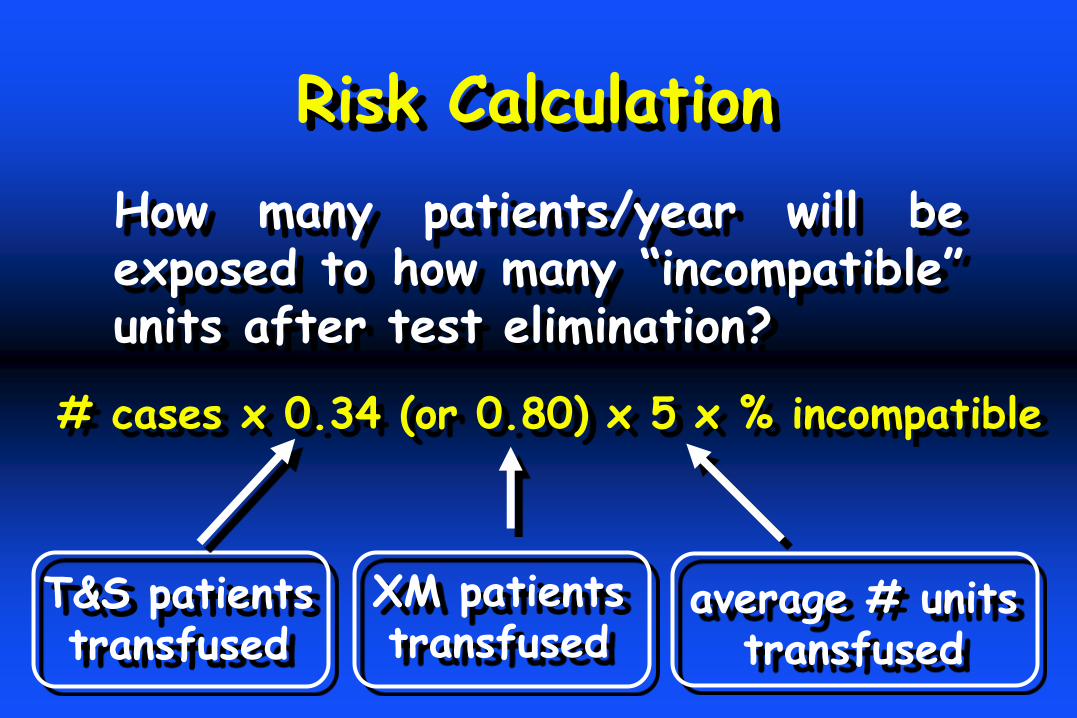
Risk Calculation
# cases x 0.34 (or 0.80) x 5 x % incompatible
How many patients/year will beexposed to how many “incompatible”units after test elimination?
T&S patientstransfused
XM patientstransfused
average # unitstransfused

RISK
test
eliminated
PV+
cases per
year
patients at
risk
transfused
# incompatible
units transfused
per patient
DAT 0.29% 3.25 1.1 2.05
IAT-XM 7.25% 9.7 7.75 1.85
37 C 21.7% 25 8.5 1.45
30,000samplestested
29,000units
transfused
46,000 crossmatches
Because we could!

Electronic Crossmatch
Replaces serological tests for ABO incompatibility
Requires validated electronic record of patient and donor ABO/Rh types
Not to be used if unexpected antibodies present

AABB/FDA Requirements
On-site validation
Only ABO incompatibility
Verification of data entry

Method Selection
IAT if unexpected antibodies
Computer if two ABO/Rh
IS if computer down







Where I would like tohave gone…

Computer Order Entry• record of ordering physician• algorithm to validate request
Sample Collection• electronic patient andphlebotomist ID
• label printed at bedside
Testing• centralized• automated• electronic operator ID• results downloaded to LIS
Remote Site• validated computerizeddonor inventory
• data access via internet• electronic XM on-site• electronic patient andtransfusionist ID
e-match

direct storage• bar coded entry
• random compatment assignment
single access retrieval• automatic dispense of ABO
matched unit
storage optimization• first in, first out
benefits• better staff utilization
• reduction of emergency requests
• reduced outdating
We Went Molecular!
Because we could
The antisera were running out and expensive!
To stay in front
To improve patient care
BeadChipTM Technology
Genotyping vs. Phenotyping
Recently transfused patients
Patients with a positive DAT
Patients with more than two alloantibodies

Milestones at Michigan
1974 WJJ arrived
1975 no anti-A,B
1979 LISS
1980 IgG DAT
1982 no RT
1985 no DAT
1986 IS-XM
1987 anti-IgG
1992 computer XM
1996 no 37 C
2003 gel automation
2007 molecular
2008 WJJ retired


No! No!
PEG adsorptions
Prewarmed tests
Rh-negative, Du-positive
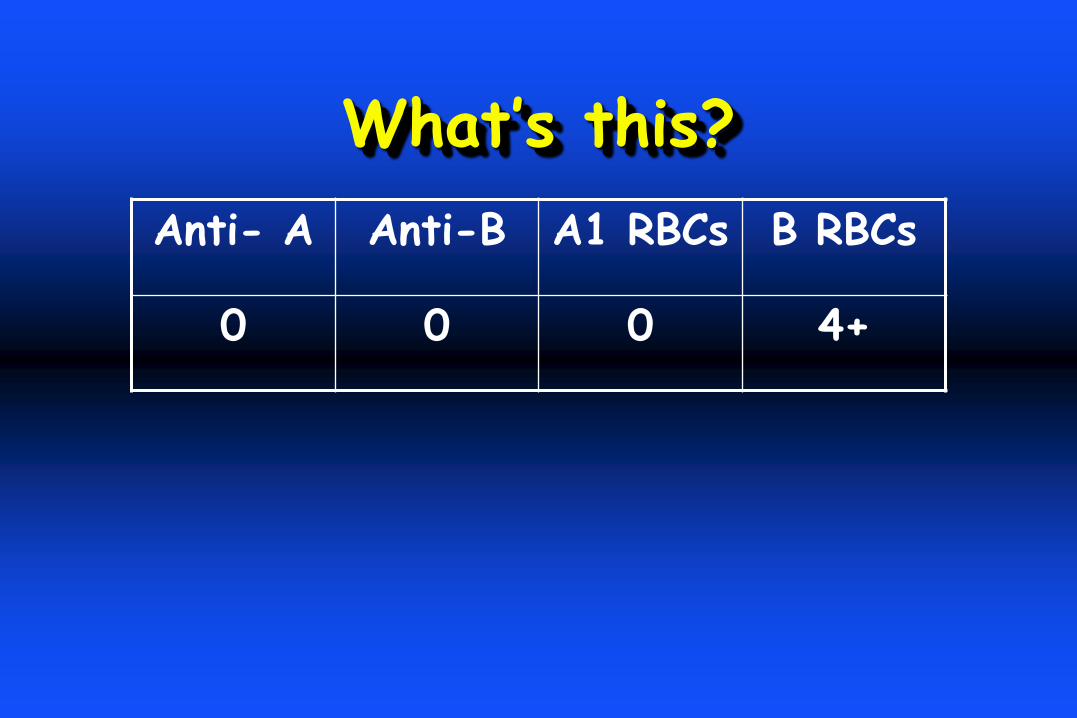
What’s this?
Anti- A Anti-B A1 RBCs B RBCs
0 0 0 4+
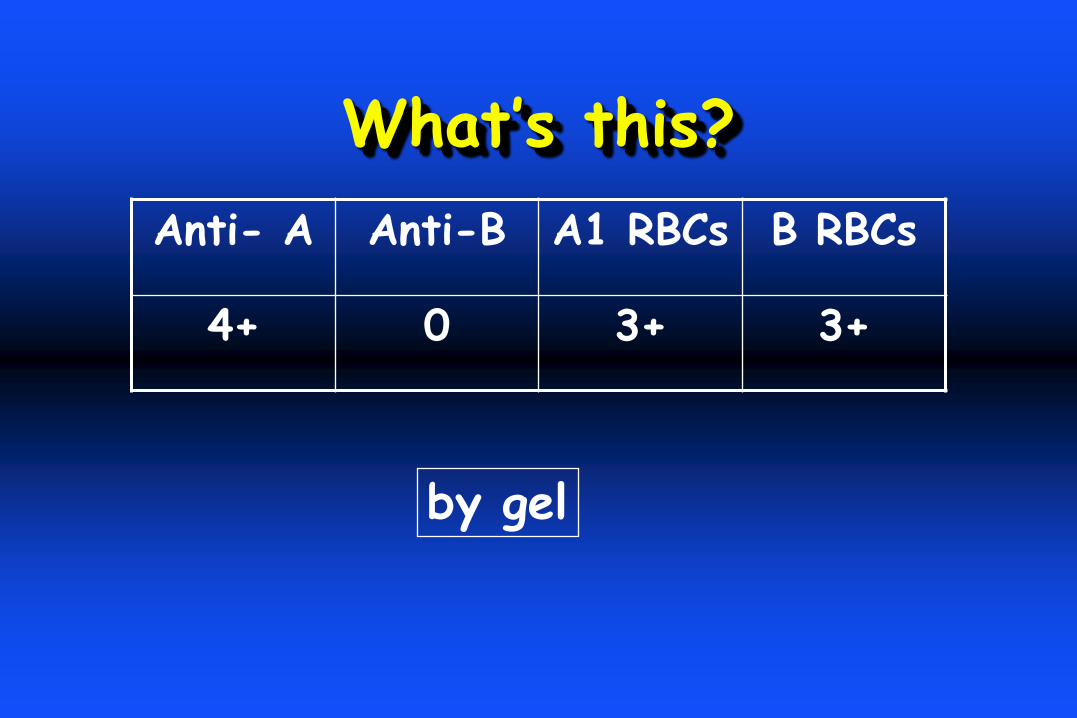
What’s this?
Anti- A Anti-B A1 RBCs B RBCs
4+ 0 3+ 3+
by gel