why patients are reluctant to start insulin, and what to do about it william h. polonsky, phd, cde...
TRANSCRIPT

Why Patients are Reluctant to Start Why Patients are Reluctant to Start Insulin, and What to Do About itInsulin, and What to Do About it
William H. Polonsky, PhD, CDEWilliam H. Polonsky, PhD, CDE
January 30, 2009January 30, 2009
[email protected]@behavioraldiabetes.org

Potential Consequences of Potential Consequences of Delayed IT InitiationDelayed IT Initiation
• May lead to long periods of chronically high May lead to long periods of chronically high blood glucose levels.blood glucose levels.
• Patients may drop out of treatment to avoid IT.Patients may drop out of treatment to avoid IT.
• Patients on insulin may come to believe that Patients on insulin may come to believe that less insulin = less disease. So they may omit less insulin = less disease. So they may omit insulin until they begin feeling “bad”. insulin until they begin feeling “bad”.

Resistance to Insulin Therapy Resistance to Insulin Therapy How Big is the Problem?How Big is the Problem?
UKPDS, 1995UKPDS, 1995 Randomization to Randomization to insulin (n = 496)insulin (n = 496)
27% refused IT27% refused IT
Polonsky et al, Polonsky et al, 20052005
Patient surveyPatient survey
(n= 708)(n= 708)
28% “not willing” to 28% “not willing” to begin IT if prescribedbegin IT if prescribed
Larkin et al, Larkin et al, 20082008
Patient surveyPatient survey
(n = 100)(n = 100)
33% “not willing” to 33% “not willing” to begin IT if prescribedbegin IT if prescribed

Prospective IT Willingness Prospective IT Willingness Ethnic DifferencesEthnic Differences
0
5
10
15
20
25
30
35
40
45
Not Slight Moderate Very
NHW (n = 380) Non-NHW (n = 328)
% in
dica
ting
som
e le
vel o
f dis
tres
s
Polonsky et al, 2005

Prospective IT Willingness Prospective IT Willingness Gender DifferencesGender Differences
0
5
10
15
20
25
30
35
40
45
Not Slight Moderate Very
Males (n = 242) Females (n = 466)
% in
dica
ting
som
e le
vel o
f dis
tres
s
Polonsky et al, 2005

Insulin Persistence in Insulin Persistence in Type 2 DiabetesType 2 Diabetes
• 8484 male veterans, 2 years of observation, 8484 male veterans, 2 years of observation, prescribed doses vs. pharmacy claim:prescribed doses vs. pharmacy claim:• ““Mean insulin complianceMean insulin compliance of 77% for chronic of 77% for chronic
users indicates that most patients are makingusers indicates that most patients are making an an effort to take insulin, albeit not as prescribed by effort to take insulin, albeit not as prescribed by theirtheir physician.”physician.”
• Factoring in wastage, overall use estimated as Factoring in wastage, overall use estimated as 58–65%.58–65%.
Cramer and Pugh, 2005

Insulin Omission in Type 1 Insulin Omission in Type 1 DiabetesDiabetes
Polonsky et al, Polonsky et al, 19951995
341 women 341 women surveyedsurveyed
31% omitted insulin; 31% omitted insulin; 9% regularly omitted9% regularly omitted
Jones et al, Jones et al, 20002000
361 female 361 female teens surveyedteens surveyed
11% omitted insulin 11% omitted insulin regularly regularly
Major contributors are fear of weight gain and Major contributors are fear of weight gain and diabetes distress, diabetes distress, notnot discomfort with insulin per se discomfort with insulin per se
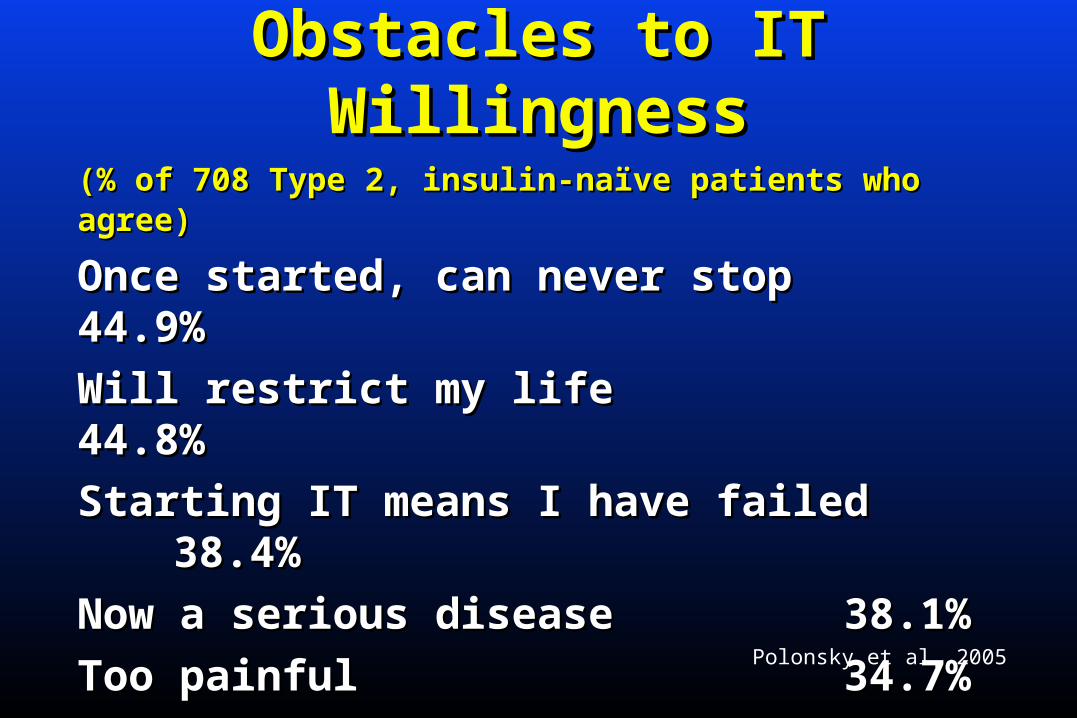
Obstacles to IT WillingnessObstacles to IT Willingness
(% of 708 Type 2, insulin-naïve patients who agree)(% of 708 Type 2, insulin-naïve patients who agree)
Once started, can never stopOnce started, can never stop 44.9%44.9%
Will restrict my lifeWill restrict my life 44.8%44.8%
Starting IT means I have failedStarting IT means I have failed 38.4%38.4%
Now a serious disease Now a serious disease 38.1%38.1%
Too painfulToo painful 34.7%34.7%
May cause blindnessMay cause blindness 10.1%10.1%
Polonsky et al, 2005

Obstacles to IT WillingnessObstacles to IT Willingness
WillingWilling NotNot
Once started, can never stopOnce started, can never stop 43% 43% 53% 53%
Will restrict my lifeWill restrict my life 42% 56% 42% 56%
Starting IT means I have failedStarting IT means I have failed 37% 55% 37% 55%
Now a serious disease Now a serious disease 35% 47% 35% 47%
Too painfulToo painful 30% 30% 51% 51%
May cause blindnessMay cause blindness 8% 17% 8% 17%
Polonsky et al, in preparation

IT ObstaclesIT Obstacles1.1. Injection-related anxiety Injection-related anxiety
• Discomfort with injectionsDiscomfort with injections
• Needle phobiaNeedle phobia

IT ObstaclesIT Obstacles2.2. Perceived lack of controlPerceived lack of control
• ““If I start taking insulin, I’ll never be able If I start taking insulin, I’ll never be able to stop.”to stop.”
• ““insulin means no more spontaneity. It insulin means no more spontaneity. It would restrict my life, making it too hard would restrict my life, making it too hard to to to travel, eat out, or even have a life!”to travel, eat out, or even have a life!”

IT ObstaclesIT Obstacles3.3. Low self-efficacy Low self-efficacy
• ““I’m just not confident I could handle the I’m just not confident I could handle the demands of insulin, like deciding how demands of insulin, like deciding how much to take and when to take it.”much to take and when to take it.”
• ““Its just too complicated; its too much for Its just too complicated; its too much for me to do.” me to do.”

IT ObstaclesIT Obstacles4.4. A sense of personal failure A sense of personal failure
• ““If I take insulin, it means I have failed, If I take insulin, it means I have failed, that I haven’t done a good enough job that I haven’t done a good enough job taking care of my diabetes.”taking care of my diabetes.”
• In DAWN, US patients report more self-In DAWN, US patients report more self-blame than patients from all other blame than patients from all other countries.countries.
Peyrot et al, 2005Peyrot et al, 2005
IT ObstaclesIT Obstacles5.5. Positive gain is not expectedPositive gain is not expected
• In DAWN, < 10% of insulin-naïve type 2 In DAWN, < 10% of insulin-naïve type 2 subjects believed IT would lead to better subjects believed IT would lead to better glycemic control, less fatigue or better glycemic control, less fatigue or better healthhealth
Skovlund et al, 2003Skovlund et al, 2003

IT ObstaclesIT Obstacles6.6. Perceived worsening of the disease process Perceived worsening of the disease process
• ““Taking insulin means my diabetes will Taking insulin means my diabetes will become a more serious disease.”become a more serious disease.”
• ““Taking insulin may cause other problems, Taking insulin may cause other problems, like frequent low blood sugars, weight like frequent low blood sugars, weight gain, or maybe even cause more serious gain, or maybe even cause more serious problems with my eyes or kidneys.”problems with my eyes or kidneys.”

IT ObstaclesIT Obstacles1.1. Injection-related anxietyInjection-related anxiety
2.2. Perceived lack of controlPerceived lack of control
3.3. Low self-efficacyLow self-efficacy
4.4. A sense of personal failureA sense of personal failure
5.5. Positive gain is not expectedPositive gain is not expected
6.6. Perceived worsening of the disease processPerceived worsening of the disease process

Why Would Patients Feel This Way?Why Would Patients Feel This Way?• Personal experience (e.g. hypoglycemia)Personal experience (e.g. hypoglycemia)
• Observation of others with diabetesObservation of others with diabetes
• Overt and covert messages from health care Overt and covert messages from health care providersproviders

Physician InfluencesPhysician Influences• Threatening patients with insulinThreatening patients with insulin
- ““If you can’t make some positive changes If you can’t make some positive changes in how you eat and exercise, then we’ll have in how you eat and exercise, then we’ll have no choice but to start insulin.”no choice but to start insulin.”
• Underlying messagesUnderlying messages
- Insulin should be avoided at all costsInsulin should be avoided at all costs
- You have failedYou have failed
- You are to be punishedYou are to be punished


Physician Resistance to ITPhysician Resistance to IT1.1. TimeTime
2.2. Lack of confidenceLack of confidence
Haque et al, 2005Haque et al, 2005

Physician Resistance to ITPhysician Resistance to IT1.1. TimeTime
2.2. Lack of confidenceLack of confidence• Gap in knowledge, ½ of respondentsGap in knowledge, ½ of respondents• ““I had no idea how to determine the dosage for I had no idea how to determine the dosage for
the patient”the patient”
Haque et al, 2005Haque et al, 2005

Physician Resistance to ITPhysician Resistance to IT1.1. TimeTime
2.2. Lack of confidenceLack of confidence
3.3. Wishes to avoid unpleasant confrontationWishes to avoid unpleasant confrontation
4.4. Believes that patient is not competentBelieves that patient is not competent
Haque et al, 2005Haque et al, 2005

Physician Resistance to ITPhysician Resistance to IT1.1. TimeTime
2.2. Lack of confidenceLack of confidence
3.3. Wishes to avoid unpleasant confrontationWishes to avoid unpleasant confrontation
4.4. Believes that patient is not competent Believes that patient is not competent
5.5. Hypoglycemia and weight gainHypoglycemia and weight gain• ““Initiating insulin in a patient who is not Initiating insulin in a patient who is not
compliant on a diabetic diet and has morbid compliant on a diabetic diet and has morbid obesity is generally not a very good idea”obesity is generally not a very good idea”
Haque et al, 2005Haque et al, 2005

Physician Resistance to ITPhysician Resistance to IT1.1. TimeTime
2.2. Lack of confidenceLack of confidence
3.3. Wishes to avoid unpleasant confrontationWishes to avoid unpleasant confrontation
4.4. Believes that patient is not competent Believes that patient is not competent
5.5. Hypoglycemia and weight gainHypoglycemia and weight gain
6.6. No beneficial outcomesNo beneficial outcomesDAWN: “Just over half of physicians/nurses agreeDAWN: “Just over half of physicians/nurses agree
that insulin can have a positive impact on care.”that insulin can have a positive impact on care.”
Haque et al, 2005, Peyrot et al, 2005Haque et al, 2005, Peyrot et al, 2005

Insulin Use and Glycemic ControlInsulin Use and Glycemic Control
0
10
20
30
40
50
60
< 6.0% < 7.0% > 8.0% > 9.0% > 10.0%
Insulin Orals Diet
% re
achi
ng li
sted
goa
ls
Harris et al, 1999

IT ObstaclesIT Obstacles1.1. Injection-related anxietyInjection-related anxiety
2.2. Perceived lack of controlPerceived lack of control
3.3. Low self-efficacyLow self-efficacy
4.4. A sense of personal failureA sense of personal failure
5.5. Positive gain is not expectedPositive gain is not expected
6.6. Perceived worsening of the disease processPerceived worsening of the disease process

What To Do?What To Do?

Overcoming IT ResistanceOvercoming IT Resistance1.1. Ask about patient’s personal obstaclesAsk about patient’s personal obstacles

Overcoming IT ResistanceOvercoming IT Resistance1.1. Ask about patient’s personal obstaclesAsk about patient’s personal obstacles
- ““What are some of the reasons why taking What are some of the reasons why taking insulin seems so unpleasant to you?”insulin seems so unpleasant to you?”

Overcoming IT ResistanceOvercoming IT Resistance1.1. Ask about patient’s personal obstaclesAsk about patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection

Overcoming IT ResistanceOvercoming IT Resistance1.1. Ask about patient’s personal obstaclesAsk about patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT


Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT• ““I’d like you to try insulin for just a month. At the I’d like you to try insulin for just a month. At the
end of the month, if you don’t think its been end of the month, if you don’t think its been worthwhile, or if it still seems as awful as you’re worthwhile, or if it still seems as awful as you’re imagining it might be, I promise to help you stop.” imagining it might be, I promise to help you stop.”
• Design IT regimen to minimize lifestyle restrictionDesign IT regimen to minimize lifestyle restriction

Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT
4.4. Consider insulin pensConsider insulin pens

Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT
4.4. Consider insulin pensConsider insulin pens
5.5. Pass along the good newsPass along the good news

For Maddy: How Insulin Affects For Maddy: How Insulin Affects Your Blood SugarsYour Blood Sugars
6
7
8
9
10
Hem
og
lob
in A
1c L
evel
3 months INSULIN 3 months 6 months 9 months 12 months3 months INSULIN 3 months 6 months 9 months 12 months
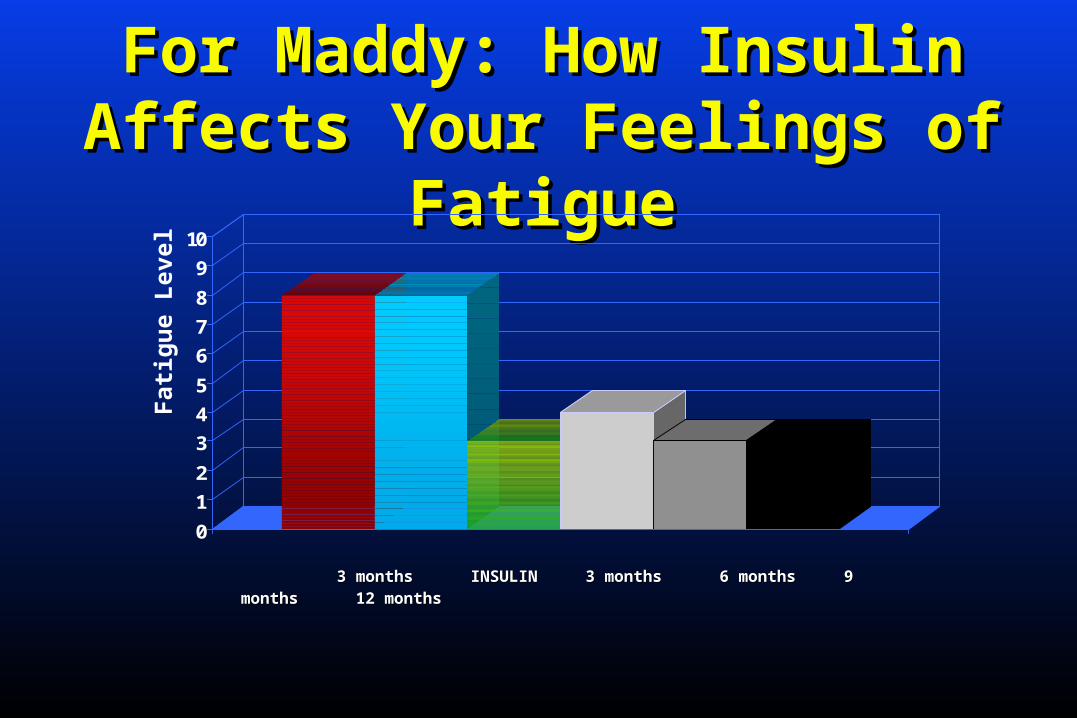
For Maddy: How Insulin Affects For Maddy: How Insulin Affects Your Feelings of FatigueYour Feelings of Fatigue
0
1
2
3
4
5
6
7
8
9
10
F
atig
ue
Lev
el
3 months INSULIN 3 months 6 months 9 months 12 months3 months INSULIN 3 months 6 months 9 months 12 months
Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT
4.4. Consider insulin pensConsider insulin pens
5.5. Pass along the good newsPass along the good news
6.6. Address patient’s concernsAddress patient’s concerns

Addressing Psychological Addressing Psychological Insulin ResistanceInsulin Resistance
• No one manages diabetes perfectly• No matter what you do, you may need
insulin, because diabetes is “progressive”
• Insulin improves glucose control; Nobel Prize not given for drugs that don’t work
• Long-term benefits of good control
• Short-term benefits include increased energy, better sleep and mood
It means I have failed with my treatment
Insulin won’t help
Will wreck my quality of life
Obstacles Discuss

Addressing Psychological Addressing Psychological Insulin ResistanceInsulin Resistance
• Hurts less than SMBG• Advantages of insulin pens and thinner,
smaller needles
• Diabetes is “progressive”; insulin helps control BG levels and keeps the disease from getting worse
• Investigate and challenge this belief • Insulin is much more likely to reduce than
raise complications risk
Injections hurt
It means diabetes is getting worse
I will get complications
Obstacles Discuss

Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT
4.4. Consider insulin pensConsider insulin pens
5.5. Pass along the good newsPass along the good news
6.6. Address patient’s concernsAddress patient’s concerns

Take-Home MessagesTake-Home Messages
• Reluctance to begin Reluctance to begin IT is widespreadIT is widespread
• But take hope! But take hope! • IT resistance can be IT resistance can be
overcomeovercome

Take-Home MessagesTake-Home MessagesCommon obstacles include:Common obstacles include:
• Injection-related anxietyInjection-related anxiety
• Perceived lack of controlPerceived lack of control
• Low self-efficacyLow self-efficacy
• A sense of personal failureA sense of personal failure
• Positive gain is not expectedPositive gain is not expected
• Perceived worsening of the disease processPerceived worsening of the disease process

Overcoming IT ResistanceOvercoming IT Resistance1.1. Identify patient’s personal obstaclesIdentify patient’s personal obstacles
2.2. Encourage an immediate injectionEncourage an immediate injection
3.3. Provide a sense of control regarding ITProvide a sense of control regarding IT
4.4. Consider insulin pensConsider insulin pens
5.5. Pass along the good newsPass along the good news
6.6. Address patient’s concernsAddress patient’s concerns


Behavioral Diabetes InstituteBehavioral Diabetes Institute
Website:Website: www.behavioraldiabetes.orgwww.behavioraldiabetes.org
INFO:INFO: [email protected]@behavioraldiabetes.org
CALL:CALL: 858-336-8693858-336-8693