why did this heart break? - internal medicine | acp · periapical region manipulation ... nishimura...
TRANSCRIPT

Why Did This Heart Break?
Montana ACP Meeting
September 2016
Sarah H. Fenton, MD, FACC
St. Peter’s Medical Group

History
56 year old male with a known muscular VSD
3 mo dry cough, post-nasal drip
PMD and 2 Urgent Care visits
Z-Pak twice
Fever 104° 6 weeks prior to ED visit
1 month DOE
1 week orthopnea and PND

Physical Exam (1)
VS: T 98°, BP 146/51, HR 99, RR 18 mildly labored, 97%
sat on RA.
Skin: Warm and dry, no rash.
HEENT: NC/AT, conjunctiva pink, sclerae anicteric,
oropharynx clear.
Neck: 10-12 cm JVD, carotids 2+ with bilateral murmur
radiation.
Lungs: Decreased at bases with crackles.

Physical Exam (2)
Heart: PMI laterally displaced, tachycardic, regular. Normal S1, S2. Grade II-III/VI systolic murmur LSB with radiation throughout precordium, Grade I/VI early diastolic murmur aortic area without radiation. No S3 or S4. No rub.
Abdomen: Normal BS, soft, nontender. No HSM.
Extremities: No clubbing, cyanosis or edema. 2+ DP and PT pulses (waterhammer) bilaterally. Trace-1+ ankle and lower pretibial edema bilaterally.
Neurologic: Slow to respond to questions (received Ativan). No gross motor deficits.
Diagnostic Studies (1)
Labs: WBC 13.8 (84% neutrophils), Hgb 12.0, plt 406K,
K+ 4.0, BUN 13, Cr 0.93, Glucose 97, AST 25, ALT 29,
troponin .08, proBNP 5676.
ECG: ST, 1° AV block, LAE, high LV voltage. No prior.
AP CXR: Pulmonary vascular congestion, small bilateral
pleural effusions, prominent pulmonary arteries.
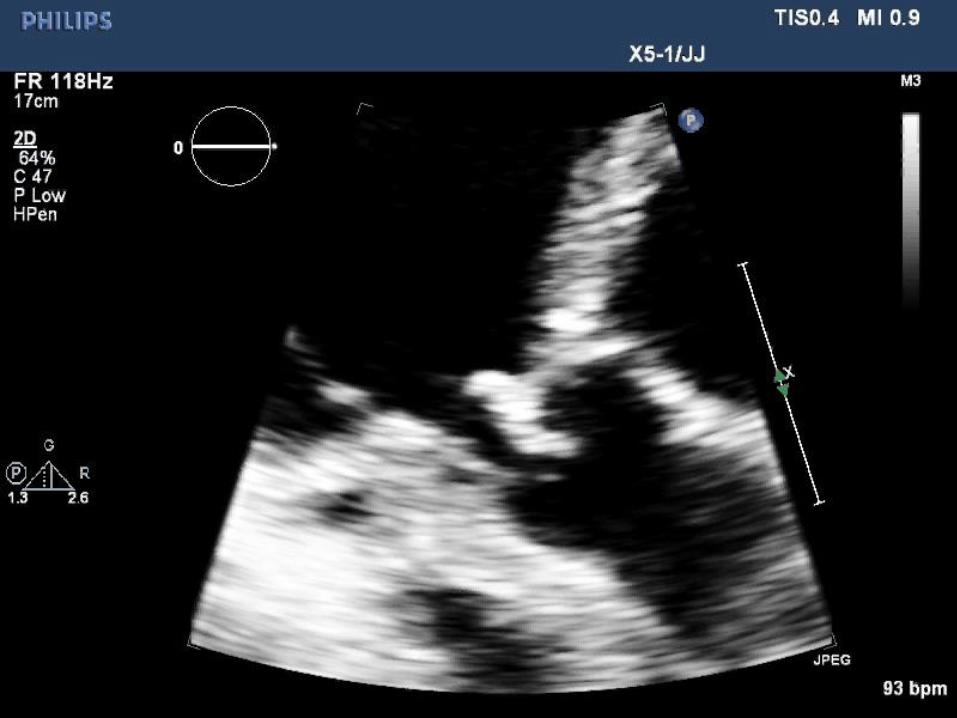
Diagnostic Studies (2)
Echocardiogram








Diagnosis
NYHA Class IV CHF due to severe aortic insufficiency as
a result of subacute aortic valve endocarditis
Severe AI due to perforation of aortic valve leaflet
Appears to be a bicuspid aortic valve
Possible aortic annular abscess with fistula vs. high
membranous VSD
Known distal muscular VSD

Treatment
Blood cultures x 2
Empiric antibiotics (Vancomycin and Gentamicin)
Diuresis
Transfer for aortic valve replacement

Surgical Findings and Treatment
Bicuspid aortic valve with large vegetation, perforation and severe AI
Small vegetation ventricular surface of anterior leaflet of mitral valve
Membranous and muscular VSDs
Ascending aortic aneurysm
25 mm Edwards pericardial aortic valve, debridement and repair of mitral valve, 30 mm Hemashield graft ascending aorta, Hemashield patch 1 cm perimembranous VSD

Infective Endocarditis
Epidemiology
Pathogenesis
Special Populations
Laboratory evaluation
Diagnosis
Modified Duke Criteria
Complications
Prevention

Epidemiology
Incidence 3-10/100,000 pt years
Higher incidence urban populations
>50% over age 60
6% Rheumatic heart disease (40 years ago 1/3)
38% AV, 34% MV, 8% AV and MV, 4% TV
3.5% congenital heart disease
75% of patients have structural heart disease
15-20% in-hospital mortality
1 year mortality 40%

Pathogenesis
Endothelial damage platelet–fibrin matrix deposition
bacterial colonization
Location: Greatest blood flow forces (atrial side of
MV/TV, ventricular side of AV/PV)

Microbiology
Typical
S. aureus, Viridans strep, enterococci, HACEK organisms
(Haemophilus, Actinobacillus, Cardiobacterium, Eikenella,
Kingella)
Prosthetic valve endocarditis
Within 60 days of surgery- S. epidermidis most common,
Others (S. aureus, GN bacteria, Diphtheroids, Fungi)
Late (> 1 year after surgery)- same as native

Special Populations (1)
Elderly
Lower rates of emboli, immune-mediated phenomenon,
septic complications, vegetations
More abscesses
Higher mortality
Dialysis
Intravascular access
Higher frequency bacteremia
Impaired immune system
Calcific valve disease challenge to identify vegetation

Special Populations (2)
IVDU
S. aureus
Right and left sided valves
Previous endocarditis
Recurrent endocarditis 4.5%
Prosthetic valves
25% of all IE cases
1-3% at 1 year
3-6% at 5 years
Incidence 50x higher than general population

Diagnosis (1)
Clinical
Fever >80%, malaise, weight loss
CHF
CVA
Musculoskeletal pain
Physical
Murmur >80%
Cutaneous (petechiae, splinter hemorrhages, Osler nodes, Janeway lesions)
Roth spots
Septic emboli (osteomyelitis, spleen, CVA, PE, abscess)

Clinical Manifestations of IE
Roth spot
Osler node
Janeway lesions
Splinter hemorrhages

Diagnosis (2)
Labs
Anemia
Normal or elevated WBC
Elevated ESR, CRP
Hematuria, proteinuria, pyuria, RBC casts
2 or more BCx over 1 hour, separate sites.
3 sets of BCx >6 hrs apart if subacute. If unstable, don’t
delay antibiotics!
BCx positive in 90% of IE pts

Diagnosis (3)
Echo
Vegetation- TTE 50-90% sensitivity, TEE 90-100% sensitivity
Leaflet perforation
Annular abscess
Aneurysm
Fistula
Prosthetic valve dehiscence

Complications
CHF- 32%
Periannular extension/abscess- 14%
Systemic embolization- CVA 17%, nonCVA 22%
Acute renal failure
Immune-complex glomerulonephritis
Embolic infarct
Multiorgan failure
Interstitial nephritis from antibiotics (gent, vanco)

Modified Duke Criteria
Major criteria
Microbiologic (typical organism from BCx or path)
Endocardial involvement (new valvular regurgitant lesion OR abn echo with mass, abscess, dehiscence
Minor criteria
Predisposition (prior IE, IVDU, prosthetic valve, cyanotic CHD, other turbulent cardiac lesions)
Fever > 100.4°
Vascular phenomenon (embolic event, mycotic aneurysm, Janeway lesion)
Immunolgic phenomenon (serologic markers (RF), GN, Osler, Roth)
Microbiologic findings not meeting major criteria
Definite IE: 2 major, 1 major + 3 minor, or 5 minor
Possible IE: 1 major + 1 minor, 3 minor
Rejected: alternate explanation or resolution with <4 days antibiotics

Treatment (1)
Microbiological eradication
Bactericidal drugs up to 6 weeks
Surveillance BCx after 3-4 days of IV therapy
Treatment (2)
Empiric native valve and late PV endocarditis
Combo PCNs (Unasyn or Augmentin) and Gentamycin
Vanco + Gent + Cipro if PCN intolerant
Empiric early PVE (<12 mo after surgery)
Vanco + Gent + Rifampin

Indications for Surgery
Class I
AI, MR with increased LVEDP and resultant CHF
Destructive lesion (perforation, fistula)
New heart block, valve dehiscence, abscess, relapsing PVE
Consider if persistent fever or positive BCx 5-7d after tx
Resistant organism (S. aureus, fungi)
Class II
Recurrent emboli after appropriate antibiotic tx (IIa)
Persistent vegetation after appropriate antibiotic tx (IIa)
Mobile vegetation > 10 mm (IIb)

Prevention (1)
Class IIa
Prosthetic valve (not prosthetic material for valve repair such as annuloplasty ring, neochords, Mitra-clip, Amplatzer)
Prior IE
Congenital heart disease
Unrepaired cyanotic CHD (palliative shunts and conduits)
During 6 mo after complete repair with prosthetic material or device
Repaired CHD with residual defects
Cardiac transplant with cardiac valvulopathy
Class III
Non-dental procedures (TEE, EGD, colonoscopy, cystoscopy) in absence of active infection

Prevention (2)
2007 AHA IE Update: eliminated widespread prophylaxis
No change in rate of rise of cases since update
Never a controlled, randomized study
Prophylaxis only in dental procedures involving:
Gingival tissue manipulation
Periapical region manipulation
Perforation of oral mucosa
No evidence for IE prophylaxis in GI/GU procedures absent known enterococcal infection

The End (o’carditis)

Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for
the Management of Patients With Valvular Heart Disease: A Report of
the American College of Cardiology/American Heart Association Task
Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57-
e185. doi:10.1016/j.jacc.2014.02.536.
Resources

Question (1)
A 50 year old white male presents to his internist to discuss preventive
health care and the use of herbal supplements. He underwent an
uncomplicated percutaneous closure of a secundum ASD 2 years ago. He
recalls that his doctor has been very thorough regarding health
maintenance. His only symptom is back pain, which he attributes to his
job in construction.
He is on no medications.
His physical exam reveals a blood pressure of 138/88, HR 84 and
regular, RR 12 and unlabored. His neck reveals no JVD, carotid
upstrokes are brisk and no bruits are present. Lungs are clear. Cardiac
exam reveals a regular rhythm, normal rate. There is a Grade I/VI
systolic murmur in the 2nd RICS. No S3 or S4. Abdomen is soft, non-
tender, without obvious hepatosplenomegaly. Extremities reveal no
edema or cyanosis with 2+ DP and PT pulses.

He would like to schedule a screening colonoscopy.
Which of the following do you recommend:
1) Ampicillin 2 g po 1 hour prior to colonoscopy
2) Amoxicillin 2 g po 1 hour prior to colonoscopy
3) Gentamicin 1.5 mg/kg IV 1 hour prior to colonoscopy
4) No antibiotics
5) TEE
Question (2)

Answer: 4
Rationale:
The patient has a completely repaired congenital heart defect (ASD) with
prosthetic material and he is greater than 6 months post-procedure.
Antibiotic prophylaxis for the prevention of infective endocarditis is not
indicated after 6 months from the time of a completely repaired cyanotic
congenital heart defect, including PFO or ASD. This includes both surgical
and percutaneous repair.
In addition, according to current ACC/AHA Guidelines, prophylaxis for the
prevention of infective endocarditis is not indicated for GI or GU
procedures. Only dental procedures that involve manipulation of gingival
tissue, manipulation of the periapical region, or perforation of oral mucosa
require prophylactic antibiotics.
Question (3)

Citation:
Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC Guideline for the
Management of Patients With Valvular Heart Disease: A Report of the American
College of Cardiology/American Heart Association Task Force on Practice
Guidelines. J Am Coll Cardiol. 2014;63(22):e57-e185.
doi:10.1016/j.jacc.2014.02.536.
Question (4)