who policy on collaborative tb/hiv activities guidelines for national
TRANSCRIPT

WHO policy on collaborative TB/HIV activities
Guidelines for national programmes and other stakeholders
Annexes for webposting and CD-Rom distribution with the policy guidelines

This is an updated version of a document originally published in 2004 as Interim policy on collaborative TB/HIV activities (WHO/HTM/TB/2004.330; WHO/HTM/HIV/2004.1)
WHO Library Cataloguing-in-Publication Data
WHO policy on collaborative TB/HIV activities: guidelines for national programmes and other stakeholders.
Contents: Annexes for webposting and CD-ROM distribution with the policy guidelines
1.HIV infections. 2.Acquired immunodeficiency syndrome - prevention and control. 3.AIDS-related opportunistic infections - prevention and control. 4.Tuberculosis, Pulmonary - prevention and control. 5.National health programs. 6.Health policy. 7.Guidelines. I.World Health Organization.
ISBN 978 92 4 150300 6 (NLM classification: WC 503.5)
These guidelines were developed in compliance with the process for evidence gathering, assessment and formulation of recommendations, as outlined in the WHO handbook for guideline development (version March 2010).
© World Health Organization 2012
All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; e-mail: [email protected]).
Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html).
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Designed by Creative Lynx, Geneva, Switzerland
WHO/HTM/TB/2012.1 WHO/HIV/2012.1

WHO policy on collaborative TB/HIV activities
Guidelines for national programmes and other stakeholders
Annexes for webposting and CD-Rom distribution
with the policy guidelines

4
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Summary of declaration of interests
All members of the Policy Updating Group were asked to complete a World Health Organization (WHO) Declaration of interests for WHO consultants form. Five members of the group declared a conflict of interest. Constance Benson declared consulting, scientific and technical advisory work on antiretroviral therapy new drug development with Merck, GlaxoSmithKline and ViiV for less than US$ 5000 each. Pedro Cahn declared ongoing research support and consulting work with Abbott for an amount of US$ 3000. He declared receiving US$ 2000 from Bristol-Myers Squibb and US$ 2000 from Tibotec for serving on a speakers’ bureau. He also declared scientific advisory work for Merck, Pfizer, GlaxoSmithKline and Avexa for an amount of US$ 2000 each. Mark Harrington declared giving testimony to the Institute of Medicine of the United States National Academies in panels on multidrug-resistant TB in 2008 and 2009. Charles Holmes declared employment by Gilead up to January 2008 in the clinical research unit focusing on phase I studies of experimental antiretroviral drugs. He declared no financial or other interest in Gilead. Salim S. Abdool Karim declared receiving US$ 2500 from Merck to attend the advisory panel meeting on microbicides in March 2011.
The declared conflicts of interest were discussed within the WHO Steering Group and with the Policy Updating Group before deliberations on the policy document, and it was concluded that these conflicts would not prohibit any of the members from participating in the process. Declarations of interest were collected from all non-WHO reviewers. Four peer reviewers declared potential conflicts of interest. Helen Ayles declared an ongoing research grant for her research unit with Delft Diagnostic Systems of € 100 000 to develop a computer-aided diagnostic for reading digital chest X-rays as well as having received a digital chest X-ray unit for an amount of US$ 250 000. François Boillot declared being the owner, director of and employed by a consulting company providing services in international health including in TB/HIV issues. Susan Swindells declared consulting services (advisory board) with Pfizer in 2008 (US$ 1800) and 2009 (US$ 1750), with Merck in 2009 (US$ 3500), with Tibotec in 2009 (US$ 1500) and with Abbott Molecular in 2010 (US$ 1000). She also declared previous research support to her institution from Bristol Myers Squibb that ended in 2010 (US$ 14929), from Pfizer that ended in 2011 (US$ 28125) and ongoing research support from GlaxoSmithKline for an amount of US$ 104034 and US$ 60676. Jay K. Varma declared non-monetary support (supplies and equipment) in 2010 valued at approximately US$ 10 000 from Cellestis to the government research unit of China and collaborators in Inner Mongolia to examine the prevalence of TB in health-care workers in collaboration with the United States Centers for Disease Control and Prevention. The WHO Steering Group discussed these declarations and concluded that they would not exclude the reviewers from the process. All declarations of conflict of interests are retained on electronic file by the WHO Stop TB Department.
Acknowledgements
The development of these guidelines was financially supported by the Joint United Nations Programme on HIV/AIDS Unified Budget and Workplan (UNAIDS UBW) and the US President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Centers for Disease Control and Prevention (CDC) and the United States Agency for International Development (USAID). Partial support for the systematic reviews on TB and HIV service integration was provided by the Global Fund to Fight AIDS, TB and Malaria.

5
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders is based on the interim policy on collaborative TB/HIV activities published in 2004 by the World Health Organization (WHO) and written by Haileyesus Getahun, Jeroen van Gorkom, Anthony Harries, Mark Harington, Paul Nunn, Jos Perriens, Alasdair Reid and Marco Vitoria on behalf of the TB/HIV policy writing committee for the Global TB/HIV Working Group of the Stop TB Partnership. This updated policy was written by Delphine Sculier and Haileyesus Getahun (Stop TB Department, WHO) in collaboration with the WHO Steering Group.
WHO Steering Group
Rachel Baggaley (HIV/AIDS Department), Haileyesus Getahun (Stop TB Department), Reuben Granich (HIV/AIDS Department), Christian Gunneberg (Stop TB Department), Craig McClure (HIV/AIDS Department), Eyerusalem Negussie (HIV/AIDS Department), Delphine Sculier (Stop TB Department), Marco Vitoria (HIV/AIDS Department).
WHO consultants for systematic and GRADE reviews
Martina Penazzato (Italy), Amitabh Suthar (USA), Helena Legido-Quigley (UK).
Policy updating group
Yibeltal Assefa (Federal HIV/AIDS Prevention and Control Office, Ethiopia), Abdool Karim S. Abdool Salim (Centre for the AIDS Programme of Research in South Africa, South Africa), Rifat Atun (Global Fund to Fight AIDS, Tuberculosis and Malaria (The Global Fund), Switzerland), Constance Benson (University of California, San Diego, USA), Amy Bloom (United States Agency for International Development (USAID), USA), Pedro Cahn (Fundación Huésped, Argentina), Rolando Cedillos (Proyecto Regional VIH SIDA para Centroamérica, El Salvador), Richard E. Chaisson (Johns Hopkins Bloomberg School of Public Health Center for TB Research, USA), Jeremiah Chakaya (Kenya Medical Research Institute (KEMRI), Kenya), Lucy Chesire (Advocacy to Control TB Internationally, Kenya), Mean Chhi Vun (National Center for HIV/AIDS, Dermatology and Sexually Transmitted Diseases, Cambodia), Gavin Churchyard (Aurum Institute for Health Research, South Africa), William Coggin (Office of the US Global AIDS Coordinator (OGAC), USA), Riitta Dlodlo (International Union Against Tuberculosis and Lung Disease (The Union), Zimbabwe), Ade Fakoya, (The Global Fund, Switzerland), Peter Godfrey-Fausset (London School of Hygiene & Tropical Medicine, UK), Anthony Harries (The Union, UK), Mark Harrington (Treatment Action Group, USA), Diane Havlir (University of California, San Francisco, USA), Charles Holmes (OGAC, USA), Nina Kerimi (United Nations Office on Drugs and Crime, Kazakhstan), Robert Makombe (United States Centers for Disease Control and Prevention (CDC), Botswana), Bess Miller (Global AIDS Program, USA), Ya-Diul Mukadi (USAID, USA), Jintanta Ngamvithayapong-Yanai (Research Institute of Tuberculosis, Japan), Alasdair Reid (Joint United Nations Programme on HIV/AIDS, Switzerland), BB Rewari (National AIDS Control Organization, India), Ashurova Rukshona (National Center for Prevention and Control of AIDS, Tajikistan), Holger Schünemann (McMaster University Health Sciences Centre, Canada), Lakhbir Singh Chauhan (Central TB Division, Ministry of Health and Family Welfare, India), Joseph Sitienei (Division of Leprosy, TB and Lung Diseases, Kenya), Alena Skrahina (Republic Scientific and Practical Center of Pulmonology and Tuberculosis, Belarus), John Stover (Future Institutes, USA), Jeroen van Gorkom (KNCV Tuberculosis Foundation, Netherlands).
External peer reviewers
Helen Ayles (ZAMBART Project, Zambia), François-Xavier Blanc (Agence nationale de recherche sur le sida et les hépatites virales, France), François Boillot (Alter-Santé Internationale et Développement, France), John T. Brooks (CDC, USA), Kevin Cain (KEMRI/CDC, Kenya), Wafaa El-Sadr (Columbia University, New York, USA), Eric Goemare (Médecins Sans Frontières (MSF), South Africa), Yared Kebede Haile (KNCV Tuberculosis Foundation, Netherlands), Steve D. Lawn (University of Cape Town, South Africa), Gary Maartens (University of Cape Town, South Africa), Barbara J. Marston (CDC, USA), Elizabeth Marum (CDC, Zambia), Max Meis (KNCV Tuberculosis Foundation, Netherlands), Sue Perez (free lance consultant, USA), Eric S. Pevzner (CDC, USA), Yogan Pillay (Strategic Health Programme, Department of Health, South Africa), Peter Saranchuk (MSF, South Africa), Kenly Sikwese (Global Network of People Living with HIV/AIDS, Zambia), Susan Swindells (University of Nebraska Medical Center, USA), Javid Syed (Treatment Action Group, USA), Nonna Turusbekova (KNCV Tuberculosis Foundation, Netherlands), Marieke van der Werf (KNCV Tuberculosis Foundation, Netherlands), Eric van Praag (Family Health International, United Republic of Tanzania), Jay K. Varma (CDC, China), Lynne Wilkinson (MSF, South Africa), Rony Zachariah (MSF, Belgium).
WHO headquarters and regional offices
Leopold Blanc (Stop TB Department), Puneet Dewan (Regional Office for South-East Asia), Gottfried Hirnschall (HIV/AIDS Department), Khurshid Hyder (Regional Office for South-East Asia), Rafael Lopez Olarte (Regional Office for the Americas), Frank Lule (Regional Office for Africa), Mario Raviglione (Stop TB Department), Ying-Ru Lo (HIV/AIDS Department), Caoimhe Smyth (HIV/AIDS Department).
Editor
Karin Ciceri
Coordination
Delphine Sculier and Haileyesus Getahun (Stop TB Department, WHO).

6
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Contents
Abbreviations 7
Annex 1: Earlier initiation of antiretroviral therapy prevents active tuberculosis in people living with HIV – summary of findings and evaluation of the quality of the evidence 8
Annex 2: Voluntary testing and counselling for HIV benefits patients with diagnosed and presumptive tuberculosis – summary of findings and evaluation of the quality of the evidence 18
Annex 3: Co-trimoxazole preventive therapy reduces morbidity and mortality in tuberculosis patients living with HIV – summary of findings and evaluation of the quality of the evidence 26
7
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Abbreviations
AFB acid-fast bacilli
AIDS acquired immunodeficiency syndrome
ART antiretroviral therapy
CI confidence interval
CPT co-trimoxazole preventive therapy
GRADE grading of recommendations assessment, development and evaluation
HAART highly active antiretroviral therapy
HIV human immunodeficiency virus
HR hazard ratio
IPT isoniazid preventive therapy
IRR incidence rate ratio
NNRTI non-nucleoside reverse transcriptase inhibitor
NRTI nucleoside reverse transcriptase inhibitor
PI protease inhibitor
PICO population, intervention, comparison, outcome
RCT randomized controlled trial
RR risk ratio
SD standard deviation
TB tuberculosis
TB/HIV The intersecting epidemics of TB and HIV
TST tuberculin skin test
VCT voluntary counselling and testing
WHO World Health Organization

8
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
PICO question: Can earlier initiation of antiretroviral therapy (ART) at higher CD4 counts (>350 cells/mm3) be used to prevent active tuberculosis in people living with HIV? Should antiretroviral therapy be used to prevent active tuberculosis?
Population: adults and adolescents living with HIVIntervention: ART at CD4 counts >350 cells/mm3
Comparison: no ART or ART deferred until CD4 counts ≤350 cells/mm3
Outcomes: TB incidence rate
1. Outcomes of interest
Outcomes Relative importance(rank 1 9 most critical) Comment
Tuberculosis incidence rate 9 Critical
2. Literature search strategy and information retrievalStudies were identified using PubMed and the Cochrane Library databases. No systematic reviews were identified using the Cochrane database.
Annex 1Earlier initiation of antiretroviral therapy prevents active tuberculosis in people living with HIV – summary of findings and evaluation of the quality of the evidence
Pubmed Search (346+ citations)
(“Antiretroviral Therapy, Highly Active”[Majr] OR “Anti-HIV gents/therapeutic use”[Majr] OR “Anti-HIV
Agents/administration and dosage”[Majr]) AND (“Tuberculosis/prevention and contro;”[Majr]) OR
“Tuberculosis/epidemiology”[Majr] OR “AIDS-Related Opportunistic Infections/epidemiology”[Majr] OR “AIDS-Related
Opportunistic Infections/prevention and control”[Majr]
By title: 43
By abstract: 21
By article: 6*

9
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Selection criteria
Studies were selected if:
• randomizedandquasi-randomizedcontrolledstudies, includinghistoricallycontrolled trialsorobservationaland cohort studies;
• participantswerepeoplelivingwithHIV;• incidenceratesforbothexposuregroupsofPICOquestionweregiven.
*Excluded observational studies:
• Tuberculosis incidence ratewasnotanoutcome:AiLian (2007),Detels (2001),Eng (2009),Girardi (2000),Losina(2007)andSantaro-Lopes(2002);
• Person-yearsforstudyarmsnotincluded:Lannoy(2008)andMiranda(2007);• InterventionwasnotART:Brodt(1997),Dore(2002),Elzi(2007),Gillini(2002),Ives(2001),Kirk(2000)andMuga(2007).
Investigators in the field were contacted by email. The NA-ACCORD and HIV-CASUAL collaborations shared abstracts which were included. ART-CC updated the data from their study which were included (Girardi et al., 2005). Three relevant studies which were not captured by the MEDLINE search were also included (Golub et al., 2007, Severe et al., 2010, Cohen et al., 2011). Therefore, five additional studies were added to the six studies identified by the literature search.
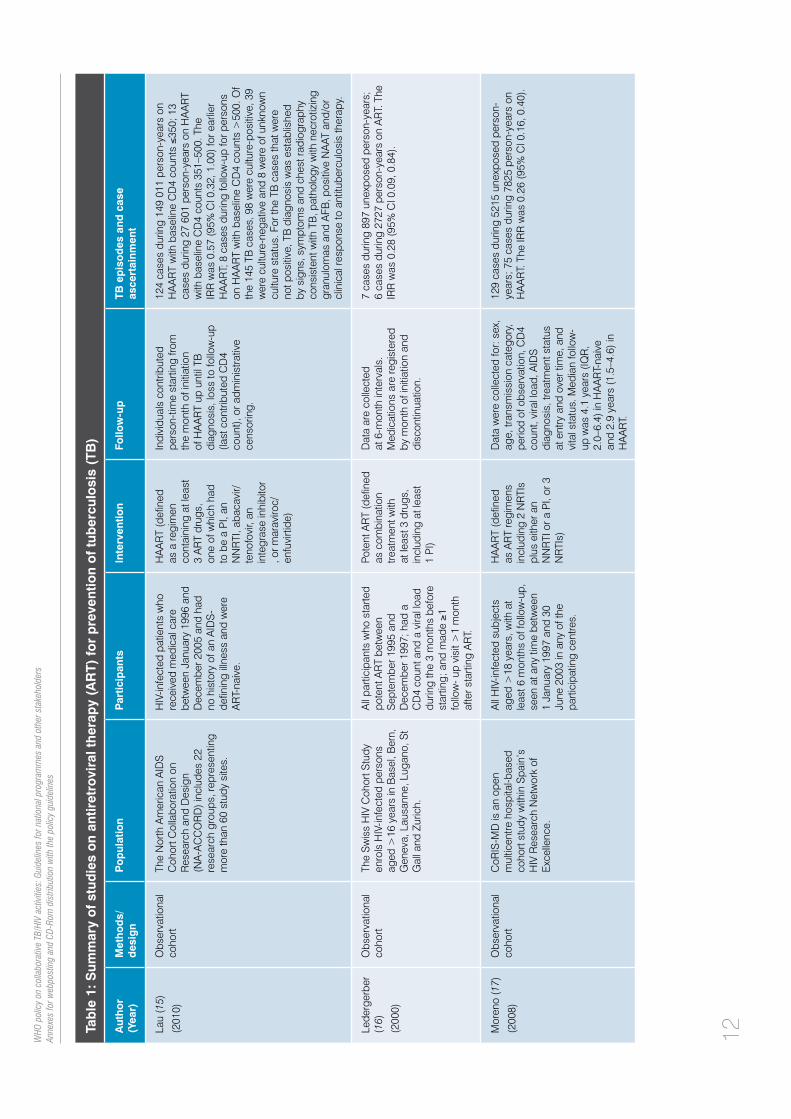
Table 1 summarizes the findings from the 11 studies meeting eligible criteria for the review. ART causes immune reconstitution, prevents the development of opportunistic infections and prevents other HIV-related conditions. Data from observational cohorts have demonstrated the benefits of ART in reducing rates of TB (1–3). Data from South Africa show that TB rates decrease in a stepwise fashion as a result of ART-induced immune reconstitution, with high rates persisting until CD4 counts recover to more than 500 cells/mm3 (4). The rates of TB for South Africans with CD4 counts less than 100 cells/mm3 were approximately 10 times the rate of South Africans with CD4 counts exceeding 500 cells/mm3. HIV-infected South Africans with CD4 counts more than 500 cells/mm3 had about a two-fold increased rate of TB compared with HIV-negative persons. Many people living with HIV in Africa start ART with CD4 counts less than 100 cells/mm3 (5). WHO treatment guidelines published in 2010 recommend initiating ART at CD4 counts ≤350 cells/mm3 regardless of the presence of signs and symptoms (6). Data from observational studies assessed in this review and that did not specify CD4 counts showed that ART halves TB incidence rates. When ART is used in CD4 count stratum 200–350 cells/mm3, TB incidence is reduced up to 88% in observational studies (7,8) and by half in randomized controlled trials (9). In CD4 stratum >350 cells/mm3, ART use reduces TB incidence rates by up to 75% in observational studies (7,8) and by half in randomized controlled trials (10). TB case ascertainment was either definite (culture-confirmed TB) or probable (AFB smear-positive or signs, symptoms and chest radiography consistent with TB or histological finding of caseating/necrotizing granulomas or clinical response to antituberculosis treatment). Observational studies also showed a greater reduction in TB risk (up to 90%) among patients receiving both ART and IPT (11,12).

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n an
tiret
rovi
ral t
her
apy
(AR
T) f
or
pre
vent
ion
of
tub
ercu
losi
s (T
B)
Aut
ho
r (Y
ear)
Met
ho
ds/
des
ign
Po
pul
atio
nP
artic
ipan
tsIn
terv
entio
nFo
llow
-up
TB e
pis
od
es a
nd c
ase
as
cert
ainm
ent
Bad
ri (7
) (2
002)
Obs
erva
tiona
l co
hort
HIV
pat
ient
s at
tend
ing
New
S
omer
set H
ospi
tal a
dult
HIV
cl
inic
, Uni
vers
ity o
f Cap
e To
wn,
be
twee
n 19
92 a
nd 2
001.
Thi
s is
a m
ajor
pub
lic h
ealth
-car
e fa
cilit
y.
Incl
usio
n: a
ged
>15
ye
ars.
Exc
lusi
on: a
cute
op
portu
nist
ic in
fect
ion,
si
gnifi
cant
labo
rato
ry
abno
rmal
ities
, cur
rent
ev
iden
ce o
f act
ive
subs
tanc
e ab
use,
pr
egna
ncy
or la
ctat
ion,
TB
at b
asel
ine
visi
t, us
e of
IP
T in
the
6 m
onth
s pr
ior
to b
asel
ine,
and
trea
tmen
t w
ith im
mun
e-m
odul
atin
g or
sy
stem
ic c
hem
othe
rape
utic
ag
ents
HA
AR
T (d
efine
d as
2
NR
TIs
plus
one
of
the
follo
win
g: (i
) an
NN
RTI
, (ii)
a P
I, or
(ii
i) a
third
NR
TI)
For p
atie
nts
on A
RT,
eve
ry
2–3
mon
ths,
clin
ical
, im
mun
olog
ical
and
vi
rolo
gica
l inf
orm
atio
n w
as
take
n, o
r mor
e fre
quen
tly
if cl
inic
ally
indi
cate
d.
For p
atie
nts
not o
n A
RT,
fo
llow
-up
was
eve
ry 3
–6
mon
ths.
Mea
n fo
llow
-up
in
thos
e ex
pose
d to
AR
T w
as
sign
ifica
ntly
gre
ater
than
in
the
cont
rols
(16.
8 (S
D 8
.3)
vs 1
3.2
(SD
15.
5) m
onth
s).
2 ca
ses
durin
g 10
0.1
pers
on-y
ears
on
AR
T w
ith b
asel
ine
CD
4 co
unts
>35
0 ce
lls/m
m3 ;
14
case
s du
ring
388.
3 pe
rson
-yea
rs o
ff A
RT
with
ba
selin
e C
D4
coun
ts >
350.
Adj
uste
d R
R w
as
0.36
(95%
CI 0
.10
to 1
.74)
for t
his
CD
4 st
ratu
m.
2 ca
ses
durin
g 12
1.2
pers
on-y
ears
on
AR
T w
ith b
asel
ine
CD
4 co
unts
200
–350
; 27
case
s du
ring
225
pers
on-y
ears
off
AR
T w
ith b
asel
ine
CD
4 co
unts
200
–350
. Adj
uste
d R
R w
as 0
.12
(95%
0.0
3 to
0.5
3) fo
r thi
s C
D4
stra
tum
.
Acr
oss
all C
D4
stra
ta, o
f the
9 T
B c
ases
on
AR
T, 5
wer
e de
finite
(cul
ture
/aut
opsy
co
nfirm
ed) a
nd 4
wer
e pr
obab
le (p
rese
nce
of A
FB o
r his
tolo
gica
l find
ing
of c
asea
ting
gran
ulom
ata)
. Of t
he 8
2 TB
cas
es o
ff A
RT,
48
wer
e pr
obab
le a
nd 3
4 w
ere
defin
ite.
del A
mo
(8)
(201
1)
Obs
erva
tiona
l co
hort
This
ana
lysi
s fro
m th
e H
IV-C
AUS
AL
Col
labo
ratio
n in
clud
es 1
1 ob
serv
atio
nal
coho
rts fr
om 1
996
to 2
007.
Th
e co
horts
are
in th
e U
K, t
he
Net
herla
nds,
Fra
nce,
Spa
in
and
the
US
A.
HIV
-infe
cted
indi
vidu
als
who
wer
e ag
ed ≥
18 y
ears
, an
tiret
rovi
ral n
aive
, with
out
AID
S, n
ot p
regn
ant,
and
in
who
m C
D4
coun
ts a
nd v
iral
load
wer
e m
easu
red
with
in
6 m
onth
s of
eac
h ot
her a
t ba
selin
e. In
divi
dual
s w
ith
TB d
urin
g th
e fir
st m
onth
of
follo
w u
p w
ere
excl
uded
(p
reva
lent
TB
cas
e).
Com
bine
d A
RT
(defi
ned
as a
re
gim
en in
clud
ing
>3
AR
Ts, 2
rito
navi
r-bo
oste
d P
Is, o
r 1
NN
RTI
and
1
boos
ted
PI)
For e
ach
patie
nt, f
ollo
w-u
p en
ded
at th
e ea
rlies
t of:
TB d
iagn
osis
, dea
th, 1
2 m
onth
s af
ter t
he m
ost r
ecen
t la
bora
tory
mea
sure
men
t, pr
egna
ncy
(if k
now
n),
or th
e co
hort-
spec
ific
adm
inis
trativ
e en
d of
follo
w-
up.
The
over
all h
azar
d ra
tio o
f TB
for c
ombi
ned
AR
T w
as 0
.56
(95%
CI 0
.44–
0. 7
2).
The
haza
rd ra
tios
wer
e si
mila
r for
indi
vidu
als
with
bas
elin
e C
D4
coun
ts >
350
(0.5
0, 9
5% C
I 0.
36–0
.69)
and
200
–350
(0.4
5, 9
5% C
I 0.2
7,
0.74
).
TB c
ases
wer
e di
agno
sed
acco
rdin
g to
st
anda
rd c
linic
al p
ract
ice
in E
urop
e an
d th
e U
SA
.
Gira
rdi (13
)
(200
5)
Obs
erva
tiona
l co
hort
The
AR
T C
ohor
t Col
labo
ratio
n (A
RT-
CC
) is
an in
tern
atio
nal
colla
bora
tion
of c
ohor
t stu
dies
fro
m E
urop
e an
d N
orth
A
mer
ica.
Thi
s st
udy
incl
uded
12
coh
orts
.
Ant
iretro
vira
l-nai
ve s
ubje
cts
had
to b
e ag
ed ≥
16 y
ears
. D
ata
wer
e fro
m s
ubje
cts
who
sta
rted
AR
T be
twee
n 19
96 a
nd 2
008
(AR
T-C
C
upda
ted
the
data
pre
sent
ed
in th
e 20
05 a
rticl
e). F
ollo
w-
up w
as c
enso
red
at 3
yea
rs
from
sta
rt of
AR
T
HA
AR
T (d
efine
d as
at
leas
t 3 d
rugs
, in
clud
ing
PIs
, N
NR
TIs
and
NR
TIs)
Dat
a on
HA
AR
T re
gim
en
(PI/N
NR
TI/N
RTI
-bas
ed),
CD
4 co
unt,
vira
l loa
d,
gend
er, a
ge, y
ear o
f HA
AR
T in
itiat
ion
and
risk
grou
p (M
SM
, inj
ectio
n dr
ug u
ser,
hete
rose
xual
, blo
od-p
rodu
ct
reci
pien
t, ot
her/n
ot k
now
n)
wer
e co
llect
ed
676
case
s du
ring
124
669
pers
on-y
ears
on
HA
AR
T w
ith b
asel
ine
CD
4 co
unts
≤35
0; 5
8 ca
ses
durin
g 23
420
per
son-
year
s on
HA
AR
T w
ith b
asel
ine
CD
4 co
unts
351
–500
.
The
IRR
was
0.4
6 (9
5% C
I 0.3
5, 0
.60)
for
high
er v
s lo
wer
bas
elin
e C
D4
coun
ts a
t HA
AR
T in
itiat
ion.
All
TB c
ases
und
erw
ent a
ntitu
berc
ulos
is
treat
men
t. S
ince
the
stan
dard
of m
edic
al
care
is to
con
firm
TB
prio
r to
star
ting
antit
uber
culo
sis
treat
men
t, in
vest
igat
ors
indi
cate
that
all
the
TB c
ases
wer
e cu
lture
-co
nfirm
ed.
10WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n an
tiret
rovi
ral t
her
apy
(AR
T) f
or
pre
vent
ion
of
tub
ercu
losi
s (T
B)
Aut
ho
r (Y
ear)
Met
ho
ds/
des
ign
Po
pul
atio
nP
artic
ipan
tsIn
terv
entio
nFo
llow
-up
TB e
pis
od
es a
nd c
ase
as
cert
ainm
ent
Gol
ub (12)
(200
9)
Obs
erva
tiona
l co
hort
HIV
pat
ient
s re
ceiv
ing
prim
ary
HIV
car
e at
two
clin
ics
affil
iate
d w
ith th
e U
nive
rsity
of t
he
Witw
ater
sran
d: th
e Pe
rinat
al
HIV
Res
earc
h U
nit (
PH
RU
) in
Sow
eto,
a la
rge,
urb
an s
ettin
g,
and
the
Tint
swal
o H
ospi
tal,
a re
mot
e, ru
ral c
linic
in
Mpu
mal
anga
Pro
vinc
e.
HIV
-infe
cted
adu
lts a
ged
>18
yea
rs. N
o ex
clus
ion
crite
ria li
sted
HA
AR
T (n
ot d
efine
d)
and/
or IP
TTi
me
betw
een
visi
ts is
sc
hedu
led
to b
e 4–
7 m
onth
s, b
ut p
atie
nts
may
vi
sit t
he c
linic
at a
ny ti
me.
Fo
llow
-up
data
col
lect
ion
focu
ses
on c
linic
al
diag
nose
s, s
ympt
oms
and
long
itudi
nal d
ata
incl
udin
g he
ight
and
wei
ght,
smok
ing
stat
us, a
lcoh
ol
cons
umpt
ion
and
mea
sure
s of
soc
ioec
onom
ic s
tatu
s.
Labo
rato
ry te
sts
incl
ude
CD
4 an
d fu
ll bl
ood
coun
ts
at re
crui
tmen
t and
eve
ry 6
m
onth
s.
200
case
s of
TB
dur
ing
2815
une
xpos
ed
pers
on-y
ears
; 44
case
s du
ring
952
pers
on-
year
s on
HA
AR
T; 1
cas
e du
ring
93 p
erso
n-ye
ars
on IP
T an
d A
RT.
The
IRR
for H
AA
RT
was
0.
65 (0
.46–
0.91
). Th
e IR
R fo
r IP
T an
d H
AA
RT
was
0.1
5 (0
.00–
0.85
). Th
e ad
just
ed H
R fo
r H
AA
RT
was
0.3
6 (0
.25,
0.5
1). T
he a
djus
ted
HR
fo
r IP
T an
d H
AA
RT
was
0.1
1 (0
.02,
0.7
8).
Gol
ub (11)
(200
7)
Obs
erva
tiona
l co
hort
Bas
elin
e m
edic
al re
cord
s w
ere
anal
ysed
for a
2-y
ear p
erio
d (fr
om 1
Sep
tem
ber 2
003
to 1
S
epte
mbe
r 200
5) in
29
publ
ic
clin
ics
in R
io d
e Ja
neiro
, Bra
zil.
Patie
nts
who
had
mad
e at
le
ast o
ne v
isit
to o
ne o
f the
cl
inic
s (fr
om 1
Sep
tem
ber
2003
to 1
Sep
tem
ber 2
005)
an
d w
ho re
ceiv
ed th
eir
prim
ary
care
from
the
clin
ics
wer
e in
clud
ed. P
atie
nts
who
at
tend
ed th
e cl
inic
to c
olle
ct
antir
etro
vira
l med
icat
ions
pr
escr
ibed
by
a pr
ivat
e ph
ysic
ian
wer
e ex
clud
ed,
as w
ere
patie
nts
who
die
d be
fore
1 S
epte
mbe
r 200
3.
AR
T (n
ot d
efine
d)
and/
or IP
TFo
llow
-up
ende
d at
TB
di
agno
sis
or th
e ea
rlier
of
thei
r las
t vis
it
to a
n H
IV c
linic
, the
dat
e of
ad
min
istra
tive
cens
orin
g or
de
ath.
Info
rmat
ion
colle
cted
in
clud
ed a
ge, s
ex, d
ate
of
HIV
dia
gnos
is, t
reat
men
t hi
stor
y (a
ntire
trovi
ral d
rugs
, IP
T), d
ates
of o
ppor
tuni
stic
di
seas
es in
clud
ing
TB, a
nd
resu
lts o
f dia
gnos
tic te
sts
incl
udin
g C
D4
coun
ts, H
IV
vira
l loa
ds a
nd T
ST.
155
case
s du
ring
3865
une
xpos
ed p
erso
n-ye
ars;
221
cas
es d
urin
g 11
627
pers
on-y
ears
on
AR
T; 1
0 ca
ses
durin
g 12
53 p
erso
n-ye
ars
on A
RT
and
IPT.
IRR
for A
RT
was
0.4
8 (0
.39,
0.
59).
IRR
for A
RT
and
IPT
was
0.2
0 (0
.09,
0.
91).
Adj
uste
d H
R w
as 0
.41
(0.3
1, 0
.54)
for
AR
T. A
djus
ted
HR
was
0.2
4 (0
.11,
0.5
3) fo
r A
RT
and
IPT.
Jone
s (14)
(200
0)
Obs
erva
tiona
l co
hort
The
Adu
lt/A
dole
scen
t S
pect
rum
of H
IV D
isea
se
proj
ect i
s a
mul
ticen
tre
obse
rvat
iona
l coh
ort s
tudy
in
clud
ing
site
s in
Atla
nta,
GA
; D
alla
s, H
oust
on, a
nd S
an
Ant
onio
, TX;
Den
ver,
CO
; D
etro
it, M
I; Lo
s A
ngel
es, C
A;
Sea
ttle,
WA
; New
Orle
ans,
LA
; N
ew Y
ork,
NY;
and
Bay
amon
, P
uerto
Ric
o.
HIV
-infe
cted
per
sons
ar
e id
entifi
ed a
t the
ir fir
st
heal
th-c
are
enco
unte
r re
gard
less
of t
he s
tage
of
thei
r HIV
infe
ctio
n. A
ll pa
tient
s ag
ed >
13 y
ears
w
ho w
ere
infe
cted
with
H
IV a
nd w
ho a
ttend
ed
parti
cipa
ting
clin
ics
durin
g th
e st
udy
perio
d w
ere
elig
ible
for e
nrol
men
t.
HA
AR
T (d
efine
d as
trip
le th
erap
y w
ith 2
NR
TIs
and
an N
NR
TI o
r PI,
or
any
com
bina
tion
incl
udin
g a
PI)
On
succ
essi
ve 6
-mon
th
follo
w-u
p in
terv
als,
med
ical
re
cord
s ar
e re
view
ed fo
r ill
ness
es, A
IDS
-defi
ning
co
nditi
ons,
pre
scrip
tions
, la
bora
tory
test
s an
d m
edic
al
care
util
izat
ion.
TB
inci
denc
e w
as a
sses
sed
by e
xam
inin
g th
e fir
st p
rosp
ectiv
e oc
curr
ence
of T
B fr
om
Janu
ary
1996
to J
une
1998
.
45 c
ases
dur
ing
6250
une
xpos
ed p
erso
n-ye
ars;
7 c
ases
dur
ing
3684
per
son-
year
s on
H
AA
RT.
The
IRR
was
0.2
(0.1
, 0.5
).
11
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines
Tab
le 1
: Sum
mar
y o
f st
udie
s o
n an
tiret
rovi
ral t
her
apy
(AR
T) f
or
pre
vent
ion
of
tub
ercu
losi
s (T
B)
Aut
ho
r (Y
ear)
Met
ho
ds/
des
ign
Po
pul
atio
nP
artic
ipan
tsIn
terv
entio
nFo
llow
-up
TB e
pis
od
es a
nd c
ase
as
cert
ainm
ent
Lau
(15)
(201
0)
Obs
erva
tiona
l co
hort
The
Nor
th A
mer
ican
AID
S
Coh
ort C
olla
bora
tion
on
Res
earc
h an
d D
esig
n (N
A-A
CC
OR
D) i
nclu
des
22
rese
arch
gro
ups,
repr
esen
ting
mor
e th
an 6
0 st
udy
site
s.
HIV
-infe
cted
pat
ient
s w
ho
rece
ived
med
ical
car
e be
twee
n Ja
nuar
y 19
96 a
nd
Dec
embe
r 200
5 an
d ha
d no
his
tory
of a
n A
IDS
-de
finin
g ill
ness
and
wer
e A
RT-
naiv
e.
HA
AR
T (d
efine
d as
a re
gim
en
cont
aini
ng a
t lea
st
3 A
RT
drug
s,
one
of w
hich
had
to
be
a P
I, an
N
NR
TI, a
baca
vir/
teno
fovi
r, an
in
tegr
ase
inhi
bito
r , o
r mar
aviro
c/en
fuvi
rtide
)
Indi
vidu
als
cont
ribut
ed
pers
on-ti
me
star
ting
from
th
e m
onth
of i
nitia
tion
of H
AA
RT
up u
ntil
TB
diag
nosi
s, lo
ss to
follo
w-u
p
(last
con
tribu
ted
CD
4 co
unt),
or a
dmin
istra
tive
cens
orin
g.
124
case
s du
ring
149
011
pers
on-y
ears
on
HA
AR
T w
ith b
asel
ine
CD
4 co
unts
≤35
0; 1
3 ca
ses
durin
g 27
601
per
son-
year
s on
HA
AR
T w
ith b
asel
ine
CD
4 co
unts
351
–500
. The
IR
R w
as 0
.57
(95%
CI 0
.32,
1.0
0) fo
r ear
lier
HA
AR
T; 8
cas
es d
urin
g fo
llow
-up
for p
erso
ns
on H
AA
RT
with
bas
elin
e C
D4
coun
ts >
500.
Of
the
145
TB c
ases
, 98
wer
e cu
lture
-pos
itive
, 39
wer
e cu
lture
-neg
ativ
e an
d 8
wer
e of
unk
now
n cu
lture
sta
tus.
For
the
TB c
ases
that
wer
e no
t pos
itive
, TB
dia
gnos
is w
as e
stab
lishe
d by
sig
ns, s
ympt
oms
and
ches
t rad
iogr
aphy
co
nsis
tent
with
TB
, pat
holo
gy w
ith n
ecro
tizin
g gr
anul
omas
and
AFB
, pos
itive
NA
AT a
nd/o
r cl
inic
al re
spon
se to
ant
itube
rcul
osis
ther
apy.
Lede
rger
ber
(16)
(200
0)
Obs
erva
tiona
l co
hort
The
Sw
iss
HIV
Coh
ort S
tudy
en
rols
HIV
-infe
cted
per
sons
ag
ed >
16 y
ears
in B
asel
, Ber
n,
Gen
eva,
Lau
sann
e, L
ugan
o, S
t G
all a
nd Z
uric
h.
All
parti
cipa
nts
who
sta
rted
pote
nt A
RT
betw
een
Sep
tem
ber 1
995
and
Dec
embe
r 199
7; h
ad a
C
D4
coun
t and
a v
iral l
oad
durin
g th
e 3
mon
ths
befo
re
star
ting;
and
mad
e ≥1
fo
llow
- up
visi
t >1
mon
th
afte
r sta
rting
AR
T.
Pote
nt A
RT
(defi
ned
as c
ombi
natio
n tre
atm
ent w
ith
at le
ast 3
dru
gs,
incl
udin
g at
leas
t 1
PI)
Dat
a ar
e co
llect
ed
at 6
-mon
th in
terv
als.
M
edic
atio
ns a
re re
gist
ered
by
mon
th o
f ini
tiatio
n an
d di
scon
tinua
tion.
7 ca
ses
durin
g 89
7 un
expo
sed
pers
on-y
ears
; 6
case
s du
ring
2727
per
son-
year
s on
AR
T. T
he
IRR
was
0.2
8 (9
5% C
I 0.0
9, 0
.84)
.
Mor
eno
(17)
(200
8)
Obs
erva
tiona
l co
hort
CoR
IS-M
D is
an
open
m
ultic
entre
hos
pita
l-bas
ed
coho
rt st
udy
with
in S
pain
’s
HIV
Res
earc
h N
etw
ork
of
Exc
elle
nce.
All
HIV
-infe
cted
sub
ject
s ag
ed >
18 y
ears
, with
at
leas
t 6 m
onth
s of
follo
w-u
p,
seen
at a
ny ti
me
betw
een
1 Ja
nuar
y 19
97 a
nd 3
0 Ju
ne 2
003
in a
ny o
f the
pa
rtici
patin
g ce
ntre
s.
HA
AR
T (d
efine
d as
AR
T re
gim
ens
incl
udin
g 2
NR
TIs
plus
eith
er a
n N
NR
TI o
r a P
I, or
3
NR
TIs)
Dat
a w
ere
colle
cted
for:
sex,
ag
e, tr
ansm
issi
on c
ateg
ory,
pe
riod
of o
bser
vatio
n, C
D4
coun
t, vi
ral l
oad,
AID
S
diag
nosi
s, tr
eatm
ent s
tatu
s at
ent
ry a
nd o
ver t
ime,
and
vi
tal s
tatu
s. M
edia
n fo
llow
-up
was
4.1
yea
rs (I
QR
, 2.
0–6.
4) in
HA
AR
T-na
ive
and
2.9
year
s (1
.5–4
.6) i
n H
AA
RT.
129
case
s du
ring
5215
une
xpos
ed p
erso
n-ye
ars;
75
case
s du
ring
7825
per
son-
year
s on
H
AA
RT.
The
IRR
was
0.2
6 (9
5% C
I 0.1
6, 0
.40)
.
12WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n an
tiret
rovi
ral t
her
apy
(AR
T) f
or
pre
vent
ion
of
tub
ercu
losi
s (T
B)
Aut
ho
r (Y
ear)
Met
ho
ds/
des
ign
Po
pul
atio
nP
artic
ipan
tsIn
terv
entio
nFo
llow
-up
TB e
pis
od
es a
nd c
ase
as
cert
ainm
ent
Coh
en (10)
(2
011)
Ran
dom
ized
co
ntro
lled
trial
The
trial
had
glo
bal
repr
esen
tatio
n w
ith 1
3 si
tes
in B
otsw
ana,
Bra
sil,
Indi
a,
Ken
ya, M
alaw
i, S
outh
Afri
ca,
Thai
land
, the
Uni
ted
Sta
tes
and
Zim
babw
e.
HIV
-ser
odis
cord
ant c
oupl
es
in w
hich
the
HIV
-infe
cted
pa
rtner
is A
RT-
naiv
e an
d ha
s a
CD
4 co
unt b
etw
een
350
and
550
cells
/mm
3
The
AR
T re
gim
ens
in th
is s
tudy
wer
e co
nsis
tent
with
W
HO
gui
delin
es
All
parti
cipa
nts
com
plet
ed
mon
thly
follo
w-u
p vi
sits
th
roug
hout
the
stud
y. F
or
thos
e on
AR
T, la
bora
tory
and
ad
here
nce
mea
sure
men
ts
took
pla
ce. F
or th
ose
not
on A
RT
labo
rato
ry a
nd
coun
selli
ng to
ok p
lace
.
33 c
ases
am
ong
the
877
adul
ts in
itiat
ing
AR
T w
ith C
D4
coun
ts <
350
cells
/µL;
17
case
s am
ong
the
886
peop
le in
itiat
ing
AR
T w
ith C
D4
coun
ts >
350
cells
/µL.
Thi
s tra
nsla
ted
into
an
RR
0.5
1 (0
.28–
0.91
).a
Sev
ere
(9)
(201
0)R
ando
miz
ed
cont
rolle
d tri
alTh
e st
udy
was
con
duct
ed a
t th
e ce
ntre
of t
he H
aitia
n G
roup
fo
r the
Stu
dy o
f Kap
osi’s
S
arco
ma
and
Opp
ortu
nist
ic
Infe
ctio
ns in
Por
t-au-
Prin
ce,
Hai
ti
HIV
-infe
cted
par
ticip
ants
ag
ed ≥
18 y
ears
with
CD
4 co
unts
from
200
and
350
ce
lls/m
m3 w
ithin
45
days
be
fore
enr
olm
ent w
ere
incl
uded
. Par
ticip
ants
with
a
hist
ory
of a
n A
IDS
-defi
ning
ill
ness
or w
ho h
ad re
ceiv
ed
AR
T pr
evio
usly
wer
e ex
clud
ed
Trea
tmen
t inc
lude
d la
miv
udin
e,
zido
vudi
ne, a
nd
efav
irenz
Adh
eren
ce w
as m
easu
red
ever
y 6
mon
ths
usin
g a
ques
tionn
aire
. Adv
erse
ev
ents
wer
e m
onito
ring
usin
g D
AID
S c
riter
ia.
Com
plet
e bl
ood
coun
t, liv
er e
nzym
e te
sts
and
seru
m c
hem
ical
test
s w
ere
repe
ated
eve
ry 3
mon
ths
for p
artic
ipan
ts o
n A
RT.
C
D4
resu
lts w
ere
colle
cted
6-
mon
thly.
36 c
ases
of T
B a
mon
g th
e 39
3 pe
ople
who
w
ere
rand
omiz
ed to
def
er A
RT
until
thei
r CD
4 co
unts
wer
e <
200;
18
case
s of
TB
am
ong
the
380
peop
le w
ho w
ere
rand
omiz
ed to
initi
ate
AR
T im
med
iate
ly (i
.e. b
etw
een
200
and
350)
. Th
is tr
ansl
ated
into
an
RR
of 0
.52
(0.3
0–0.
89).b
AFB,
aci
d-fa
st b
acilli
; ART
, ant
iretro
vira
l the
rapy
; HAA
RT, h
ighl
y ac
tive
antir
etro
vira
l the
rapy
; HIV
, hum
an im
mun
odefi
cien
cy v
irus;
IPT,
ison
iazid
pre
vent
ive
ther
apy;
IQR,
inte
rqua
rtile
rang
e; IR
R,
inci
denc
e ra
te ra
tio; N
AAT,
nuc
leic
aci
d am
plifi
catio
n te
st; N
NRTI
, non
-nuc
leos
ide
reve
rse
trans
crip
tase
inhi
bito
r; NR
TI, n
ucle
osid
e re
vers
e tra
nscr
ipta
se in
hibi
tor;
PI, p
rote
ase
inhi
bito
r; RR
, ris
k ra
tio; S
D, s
tand
ard
devi
atio
n; T
B, tu
berc
ulos
is; T
ST, t
uber
culin
ski
n te
st
a
The
AIDS
Clin
ical
Tria
ls G
roup
defi
nitio
n fo
r con
firm
ed o
r pro
babl
e TB
was
use
d:
•ConfirmedpulmonaryTB:M
ycob
acte
rium
tube
rcul
osis
cul
ture
d fro
m s
putu
m, b
ronc
ho-a
lveo
lar l
avag
e flu
id o
r lun
g tis
sue.
•ProbablepulmonaryTB:(i)clinicalsyndromeconsistentwithpulmonaryTB,including>1ofthefollowing:fever>38°C,nightsweats,productivecough,haemoptysis,weightloss;
and(ii)AFBsmearfromsputum,gastricaspirate,broncho-alveolarlavagefluidorlungtissue;orAFBidentifiedonhistopathologyoflungtissueand
M. a
vium
com
plex
and
oth
er a
typi
cal
myc
obac
teria
exc
lude
d; a
nd(iii)abnormalchestX-rayconsistentwithpulmonaryTB;a
nd(iv)specificmulti-drugantituberculoustherapyinitiated.
•ConfirmedextrapulmonaryTB:positivecultureforM
. tub
ercu
losi
s fro
m e
xtra
pulm
onar
y si
te.
• ProbableextrapulmonaryTB:(i)positiveAFBsmearorapositivehistopathologyfromanextrapulmonarysite;a
nd(ii)>1ofthefollowingsignsorsymptomsconsistentwithaclinical
syndromeforextrapulmonaryTB:fever>38°C,nightsweats,malaise,weightlossand/oradenopathy;a
nd(iii)specificmulti-drugantituberculoustherapyinitiated.
bTheAmericanThoracicSociety’scasedefinitionwasused:twoofthefollowingthreecriteriaweremet:(i)>1offever(temperature>38ºC)foratleast1week,nightsweatsforatleast
1 week,weightloss(>10%bodyweight),cough,dyspnoea,haemoptysisorlymphadenopathyforatleast4weeks;(ii)AFBvisibleinsputum,M
. tub
ercu
losi
s cu
lture
d fro
m s
putu
m, o
r hi
stop
atho
logi
cal fi
ndin
gs in
bio
psy
sam
ples
con
sist
ent w
ith m
ycob
acte
rial d
isea
se; a
nd(iii)achestradiographinterpretedashighlysuggestiveofTBbytwoindependentradiologists.Clinical
responsetoantituberculosismedicationswasdefinedasresolutionofclinicalsymptomsandsigns,anda50%decreaseinthesizeoftheeffusion,infiltrateorhilaradenopathyat8weeks,as
judg
ed b
y an
inde
pend
ent r
adio
logi
st.
13
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

14
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
3. GRADE profileThe quality of evidence across a body of evidence was assessed using the GRADE approach. For systematic reviews, the GRADE approach defines the quality of a body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the quantity of specific interest.
The quality rating across studies has four levels: high, moderate, low, or very low. Randomized trials are categorized as high quality but can be downgraded. Observational studies are categorized as low but can be upgraded. Factors that decrease the quality of evidence include design limitations, inconsistency among studies, indirectness of evidence and imprecision of effect measures, among other biases. Factors that can increase the quality level of a body of evidence include a large magnitude of effect, plausible confounding reducing a demonstrated effect and a dose-response gradient.
The GRADE Profiler software was used to perform the GRADE analyses (GRADE profiler version 3.2.2).

Tab
le 2
: Sh
oul
d a
ntir
etro
vira
l th
erap
y (A
RT)
be
used
to
pre
vent
act
ive
tub
ercu
losi
s (T
B)?
Set
ting
s: A
ll
Bib
liogr
aphy
: Bad
ri et
al.
(200
2), C
ohen
et a
l. (2
011)
, del
Am
o et
al.
(201
1), G
olub
et a
l. (2
007)
, Gol
ub e
t al.
(200
9), J
ones
et a
l. (2
000)
, Led
erge
rber
et a
l. (1
999)
, Mor
eno
et a
l. (2
008)
, Sev
ere
et a
l. (2
010)
Qua
lity
asse
ssm
ent
Sum
mar
y o
f fin
din
gs
Impo
rtan
ce
No
of
pat
ient
sE
ffec
t
Qual
ityNo
of
stud
ies
Desi
gnLi
mita
tions
Inco
nsis
tenc
yIn
dire
ctne
ssIm
prec
isio
nOt
her
cons
ider
atio
nsAR
TCo
ntro
lRe
lativ
e (9
5% C
I)Ab
solu
te
TB in
cid
ence
, bas
elin
e C
D4
coun
ts 2
00–3
50 (
ob
serv
atio
nal)
2Ob
serv
atio
nal
stud
ies1
No s
erio
us
limita
tions
No s
erio
us
inco
nsis
tenc
ySe
rious
in
dire
ctne
ss2
No s
erio
us
impr
ecis
ion
Stro
ng
asso
ciat
ion3
Not r
epor
ted
Not r
epor
ted
RR 0
.39
(0.2
4–0.
63)4
Not e
stim
ated
sin
ce
rate
dat
a us
edLO
WCR
ITIC
AL
TB in
cid
ence
, bas
elin
e C
D4
coun
ts 2
00–3
50 (
rand
om
ized
co
ntro
lled
tri
als)
1Ra
ndom
ized
cont
rolle
d tri
al5
No s
erio
us
limita
tions
No s
erio
us
inco
nsis
tenc
yNo
ser
ious
in
dire
ctne
ssNo
ser
ious
im
prec
isio
nNo
ne18
/380
36/3
93RR
0.5
2 (0
.30–
0.89
)6
44 fe
wer p
er 1
000
(from
10
fewe
r to
64
fewe
r)HI
GHCR
ITIC
AL
TB in
cid
ence
, bas
elin
e C
D4
coun
ts >
350
(ob
serv
atio
nal)
2Ob
serv
atio
nal
stud
ies1
No s
erio
us
limita
tions
No s
erio
us
inco
nsis
tenc
ySe
rious
in
dire
ctne
ss2
No s
erio
us
impr
ecis
ion
Stro
ng
asso
ciat
ion3
Not r
epor
ted
Not r
epor
ted
RR 0
.49
(0.3
6–0.
68)4
Not e
stim
ated
sin
ce
rate
dat
a us
edLO
WCR
ITIC
AL
TB in
cid
ence
, bas
elin
e C
D4
coun
ts >
350
(ran
do
miz
ed c
ont
rolle
d t
rial
s)
1Ra
ndom
ized
cont
rolle
d tri
al7
No s
erio
us
limita
tions
No s
erio
us
inco
nsis
tenc
yNo
ser
ious
in
dire
ctne
ssNo
ser
ious
im
prec
isio
nNo
ne17
/886
33/8
77RR
0.5
1 (0
.29–
0.91
)6
18 fe
wer p
er 1
000
(from
3 fe
wer t
o 27
fe
wer)
HIGH
CRIT
ICAL
TB in
cid
ence
, bas
elin
e C
D4
coun
ts n
ot
pro
vid
ed
5Ob
serv
atio
nal
stud
ies8
No s
erio
us
limita
tions
No s
erio
us
inco
nsis
tenc
yNo
ser
ious
in
dire
ctne
ssNo
ser
ious
im
prec
isio
nSt
rong
as
soci
atio
n213
2/15
188
(0.9
%)9
381/
1517
7 (2
.5%
)9RR
0.4
7 (0
.41–
0.53
)4No
t est
imat
ed s
ince
ra
te d
ata
used
MOD
ERAT
ECR
ITIC
AL
TB in
cid
ence
, AR
T an
d IP
T (b
asel
ine
CD
4 co
unts
no
t p
rovi
ded
)
2Ob
serv
atio
nal
stud
ies10
serio
us11
No s
erio
us
inco
nsis
tenc
yNo
ser
ious
in
dire
ctne
ssNo
ser
ious
im
prec
isio
nVe
ry s
trong
as
soci
atio
n1211
/134
6 (0
.8%
)935
5/66
80
(5.3
%)9
RR 0
.15
(0.0
8–0.
28)4
Not e
stim
ated
sin
ce
rate
dat
a us
edM
ODER
ATE
CRIT
ICAL
1delAmoetal.(2011)andBadrietal.(2002).
2delAmoetal(2011)studyconductedinEuropeandNorthAmerica,
setti
ngs
with
low
TB
trans
mis
sion
.
3LargemagnitudeofeffectasdefinedbyGRADE(RRestimate<0.5).
4Themeasureofeffectisanincidencerateratio.
5Severeetal.(2010).
6
The
mea
sure
of e
ffect
is a
risk
ratio
.
7Cohenetal.(2011).
8Golubetal.(2007),Golubetal.(2009),Morenoetal.(2008),Ledergerber
etal.(2000),andJonesetal.(2000).
9NumeratorisTBcases,denominatorisperson-yearsatrisk.
10Golubetal.(2007)andGolubetal.(2009).
11Antiretroviraltherapynotdefinedineitherstudy(Golubetal.2007and
Golubetal.2009).
12VerylargemagnitudeofeffectasdefinedbyGRADE(RRestimate<0.2).
15
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

16
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
4. Risk and benefits assessment
Recommendation: People living with HIV with CD4 counts >350 cells/mm3 should receive ART to prevent active TB
Population: People living with HIV with CD4 counts >350 cells/mm3
Intervention: Antiretroviral therapy
Factor Decision Explanation
Quality of evidence High The reduction in tuberculosis incidence is supported by HIGH quality randomized trial
evidence
Benefits or desired effects
Strong (benefits outweigh risks)
Reduction in tuberculosis incidence.
Additional benefits of ART in reducing mortality, other HIV related morbidity, and HIV transmission
Risks or undesired effects
Reduction in tuberculosis incidence.
Additional benefits of ART in reducing mortality, other HIV related morbidity, and HIV transmission
Values and preferences Variable
Improved quality of HIV treatment and care.
Also prevents life-threatening opportunistic infections, increases survival, and prevents HIV transmission to others
Life-long therapy with issues of adherence and side effects in the long term.
High pill burden when ART taken with other preventive or curative treatment.
Costs Weak
Costs will increase as the volume of patients will at least double, with impact on drug and non-drug costs.
Evidence on long run cost savings only demonstrated by mathematical modelling.
Cheaper interventions exist such as isoniazid preventive therapy which is yet to be scaled-up
Feasibility Weak
A move to CD4 threshold >350 for ART initiation will at least double the number of eligible patients to start ART. In a context of low uptake, late presentation for treatment and limited resources in majority of high HIV prevalence settings, it can generate confusing messaging, competing forces in terms of infrastructure demand and very serious issues of equity towards patients with lower CD4 counts and who have not accessed yet ART
Not recommended

17
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
5. References1. Miranda A et al. Impact of antiretroviral therapy on the incidence of tuberculosis: the Brazilian experience,
1995–2001. PLoSONE, 2007;2(9):e826.
2. Santoro-Lopes G et al. Reduced risk of tuberculosis among Brazilian patients with advanced human immunodeficiency virus infection treated with highly active antiretroviral therapy. ClinicalInfectiousDiseases, 2002 Feb 15;34(4):543-6.
3. Girardi E et al. Impact of combination antiretroviral therapy on the risk of tuberculosis among persons with HIV infection. AIDS, 2000, 14(13):1985–1991.
4. Lawn SD et al. Short-term and long-term risk of tuberculosis associated with CD4 cell recovery during antiretroviral therapy in South Africa. AIDS, 2009, 23(13):1717–1725.
5. Egger M, ed. Outcomes of ART in resource-limited and industrialized countries. 14thConferenceonretrovirusesandopportunisticinfections(CROI2007), Los Angeles, USA, CROI.
6. AntiretroviraltherapyforHIVinfectioninadultsandadolescents:recommendationsforapublichealthapproach, 2010 revision. Geneva, World Health Organization, 2010.
7. Badri M, Wilson D, Wood R. Effect of highly active antiretroviral therapy on incidence of tuberculosis in South Africa: a cohort study. Lancet, 2002, 359(9323):2059–2064.
8. Del Amo J, Hernan, M. (HIV-CASUAL). Combined antiretroviral therapy and the incidence of tuberculosisamongHIV-positiveindividualsinhigh-incomecountries [personal communication], 2011.
9. Severe P et al. Early versus standard antiretroviral therapy for HIV-infected adults in Haiti. NewEnglandJournalofMedicine, 2010, 363(3):257–265.
10. Cohen MS et al. Prevention of HIV-1 Infection with Early Antiretroviral Therapy. New England Journal ofMedicine, 2011, 365(6):493–505.
11. Golub JE et al. The impact of antiretroviral therapy and isoniazid preventive therapy on tuberculosis incidence in HIV-infected patients in Rio de Janeiro, Brazil. AIDS, 2007, 21(11):1441–1418.
12. Golub JE et al. Isoniazid preventive therapy, HAART and tuberculosis risk in HIV-infected adults in South Africa: a prospective cohort. AIDS, 2009, 23(5):631–636.
13. Girardi E et al. Incidence of Tuberculosis among HIV-infected patients receiving highly active antiretroviral therapy in Europe and North America. ClinicalInfectiousDiseases, 2005, 41(12):1772–1782.
14. Jones JL et al. HIV-associated tuberculosis in the era of highly active antiretroviral therapy. The Adult/Adolescent Spectrum of HIV Disease Group. InternationalJournalofTuberculosisandLungDisease, 2000, 4(11):1026–1031.
15. Lau B, Zhang, J. (NA-ACCORD). Incidence of Tuberculosis after HAART Initiation in HIV-infected persons [personal communication], 2011.
16. Ledergerber B et al. AIDS-related opportunistic illnesses occurring after initiation of potent antiretroviral therapy: the Swiss HIV Cohort Study. JAMA, 1999, 282(23):2220–2226.
17. Moreno S et al. Incidence and risk factors for tuberculosis in HIV-positive subjects by HAART status. InternationalJournalofTuberculosisandLungDisease, 2008, 12(12):1393–1400.

18
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
PICO question: What are the benefits of HIV testing and counselling in patients with presumptive and diagnosed tuberculosis and among the partners and family members of patients who are found to be HIV-positive?
Population: people with presumptive and diagnosed TB, and the partners and family members of patients who are found to be HIV positiveIntervention: HIV testing and counsellingComparison: no HIV testing and counsellingOutcomes: yield of positive HIV cases
1. Outcomes of interest
Outcomes Relative importance(rank 1 9 most critical) Comment
Among presumptive and confirmed TB patients
HIV cases (yield of positive HIV and TB cases by clinical settings and by epidemiological settings)
9 critical
Improved access to prevention, care and treatment
(reduced morbidity and mortality events due to TB and HIV diseases)
9 critical
Among partners and family members
HIV cases 9 critical
Improved access to prevention, care and treatment 8 critical
2. Literature search strategy and information retrievalStudies were identified using PubMed, EMBASE, Web of Science, Google Scholar and the Cochrane Library databases. Proceedings and abstracts from international conferences (CROI, IAS, ICAAC, World AIDS Conference) were searched.
Selection criteria
Studies were included if:
• randomizedandquasi-randomizedcontrolledtrials,includinghistoricallycontrolledtrialsorobservationalandcohort studies;
• participantsbeingpresumedorconfirmedTBcasesor/andpartnersandfamilymembersofthosewhoturntobe HIV positive;
• comparisonbeingaddressedwas:routineHIVtestingvs.noHIVtesting.
Annex 2Voluntary counselling and testing for HIV benefits patients with diagnosed and presumptive tuberculosis – summary of findings and evaluation of the quality of the evidence
19
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Most data that can be found on this topic is circumstantial evidence, most likely because it is deemed unethical to compare groups in which HIV testing is offered against one in which it is not. This would deprive people of the right to then make choices about treatment.
The only study which has a comparison group was carried out in Malawi and compared patients after the introduction of voluntary counselling and testing (VCT) and co-trimoxazole prophylaxis therapy (CPT) to patients before (1); unfortunately, there was no stratification and therefore it is not amenable to GRADE appraisal.
It is now clear that people with HIV-associated TB fare a lot worse than those with HIV or TB separately. Treatment for HIV is becoming increasingly available, and evidence shows that even just CPT is beneficial in decreasing morbidity and mortality. Knowledge of HIV status is also beneficial for sexual partners and unborn children. Thus it is hard to imagine the need for evidence to be collected to prove that testing patients with TB for HIV is beneficial.
A large number of studies show that testing for HIV in confirmed TB patients (mostly) and in presumptive TB patients and their contacts (occasionally) yields a high number of new diagnoses of HIV. The assumption is that this allows newly diagnosed HIV-positive people to receive CPT and ART, thus hypothetically decreasing their morbidity and mortality and preventing HIV transmission. These same descriptive studies also show that often after diagnosis, either the HIV treatment is not offered or available, or it is not taken up. According to the HIV/AIDS universal access report, only 17% of the estimated number of TB patients living with HIV were receiving ART, a figure considerably lower than the estimated coverage rate of antiretroviral therapy for all HIV patients in low- and middle-income countries (2).
Table 1 summarizes the 24 studies retrieved from the systematic literature search. It shows that in these studies HIV testing in TB patients can yield positive results anywhere between 6.3% and 77% depending on the epidemiologic setting. Although 6.3% appears low, consideration should be given to the fact that HIV is a transmissible, 100% fatal disease without available treatment and prevention measures. A few of the studies addressed the issue of contacts or cases with presumptive TB, although they yield very little data. In one study carried out in Kenya on presumptive TB patients, 61% diagnosed with TB were also HIV-positive, whereas 63% without TB were positive (3). Another study in Uganda (4) found that 39% patients diagnosed with TB were also HIV-positive, whereas 49% of those who had no active TB were HIV-positive. The yield of HIV-positive results among those with presumptive TB was 39% in Guinea-Bissau and 61% in Zimbabwe (5,6).
Only one study addressed the issue of testing close contacts of TB patients and on doing so found that 13.8% of contacts of TB patients living with HIV were HIV-infected, whereas 2.5% of contacts of HIV-negative TB patients were HIV-infected (7). One study attempted to quantify the benefit of testing by looking at relative risk of death of a cohort of patients in one programme before and after the introduction of VCT (1). It found the adjusted relative risk of death to be 0.81 (p<0.001).
By article: 24Appraisable by GRADE methodology 0
By title: 51
By abstract: 33
Pubmed Search (“Tuberculosis”[Mesh] AND “HIV Infections”[Mesh]) AND “Testing”[Mesh] 149

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n te
stin
g f
or
HIV
infe
ctio
n in
TB
pat
ient
s, p
eop
le w
ith s
usp
ecte
d T
B a
nd c
ont
acts
of
TB p
atie
nts
Aut
ho
r an
d y
ear
(ref
eren
ce)
Co
untr
yB
ackg
roun
d
HIV
pre
vale
nce
(14–
59ye
ars)
Typ
e o
f st
udy
Sam
ple
siz
eTe
stin
g s
ite
and
per
sonn
elH
IV t
estin
g
upta
ke%
tes
ted
HIV
-p
osi
tive
CP
T up
take
AR
T up
take
Aye
new
A, 2
010
(8)
Eth
iopi
a2%
Cas
e-co
ntro
l 28
2 TB
pat
ient
s–
70.6
%36
.2%
––
Njo
zing
NB
, 20
10 (9
)C
amer
oon
5.1%
Ret
rosp
ectiv
e co
hort
2270
TB
pat
ient
sC
ouns
ello
rs
with
in T
B u
nits
94.7
%68
.5%
47%
50.3
%
Vija
y S
, 200
9 (10)
Indi
a0.
3%P
rosp
ectiv
e co
hort
5299
TB
pat
ient
s (4
701
unkn
own
HIV
sta
tus)
Phy
sici
an re
ferr
al
to in
tegr
ated
co
unse
lling
and
te
stin
g ce
ntre
s
66%
6.4%
(of
prev
ious
ly
undi
agno
sed)
–37
%
Low
SY,
200
9 (11)
Sin
gapo
re0.
2%R
etro
spec
tive
493
TB p
atie
nts
–37
.3%
8.2%
––
Nat
eniy
om S
, 20
08 (12)
Thai
land
1.4%
Pro
spec
tive
coho
rt10
86 T
B p
atie
nts
(100
0 un
know
n H
IV s
tatu
s)
Trai
ned
nurs
es
and
soci
al
wor
kers
in T
B
clin
ics
93%
11%
36%
42%
Pope
DS
, 200
8 (13)
Sou
th A
frica
18.1
%C
lust
er-
rand
omiz
ed75
4 TB
pat
ient
sTB
nur
se in
TB
cl
inic
13.8
%36
–42%
19%
21%
Van
Rie
A, 2
008
(14)
Dem
ocra
tic
Rep
ublic
of t
he
Con
go
(opt
-in v
s op
t-ou
t)12
46 T
B p
atie
nts
VCT
clin
ic v
s pr
imar
y ca
re
cent
re v
s TB
nu
rse
95–9
8%18
.8%
89.8
%–
Cha
kaya
JM
, 20
08 (15)
Ken
ya7.
1-8.
3%R
etro
spec
tive
coho
rt46
428
TB
patie
nts
Hea
lth-c
are
wor
kers
in T
B
care
ser
vice
s
31.5
–59%
55%
85%
28%
Mor
bidi
ty a
nd
Mor
talit
y W
eekl
y R
epor
t, 20
08
(16)
Zam
bia
13.1
%D
escr
iptiv
e41
48 T
B p
atie
nts
VCT
offs
ite, V
CT
onsi
te, P
ITC
by
TB s
taff
50%
72%
––
20WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n te
stin
g f
or
HIV
infe
ctio
n in
TB
pat
ient
s, p
eop
le w
ith s
usp
ecte
d T
B a
nd c
ont
acts
of
TB p
atie
nts
Aut
ho
r an
d y
ear
(ref
eren
ce)
Co
untr
yB
ackg
roun
d
HIV
pre
vale
nce
(14–
59ye
ars)
Typ
e o
f st
udy
Sam
ple
siz
eTe
stin
g s
ite
and
per
sonn
elH
IV t
estin
g
upta
ke%
tes
ted
HIV
-p
osi
tive
CP
T up
take
AR
T up
take
Jere
ne D
, 20
07(17)
Eth
iopi
a2%
–19
0 TB
pat
ient
sTr
aine
d co
unse
llor a
t TB
cl
inic
in h
ospi
tal
58%
20.6
%–
–
Mor
bidi
ty a
nd
Mor
talit
y W
eekl
y R
epor
t, 20
06
(18)
Guy
ana
–D
escr
iptiv
e17
4 TB
pat
ient
s of
unk
now
n st
atus
–91
%10
%–
–
van
der W
erf M
J,
2005
(19)
Ukr
aine
–P
rosp
ectiv
e91
4 TB
pat
ient
sTB
phy
sici
ans
84%
6.3%
––
Chi
mzi
zi R
B,
2004
(20)
Mal
awi
12%
Eva
luat
ion
of
proj
ect
2397
TB
pat
ient
sC
ouns
ello
rs in
la
bora
tory
, war
d or
VC
T un
it
59%
68%
97%
–
Chi
mzi
zi R
B,
2004
(21)
Mal
awi
12%
Des
crip
tive
1103
TB
pat
ient
sC
ouns
ello
rs in
la
bora
tory
, war
d or
VC
T un
it
91%
77%
69%
Zach
aria
h R
, Jan
20
03 (22)
Mal
awi
12%
Coh
ort s
tudy
1049
TB
pat
ient
sH
ospi
tal H
IV
VCT
unit
91%
77%
94%
Zach
aria
h R
, M
ay 2
003
(1)
Mal
awi
12%
Coh
ort s
tudy
1986
TB
pat
ient
sH
ospi
tal H
IV
VCT
unit
91%
77%
93%
Abo
uya
L, 1
998
(23)
Côt
e d’
Ivoi
re–
Coh
ort s
tudy
w
ith h
isto
rical
co
ntro
ls
1959
4 TB
pa
tient
sP
hysi
cian
s,
nurs
es a
nd
soci
al w
orke
rs
91.8
%43
.2%
––
Ban
erje
e A
, 19
97 (24)
Mal
awi
12%
Ret
rosp
ectiv
e20
5 TB
pat
ient
s–
54%
66%
––
21
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n te
stin
g f
or
HIV
infe
ctio
n in
TB
pat
ient
s, p
eop
le w
ith s
usp
ecte
d T
B a
nd c
ont
acts
of
TB p
atie
nts
Aut
ho
r an
d y
ear
(ref
eren
ce)
Co
untr
yB
ackg
roun
d
HIV
pre
vale
nce
(14–
59ye
ars)
Typ
e o
f st
udy
Sam
ple
siz
eTe
stin
g s
ite
and
per
sonn
elH
IV t
estin
g
upta
ke%
tes
ted
HIV
-p
osi
tive
CP
T up
take
AR
T up
take
Stu
die
s in
clud
ing
pre
sum
ptiv
e TB
pat
ient
s
Pors
krog
A,
2011
(6)
Gui
nea-
Bis
sau
9%P
rosp
ectiv
e co
hort
86 w
ith
pres
umpt
ive
TBVC
T un
it51
%39
%–
–
Dim
airo
M, 2
010
(5)
Zim
babw
e–
Pro
spec
tive
coho
rt ne
sted
w
ithin
clu
ster
ra
ndom
ized
tria
l
1195
with
pr
esum
ptiv
e TB
VCT
unit
and
stud
y cl
inic
95%
61%
–15
%
Odh
iam
bo J
, 20
08 (3
)K
enya
7.1–
8.3%
Pilo
t stu
dy-
desc
riptiv
e54
57 w
ith
pres
umpt
ive
TB
Clin
ical
offi
cers
an
d TB
nur
ses
in
TB c
linic
s
89%
61–6
3%–
83%
Srik
antia
h P,
20
07 (4
)U
gand
a5.
4%P
rosp
ectiv
e co
hort
665
with
pr
esum
ptiv
e TB
Trai
ned
coun
sello
rs a
t TB
clin
ic
85%
42%
––
Mun
thal
i L, 2
006
(25)
Mal
awi
12%
Cro
ss-s
ectio
nal
surv
ey56
5 w
ith
pres
umpt
ive
TB–
95%
56%
––
Stu
die
s in
clud
ing
co
ntac
ts
Sug
gara
vets
iri P
, 20
03(7
)Th
aila
nd1.
4%D
escr
iptiv
e49
9 TB
pat
ient
s
1200
TB
co
ntac
ts
–74
.2%
39.5
%
13.8
% (i
f con
tact
ca
se H
IV-
posi
tive)
2.5%
(if c
ase
HIV
-neg
ativ
e)
––
Ran
ges
13.8
–98%
6.3–
77%
21–8
3%
ART,antiretroviraltherapy;CPT,co-trimoxazolepreventivetherapy;PICT,providerinitiatedcounsellingandtesting;VCT,voluntarycounsellingandtesting;%,percentage
22WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

23
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
In all studies, the prevalence of HIV was found to be higher in TB patients, those with presumptive TB and possibly even among TB contacts than the expected national adult HIV prevalence. One study highlighted higher rates of mortality among HIV-positive TB patients (29%) compared to those with TB only (8%) (24). Interestingly, 34% of those who refused testing died, but a possible bias is that anybody very unwell and suspicious of having HIV is possibly more likely not to test.
3. GRADE profileThe quality of evidence across a body of evidence was assessed using the GRADE approach but risk ratios could not be calculated as none of the studies available assessed the question of interest. GRADE profiles were therefore not produced.
4. Risk and benefits assessment
Recommendation: Routine HIV testing should be offered to all patients with presumptive and confirmed TB, their partners and family members
Population: TB patients, patients with presumptive TB, and their partners and family members
Intervention: Routine HIV testing
Factor Decision Explanation
Quality of evidence Low
There is a wealth of evidence documenting that TB and HIV coinfection has a worse outcome than TB alone. There is plenty of evidence that the population in question (patients with presumptive and confirmed TB) has a high prevalence of HIV and that those with HIV have high prevalence of TB. There is little evidence that contacts of HIV-positive TB patients have high prevalence of HIV.
Unfortunately, there are no randomized controlled trials or high-quality studies for GRADE appraisal.
Benefits
or desired effects Strong
Knowledge about status is a prerequisite for HIV prevention, treatment, care and support, including CPT and ART, which reduce morbidity and mortality. Even those who test negative have increased awareness, allowing them to avoid risk-taking behaviour, promote safer sexual behaviour and practices, and encourage their partners to do the same and/or be on ART and anti-TB treatment if indicated.
Risks or undesired effects
False-positive results; false negative results.
Stigma of HIV diagnosis once known.
Values and preferences Strong
Improved individual and family care
Better health for individual, partners, family and community
Prevent HIV transmission to loved ones
Stigma and problem of disclosure might lead to low uptake
Costs StrongTesting using rapid tests is inexpensive and incorporated in health package.
Savings by decreasing HIV and TB transmission and resulting morbidity and mortality.
Feasibility Strong
Structure for testing already in place and working.
Increased workload on health workers – actually less in the long term if fewer people have TB and HIV
Feasibility studies from India and Rwanda showed that it is feasible to routinely test TB patients for HIV (26,27)
Strength of recommendationStrong

24
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
5. References1. Zachariah R et al. Voluntary counselling, HIV testing and adjunctive cotrimoxazole reduces mortality in
tuberculosis patients in Thyolo, Malawi. AIDS, 2003, 17(7):1053–1061.
2. Towardsuniversalaccess:scalinguppriorityHIV/AIDSinterventionsinthehealthsector.Progressreport2010. Geneva, World Health Organization, 2010.
3. Odhiambo J et al. Provider-initiated HIV testing and counselling for TB patients and suspects in Nairobi, Kenya. InternationalJournalofTuberculosisandLungDisease, 12(3 Suppl 1):63–68.
4. Srikantiah P et al. Elevated HIV seroprevalence and risk behavior among Ugandan TB suspects: implications for HIV testing and prevention. InternationalJournalofTuberculosisandLungDisease, 2007, 11(2):168–174.
5. Dimairo M et al. The risk and timing of tuberculosis diagnosed in smear-negative TB suspects: a 12 month cohort study in Harare, Zimbabwe. PLoSONE, 2010, 5(7):e11849.
6. Porskrog A et al. Enhanced tuberculosis identification through 1-month follow-up of smear-negative tuberculosis suspects. InternationalJournalofTuberculosisandLungDisease, 2011, 15(4):459–464.
7. Suggaravetsiri P et al. Integrated counseling and screening for tuberculosis and HIV among household contacts of tuberculosis patients in an endemic area of HIV infection: Chiang Rai, Thailand. International JournalofTuberculosisandLungDisease, 2003, 7(12 Suppl 3):S424–431.
8. Ayenew A et al. Predictors of HIV testing among patients with tuberculosis in North West Ethiopia: a case-control study. PLoSONE, 2010, 5(3):e9702.
9. Njozing NB et al. Assessing the accessibility of HIV care packages among tuberculosis patients in the Northwest Region, Cameroon. BMCPublicHealth, 2010, 10:129.
10. Vijay S et al. Feasibility of provider-initiated HIV testing and counselling of tuberculosis patients under the TB control programme in two districts of South India. PLoSONE, 2009, 4(11):e7899.
11. Low SY, Eng P. Human immunodeficiency virus testing in patients with newly-diagnosed tuberculosis in Singapore. SingaporeMedicalJournal, 2009, 50(5):479–481.
12. Nateniyom S et al. Provider-initiated diagnostic HIV counselling and testing in tuberculosis clinics in Thailand. InternationalJournalofTuberculosisandLungDisease, 2008, 12(8):955–961.
13. Pope DS et al. A cluster-randomized trial of provider-initiated (opt-out) HIV counseling and testing of tuberculosis patients in South Africa. JAIDS, 2008, 48(2):190–195.
14. Van Rie A et al. Counseling and testing TB patients for HIV: evaluation of three implementation models in Kinshasa, Congo. InternationalJournalofTuberculosisandLungDisease, 2008, 12(3 Suppl 1):73–78.
15. Chakaya JM et al. National scale-up of HIV testing and provision of HIV care to tuberculosis patients in Kenya. InternationalJournalofTuberculosisandLungDisease, 2008, 12(4):424–429.
16. Provider-initiated HIV testing and counseling of TB patients—Livingstone District, Zambia, September 2004–December 2006. MMWR, 2008, 57(11):285–289.
17. Jerene D, Endale A, Lindtjorn B. Acceptability of HIV counselling and testing among tuberculosis patients in south Ethiopia. BMCInternationalHealthandHumanRights, 2007, 7:4.
18. HIV counseling, testing, and care of tuberculosis patients at chest clinics—Guyana, 2005–2006. MMWR, 2006, 55(31):849–851.
19. van der Werf MJ et al. HIV testing practices of TB patients after introduction of a new testing policy in Kiev City, Ukraine. InternationalJournalofTuberculosisandLungDisease, 2005, 9(7):733–739.
20. Chimzizi RB et al. Counselling, HIV testing and adjunctive cotrimoxazole for TB patients in Malawi: from research to routine implementation. InternationalJournalofTuberculosisandLungDisease, 2004, 8(8):938–944.

25
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
21. Chimzizi R et al. Voluntary counselling, HIV testing and adjunctive cotrimoxazole are associated with improved TB treatment outcomes under routine conditions in Thyolo District, Malawi. InternationalJournalofTuberculosisandLungDisease, 2004, 8(5):579–585.
22. Zachariah R et al. Voluntary counselling, HIV testing and sexual behaviour among patients with tuberculosis in a rural district of Malawi. InternationalJournalofTuberculosisandLungDisease, 2003, 7(1):65–71.
23. Abouya L et al. The Côte d’Ivoire national HIV counseling and testing program for tuberculosis patients: implementation and analysis of epidemiologic data. AIDS, 1998, 12(5):505–512.
24. Banerjee A et al. HIV testing and tuberculosis treatment outcome in a rural district in Malawi. Transactions of theRoyalSocietyofTropicalMedicineandHygiene, 1997, 91(6):707–708.
25. Munthali L et al. Using tuberculosis suspects to identify patients eligible for antiretroviral treatment. International JournalofTuberculosisandLungDisease, 2006, 10(2):199–202.
26. Thomas BE et al. Perceptions of tuberculosis patients on provider-initiated HIV testing and counseling—a study from south India. PLoSONE, 2009, 4(12):e8389.
27. Gasana M et al. Integrating tuberculosis and HIV care in rural Rwanda. InternationalJournalofTuberculosisandLungDisease, 2008, 12(3 Suppl 1):39–43.

26
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
PICO question: Does the administration of routine CPT compared with no CPT reduce the number of illness episodes and deaths in TB patients living with HIV?
Population: TB patients living with HIVIntervention: CPTComparison: no CPT or placeboOutcomes: mortality, morbidity/hospital admissions/adverse events
1. Outcomes of interest
Outcomes Relative importance(rank 1 9 most critical) Comment
Mortality (deaths occurring during the follow up period) 9 Critical
Morbidity/hospital admissions
(as defined by the trial researchers)
9 Critical
Adverse events (leading to hospitalization or treatment cessation)
9 Critical
2. Literature search strategy and information retrievalStudies were identified using PubMed, EMBASE, Web of Science, Google Scholar and the Cochrane Library databases. Proceedings and abstracts from international conferences (CROI, IAS, ICAAC, World AIDS Conference) were searched.
Annex 3Co-trimoxazole preventive therapy (CPT) reduces morbidity and mortality in tuberculosis patients living with HIV – summary of findings and evaluation of the quality of the evidence
Pubmed Search (“Tuberculosis”[Mesh] AND “HIV Infections”[Mesh]) AND “Cotrimoxazole”[Mesh] 55
By title: 35
By abstract: 8
By article: 7
27
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Selection criteria
Studies were selected if:
• randomizedandquasi-randomizedcontrolledtrials,includinghistoricallycontrolledtrialsorobservationalandcohort studies;
• participantsbeingpeoplelivingwithHIVwithactiveTB(studiesthatincludeparticipantsbothwithandwithoutactiveTBdiseasewereconsideredwherethedataforthosewithTBdiseasecouldbeextracted);
• comparisonbeingaddressedwas:routineCPTvs.placeboornoCPT.
Table 1 summarizes the findings from the two randomized controlled trials (RCTs) and the six observational studies, using historical controls or observational cohorts, identified by the systematic literature search. All studies were conducted in Africa.
Co-trimoxazole, a fixed-dose combination of sulfamethoxazole and trimethoprim, is a broad-spectrum antimicrobial agent that has been used since the mid-1980s to prevent Pneumocystisjirovecci pneumonia and toxoplasmosis in people living with HIV. It is also effective against other bacterial and parasitic diseases and it reduces the incidence of malaria in people living with HIV.
Data on CPT among TB patients living with HIV showed that survival of those receiving CPT is improved up to 18 months after diagnosis of TB disease in observational studies and up to 24 months of follow-up in one of the two RCTs (1). The number needed to treat to prevent one death during TB treatment was 24 in one observational study using historical controls conducted in South Africa (2) and 12.5 in another cohort study evaluating the benefit of a combination of HIV testing and provision of CPT in Malawi (3). All studies showed that adverse reactions, defined as those causing cessation of CPT or hospitalization, were infrequent with few patients having to definitely stop prophylaxis. Only one RCT studied the effect of CPT on morbidity through hospital admission for all diseases that could potentially have been prevented by CPT (septicaemia, enteritis, chest infection, urinary tract infection and toxoplasmosis) (4). The rate of admissions was significantly lower in the co-trimoxazole group (2.7/100 person-years) than in the placebo group (8.7/100 person-years; P=0.001). This trial also showed that the mortality rate was significantly lower in patients with CD4 counts ≤350 cells/mm3 receiving CPT than those receiving a placebo (hazard ratio: 0.44, 95% CI: 0.29–0.66). There is also a wealth of evidence on the benefits of CPT in reducing mortality and morbidity among people living with HIV without TB and their household members.

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Mw
aung
ulu
2004
(5)
(Mal
awi)
Nun
n 20
08 (
1)(Z
amb
ia)
Gri
mw
ade
2005
(2)
(So
uth
Afr
ica)
Kal
ou
2005
(6)
(Cô
te d
’Ivo
ire)
Met
ho
ds/
des
ign
A c
ohor
t stu
dy w
ith a
retro
spec
tive
cont
rol g
roup
.D
oubl
e-bl
ind
plac
ebo
cont
rolle
d ra
ndom
ized
clin
ical
tri
al.
Coh
ort s
tudy
usi
ng h
isto
rical
co
ntro
ls.
Con
trolle
d ra
ndom
ized
clin
ical
tria
l usi
ng
retro
spec
tive
data
from
a p
revi
ous
stud
y.
Po
pul
atio
nTB
pat
ient
s re
gist
ered
in 1
999
and
2000
in K
aron
ga D
istri
ct, M
alaw
i; 33
5 an
d 36
2 re
spec
tivel
y, o
f who
m
70%
wer
e H
IV-p
ositi
ve.
Two
grou
ps o
f HA
AR
T-na
ive
adul
ts w
ith H
IV in
fect
ion:
pa
tient
s ne
wly
dia
gnos
ed a
s ha
ving
TB
and
rece
ivin
g an
ti-TB
trea
tmen
t eith
er fo
r the
firs
t tim
e or
for
retre
atm
ent a
fter r
elap
se; p
revi
ousl
y tre
ated
pat
ient
s no
t rec
eivi
ng tr
eatm
ent.
Lusa
ka, Z
ambi
a, U
nive
rsity
Te
achi
ng H
ospi
tal (
UTH
) che
st c
linic
.
1003
pat
ient
s w
ere
rand
omiz
ed: 8
35 (4
16 C
PT,
419
pl
aceb
o) re
ceiv
ed a
nti-T
B tr
eatm
ent;
762
(376
CP
T,
386
plac
ebo)
wer
e ne
wly
dia
gnos
ed p
revi
ousl
y un
treat
ed p
atie
nts
and
73 (4
0 C
PT,
33
plac
ebo)
wer
e re
ceiv
ing
a re
treat
men
t reg
imen
; 168
(CP
T 84
pla
cebo
) w
ere
not o
n tre
atm
ent b
ut h
ad b
een
treat
ed in
the
past
.
Adu
lts tr
eate
d fo
r TB
bet
wee
n 19
98 a
nd 2
000
(con
trol g
roup
: 20
04)
All
adul
ts s
tarti
ng tr
eatm
ent f
or
TB b
etw
een
June
200
1 an
d Ju
ne
2002
irre
spec
tive
of
HIV
sta
tus
(inte
rven
tion
grou
p: 1
321)
.
HIV
-1-in
fect
ed p
atie
nts
with
new
ly d
iagn
osed
, sp
utum
-sm
ear p
ositi
ve fo
r Mycobacterium
tube
rcul
osis
pul
mon
ary
infe
ctio
n.
All
patie
nts
rece
ived
a s
tand
ard
TB re
gim
en
with
or w
ithou
t CP
T. P
atie
nts
in th
e C
PT
arm
w
ere
com
pare
d w
ith th
ose
in th
e pl
aceb
o ar
m
at th
e st
art o
f tre
atm
ent,
and
sim
ilarly
wer
e co
mpa
red
with
the
patie
nts
of b
oth
arm
s to
ea
ch o
ther
12
mon
ths
afte
r ini
tiatio
n of
the
treat
men
t.
Of t
he 4
4 pa
tient
s (2
3 m
ales
, 52%
) elig
ible
fo
r ana
lysi
s in
this
stu
dy, 2
5 (5
6.8%
) wer
e on
co
mbi
ned
treat
men
t of T
B (C
PT
grou
p) a
nd 1
9 (4
3.2%
) wer
e on
sta
ndar
d tre
atm
ent o
f TB
onl
y (p
lace
bo g
roup
); 3
2/44
(70%
) wer
e in
fect
ed
with
HIV
-1, a
nd 3
0% w
ere
dual
ly s
ero-
reac
tive
to H
IV-1
and
HIV
-2.
Inte
rven
tion
CP
T (9
60 m
g O
D) w
as g
iven
to
HIV
pat
ient
s en
rolle
d si
nce
Janu
ary
2000
.
Red
uced
dos
es w
ere
give
n to
ch
ildre
n.
Cas
e as
certa
inm
ent,
follo
w u
p an
d ca
re w
ere
iden
tical
in th
e 2
year
s ex
cept
that
in 2
000
CP
T w
as
adm
inis
tere
d to
HIV
pat
ient
s.
CP
T w
as g
iven
from
the
time
a pa
tient
was
iden
tified
as
HIV
-po
sitiv
e un
til 1
2 m
onth
s af
ter
regi
stra
tion.
Inte
ntio
n to
trea
t ana
lysi
s
Ran
dom
ized
par
ticip
ants
in a
1:1
ratio
to re
ceiv
e a
supp
ly o
f pre
-labe
lled
trial
med
icin
e (i)
CP
T or
(ii
) mat
chin
g pl
aceb
o; (2
tabl
ets
to b
e ta
ken
daily
). E
ach
CP
T (4
00 m
g su
lfam
etho
xazo
le a
nd 8
0 m
g tri
met
hopr
im).
All
adul
ts s
tarti
ng T
B tr
eatm
ent
betw
een
June
200
1 an
d Ju
ne 2
002
wer
e of
fere
d C
PT
prop
hyla
xis
(960
mg
OD
for 6
m
onth
s) d
urin
g TB
trea
tmen
t irr
espe
ctiv
e of
HIV
sta
tus.
960
mg
OD
of C
PT
or p
lace
bo s
tarti
ng 1
m
onth
into
sta
ndar
d tre
atm
ent o
f TB
.
Ana
lysi
sIn
tent
ion
to tr
eat a
naly
sis
Inte
ntio
n to
trea
t ana
lysi
sIn
tent
ion
to tr
eat a
naly
sis
Inte
ntio
n to
trea
t ana
lysi
s
28WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines
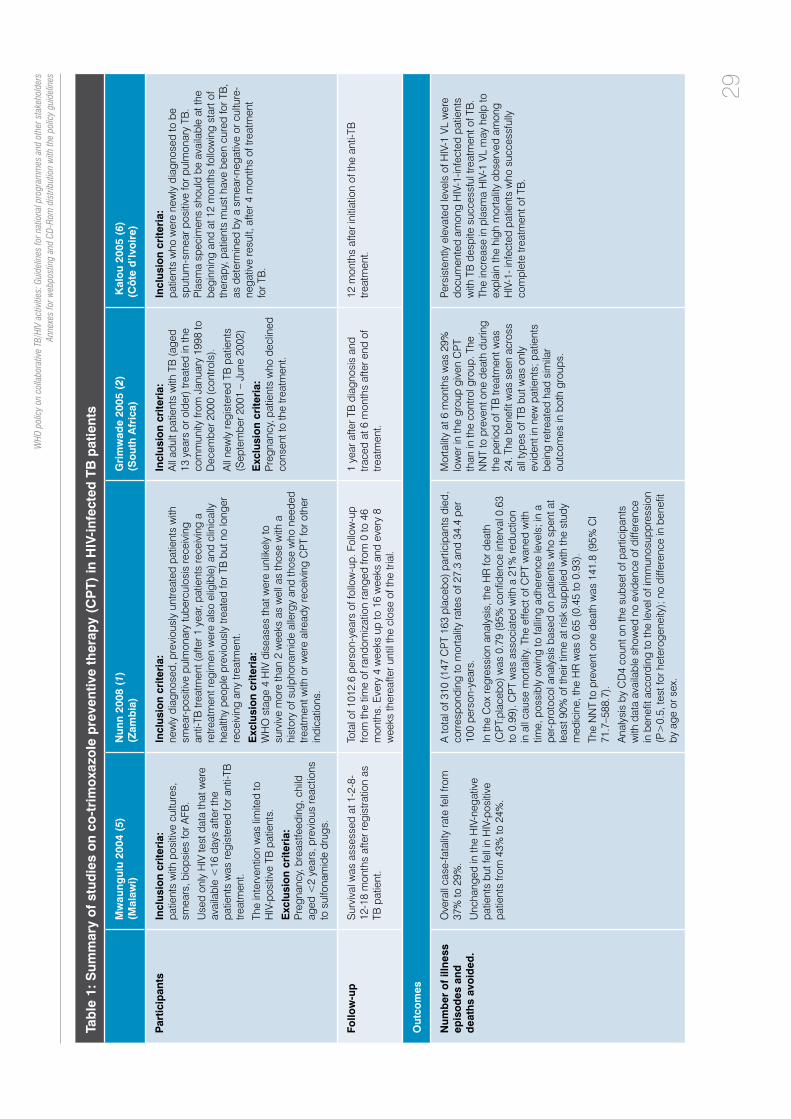
Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Mw
aung
ulu
2004
(5)
(Mal
awi)
Nun
n 20
08 (
1)(Z
amb
ia)
Gri
mw
ade
2005
(2)
(So
uth
Afr
ica)
Kal
ou
2005
(6)
(Cô
te d
’Ivo
ire)
Par
ticip
ants
In
clus
ion
crite
ria:
patie
nts
with
pos
itive
cul
ture
s,
smea
rs, b
iops
ies
for A
FB.
Use
d on
ly H
IV te
st d
ata
that
wer
e av
aila
ble
<16
day
s af
ter t
he
patie
nts
was
regi
ster
ed fo
r ant
i-TB
tre
atm
ent.
The
inte
rven
tion
was
lim
ited
to
HIV
-pos
itive
TB
pat
ient
s.
Exc
lusi
on
crite
ria:
P
regn
ancy
, bre
astfe
edin
g, c
hild
ag
ed <
2 ye
ars,
pre
viou
s re
actio
ns
to s
ulfo
nam
ide
drug
s.
Incl
usio
n cr
iteri
a:
new
ly d
iagn
osed
, pre
viou
sly
untre
ated
pat
ient
s w
ith
smea
r-pos
itive
pul
mon
ary
tube
rcul
osis
rece
ivin
g an
ti-TB
trea
tmen
t (af
ter 1
yea
r, pa
tient
s re
ceiv
ing
a re
treat
men
t reg
imen
wer
e al
so e
ligib
le) a
nd c
linic
ally
he
alth
y pe
ople
pre
viou
sly
treat
ed fo
r TB
but
no
long
er
rece
ivin
g an
y tre
atm
ent.
Exc
lusi
on
crite
ria:
W
HO
sta
ge 4
HIV
dis
ease
s th
at w
ere
unlik
ely
to
surv
ive
mor
e th
an 2
wee
ks a
s w
ell a
s th
ose
with
a
hist
ory
of s
ulph
onam
ide
alle
rgy
and
thos
e w
ho n
eede
d tre
atm
ent w
ith o
r wer
e al
read
y re
ceiv
ing
CP
T fo
r oth
er
indi
catio
ns.
Incl
usio
n cr
iteri
a:A
ll ad
ult p
atie
nts
with
TB
(age
d 13
yea
rs o
r old
er) t
reat
ed in
the
com
mun
ity fr
om J
anua
ry 1
998
to
Dec
embe
r 200
0 (c
ontro
ls).
All
new
ly re
gist
ered
TB
pat
ient
s (S
epte
mbe
r 200
1 –
June
200
2)
Exc
lusi
on
crite
ria:
P
regn
ancy
, pat
ient
s w
ho d
eclin
ed
cons
ent t
o th
e tre
atm
ent.
Incl
usio
n cr
iteri
a:
patie
nts
who
wer
e ne
wly
dia
gnos
ed to
be
sput
um-s
mea
r pos
itive
for p
ulm
onar
y TB
. P
lasm
a sp
ecim
ens
shou
ld b
e av
aila
ble
at th
e be
ginn
ing
and
at 1
2 m
onth
s fo
llow
ing
star
t of
ther
apy,
pat
ient
s m
ust h
ave
been
cur
ed fo
r TB
, as
det
erm
ined
by
a sm
ear-n
egat
ive
or c
ultu
re-
nega
tive
resu
lt, a
fter 4
mon
ths
of tr
eatm
ent
for T
B.
Follo
w-u
pS
urvi
val w
as a
sses
sed
at 1
-2-8
-12
-18
mon
ths
afte
r reg
istra
tion
as
TB p
atie
nt.
Tota
l of 1
012.
6 pe
rson
-yea
rs o
f fol
low
-up.
Fol
low
-up
from
the
time
of ra
ndom
izat
ion
rang
ed fr
om 0
to 4
6 m
onth
s. E
very
4 w
eeks
up
to 1
6 w
eeks
and
eve
ry 8
w
eeks
ther
eafte
r unt
il th
e cl
ose
of th
e tri
al.
1 ye
ar a
fter T
B d
iagn
osis
and
tra
ced
at 6
mon
ths
afte
r end
of
treat
men
t.
12 m
onth
s af
ter i
nitia
tion
of th
e an
ti-TB
tre
atm
ent.
Out
com
es
Num
ber
of
illne
ss
epis
od
es a
nd
dea
ths
avo
ided
.
Ove
rall
case
-fata
lity
rate
fell
from
37
% to
29%
.
Unc
hang
ed in
the
HIV
-neg
ativ
e pa
tient
s bu
t fel
l in
HIV
-pos
itive
pa
tient
s fro
m 4
3% to
24%
.
A to
tal o
f 310
(147
CP
T 16
3 pl
aceb
o) p
artic
ipan
ts d
ied,
co
rres
pond
ing
to m
orta
lity
rate
s of
27.
3 an
d 34
.4 p
er
100
pers
on-y
ears
.
In th
e C
ox re
gres
sion
ana
lysi
s, th
e H
R fo
r dea
th
(CP
T:pl
aceb
o) w
as 0
.79
(95%
con
fiden
ce in
terv
al 0
.63
to 0
.99)
. CP
T w
as a
ssoc
iate
d w
ith a
21%
redu
ctio
n in
all
caus
e m
orta
lity.
The
effe
ct o
f CP
T w
aned
with
tim
e, p
ossi
bly
owin
g to
falli
ng a
dher
ence
leve
ls; i
n a
per-p
roto
col a
naly
sis
base
d on
pat
ient
s w
ho s
pent
at
leas
t 90%
of t
heir
time
at ri
sk s
uppl
ied
with
the
stud
y m
edic
ine,
the
HR
was
0.6
5 (0
.45
to 0
.93)
.
The
NN
T to
pre
vent
one
dea
th w
as 1
41.8
(95%
CI
71.7
–588
.7).
Ana
lysi
s by
CD
4 co
unt o
n th
e su
bset
of p
artic
ipan
ts
with
dat
a av
aila
ble
show
ed n
o ev
iden
ce o
f diff
eren
ce
in b
enefi
t acc
ordi
ng to
the
leve
l of i
mm
unos
uppr
essi
on
(P>
0.5,
test
for h
eter
ogen
eity
); n
o di
ffere
nce
in b
enefi
t by
age
or s
ex.
Mor
talit
y at
6 m
onth
s w
as 2
9%
low
er in
the
grou
p gi
ven
CP
T th
an in
the
cont
rol g
roup
. The
N
NT
to p
reve
nt o
ne d
eath
dur
ing
the
perio
d of
TB
trea
tmen
t was
24
. The
ben
efit w
as s
een
acro
ss
all t
ypes
of T
B b
ut w
as o
nly
evid
ent i
n ne
w p
atie
nts;
pat
ient
s be
ing
retre
ated
had
sim
ilar
outc
omes
in b
oth
grou
ps.
Pers
iste
ntly
ele
vate
d le
vels
of H
IV-1
VL
wer
e do
cum
ente
d am
ong
HIV
-1-in
fect
ed p
atie
nts
with
TB
des
pite
suc
cess
ful t
reat
men
t of T
B.
The
incr
ease
in p
lasm
a H
IV-1
VL
may
hel
p to
ex
plai
n th
e hi
gh m
orta
lity
obse
rved
am
ong
HIV
-1- i
nfec
ted
patie
nts
who
suc
cess
fully
co
mpl
ete
treat
men
t of T
B.
29
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Mw
aung
ulu
2004
(5)
(Mal
awi)
Nun
n 20
08 (
1)(Z
amb
ia)
Gri
mw
ade
2005
(2)
(So
uth
Afr
ica)
Kal
ou
2005
(6)
(Cô
te d
’Ivo
ire)
Sec
ond
ary
out
com
es
Mo
rbid
ity/h
osp
ital
adm
issi
ons
N
AN
AN
AN
A
Ad
vers
e ev
ents
(d
efine
d a
s th
ose
ca
usin
g c
essa
tion
of
the
ther
apy
or
ho
spita
lizat
ion)
NA
Sus
pect
ed a
dver
se e
vent
s le
adin
g to
a p
lann
ed
inte
rrup
tion
of tr
ial m
edic
ine
occu
rred
in 1
8 pa
tient
s (1
2 C
PT,
6 p
lace
bo);
all
exce
pt 6
(all
CP
T) re
sum
ed
the
trial
med
icin
e. T
he re
actio
ns le
adin
g to
per
man
ent
disc
ontin
uatio
n w
ere
Ste
vens
–Joh
nson
syn
drom
e an
d an
aem
ia, i
tchy
rash
, sw
olle
n fa
ce a
nd li
ps, p
erip
hera
l ne
urop
athy
, and
ana
emia
(2 c
ases
).
Adv
erse
eve
nts
wer
e in
frequ
ent
and
min
or (o
nly
2 pa
rtici
pant
s st
oppe
d tre
atm
ent f
or th
is
reas
on).
Perc
eive
d ad
vers
e re
actio
ns
wer
e gi
ven
as th
e re
ason
for
stop
ping
pro
phyl
axis
by
23
patie
nts
but o
nly
2 si
gnifi
cant
ad
vers
e re
actio
ns w
ere
iden
tified
. O
ne p
atie
nt d
evel
oped
Ste
vens
–Jo
hnso
n sy
ndro
me
whi
le s
till
taki
ng a
nti-T
B tr
eatm
ent;
this
im
prov
ed o
n ce
ssat
ion
of
both
pro
phyl
axis
and
ant
i-TB
m
edic
atio
n. A
sec
ond
patie
nt
(kno
wn
to b
e H
IV-p
ositi
ve)
deve
lope
d ea
rly e
xfol
iativ
e de
rmat
itis
at 9
mon
ths
afte
r TB
di
agno
sis.
NA
Loss
to
fo
llow
up
NA
No
info
rmat
ion
on 7
8 (3
7 C
PT,
41
plac
ebo)
(9.3
%)
parti
cipa
nts
afte
r ran
dom
izat
ion.
429
parti
cipa
nts
No
loss
to fo
llow
up
Co
mm
ents
Ana
lyse
s in
clud
ing
all T
B p
atie
nts
wer
e al
so p
erfo
rmed
.Pa
tient
s pr
evio
usly
trea
ted
for T
B s
houl
d be
exc
lude
d.11
5 pa
tient
s re
sulte
d H
IV-p
ositi
ve
(8.8
%).
30WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Zach
aria
h 2
003
(Mal
awi)
(3)
Wik
tor
1999
(I
vory
Co
ast)
(4)
Ch
imzi
zi 2
004
(Mal
awi)
(7)
Met
ho
ds/
des
ign
Coh
ort s
tudy
usi
ng h
isto
rical
con
trols
Ran
dom
ized
dou
ble
blin
d ca
se-c
ontro
l C
ohor
t stu
dy u
sing
rout
inel
y co
llect
ed p
rogr
amm
e da
ta.
Po
pul
atio
nA
coh
ort o
f TB
pat
ient
s re
gist
ered
und
er ro
utin
e pr
ogra
mm
e co
nditi
ons
in a
rura
l dis
trict
of M
alaw
i.
A to
tal o
f 198
6 pa
tient
s w
ere
regi
ster
ed in
the
stud
y: 1
061
(inte
rven
tion)
and
925
(con
trol).
Bet
wee
n 1
July
199
9 an
d 30
Ju
ne 2
000
all T
B p
atie
nts
wer
e st
arte
d on
sta
ndar
dize
d an
ti-TB
tre
atm
ent,
and
offe
red
VCT.
Bet
wee
n O
ctob
er, 1
995,
and
Apr
il, 1
998,
wer
e en
rolle
d 77
1 H
IV-1
and
HIV
-1 &
HIV
-2 d
ually
ser
orea
ctiv
e pa
tient
s w
ho h
ad s
putu
m-s
mea
r-pos
itive
pul
mon
ary
TB (m
edia
n ag
e 32
yea
rs [r
ange
18–
64],
atte
ndin
g
Abi
djan
’s fo
ur la
rges
t out
patie
nt T
B tr
eatm
ent c
entre
s.
Two
rura
l dis
trict
s in
Mal
awi:
Thyo
lo (1
103
pts)
, w
here
VC
T is
offe
red
to a
ll TB
pat
ient
s an
d ad
junc
tive
CP
T to
HIV
-pos
itive
s, a
nd M
ulan
je
(123
9), w
here
no
such
inte
rven
tions
are
offe
red.
Inte
rven
tion
Patie
nts
foun
d to
be
HIV
-pos
itive
wer
e of
fere
d C
PT
(480
mg
BD
), pr
ovid
ed th
ere
wer
e no
con
train
dica
tions
.P
atie
nts
wer
e ra
ndo
mly
ass
igne
d o
ne d
aily
tab
let
of
CP
T (n
=38
6) o
r p
lace
bo
(n=
385)
1 m
ont
h a
fter
th
e st
art
of
a st
and
ard
6-m
ont
h T
B r
egim
en.
In T
hyol
o D
istri
ct, a
ll TB
pat
ient
s re
gist
ered
bet
wee
n Ju
ly 1
999
and
June
200
0 w
ere
offe
red
VCT,
and
th
ose
foun
d to
be
HIV
-pos
wer
e gi
ven
CP
T (4
80 m
g B
D),
prov
ided
ther
e w
ere
no c
ontra
indi
catio
ns.
Ana
lysi
sIn
tent
ion-
to-tr
eat
Inte
ntio
n-to
-trea
tIn
tent
ion-
to-tr
eat
Par
ticip
ants
In
clus
ion
crite
ria:
B
etw
een
1 Ju
ly 1
999
and
30 J
une
2000
, all
TB p
atie
nts
who
wer
e re
gist
ered
in T
hyol
o di
stric
t, at
eith
er th
e go
vern
men
t hos
pita
l or
the
mis
sion
hos
pita
l, w
ere
enro
lled
into
the
VCT
and
adju
nctiv
e C
PT
treat
men
t stu
dy (i
nter
vent
ion
grou
p).
Bet
wee
n 1
July
199
8 an
d 30
Jun
e 19
99, a
ll TB
pat
ient
s w
ho w
ere
regi
ster
ed in
the
sam
e tw
o ho
spita
ls in
the
dist
rict w
ere
star
ted
on th
e sa
me
stan
dard
ized
ant
i-TB
trea
tmen
t (co
ntro
l gro
up).
Exc
lusi
on
crite
ria:
K
now
n al
lerg
ies
to s
ulfo
nam
ide
drug
s, p
regn
ancy
, bre
ast-
feed
ing
until
2 m
onth
s an
d ch
ildre
n ag
ed le
ss th
an 2
yea
rs
(bec
ause
of u
ncer
tain
ty a
bout
HIV
-ser
osta
tus)
.
Incl
usio
n cr
iteri
a:
All
thos
e ag
ed 1
8 ye
ars
or o
lder
who
live
d in
Abi
djan
, w
ho h
ad s
putu
m-s
mea
r-pos
itive
TB
, and
who
wer
e H
IV-1
se
ropo
sitiv
e or
HIV
-1 a
nd H
IV-2
dua
lly s
eror
eact
ive.
Exc
lusi
on
crite
ria:
H
IV-2
-ser
opos
itive
pat
ient
s be
caus
e of
low
mor
talit
y ris
k,
preg
nant
wom
en,
patie
nts
with
pre
viou
sly
treat
ed tu
berc
ulos
is, t
hose
al
lerg
ic to
CP
T,
and
thos
e re
ceiv
ing
CP
T pr
ophy
laxi
s fo
r pre
vent
ion
of a
re
curr
ence
of t
oxop
lasm
osis
.
Incl
usio
n cr
iteri
a:
Sm
ear p
ositi
ve P
TB a
nd E
PTB
, sm
ear n
egat
ive
PTB
an
d E
PTB
. Ret
reat
men
t pat
ient
s (B
oth
arm
s), H
IV
posi
tive
test
(int
erve
ntio
n ar
m).
Exc
lusi
on
crite
ria:
Pa
tient
s w
ere
not g
iven
CP
T if
preg
nant
or a
llerg
ic
to C
PT.
Follo
w-u
pU
ntil
end
of T
B tr
eatm
ent
24 m
onth
sN
A
31
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Zach
aria
h 2
003
(Mal
awi)
(3)
Wik
tor
1999
(I
vory
Co
ast)
(4)
Ch
imzi
zi 2
004
(Mal
awi)
(7)
Num
ber
of
illne
ss
epis
od
es a
nd
dea
ths
avo
ided
.
Dea
th w
as d
efine
d as
a d
eath
at a
ny ti
me
durin
g th
e 8–
12
mon
ths
of tr
eatm
ent f
rom
wha
teve
r cau
se.
The
crud
e re
lativ
e ris
k (R
R) o
f dea
th b
y th
e en
d of
trea
tmen
t in
the
inte
rven
tion
com
pare
d gr
oup
with
the
cont
rol g
roup
was
0.7
8 (9
5% C
I, 0.
69–0
.89;
p=
0.00
1). A
djus
ted
for t
ype
and
cate
gory
of
TB
as
wel
l as
anti-
TB tr
eatm
ent,
the
RR
was
0.8
1 (9
5% C
I, 0.
75–0
.87;
p=
0.0
01).
The
deat
h ra
te fo
r all
regi
ster
ed T
B p
atie
nts
was
4.0
per
100
pe
rson
-mon
ths
of fo
llow
-up
in th
e in
terv
entio
n gr
oup
and
5.3
in th
e co
ntro
l gro
up, c
orre
spon
ding
to a
25%
redu
ctio
n in
risk
of
dea
th (9
5% C
I, 12
.3–3
5.8)
. Adj
uste
d fo
r typ
e an
d ca
tego
ry
of T
B a
s w
ell a
s an
ti-TB
trea
tmen
t, th
e H
R w
as 0
.76
(95%
CI,
0.69
–0.8
3).
The
NN
T to
pre
vent
one
dea
th (b
y pr
ovid
ing
VCT
plus
CP
T)
durin
g th
e co
urse
of a
nti-T
B tr
eatm
ent w
as 1
2.5.
51 p
atie
nts
in th
e C
PT
grou
p (1
3.8/
100
pers
on-y
ears
) and
86
in th
e pl
aceb
o gr
oup
(25.
4/10
0 pe
rson
-yea
rs) d
ied
(dec
reas
e In
risk
46%
[95%
CI 2
3–62
], p<
0·00
1).
Adj
uste
d fo
r typ
e an
d ca
tego
ry o
f TB
, TB
trea
tmen
t re
gim
en a
nd s
ite o
f reg
istra
tion,
the
rela
tive
risks
fo
r all
TB p
atie
nts
in T
hyol
o co
mpa
red
with
thos
e in
M
ulan
je w
ere:
- Tre
atm
ent s
ucce
ss R
R 1
.23
(95%
CI 1
.19–
1.26
, p=
0.
001)
;
- Dea
th R
R 0
.84
(95%
CI 0
.78–
0.91
, p=
0.00
1);
- “O
ther
out
com
es”
(def
ault,
tran
sfer
out
, unk
now
n an
d, fo
r sm
ear-p
ositi
ve p
atie
nts,
failu
re) R
R 0
.27
(95%
CI 0
.23–
0.32
, p=
0.0
01).
Sec
ond
ary
out
com
es
Mo
rbid
ity/h
osp
ital
adm
issi
ons
NA
29 p
atie
nts
on C
PT
(8.2
/100
per
son-
year
s) a
nd 4
7 on
pl
aceb
o (1
5.0/
100
pers
on-y
ears
) wer
e ad
mitt
ed to
ho
spita
l at l
east
onc
e af
ter r
ando
miz
atio
n (d
ecre
ase
43%
[10–
64])
, p=
0.02
). Th
e ra
te o
f adm
issi
ons
for a
ll di
seas
es th
at c
ould
pot
entia
lly h
ave
been
pre
vent
ed b
y C
PT
(sep
ticae
mia
, ent
eriti
s, c
hest
infe
ctio
n, u
rinar
y-tra
ct
infe
ctio
n, a
nd to
xopl
asm
osis
) was
sig
nific
antly
low
er fo
r pa
tient
s in
the
CP
T gr
oup
(2.7
/100
per
son-
year
s) th
an
in th
e pl
aceb
o gr
oup
(8.7
/100
per
son-
year
s; H
R 0
.3
[0.2
–0.7
], p=
0.00
1).
Ther
e w
ere
sign
ifica
ntly
few
er a
dmis
sion
s fo
r sep
ticae
mia
an
d en
terit
is in
the
CP
T gr
oup
than
in th
e pl
aceb
o gr
oup.
NA
Ad
vers
e ev
ents
, d
efine
d a
s th
ose
ca
usin
g c
essa
tion
of
the
ther
apy
or
ho
spita
lizat
ion
Of 6
93 p
atie
nts
on C
PT,
14
(2%
) had
a d
erm
atol
ogic
al re
actio
n.
No
reac
tions
wer
e se
rious
or i
nvol
ved
muc
osal
mem
bran
es, a
nd
all w
ere
reve
rsib
le o
n di
scon
tinui
ng tr
eatm
ent.
All
derm
atol
ogic
al
reac
tions
occ
urre
d in
the
first
2 m
onth
s of
trea
tmen
t, w
ith 9
(6
4%) o
ccur
ring
durin
g th
e fir
st m
onth
. In
13 p
atie
nts,
CP
T w
as
disc
ontin
ued
inde
finite
ly, a
nd in
one
pat
ient
it w
as re
-sta
rted
(by
mis
take
) with
out p
robl
ems.
Abo
ut 1
6 %
of p
atie
nts
in th
e pl
aceb
o gr
oup
and
12%
in
the
CP
T gr
oup
had
at le
ast o
ne s
ever
e cl
inic
al a
dver
se
even
t.
Abo
ut 8
% o
f the
pat
ient
s in
eac
h gr
oup
had
a se
vere
to
xic
effe
ct b
ased
on
labo
rato
ry m
easu
rem
ents
.
Rat
es o
f lab
orat
ory
and
clin
ical
adv
erse
eve
nts
wer
e si
mila
r in
the
two
grou
ps.
NA
32WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines
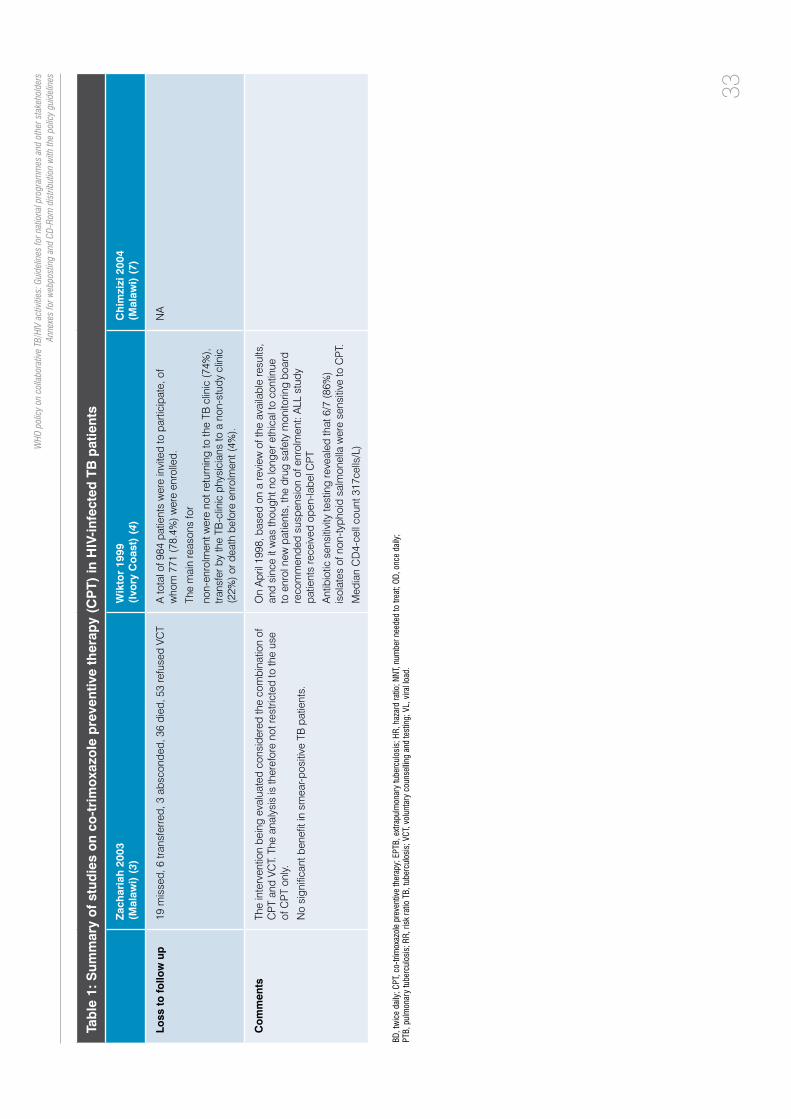
Tab
le 1
: Sum
mar
y o
f st
udie
s o
n co
-tri
mo
xazo
le p
reve
ntiv
e th
erap
y (C
PT)
in H
IV-i
nfec
ted
TB
pat
ient
s
Zach
aria
h 2
003
(Mal
awi)
(3)
Wik
tor
1999
(I
vory
Co
ast)
(4)
Ch
imzi
zi 2
004
(Mal
awi)
(7)
Loss
to
fo
llow
up
19 m
isse
d, 6
tran
sfer
red,
3 a
bsco
nded
, 36
died
, 53
refu
sed
VCT
A to
tal o
f 984
pat
ient
s w
ere
invi
ted
to p
artic
ipat
e, o
f w
hom
771
(78.
4%) w
ere
enro
lled.
The
mai
n re
ason
s fo
r
non-
enro
lmen
t wer
e no
t ret
urni
ng to
the
TB c
linic
(74%
), tra
nsfe
r by
the
TB-c
linic
phy
sici
ans
to a
non
-stu
dy c
linic
(2
2%) o
r dea
th b
efor
e en
rolm
ent (
4%).
NA
Co
mm
ents
The
inte
rven
tion
bein
g ev
alua
ted
cons
ider
ed th
e co
mbi
natio
n of
C
PT
and
VCT.
The
ana
lysi
s is
ther
efor
e no
t res
trict
ed to
the
use
of C
PT
only.
No
sign
ifica
nt b
enefi
t in
smea
r-pos
itive
TB
pat
ient
s.
On
Apr
il 19
98, b
ased
on
a re
view
of t
he a
vaila
ble
resu
lts,
and
sinc
e it
was
thou
ght n
o lo
nger
eth
ical
to c
ontin
ue
to e
nrol
new
pat
ient
s, th
e dr
ug s
afet
y m
onito
ring
boar
d re
com
men
ded
susp
ensi
on o
f enr
olm
ent:
ALL
stu
dy
patie
nts
rece
ived
ope
n-la
bel C
PT
Ant
ibio
tic s
ensi
tivity
test
ing
reve
aled
that
6/7
(86%
) is
olat
es o
f non
-typh
oid
salm
onel
la w
ere
sens
itive
to C
PT.
Med
ian
CD
4-ce
ll co
unt 3
17ce
lls/L
)
BD,twicedaily;CPT,co-trimoxazolepreventivetherapy;EPTB,extrapulmonarytuberculosis;HR,hazardratio;NNT,numberneededtotreat;OD,oncedaily;
PTB,pulmonarytuberculosis;RR,riskratioTB,tuberculosis;VCT,voluntarycounsellingandtesting;VL,viralload.
33
WHO
pol
icy
on c
olla
bora
tive
TB/H
IV a
ctiv
ities
: Gui
delin
es fo
r nat
iona
l pro
gram
mes
and
oth
er s
take
hold
ers
Anne
xes
for w
ebpo
stin
g an
d CD
-Rom
dis
tribu
tion
with
the
polic
y gu
idel
ines

34
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
3. GRADE profileThe quality of evidence across a body of evidence was assessed using the GRADE approach. For purposes of systematic reviews, the GRADE approach defines the quality of a body of evidence as the extent to which one can be confident that an estimate of effect or association is close to the quantity of specific interest (8). The quality of a body of evidence involves consideration of within-study risk of bias (methodological quality), directness of evidence, heterogeneity, precision of effect estimates and risk of publication bias. The GRADE system entails an assessment of the quality of a body of evidence for each individual outcome.
The quality rating across studies has four levels: high, moderate, low or very low. Randomized trials are categorized as high-quality but can be downgraded; similarly, observational studies can be upgraded. Factors that decrease the quality of evidence include limitations in design, indirectness of evidence, unexplained heterogeneity or inconsistency of results, imprecision of results, or high probability of publication bias. Factors that can increase the quality level of a body of evidence include a large magnitude of effect, if all plausible confounding would reduce a demonstrated effect and if there is a dose-response gradient. The GRADE Profiler software was used to perform the GRADE analyses (GRADE pro 2008).
Given the availability of two randomized controlled trials and the unlikelihood of achieving a better quality of evidence by including the observational studies, the GRADE analyses were restricted to the two randomized controlled trials available as follows.

35
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Table 2Question: Should routine co-trimoxazole preventive therapy (CPT) be used in HIV-infected individuals with active TB?Settings: High TB/HIV prevalence settingsBibliography: Nunn A, 2008 (1) Wiktor SZ, 1999 (4)
Routine CPT prophylaxis for HIV-infected individuals with active TB
Patient or population: HIV-infected individuals with active TB
Settings: High TB/HIV prevalence settings
Intervention: Routine CPT prophylaxis
Outcomes Illustrative comparative risks* (95% CI)
Relative effect(95% CI)
No of participants(studies)
Quality of the evidence(GRADE)
Comments
Assumed risk Corresponding risk
Control Routine CPT prophylaxis
Mortality
Medical record
Follow-up: 332–538 patient-years
Study population RR 0.70 (0.6 to 0.83)
1711(2 studies)
++++high1
309 per 1000 216 per 1000(185 to 256)
Medium risk population
300 per 1000 210 per 1000(180 to 249)
Morbidity/hospital admission
Medical and hospital record
Follow-up: 332–366 patient-years
Study population HR 0.54 (0.39 to 0.74)
698(1 study)
+++-moderate2
259 per 1000 140 per 1000(101 to 192)
Adverse events
Medical record
Follow-up: 332–538 patient-years
58 per 1000 46 per 1000(31 to 67)
RR 0.79 (0.54 to 1.15)
1599(2 studies)
+++-moderate3
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI, confidence interval; RR, risk ratio; HR, hazard ratio
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 PatientswerenotonHAARTandthiscouldbeconsideredasasignificantdifferencebetweenthetrialsubjectsandthepatientsforwhomtherecommendationisintended;however,thisislikely to be a minor issue therefore the studies were not downgraded.
2 Onlyonestudyavailable.
3 WideCI.
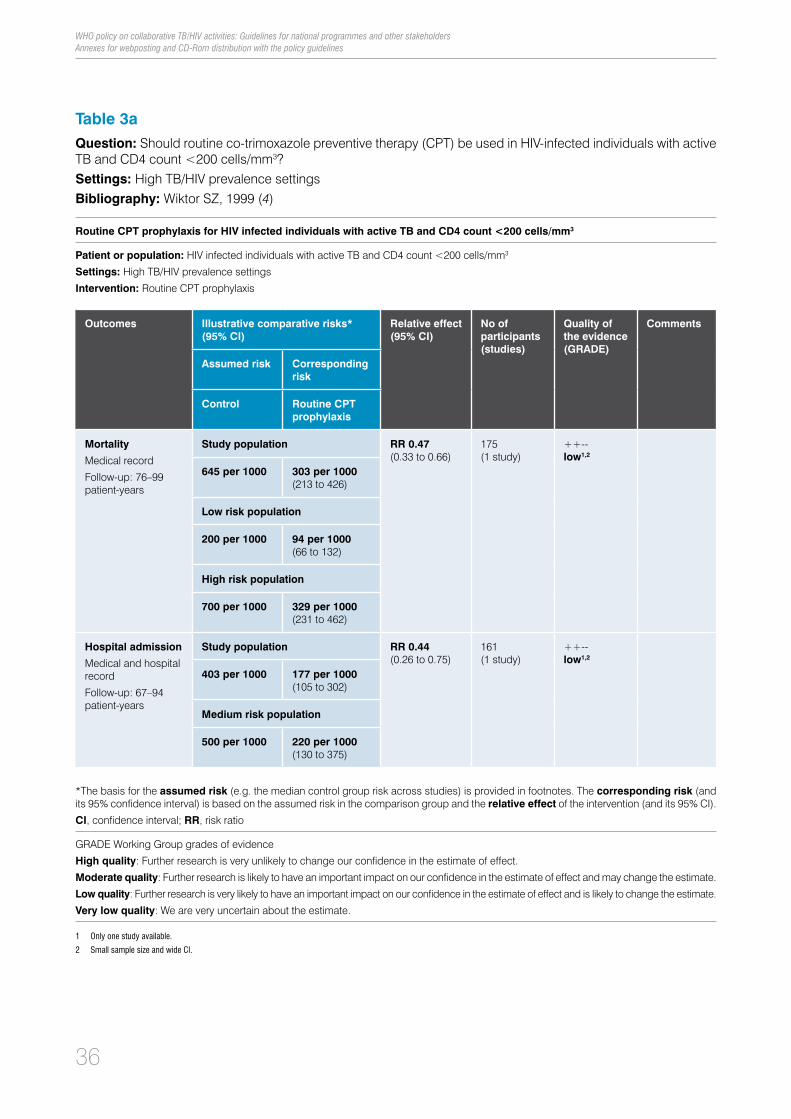
36
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Table 3aQuestion: Should routine co-trimoxazole preventive therapy (CPT) be used in HIV-infected individuals with active TB and CD4 count <200 cells/mm3?Settings: High TB/HIV prevalence settingsBibliography: Wiktor SZ, 1999 (4)
Routine CPT prophylaxis for HIV infected individuals with active TB and CD4 count <200 cells/mm3
Patient or population: HIV infected individuals with active TB and CD4 count <200 cells/mm3
Settings: High TB/HIV prevalence settings
Intervention: Routine CPT prophylaxis
Outcomes Illustrative comparative risks* (95% CI)
Relative effect(95% CI)
No of participants(studies)
Quality of the evidence(GRADE)
Comments
Assumed risk Corresponding risk
Control Routine CPT prophylaxis
Mortality
Medical record
Follow-up: 76–99 patient-years
Study population RR 0.47 (0.33 to 0.66)
175(1 study)
++--low1,2
645 per 1000 303 per 1000(213 to 426)
Low risk population
200 per 1000 94 per 1000(66 to 132)
High risk population
700 per 1000 329 per 1000(231 to 462)
Hospital admission
Medical and hospital record
Follow-up: 67–94 patient-years
Study population RR 0.44 (0.26 to 0.75)
161(1 study)
++--low1,2
403 per 1000 177 per 1000(105 to 302)
Medium risk population
500 per 1000 220 per 1000(130 to 375)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI, confidence interval; RR, risk ratio
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Onlyonestudyavailable.
2 SmallsamplesizeandwideCI.

37
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
Table 3bQuestion: Should routine co-trimoxazole preventive therapy (CPT) be used in HIV-infected individuals with active TB and CD4 count >200 cells/mm3?Settings: High TB/HIV prevalence settingsBibliography: Wiktor SZ, 1999 (4)
Routine CPT prophylaxis for HIV-infected individuals with active TB and CD4 count >200 cells/mm3
Patient or population: HIV-infected individuals with active TB and CD4 count >200 cells/mm3
Settings: High TB/HIV prevalence settings
Intervention: Routine CPT prophylaxis
Outcomes Illustrative comparative risks* (95% CI)
Relative effect(95% CI)
No of participants(studies)
Quality of the evidence(GRADE)
Comments
Assumed risk Corresponding risk
Control Routine CPT prophylaxis
Mortality
Medical record
Follow-up: 251 patient-years
Study population RR 0.48 (0.26 to 0.89)
502(1 study)
++--low1,2
116 per 1000 56 per 1000(30 to 103)
Low risk population
100 per 1000 48 per 1000(26 to 89)
High risk population
400 per 1000 192 per 1000(104 to 356)
Hospital admission
Medical and hospital record
Follow-up: 241–244 patient-years
Study population RR 0.60 (0.27 to 1.35)
485(1 study)
++--low1,2
62 per 1000 37 per 1000(17 to 84)
Medium risk population
200 per 1000 120 per 1000(54 to 270)
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI, confidence interval; RR, risk ratio
GRADE Working Group grades of evidence
High quality: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: We are very uncertain about the estimate.
1 Onlyonestudyavailable.
2 SmallsamplesizeandwideCI.
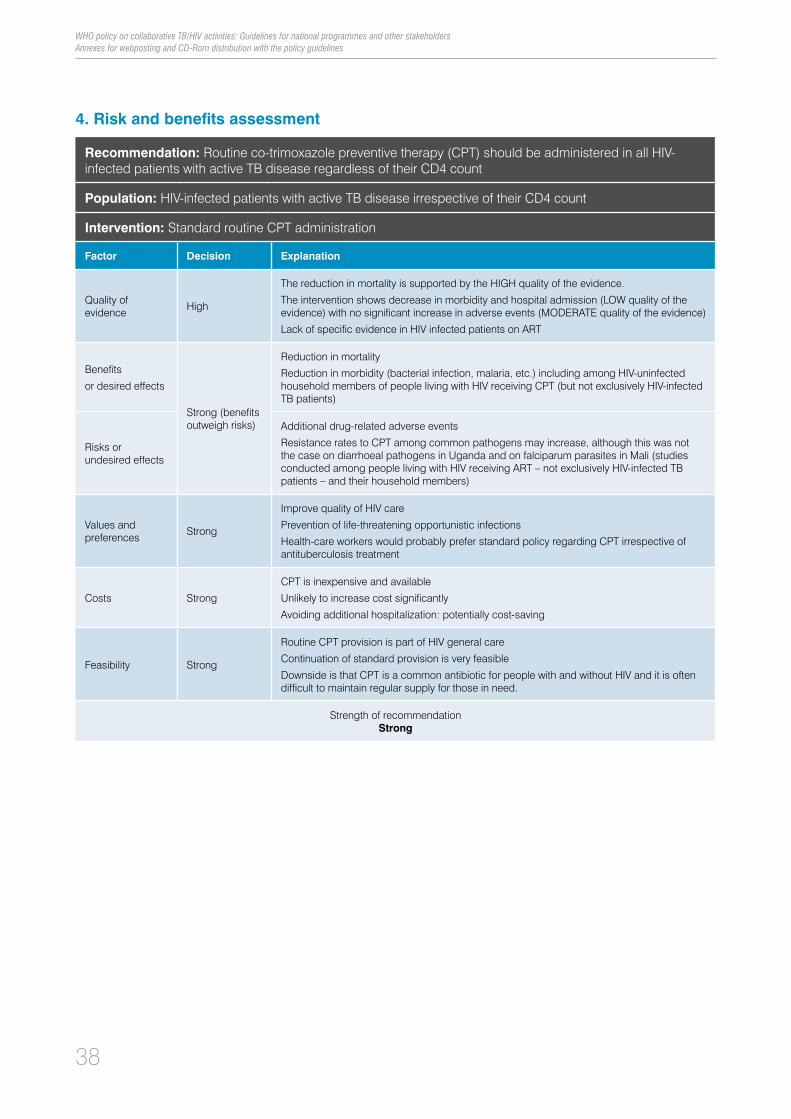
38
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
4. Risk and benefits assessment
Recommendation: Routine co-trimoxazole preventive therapy (CPT) should be administered in all HIV-infected patients with active TB disease regardless of their CD4 count
Population: HIV-infected patients with active TB disease irrespective of their CD4 count
Intervention: Standard routine CPT administration
Factor Decision Explanation
Quality of evidence High
The reduction in mortality is supported by the HIGH quality of the evidence.
The intervention shows decrease in morbidity and hospital admission (LOW quality of the evidence) with no significant increase in adverse events (MODERATE quality of the evidence)
Lack of specific evidence in HIV infected patients on ART
Benefits
or desired effects
Strong (benefits outweigh risks)
Reduction in mortality
Reduction in morbidity (bacterial infection, malaria, etc.) including among HIV-uninfected household members of people living with HIV receiving CPT (but not exclusively HIV-infected TB patients)
Risks or undesired effects
Additional drug-related adverse events
Resistance rates to CPT among common pathogens may increase, although this was not the case on diarrhoeal pathogens in Uganda and on falciparum parasites in Mali (studies conducted among people living with HIV receiving ART – not exclusively HIV-infected TB patients – and their household members)
Values and preferences Strong
Improve quality of HIV care
Prevention of life-threatening opportunistic infections
Health-care workers would probably prefer standard policy regarding CPT irrespective of antituberculosis treatment
Costs Strong
CPT is inexpensive and available
Unlikely to increase cost significantly
Avoiding additional hospitalization: potentially cost-saving
Feasibility Strong
Routine CPT provision is part of HIV general care
Continuation of standard provision is very feasible
Downside is that CPT is a common antibiotic for people with and without HIV and it is often difficult to maintain regular supply for those in need.
Strength of recommendationStrong

39
WHO policy on collaborative TB/HIV activities: Guidelines for national programmes and other stakeholders Annexes for webposting and CD-Rom distribution with the policy guidelines
5. References1. Nunn AJ et al. Role of co-trimoxazole prophylaxis in reducing mortality in HIV infected adults being treated for
tuberculosis: randomised clinical trial. BMJ, 2008, 337:a257.
2. Grimwade K et al. Effectiveness of cotrimoxazole prophylaxis on mortality in adults with tuberculosis in rural South Africa. AIDS, 2005, 19(2):163–168.
3. Zachariah R et al. Voluntary counselling, HIV testing and adjunctive cotrimoxazole reduces mortality in tuberculosis patients in Thyolo, Malawi. AIDS, 2003, 17(7):1053–1061.
4. Wiktor SZ et al. Efficacy of trimethoprim-sulphamethoxazole prophylaxis to decrease morbidity and mortality in HIV-1-infected patients with tuberculosis in Abidjan, Côte d’Ivoire: a randomised controlled trial. Lancet, 1999, 353(9163):1469–1475.
5. Mwaungulu FB et al. Cotrimoxazole prophylaxis reduces mortality in human immunodeficiency virus-positive tuberculosis patients in Karonga District, Malawi. BulletinoftheWorldHealthOrganization, 2004, 82(5):354–363.
6. Kalou M et al. Changes in HIV RNA viral load, CD4+ T-cell counts, and levels of immune activation markers associated with anti-tuberculosis therapy and cotrimoxazole prophylaxis among HIV-infected tuberculosis patients in Abidjan, Côte d’Ivoire. JournalofMedicalVirology, 2005, 75(2):202–208.
7. Chimzizi R et al. Voluntary counselling, HIV testing and adjunctive cotrimoxazole are associated with improved TB treatment outcomes under routine conditions in Thyolo District, Malawi. InternationalJournalofTuberculosisandLungDisease, 2004, 8(5):579–585.
8. Atkins D et al. Grading quality of evidence and strength of recommendations. BMJ, 2004, 328(7454):1490.

9789241503006
For further information contact:
World Health Organization20, Avenue Appia CH-1211 Geneva 27 SwitzerlandStop TB DepartmentE-mail: [email protected] site: www.who.int/tb
Department of HIV/AIDSEmail: [email protected] site: www.who.int/hiv