whitney pope, md, phd director of neuro core, medqia director of brain tumor imaging, assistant...
TRANSCRIPT

Whitney Pope, MD, PhD
Director of Neuro Core, MedQIADirector of Brain Tumor Imaging,
Assistant Professor of Neuroradiology,University of California, Los Angeles
XL184-205 Investigator MeetingJune 3rd, 2010
Scientific Aspect ofGB Imaging
XL184-205 Investigator Meeting - Confidential 2
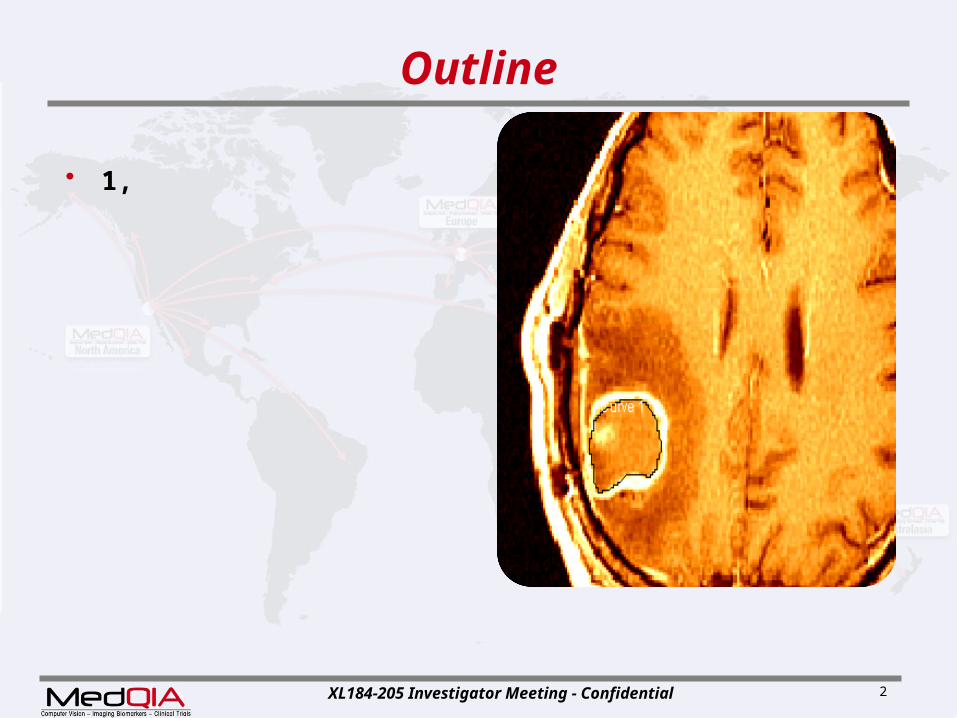
Outline
• 1,
XL184-205 Investigator Meeting - Confidential 3
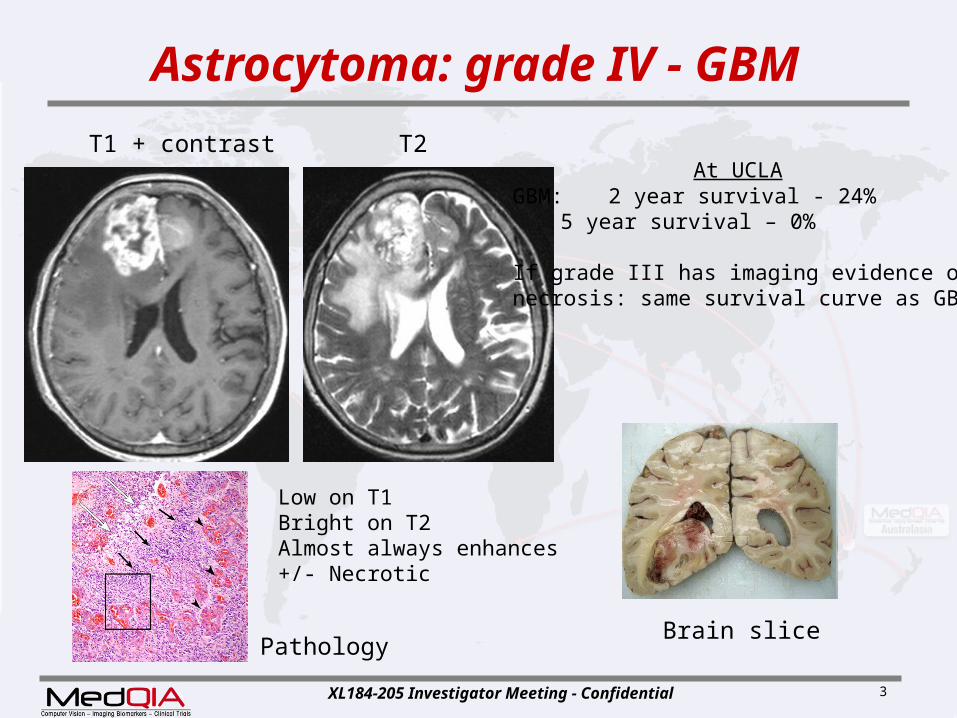
Astrocytoma: grade IV - GBM
GBM: 2 year survival - 24%5 year survival – 0%
If grade III has imaging evidence of necrosis: same survival curve as GBM
At UCLA
Low on T1Bright on T2Almost always enhances+/- Necrotic
Brain slicePathology
T1 + contrast T2
XL184-205 Investigator Meeting - Confidential 4
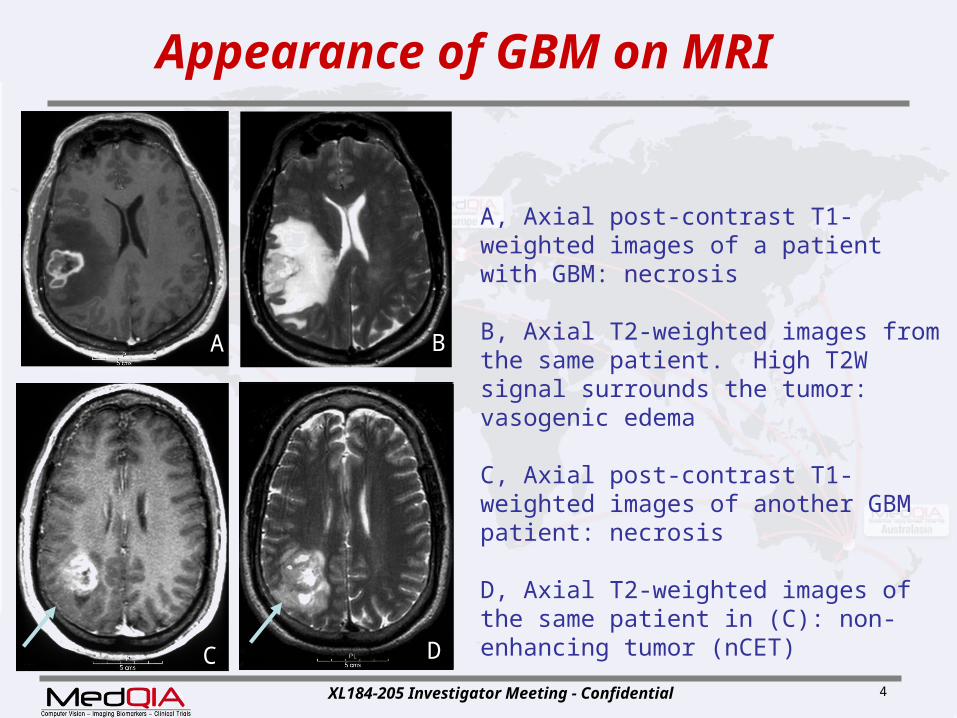
A, Axial post-contrast T1-weighted images of a patient with GBM: necrosis
B, Axial T2-weighted images from the same patient. High T2W signal surrounds the tumor: vasogenic edema
C, Axial post-contrast T1-weighted images of another GBM patient: necrosis
D, Axial T2-weighted images of the same patient in (C): non-enhancing tumor (nCET)
Appearance of GBM on MRI
A B
C D
XL184-205 Investigator Meeting - Confidential 5
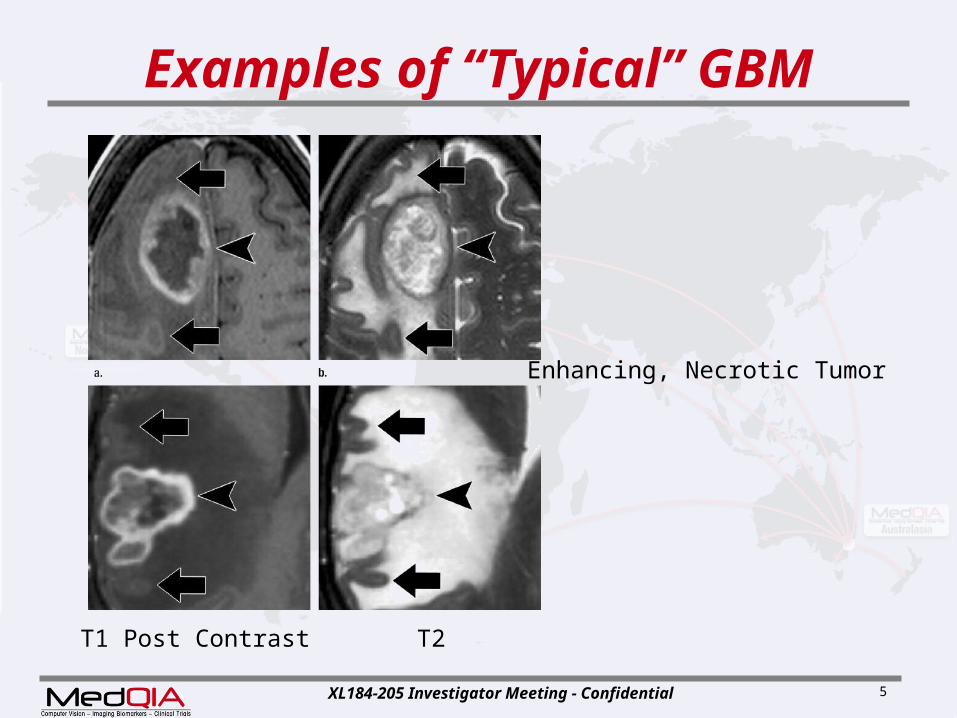
Examples of “Typical” GBM
Enhancing, Necrotic Tumor
T1 Post Contrast T2
XL184-205 Investigator Meeting - Confidential 6
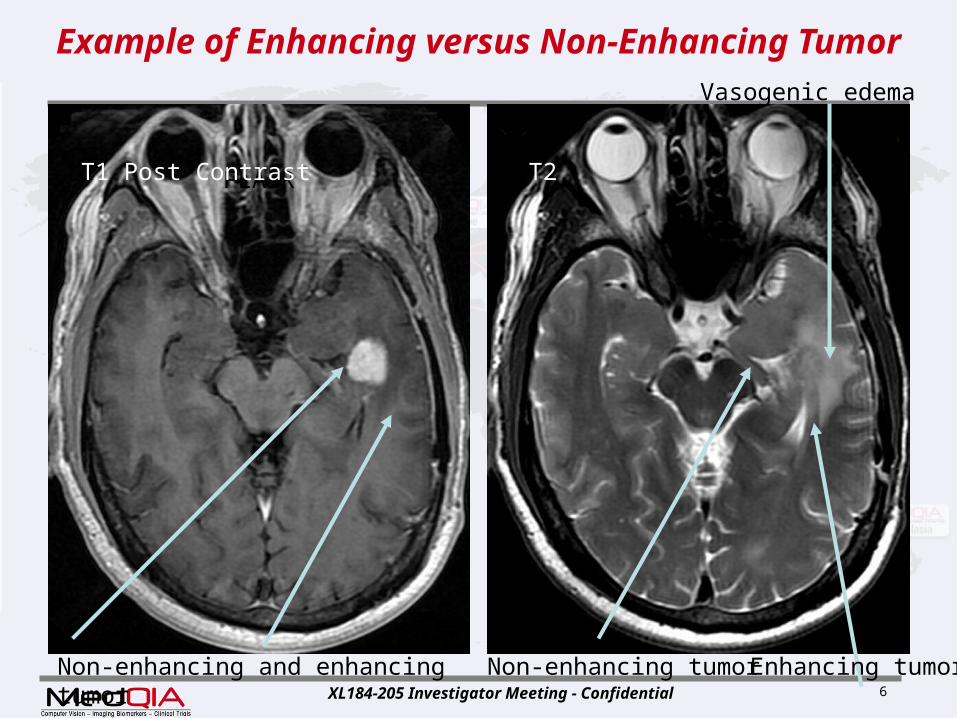
Example of Enhancing versus Non-Enhancing Tumor
FLAIR T2
Non-enhancing and enhancing tumor Non-enhancing tumor
T1 Post Contrast
Enhancing tumor
Vasogenic edema

XL184-205 Investigator Meeting - Confidential 7
FLAIR Can Improve Tumor Visualizationinsert slide to encourage dwi
T2 FLAIR
Tumor
Insert next slide a dwi slide to encourage this is done

XL184-205 Investigator Meeting - Confidential 8
T2 versus FLAIR: More examples
Tumor and edema
Tumor only
T2 FLAIR

XL184-205 Investigator Meeting - Confidential 9
Examples of non contrast enhancing tumor GBM
Non-enhancing GBM showing biopsy site
Intraventricular GBM with enhancing and non-enhancing tumor
GB
M I
mag
ing
XL184-205 Investigator Meeting - Confidential 10
Role of Imaging in Clinical Trials
• Imaging plays an important role in all Clinical trials– Phase I
Primary goal tolerated dose Imaging exploratory
o Mechanism of actiono Pilot efficacy
– Phase III Primary goal overall survival Imaging
o used at clinical sites to manage patientso Secondary endpoints

XL184-205 Investigator Meeting - Confidential 11
Challenges in GBM assessment
– Phase II goal therapeutic effect Imaging is a primary endpoint
o ( radiographic response + with clinical status)
• Substantial challenges in Radiologic
evaluation of tumor size during clinical trials
• Critical Role of IRF to standardize– Image acquisition
Across sites Across time lines
– Assessment of tumor burden

XL184-205 Investigator Meeting - Confidential 12
Challenges in GBM assessment
• Challenges include:• – Technical imaging considerations (Please add
slides, move slide 39)• – Selection of lesions (Please add slides)• – Measurement approaches (Discuss confluence and
splitting lesions, also measuring multi nodular lesions, measuring around surgical cavity…)
• – Response criteria • – Interval between tumor measurements and
response confirmation (delete this bullet)• – Validity of imaging as a measure of efficacy (delete
this bullet)
XL184-205 Investigator Meeting - Confidential 13
Technical Considerations
• Same imaging technique at every time point
• Measurements in the Axial plane
• Acquisition 3-mm, skip 0-mm T1-weighted C+ images improve resolution – Increase acquisition time from 3 minutes to 5–6
minutes improved resolution is a great benefit
• Postcontrast axial – Same Gd dose each time– Standardized time interval post Gd (>5min <
10min)
Move to follow slide 15.

XL184-205 Investigator Meeting - Confidential 14
Measurement Techniques
Two major approaches for evaluation of contrast-enhancing tumor size:
1. Diameter-based measurement on – single-axial section containing largest
diameter
2. Computer-assisted volumetric
analysis– all sections containing tumor
– Slide 16 and 17: Need to add diameter based measurement examples, goal here is for site measurements to hopefully be in line with IRF measurements (may want to take off volumetrics, not assessable at site level)
XL184-205 Investigator Meeting - Confidential 15
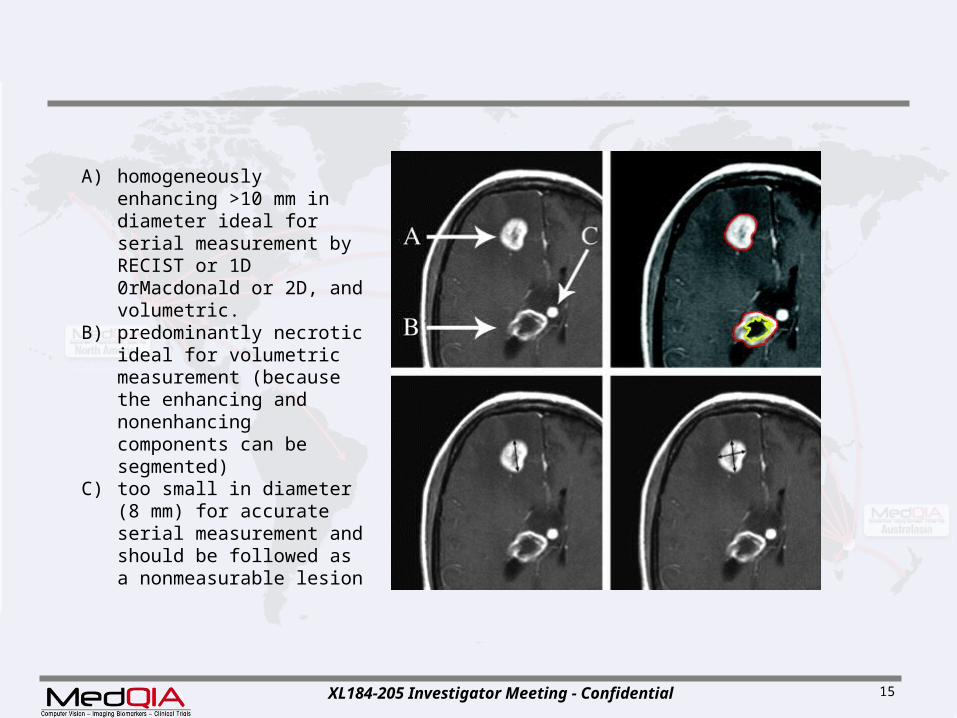
A) homogeneously enhancing >10 mm in diameter ideal for serial measurement by RECIST or 1D 0rMacdonald or 2D, and volumetric.
B) predominantly necrotic ideal for volumetric measurement (because the enhancing and nonenhancing components can be segmented)
C) too small in diameter (8 mm) for accurate serial measurement and should be followed as a nonmeasurable lesion
XL184-205 Investigator Meeting - Confidential 16
Macdonald Criteria (2D)
• To date, most trials for GBM use the WHO-based “Macdonald criteria”– Measure
maximal enhancing tumor diameter on single axial Post C T1 image, and
largest perpendicular diameter same image– Calculate product of the 2 diameters– Sum Measurements from multiple lesions
Macdonald DR Response criteria for phase II studies of supratentorial malignant glioma. J Clin Oncol. 1990;8: 1277-1280

XL184-205 Investigator Meeting - Confidential 17
Limitations of Macdonald• Key Limitations
– Necrotic portions of lesions– Assumption contrast enhanced tissue =
tumor enhancement nonspecific
o reflects disrupted blood-brain barriero induced by of nontumoral processes
» inflammation,
» seizure activity, » postsurgical changes, and » radiation necrosis.
enhancement influencedo changes in corticosteroid dose and o radiologic technique
– Changes in the enhancing area cannot be equated with changes in tumor size or tumor growth/activity
XL184-205 Investigator Meeting - Confidential 18
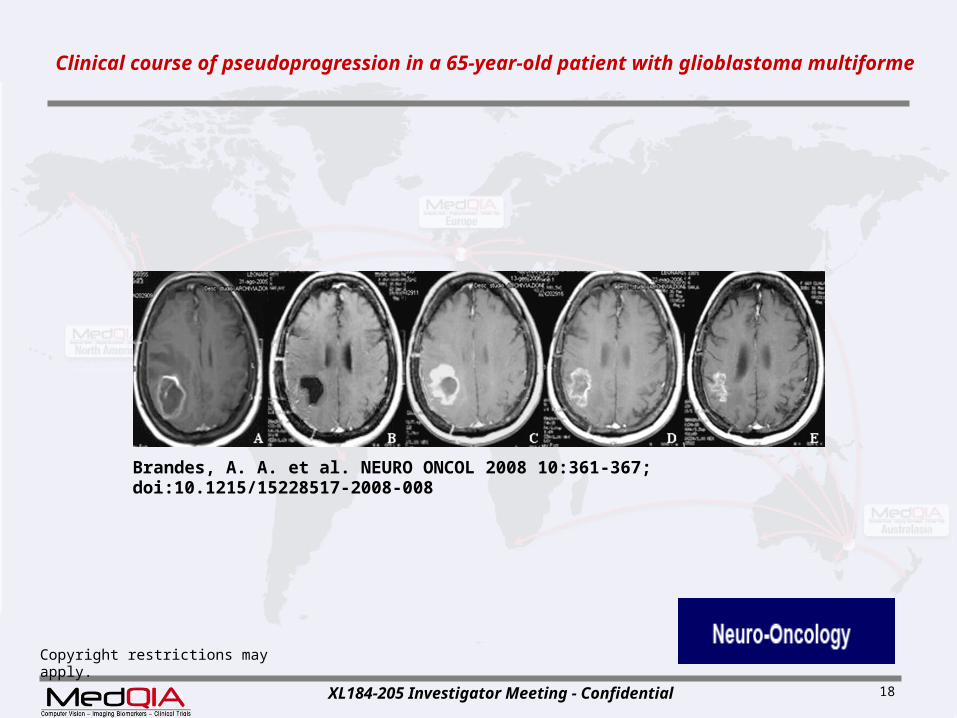
Copyright restrictions may apply.
Brandes, A. A. et al. NEURO ONCOL 2008 10:361-367; doi:10.1215/15228517-2008-008
Clinical course of pseudoprogression in a 65-year-old patient with glioblastoma multiforme
XL184-205 Investigator Meeting - Confidential 19
Journal of Clinical Oncology, Vol 28, No 11 (April 10), 2010: pp. 1963-1972
Updated Response Assessment Criteria for High-Grade Gliomas: Response Assessment in Neuro-Oncology Working Group
Patrick Y. Wen, David R. Macdonald, David A. Reardon, Timothy F. Cloughesy, A. Gregory Sorensen, Evanthia
Galanis, John DeGroot, Wolfgang Wick, Mark R. Gilbert, Andrew B. Lassman, Christina Tsien, Tom Mikkelsen, Eric T.
Wong, Marc C. Chamberlain, Roger Stupp, Kathleen R. Lamborn, Michael A. Vogelbaum, Martin J. van den Bent,
Susan M. Chang
XL184-205 Investigator Meeting - Confidential 20
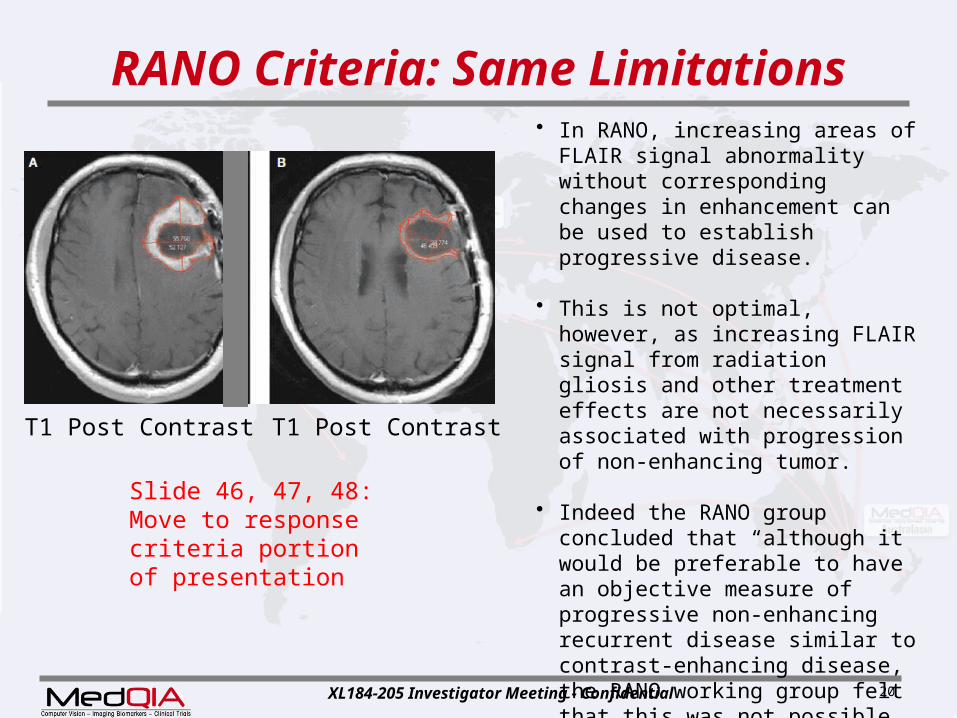
RANO Criteria: Same Limitations
• In RANO, increasing areas of FLAIR signal abnormality without corresponding changes in enhancement can be used to establish progressive disease.
• This is not optimal, however, as increasing FLAIR signal from radiation gliosis and other treatment effects are not necessarily associated with progression of non-enhancing tumor.
• Indeed the RANO group concluded that “although it would be preferable to have an objective measure of progressive non-enhancing recurrent disease similar to contrast-enhancing disease, the RANO working group felt that this was not possible at present given the limitations of current technology.”
T1 Post Contrast T1 Post Contrast
Slide 46, 47, 48: Move to response criteria portion of presentation
XL184-205 Investigator Meeting - Confidential 21
Multicentric Lesions• Approximately one third of malignant
gliomas are multicentric at the time of diagnosis, and in half of these cases, there are discrete foci of enhancement.
• The approach in this situation is to measure and record each separately enhancing lesion that meets inclusion criteria and sum the measurements.
Move to response criteria portion of presentation

XL184-205 Investigator Meeting - Confidential 22
Nonmeasurable Lesions
• Important in Clinical Trials – Tumor progression may occur in these
sites
• Nonmeasurable lesion includes:– Foci of enhancement <8mm– Region of T2-weighted hyperintensity
surrounding enhancing tumor – Discrete foci of non-enhancing T2-
weighted hyperintensity (multicentric tumor)
– Hemorrhagic or predominantly cystic or necrotic lesions
– Leptomeningeal tumor Move to lesion selection portion of the presentation.

XL184-205 Investigator Meeting - Confidential 23
2nd f/u: remote non-enhancing disease
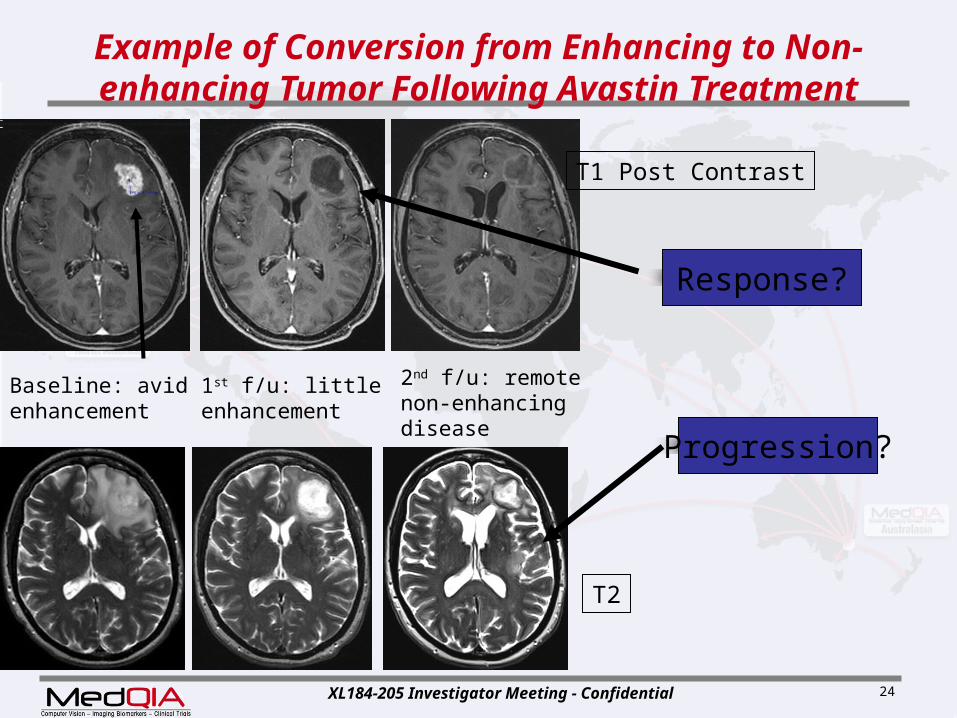
Example of Conversion from Enhancing to Non-enhancing Tumor Following Avastin
Treatment
Baseline: avid enhancement
T1 Post Contrast
T2
1st f/u: little enhancement
XL184-205 Investigator Meeting - Confidential 24
Example of Conversion from Enhancing to Non-enhancing Tumor Following Avastin
Treatment
Baseline: avid enhancement
1st f/u: little enhancement
T1 Post Contrast
2nd f/u: remote non-enhancing disease
T2
Response?
Progression?

XL184-205 Investigator Meeting - Confidential 25
Example of Faintly Enhancing Tumor (Post Treatment)
FLAIR FLAIR
Faintly enhancing tumor Faintly enhancing tumor
T1 Post Contrast
: Can you add measurement caliper placements on these images (to be consistent with IRF measurements)

XL184-205 Investigator Meeting - Confidential 26
Example of Conversion from Enhancing to Non-enhancing Tumor Following Treatment
Baseline: avid enhancement 1st Follow-up: only tiny nodular peripheral enhancement
T1 Post ContrastT1 Post ContrastT1 Post Contrast
2nd Follow-up: no enhancement. New distant disease (see next slide)

XL184-205 Investigator Meeting - Confidential 27
Same Case: Development of distant non-enhancing tumor. Example of conversion from local to diffuse
disease following treatment.
Baseline: enhancing tumorand vasogenic edema
1st Follow-up: much lessedema. Non-enhancingtumor remains.
T2T2T2
2nd Follow-up: interval development of non-enhancing, ill-defined, tumor > 3cm from primary site, thus scored as diffuse progression

XL184-205 Investigator Meeting - Confidential 28
Example of Multifocal Disease
T2
Two sites of enhancing tumorGreater than 3 cm from primary site, separated by normal brain
T1 Post Contrast

XL184-205 Investigator Meeting - Confidential 29
Same Patient: Conversion from Multifocal to Diffuse Disease Following Treatment
T2
Distant non-enhancing tumorwith ill-defined margins, enhancement atprimary site goes away.
Non-enhancing tumor – no cortical ribbonVasogenic Edema – cortical ribbon seen
T1 Post Contrast

XL184-205 Investigator Meeting - Confidential 30
Another Example of Multifocal Disease
T1 Post Contrast FLAIR
Multifocal, enhancing tumor
XL184-205 Investigator Meeting - Confidential 31
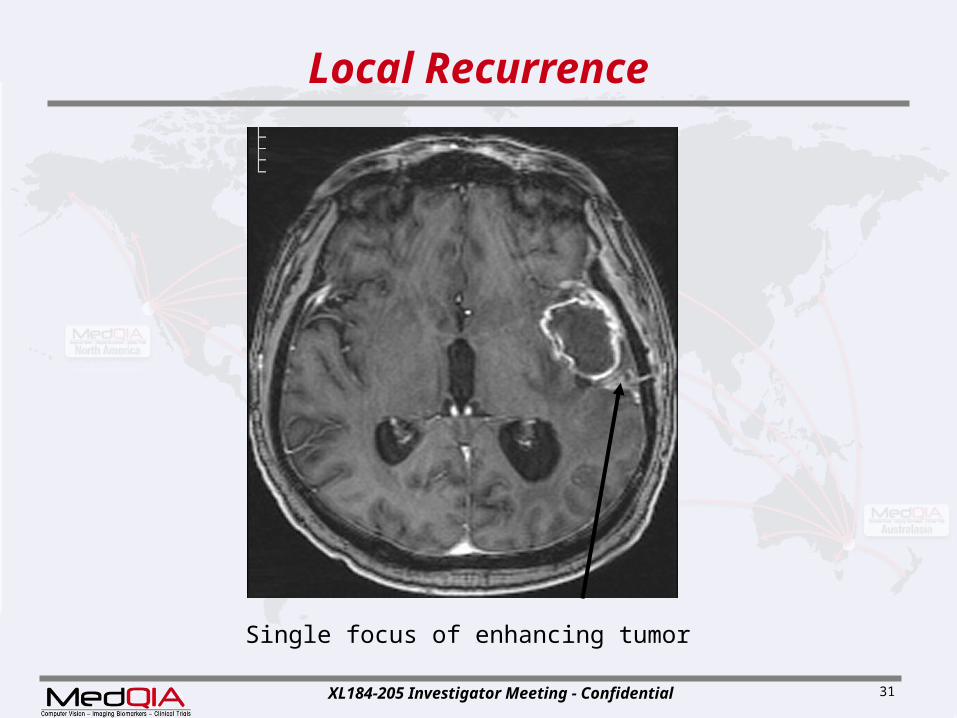
Local Recurrence
Single focus of enhancing tumor
XL184-205 Investigator Meeting - Confidential 32
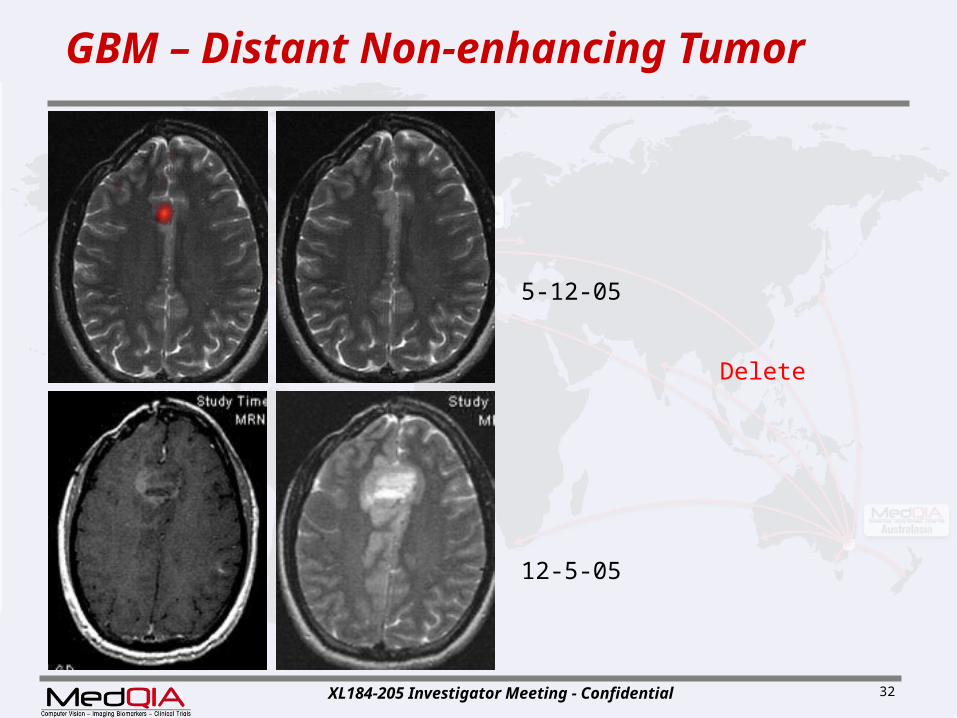
5-12-05
GBM – Distant Non-enhancing Tumor
12-5-05
Delete
XL184-205 Investigator Meeting - Confidential 33
Corticosteroid-induced Magnetic Resonance Imaging Changes
Post Steroids – 90% patients had decreased
enhancement or T2 signal 30% patients had 25%+ reduction in
enhancing tumor 50% had 25%+ reduction in edema
– Maximal effect was achieved at 2 weeks Thus 2 weeks stable dose steroid
recommended before baseline imaging.
J Clin Oncol. 1994 Sep;12(9):1886-9.
How to add steroid on study to maintain image accuracy (ie, contrast intolerant subjects what steroid prescribed previous to next MRI)

XL184-205 Investigator Meeting - Confidential 34
Initial scan 2 weeks after steroid tx
Edema – often only temporary reduction in edema
T1 Post Contrast
Steroids: Example of Effect on Edema and Enhancement

XL184-205 Investigator Meeting - Confidential 35
Computer-Aided Volumetric Methods
• Segmentation Algorithm generates border between the enhancing and non-enhancing
regions on all adjacent axial sections
• Neuroradiologist – Reviews contours– Edits contour if needed
• Program Calculates– enhancing volume,– Non-enhancing volume (i.e., the centrally necrotic
or cystic portion)– Total or combined lesion volume in cubic– Bi dimensional measurements
XL184-205 Investigator Meeting - Confidential 36
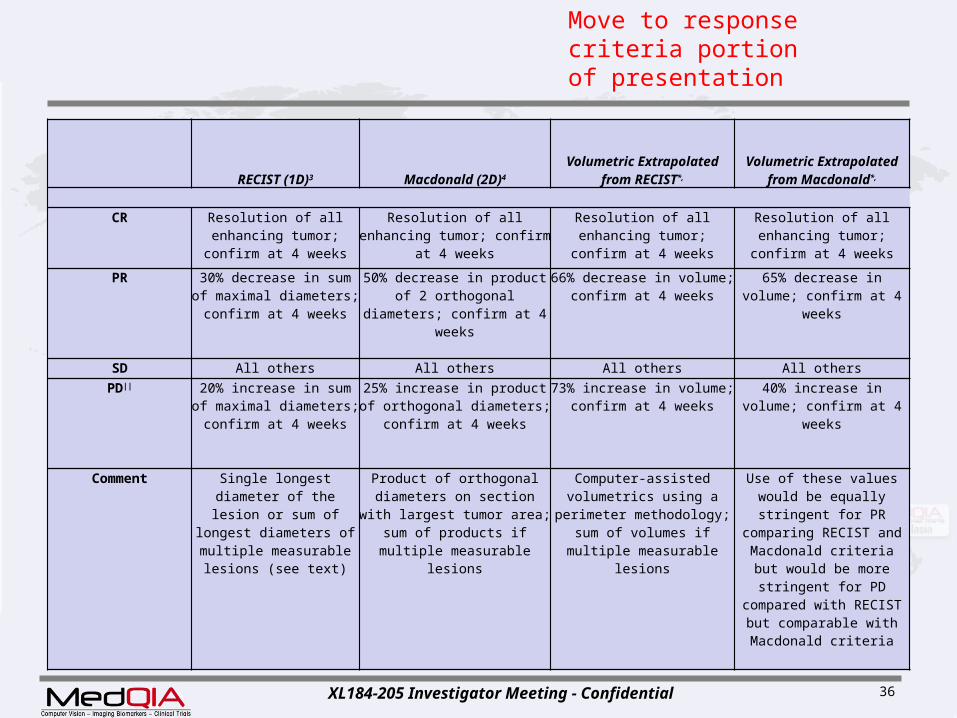
RECIST (1D)3 Macdonald (2D)4
Volumetric Extrapolated from RECIST*,
Volumetric Extrapolated from
Macdonald*,
CR Resolution of all enhancing tumor; confirm at 4 weeks
Resolution of all enhancing tumor; confirm at 4 weeks
Resolution of all enhancing tumor; confirm at 4 weeks
Resolution of all enhancing tumor; confirm
at 4 weeks
PR 30% decrease in sum of maximal diameters; confirm at 4 weeks
50% decrease in product of 2 orthogonal diameters;
confirm at 4 weeks
66% decrease in volume; confirm at 4 weeks
65% decrease in volume; confirm at 4 weeks
SD All others All others All others All others
PD|| 20% increase in sum of maximal diameters; confirm at 4 weeks
25% increase in product of orthogonal diameters;
confirm at 4 weeks
73% increase in volume; confirm at 4 weeks
40% increase in volume; confirm at 4 weeks
Comment Single longest diameter of the lesion or sum of longest diameters of multiple measurable
lesions (see text)
Product of orthogonal diameters on section with largest tumor area; sum of
products if multiple measurable lesions
Computer-assisted volumetrics using a
perimeter methodology; sum of volumes if multiple
measurable lesions
Use of these values would be equally stringent for
PR comparing RECIST and Macdonald criteria but
would be more stringent for PD compared with
RECIST but comparable with Macdonald criteria
Move to response criteria portion of presentation

XL184-205 Investigator Meeting - Confidential 37
Dynamic Contrast Enhanced (DCE)-MRIPhysics
• Gadolinium causes a change in the longitudinal relaxivity (R1 = 1/T1) of surrounding water proportional to concentration
• Dynamic Contrast Enhanced MRI uses gadolinium-based contrast agents as a tracer for pharmacokinetic analysis by collecting dynamic T1-weighted images during a bolus
Plasma Cp(t)
RBC
Vein, Cv(t)
TissueEESCe(t)Ve
Ktrans
kep
1-Hct
Artery, Ca(t)
Two-CompartmentTofts Model(most common)
XL184-205 Investigator Meeting - Confidential 38
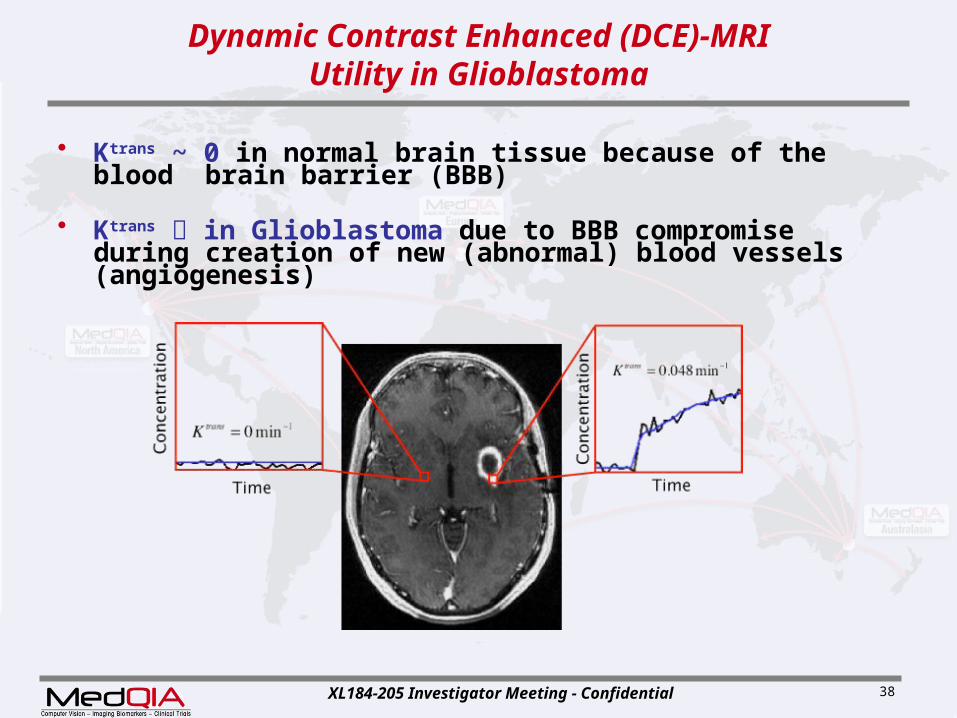
Dynamic Contrast Enhanced (DCE)-MRIUtility in Glioblastoma
• Ktrans ~ 0 in normal brain tissue because of the blood brain barrier (BBB)
• Ktrans in Glioblastoma due to BBB compromise during creation of new (abnormal) blood vessels (angiogenesis)
XL184-205 Investigator Meeting - Confidential 39
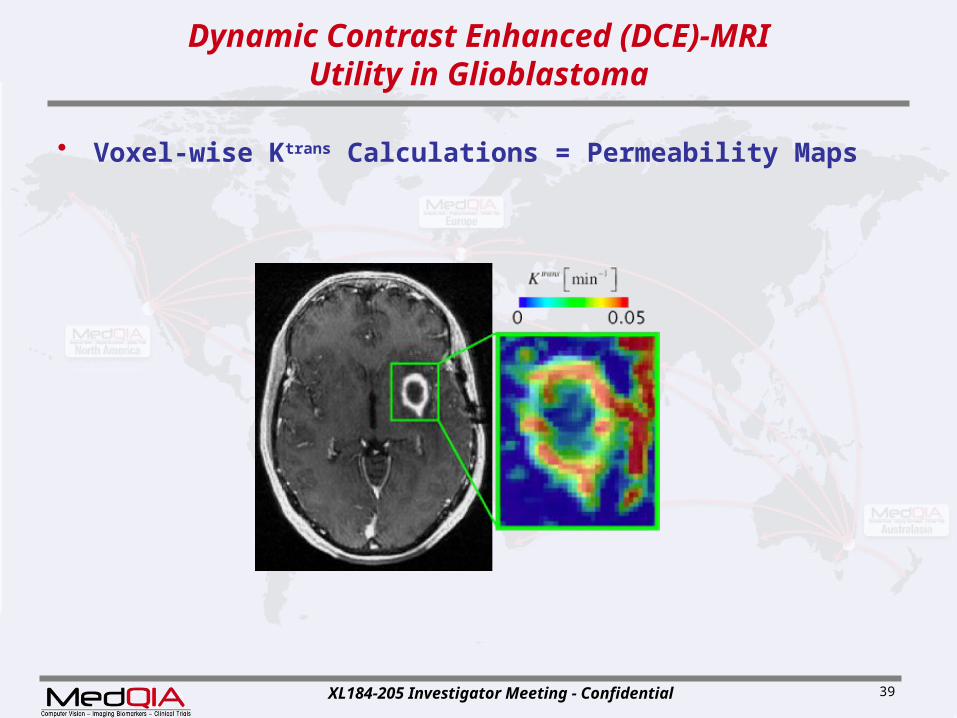
Dynamic Contrast Enhanced (DCE)-MRIUtility in Glioblastoma
• Voxel-wise Ktrans Calculations = Permeability Maps

XL184-205 Investigator Meeting - Confidential 40
Dynamic Contrast Enhanced (DCE)-MRIUtility in Glioblastoma
• Voxel-wise Ktrans Calculations = Permeability Maps– Biomarker for anti-angiogenic drugs targeting abnormal blood
vessels
Early Treatment Failure

XL184-205 Investigator Meeting - Confidential 41
Dynamic Contrast Enhanced (DCE)-MRIUtility in Glioblastoma
• Voxel-wise Ktrans Calculations = Permeability Maps– Biomarker for anti-angiogenic drugs targeting abnormal blood
vessels– Widely accepted in clinical trials of other cancers
O’Connor, Br J Cancer 2007
XL184-205 Investigator Meeting - Confidential 42
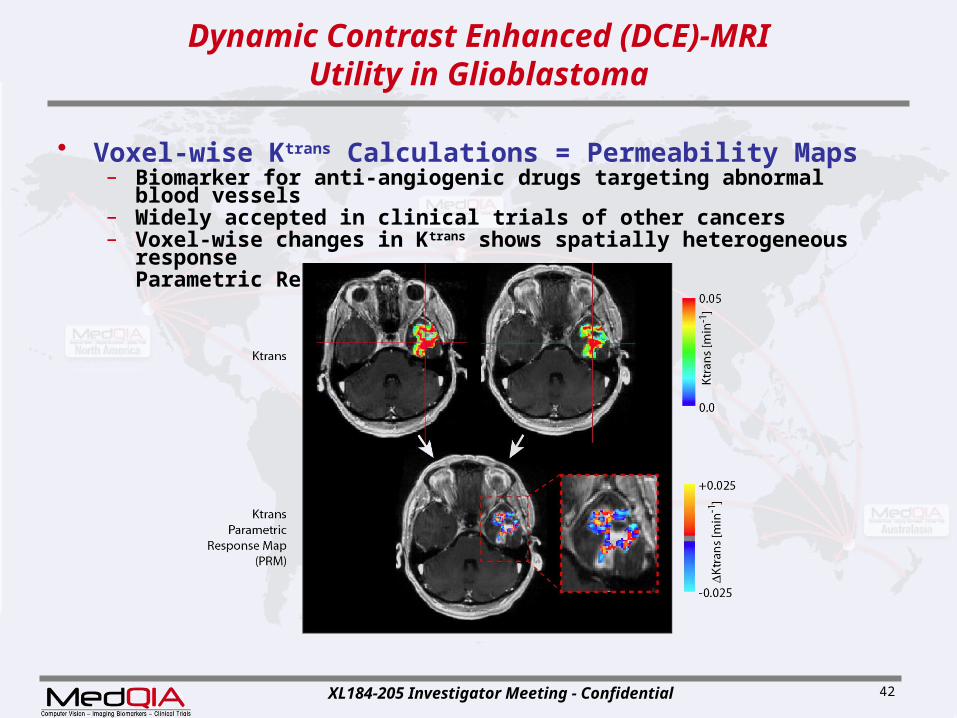
Dynamic Contrast Enhanced (DCE)-MRIUtility in Glioblastoma
• Voxel-wise Ktrans Calculations = Permeability Maps– Biomarker for anti-angiogenic drugs targeting abnormal blood
vessels– Widely accepted in clinical trials of other cancers– Voxel-wise changes in Ktrans shows spatially heterogeneous
responseParametric Response Maps (PRM)

XL184-205 Investigator Meeting - Confidential 43
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements• QC:
• T1 fit (R2 > 0.7, P < 0.05)• T1 in Normal Tissues
1.5T: Breger, 1989; Steen, 1994; Whittall, 1997; Haacke, 19993.0T: Wansapura, 1999; Helms, 2008
XL184-205 Investigator Meeting - Confidential 44
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements
• Issues with Repeatability• Random error, biological variation• Confidence depends on
• Choice of model (2-compartment, 3-compartment, etc)
• ROI definition• AIF determination
XL184-205 Investigator Meeting - Confidential 45
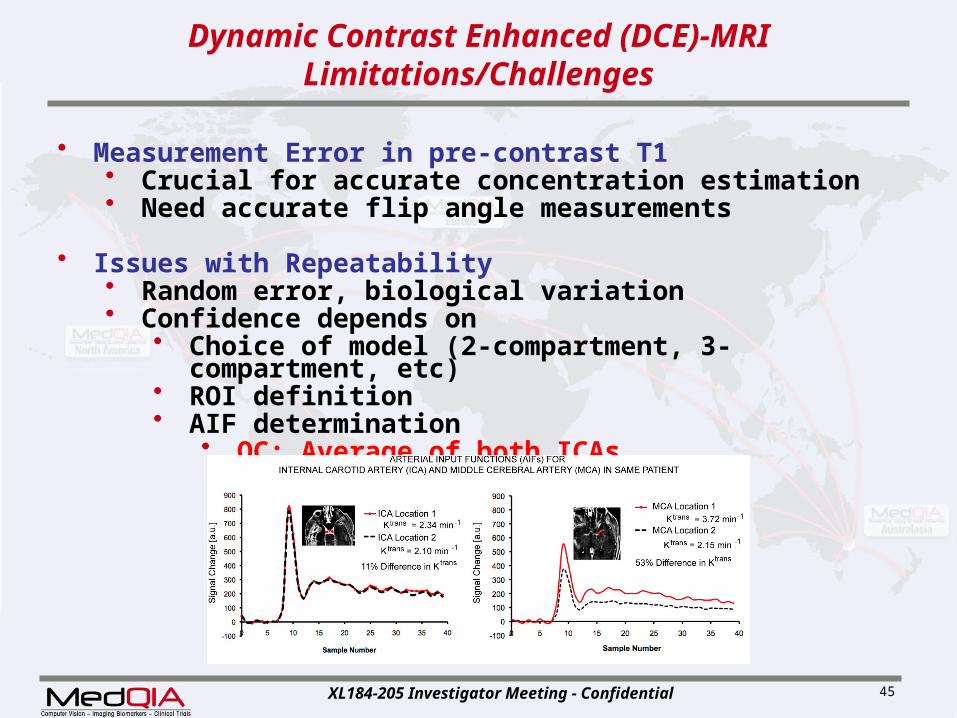
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements
• Issues with Repeatability• Random error, biological variation• Confidence depends on
• Choice of model (2-compartment, 3-compartment, etc)
• ROI definition• AIF determination
• QC: Average of both ICAs
XL184-205 Investigator Meeting - Confidential 46
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements
• Issues with Repeatability• Random error, biological variation• Confidence depends on
• Choice of model (2-compartment, 3-compartment, etc)
• ROI definition• AIF determination
• Median Change in Ktrans > 40% Reflects True Response
XL184-205 Investigator Meeting - Confidential 47
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements
• Issues with Repeatability• Random error, biological variation• Confidence depends on
• Choice of model (2-compartment, 3-compartment, etc)
• ROI definition• AIF determination
• Median Change in Ktrans > 40% Reflects True Response
• Failure to Detect Response• Sampling at wrong time point during treatment• Averaging effects over ROI/VOI
XL184-205 Investigator Meeting - Confidential 48
Dynamic Contrast Enhanced (DCE)-MRILimitations/Challenges
• Measurement Error in pre-contrast T1• Crucial for accurate concentration estimation• Need accurate flip angle measurements
• Issues with Repeatability• Random error, biological variation• Confidence depends on
• Choice of model (2-compartment, 3-compartment, etc)
• ROI definition• AIF determination
• Median Change in Ktrans > 40% Reflects True Response
• Failure to Detect Response• Sampling at wrong time point during treatment• Averaging effects over ROI/VOI
• Solution: Histogram and Voxel-wise analyses

XL184-205 Investigator Meeting - Confidential 49
Dynamic Susceptibility Contrast MRIPhysics
• Gadolinium also has a transient effect on the magnetic susceptibility on blood and tissue water in high concentrations
Magnetic Susceptibility

XL184-205 Investigator Meeting - Confidential 50
Dynamic Susceptibility Contrast (DSC) MRIPhysics
• Gadolinium also has a transient effect on the magnetic susceptibility on blood and tissue water in high concentrations
• Gadolinium causes signal loss on T2*-weighted images
Pre-Injection During Bolus Passage
Dark = Vessels
XL184-205 Investigator Meeting - Confidential 51
Dynamic Susceptibility Contrast (DSC) MRIPhysics
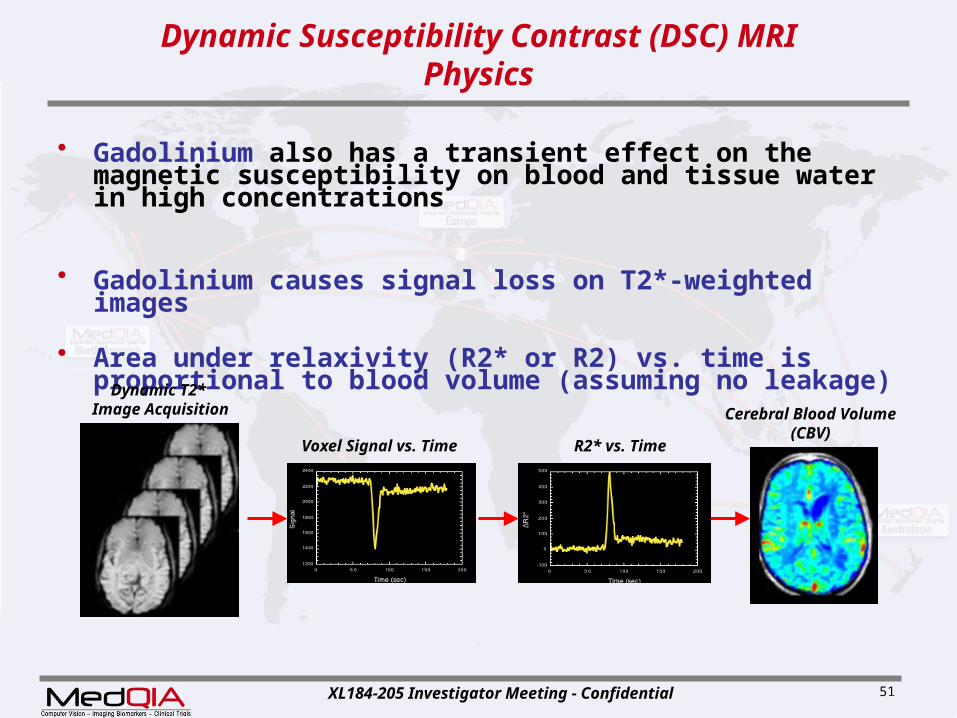
• Gadolinium also has a transient effect on the magnetic susceptibility on blood and tissue water in high concentrations
• Gadolinium causes signal loss on T2*-weighted images
• Area under relaxivity (R2* or R2) vs. time is proportional to blood volume (assuming no leakage)
Voxel Signal vs. Time
Dynamic T2* Image Acquisition
R2* vs. Time
Cerebral Blood Volume(CBV)

XL184-205 Investigator Meeting - Confidential 52
Dynamic Susceptibility Contrast (DSC) MRIUtility in Glioblastoma
• Glioblastoma has elevated CBV due to angiogenesis
Post-Contrast T1-Weighted Image DSC-MRI Estimate of CBV
Normal Vessels
AbnormalVascularity

XL184-205 Investigator Meeting - Confidential 53
Dynamic Susceptibility Contrast (DSC) MRIUtility in Glioblastoma
• Change in CBV is associated with successful treatment
XL184-205 Investigator Meeting - Confidential 54
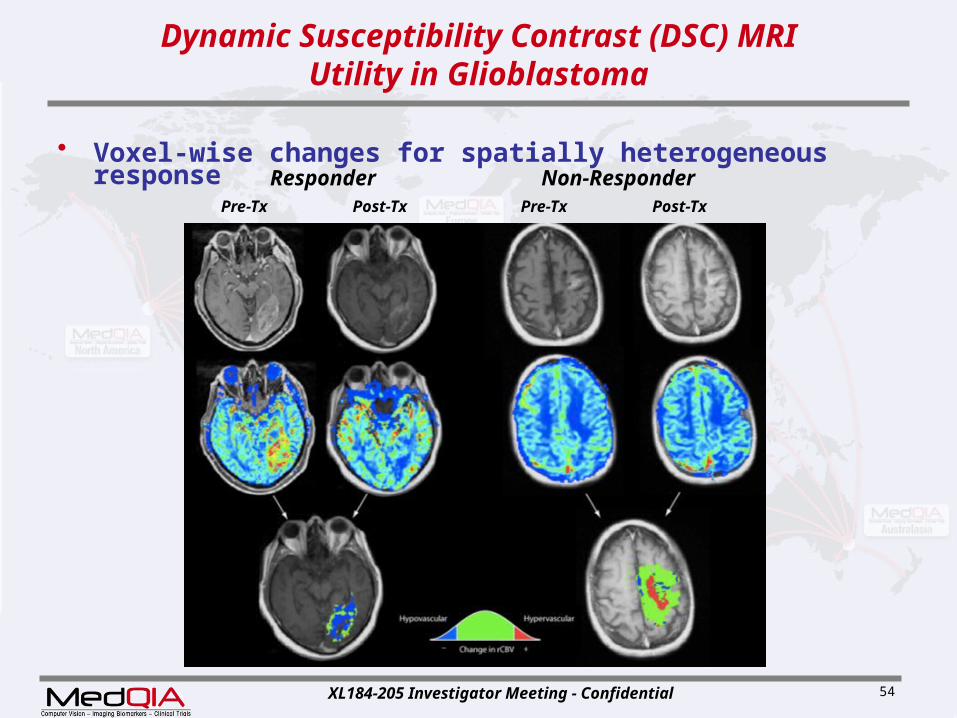
Dynamic Susceptibility Contrast (DSC) MRIUtility in Glioblastoma
• Voxel-wise changes for spatially heterogeneous response
Pre-Tx Post-Tx Pre-Tx Post-Tx
Responder Non-Responder

XL184-205 Investigator Meeting - Confidential 55
Dynamic Susceptibility Contrast (DSC) MRILimitations/Challenges
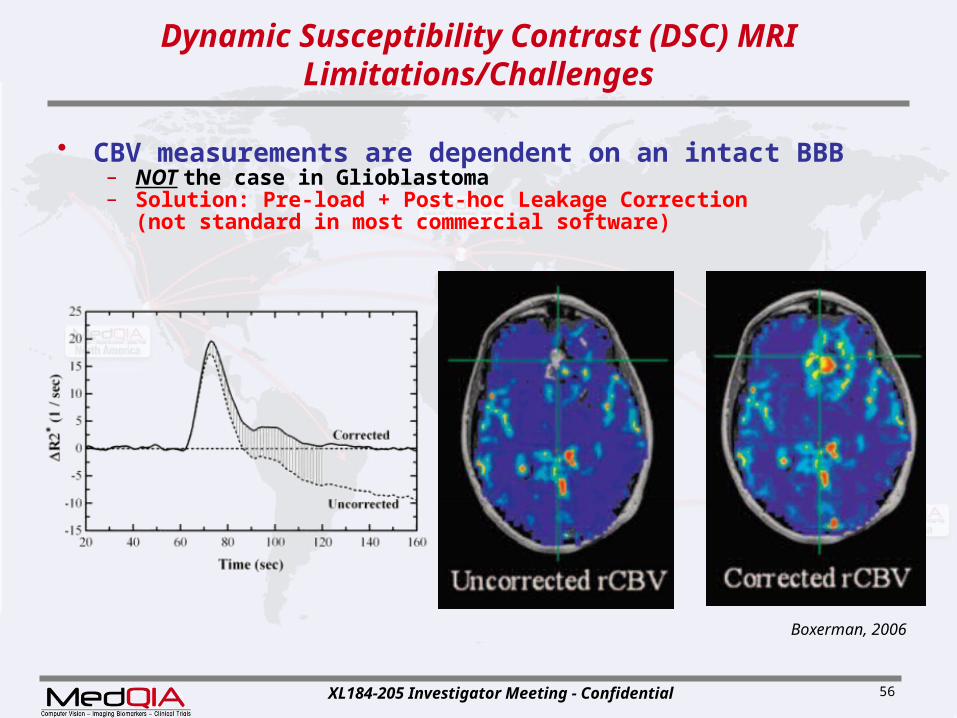
• CBV measurements are dependent on an intact BBB– NOT the case in Glioblastoma
Boxerman, 2006
XL184-205 Investigator Meeting - Confidential 56
Dynamic Susceptibility Contrast (DSC) MRILimitations/Challenges
• CBV measurements are dependent on an intact BBB– NOT the case in Glioblastoma– Solution: Pre-load + Post-hoc Leakage Correction
(not standard in most commercial software)
Boxerman, 2006

XL184-205 Investigator Meeting - Confidential 57
Dynamic Susceptibility Contrast (DSC) MRILimitations/Challenges
• CBV measurements are dependent on an intact BBB– NOT the case in Glioblastoma– Solution: Pre-load + Post-hoc Leakage Correction
(not standard in most commercial software)
• CBV measurements are “relative” – Typical solution is to “normalize” to contralateral tissue– Our Solution: Image Intensity “Standardization” (piecewise
histogram)

XL184-205 Investigator Meeting - Confidential 58
Dynamic Susceptibility Contrast (DSC) MRILimitations/Challenges
• CBV measurements are dependent on an intact BBB– NOT the case in Glioblastoma– Solution: Pre-load + Post-hoc Leakage Correction
(not standard in most commercial software)
• CBV measurements are “relative” – Typical solution is to “normalize” to contralateral tissue– Our Solution: Image Intensity “Standardization” (piecewise
histogram)
• Prone to susceptibility artifacts if patient has surgical hardware
• Must have a good bolus (AIF)– If tight bolus of contrast agent is not achievable, data will be
poor
XL184-205 Investigator Meeting - Confidential 59
[18F]-fluorodeoxyglucose (FDG) PETPhysics
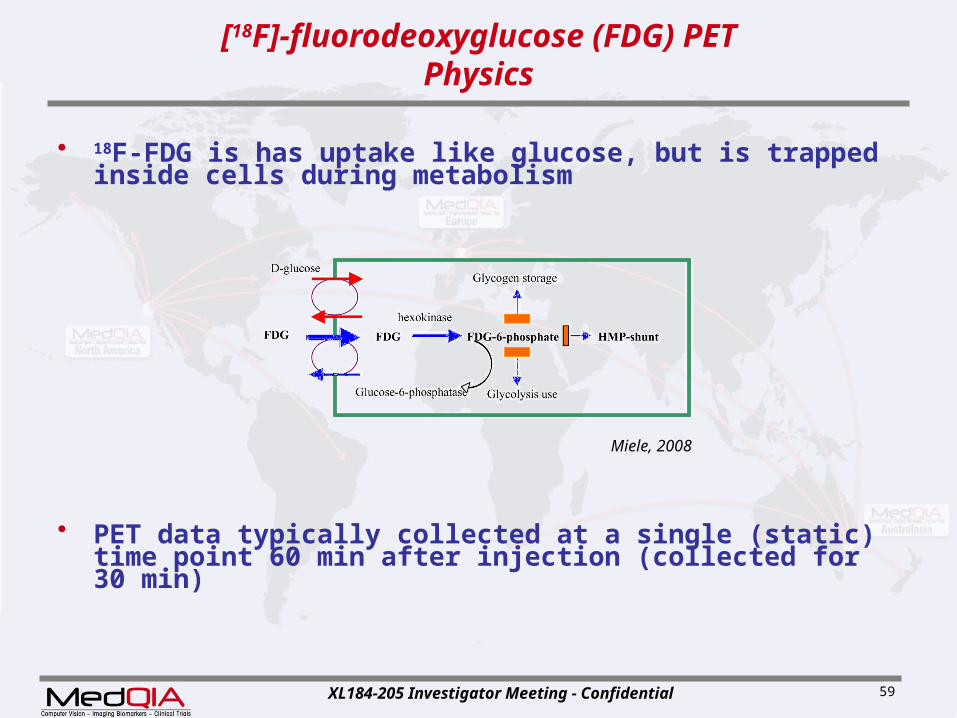
• 18F-FDG is has uptake like glucose, but is trapped inside cells during metabolism
• PET data typically collected at a single (static) time point 60 min after injection (collected for 30 min)
Miele, 2008
XL184-205 Investigator Meeting - Confidential 60
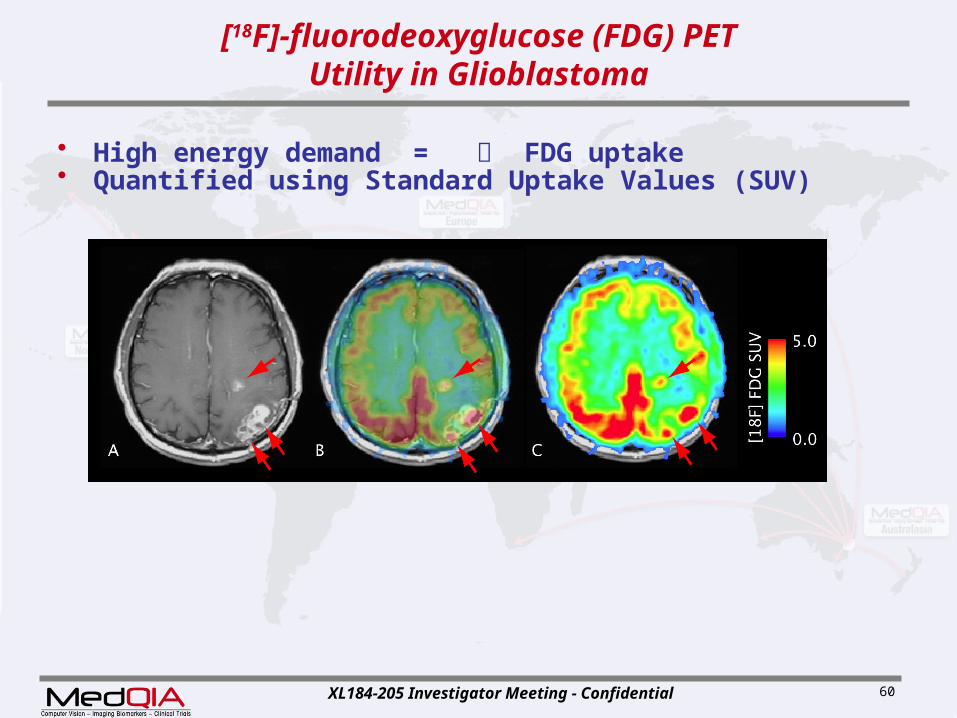
[18F]-fluorodeoxyglucose (FDG) PETUtility in Glioblastoma
• High energy demand = FDG uptake• Quantified using Standard Uptake Values (SUV)

XL184-205 Investigator Meeting - Confidential 61
[18F]-fluorodeoxyglucose (FDG) PETUtility in Glioblastoma
• Voxel-wise changes in PET show heterogeneous response [18F]-FDOPA shown below

XL184-205 Investigator Meeting - Confidential 62
[18F]-fluorodeoxyglucose (FDG) PETLimitations/Challenges
• High uptake in normal cortex

XL184-205 Investigator Meeting - Confidential 63
Multiparametric Imaging
• Combining voxel-wise changes in Perfusion & Diffusion
3 Mo. Post-Tx 6 Mo. Post-Tx 12 Mo. Post-Tx

XL184-205 Investigator Meeting - Confidential 64
Multiparametric Imaging
• Combining Perfusion, Diffusion, & PET