whiplash associated disorders: the pathway from acute to chronic
TRANSCRIPT
Whiplash Associated Disorders: The pathway from
acute to chronic pain James J. Lehman, DC, MBA, FACO
University of Bridgeport College of Chiroprac@c
Learning Objectives
• Determine pa@ent’s prognosis and poten@al to experience chronic pain syndrome following a whiplash injury, prior to providing chiroprac@c services.
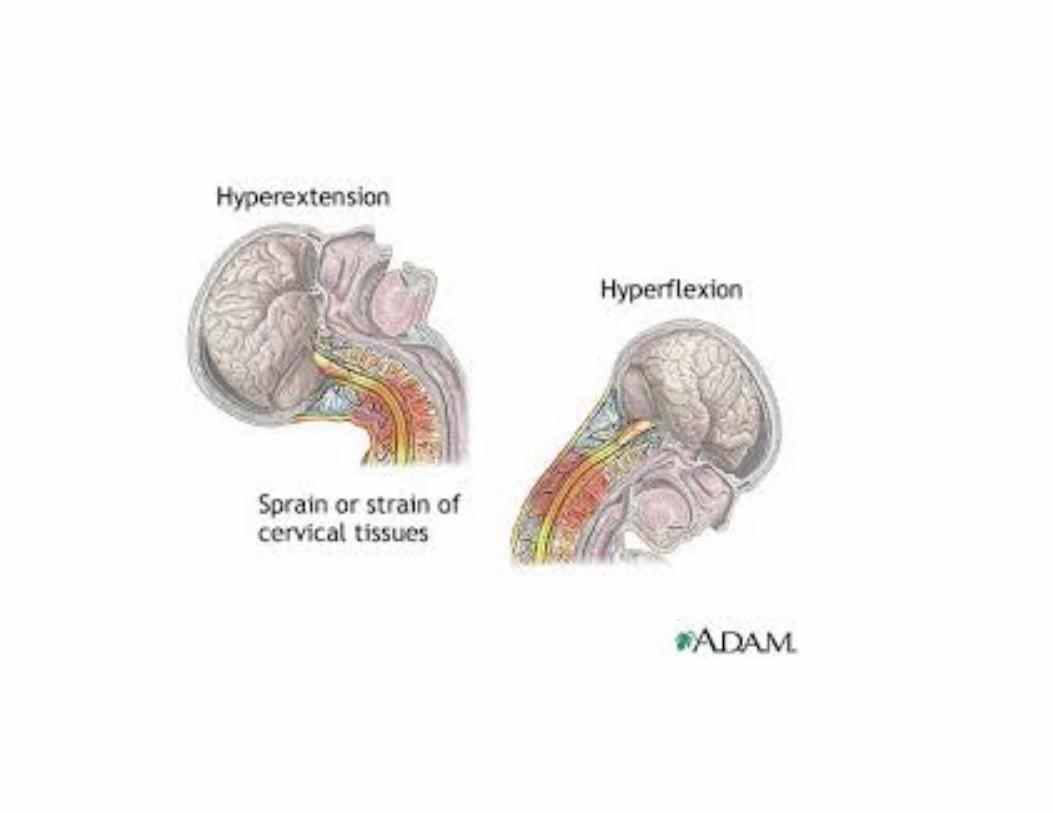
Whiplash Neck Injury
• First described by Crowe in 1928.
• Most common type of injury following motor vehicle crashes
• Usually 2-‐3 weeks for recovery • Yet, up to 42% transi@on from acute to chronic pain status.(1)

“Diagnosis is the key to successful treatment!”
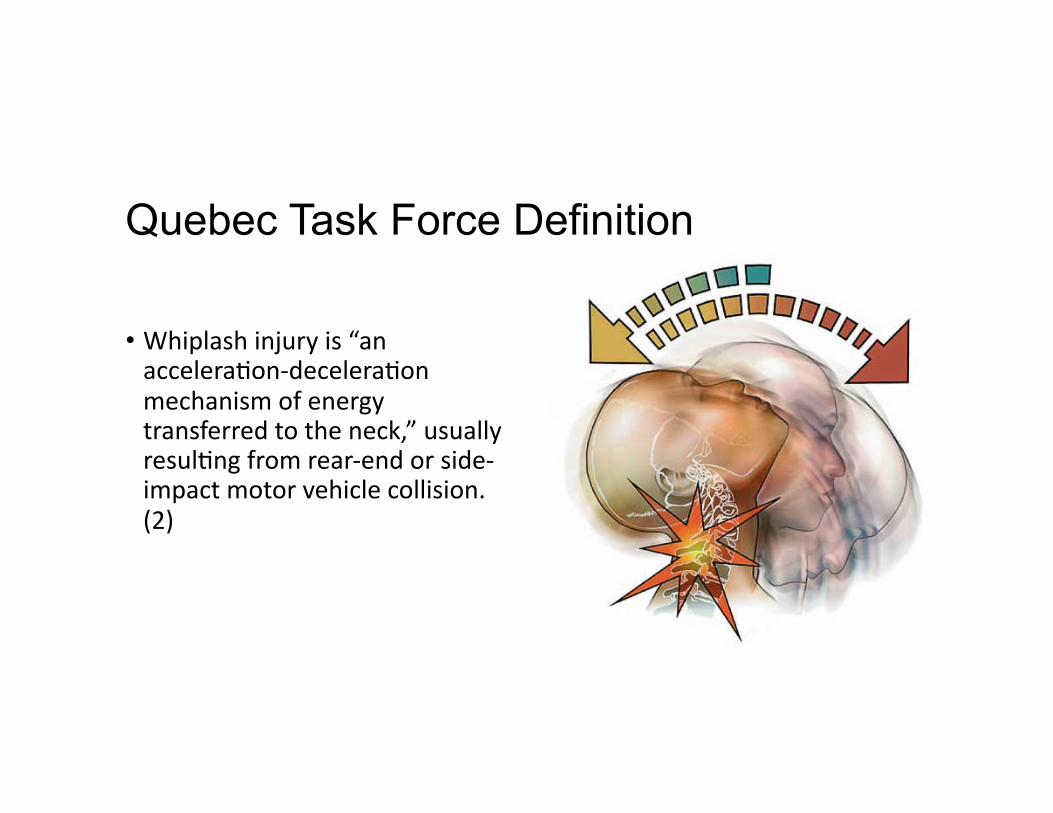
Quebec Task Force Definition
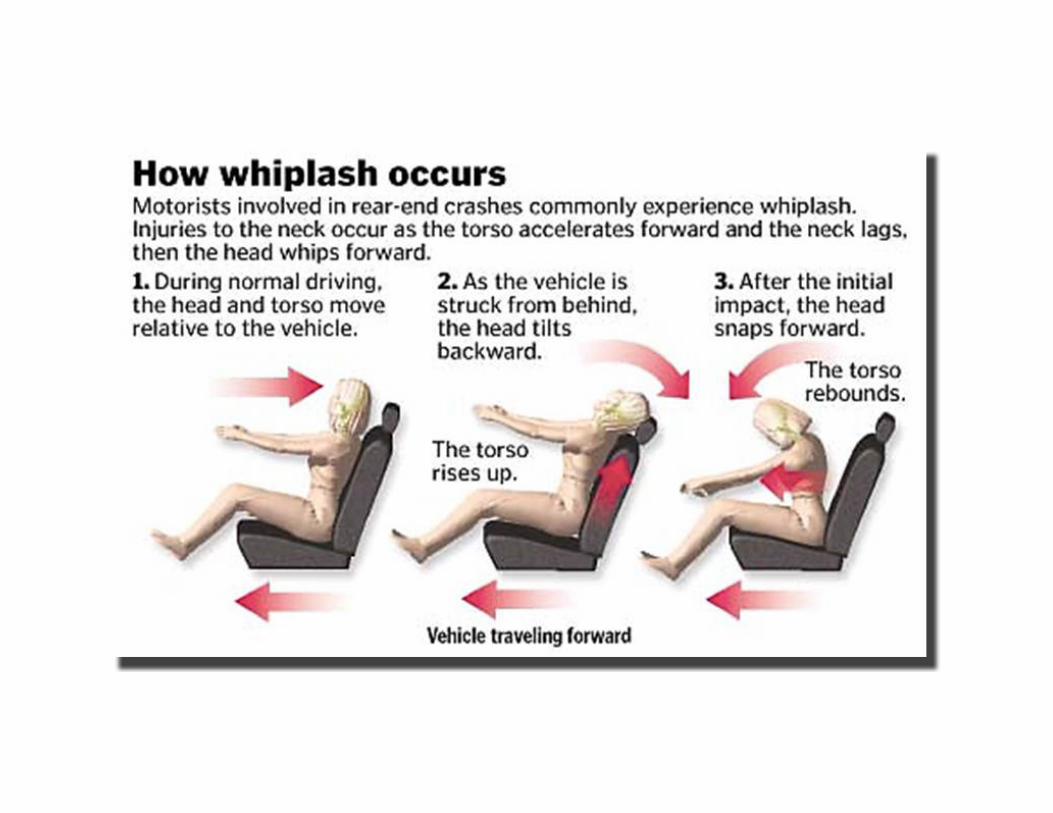
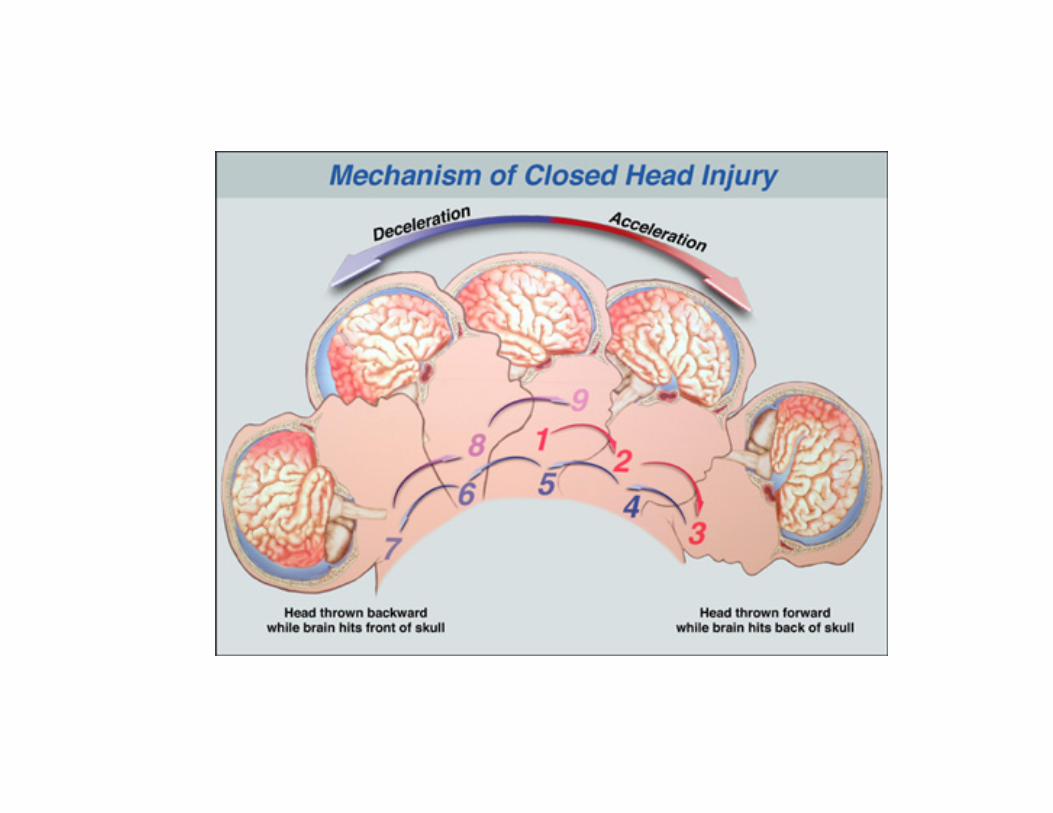
• Whiplash injury is “an accelera@on-‐decelera@on mechanism of energy transferred to the neck,” usually resul@ng from rear-‐end or side-‐impact motor vehicle collision. (2)

Whiplash Injury Costs • Queensland, Australia = $500 million Australian dollars (1994-‐2001)
• MAIC. Whiplash — Review of CTP Queensland Data to 31 Dec 2001. Brisbane, Australia: The Motor Accident Insurance Commission (MAIC); 2002.
• United Kingdom = L3 billion per annum
• Joslin CC, Khan SN, Bannister GC. Long-‐term disability ager neck injury: a compara@ve study. J Bone Joint Surg Br. 2004;86:1032–1034.
• United States = USD $29 billion per annum
• Blincoe L, Seay A, Zaloshnja E, et al . The Economic Impact of Motor Vehicle Crashes, 2000. Washington, DC; Na@onal Highway Traffic Safety Administra@on: 2002.
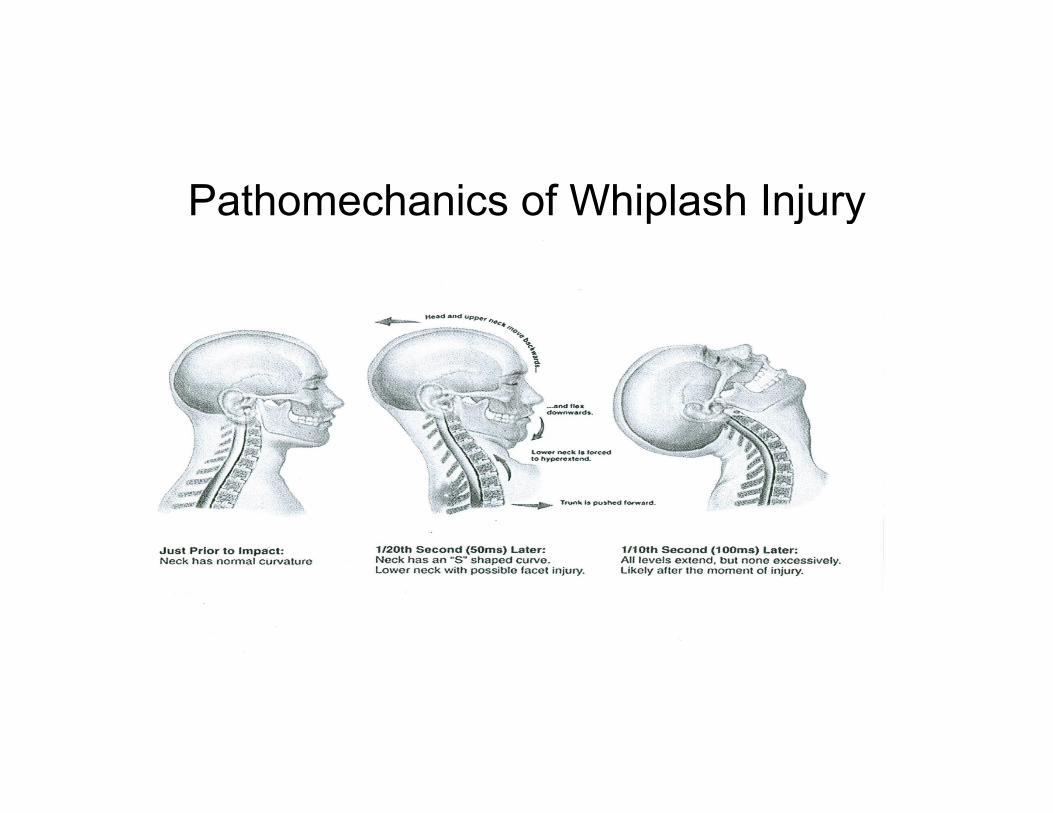
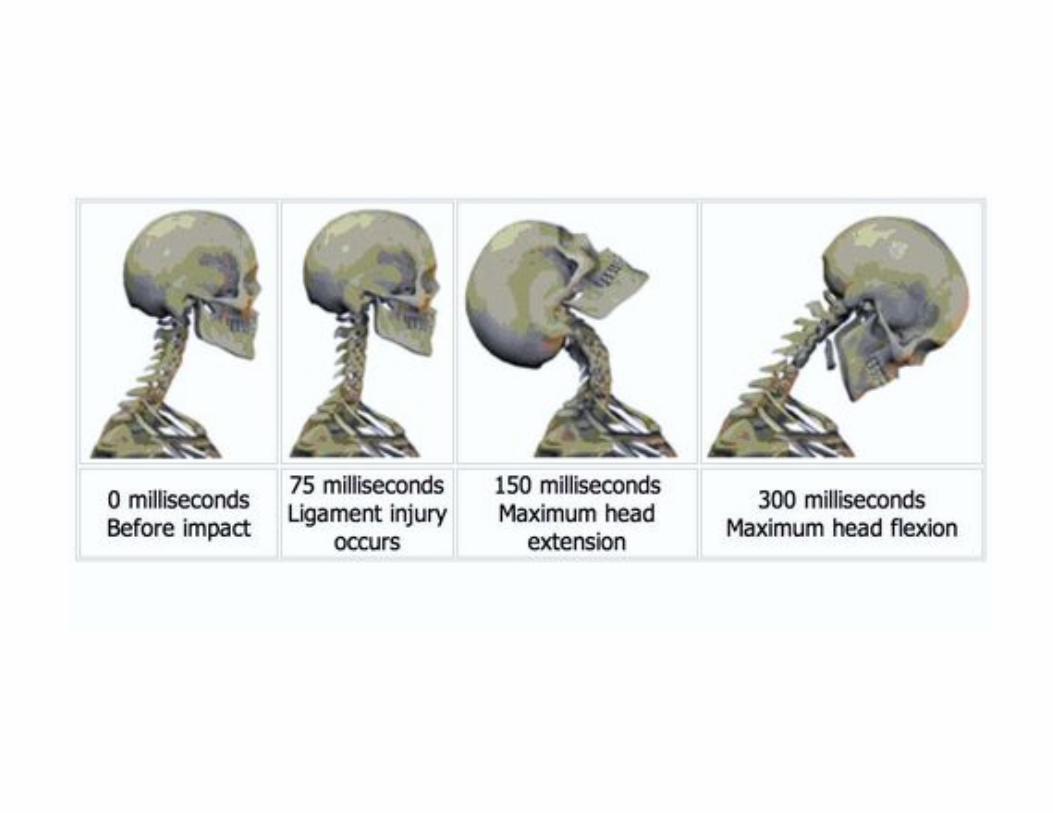
Pathomechanics of Whiplash Injury
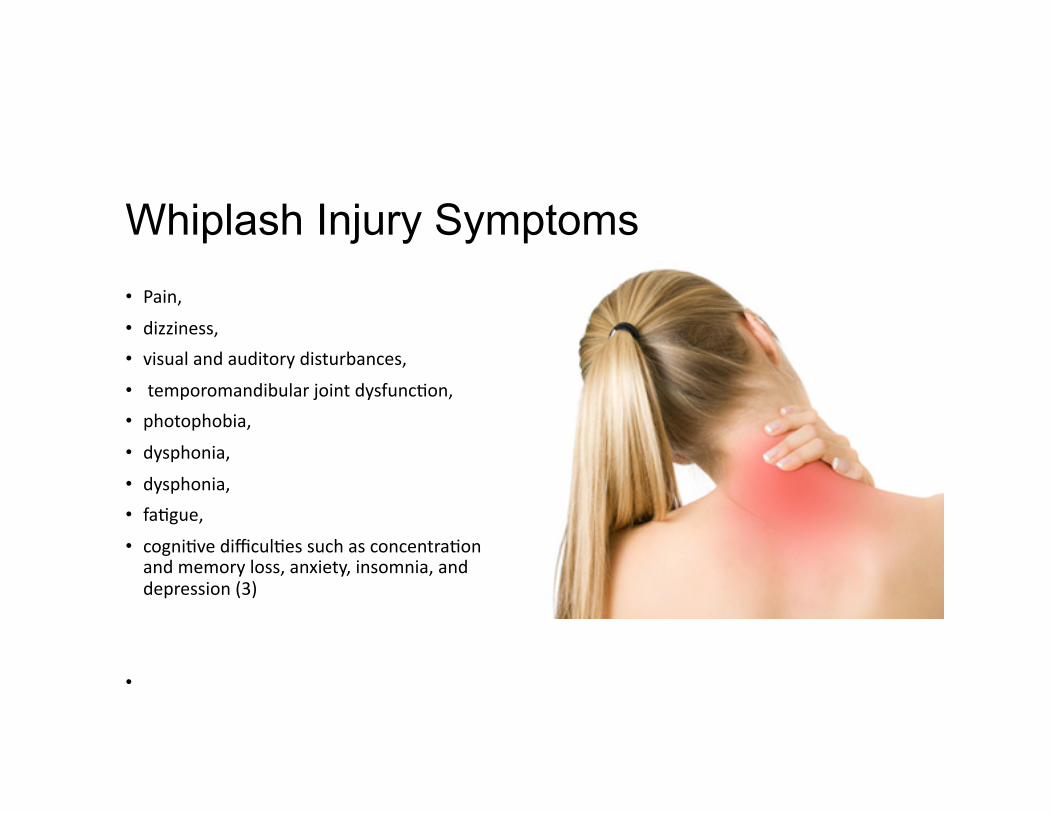
Whiplash Injury Symptoms • Pain, • dizziness, • visual and auditory disturbances, • temporomandibular joint dysfunc@on,
• photophobia, • dysphonia, • dysphonia, • fa@gue, • cogni@ve difficul@es such as concentra@on and memory loss, anxiety, insomnia, and depression (3)
•
Case One = WAD I
• Pa@ent presents with neck complaints including s@ffness or tenderness in the neck regions and no physical signs of injury.
• Spitzer WO, Skovron ML, Salmi LR, et al. Scien@fic monograph of the Quebec Task Force on Whiplash-‐Associated Disorders: redefining “whiplash” and its management. Spine. 1995;20:1S–73S.
• Most likely diagnosis is acute, mild cervical strain
• Prognosis is good • Spontaneous recovery within 2-‐3 weeks is common.
Case Two: WAD II
• Pa@ent presents with neck complaints including s@ffness or tenderness, and some physical signs of injury, such as point tenderness or trouble turning the head.
• Acute, moderate cervical sprain/strain is most likely DX
• Prognosis is difficult to predict
• Current management does not appear to lessen transi@on from acute to chronic pain status
• Physical and psychological impairment poorly addressed by treatments predic@ve of poor recovery
Case Three: WAD III
• Pa@ent presents with neck complaints including s@ffness or tenderness and neurological signs of injury such as deep tendon reflex or motor deficits.
• Acute, moderate sprain/strain with resultant cervical radiculopathy
• Current management does not appear to lessen transi@on from acute to chronic pain status
• Physical and psychological impairment poorly addressed by treatments predic@ve of poor recovery
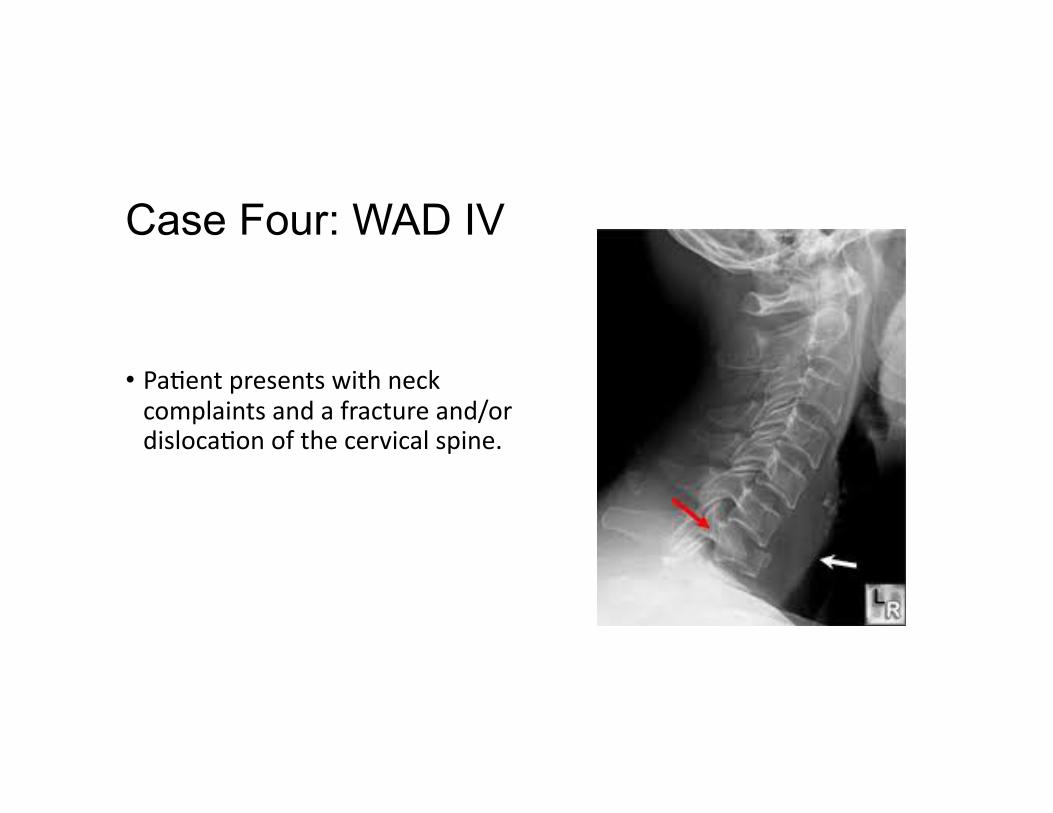
Case Four: WAD IV
• Pa@ent presents with neck complaints and a fracture and/or disloca@on of the cervical spine.
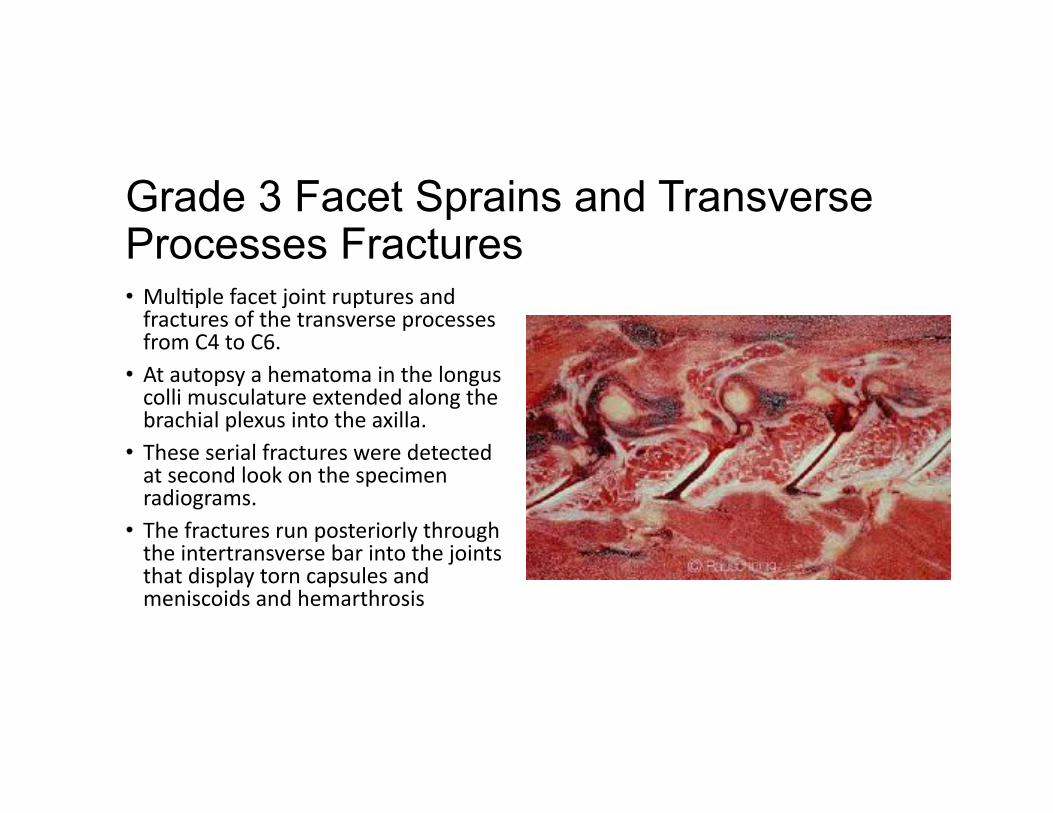
Grade 3 Facet Sprains and Transverse Processes Fractures • Mul@ple facet joint ruptures and fractures of the transverse processes from C4 to C6.
• At autopsy a hematoma in the longus colli musculature extended along the brachial plexus into the axilla.
• These serial fractures were detected at second look on the specimen radiograms.
• The fractures run posteriorly through the intertransverse bar into the joints that display torn capsules and meniscoids and hemarthrosis
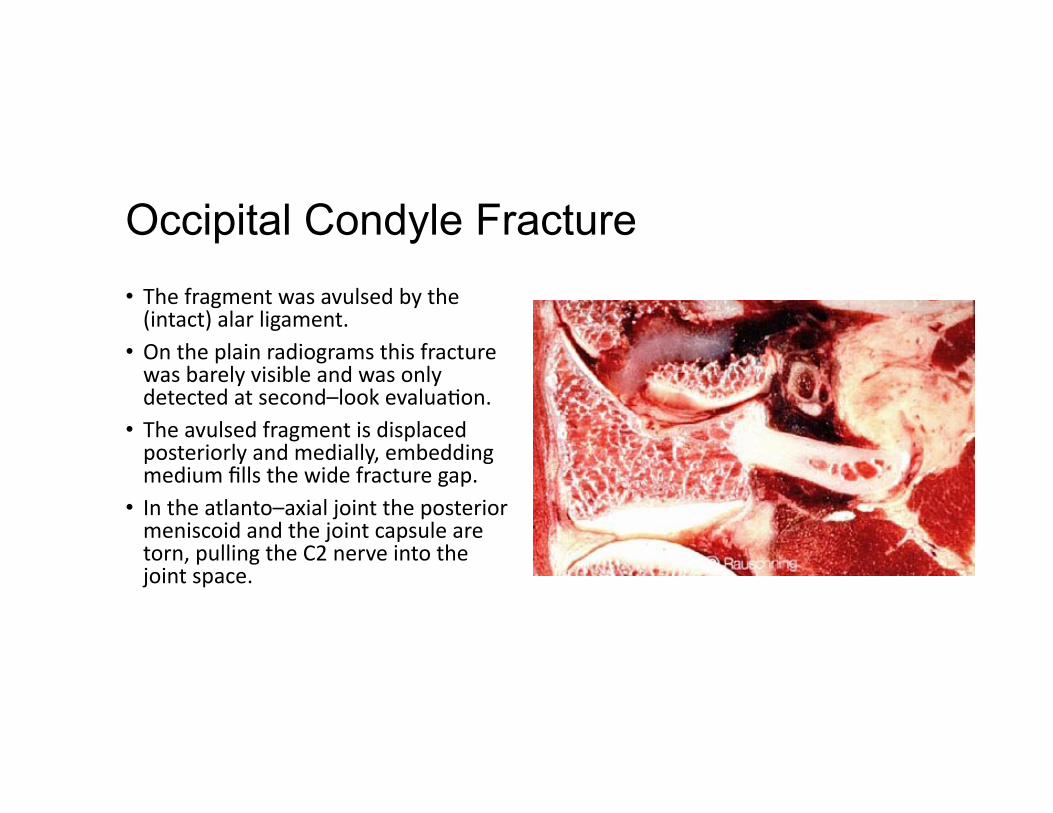
Occipital Condyle Fracture • The fragment was avulsed by the (intact) alar ligament.
• On the plain radiograms this fracture was barely visible and was only detected at second–look evalua@on.
• The avulsed fragment is displaced posteriorly and medially, embedding medium fills the wide fracture gap.
• In the atlanto–axial joint the posterior meniscoid and the joint capsule are torn, pulling the C2 nerve into the joint space.

“Diagnosis is the key to successful treatment!”

Quebec Task Force (QTF) Classifications
• Sponsored by a public insurer in Canada. • QTF submived recommenda@ons regarding classifica@on and treatment of WAD, which was used to develop a guide for managing whiplash in 1995.
• An updated report was published in 2001. • Each of the grades corresponds to a specific treatment recommenda@on.
Quebec Task Force (1995) Criticisms
1. Largely consensus based rather than evidence-‐based
2. Selec@on bias for the literature review
Swedish Study and Quebec Task Force
• Neither the WAD classifica@on nor the QTF follow-‐up regimen could be linked to a bever outcome.
• Jouko Kivioja, Irene Jensen, and Urban Lindgren. Neither the WAD-‐classifica@on nor the Quebec Task Force follow-‐up regimen seems to be important for the outcome ager a whiplash injury. A prospec@ve study on 186 consecu@ve pa@ents. Eur Spine J. 2008 Jul; 17(7): 930–935.
Swedish Study and Quebec Task Force
• The mul@ple-‐follow-‐up regimen is both @me consuming and costly and appears not be jus@fied in a rou@ne clinical sewng.
Swedish Study and Quebec Task Force
• The WAD-‐classifica@on could not predict persistent neck pain ager a whiplash injury in this hospital emergency department based popula@on.
Swedish Study and Quebec Task Force
• Nor was there a sta@s@cally significant difference in the rate of chronic neck pain between the no-‐follow-‐up regimen and the mul@ple-‐follow-‐up regimen proposed by the QTF.
Swedish Study and Quebec Task Force
• At the first visit we recommend a careful history, physical examina@on and informa@on about the nature of the condi@on.
Swedish Study Findings
• In this study cases with neck pain before the accident and a high degree of emo@onal distress from the accident had a tenfold increased risk of developing chronic neck pain.(4)
Transition from Acute to Chronic Pain Status
• Pa@ents that do not resolve within weeks ogen exhibit a myriad of symptoms soon ager the injury event.

“Diagnosis is the key to successful treatment!”

Pathoanatomical Lesions in the Whiplash Injury
1. Cervical Facet joints (Zygapophyseal Joints)
2. Dorsal Root Ganglion (DRG) and Nerve Roots
3. Cervical Ligaments 4. Intervertebral Disc Injuries 5. Muscle Injuries
Facet Joint Injury Model
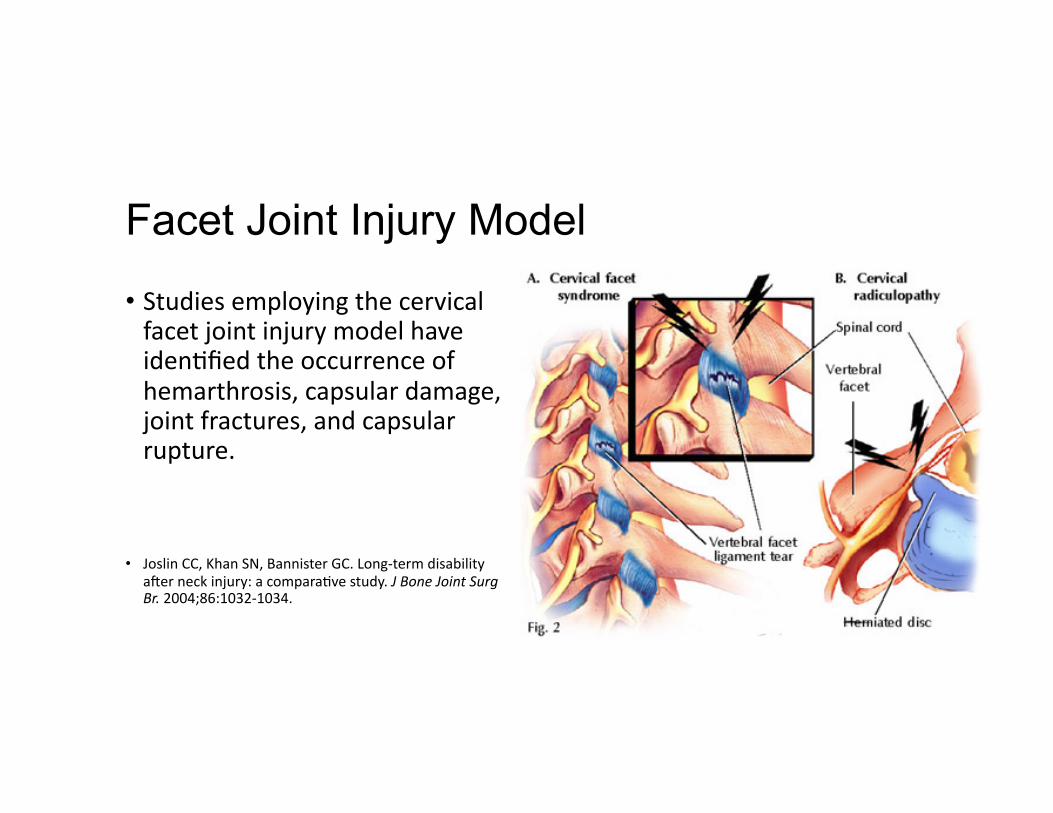
• Studies employing the cervical facet joint injury model have iden@fied the occurrence of hemarthrosis, capsular damage, joint fractures, and capsular rupture.
• Joslin CC, Khan SN, Bannister GC. Long-‐term disability ager neck injury: a compara@ve study. J Bone Joint Surg Br. 2004;86:1032-‐1034.
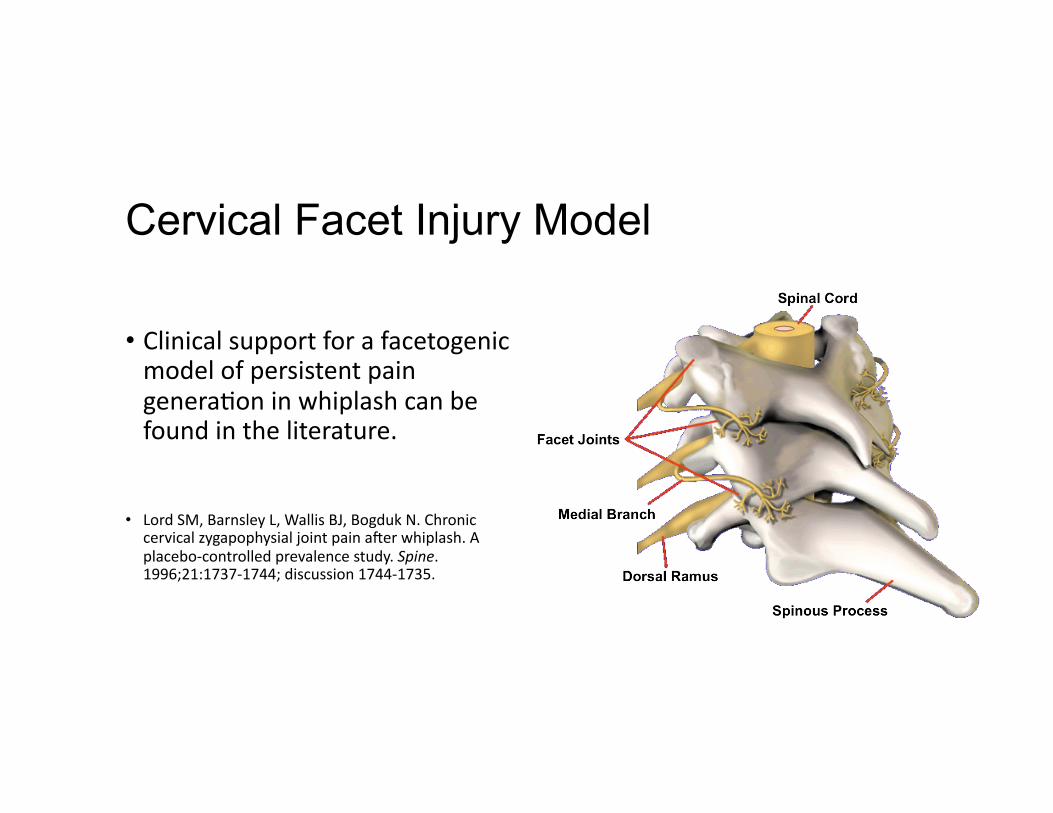
Cervical Facet Injury Model
• Clinical support for a facetogenic model of persistent pain genera@on in whiplash can be found in the literature.
• Lord SM, Barnsley L, Wallis BJ, Bogduk N. Chronic cervical zygapophysial joint pain ager whiplash. A placebo-‐controlled prevalence study. Spine. 1996;21:1737-‐1744; discussion 1744-‐1735.
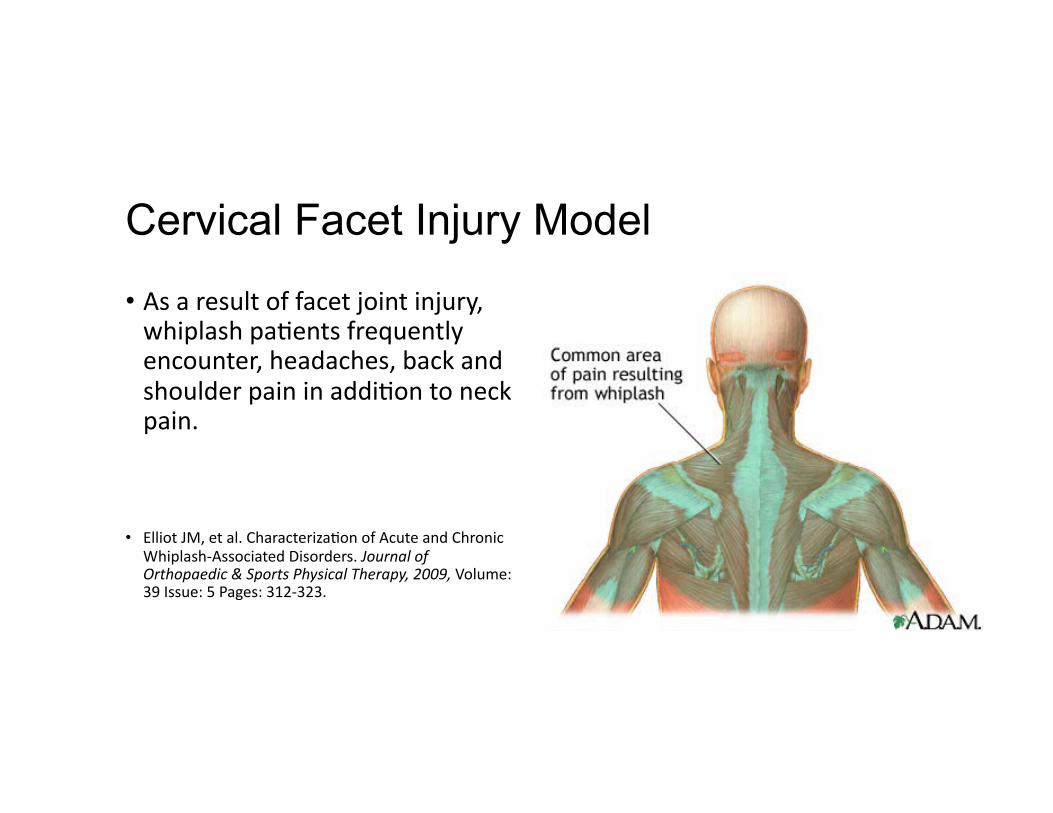
Cervical Facet Injury Model
• As a result of facet joint injury, whiplash pa@ents frequently encounter, headaches, back and shoulder pain in addi@on to neck pain.
• Elliot JM, et al. Characteriza@on of Acute and Chronic Whiplash-‐Associated Disorders. Journal of Orthopaedic & Sports Physical Therapy, 2009, Volume: 39 Issue: 5 Pages: 312-‐323.
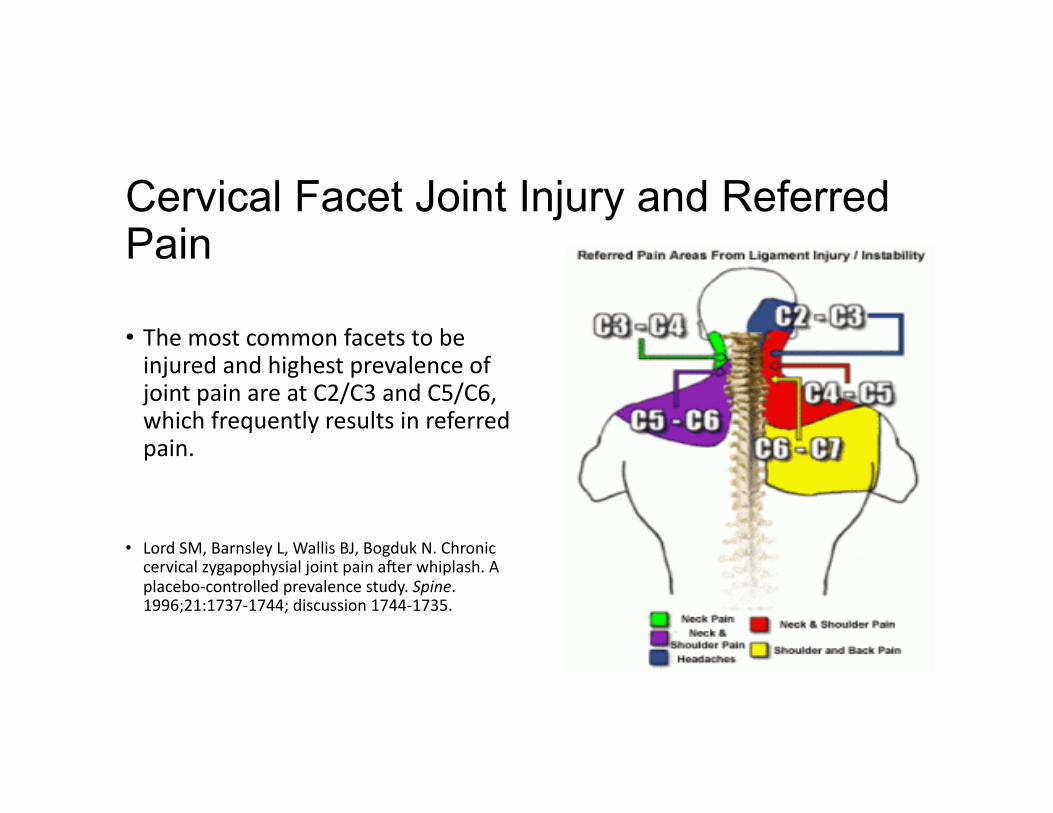
Cervical Facet Joint Injury and Referred Pain
• The most common facets to be injured and highest prevalence of joint pain are at C2/C3 and C5/C6, which frequently results in referred pain.
• Lord SM, Barnsley L, Wallis BJ, Bogduk N. Chronic cervical zygapophysial joint pain ager whiplash. A placebo-‐controlled prevalence study. Spine. 1996;21:1737-‐1744; discussion 1744-‐1735.
Dorsal Root Ganglion and Nerve Roots
• Vulnerable to excessive stretching and injury during rapid accelera@on/decelera@on (“S-‐shaped” curve) or lateral bending of the neck as demonstrated in rear-‐end or side-‐vector impact whiplash.
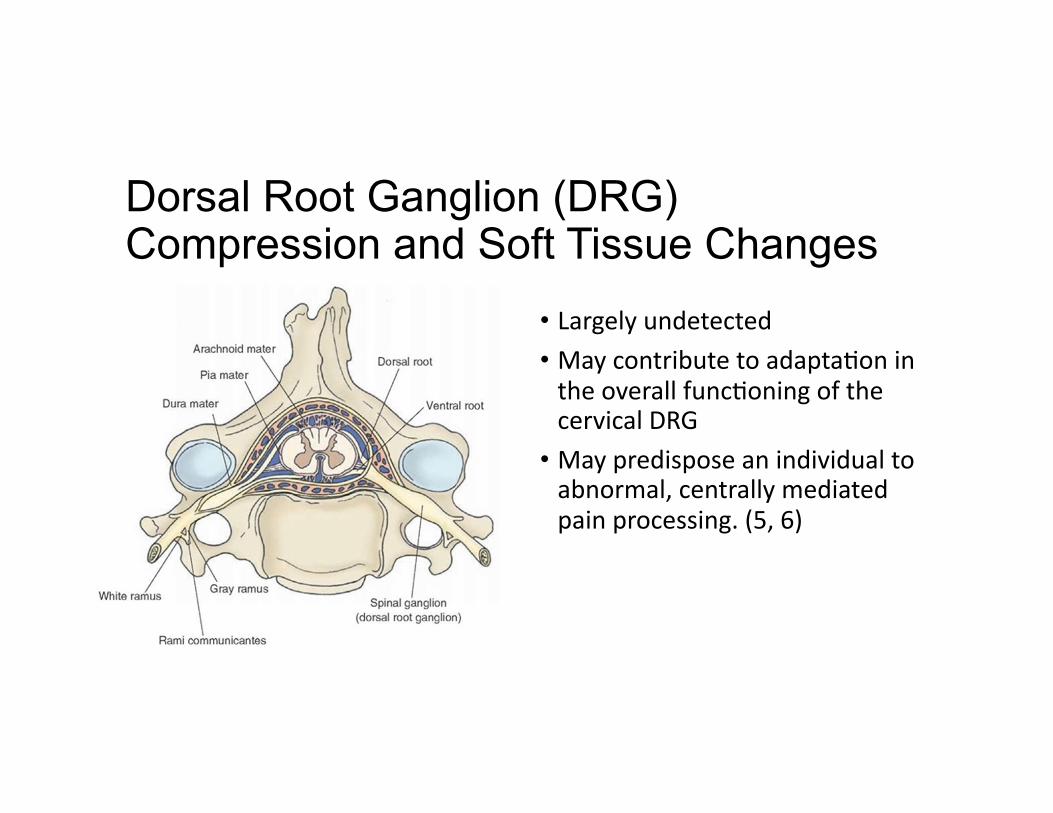
Dorsal Root Ganglion (DRG) Compression and Soft Tissue Changes
• Largely undetected • May contribute to adapta@on in the overall func@oning of the cervical DRG
• May predispose an individual to abnormal, centrally mediated pain processing. (5, 6)
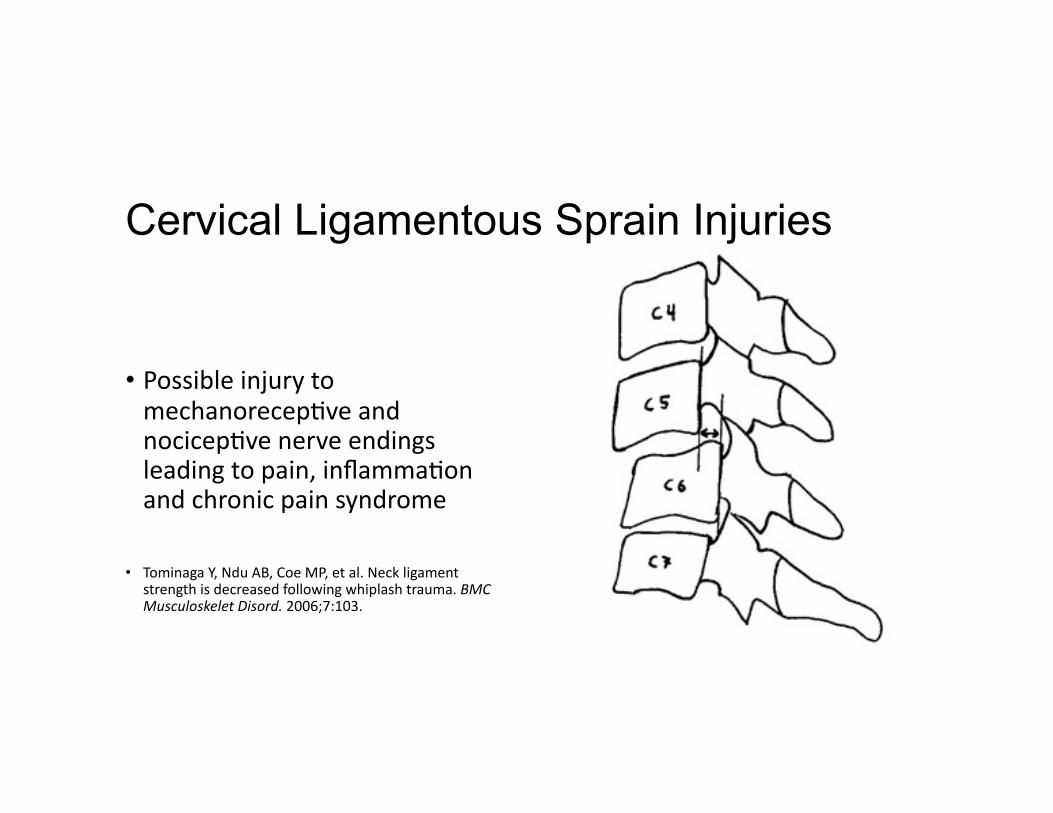
Cervical Ligamentous Sprain Injuries
• Possible injury to mechanorecep@ve and nocicep@ve nerve endings leading to pain, inflamma@on and chronic pain syndrome
• Tominaga Y, Ndu AB, Coe MP, et al. Neck ligament strength is decreased following whiplash trauma. BMC Musculoskelet Disord. 2006;7:103.
Persistent Pain: A Chronic Illness
• Acute pain usually goes away ager an injury or illness resolves. But when pain persists for months or even years, long ager whatever started the pain has gone or because the injury con@nues, it becomes a chronic condi@on and illness in its own right.
• A Call to Revolu@onize Chronic Pain Care in America: An Opportunity in Health Care Reform. The Mayday Fund. November 4, 2009. Amended March 4, 2010.
National Pain Strategy
• Chronic pain -‐ Pain that occurs on at least half the days for six months or more.
James J. Lehman, DC, MBA, DABCO
Upper Cervical Ligament Sprain Injuries and the Presence of Rust’s Sign
• History of roll-‐over MVA or blow to head
• Suspect upper cervical spine instability
• Order immediate CT Scan to check for non-‐displaced cervical spine fracture

“Diagnosis is the key to successful treatment!”

Upper Cervical Ligament Sprain Injuries Leading Chronic Pain
• Severity of alar ligament injury, head posi@on at @me of impact, Neck Disability Index (NDI) scores and reproduc@on of pain and excessive mobility with manual examina@on. (7, 8)
• Sharp Purser Maneuver test for upper cervical spine instability.
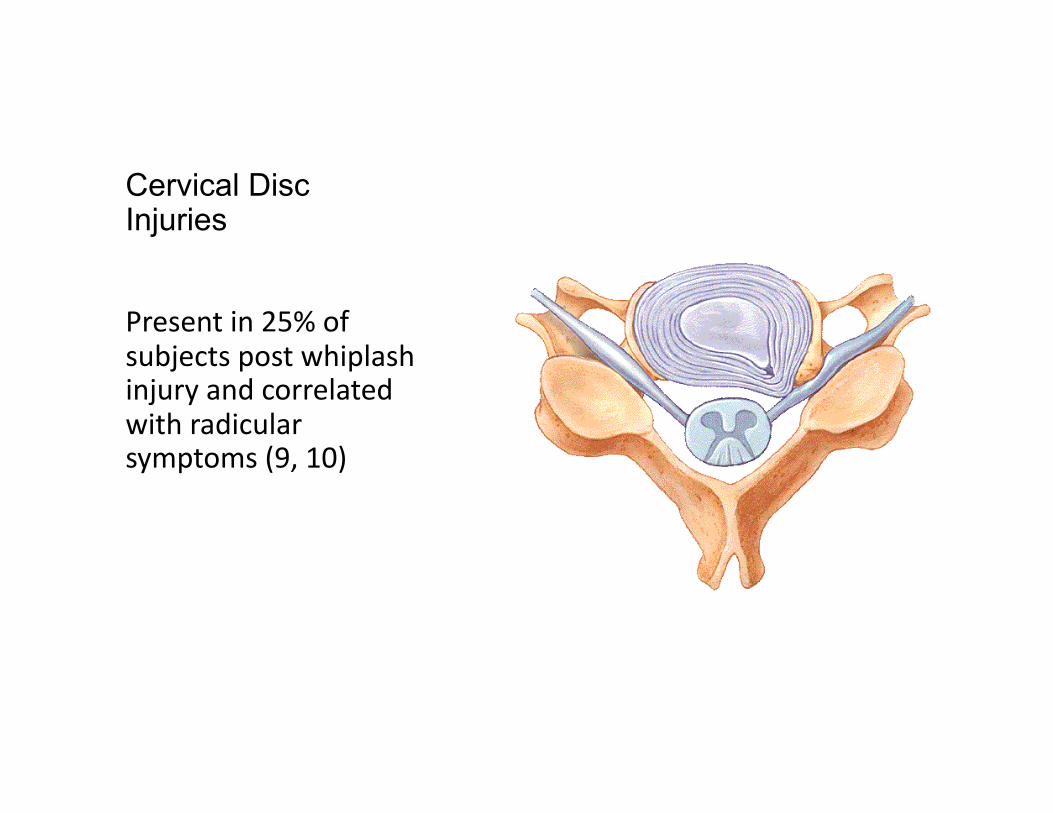
Cervical Disc Injuries
Present in 25% of subjects post whiplash injury and correlated with radicular symptoms (9, 10)
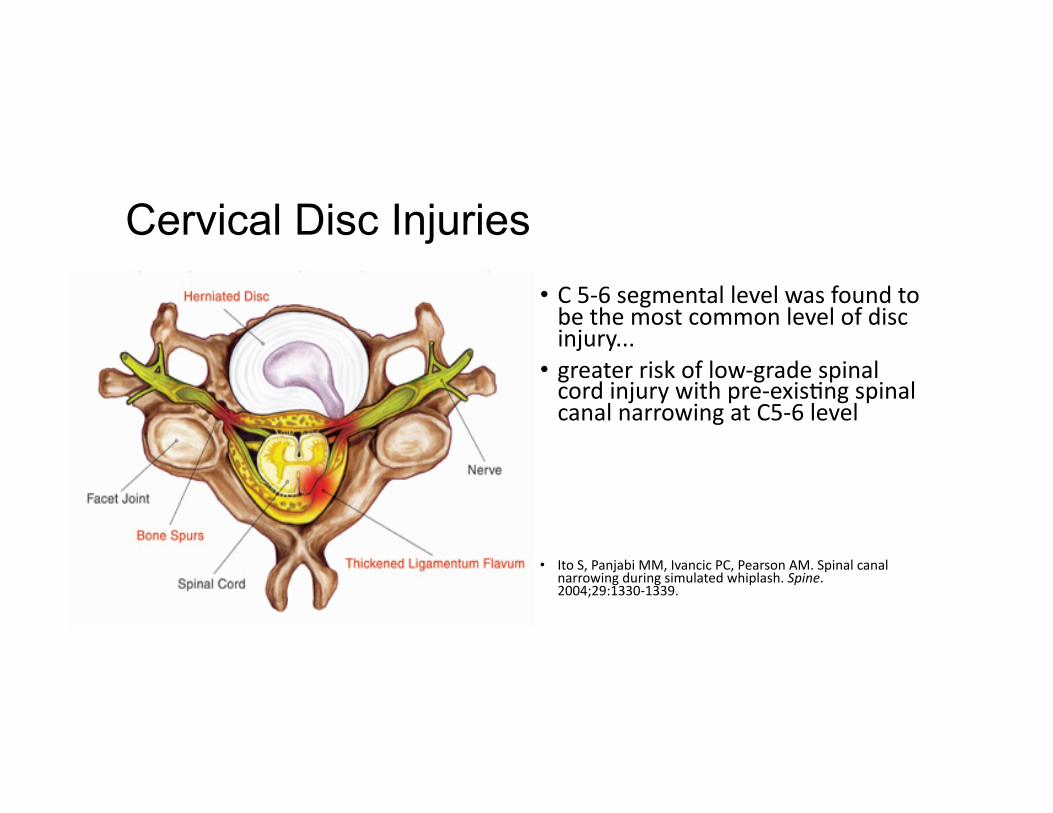
Cervical Disc Injuries • C 5-‐6 segmental level was found to be the most common level of disc injury...
• greater risk of low-‐grade spinal cord injury with pre-‐exis@ng spinal canal narrowing at C5-‐6 level
• Ito S, Panjabi MM, Ivancic PC, Pearson AM. Spinal canal narrowing during simulated whiplash. Spine. 2004;29:1330-‐1339.
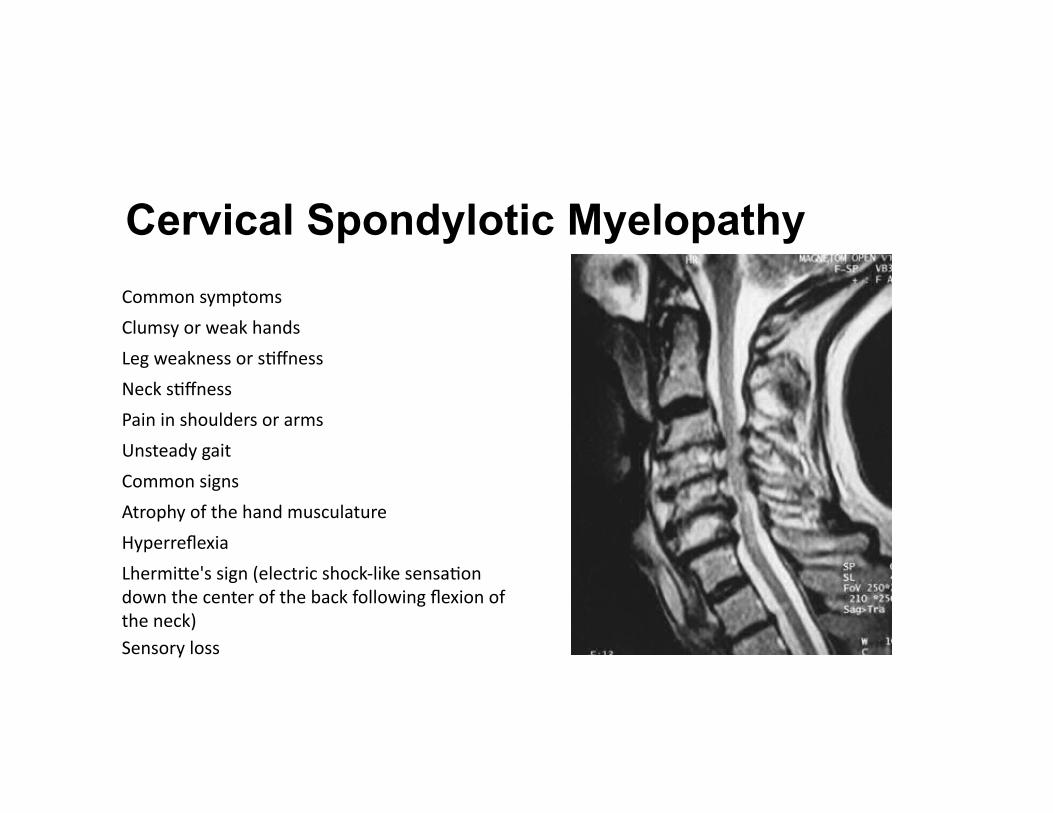
Cervical Spondylotic Myelopathy Common symptoms
Clumsy or weak hands
Leg weakness or s@ffness
Neck s@ffness
Pain in shoulders or arms
Unsteady gait
Common signs
Atrophy of the hand musculature
Hyperreflexia
Lhermive's sign (electric shock-‐like sensa@on down the center of the back following flexion of the neck) Sensory loss
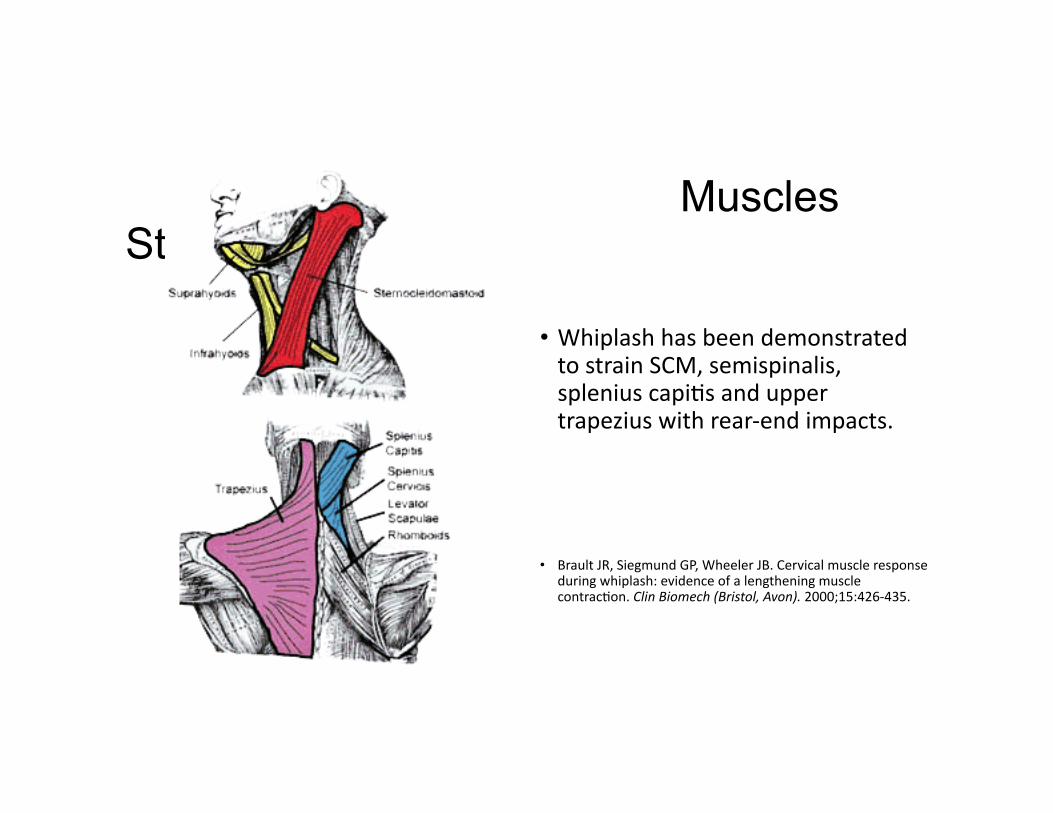
Muscles Strained
• Whiplash has been demonstrated to strain SCM, semispinalis, splenius capi@s and upper trapezius with rear-‐end impacts.
• Brault JR, Siegmund GP, Wheeler JB. Cervical muscle response during whiplash: evidence of a lengthening muscle contrac@on. Clin Biomech (Bristol, Avon). 2000;15:426-‐435.
Physical and Psychological Features Leading to Chronic Pain Syndrome
• Poor outcomes at 2-‐3 years post injury
• High pain and disability levels with physical and psychological factors
• Early presence of cervical movement loss, cold temperature hyperalgesia, and posvrauma@c stress symptoms
• Sterling M, Jull G, Kenardy J. Physical and psychological factors maintain long-‐term predic@ve capacity post-‐whiplash injury. Pain. 2006;122:102-‐108.

“Diagnosis is the key to successful treatment!”
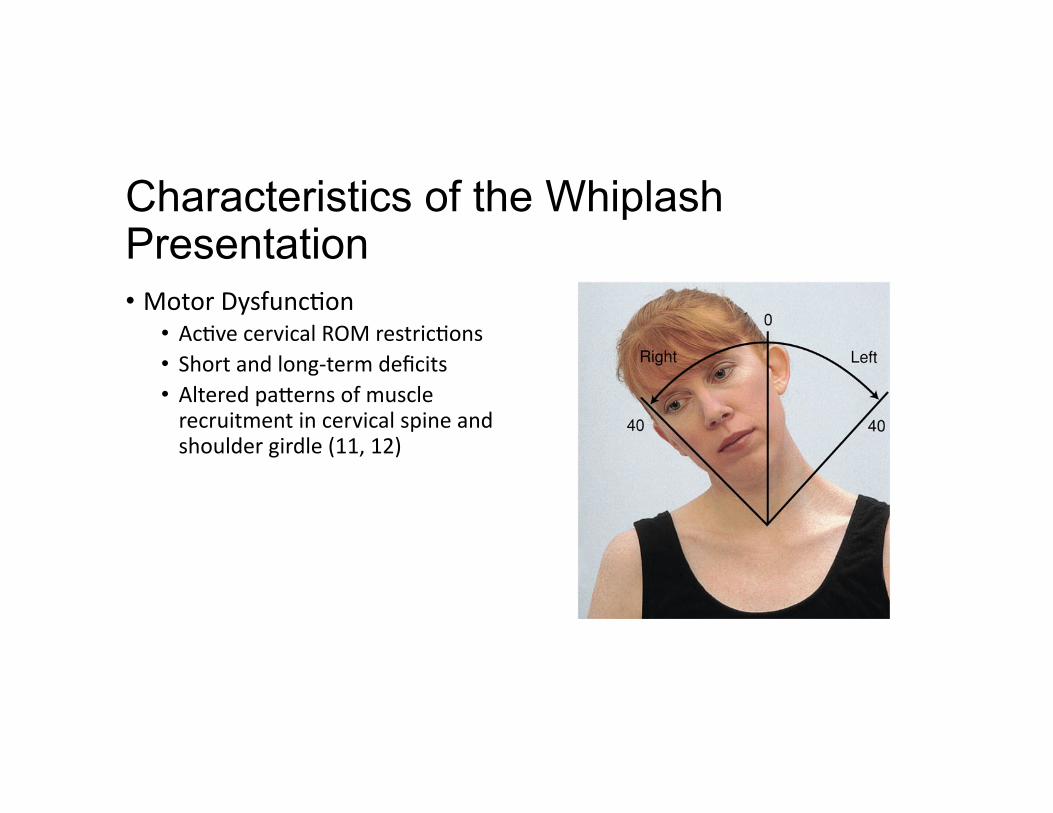
Characteristics of the Whiplash Presentation • Motor Dysfunc@on
• Ac@ve cervical ROM restric@ons • Short and long-‐term deficits • Altered paverns of muscle recruitment in cervical spine and shoulder girdle (11, 12)
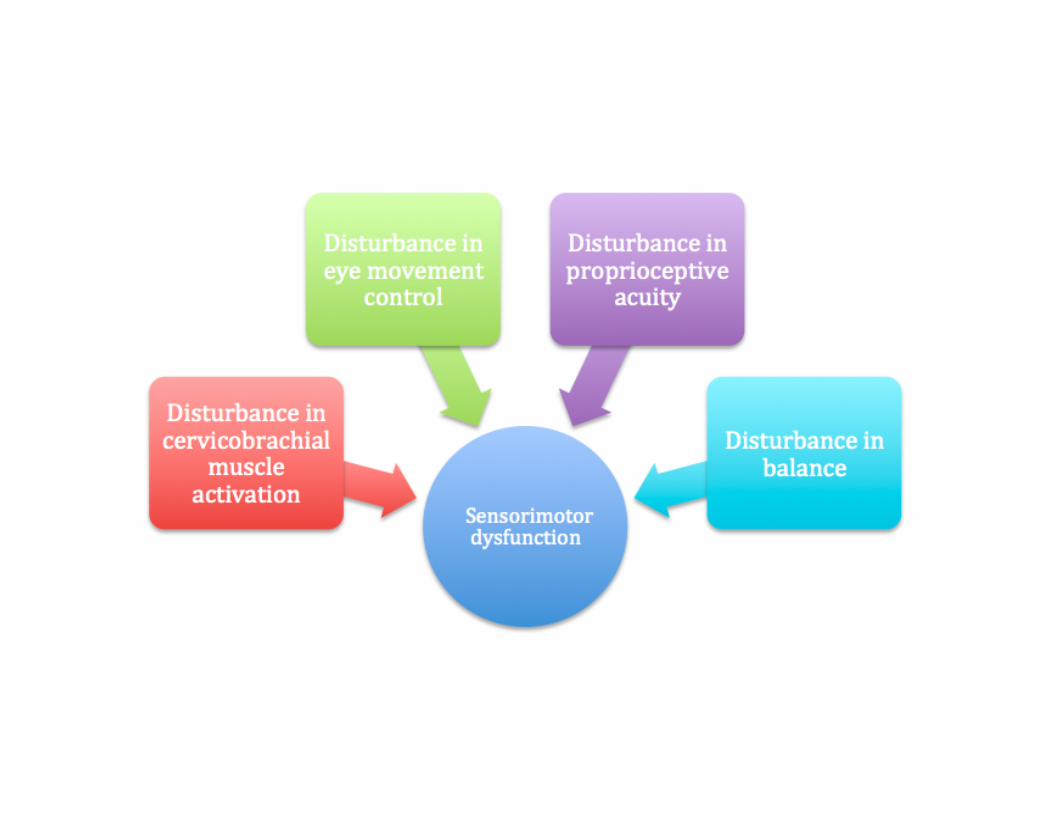
Characteristics of the Whiplash Presentation
• Sensorimotor Dysfunc@on • Acute and chronic WAD • Greater joint reposi@oning errors with chronic WAD and acute with more severe pain and disability
• Loss of balance and disturbed neck-‐influenced eye movements with chronic WAD
• Elliov JM, et al. Characteriza@ons of Acute and Chronic Whiplash-‐Associated Disorders. JOSPT, May 2009; Vol 39:5:312-‐323.
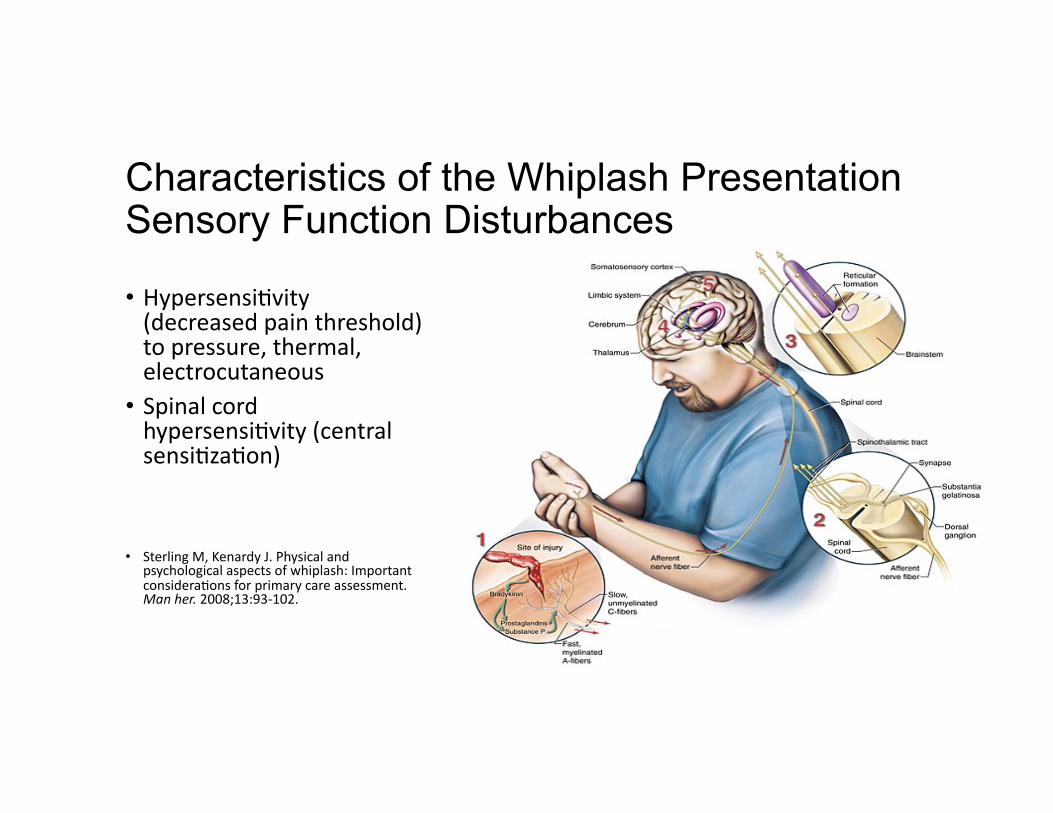
Characteristics of the Whiplash Presentation Sensory Function Disturbances
• Hypersensi@vity (decreased pain threshold) to pressure, thermal, electrocutaneous
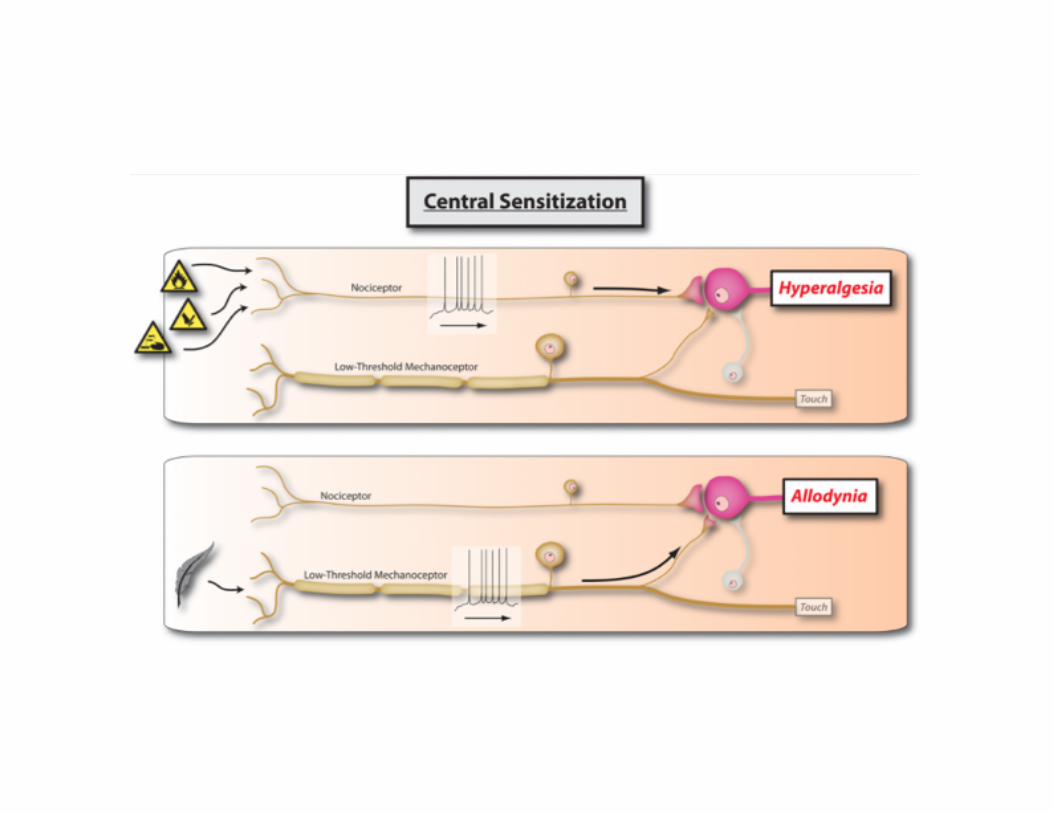
• Spinal cord hypersensi@vity (central sensi@za@on)
• Sterling M, Kenardy J. Physical and psychological aspects of whiplash: Important considera@ons for primary care assessment. Man her. 2008;13:93-‐102.
Psychological Factors and Chronic WAD or Chronic Pain Syndrome-Post-Traumatic
• Affec@ve disorders • Anxiety • Depression • Behavioral abnormali@es (fear of movement)
• Posvrauma@c stress
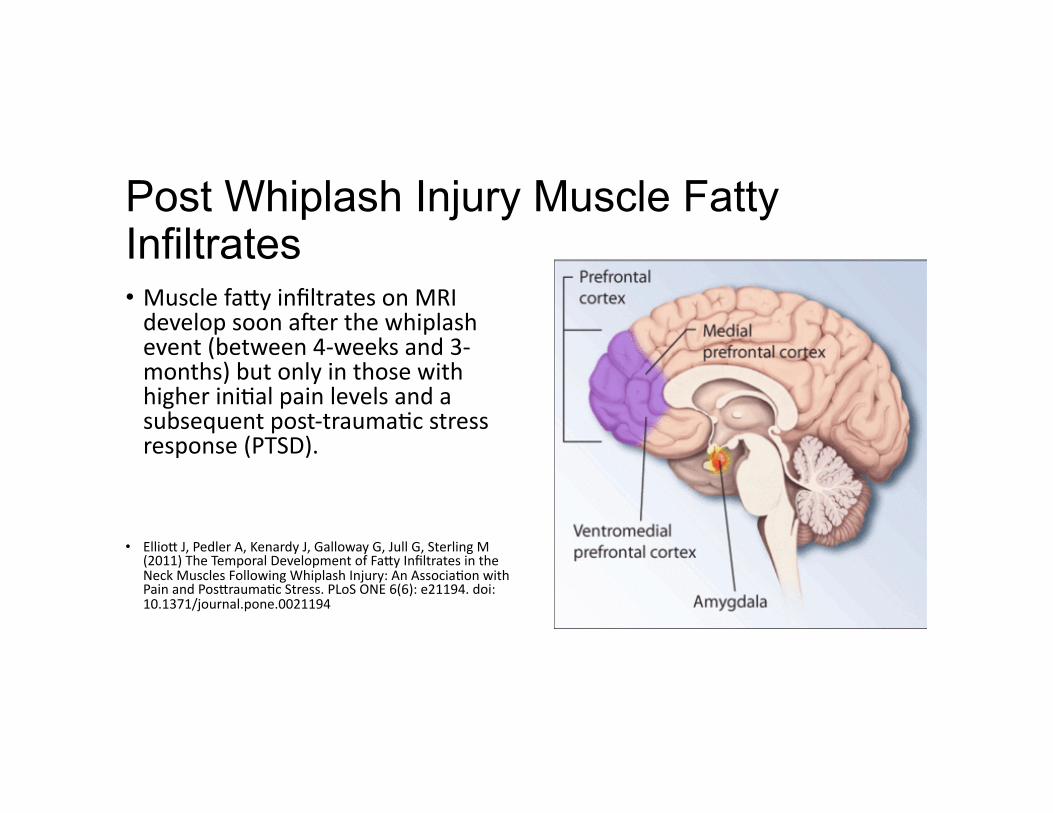
Post Whiplash Injury Muscle Fatty Infiltrates • Muscle favy infiltrates on MRI develop soon ager the whiplash event (between 4-‐weeks and 3-‐months) but only in those with higher ini@al pain levels and a subsequent post-‐trauma@c stress response (PTSD).
• Elliov J, Pedler A, Kenardy J, Galloway G, Jull G, Sterling M (2011) The Temporal Development of Favy Infiltrates in the Neck Muscles Following Whiplash Injury: An Associa@on with Pain and Posvrauma@c Stress. PLoS ONE 6(6): e21194. doi:10.1371/journal.pone.0021194

Degeneration of the Cervical Extensor Musculature in Chronic WAD
Content not quan@ty is a bever measure of muscle degenera@on in whiplash.
Elliov JM, et al. Manual Therapy (2013)
Whiplash Presentation
• “Whiplash is a markedly heterogeneous and complex condi@on with varied disturbances in motor, sensorimotor and sensory func@on as well as psychological distress.”
Clinical Implications and Prognosis of Chronic Pain • Kinesthe@c deficits (joint posi@on error)
• Cervical muscle recruitment paverns
• Altered ac@vity in upper trapezius muscle
• Poor control of balance • Impaired eye movement (13-‐17)
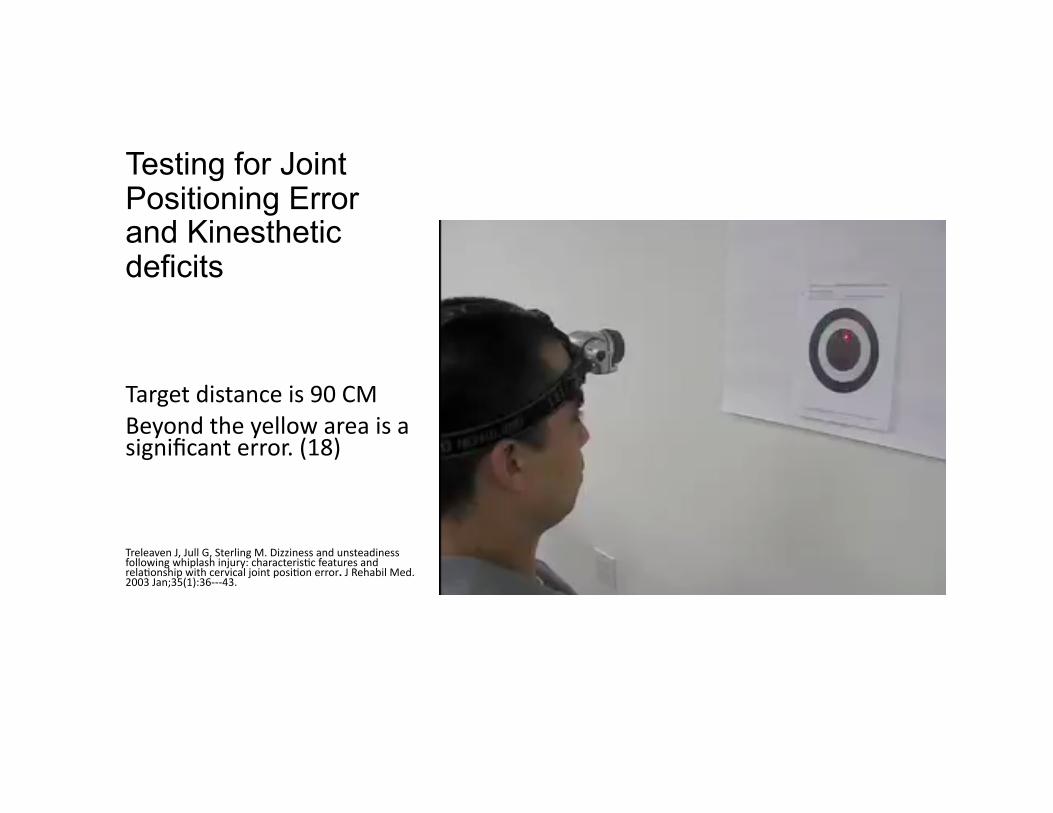
Testing for Joint Positioning Error and Kinesthetic deficits
Target distance is 90 CM Beyond the yellow area is a significant error. (18)
Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness following whiplash injury: characteris@c features and rela@onship with cervical joint posi@on error. J Rehabil Med. 2003 Jan;35(1):36-‐-‐-‐43.
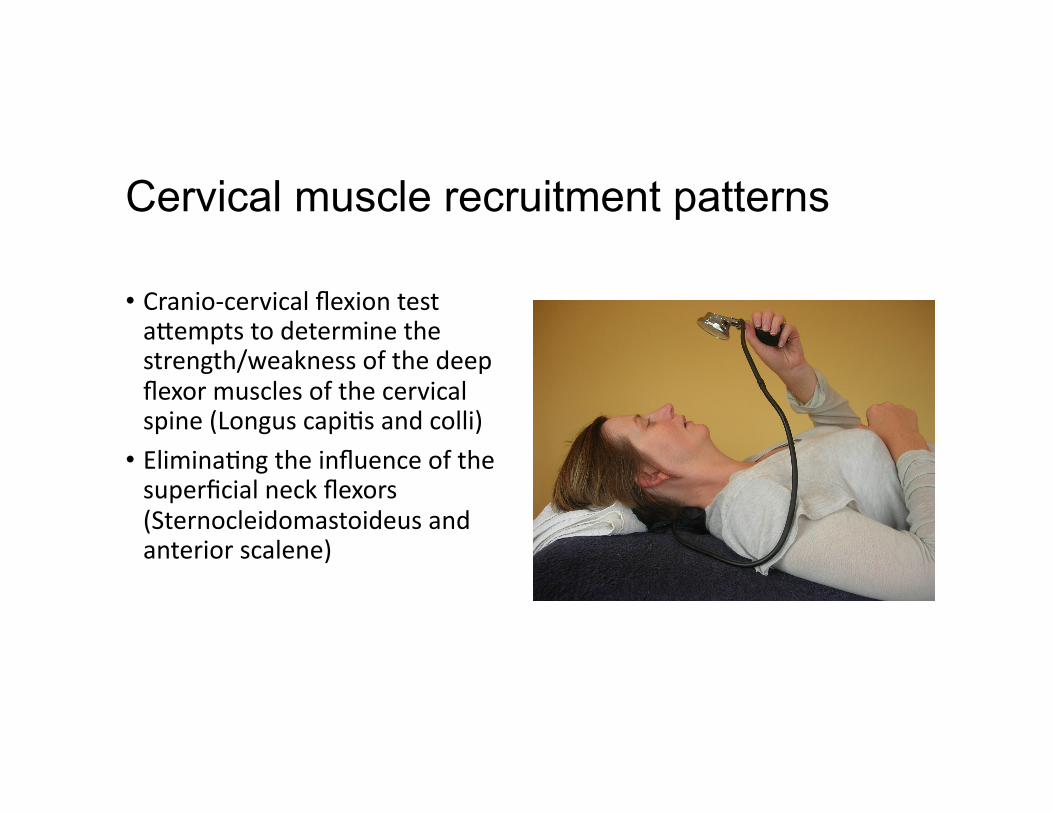
Cervical muscle recruitment patterns
• Cranio-‐cervical flexion test avempts to determine the strength/weakness of the deep flexor muscles of the cervical spine (Longus capi@s and colli)
• Elimina@ng the influence of the superficial neck flexors (Sternocleidomastoideus and anterior scalene)

Oculomotor Control
The assessment of smooth pursuit and gaze stability is an important part of the assessment of sensorimotor impairment following whiplash injury.
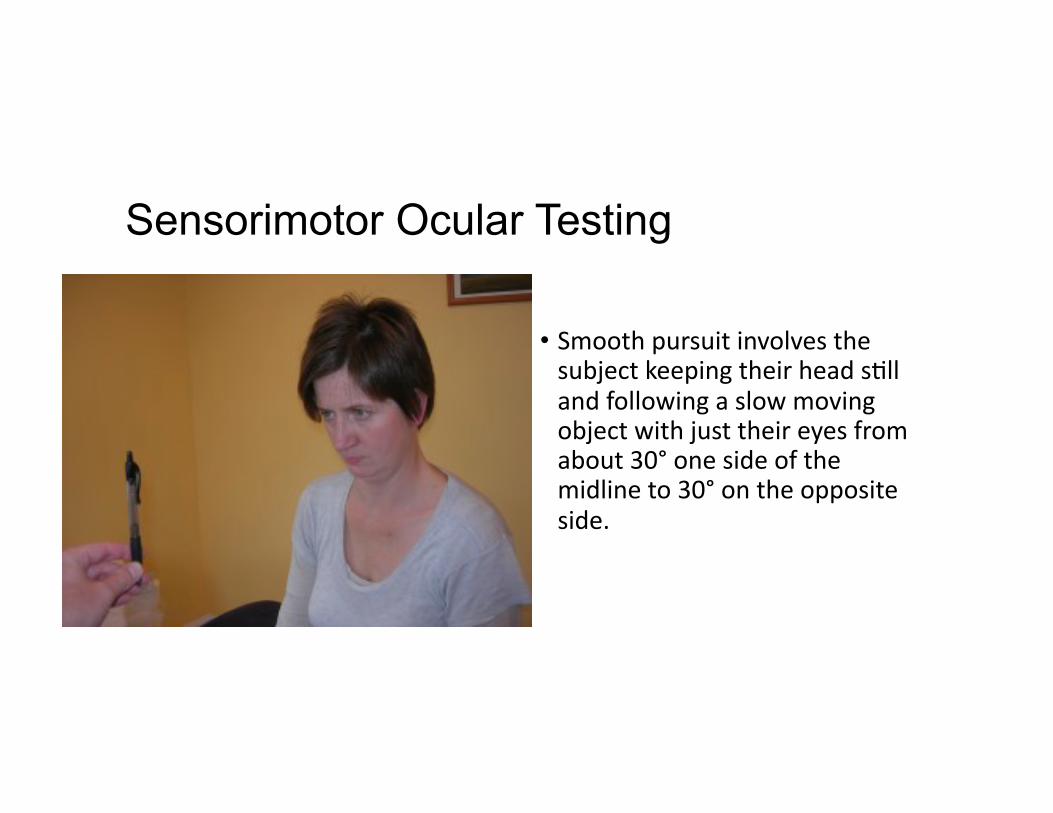
Sensorimotor Ocular Testing
• Smooth pursuit involves the subject keeping their head s@ll and following a slow moving object with just their eyes from about 30° one side of the midline to 30° on the opposite side.
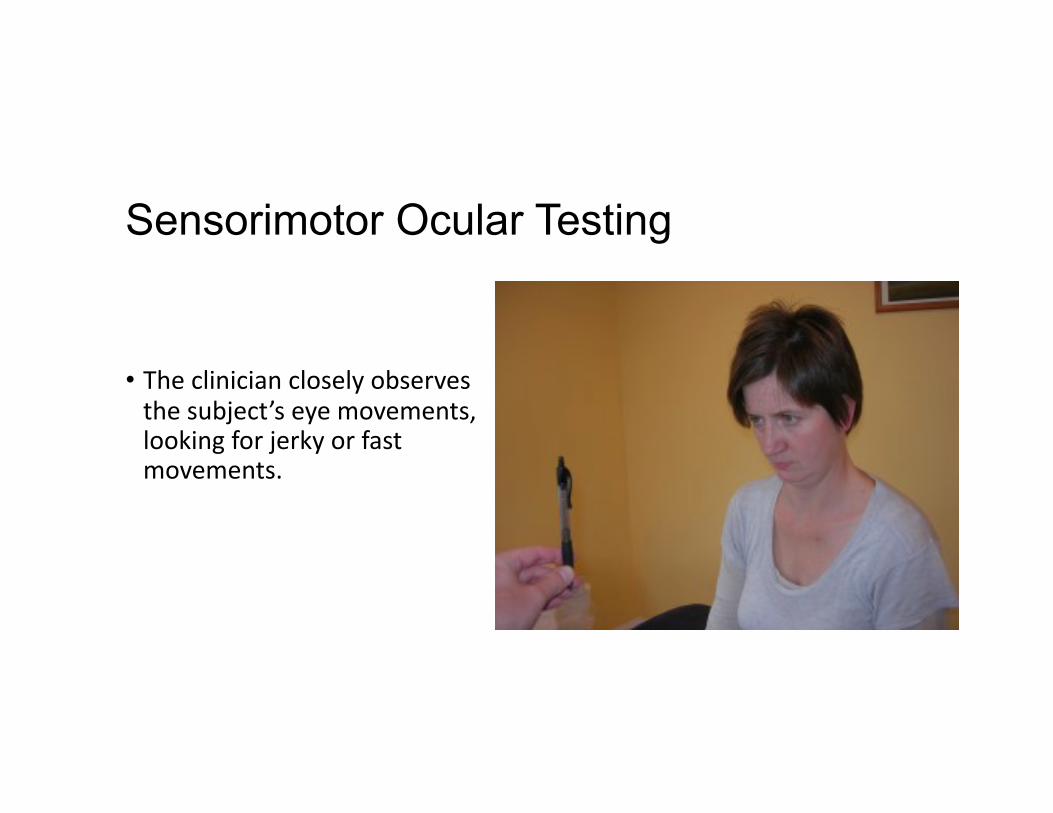
Sensorimotor Ocular Testing
• The clinician closely observes the subject’s eye movements, looking for jerky or fast movements.
Sensorimotor Ocular Testing
• Reproduc@on of dizziness or pain, increased effort or difficulty performing the test, all suggest sensorimotor impairment.
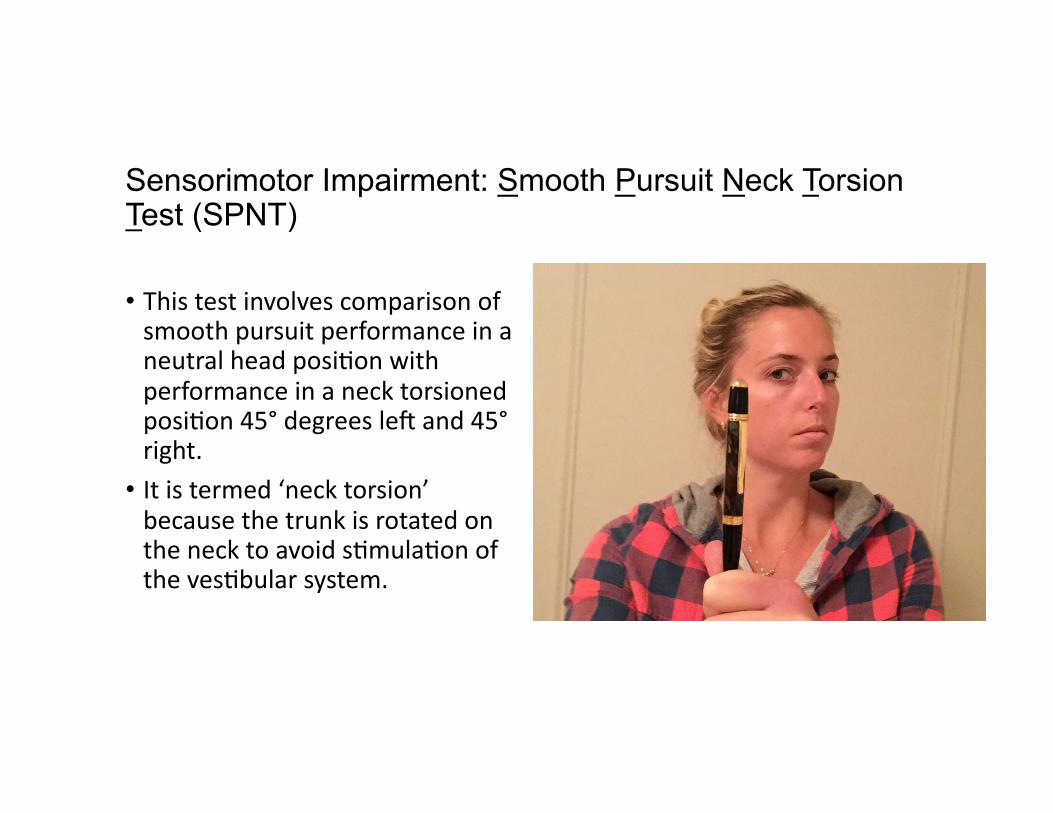
Sensorimotor Impairment: Smooth Pursuit Neck Torsion Test (SPNT)
• This test involves comparison of smooth pursuit performance in a neutral head posi@on with performance in a neck torsioned posi@on 45° degrees leg and 45° right.
• It is termed ‘neck torsion’ because the trunk is rotated on the neck to avoid s@mula@on of the ves@bular system.
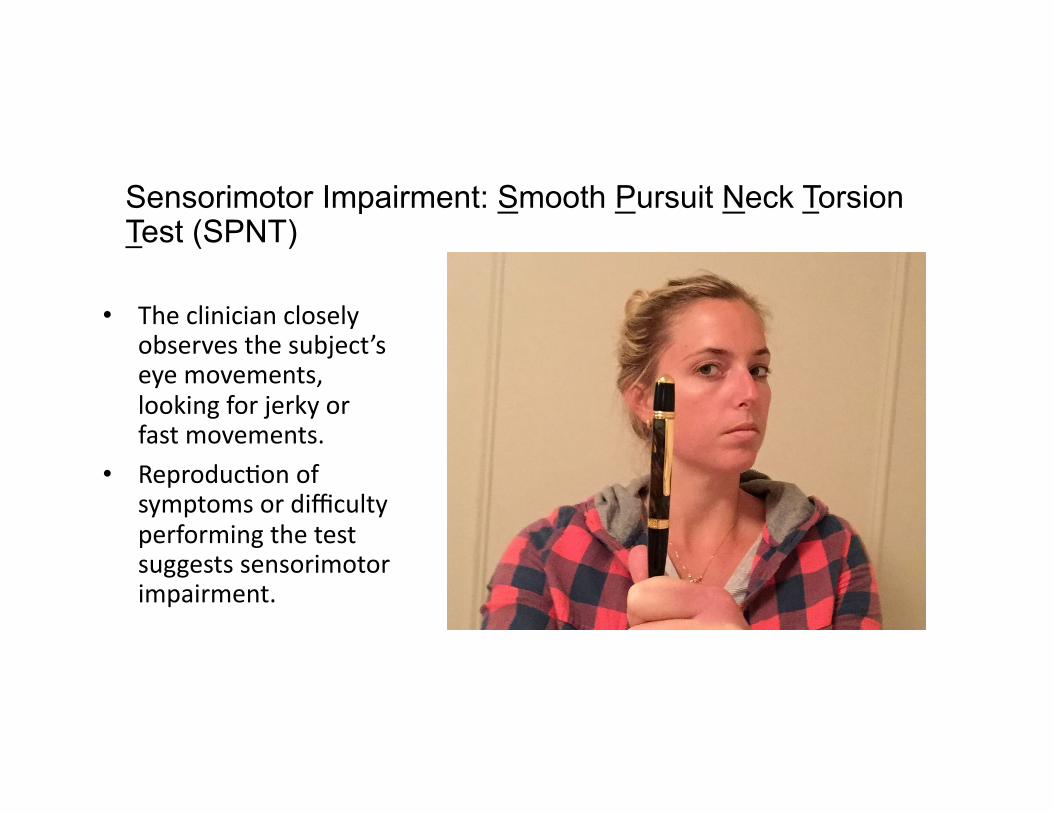
Sensorimotor Impairment: Smooth Pursuit Neck Torsion Test (SPNT)
• The clinician closely observes the subject’s eye movements, looking for jerky or fast movements.
• Reproduc@on of symptoms or difficulty performing the test suggests sensorimotor impairment.
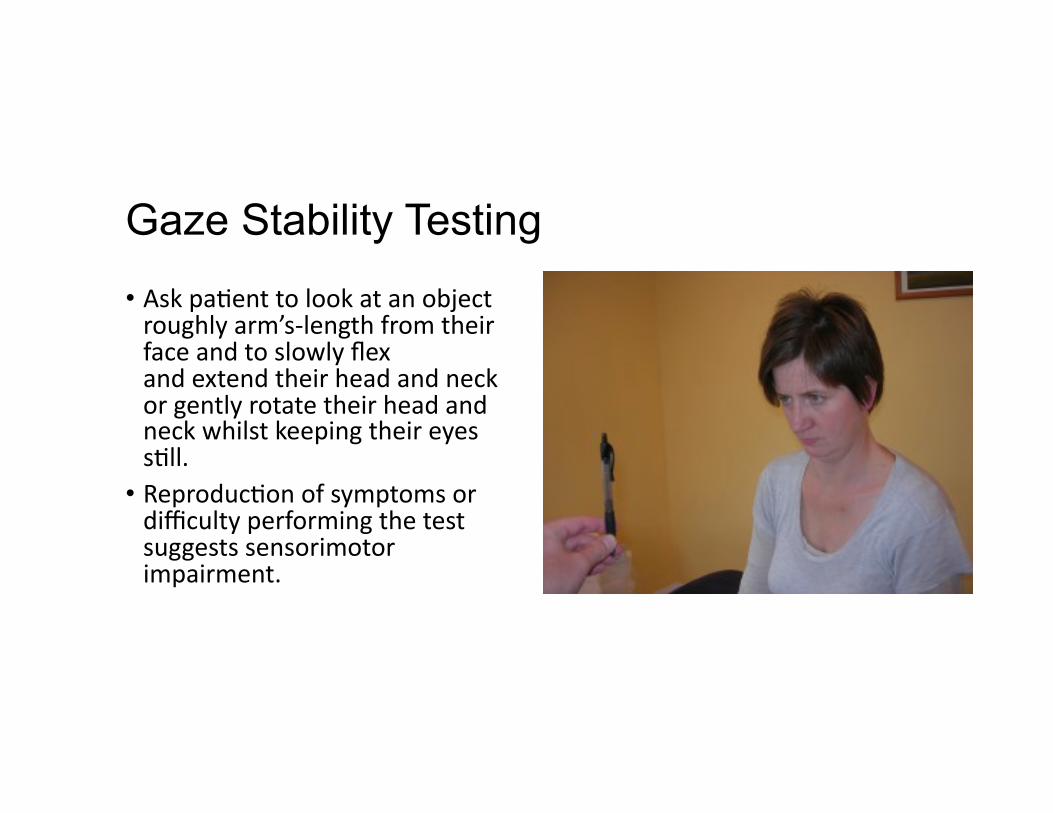
Gaze Stability Testing
• Ask pa@ent to look at an object roughly arm’s-‐length from their face and to slowly flex and extend their head and neck or gently rotate their head and neck whilst keeping their eyes s@ll.
• Reproduc@on of symptoms or difficulty performing the test suggests sensorimotor impairment.
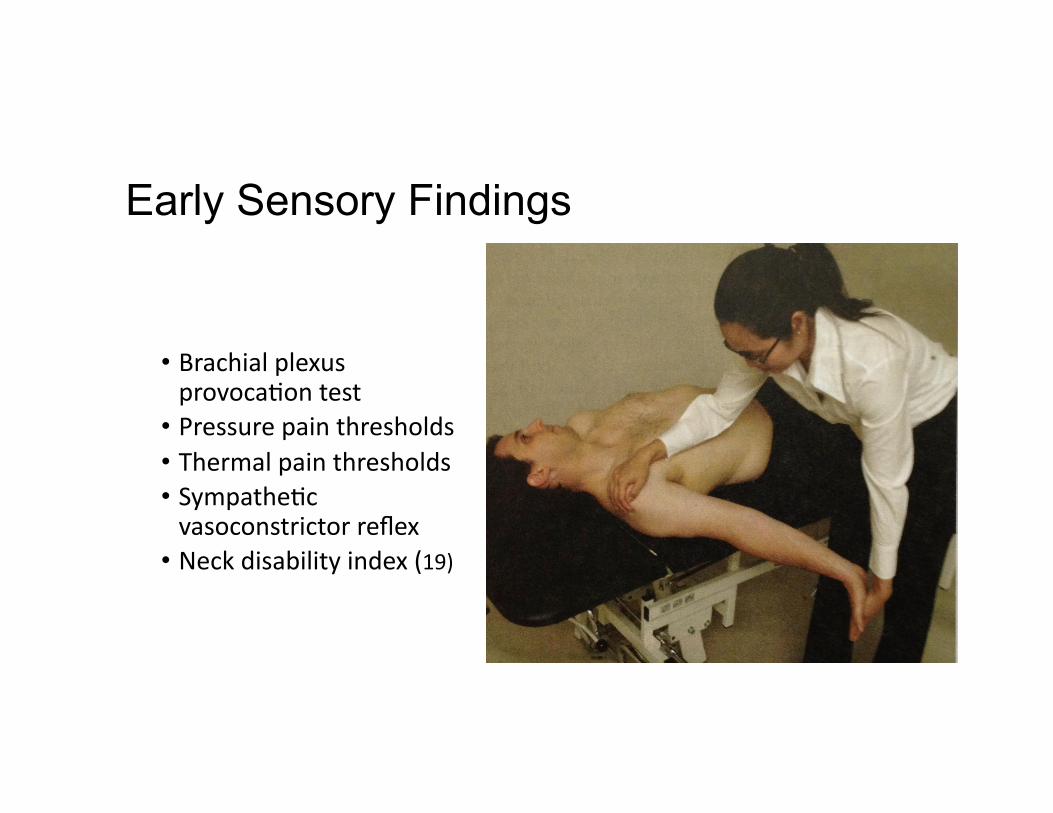
Early Sensory Findings
• Brachial plexus provoca@on test
• Pressure pain thresholds • Thermal pain thresholds • Sympathe@c vasoconstrictor reflex
• Neck disability index (19)
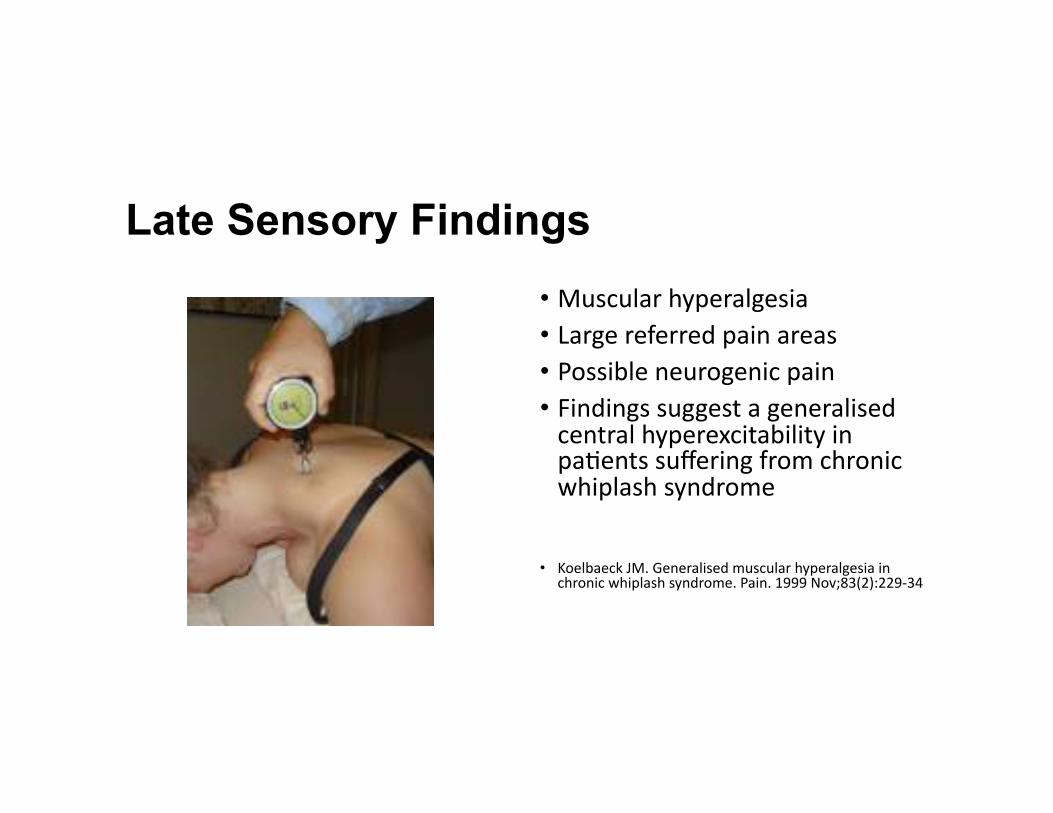
Late Sensory Findings
• Muscular hyperalgesia • Large referred pain areas • Possible neurogenic pain • Findings suggest a generalised central hyperexcitability in pa@ents suffering from chronic whiplash syndrome
• Koelbaeck JM. Generalised muscular hyperalgesia in chronic whiplash syndrome. Pain. 1999 Nov;83(2):229-‐34
Algometry with Clothes Peg
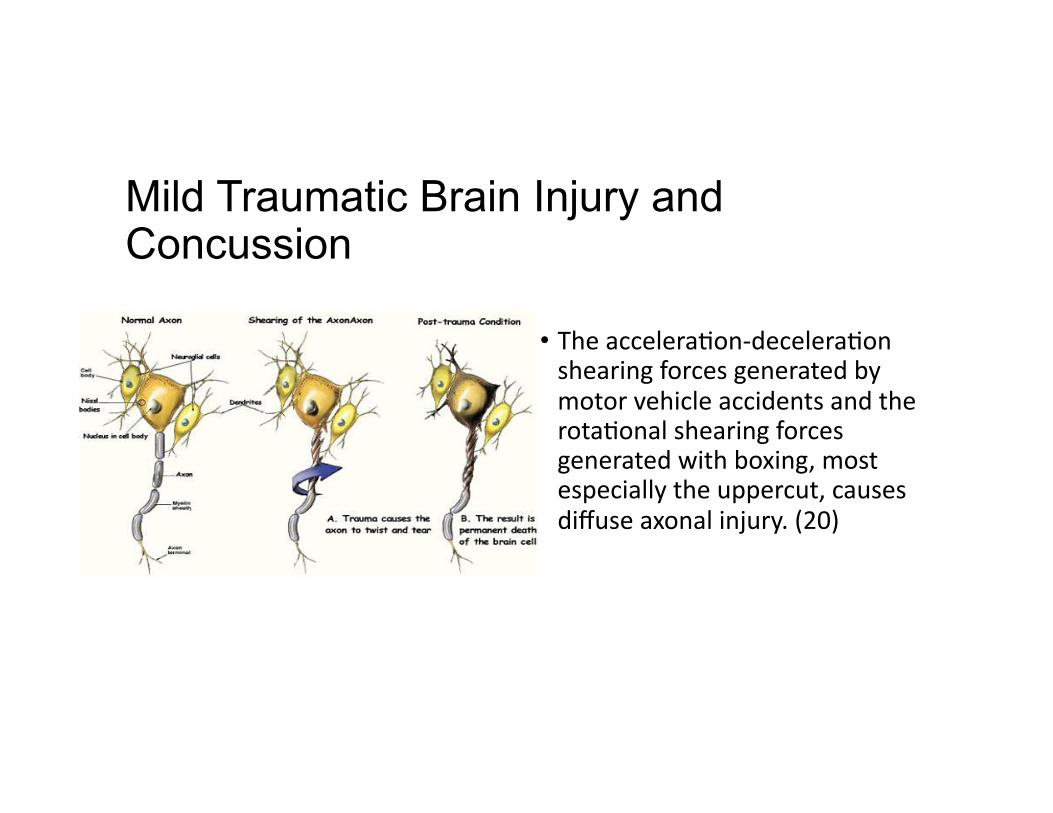
Mild Traumatic Brain Injury and Concussion
• The accelera@on-‐decelera@on shearing forces generated by motor vehicle accidents and the rota@onal shearing forces generated with boxing, most especially the uppercut, causes diffuse axonal injury. (20)
Conclusions: The evaluation and management of whiplash injuries must attempt to: • Discover mechanism of injury • Reveal pain severity • Determine the injured @ssues and pain generators
• Understand biopsychosocial factors • Perform a differen@al diagnosis • Provide a reasonable prognosis (acute and chronic) • Offer appropriate treatment
• Integrate a health care team of providers
First Evaluate Patient and Make a Diagnosis/Prognosis Before Treating Patient
Evidence-based, patient-centered and ethical report of findings with whiplash
injuries • Report the diagnoses, suggest appropriate treatment, gain permission to treat (informed consent), and discuss the prognosis
• Avempt to reduce disability and chronic pain with use of placebo effect
• Report impairment with medical legal cases but avoid nocebo effect

“Diagnosis is the key to successful treatment!”
Case • 56 y/o male professor presents with the following HPI
• Acute, exacerba@ons of neck pain and unilateral upper extremity paresthesia in the C6 dermatome.
• Past history of side impact motor vehicle collision (MVC) with whiplash injury some 20 years earlier. Resulted in fractured teeth, spinal and hand strain/sprain injuries, confusion and short-‐term memory loss.
• MRI demonstrated cervical discopathy at C5-‐6-‐7 two years following the motor vehicle collision
• Discon@nued racquetball due to pain and weakness in RUE • He has experienced daily neck pain and s@ffness since the MVC with episodic neck/arm pain with paresthesias.
Engaged Learning Task (30 minutes)
• Form groups of 6 doctors each
• Complete discussion in 10 minutes
• Select a spokesperson who will provide a brief presenta@on
Active learning tasks
Please state the following for this 56 year-‐old pa@ent:
• Differen@al diagnosis • Working diagnosis • Prognosis

“Diagnosis is the key to successful treatment!”

References 1. Barnsley L, Lord S, Bogduk N. Whiplash injury. Pain. 1994;58:283–307.
2. Spitzer WO, Skovron ML, Salmi LR, et al. Scien@fic monograph of the Quebec Task Force on Whiplash-‐Associated Disorders: redefining “whiplash” and its management. Spine. 1995;20:1S–73S.
3. Elliot JM, et al. Characteriza@on of Acute and Chronic Whiplash-‐Associated Disorders. Journal of Orthopaedic & Sports Physical Therapy, 2009, Volume: 39 Issue: 5 Pages: 312-‐323.
4. Jouko Kivioja, Irene Jensen, and Urban Lindgren. Neither the WAD-‐classifica@on nor the Quebec Task Force follow-‐up regimen seems to be important for the outcome ager a whiplash injury. A prospec@ve study on 186 consecu@ve pa@ents. Eur Spine J. 2008 Jul; 17(7): 930–935.
5. Hasue M. Pain and the nerve root. An interdisciplinary approach. Spine. 1993;18:2053-‐2058.
6. Jansen J, Bardosi A, Hildebrandt J, Lucke A. Cervicogenic, hemicranial avacks associated with vascular irrita@on or compression of the cervical nerve root C2. Clinical manifesta@ons and morphological findings. Pain. 1989;39:203-‐212.
7. Kaale BR, Krakenes J, Albrektsen G, Wester K. Head posi@on and impact direc@on in whiplash injuries: associa@ons with MRI-‐verified lesions of ligaments and membranes in the upper cervical spine. J Neurotrauma. 2005;22:1294-‐1302.
8. Kaale BR, Krakenes J, Albrektsen G, Wester K. Whiplash-‐associated disorders impairment ra@ng: neck disability index score according to severity of MRI findings of ligaments and membranes in the upper cervical spine. J Neurotrauma. 2005;22:466-‐475.
9. Jonsson H, Jr, Bring G, Rauschning W, Sahlstedt B. Hidden cervical spine injuries in traffic accident vic@ms with skull fractures. J Spinal Disord. 1991;4:251.
10. Peversson K, Hildingsson C, Toolanen G, Fagerlund M, Bjornebrink J. Disc pathology ager whiplash injury. A prospec@ve magne@c resonance imaging and clinical inves@ga@on. Spine. 1997;22:283-‐287; discussion 288.263.
References 11. Borchgrevink GE, Kaasa A, McDonagh D, S@les TC, Haraldseth O, Lereim I. Acute treatment of whiplash neck sprain injuries. A randomized trial of treatment during the first 14 days ager a car accident. Spine. 1998;23:25-‐31.
12. Kasch H, Qerama E, Bach FW, Jensen TS. Reduced cold pressor pain tolerance in non-‐recovered whiplash pa@ents: a 1-‐year prospec@ve study. Eur J Pain. 2005;9:561-‐569.
13. Tjell, C. and U. Rosenhall (1998). “Smooth pursuit neck torsion test: a specific test for cervical dizziness.” Otology & Neurotology 19(1): 76.
14. Treleaven, J., G. Jull, et al. (2003). “Dizziness and unsteadiness following whiplash injury: characteris@c features and rela@onship with cervical joint posi@on error.” Journal of Rehabilita@on Medicine 35(1): 36-‐43.
15. Treleaven, J., G. Jull, et al. (2005). “Smooth pursuit neck torsion test in whiplash-‐associated disorders: rela@onship to self-‐reports of neck pain and disability, dizziness and anxiety.” Journal of Rehabilita@on Medicine 37(4): 219-‐223.
16. Treleaven, J., G. Jull, et al. (2005). “Standing balance in persistent whiplash: a comparison between subjects with and without dizziness.” Journal of Rehabilita@on Medicine 37(4): 224-‐229.
17. Jull, G., D. Falla, et al. (2007). “Retraining cervical joint posi@on sense: The effect of two exercise regimes.” Journal of Orthopaedic Research 25(3): 404-‐412.
18. Treleaven J, Jull G, Sterling M. Dizziness and unsteadiness following whiplash injury: characteris@c features and rela@onship with cervical joint posi@on error. J Rehabil Med. 2003 Jan;35(1):36-‐-‐-‐43.
19. Sterling M, et al. Sensory hypersensi@vity occurs soon ager whiplash injury and is associated with poor recovery Pain 104 (2003) 509-‐517.
20. Adams JH, Doyle D, Ford I, Gennarelli TA, Graham DI, McLellan DR. Diffuse axonal injury in head injury: defini@on, diagnosis and grading. Histopathology. 1989; 15: 49–59.

Cranio-cervical Flexion Test • Performed with the pa@ent in supine crook lying with the neck in a neutral posi@on (no pillow) such that the line of the face is horizontal and a line bisec@ng the neck longitudinally is horizontal to the tes@ng surface. Layers of towel may be placed under the head if necessary to achieve a neutral posi@on. The uninflated pressure sensor is placed behind the neck so that it abuts the occiput and is inflated to a stable baseline pressure of 20 mm Hg, a standard pressure sufficient to fill the space between the tes@ng surface and the neck but not push the neck into a lordosis. The device provides the feedback and direc@on to the pa@ent to perform the required five stages of the test. The pa@ent is instructed that the test is not one of strength but rather one of precision. The movement is performed gently and slowly as a head nodding ac@on (as if saying “yes”). The CCFT tests the ac@va@on and endurance of the deep cervical flexors in progressive inner range posi@ons as the pa@ent avempts to sequen@ally target five, 2-‐mm Hg progressive pressure increases from the baseline of 20 mm Hg to a maximum of 30 mm Hg as well as to maintain a isometric contrac@on at the progressive pressures as an endurance task