when does my patient need a medical geneticist?/media/files/childrens/medical-professionals/... ·...
TRANSCRIPT
When does my patient need a Medical Geneticist?Rossana Sánchez, MDMedical Biochemical Genetics FellowEmory UniversityDepartment of Human Genetics
Children’s Healthcare of Atlanta | Emory University
Learning Objectives
• Describe the role of the Primary care provider in the medical genetics consultation
• Discuss when is it appropriate to consider a medical genetics consultation
• Discuss the value of a medical genetics consultation
• Describe some genetics resources for Primary care providers
Children’s Healthcare of Atlanta | Emory University
What is Medical Genetics?
• Broad and unique specialty that encompasses all organ systems, all periods of life and many disease entities
• Application of the principles of inheritance and our knowledge of human genes to:
• Diagnose
• Prevent/ Detect complications
• Treat disease
• Improve health
• Formally recognized as a medical specialty in the United States only within the past decade
ACMG Policy Statement. Scope of practice: a statement of the American College ofMedical Genetics and Genomics (ACMG)ACMG Board of Directors
Children’s Healthcare of Atlanta | Emory University
Role of the Medical Geneticist
• Focuses on conditions that are or may be heritable
• Provide consultations both inpatient and outpatient that consists of:
– Personal/family history
– Physical and neuro examination
– Risk assessment
– Ordering and interpreting genetic tests
– Management of inherited conditions
– Genetic counseling
Children’s Healthcare of Atlanta | Emory University
Role of the Medical Geneticist Ctd’
• Outside of direct patient care:
– Public health administration
– Health‐professional education
– Research
Children’s Healthcare of Atlanta | Emory University
Genetic counseling
• Process of helping people understand and adapt to the medical, psychological and familial implications of genetic contributions to disease
• Communicate complex information in a clear and relevant way
• This process integrates:– Interpretation of family and medical histories to assess the
chance of disease occurrence or recurrence– Education about inheritance, testing, management, prevention,
resources and research– Counseling to promote informed choices and adaptation to the
risk or condition
• Provided by physicians, physician assistants, genetic counselors, nurses
National Society of Genetic Counselors, 2005
Children’s Healthcare of Atlanta | Emory University
How will physicians use genetics in their practice in the coming years?
• Role of the Primary Care Provider:
– Considering the possibility of a genetic disease in the differential diagnosis
– Collecting a detailed family history
– Ordering testing as indicated
– Appropriately referring patients to genetic specialists
– Coordinate care
– Provide longitudinal care and support the patient and family
– Aiding in making medical decisions
Genetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services.Washington (DC): Genetic Alliance; 2009 Jul 8.
Children’s Healthcare of Atlanta | Emory University
Why might someone have/need a genetic consultation?
• A personal or family history of a genetic condition
• A birth defect or suspected chromosomal disorder
• A Personal or family history of a hereditary cancer
• A child with intellectual disability or developmental delay
• A history of recurrent miscarriages, a stillbirth, or a baby who died
• Advanced maternal age
• Abnormal test results that suggest a genetic or chromosomal condition
Genetics home reference: https://ghr.nlm.nih.gov/
Children’s Healthcare of Atlanta | Emory University
Clinical Case # 1
• Mrs. Smith is a 37 year old Caucasian female G5P0A4 who presents to your office for her first prenatal visit at 10 weeks of gestation
• She has had 4 spontaneous miscarriages in the first trimester• She has had extensive testing done to rule out
antiphospholipid syndrome, endocrine imbalance and uterine anomalies
• Chromosome studies (karyotype) on her and her husband were normal
• She has also had MTHFR gene testing which showed a heterozygous common polymorphism: c.665C>T (p.Ala222Val)
What are her indications for referral to Genetics?
Children’s Healthcare of Atlanta | Emory University
Clinical Case # 1 Ctd’
• She was referred to Genetic counseling for:
– Advanced maternal age (AMA ‐ > 35 yo) and discussion of testing options
• First trimester screen
• Second trimester screen
• Sequential or Integrated screen
• Non‐invasive prenatal testing (NIPT)
• CVS/Amnio
• No testing
– History of multiple miscarriages (≥ 2)
• Chromosome anomalies ruled out
– MTHFR testing
Credit: Thompson & Thompson genetics in medicine / Robert L. Nussbaum, Roderick R. McInnes, Huntington F. Willard.—Eighth edition.
Couple decided not to have fetal DNA studies and to await 2nd trimester ultrasound
Aneuploidy:presence of an abnormal number of chromosomes in a cell
35 yo risk of having a baby with Down syndrome equals risk of pregnancy loss from amniocentesis
Children’s Healthcare of Atlanta | Emory University
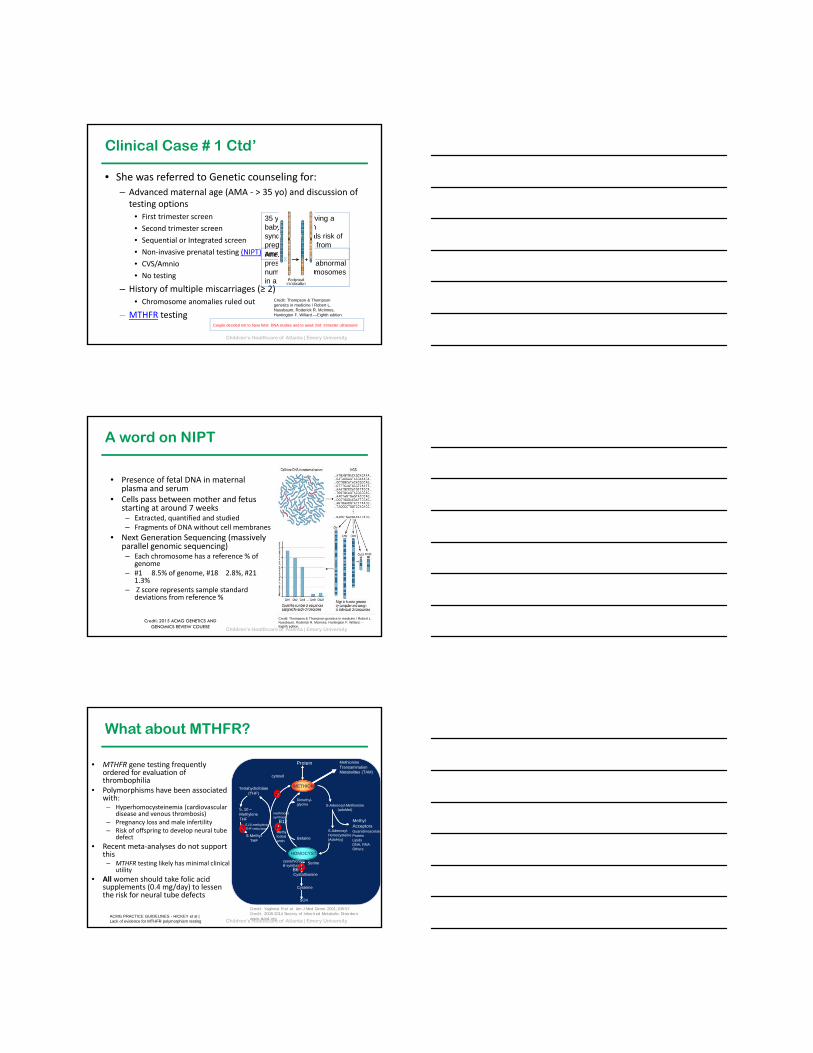
A word on NIPT
• Presence of fetal DNA in maternal plasma and serum
• Cells pass between mother and fetus starting at around 7 weeks– Extracted, quantified and studied– Fragments of DNA without cell membranes
• Next Generation Sequencing (massively parallel genomic sequencing)– Each chromosome has a reference % of
genome– #1 � 8.5% of genome, #18 � 2.8%, #21 �
1.3%– Z score represents sample standard
deviations from reference %
Credit: Thompson & Thompson genetics in medicine / Robert L. Nussbaum, Roderick R. McInnes, Huntington F. Willard.—Eighth edition.
Credti: 2015 ACMG GENETICS AND GENOMICS REVIEW COURSE
Children’s Healthcare of Atlanta | Emory University
What about MTHFR?
• MTHFR gene testing frequently ordered for evaluation of thrombophilia
• Polymorphisms have been associated with:– Hyperhomocysteinemia (cardiovascular
disease and venous thrombosis)– Pregnancy loss and male infertility – Risk of offspring to develop neural tube
defect
• Recent meta‐analyses do not support this – MTHFR testing likely has minimal clinical
utility
• All women should take folic acid supplements (0.4 mg/day) to lessen the risk for neural tube defects
ACMG PRACTICE GUIDELINES - HICKEY et al | Lack of evidence for MTHFR polymorphism testing
METHIONINE
Protein MethionineTransaminationMetabolites (TAM)
cytosol
Tetrahydrofolate(THF)
Dimethyl-glycine
5, 10 –MethyleneTHF
5,10-methyleneTHF reductase
5-MethylTHF
methinionesynthase
B12
Methylcobalamin
Betaine
S-Adenosyl-Methionine(adoMet)
MethylAcceptorsGuanidinoacetateProteinLipidsDNA, RNAOthers
S-Adenosyl-Homocysteine(AdoHcy)
HOMOCYSTEINE
cystathionineB-synthase
B6Serine
Cystathionine
Cysteine
SO4
Credit: Yaghmai R et al. Am J Med Genet 2001;108:57Credit: 2008-2014 Society of Inherited Metabolic Disorders www.simd.org
Children’s Healthcare of Atlanta | Emory University
Other indications for Preconception or Prenatal referrals to genetics• Women/couples who are interested in genetic testing or screening
• Neonatal deaths/previous child with birth defect
• Exposure to radiation, medications, illegal drugs, chemicals
• Couples who are first cousins or other close blood relatives
• Abnormal prenatal screening
• Abnormal ultrasound findings
• Abnormal results from confirmatory testingGenetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services.Washington (DC): Genetic Alliance; 2009 Jul 8.
Children’s Healthcare of Atlanta | Emory University
Clinical Case # 1 Ctd’
• Anatomy scan at 20 weeks of age showed:
– IUGR
– VSD
• After another discussion with genetic counselor they opted for NIPT which was normal for 13,18,21, XY
• What could be missed?
– Unbalanced translocation
– Aneuploidy of other autosomes
– Microdeletion/duplication
– Triploidy
Children’s Healthcare of Atlanta | Emory University
Clinical Case # 1 Ctd’
• What about the family history?
37 yoMultiple miscarriages
40 yo
72 yoBreast CA dx 70
76 yoMTC dx 54Pheo dx 67
43 yoMTC dx 22HPT dx 24
18 yoProphylactic thyroidectomy at 5 yo
d. 41 yoMTC dx 38 yo
40 yoArthritisCleft palate
46 yoRetinal detachment
d. 60 yoMIDMHTNRetinal detachment
d. 80 yoAlzheimer dx 78 yo
male
female
spontaneous abortion
unknown gender
pregnancy
arrow indicates proband
d. : deceasedPheo: pheochromocytomaMTC: medullary thyroid carcinomaHPT: Hyperparathyroidism
P
P
68 yoHealthy
Children’s Healthcare of Atlanta | Emory University
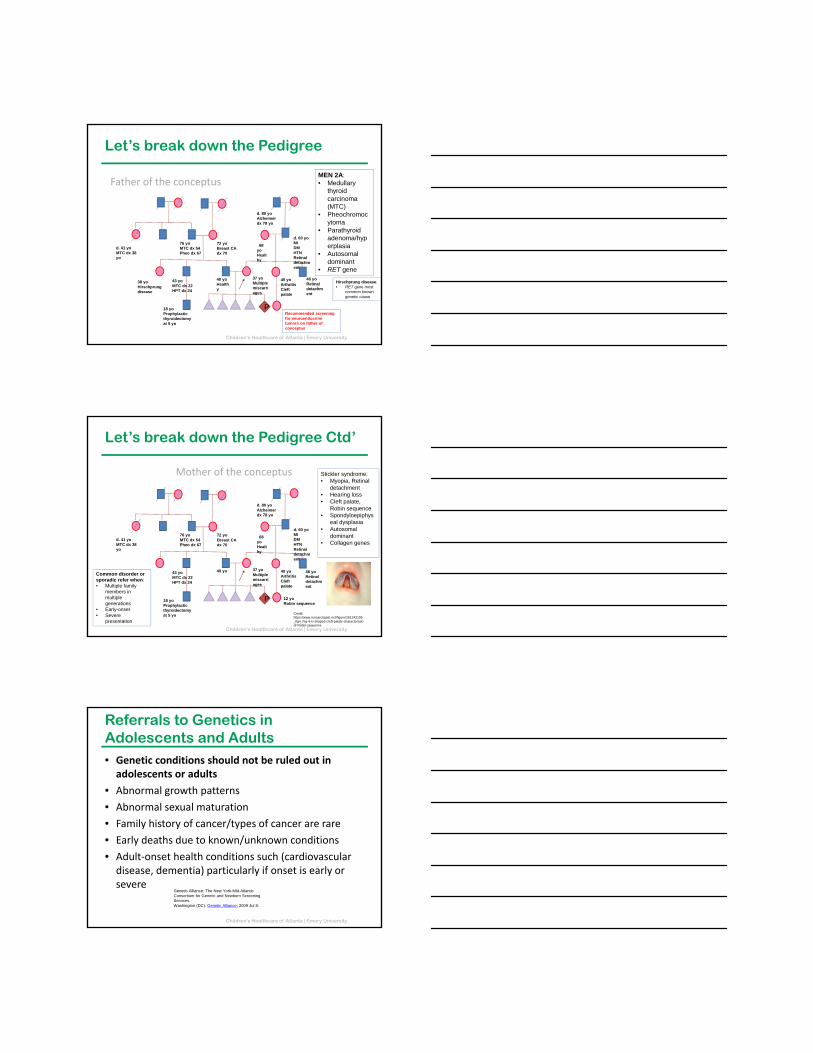
Let’s break down the Pedigree
Father of the conceptus
37 yoMultiple miscarriages
40 yoHealthy
72 yoBreast CA dx 70
76 yoMTC dx 54Pheo dx 67
43 yoMTC dx 22HPT dx 24
18 yoProphylactic thyroidectomy at 5 yo
d. 41 yoMTC dx 38 yo
40 yoArthritisCleft palate
46 yoRetinal detachment
d. 60 yoMIDMHTNRetinal detachment
d. 80 yoAlzheimer dx 78 yo
MEN 2A:• Medullary
thyroid carcinoma (MTC)
• Pheochromocytoma
• Parathyroid adenoma/hyperplasia
• Autosomal dominant
• RET gene
38 yoHirschprungdisease
Hirschprung disease:• RET gene most
common known genetic cause
P
68 yoHealthy
Recommended screening for neuroendocrine tumors on father of conceptus
Children’s Healthcare of Atlanta | Emory University
Let’s break down the Pedigree Ctd’
Mother of the conceptus
Credit: https://www.researchgate.net/figure/281243195_fig4_Fig-4-U-shaped-cleft-palate-characteristic-of-Robin-sequence
37 yoMultiple miscarriages
40 yo
72 yoBreast CA dx 70
76 yoMTC dx 54Pheo dx 67
43 yoMTC dx 22HPT dx 24
18 yoProphylactic thyroidectomy at 5 yo
d. 41 yoMTC dx 38 yo
40 yoArthritisCleft palate
46 yoRetinal detachment
d. 60 yoMIDMHTNRetinal detachment
d. 80 yoAlzheimer dx 78 yo
Stickler syndrome:• Myopia, Retinal
detachment• Hearing loss• Cleft palate,
Robin sequence• Spondyloepiphys
eal dysplasia• Autosomal
dominant• Collagen genes
12 yoRobin sequence
P
68 yoHealthy
Common disorder or sporadic refer when:• Multiple family
members in multiple generations
• Early-onset• Severe
presentation
Children’s Healthcare of Atlanta | Emory University
Referrals to Genetics in Adolescents and Adults• Genetic conditions should not be ruled out in adolescents or adults
• Abnormal growth patterns
• Abnormal sexual maturation
• Family history of cancer/types of cancer are rare
• Early deaths due to known/unknown conditions
• Adult‐onset health conditions such (cardiovascular disease, dementia) particularly if onset is early or severe
Genetic Alliance; The New York-Mid-Atlantic Consortium for Genetic and Newborn Screening Services.Washington (DC): Genetic Alliance; 2009 Jul 8.
Children’s Healthcare of Atlanta | Emory University
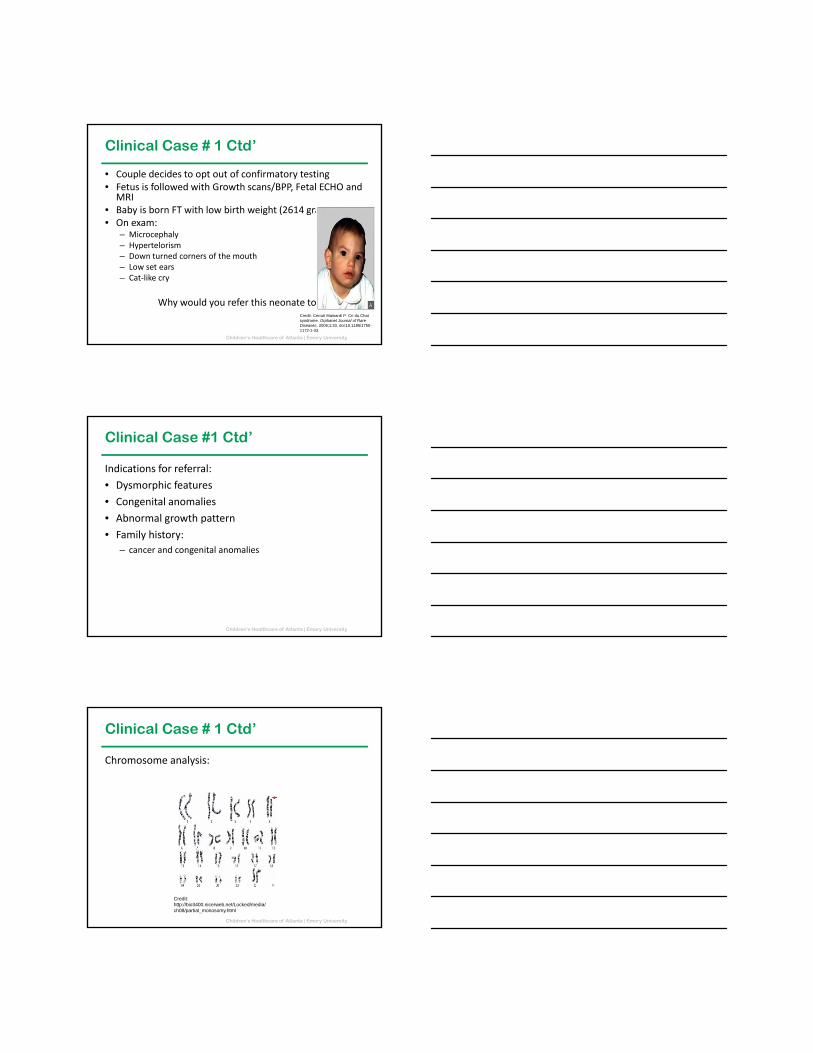
Clinical Case # 1 Ctd’
• Couple decides to opt out of confirmatory testing• Fetus is followed with Growth scans/BPP, Fetal ECHO and
MRI• Baby is born FT with low birth weight (2614 grams)• On exam:
– Microcephaly– Hypertelorism– Down turned corners of the mouth– Low set ears– Cat‐like cry
Why would you refer this neonate to genetics?Credit: Cerruti Mainardi P. Cri du Chat syndrome. Orphanet Journal of Rare Diseases. 2006;1:33. doi:10.1186/1750-1172-1-33.
Children’s Healthcare of Atlanta | Emory University
Clinical Case #1 Ctd’
Indications for referral:
• Dysmorphic features
• Congenital anomalies
• Abnormal growth pattern
• Family history:
– cancer and congenital anomalies
Children’s Healthcare of Atlanta | Emory University
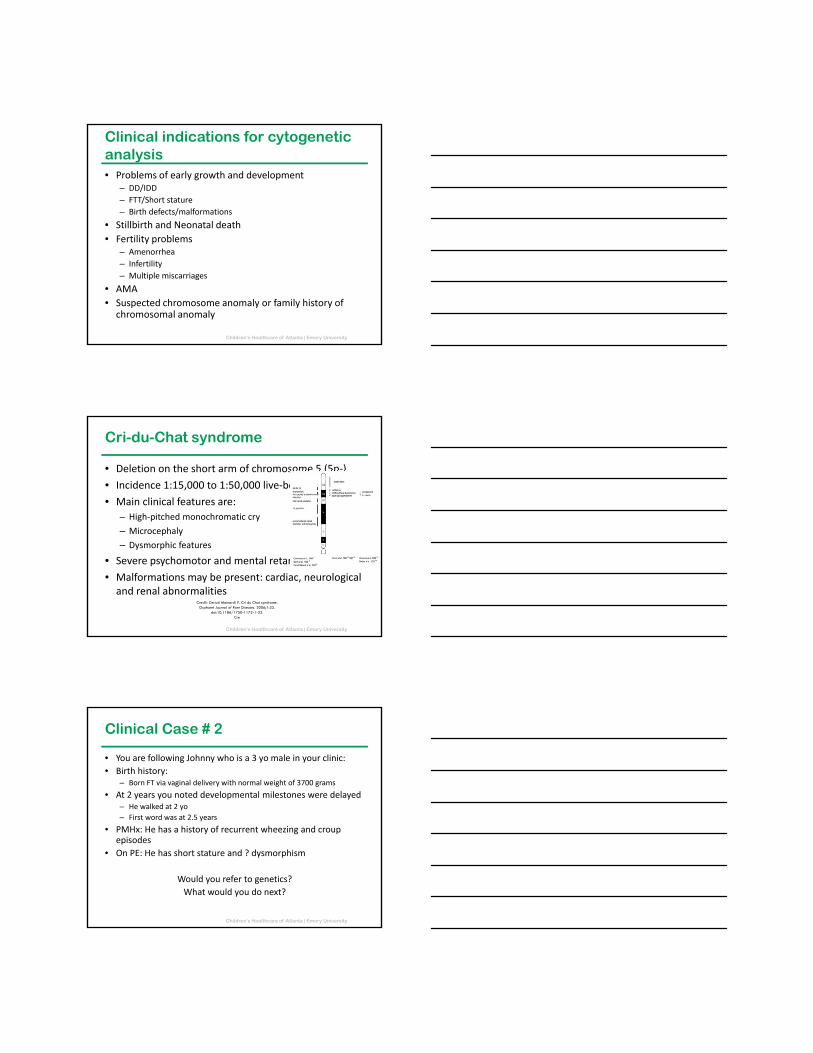
Clinical Case # 1 Ctd’
Chromosome analysis:
Credit: http://bio3400.nicerweb.net/Locked/media/ch08/partial_monosomy.html
Children’s Healthcare of Atlanta | Emory University
Clinical indications for cytogenetic analysis• Problems of early growth and development
– DD/IDD
– FTT/Short stature
– Birth defects/malformations
• Stillbirth and Neonatal death
• Fertility problems– Amenorrhea
– Infertility
– Multiple miscarriages
• AMA
• Suspected chromosome anomaly or family history of chromosomal anomaly
Children’s Healthcare of Atlanta | Emory University
Cri-du-Chat syndrome
• Deletion on the short arm of chromosome 5 (5p‐)
• Incidence 1:15,000 to 1:50,000 live‐born infants
• Main clinical features are:
– High‐pitched monochromatic cry
– Microcephaly
– Dysmorphic features
• Severe psychomotor and mental retardation.
• Malformations may be present: cardiac, neurological and renal abnormalities
Credit: Cerruti Mainardi P. Cri du Chat syndrome. Orphanet Journal of Rare Diseases. 2006;1:33.
doi:10.1186/1750-1172-1-33.Cre
Children’s Healthcare of Atlanta | Emory University
Clinical Case # 2
• You are following Johnny who is a 3 yo male in your clinic:
• Birth history:– Born FT via vaginal delivery with normal weight of 3700 grams
• At 2 years you noted developmental milestones were delayed– He walked at 2 yo
– First word was at 2.5 years
• PMHx: He has a history of recurrent wheezing and croup episodes
• On PE: He has short stature and ? dysmorphism
Would you refer to genetics?
What would you do next?
Children’s Healthcare of Atlanta | Emory University
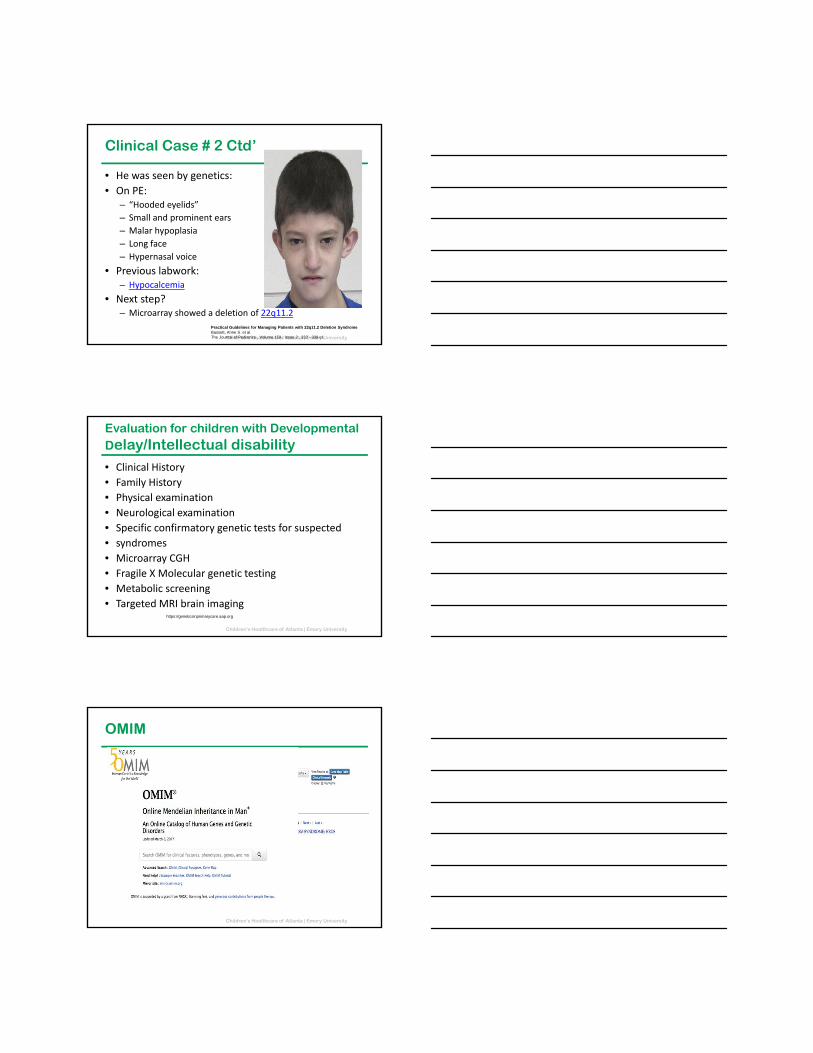
Clinical Case # 2 Ctd’
• He was seen by genetics:
• On PE:– “Hooded eyelids”
– Small and prominent ears
– Malar hypoplasia
– Long face
– Hypernasal voice
• Previous labwork:– Hypocalcemia
• Next step?– Microarray showed a deletion of 22q11.2
Practical Guidelines for Managing Patients with 22q11.2 Deletion SyndromeBassett, Anne S. et al.The Journal of Pediatrics , Volume 159 , Issue 2 , 332 - 339.e1
Children’s Healthcare of Atlanta | Emory University
Evaluation for children with Developmental Delay/Intellectual disability• Clinical History
• Family History
• Physical examination
• Neurological examination
• Specific confirmatory genetic tests for suspected
• syndromes
• Microarray CGH
• Fragile X Molecular genetic testing
• Metabolic screening
• Targeted MRI brain imaginghttps://geneticsinprimarycare.aap.org
Children’s Healthcare of Atlanta | Emory University
OMIM
https://omim.org/
Children’s Healthcare of Atlanta | Emory University
22q11.2 Deletion Syndrome
• Contiguous gene deletion: 22q11.2 (93% de novo)
• Autosomal dominant
• Clinical Findings:– Congenital heart disease (TOF, interrupted aortic arch)
– Palatal abnormalities
– Characteristic facial features (Caucasian)
– Developmental delay and Learning difficulties (70%‐90%)
– Autism in approximately 20% and schizophrenia in 25% of adults
– Immune deficiency – T Cell (77%)
– Hypocalcemia 50%
Children’s Healthcare of Atlanta | Emory University
GeneReviews
www.ncbi.nlm.nih.gov/books/NBK1116/
Children’s Healthcare of Atlanta | Emory University
Genetics Home Reference
https://ghr.nlm.nih.gov/

Children’s Healthcare of Atlanta | Emory University
Unique
http://www.rarechromo.org/html/home.asp
Children’s Healthcare of Atlanta | Emory University
Other indications for referral in Infancy and Childhood• Positive newborn screen
• Developmental delay/regression
• Autism spectrum disorder
• Hypotonia/muscle weakness
• Difficult to control seizures
• Abnormal brain MRI
• Growth problems: failure to thrive, overgrowth, short stature, disproportionate growth, micro or macrocephaly
• Suspected skeletal dysplasia (Proportionate or disproportionate)
• Congenital or early onset blindness or deafness
Children’s Healthcare of Atlanta | Emory University
Benefits of a Genetic Referral
• Confirm a genetic diagnosis
• End “Diagnostic odyssey”
• Guide diagnostic studies and surveillance
• Interpret diagnostic studies
• Highlight/detect/prevent complications
• Provide recurrence risk/occurrence risk or prognostic information
• Family planning discussion
• Evaluate at risk family members
Children’s Healthcare of Atlanta | Emory University
Explaining the Referral to Patients/Parents• Explain findings on physical exam and why a referral may
be indicated• If autism or developmental delays – explain you may
identify a cause for these or sometimes association with other malformations
• If abnormal newborn screen – explain what a screen is and why follow up confirmatory testing is needed
• If family history is abnormal explain possible risks for patient and family members
• Ask to set aside sufficient time for prolonged visit• Ask about family history beforehand• May bring pictures of patient and family
Children’s Healthcare of Atlanta | Emory University
What should a referral include?
• Patient information
• Name and address of the referrer
• Reason for the referral
• Information about the suspected diagnosis
• Family history
• Growth charts
• Developmental screens
• Copies of evaluations of speech, physical, occupational therapists
• Previous testing done – laboratory and imaging studies
• If skeletal dysplasia is suspected – need actual images (CD)
• Reports from other subspecialists
Children’s Healthcare of Atlanta | Emory University
Resources
• ACMG Standards & Guidelines – www.acmg.net
• OMIM– https://omim.org/
• GeneReviews– www.ncbi.nlm.nih.gov/books/NBK1116/
• GeneTests Reviews – www.genetests.org
• Genetic Home Reference – https://ghr.nlm.nih.gov/
• Unique Rare Chromosomes – http://www.rarechromo.org/html/home.asp
Credit: U.S. National Library of Medicine
Children’s Healthcare of Atlanta | Emory University
Resources Ctd’
• Genetic Alliance– http://geneticalliance.org/
• National Organization of Rare Disorders– www.rarediseases.org
• Genetics in Primary Care Institute– https://geneticsinprimarycare.aap.org
Newborn screening• ACMG ACT sheets
– https://www.ncbi.nlm.nih.gov/books/NBK55827/
• New England Emergency Protocols – http://newenglandconsortium.org/for‐professionals/acute‐illness‐
protocols/
• Baby’s first test– http://www.babysfirsttest.org/
Children’s Healthcare of Atlanta | Emory University
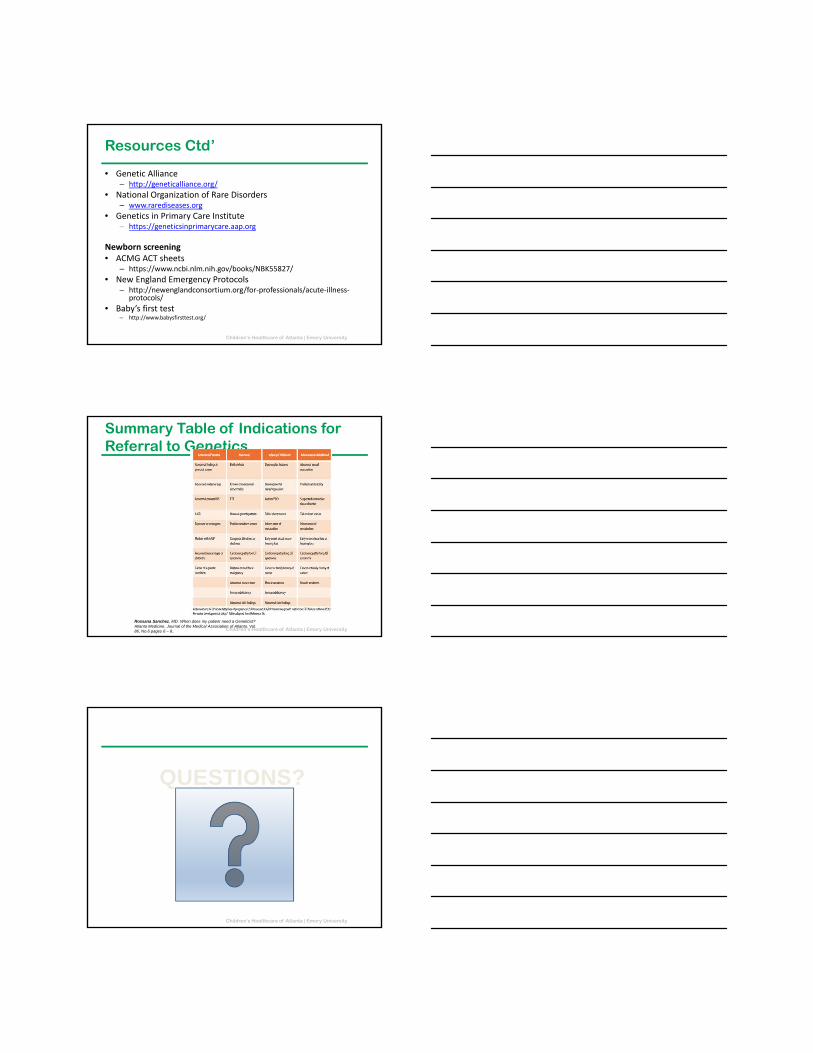
Summary Table of Indications for Referral to Genetics
Rossana Sanchez, MD. When does my patient need a Geneticist? Atlanta Medicine, Journal of the Medical Association of Atlanta. Vol. 86, No.6 pages 6 – 8..
Children’s Healthcare of Atlanta | Emory University
QUESTIONS?