when does huntington’s disease begin? richard dubinsky, md, mph university of kansas 11/16/12
TRANSCRIPT
When does Huntington’s Disease Begin?
Richard Dubinsky, MD, MPH
University of Kansas
11/16/12

Disclosures Current NIH/NCAM and FDA
OPD 2CARE CRESTE
CHDI ENROLL-HD Facilitator, redefining
HD across the life span
Completed: NIH: CARE-HD,
PHAROS, PREDICT-HD FDA: RID-HD HSG: Longitudinal
database CHDI: COHORT

HD Gene Cloned 1993,from the Venezuela project Trinucleotide repeat, one of the first three
described CAG expansion Gene product
huntingtin htt

Ross C, Lancet Neurology 2011;10:83-98

CAGn Ranges
<26 normal, 17 most common 26-29 rarely expand 30-36 expand, mostly 35 and 36 35-38 unstable expansion
HD in future generations 39 and above: HD
80% of people with 39 repeats will develop HD

What happened?
Founder effect, maternal germ cell mosaicism
Maternal transmission rarely changes CAGn
Paternal transmission usually expands Mean expansion 6.2 Mean contraction 1.3

Lee JM. Neurology 2012;78:690-5

Onset of HD
Traditionally defined as onset of chorea Always gradual, never sudden Cognitive, behavioral and motor changes
can precede chorea

Determining Clinical Onset
Historical data Chorea Other domains:
Behavior Cognition

UHDRS-99
Copyright © HSG Ltd.

HD: Juvenile Form
Predominance of dystonic rigidity Early cognitive problems Prolonged survival

http://promotingexcellence.org/huntingtons/

Is the initial symptom disease onset?
Frequent phenoconversion after predictive testing
4 x > normal population suicide rate around phenoconversion
HD is not protective against other disorders

HD: Progression
Total Functional Capacity Five domains
Occupation (3) Fiscal (3) Activities of daily living (3) Household chores (2) Residence (2)
T
Slope ~ 0.9/y
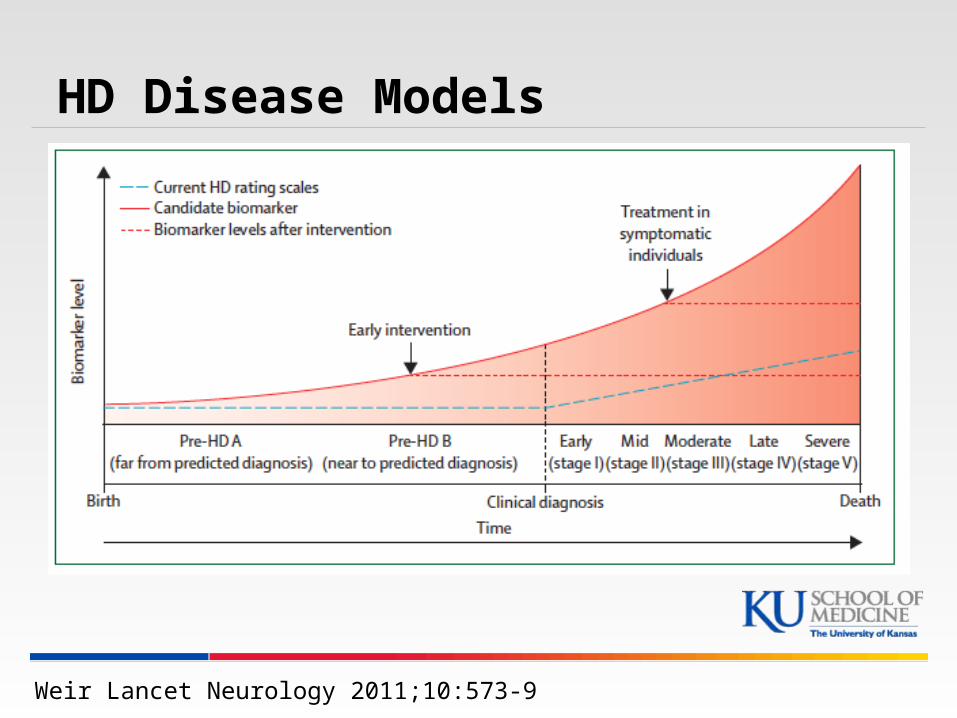
HD Disease Models
Weir Lancet Neurology 2011;10:573-9

Ross C, Lancet Neurology 2011;10:83-98

Ross C, Lancet Neurology 2011;10:83-98
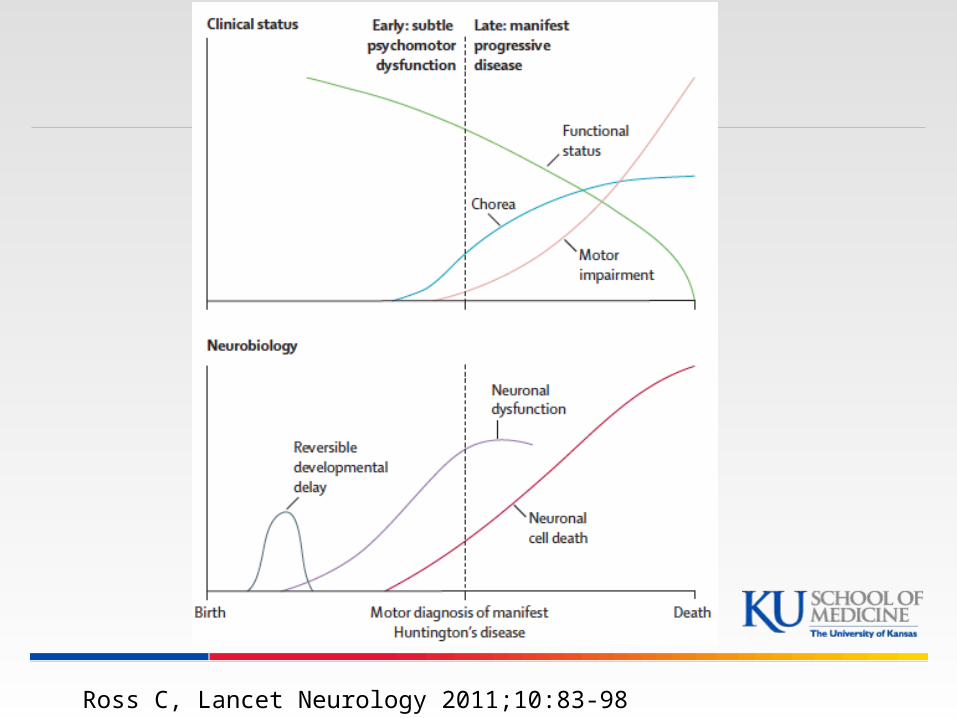
Ross C, Lancet Neurology 2011;10:83-98

Lee JM. Neurology 2012;78:690-5

Brinkman R Am J Hum Genet, 1997;60:1202-10

Brinkman R Am J Hum Genet, 1997;60:1202-10

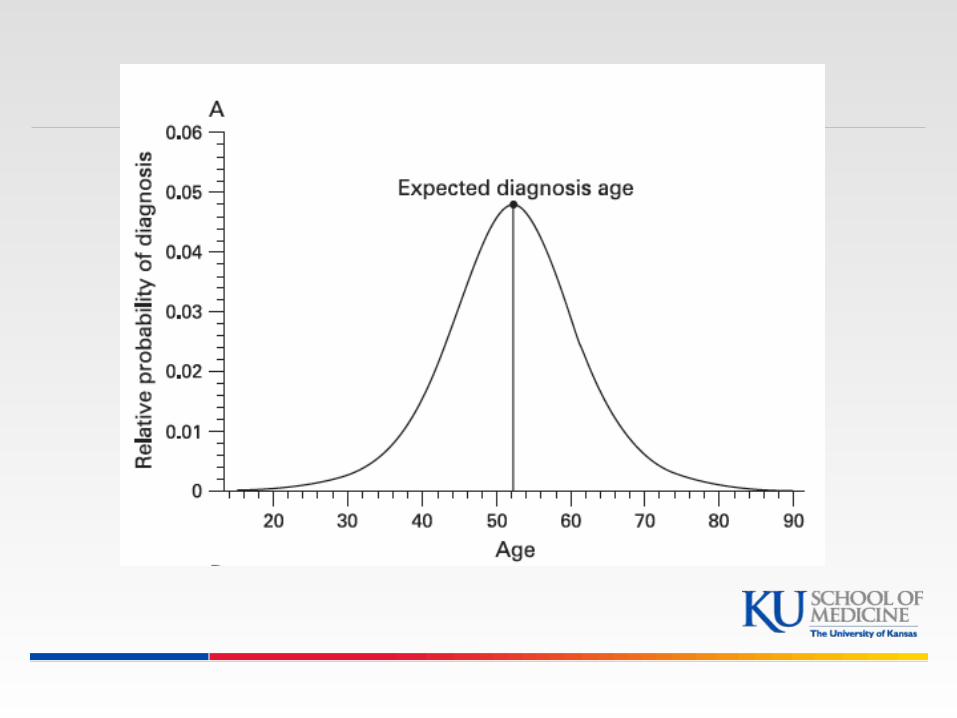
Langbehn D, Am J Med Genet B Neuropscyh 2010;153B:397-408

PREDICT-HD
Prospective cohort study of gene +, asymptomatic subjects and gene – controls Near (onset < 9 years) Mid (onset 9-15 years) Far (onset > 15 years)
Yearly neuroimaging, cognitive and psychomotor testing


Paulsen J, JNNSP 2008;79:874-80

Paulsen J, JNNSP 2008;79:874-80

Paulsen J, Brain Res Bull 2010;82:201-7

Aylward E, JNNSP, 2011;82:405

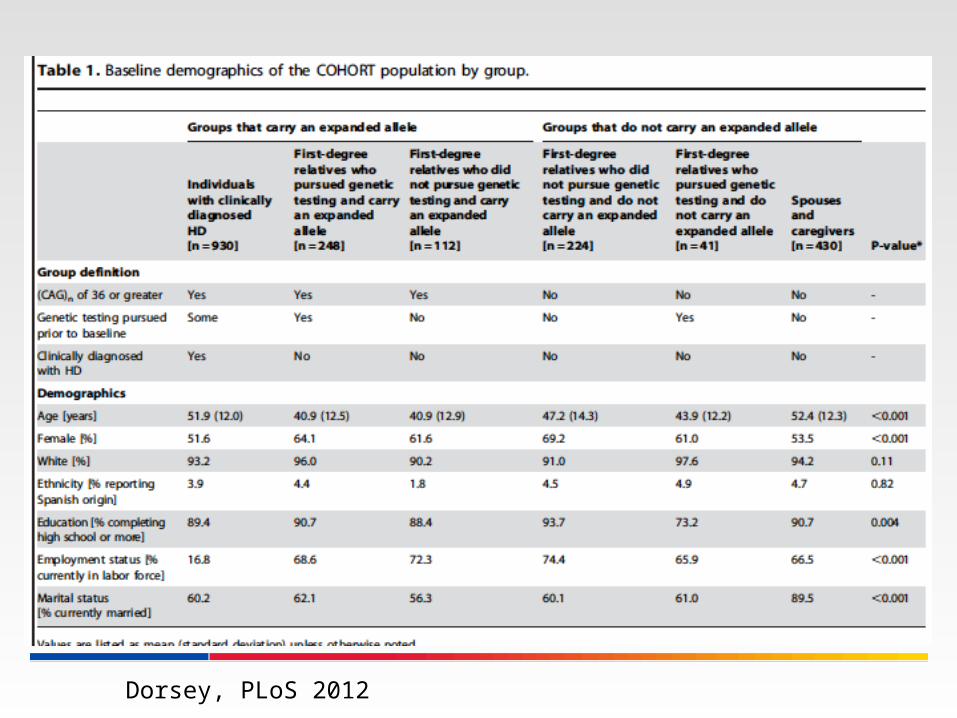
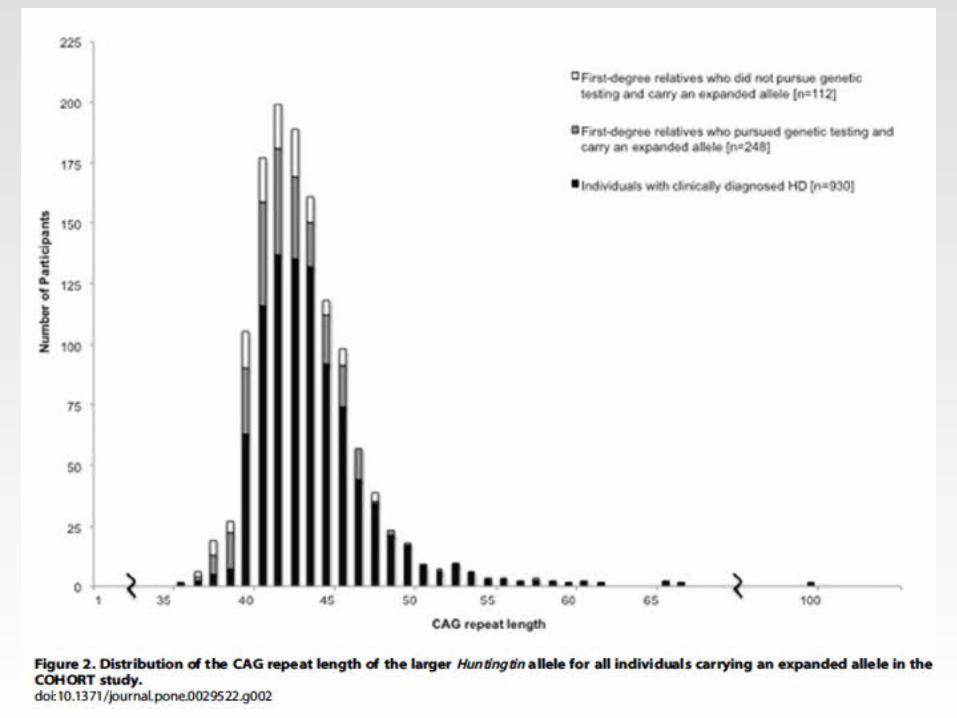
COHORT
Multi-site, international natural history of HD
People with HD, those at risk, family members, some children
2006-2011 Funded by CHDI
Dorsey, PLoS 2012

Dorsey, PLoS 2012
Dorsey, PLoS 2012

Dorsey, PLoS 2012

Dorsey, PLoS 2012

Symbol Digit Modality / Stroop
red green blue blue green red
red green blue blue green red
+ ( ! < & ^ @ )
1 2 3 4 5 6 7 8
@ @ ) ^ ( + ! +

COHORT: Medication Use
Dorsey, PLoS 2012

Dorsey, PLoS 2012

TRACK-HD
Prospective, longitudinal cohort study Manifest HD Gene + (pre-manifest HD)
Burden of pathology scoreAge x (CAG-35.5)> 250
Gene -, non-matched controls

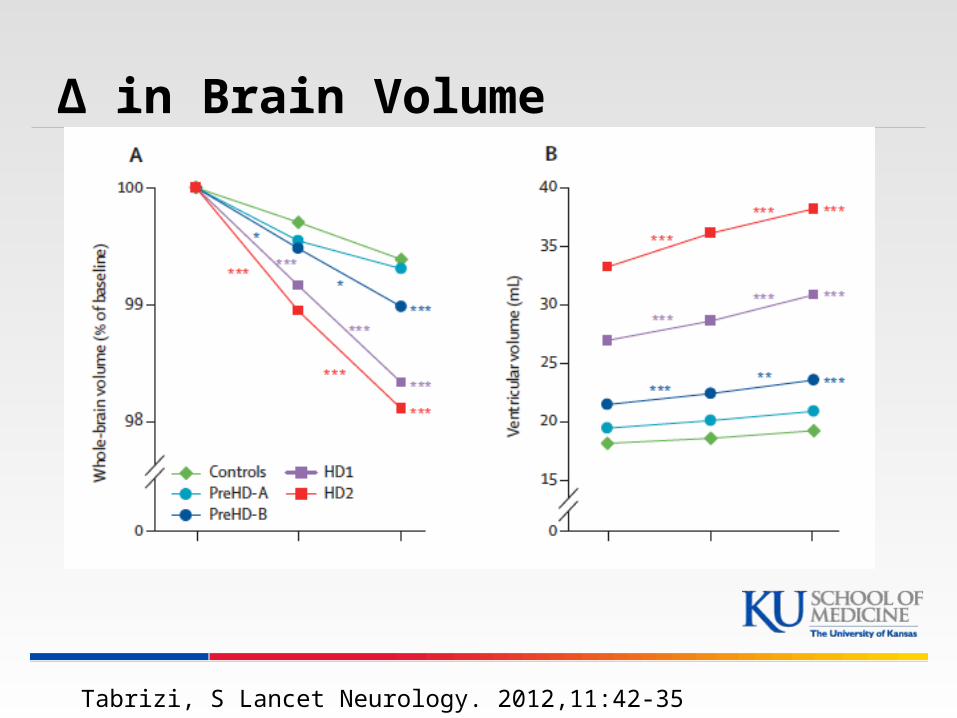
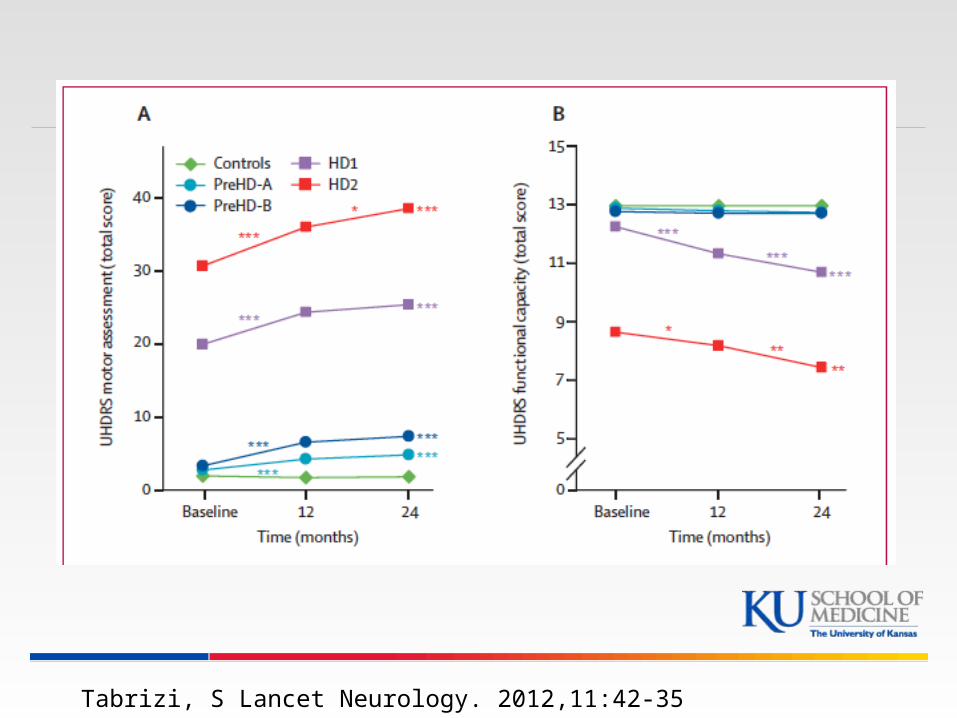
HD Cohorts
PreHD-A and PreHD-B Dichotomized at median predicted years
to diagnosis (Langbehn score) HD1 and HD2
Stage 1 TFC 11-13 Stage 2 TFC 7-10

TRACK-HD Baseline Characteristics
Tabrizi S, Lancet Neurology 2009

Tabrizi S, Lancet Neurology 2009

Tabrizi S, Lancet Neurology 2009
Tabrizi, S Lancet Neurology. 2012,11:42-35
∆ in Brain Volume

Tabrizi, S Lancet Neurology. 2012,11:42-35
Striatal volumes

Tabrizi, S Lancet Neurology. 2012,11:42-35

Tabrizi, S Lancet Neurology. 2012,11:42-35

Tabrizi, S Lancet Neurology. 2012,11:42-35
Neuropsychological Tests

Tabrizi, S Lancet Neurology. 2012,11:42-35
Tabrizi, S Lancet Neurology. 2012,11:42-35

HD Clinical Trials Completed
CARE-HD RID-HD TETRA-HD TREND-HD MINOS CYTE I PHEND-HD DIMEBOND 1 & 2 HSG Database PHAROS COHORT
Ongoing 2CARE CRESTE-HD PRE-CREST REACH-HD PREDICT-HD

Potential Treatments
RNA Silencing Anti-sense oligonucleotides RNA interference

Delivery Mechanisms
RNAi injected into CSF Virus injected into:
CSF Putamen
Virus inserted into bone marrow Inserted via nanotube and heavy metal
through the olfactory bulbs

Bone Marrow Transplantation?
Mutant htt expressed in many cells Inflammatory markers before and at
phenoconversion Bone marrow derived cells get into the brain
Lancet 2004;363:1432-7



Aronin N NEJM 2012;367-1753

Conclusion
Changes that lead to HD start > 10 years before ‘phenoconversion’
Redefining the onset Research Clinical diagnosis
Implications

Huntington Study Group

Sleep and HD
Insomnia is very common Sun downing Delusions of not sleeping

