whats up with my gut comparing crohn's disease and ibs ...c.ymcdn.com/sites/ · pdf...
TRANSCRIPT
1
What's Up with My Gut? What's Up with My Gut? Comparing Comparing Crohn's Crohn's Disease Disease
and Irritable Bowel and Irritable Bowel SyndromeSyndrome
Fl id Ph i A i iFl id Ph i A i iFlorida Pharmacist AssociationFlorida Pharmacist Association
St. Augustine, 2015St. Augustine, 2015
Jose Barboza, Jose Barboza, Pharm.DPharm.D., C.D.E.., C.D.E.Pharmacotherapeutics & Clinical ResearchPharmacotherapeutics & Clinical Research
University of South FloridaUniversity of South Florida College of PharmacyCollege of Pharmacy
ObjectivesObjectives
Compare and contrast functional disorders and inflammatory diseases
Recognize the differences in symptoms between Crohn’s Disease and Irritable Bowel Syndrome (IBS)y ( )
Review the medications used to treat Crohn’s disease and IBS
Identify the mechanism of action, contraindications and major adverse effects of the medications used to treat Crohn’s disease and IBS
Compare and Contrast: Definition
Inflammatory BowelDisease (IBD)
Inflammatory BowelDisease (IBD)
Ch i i fl i
Irritable BowelSyndrome (IBS)Irritable BowelSyndrome (IBS)
Pain/ DiscomfortChronic inflammation
of the intestine
Crohn disease (CD)
Ulcerative colitis (UC)
Change in Bowel habits
Absence of organic cause
Diarrhea (IBS-D)
Constipation (IBS-C)
Alternating/Mixed (IBS-M)
2
Irritable Bowel Syndrome: DefinitionIrritable Bowel Syndrome: Definition Gastrointestinal (GI) syndrome characterized by Gastrointestinal (GI) syndrome characterized by
abdominal pain or discomfort abdominal pain or discomfort associated with associated with altered altered bowel habits bowel habits in the in the absence of organic causeabsence of organic cause
Presents with chronically recurring symptomsPresents with chronically recurring symptomsL bd i l i Lower abdominal pain
Altered bowel function
Diarrhea predominant (IBS-D)
Constipation predominant (IBS-C)
Constipation and diarrhea (IBS-M)
Incomplete evacuation
Urgency
Bloating
Irritable Bowel Syndrome: DiagnosisIrritable Bowel Syndrome: Diagnosis
Rome III Criteria for Irritable Bowel Syndrome
Recurrent abdominal pain or discomfort occurring for three episodes per month in the last 3 months associated with two or more of:
1 Improvement with defecation
2 Onset associated with change in frequency of stool
3 Onset associated with a change in form of stool
Am J Gastroenterol, 2009. 104 Suppl 1: p. S1-35.
Irritable Bowel Syndrome: Irritable Bowel Syndrome: EpidemiologyEpidemiology
Prevalence in US is 10Prevalence in US is 10--15%15% More common More common
FFemales (~2:1)emales (~2:1)
Young adulthoodYoung adulthood
15% of those affected seek medical attention15% of those affected seek medical attention
Most commonly diagnosed GI conditionMost commonly diagnosed GI condition 2525--50% of gastroenterologist referrals 50% of gastroenterologist referrals
Clin Epidemiol. 2014; 6: 71–80.

3
Inflammatory Bowel DiseaseInflammatory Bowel Disease
https://gi.jhsps.org/GDL_Disease
Ulcerative ColitisUlcerative Colitis Inflammatory process in the Inflammatory process in the
colon and rectumcolon and rectum Affects the mucosa & Affects the mucosa & submucosasubmucosa
Continuous lesionsContinuous lesions
Inflammatory Bowel Disease: DefinitionInflammatory Bowel Disease: Definition
Crohn’s DiseaseCrohn’s Disease Inflammatory process in Inflammatory process in
any part any part of the GI tract of the GI tract BowelBowel--wall injury, wall injury,
narrowing of the intestinal narrowing of the intestinal Continuous lesionsContinuous lesionslumenlumen
Terminal ileum is the most Terminal ileum is the most common sitecommon site
Affects the entire wall of Affects the entire wall of the bowelthe bowel Discontinuous lesions Discontinuous lesions
https://gi.jhsps.org/GDL_Disease
Inflammatory Bowel Disease: Inflammatory Bowel Disease: EpidemiologyEpidemiology
Crohn’s DiseaseCrohn’s Disease 10.7 cases per 10.7 cases per 100,000 100,000 in in
USAUSA
33 00033 000
Ulcerative Colitis Ulcerative Colitis 12.2 cases 7 per 100,000 12.2 cases 7 per 100,000
in USAin USA
38 00038 000 33,000 new cases per year33,000 new cases per year
Equal prevalenceEqual prevalence
Typically diagnosed in Typically diagnosed in ages 15ages 15--35 (median age 35 (median age 29.5)29.5)
38,000 new cases per year38,000 new cases per year
Higher in malesHigher in males
Typically diagnosed at Typically diagnosed at ages 15ages 15--35 (median 34.935 (median 34.9
http://www.ccfa.org/assets/pdfs/updatedibdfactbook.pdf
4
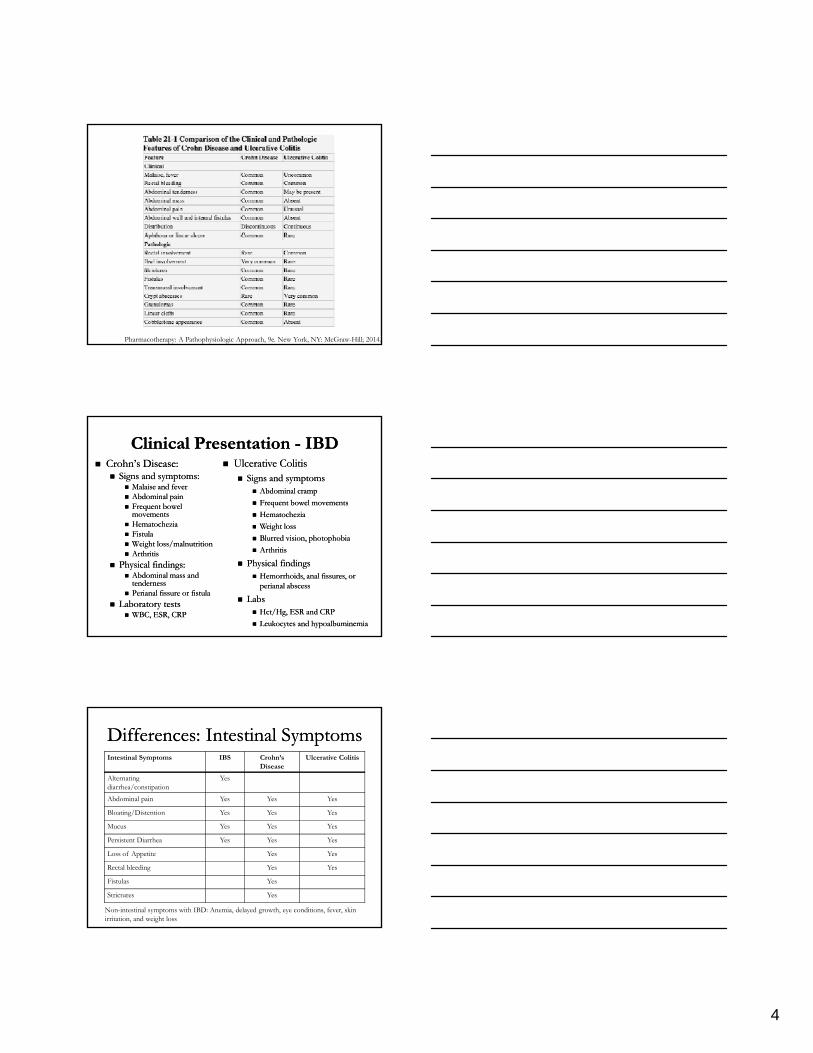
Pharmacotherapy: A Pathophysiologic Approach, 9e. New York, NY: McGraw-Hill; 2014.
Clinical Presentation Clinical Presentation -- IBDIBD Crohn’s Disease:Crohn’s Disease:
Signs and symptoms:Signs and symptoms: Malaise and feverMalaise and fever Abdominal painAbdominal pain Frequent bowel Frequent bowel
movementsmovements HematocheziaHematochezia
Ulcerative ColitisUlcerative Colitis Signs and symptomsSigns and symptoms
Abdominal crampAbdominal cramp
Frequent bowel movementsFrequent bowel movements
HematocheziaHematochezia
Weight lossWeight lossHematocheziaHematochezia FistulaFistula Weight loss/malnutritionWeight loss/malnutrition ArthritisArthritis
Physical findings:Physical findings: Abdominal mass and Abdominal mass and
tendernesstenderness Perianal fissure or fistulaPerianal fissure or fistula
Laboratory testsLaboratory tests WBC, ESR, CRPWBC, ESR, CRP
Weight lossWeight loss
Blurred vision, photophobiaBlurred vision, photophobia
ArthritisArthritis
Physical findingsPhysical findings Hemorrhoids, anal fissures, or Hemorrhoids, anal fissures, or
perianal abscess perianal abscess
LabsLabs HctHct/Hg, ESR and CRP/Hg, ESR and CRP
Leukocytes and Leukocytes and hypoalbuminemiahypoalbuminemia
Differences: Intestinal SymptomsDifferences: Intestinal SymptomsIntestinal Symptoms IBS Crohn’s
DiseaseUlcerative Colitis
Alternatingdiarrhea/constipation
Yes
Abdominal pain Yes Yes Yes
Bloating/Distention Yes Yes Yes
Mucus Yes Yes Yes
Persistent Diarrhea Yes Yes Yes
Loss of Appetite Yes Yes
Rectal bleeding Yes Yes
Fistulas Yes
Strictures Yes
Non-intestinal symptoms with IBD: Anemia, delayed growth, eye conditions, fever, skin irritation, and weight loss
5
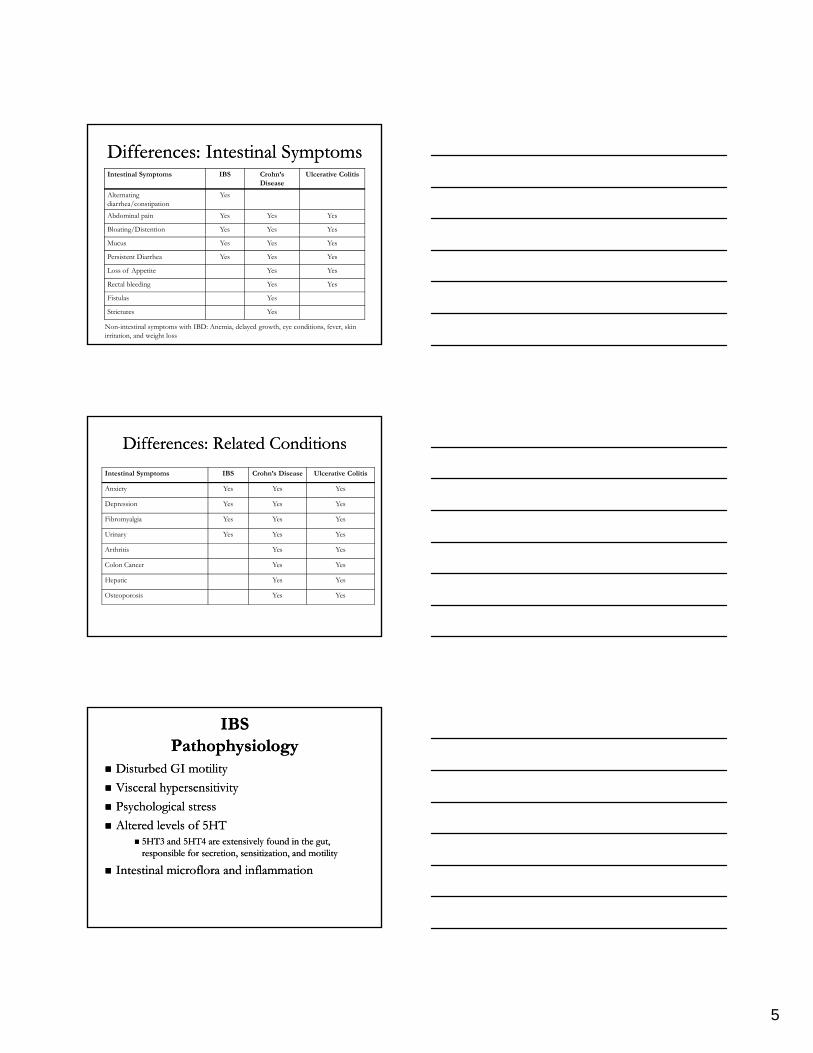
Differences: Intestinal SymptomsDifferences: Intestinal SymptomsIntestinal Symptoms IBS Crohn’s
DiseaseUlcerative Colitis
Alternatingdiarrhea/constipation
Yes
Abdominal pain Yes Yes Yes
Bloating/Distention Yes Yes Yes
Mucus Yes Yes Yes
Persistent Diarrhea Yes Yes Yes
Loss of Appetite Yes Yes
Rectal bleeding Yes Yes
Fistulas Yes
Strictures Yes
Non-intestinal symptoms with IBD: Anemia, delayed growth, eye conditions, fever, skin irritation, and weight loss
Differences: Differences: Related ConditionsRelated Conditions
Intestinal Symptoms IBS Crohn’s Disease Ulcerative Colitis
Anxiety Yes Yes Yes
Depression Yes Yes Yes
Fibromyalgia Yes Yes Yes
Urinary Yes Yes Yes
Arthritis Yes Yes
Colon Cancer Yes Yes
Hepatic Yes Yes
Osteoporosis Yes Yes
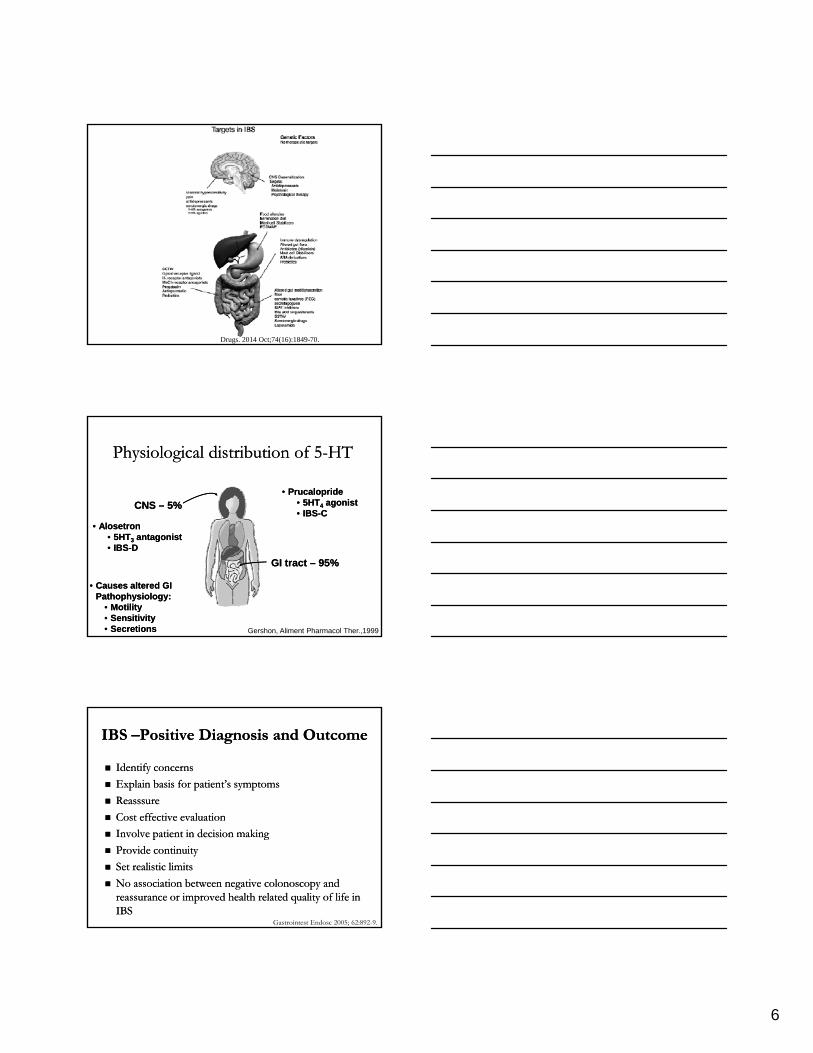
IBSIBSPathophysiologyPathophysiology
Disturbed Disturbed GI GI motilitymotility
VVisceral hypersensitivityisceral hypersensitivity
Psychological stressPsychological stress
Altered levels of 5HTAltered levels of 5HT 5HT3 and 5HT4 are extensively found in the gut, 5HT3 and 5HT4 are extensively found in the gut,
responsible for secretion, sensitization, and motilityresponsible for secretion, sensitization, and motility
IIntestinal ntestinal microfloramicroflora and inflammationand inflammation
6
Drugs. 2014 Oct;74(16):1849-70.
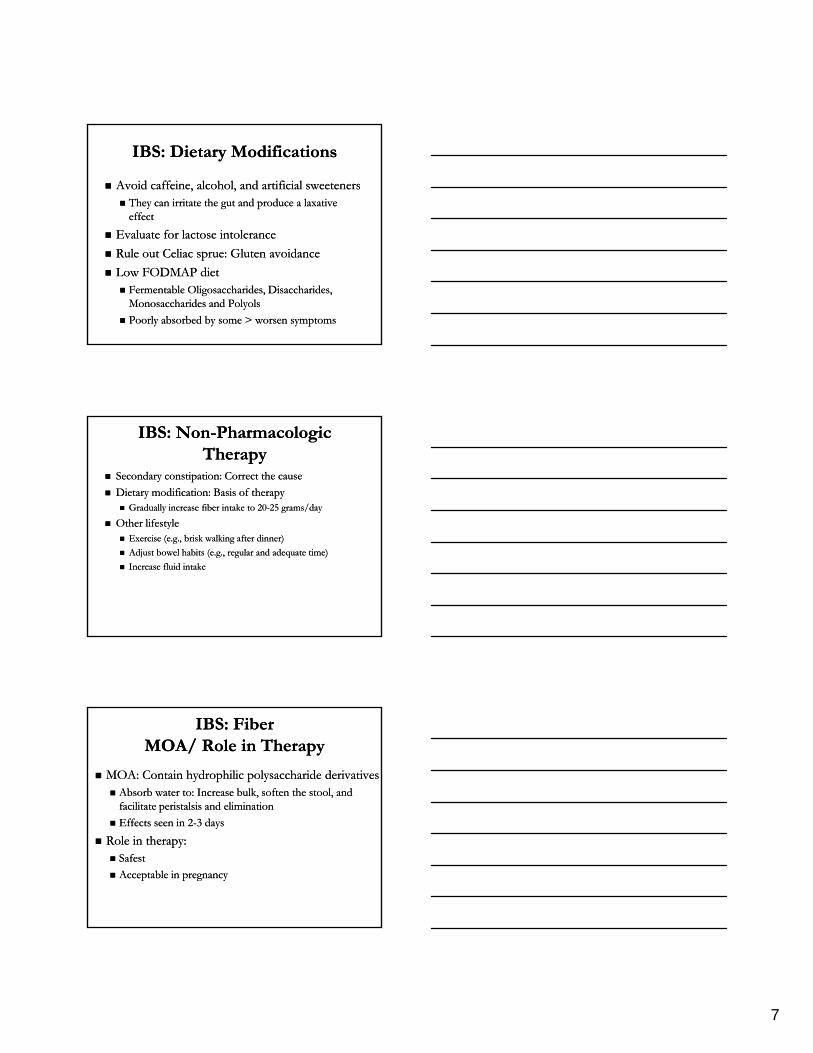
Physiological distribution of 5Physiological distribution of 5--HTHT
CNS CNS –– 5%5%
•• AlosetronAlosetron
•• PrucalopridePrucalopride•• 5HT5HT44 agonist agonist •• IBSIBS--CC
•• AlosetronAlosetron•• 5HT5HT33 antagonist antagonist •• IBSIBS--DD
GI tract GI tract –– 95%95%
Gershon, Aliment Pharmacol Ther.,1999
•• Causes altered GI Causes altered GI Pathophysiology:Pathophysiology:
•• MotilityMotility•• SensitivitySensitivity•• SecretionsSecretions
IBS IBS ––Positive Diagnosis and OutcomePositive Diagnosis and Outcome
Identify concernsIdentify concerns
Explain basis for patient’s symptomsExplain basis for patient’s symptoms
ReasssureReasssure
Cost effective evaluationCost effective evaluation Cost effective evaluationCost effective evaluation
Involve patient in decision makingInvolve patient in decision making
Provide continuityProvide continuity
Set realistic limitsSet realistic limits
No association between negative colonoscopy and No association between negative colonoscopy and reassurance or improved health related quality of life in reassurance or improved health related quality of life in IBSIBS
Gastrointest Endosc 2005; 62:892-9.
7
IBS: Dietary ModificationsIBS: Dietary Modifications
Avoid caffeine, alcohol, and artificial sweetenersAvoid caffeine, alcohol, and artificial sweeteners They can irritate the gut and produce a laxative They can irritate the gut and produce a laxative
effecteffect
Evaluate for lactose intoleranceEvaluate for lactose intolerance Evaluate for lactose intoleranceEvaluate for lactose intolerance
Rule out Celiac Rule out Celiac spruesprue: Gluten avoidance: Gluten avoidance
Low FODMAP dietLow FODMAP diet FermentableFermentable OligosaccharidesOligosaccharides, , DisaccharidesDisaccharides, ,
MonosaccharidesMonosaccharides and and PolyolsPolyols
PPoorly absorbed by some > worsen symptoms oorly absorbed by some > worsen symptoms
IBS: IBS: NonNon--Pharmacologic Pharmacologic TherapyTherapy
Secondary constipation: Correct Secondary constipation: Correct the causethe cause
Dietary modification: Basis of therapyDietary modification: Basis of therapy Gradually increase fiber intake to 20Gradually increase fiber intake to 20--25 grams/day25 grams/day
Other lifestyleOther lifestyleOther lifestyleOther lifestyle Exercise (e.g., brisk walking after dinner)Exercise (e.g., brisk walking after dinner)
Adjust bowel habits (e.g., regular and adequate time)Adjust bowel habits (e.g., regular and adequate time)
Increase fluid intake Increase fluid intake
IBS: FiberIBS: FiberMOA/ Role in TherapyMOA/ Role in Therapy
MOA: Contain hydrophilic polysaccharide derivativesMOA: Contain hydrophilic polysaccharide derivatives Absorb water to: Increase bulk, soften the stool, and Absorb water to: Increase bulk, soften the stool, and
facilitate peristalsis and eliminationfacilitate peristalsis and elimination
Effects seen in 2Effects seen in 2--3 days3 days
Role in therapy: Role in therapy: Safest Safest
Acceptable in pregnancyAcceptable in pregnancy
8
IBS: FiberIBS: FiberAgents and Availability Agents and Availability
AgentsAgents Methylcellulose (Citrucel)Methylcellulose (Citrucel)
Calcium Calcium PolycarbophilPolycarbophil ((FiberConFiberCon))
PsylliumPsyllium (Metamucil)(Metamucil)
Barley malt extract (Barley malt extract (MaltsupexMaltsupex))
Available as powders, flakes, granules, tablets, and liquidsAvailable as powders, flakes, granules, tablets, and liquids
Caution in diabetes due to glucose contentCaution in diabetes due to glucose content
Doses vary, typically administered in divided doses Doses vary, typically administered in divided doses
IBS: FiberIBS: FiberAdverse Effects/Drug InteractionsAdverse Effects/Drug Interactions Adverse effectsAdverse effects
Abdominal distention, cramping, and flatulenceAbdominal distention, cramping, and flatulence Minimized by gradual increase, resolved with continued useMinimized by gradual increase, resolved with continued use
Drug InteractionsDrug Interactions Possible binding to Possible binding to digoxindigoxin and warfarinand warfarin
Calcium Calcium polycarbophilpolycarbophil may bind with may bind with tetracyclinestetracyclines
Separate bulkSeparate bulk--forming agents by 1forming agents by 1--2 hours of other medications2 hours of other medications
CautionCaution Inappropriate for patients who must severely restrict fluid intakeInappropriate for patients who must severely restrict fluid intake
May cause May cause hypersentitivityhypersentitivity
Danger of fecal impaction or intestinal obstructionDanger of fecal impaction or intestinal obstruction Avoid in patients with intestinal ulcerations, Avoid in patients with intestinal ulcerations, stenosisstenosis, or disabling adhesions, or disabling adhesions
IBS: FiberIBS: FiberEvidenceEvidence
PsylliumPsyllium//ispaghulaispaghula husk showed improvement over husk showed improvement over placeboplacebo NNT=6 (IBS type not differentiated)NNT=6 (IBS type not differentiated)
Other agents are similar to placeboOther agents are similar to placebog pg p PsylliumPsyllium/ispaghula husk (20/ispaghula husk (20--30 g/day) improves 30 g/day) improves
constipationconstipation
Recommend BulkRecommend Bulk--forming agents for IBSforming agents for IBS--CC
Drugs. 2014 Oct;74(16):1849-70.
9
IBS: IBS: AntispasmodicsAntispasmodics//AnticholinergicsAnticholinergics MOA: Relax smooth muscles in the colon and MOA: Relax smooth muscles in the colon and
small bowel small bowel
Symptomatic relief Symptomatic relief –– PainPain
A P i ilA P i il h ih i i ii i Agents: Peppermint oil, Agents: Peppermint oil, hyoscinehyoscine, , cimetropiumcimetropium, , pinaveriumpinaverium, , mebeverinemebeverine, and , and otiloniumotilonium
Side Side effectseffects: Anticholinergic, generally safe: Anticholinergic, generally safe
Drugs. 2014 Oct;74(16):1849-70.
IBS: AntidepressantsIBS: Antidepressants
MOA: Improve MOA: Improve dysregulationdysregulation of of neuroentericneuroenteric pathway pathway
Symptomatic Symptomatic treatment: Abdominal treatment: Abdominal painpain
Reserved Reserved for patients with severe for patients with severe or or refractory refractory painpain
Visceral analgesia, changes in motility, smooth muscle relaxationVisceral analgesia, changes in motility, smooth muscle relaxationg , g y,g , g y,
Agents: Paroxetine, fluoxetine, citalopram, Agents: Paroxetine, fluoxetine, citalopram, amitryptilineamitryptiline, and , and imipramineimipramine
Adverse effects (antibiotic dependent): insomnia, restlessness, sexual Adverse effects (antibiotic dependent): insomnia, restlessness, sexual dysfunction, nausea, constipation, diarrheadysfunction, nausea, constipation, diarrhea
Drugs. 2014 Oct;74(16):1849-70.
IBS: ProbioticsIBS: Probiotics
MOA: restore normal floraMOA: restore normal flora Alterations may causeAlterations may cause
Increased fermentation of food Increased fermentation of food
Changes in intestinal motor and sensory function,Changes in intestinal motor and sensory function,Changes in intestinal motor and sensory function, Changes in intestinal motor and sensory function,
MMucosal immune activationucosal immune activation
Malabsorption Malabsorption
Multiple agents studiedMultiple agents studied Lactobacillus, Lactobacillus, bifidobacteriumbifidobacterium, streptococcus, streptococcus
Limitations in clinical trialsLimitations in clinical trials
Generally safeGenerally safe
10
IBSIBS--D: D: LoperamideLoperamide
EEvaluated in randomized controlled trialsvaluated in randomized controlled trials
Effective for treatment of diarrheaEffective for treatment of diarrhea
No impact on abdominal bloating or global IBS No impact on abdominal bloating or global IBS symptomssymptoms
ACG Task Force on IBS. Am J Gastro. 2009
IBSIBS--D: AlosetronD: AlosetronMOA/AgentMOA/Agent
MOA: Potent and selective MOA: Potent and selective 55--HTHT33 antagonist antagonist Results in modulation of the enteric nervous Results in modulation of the enteric nervous systmsystm
Alosetron (Alosetron (LotronexLotronex))A d i h iA d i h i IBSIBS DD f i hf i h Approved in chronicApproved in chronic, severe IBS, severe IBS--D D for patients who for patients who failed to responded failed to responded to conventional to conventional treatmentstreatments
Starting dose: 0.5mg BIDStarting dose: 0.5mg BID
Reassess at 4 weeksReassess at 4 weeks No adequate control of symptoms: Increase to 1mg BIDNo adequate control of symptoms: Increase to 1mg BID
ReRe--assess at 4 weeksassess at 4 weeks No adequate control of symptoms: Discontinue medicationNo adequate control of symptoms: Discontinue medication
IBSIBS--D: D: AlosetronAlosetronRestricted Use/PrecautionsRestricted Use/Precautions
Adverse effects (dose related)Adverse effects (dose related) Constipation Constipation
GI discomfort/painGI discomfort/pain
Restricted useRestricted use Restricted useRestricted use
FFemales onlyemales only
Enroll in Prometheus prescribing programEnroll in Prometheus prescribing program
IIschemic colitis (FDA warning)schemic colitis (FDA warning)
1.1 cases/1,000 patient1.1 cases/1,000 patient--yearsyears
Precautions: Constipation, ischemic colitisPrecautions: Constipation, ischemic colitis
Chang L et al. Am J Gastro 2010
11
IBSIBS--D: D: AlosetronAlosetronContraindicationsContraindications
CConstipationonstipation
intestinal intestinal obstruction, stricture, toxic obstruction, stricture, toxic megacolonmegacolon, , gastrointestinal perforation, and/or adhesionsgastrointestinal perforation, and/or adhesions
Ischemic Ischemic colitis, impaired intestinal circulation, colitis, impaired intestinal circulation, thrombophlebitis, or thrombophlebitis, or hypercoagulablehypercoagulable statestate
Crohn's disease or ulcerative colitisCrohn's disease or ulcerative colitis
DiverticulitisDiverticulitis
Severe Severe hepatic impairmenthepatic impairment
Concomitant fluvoxamine useConcomitant fluvoxamine use
IBSIBS--D: RifaximinD: Rifaximin
Broad spectrum antibiotic with low bioavailabilityBroad spectrum antibiotic with low bioavailability <0.4% absorbed<0.4% absorbed
Not FDA approvedNot FDA approved
Dose: 550mg BIDDose: 550mg BID TID for 2 weeksTID for 2 weeks Dose: 550mg BIDDose: 550mg BID--TID for 2 weeks TID for 2 weeks Improvement shown in up to 10 weeksImprovement shown in up to 10 weeks
Showed to improve global IBS symptomsShowed to improve global IBS symptoms TARGET 1 and 2 trialsTARGET 1 and 2 trials
Adverse effects: Flatulence, abdominal pain, Adverse effects: Flatulence, abdominal pain, tenesmustenesmus, fecal incontinence, nausea, and headaches, fecal incontinence, nausea, and headaches
IBSIBS--C: Osmotic LaxativesC: Osmotic LaxativesMOA/ Role in TherapyMOA/ Role in Therapy
MOA: Osmotic agent, causes water retention in the MOA: Osmotic agent, causes water retention in the stool and increases stool frequencystool and increases stool frequency Not absorbed systemicallyNot absorbed systemically
Onset 1Onset 1--4 days4 days
Role in therapyRole in therapy Low doses for constipationLow doses for constipation
Bowel cleansing before diagnostic or colorectal proceduresBowel cleansing before diagnostic or colorectal procedures
Safe use chronically, studied in up to 6 monthsSafe use chronically, studied in up to 6 months
Other names: PEGOther names: PEG
12
IBSIBS--C: Osmotic LaxativesC: Osmotic LaxativesAgentsAgents
AgentsAgents Polyethylene Glycol 3350 (Polyethylene Glycol 3350 (MiralaxMiralax))
Prescription onlyPrescription only
Available with and without electrolytesAvailable with and without electrolytes Available with and without electrolytesAvailable with and without electrolytes
Constipation Constipation 1010––30 g or 1730 g or 17––34 g per 12034 g per 120––240 240 mLmL QD or BID QD or BID
Also used for Also used for bbowel prepsowel preps
IBSIBS--C: Osmotic Laxatives:C: Osmotic Laxatives:Side Effects/ PrecautionsSide Effects/ Precautions
Side effectsSide effects Bloating, abdominal discomfort, cramping, flatulenceBloating, abdominal discomfort, cramping, flatulence
PrecautionsPrecautions LavageLavage is NOT recommended for routine treatment of is NOT recommended for routine treatment of
constipationconstipation
ContraindicationContraindication GI obstructionGI obstruction
IBSIBS--C: Chloride Channel ActivatorC: Chloride Channel ActivatorLubiprostoneLubiprostone-- MOA/ AgentMOA/ Agent
MOA: Chloride channel activatorMOA: Chloride channel activator Open chloride channels locally on the GI luminal epitheliumOpen chloride channels locally on the GI luminal epithelium
Stimulates chlorideStimulates chloride--rich fluid secretion into the lumenrich fluid secretion into the lumen
Results in softening of the stool and increased motility Results in softening of the stool and increased motility
Onset: 24Onset: 24--48 hours48 hours
Agent: Agent: LubiprostoneLubiprostone ((AmitizaAmitiza) ) Rx onlyRx only
Approved to treat chronic constipation in adultsApproved to treat chronic constipation in adults
Constipation: 24mcg BID with foodConstipation: 24mcg BID with food
Approved for IBSApproved for IBS--C: C: 8 mcg BID with food8 mcg BID with food
13
IBSIBS--C: Chloride Channel ActivatorC: Chloride Channel ActivatorLubiprostoneLubiprostone-- Role in Therapy/ Adverse EffectsRole in Therapy/ Adverse Effects
Role in therapyRole in therapy Chronic constipation in those who fail firstChronic constipation in those who fail first--line agentsline agents
Adverse effects Adverse effects Nausea (dose dependent), diarrhea, abdominal pain, Nausea (dose dependent), diarrhea, abdominal pain,
flatulence, headaches, dyspneaflatulence, headaches, dyspnea
Pregnancy (category C)Pregnancy (category C)
ContraindicationContraindication GI obstructionGI obstruction
IBSIBS--C: Guanylate CyclaseC: Guanylate Cyclase--C C agonisagonisttLinaclotideLinaclotide-- MOA/ AgentsMOA/ Agents
MOA: MOA: GuanylateGuanylate cyclasecyclase--C agonistC agonist Act on the luminal surface of the intestinal epitheliumAct on the luminal surface of the intestinal epithelium
Stimulates the secretion of chloride and bicarbonate into the Stimulates the secretion of chloride and bicarbonate into the intestinal lumenintestinal lumen
Results in increased intestinal fluid and accelerated GI transitResults in increased intestinal fluid and accelerated GI transit
Decreased visceral pain Decreased visceral pain
Agent: Agent: LinaclotideLinaclotide ((LinzessLinzess))-- Approved in August 2012Approved in August 2012
Chronic Constipation: 145 mcg PO QD on an empty stomach Chronic Constipation: 145 mcg PO QD on an empty stomach at least 30 minutes prior to the first meal of the dayat least 30 minutes prior to the first meal of the day
Approved for IBSApproved for IBS--C: 290mcg PO C: 290mcg PO QD on an empty stomach QD on an empty stomach at least 30 minutes prior to the first meal of the dayat least 30 minutes prior to the first meal of the day
IBSIBS--C: Guanylate CyclaseC: Guanylate Cyclase--C C agonisagonisttSide Effects/ ContraindicationsSide Effects/ Contraindications
Side effects:Side effects: Diarrhea, abdominal pain, flatulenceDiarrhea, abdominal pain, flatulence
P t CP t C Pregnancy category CPregnancy category C
ContraindicatedContraindicated GI obstructionGI obstruction
Children <6 years oldChildren <6 years old

14
IBSIBS--C: Serotonin AgonistsC: Serotonin AgonistsPrucalopridePrucalopride
MOAMOA Selective Selective high affinity 5high affinity 5--HTHT44
receptor agonistreceptor agonist
Promotes enteric neurons toPromotes enteric neurons to
SafetySafety TegaserodTegaserod-- withdrawn from the withdrawn from the
market due to CV adverse market due to CV adverse events likely due to its actions events likely due to its actions
Promotes enteric neurons to Promotes enteric neurons to stimulate the peristaltic reflex, stimulate the peristaltic reflex, intestinal secretions, and GI intestinal secretions, and GI motility motility
AgentsAgents PrucalopridePrucalopride-- Not available in Not available in
USA, available in EuropeUSA, available in Europe
yyon on hERGhERG channel channel
Prucalopride: no actions on Prucalopride: no actions on hERGhERG channel and higher channel and higher affinity to affinity to --5HT5HT44
PrucalopridePrucalopride has been safely has been safely tolerated in clinical trialstolerated in clinical trials No adverse CV effects compared No adverse CV effects compared
to placeboto placebo
Treatment AlgorithmTreatment Algorithm
Symptomatic treatment
Stress management and patient educations
Symptomatic treatment
Stress management and patient educations
Constipation PredominantConstipation Predominant Diarrhea PredominantDiarrhea Predominant
Di t L t f nd ff in fr di tDi t L t f nd ff in fr di tIncrease: Fiber and Liquid intakeIncrease: Fiber and Liquid intake
Add bulk-forming laxatives, consider antispasmodic agentsAdd bulk-forming laxatives,
consider antispasmodic agents
Add 5HT-4 agonists (prucalopride) or
guanylate cyclase-c agonist (linaclotide)
Add 5HT-4 agonists (prucalopride) or
guanylate cyclase-c agonist (linaclotide)
Diet: Lactose-fee and caffeine-free diet, avoid other diarrhea causing agents
Diet: Lactose-fee and caffeine-free diet, avoid other diarrhea causing agents
Add loperamide or antispasmodic agentsAdd loperamide or antispasmodic agents
Add 5HT-3 antagonists (alosetron)
Add 5HT-3 antagonists (alosetron)
Add psychotherapeutic behavior modifications, consider antidepressants
Add psychotherapeutic behavior modifications, consider antidepressants
Drugs. 2014 Oct;74(16):1849-70.
Altered Bowel Motility
Pain:Antispasmodics
Altered Bowel Motility: IBS-DRifaximin, loperamide, 5HT3 receptor antagonistsEmerging Therapies:•Bile acid sequestrants•Crofelemer•ASA derivatives
Altered Bowel Motility: IBS-CPsyllium, osmotic laxatives (PEG), sorbitol/lactulose, lubiprostone, linaclotide, 5HT4 receptor agonists, STW5Emerging Therapies•IBAT
BloatingPain
Antispasmodics, antidepressants, probiotics, STW5, melatoninEmerging Therapies•Mixed visceral Mu-opioid •Receptor agonists/antagonists, •Pregabalin•Selective visceral K opioid receptor agonist•H1 receptor antagonists•NK receptor antagonists
Bloating:Antispasmodics, antiflatulents, probiotics, linaclotide, rifaximin, antidepressants: citalopram, fluxoetineDrugs. 2014 Oct;74(16):1849-70.

15
IBD: Pharmacologic TreatmentsIBD: Pharmacologic Treatments
AminosalicylatesAminosalicylates
CorticosteroidsCorticosteroids
ImmunosuppressantsImmunosuppressants
AntimicrobialsAntimicrobials
BiologicsBiologics TNFTNFαα inhibitorsinhibitors
Inhibitors of leukocyte adhesion/migrationInhibitors of leukocyte adhesion/migration
Ulcerative Colitis: ClassificationUlcerative Colitis: Classification
Mild: <4 stools/day, no systemic disturbance, Mild: <4 stools/day, no systemic disturbance, normal ESRnormal ESR
Moderate: >4 stools/day, minimal systemic Moderate: >4 stools/day, minimal systemic dist rbancedist rbancedisturbancedisturbance
Severe: >6 stools/day with blood, evidence of Severe: >6 stools/day with blood, evidence of systemic disturbance (fever, tachycardia, anemiasystemic disturbance (fever, tachycardia, anemia, , or or ESR of greater than 30 mm/h (8.3 ESR of greater than 30 mm/h (8.3 μmμm/s/s))
Fulminant: >10 stools/day, bleeding, toxicity, Fulminant: >10 stools/day, bleeding, toxicity, abdominal tendernessabdominal tenderness, requirement for , requirement for transfusion, and colonic dilationtransfusion, and colonic dilation
Crohn’s Disease: ClassificationCrohn’s Disease: Classification
Mild/moderate: Ambulatory, no evidence of Mild/moderate: Ambulatory, no evidence of dehydration, toxicity, loss of weight, or abdominal dehydration, toxicity, loss of weight, or abdominal tenderness, mass, or obstructiontenderness, mass, or obstruction
Moderate/ severe: Fail to respond to treatment for Moderate/ severe: Fail to respond to treatment for mild/ moderate OR fever weight loss abdominalmild/ moderate OR fever weight loss abdominalmild/ moderate OR fever, weight loss, abdominal mild/ moderate OR fever, weight loss, abdominal pain, vomiting, intestinal obstruction, or significant pain, vomiting, intestinal obstruction, or significant anemiaanemia
Severe/fulminant: Persistent symptoms OR Severe/fulminant: Persistent symptoms OR systemic toxicity despite corticosteroid or biologic systemic toxicity despite corticosteroid or biologic therapy, or presence of cachexia, rebound therapy, or presence of cachexia, rebound tenderness, obstruction, or abscesstenderness, obstruction, or abscess
Disease activity is correlated with CRPDisease activity is correlated with CRP

16
IBD: IBD: AminosalicylatesAminosalicylatesMOA and AgentsMOA and Agents
MOA: Specific mechanism is unknownMOA: Specific mechanism is unknown Thought to modulate chemical mediators of Thought to modulate chemical mediators of
inflammation or act as a inflammation or act as a ffree radical scavenger or ree radical scavenger or inhibitor of tumor necrosis factorinhibitor of tumor necrosis factor
A tA t AgentsAgents MesalamineMesalamine ((AsacolAsacol, , DDelzicolelzicol, , LialdaLialda, , PentasaPentasa), ),
sulfasalazine, sulfasalazine, balsalazidebalsalazide, , olsalazineolsalazine MesalamineMesalamine doses >3g/day in UCdoses >3g/day in UC
Place in therapy: Mild/moderate IBDPlace in therapy: Mild/moderate IBD OffOff--label for Crohn’s Diseaselabel for Crohn’s Disease
IBD: IBD: AminosalicylatesAminosalicylatesAdverse effectsAdverse effects and Precautionsand Precautions
Adverse effects:Adverse effects: Nausea, dyspepsia, skin rash, headache, abdominal Nausea, dyspepsia, skin rash, headache, abdominal
painpain
Occur in 45% of patients with sulfasalazine and 15%Occur in 45% of patients with sulfasalazine and 15% Occur in 45% of patients with sulfasalazine and 15% Occur in 45% of patients with sulfasalazine and 15% of patients with of patients with mesalaminemesalamine
ContraindicationsContraindications (sulfasalazine): sulfa allergy, (sulfasalazine): sulfa allergy, intestinal or urinary obstruction, porphyriaintestinal or urinary obstruction, porphyria
Warnings: Hepatic or renal impairmentWarnings: Hepatic or renal impairment
IBD: CorticosteroidsIBD: CorticosteroidsMOA and AgentsMOA and Agents
MOA: Suppress cytokine migration modulating MOA: Suppress cytokine migration modulating the immune system and decreasing inflammationthe immune system and decreasing inflammation
Agents: budesonide prednisone, prednisoloneAgents: budesonide prednisone, prednisoloneB d id P l b b d li i d i iB d id P l b b d li i d i i Budesonide: Poorly absorbed, limited toxicityBudesonide: Poorly absorbed, limited toxicity
Regimens varyRegimens vary Many wean therapy by decreasing 5mg/day at Many wean therapy by decreasing 5mg/day at
weekly intervalsweekly intervals
Place in therapy: Induce remission in IBDPlace in therapy: Induce remission in IBD

17
IBD: CorticosteroidsIBD: CorticosteroidsAdverse Effects and PrecautionsAdverse Effects and Precautions Adverse effects: Adverse effects: many, edema, CV affects, many many, edema, CV affects, many
endocrine and metabolic effects i.e. adrenal endocrine and metabolic effects i.e. adrenal suppression and hyperglycemiasuppression and hyperglycemia
Preca tions: Heart fail re hypertension MIPreca tions: Heart fail re hypertension MI Precautions: Heart failure, hypertension, MI, Precautions: Heart failure, hypertension, MI, hepatic impairment, osteoporosis, thyroid hepatic impairment, osteoporosis, thyroid disease, and advanced agedisease, and advanced age
Drug interactions: care when combining more Drug interactions: care when combining more than one immunosuppressant drug than one immunosuppressant drug ––contraindicated with Natalizumab, may increase contraindicated with Natalizumab, may increase toxic effects of NSAIDStoxic effects of NSAIDS
IBD: IBD: ThiopurinesThiopurinesMOA and AgentsMOA and Agents
MOA: Induce TMOA: Induce T--cell apoptosis by modulating cell apoptosis by modulating cell signalingcell signaling
Agents: Agents: A hi iA hi i (AZA) 1 5(AZA) 1 5 2 5 /k /d2 5 /k /d llll Azathioprine Azathioprine (AZA) 1.5(AZA) 1.5--2.5mg/kg/day 2.5mg/kg/day orallyorally
MercaptopurineMercaptopurine (MP) (MP) 1.51.5--2.5mg/kg/day orally2.5mg/kg/day orally
Place in therapy: Adjunctive in IBDPlace in therapy: Adjunctive in IBD OffOff--labellabel
Test for Test for thiopurinethiopurine methyl methyl transferasetransferasepolymorphism polymorphism
IBD: IBD: ThiopurinesThiopurinesAdverse Effects and PrecautionsAdverse Effects and Precautions Adverse effects (20% of patients): Fever, arthralgia, rashAdverse effects (20% of patients): Fever, arthralgia, rash
Typically occur in 2Typically occur in 2--3 weeks, cease when medication is 3 weeks, cease when medication is withdrawnwithdrawn
LongLong--term benefit can be expected if tolerated for 3 weeksterm benefit can be expected if tolerated for 3 weeks
Precaution: Precaution: GI toxicity, hepatotoxicity, infections, hematologic toxicityGI toxicity, hepatotoxicity, infections, hematologic toxicity
Malignancy:Malignancy:
Risk of nonRisk of non--melanoma skin cancer, melanoma skin cancer, lymphoproliferativelymphoproliferativedisorders (1% risk with 10 years)disorders (1% risk with 10 years)
Contraindication (AZA): Pregnancy (RA), RA and Contraindication (AZA): Pregnancy (RA), RA and treatment with alkylating agentstreatment with alkylating agents
18
IBD: MethotrexateIBD: MethotrexateMOA and AgentMOA and Agent
MOA: Inhibits MOA: Inhibits dihydrofolatedihydrofolate reductasereductase, cytokine, , cytokine, and eicosanoid synthesisand eicosanoid synthesis
Methotrexate (MTX)15Methotrexate (MTX)15--25mg 25mg weekly weekly IM/IV/orallyIM/IV/orally
Place in therapy: SecondPlace in therapy: Second--line in patients resistant line in patients resistant or tolerant to AZA or MP (offor tolerant to AZA or MP (off--label)label)
IBD: MethotrexateIBD: MethotrexateAdverse Effects and PrecautionsAdverse Effects and Precautions
Adverse Effects (27Adverse Effects (27--49%) d/c in 1049%) d/c in 10--25%25% Early: Nausea (co administer with folate to limit), Early: Nausea (co administer with folate to limit),
vomiting, diarrhea, and stomatitisvomiting, diarrhea, and stomatitis
Long term: Hepatotoxicity, pneumonitis, and infectionsLong term: Hepatotoxicity, pneumonitis, and infections
PrecautionsPrecautions Acute renal failure, bone marrow suppression, CNS, Acute renal failure, bone marrow suppression, CNS,
dermatologic, fertility, GI, hepatotoxicity, infections, dermatologic, fertility, GI, hepatotoxicity, infections, pneumonitis, secondary malignancy, and tumor pneumonitis, secondary malignancy, and tumor lysislysissyndromesyndrome
Contraindication: Pregnancy Contraindication: Pregnancy
IBD: CyclosporineIBD: Cyclosporine MOA: Inhibits MOA: Inhibits calcineurincalcineurin preventing the clonal preventing the clonal
expansion of T cell subsetsexpansion of T cell subsets
Cyclosporine 4mg/kg/day IVCyclosporine 4mg/kg/day IV
Place in therapy: Refractory in ulcerative colitis (offPlace in therapy: Refractory in ulcerative colitis (off--label)label)
No place in Crohn’s diseaseNo place in Crohn’s disease
Adverse effects (31Adverse effects (31--51%): tremor, malaise, paresthesia, 51%): tremor, malaise, paresthesia, headache, liver function abnormality, gingival headache, liver function abnormality, gingival hyperplasia, hyperplasia, hirsutismhirsutism
Precautions: Hypertension, malignancy and skin Precautions: Hypertension, malignancy and skin cancer, nephrotoxicity, infections, neurotoxicitycancer, nephrotoxicity, infections, neurotoxicity Not recommended in lactationNot recommended in lactation
19
IBD: AntiIBD: Anti--TNFTNFMOA and AgentMOA and Agent
MOA: Inhibits MOA: Inhibits dihydrofolatedihydrofolate reductasereductase, cytokine, , cytokine, and eicosanoid synthesisand eicosanoid synthesis
IBDIBD Infliximab (Infliximab (RemicadeRemicade) 5mg/kg at 0, 2, and 6 weeks ) 5mg/kg at 0, 2, and 6 weeks
followed by 5mg/kg every 8 weeks thereafterfollowed by 5mg/kg every 8 weeks thereafter
AdalimumabAdalimumab ((HumiraHumira) 40mg ) 40mg subQsubQ every other weekevery other week
Crohn’s DiseaseCrohn’s Disease CertolizumabCertolizumab ((CimziaCimzia): 400mg at 0, 2, and 4 followed by ): 400mg at 0, 2, and 4 followed by
400mg every 4 weeks 400mg every 4 weeks
NatalizumabNatalizumab ((TsyabriTsyabri)300mg IV every 4 weeks)300mg IV every 4 weeks
Place in therapy: Moderate/severe IBDPlace in therapy: Moderate/severe IBD
AntiAnti--TNFTNFAdverse Effects and PrecautionsAdverse Effects and Precautions
Baseline screening for TB requiredBaseline screening for TB required
Adverse Effects: Infections, infusion site reactions, Adverse Effects: Infections, infusion site reactions, autoimmunityautoimmunity
Precautions: Antibody formation, malignancy, Precautions: Antibody formation, malignancy, y , g y,y , g y,demyelination, congestive heart failuredemyelination, congestive heart failure NatalizumabNatalizumab should not be used with should not be used with immunosuppressantsimmunosuppressants or TNF or TNF
inhibitors and can cause inhibitors and can cause leukoencephalopathyleukoencephalopathy
Drug interactions: other biologics and Drug interactions: other biologics and immunosuppressantsimmunosuppressants, , may decrease effects of vaccinationsmay decrease effects of vaccinations
Contraindication (infliximab): heart failure (high doses)Contraindication (infliximab): heart failure (high doses)
IBD Complications: AntibioticsIBD Complications: Antibiotics
Treat secondary complications in IBDTreat secondary complications in IBD
Abscess and bacterial overgrowthAbscess and bacterial overgrowth MetronidazoleMetronidazole
Ci fl iCi fl i Ciprofloxacin Ciprofloxacin
RifaximinRifaximin
20
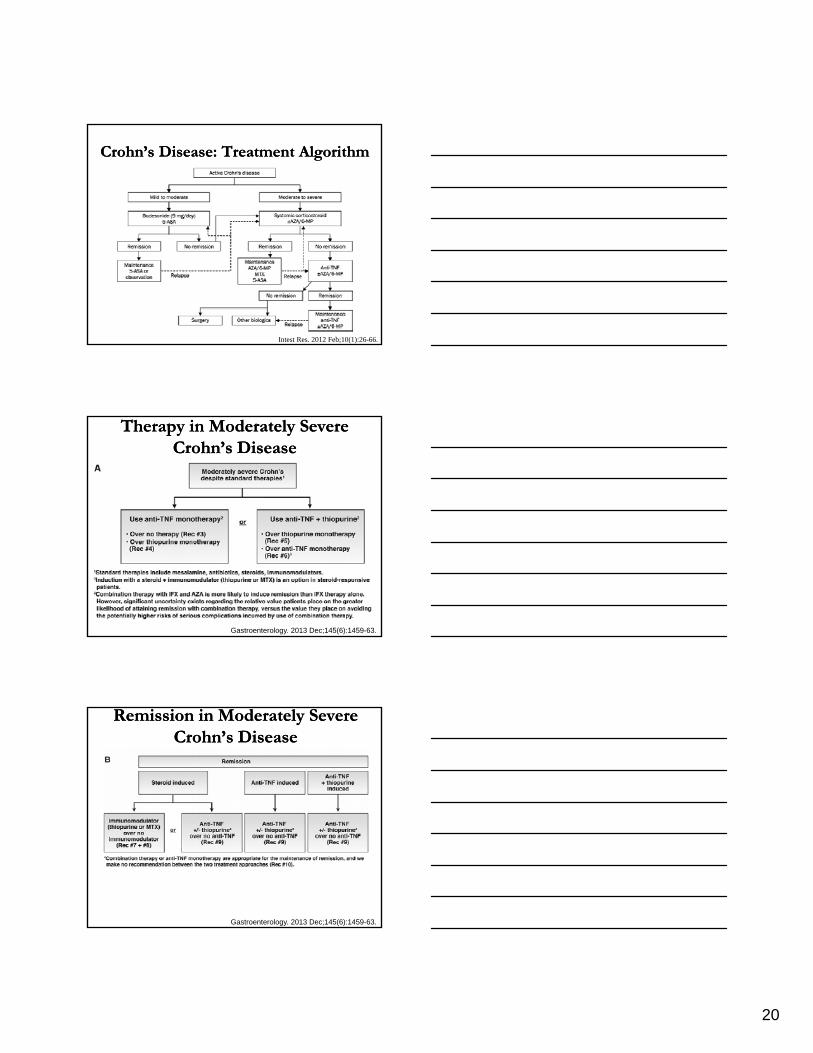
Crohn’s Disease: Treatment Algorithm Crohn’s Disease: Treatment Algorithm
Intest Res. 2012 Feb;10(1):26-66.
Therapy in Moderately Severe Therapy in Moderately Severe Crohn’s DiseaseCrohn’s Disease
Gastroenterology. 2013 Dec;145(6):1459-63.
Remission in Moderately Severe Remission in Moderately Severe Crohn’s DiseaseCrohn’s Disease
Gastroenterology. 2013 Dec;145(6):1459-63.
21
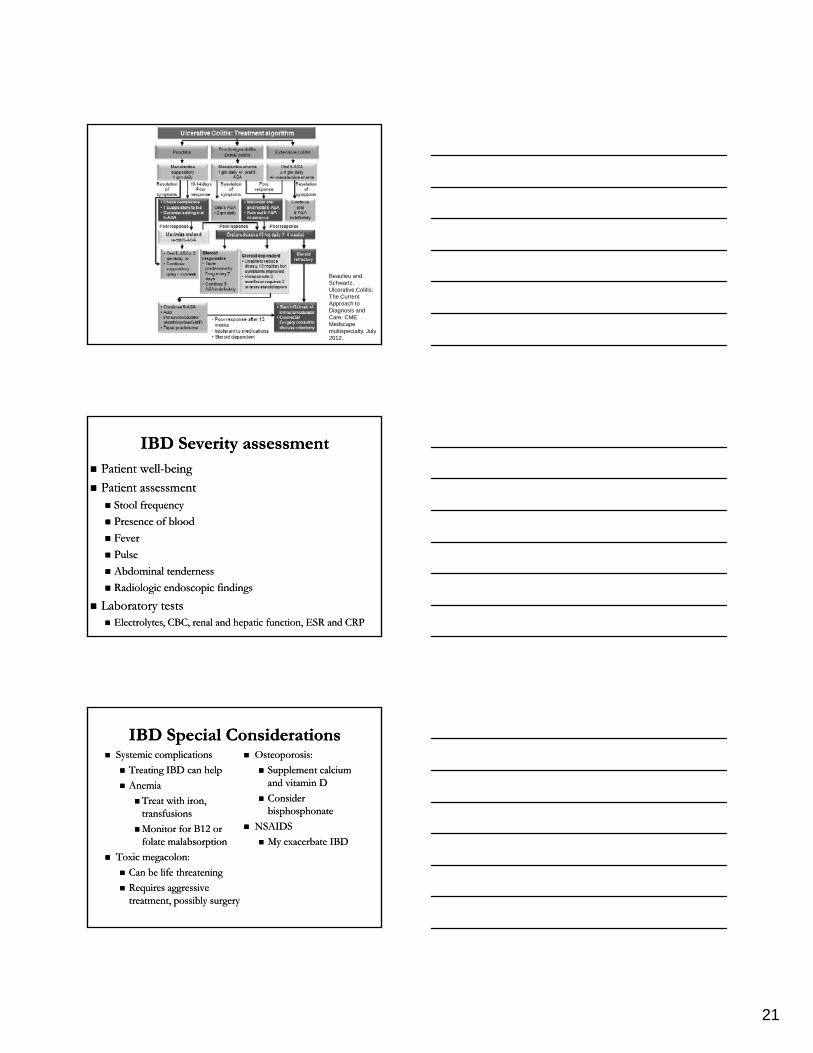
Beaulieu and Schwartz. Ulcerative Colitis: The Current Approach to Diagnosis and Care. CME Medscape multispecialty. July 2012.
IBD Severity assessmentIBD Severity assessment Patient wellPatient well--beingbeing
Patient assessmentPatient assessment Stool frequencyStool frequency
Presence of bloodPresence of blood
FeverFever
PulsePulse
Abdominal tendernessAbdominal tenderness
Radiologic endoscopic findingsRadiologic endoscopic findings
Laboratory testsLaboratory tests EElectrolyteslectrolytes, CBC, renal and hepatic function, ESR and CRP, CBC, renal and hepatic function, ESR and CRP
IBD Special ConsiderationsIBD Special Considerations Systemic complicationsSystemic complications
Treating IBD can helpTreating IBD can help
AnemiaAnemia
Treat with iron, Treat with iron, transfusionstransfusions
Osteoporosis: Osteoporosis:
Supplement calcium Supplement calcium and vitamin Dand vitamin D
Consider Consider bisphosphonatebisphosphonate
Monitor for B12 or Monitor for B12 or folate folate malabsorptionmalabsorption
Toxic Toxic megacolonmegacolon: :
Can be life threateningCan be life threatening
Requires aggressive Requires aggressive treatment, possibly surgerytreatment, possibly surgery
NSAIDSNSAIDS
My exacerbate IBDMy exacerbate IBD
22
SummarySummary IBS and IBD result in similar symptoms and can IBS and IBD result in similar symptoms and can
be difficult to managebe difficult to manage Diagnosis can be difficult Diagnosis can be difficult
IBS: Increased morbidityIBS: Increased morbidity
IBD: Increased morbidity and mortalityIBD: Increased morbidity and mortality
Cost of therapy can be highCost of therapy can be high
Monitor for medication adverse effects, Monitor for medication adverse effects, precautions, and contraindicationsprecautions, and contraindications
Questions?Questions?
[email protected]@health.usf.edu