whats the optimal pharmacological therapy after valve intervention
TRANSCRIPT

Optimal Pharmacological Therapy After Valve Intervention
JEFFREY S. BORER, M.D.Professor of Medicine, Cell Biology, Radiology and Surgery
Director, The Howard Gilman Institute for Heart Valve Disease and
The Schiavone Cardiovascular Translational Research Institute
Former Chairman, Department of Medicine
and Former Chief, Division of Cardiovascular Medicine
State University of New York Downstate Medical Center

Disclosures
• Consulting fees, Committee fees with– Servier– Amgen– Novartis– Cardiorentis– Pfizer– ARMGO– Takeda USA– Celladon– BioMARIN (stock)

UNDERLYING PRINCIPLES/ISSUES• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention

UNDERLYING PRINCIPLES/ISSUES• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Therefore, no specific drug regimen exists for post-intervention pts who had had low flow/low gradient AS

UNDERLYING PRINCIPLES/ISSUES• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Therefore, no specific drug regimen exists for post-intervention pts who had had low flow/low gradient AS
• BUT low flow/low gradient AS commonly is associated with many adversities common to other AS presentations (e.g., associated MR) and, after intervention, commonly is associated with additional adversities (e.g., paraprosthetic AR, etc.)

UNDERLYING PRINCIPLES/ISSUES• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Therefore, no specific drug regimen exists for post-intervention pts who had had low flow/low gradient AS
• BUT low flow/low gradient AS commonly is associated with many adversities common to other AS presentations (e.g., associated MR) and, after intervention, commonly is associated with additional adversities (e.g., paraprosthetic AR, etc.)
• Therefore, it is useful to discuss the general principles of selection of drug therapy after any valve intervention.
UNDERLYING PRINCIPLES/ISSUES• Use of drugs after a mechanical valve intervention primarily is a function of
– Type of procedure performed • Surgical
– Diuretics for removal of procedural fluid load – early: days to weeks– Other pre-op HF drugs if HF was present – early and as needed thereafter– Anticoagulant and antiplatelet agents
• Transcutaneous– pre-op HF drugs if HF was present – early and as needed thereafter– Anticoagulant and antiplatelet agents
• Repair– pre-op HF drugs if HF was present – early and as needed thereafter– Possibly anticoagulant and antiplatelet agents short-term
• Replacement– Pre-op HF drugs if HF was present – early and as needed thereafter– Bioprosthetic – possibly antiplatelet drugs, possibly short term anticoagulants– Mechanical – permanent anticoagulation (only warfarin at present – NOACs
contraindicated)
– Time after procedure at which drugs are to be given (<4 weeks post-op vs chronic)

UNDERLYING PRINCIPLES/ISSUES• Use of drugs after a mechanical valve intervention primarily is a function of
– Type of procedure performed • Surgical
– Diuretics for removal of procedural fluid load – early: days to weeks– Other pre-op HF drugs if HF was present – early and as needed thereafter– Anticoagulant and antiplatelet agents
• Transcutaneous– pre-op HF drugs if HF was present – early and as needed thereafter– Anticoagulant and antiplatelet agents
• Repair– pre-op HF drugs if HF was present – early and as needed thereafter– Possibly anticoagulant and antiplatelet agents short-term
• Replacement– Pre-op HF drugs if HF was present – early and as needed thereafter– Bioprosthetic – possibly antiplatelet drugs, possibly short term anticoagulants– Mechanical – permanent anticoagulation (only warfarin at present – NOACs
contraindicated)
– Time after procedure at which drugs are to be given (<4 weeks post-op vs chronic)

0
10
20
30
40
50
60
Pre-op <1 1-2 2-3 4-6
YEARS AFTER AVR
LV E
JEC
TIO
N F
RA
CTI
ON
(%)
0
NSNSNS
NSNS
p<.01p<.01
p<.05
NATURAL HISTORY OF LVEF AFTER AVR FOR AR:EFFECT OF DRUGS MAY VARY WITH CHANGING MYOCARDIUM
Borer et al, Circulation 1990

UNDERLYING PRINCIPLES/ISSUES
Use of drugs after a mechanical valve intervention primarily is a function of
– Hemodynamic success of the procedure (?residual stenosis or regurgitation?)
– Comorbidities that are likely to directly affect cardiac function (most important: hypertension; dysrhythmia)
– Residual symptom status (is there clinical heart failure?)
– Residual ventricular/myocardial function

Relative risk ratio for short-term mortality versus severity of valve prosthesis-patient mismatch
Claudia Blais et al. Circulation. 2003;108:983-988
Copyright © American Heart Association, Inc. All rights reserved.

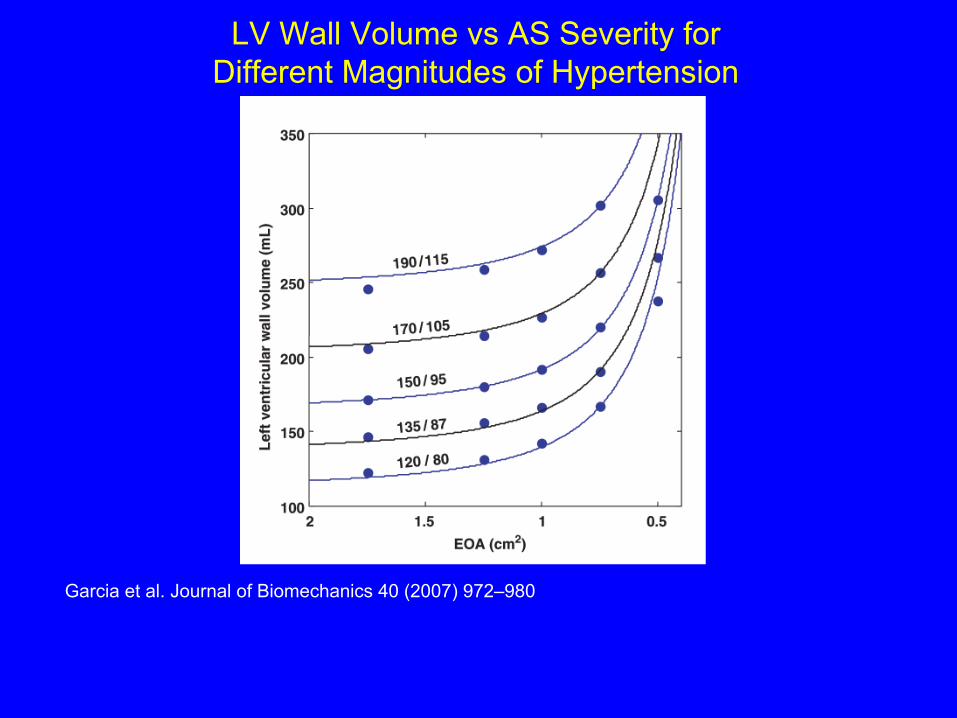
LV Wall Volume vs AS Severity for Different Magnitudes of Hypertension
Garcia et al. Journal of Biomechanics 40 (2007) 972–980
BUT no evidence that residual obstruction can be beneficiallyovercome with drugs; better to mechanically relieve obstruction
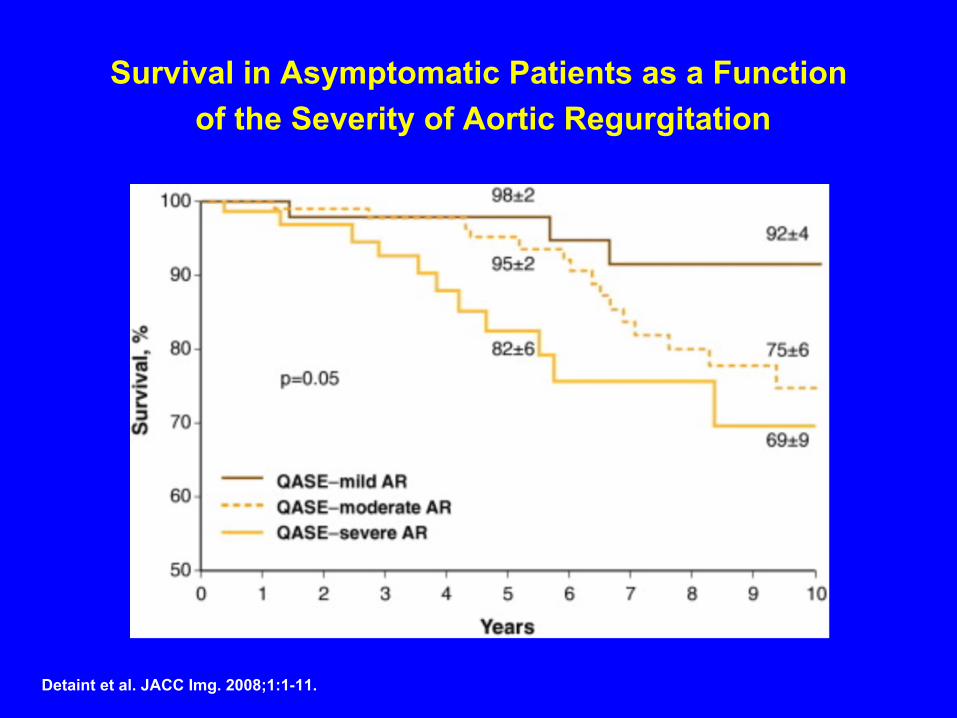
Survival in Asymptomatic Patients as a Function of the Severity of Aortic Regurgitation
Detaint et al. JACC Img. 2008;1:1-11.
Copyright © The American College of Cardiology. All rights reserved.
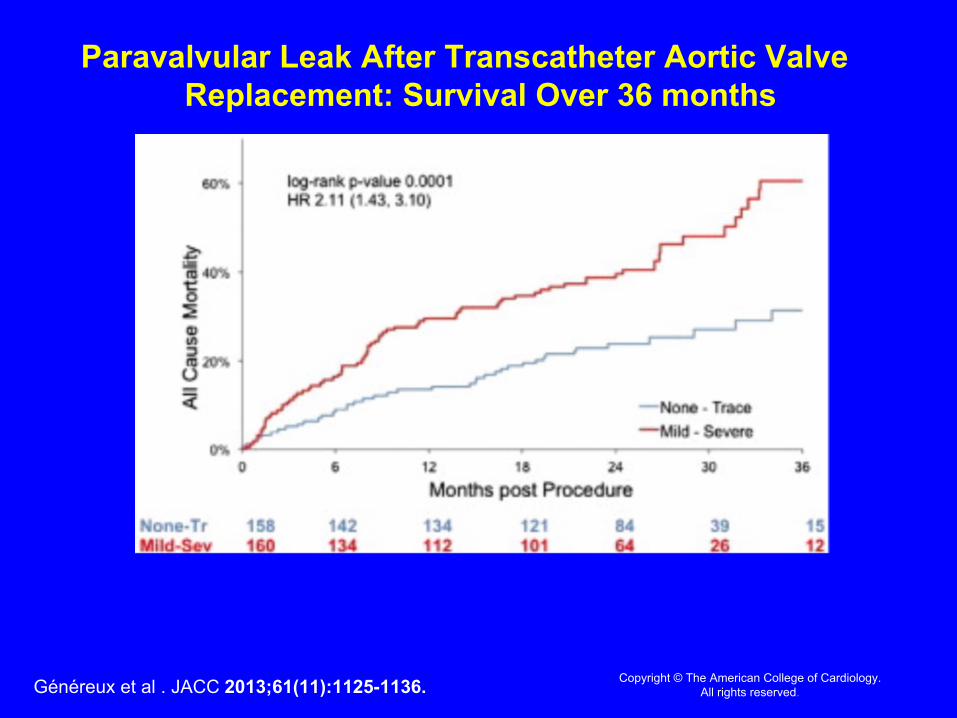
Paravalvular Leak After Transcatheter Aortic Valve Replacement: Survival Over 36 months
Généreux et al . JACC 2013;61(11):1125-1136.

CHRONIC VASODILATOR DRUG (VDD) USE vs. CARDIAC EVENTS
0 2 4 6 8 10 12Years After Study Entry
100
0102030405060708090
% C
ardi
ac E
vent
Fre
e No VDD: Avg Annual Risk = 3.99%
VDD : Avg Annual Risk = 17.46%
p = .0005
Supino, Borer, Herrold et al, AJC 2005
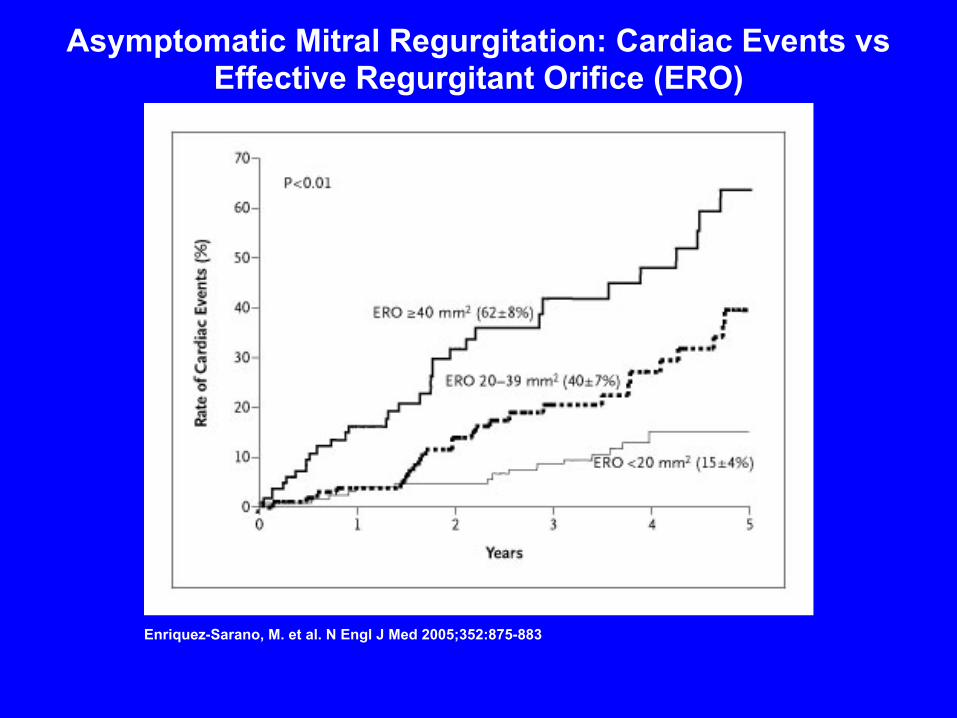
Enriquez-Sarano, M. et al. N Engl J Med 2005;352:875-883
Asymptomatic Mitral Regurgitation: Cardiac Events vs Effective Regurgitant Orifice (ERO)

Study, year Pts Drug ResultHeck et al 1985 10 Captopril Neg/neutralWisenbaugh et al l994
12 Captopril Neg/neutral
Schon et al 1994 12 Quinapril Neg/neutralSampaio et al 2005 47 Enalapril Neg (reduction in
anaerobic threshold at 12 months)
MR: “LONG-TERM” PHARMACOLOGICAL AFTERLOAD REDUCTION, n=81
(=included some symptomatic pts)
UNDERLYING PRINCIPLES/ISSUES
– Hemodynamic success of the procedure (?residual stenosis or regurgitation?)
– Comorbidities that are likely to directly affect cardiac function (most important: hypertension; dysrhythmia)
– Residual symptom status (is there clinical heart failure?)
– Residual ventricular/myocardial function

Clinical Risk Markers for Aortic Stenosis
Stewart et al. J Am Coll Cardiol 1997;29:630–4
BUT – though eventually there should be no difference between the myocardiumof a pt with prior AS and a person with hypertension without prior AS, as yet no evidence that treatment of hypertension after AVR for AS impactsbeneficially on outcome – or of when after AVR the treatment works well, or ifthere is a difference among effects of different antihypertensives
LV Wall Volume vs AS Severity for Different Magnitudes of Hypertension
Garcia et al. Journal of Biomechanics 40 (2007) 972–980

CARDIAC EVENT-FREE SURVIVAL IN CHRONIC SEVERE AR: IMPACT OF HYPERTENSION
(N=73)
p<.005, age/gender adjusted Supino, Borer, et al. Am J Cardiol. 2005
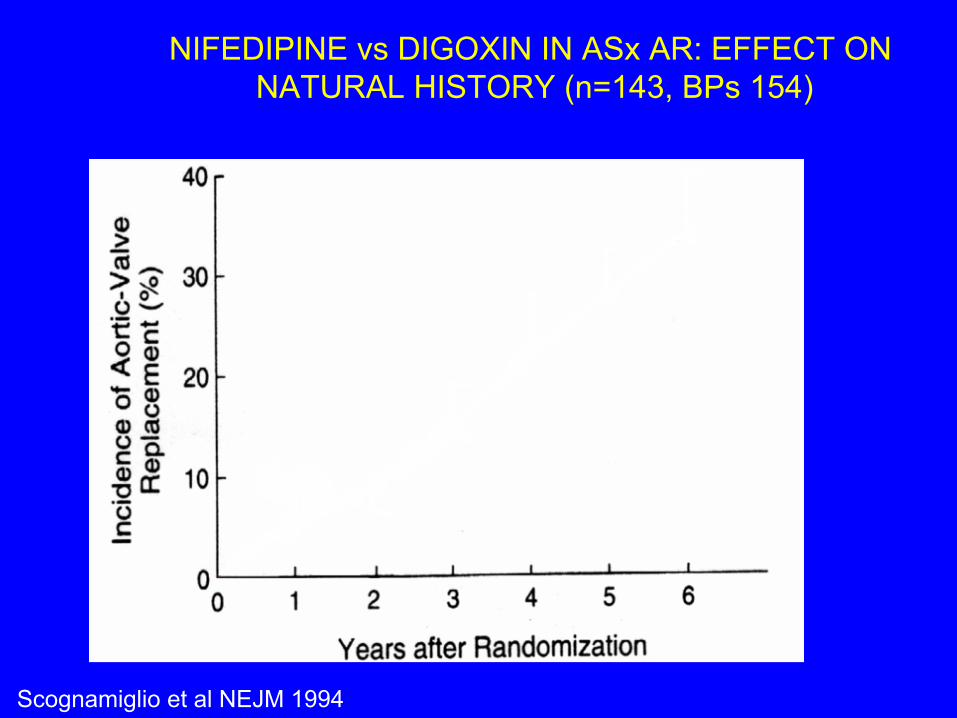
NIFEDIPINE vs DIGOXIN IN ASx AR: EFFECT ON NATURAL HISTORY (n=143, BPs 154)
Scognamiglio et al NEJM 1994

NIFEDIPINE vs DIGOXIN IN ASx AR: EFFECT ON NATURAL HISTORY (n=143, BPs 154)
Scognamiglio et al NEJM 1994

NIFEDIPINE vs DIGOXIN IN ASx AR: EFFECT ON NATURAL HISTORY (n=143, BPs 154)
Scognamiglio et al NEJM 1994
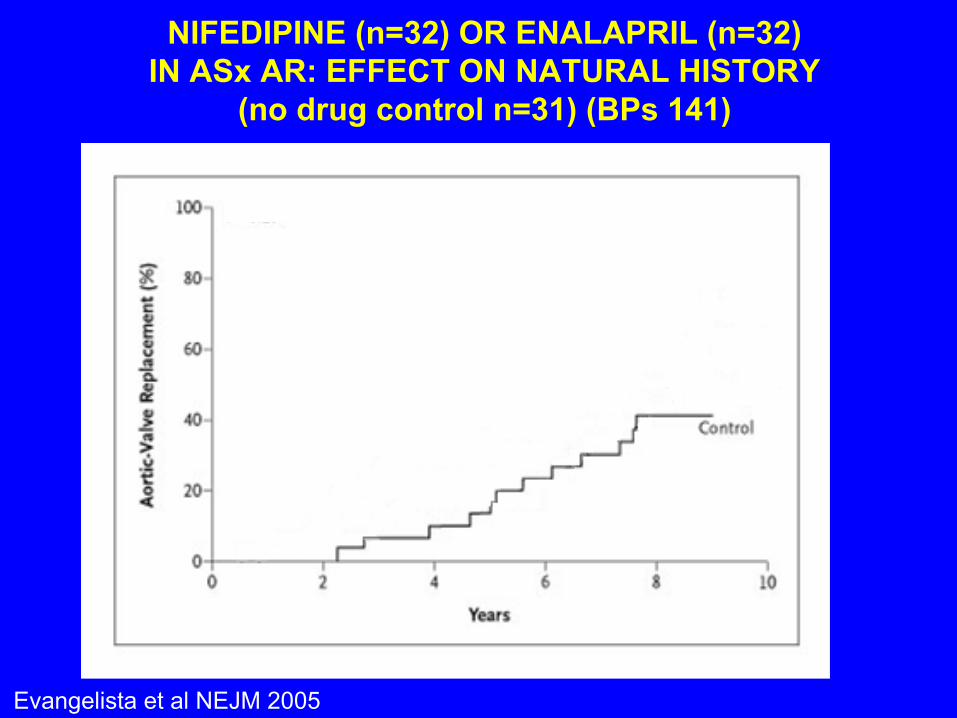
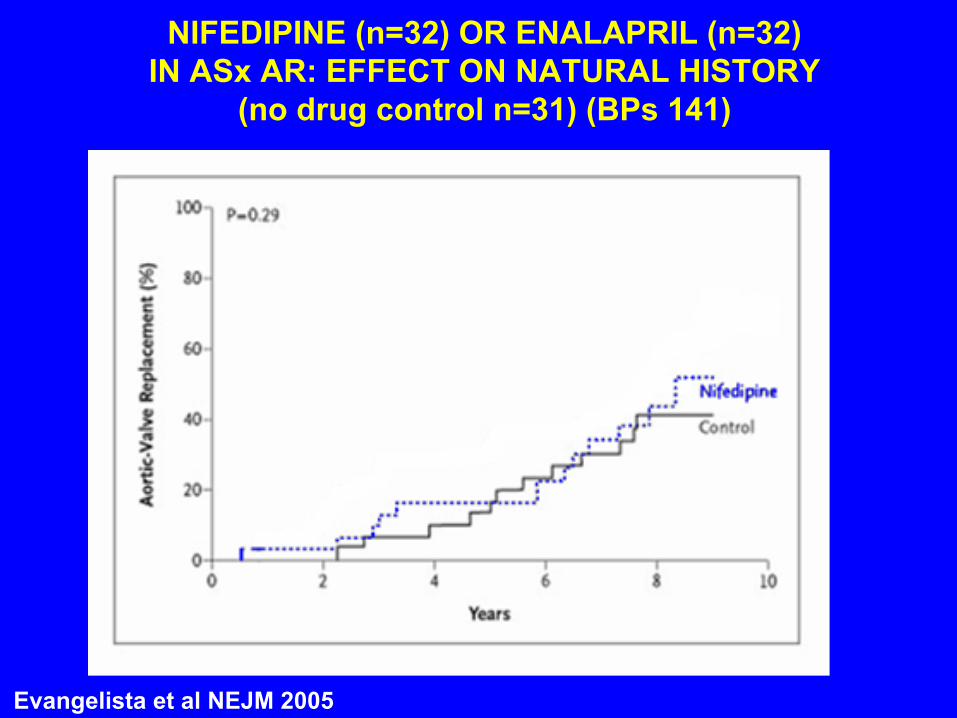
NIFEDIPINE (n=32) OR ENALAPRIL (n=32) IN ASx AR: EFFECT ON NATURAL HISTORY
(no drug control n=31) (BPs 141)
Evangelista et al NEJM 2005
Evangelista et al NEJM 2005
NIFEDIPINE (n=32) OR ENALAPRIL (n=32) IN ASx AR: EFFECT ON NATURAL HISTORY
(no drug control n=31) (BPs 141)
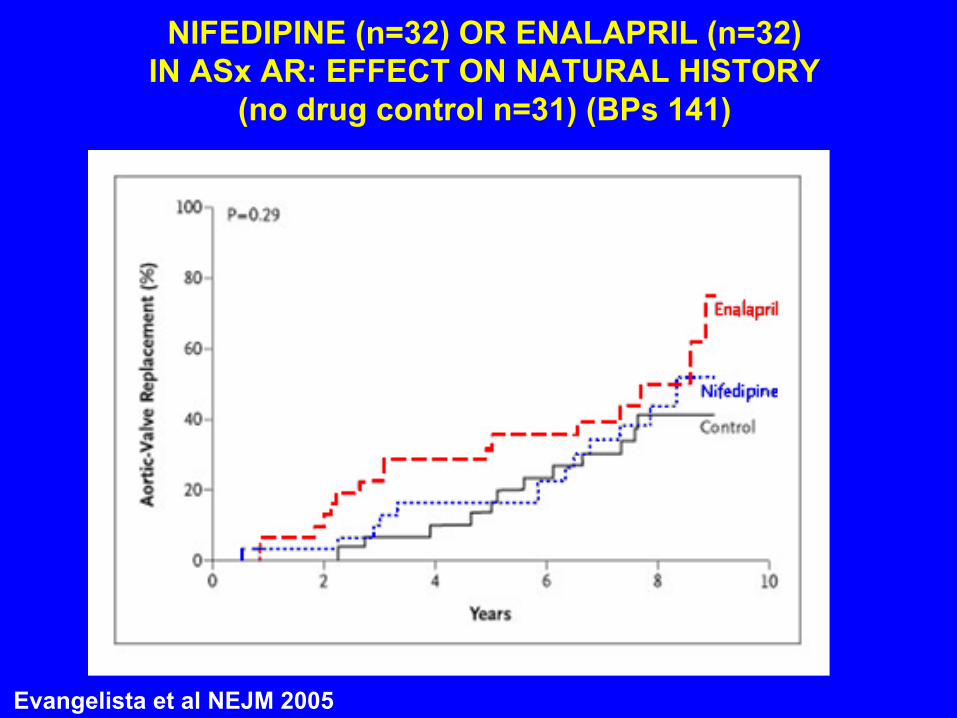
Evangelista et al NEJM 2005
NIFEDIPINE (n=32) OR ENALAPRIL (n=32) IN ASx AR: EFFECT ON NATURAL HISTORY
(no drug control n=31) (BPs 141)

Mitral Regurgitation: Chronic Vasodilator Therapy Use at Entry
vs. Event-Free Survival: All patients (N=56)
Years After Study Entry
% F
ree
of C
ardi
ac D
eath
of S
urgi
cal I
ndic
atio
n
Supino, Borer, et al. Cardiology 2014; 129:262-266
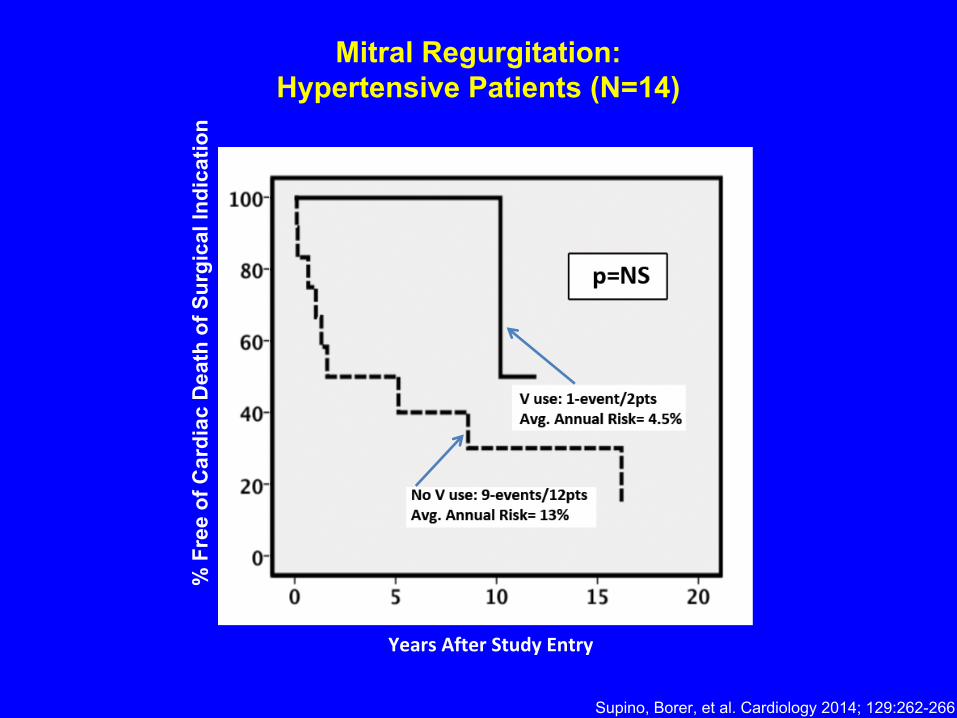
Mitral Regurgitation:Hypertensive Patients (N=14)
% F
ree
of C
ardi
ac D
eath
of S
urgi
cal I
ndic
atio
n
Years After Study Entry
Supino, Borer, et al. Cardiology 2014; 129:262-266

UNDERLYING PRINCIPLES/ISSUES
– Hemodynamic success of the procedure (?residual stenosis or regurgitation?)
– Comorbidities that are likely to directly affect cardiac function (most important: hypertension; dysrhythmia)
– Residual symptom status (is there clinical heart failure?)
– Residual ventricular/myocardial function

RESIDUAL SYMPTOMS
• Treat empirically to relieve symptoms– If heart failure symptoms and systolic dysfunction is present,
follow systolic HF guidelines

UNDERLYING PRINCIPLES/ISSUES
– Hemodynamic success of the procedure (?residual stenosis or regurgitation?)
– Comorbidities that are likely to directly affect cardiac function (most important: hypertension; dysrhythmia)
– Residual symptom status (is there clinical heart failure)
– Residual ventricular/myocardial function

RESIDUAL VENTRICULAR DYSFUNCTION
• Follow guidelines for systolic heart failure– ACEI/ARB– Beta blockers– MRA– Ivabradine if LVEF ≤35% and heart rate ≥70 bpm in sinus rhythm– + diuretics if volume excessive

CONCLUSIONS• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention

CONCLUSIONS• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Drug treatment after valve intervention is largely based on extrapolation from data from patients with unintervened valve disease

CONCLUSIONS• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Drug treatment after valve intervention is largely based on extrapolation from data from patients with unintervened valve disease
• Modified by judgment based on– Time after procedure at which drugs are to be given– Hemodynamic success of the procedure (?residual stenosis or
regurgitation?)– Comorbidities that are likely to directly affect cardiac function
(most important: hypertension; dysrhythmia)– Residual symptom status (is there clinical heart failure?)– Residual ventricular/myocardial function
CONCLUSIONS• There is no established/evidence-based cardiovascular
pharmacological therapy for – any uncomplicated valve disease– post-procedural adjunctive benefit for any valve intervention
• Drug treatment after valve intervention is largely based on extrapolation from data from patients with unintervened valve disease
• Modified by judgment based on– Time after procedure at which drugs are to be given– Hemodynamic success of the procedure (?residual stenosis or
regurgitation?)– Comorbidities that are likely to directly affect cardiac function
(most important: hypertension; dysrhythmia)– Residual symptom status (is there clinical heart failure?)– Residual ventricular/myocardial function
• The myocardium of valve-diseased hearts recovers slowly (years) after intervention– EFFECT OF DRUGS MAY VARY WITH THE CHANGES IN
MYOCARDIUM