what’s new in the treatment k, et al. eadv 2017, d3t01.1h sponsored by merck & co., inc. 84 81...
TRANSCRIPT
What’s New in the Treatment
of Psoriasis
Mark Lebwohl, MD Waldman Professor
And Chairman
Kimberly and Eric J. Waldman Department of Dermatology
Icahn School of Medicine at Mount Sinai

Mark Lebwohl is an employee of Mount Sinai which receives
research funds from: Abbvie, Amgen, Boehringer Ingelheim,
Celgene, Eli Lilly, Janssen / Johnson & Johnson, Kadmon,
Medimmune/Astra Zeneca, Novartis, Pfizer and ViDac.
Dr. Lebwohl is also a consultant for Allergan, Leopharma,
and Promius.
• Tildrakizumab
• Guselkumab – Tremfya ®
• Brodalumab – Siliq ®
• Ixekizumab – Taltz ®
• Secukinumab – Cosentyx ®
• Ustekinumab –Stelara ®
• Adalimumab – Humira®
• Etanercept –Enbrel ®
• Apremilast – Otezla ®
• Certolizumab - Cimzia ®
• Tofacitinib – Xeljanz ®
• Bimekizumab
• Risankizumab/Mirikizumab
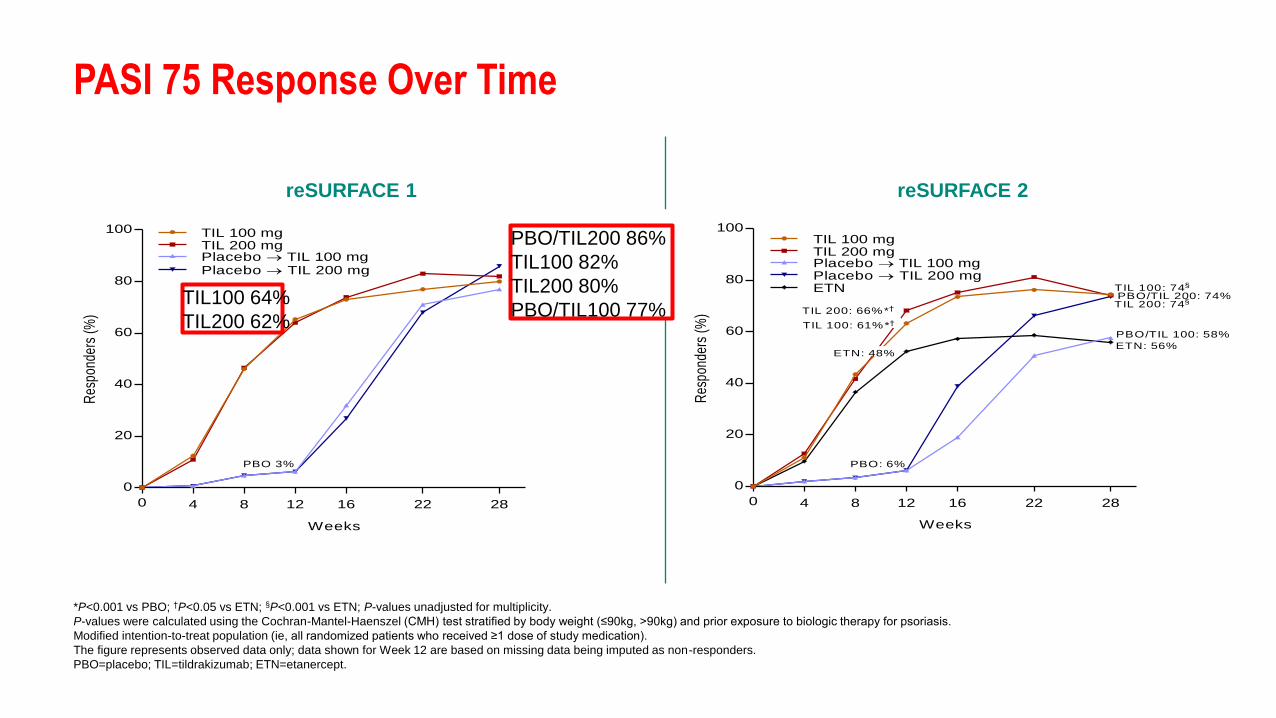
PASI 75 Response Over Time
*P<0.001 vs PBO; †P<0.05 vs ETN; §P<0.001 vs ETN; P-values unadjusted for multiplicity.
P-values were calculated using the Cochran-Mantel-Haenszel (CMH) test stratified by body weight (≤90kg, >90kg) and prior exposure to biologic therapy for psoriasis.
Modified intention-to-treat population (ie, all randomized patients who received ≥1 dose of study medication).
The figure represents observed data only; data shown for Week 12 are based on missing data being imputed as non-responders.
PBO=placebo; TIL=tildrakizumab; ETN=etanercept.
0
0
20
40
60
80
100
Weeks
Res
pond
ers
(%)
TIL 100 mgTIL 200 mgPlacebo TIL 100 mgPlacebo TIL 200 mg
4 8 12 16 22 28
TIL 200: 62%*
PBO 3%
TIL 200: 82%
TIL 100: 64%*
PBO/TIL 100: 77%
PBO/TIL 200: 86%
TIL 100: 80%*
0
0
20
40
60
80
100
Weeks
Res
pond
ers
(%)
4 8 12 16 22 28
TIL 200: 66%*†
PBO: 6%
TIL 200: 74§
PBO/TIL 100: 58%
PBO/TIL 200: 74%TIL 100: 74§
TIL 100 mgTIL 200 mgPlacebo TIL 100 mgPlacebo TIL 200 mgETN
ETN: 48%ETN: 56%
TIL 100: 61%*†
reSURFACE 1 reSURFACE 2
TIL100 64%
TIL200 62%
PBO/TIL200 86%
TIL100 82%
TIL200 80%
PBO/TIL100 77%

reSURFACE 1 and 2: Overall efficacy after 2 years of treatment
FAS (full analysis set; subjects with ≥1 dose of extension treatment based on assigned treatment); as observed data
Patients entering OLE after 64 weeks (reSURFACE 1) or 52 weeks (reSURFACE 2) were at least partial responders (PASI ≥50).
For reSURFACE 1, patients had to have received active drug within 12 weeks of end of base study
Papp K, et al. EADV 2017, D3T01.1H Sponsored by Merck & Co., Inc.
84 81
88 84
52 54
66 61
22 23
34 33
58 55
66 67
0
10
20
30
40
50
60
70
80
90
100
TIL 100 mg(n=219)
TIL 200 mg(n=255)
TIL 100 mg(n=355)
TIL 200(n=333)
Patients
(%
)
PASI 75
PASI 90
PASI 100
PGA (0/1)
reSURFACE 1 – w.64 reSURFACE 2 – w.52
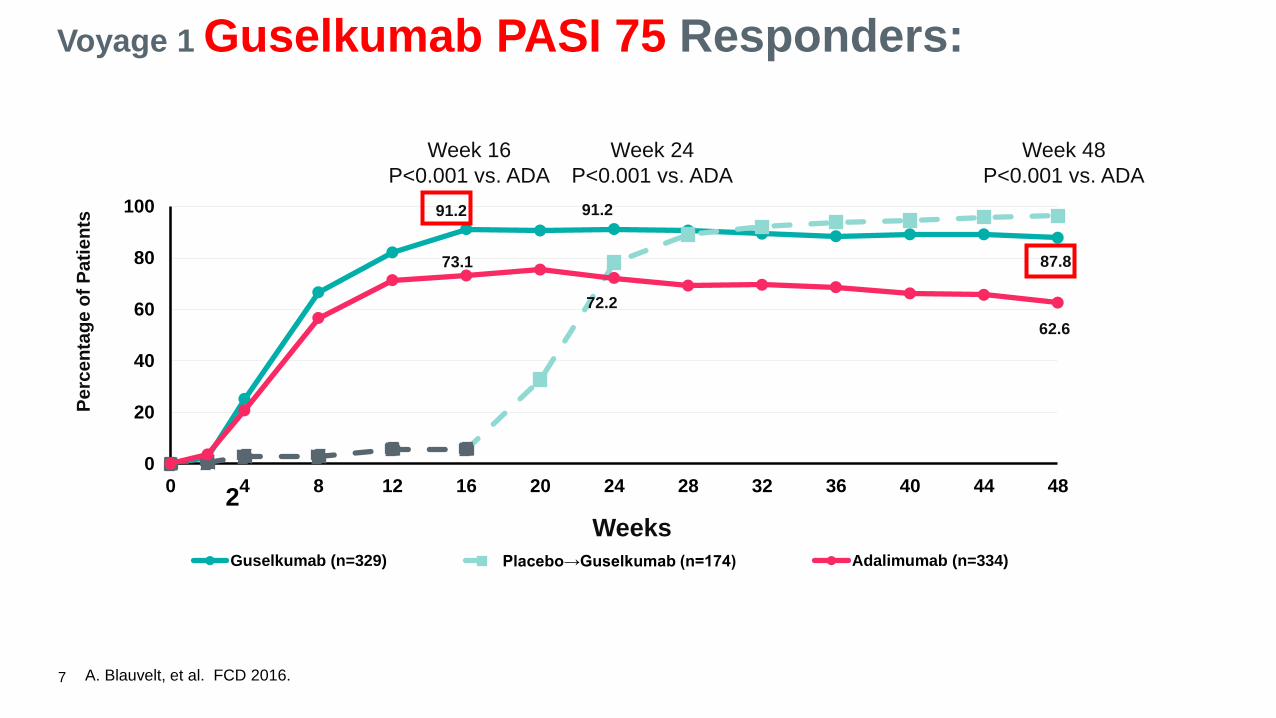
Voyage 1 Guselkumab PASI 75 Responders:
7
91.2
73.1
62.6
91.2
72.2
87.8
0
20
40
60
80
100
0 4 8 12 16 20 24 28 32 36 40 44 48
Perc
en
tag
e o
f P
ati
en
ts
Guselkumab (n=329) Placebo→Guselkumab (n=174) Adalimumab (n=334)
Weeks
2
Week 24
P<0.001 vs. ADA
Week 48
P<0.001 vs. ADA
Week 16
P<0.001 vs. ADA
A. Blauvelt, et al. FCD 2016.
Griffiths CEM, et al. EADV 2017, D3T01.I Sponsored by Janssen Research and Development LLC
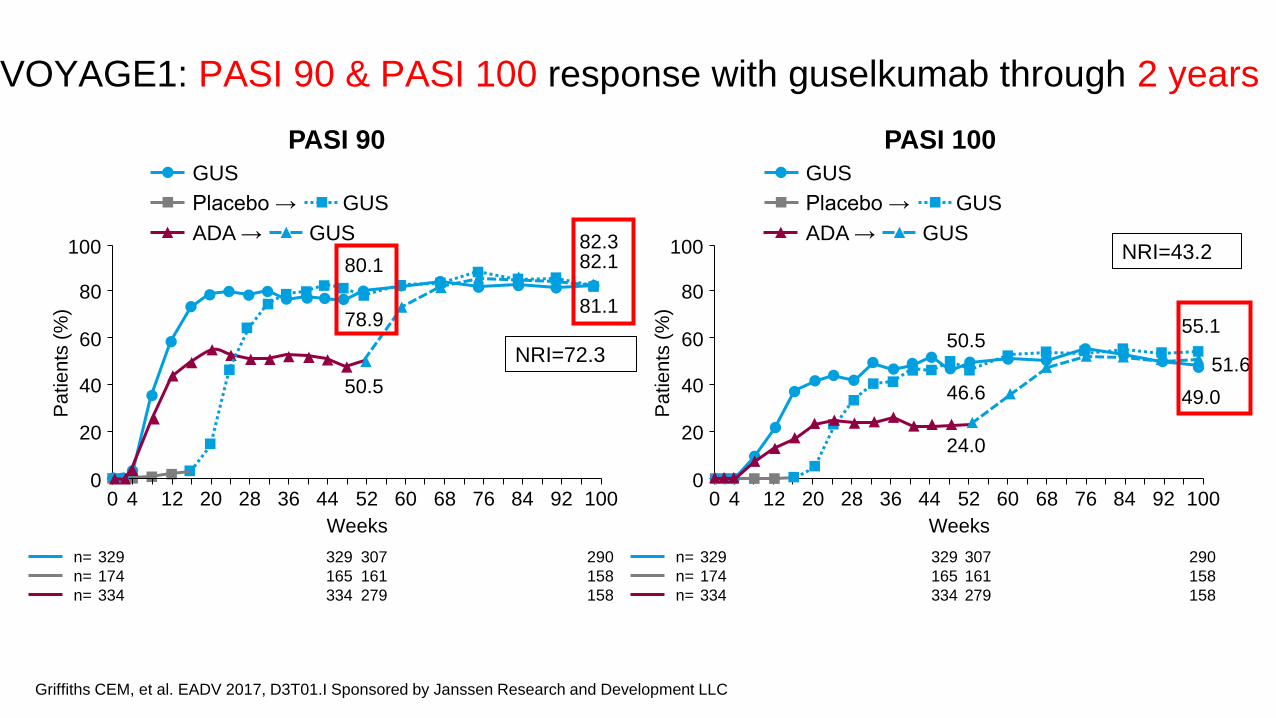
VOYAGE1: PASI 90 & PASI 100 response with guselkumab through 2 years
PASI 90 PASI 100
n= 329 329 307 290
n= 174 165 161 158
n= 334 334 279 158
n= 329 329 307 290
n= 174 165 161 158
n= 334 334 279 158
0
20
0 12
Weeks
100
40
80
60
4 20 44 36 28 52 60 84 76 68 92 100
Pa
tie
nts
(%
)
24.0
46.6
50.5 55.1
51.6
49.0
0
20
0 12
Weeks
100
40
80
60
4 20 44 36 28 52 60 84 76 68 92 100
Pa
tie
nts
(%
)
50.5
78.9
80.1
82.3 82.1
81.1
NRI=72.3
NRI=43.2
GUS
Placebo → GUS
ADA → GUS
GUS
Placebo → GUS
ADA → GUS

ACR 20/50/70 Responses at Week 24
18.4
10.2
2.0
58.0
34.0
14.0
0
20
40
60
80
100
ACR20 ACR50 ACR70
% o
f P
ati
en
ts
Placebo (n=49) Guselkumab (n=100)
p<0.001
p=0.023 (post hoc) p=0.002
Primary Endpoint
RESULTS
Gottlieb A, et al. AAD 2017. P4454.

Percent of Patients with Resolution of Enthesitis at Week 24 in Patients with Enthesitis at Baseline
29.0
56.6
0
10
20
30
40
50
60
70
80
90
100%
of
Pa
tien
ts
Placebo (n=31) Guselkumab (n=76)
p=0.012
Enthesitis assessed by Leeds Enthesitis Index (LEI)
Median % improvement in LEI at Week 24: 100% in guselkumab vs 33.3% in placebo (p=0.009)
RESULTS
Gottlieb A, et al. AAD 2017. P4454.
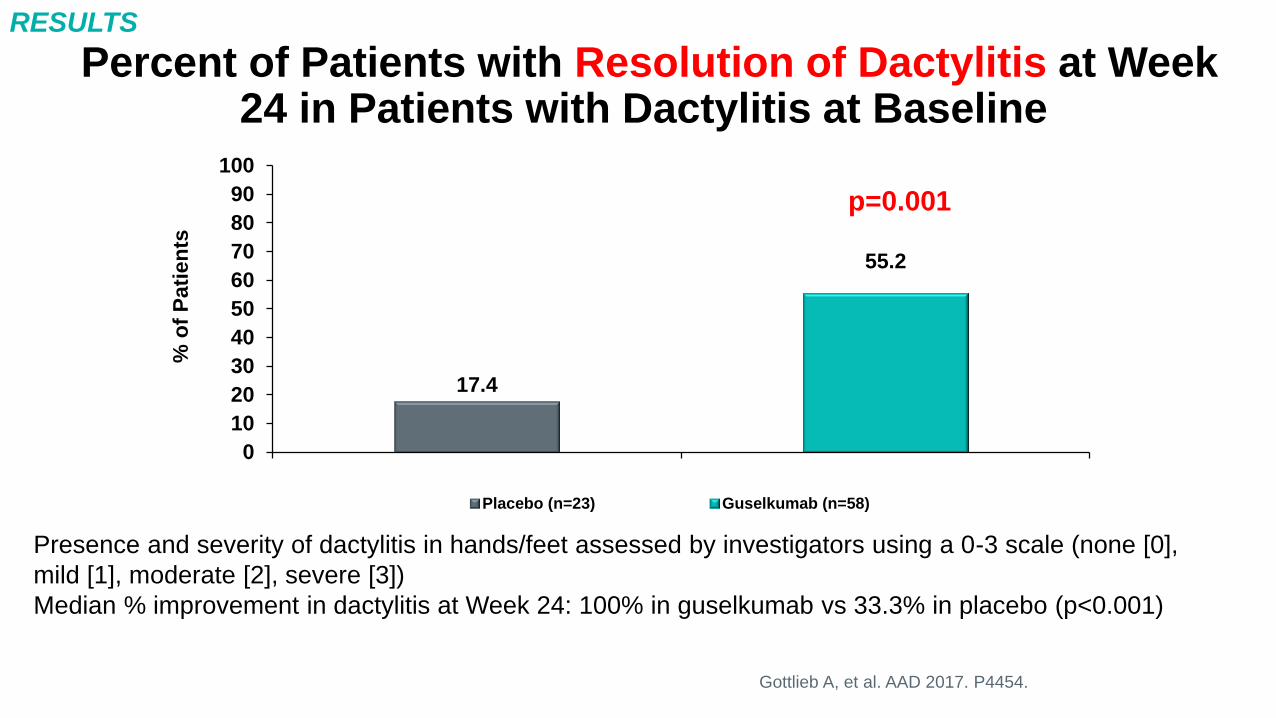
Percent of Patients with Resolution of Dactylitis at Week 24 in Patients with Dactylitis at Baseline
17.4
55.2
0
10
20
30
40
50
60
70
80
90
100%
of
Pa
tien
ts
Placebo (n=23) Guselkumab (n=58)
p=0.001
Gottlieb A, et al. AAD 2017. P4454.
Presence and severity of dactylitis in hands/feet assessed by investigators using a 0-3 scale (none [0],
mild [1], moderate [2], severe [3])
Median % improvement in dactylitis at Week 24: 100% in guselkumab vs 33.3% in placebo (p<0.001)
RESULTS

62.9 62.4 52.3
60.3 60.2
43
27.4 22.4
23.5 19.8 17.1
18.7
0
10
20
30
40
50
60
70
80
90
100
12 48 96 168 240 264
Pa
tie
nts
(%
)
Week
sPGA 0 sPGA 1
95.4 94.6 91.7 93.7 92.1
85.7
94.5 95.5 92.4 93.4 92.8
88.2
0
10
20
30
40
50
60
70
80
90
100
12 48 96 168 240 264
Me
an
im
pro
ve
me
nt
(%)
Week
PASI BSA
n= 175 165 153 141 128 106
Pts off
treatmenta
aAt week 264, patients had been off treatment for ≥6 weeks
Papp K, et al. EADV 2017, P1798 Sponsored by LEO Pharma
Efficacy of brodalumab for moderate to severe psoriasis through 5 years
sPGA 0/1 response Improvement in PASI score and % BSA
Pts off
treatmenta
84.8
75.8 80.1
77.3
61.7
n= 175 165 153 141 128 107
aAt week 264, patients had been off treatment for ≥6 weeks. Error bars represent 95% CI
Papp K, et al. EADV 2017, P1798 Sponsored by LEO Pharma
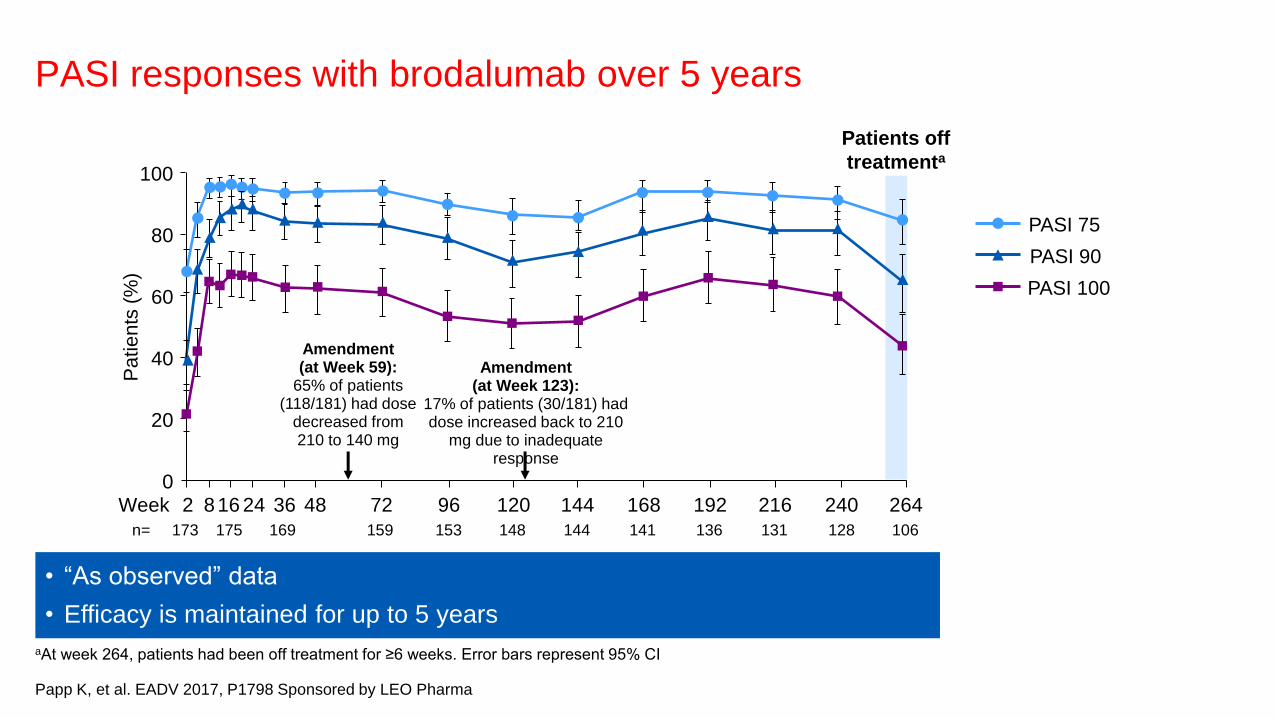
PASI responses with brodalumab over 5 years
• “As observed” data
• Efficacy is maintained for up to 5 years
PASI 90
PASI 100
PASI 75
Patients off
treatmenta
n= 173 175 169 159 153 148 144 141 136 131 128 106
40
20
0
80
60
100
Week 8 72 96 192 216 264 24 48 240 168 144 120 36 16 2
Amendment (at Week 123):
17% of patients (30/181) had dose increased back to 210
mg due to inadequate response
Amendment (at Week 59):
65% of patients (118/181) had dose
decreased from 210 to 140 mg
Pa
tie
nts
(%
)

*P<0.05; †P<0.01; ‡P<0.001 vs IXE q4w aDose adjustment based on achievement of sPGA ≥2 at 2 consecutive visits during
Week 12 through Week 40; investigators were blinded to the predefined criteria and timing
Langley RG, et al. EADV 2017, OP04.03 Sponsored by Eli Lilly and Company
IXORA-P: Efficacy and safety of continuous 2-weekly dosing of ixekizumab over 52 weeks in patients with moderate to severe psoriasis
71 79
73 84 79
86
0
20
40
60
80
100
sPGA (0/1) PASI 75
sPGA (0/1) and PASI 75 responses at Week 52
(NRI)
Pa
tie
nts
(%
)
IXE q4w (n=310) IXE q4w/IXE q2w
(n=306)
IXE q2w (n=611)
PASI 90 and PASI 100 responses at Week 52
(NRI)
65
44
74
49
80
60
0
20
40
60
80
100
PASI 90 PASI 100
†
*
†
‡
‡
IXORA-P: study design
IXE q2w (n=611)
R
Blinded treatment dosing period Screening
Week 16
Follow-
up 0 20 24 40 52 28 32 36
N=1227
2:1:1
IXE q2w
IXE q4w/IXE q2w (n=306)
Dose adjustment per protocola
IXE q4w (n=310)
• IXE q2w is better at Week 52
Pa
tie
nts
(%
)

Ixekizumab, an interleukin-17A specific
monoclonal antibody, for the treatment of
biologic-naive patients with active psoriatic
arthritis: results from the 24-week randomised,
double-blind, placebo-controlled and active
(adalimumab)-controlled period of the phase
III trial SPIRIT-P1.
Mease PJ, et al
Ann Rheum Dis. 2017;76:79-87.

Ixekizumab, an interleukin-17A specific monoclonal antibody, for the treatment of biologic-naive patients with active psoriatic arthritis: results from the 24-week randomised, double-blind, placebo-controlled and active
(adalimumab)-controlled period of the phase III trial SPIRIT-P1. Mease PJ, et al; Ann Rheum Dis. 2017;76:79-87.
0
20
40
60
80
100
0 2 4 6 8 10 12
PBO (N=74) IXE Q2W (N=75)
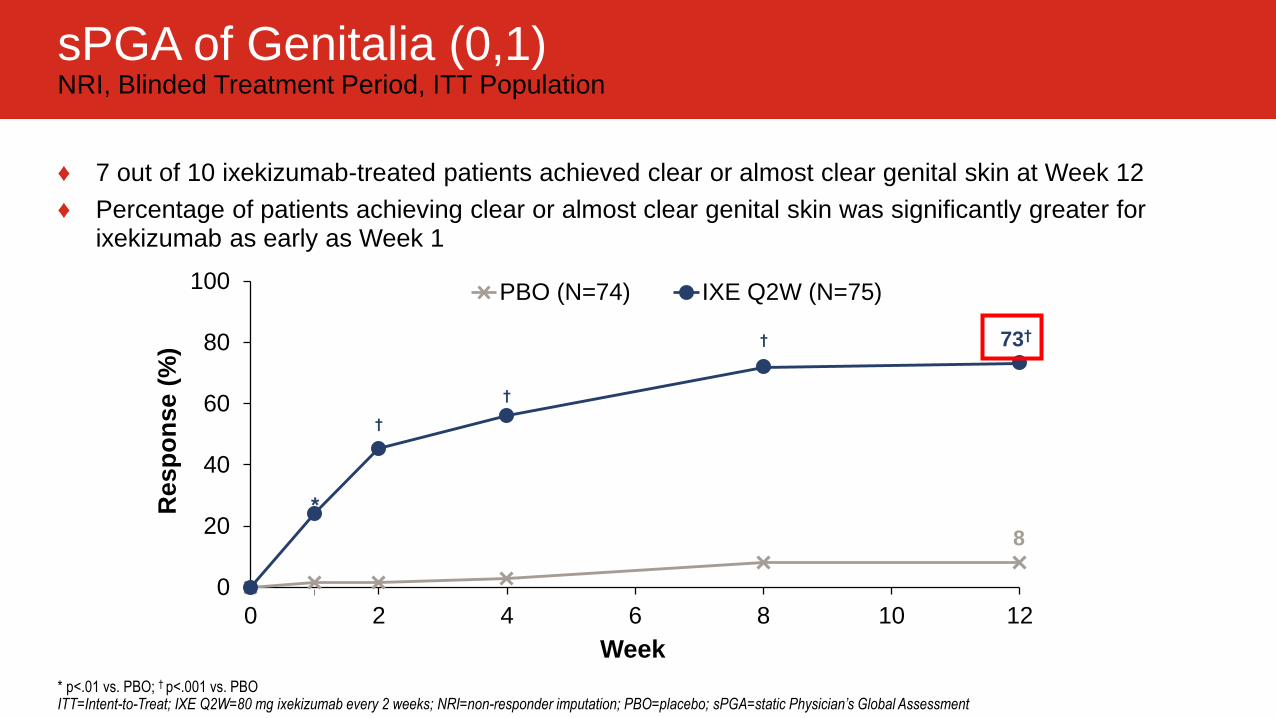
sPGA of Genitalia (0,1) NRI, Blinded Treatment Period, ITT Population
* p<.01 vs. PBO; † p<.001 vs. PBO ITT=Intent-to-Treat; IXE Q2W=80 mg ixekizumab every 2 weeks; NRI=non-responder imputation; PBO=placebo; sPGA=static Physician’s Global Assessment
Resp
on
se (
%) 73†
8
†
*
Week
†
†
♦ 7 out of 10 ixekizumab-treated patients achieved clear or almost clear genital skin at Week 12
♦ Percentage of patients achieving clear or almost clear genital skin was significantly greater for ixekizumab as early as Week 1
0
20
40
60
80
100
0 2 4 6 8 10 12
PBO (N=60) IXE Q2W (N=62)
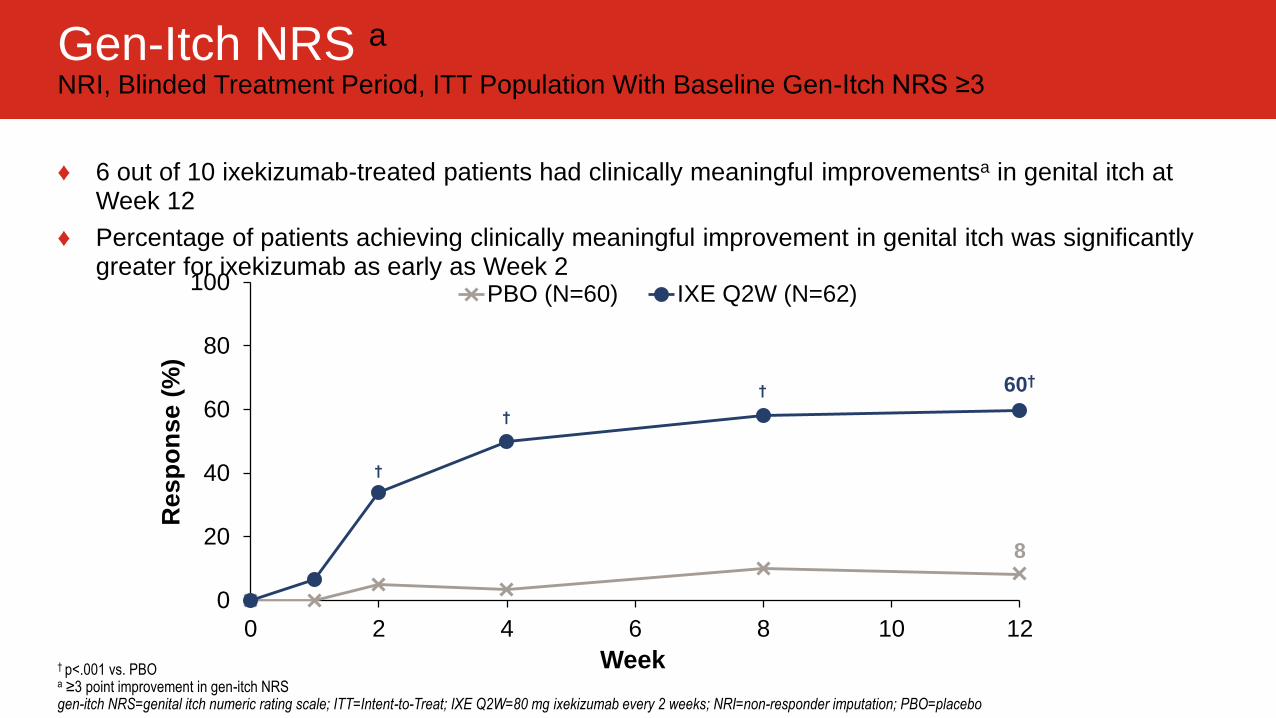
Gen-Itch NRS a NRI, Blinded Treatment Period, ITT Population With Baseline Gen-Itch NRS ≥3
† p<.001 vs. PBO a ≥3 point improvement in gen-itch NRS gen-itch NRS=genital itch numeric rating scale; ITT=Intent-to-Treat; IXE Q2W=80 mg ixekizumab every 2 weeks; NRI=non-responder imputation; PBO=placebo
♦ 6 out of 10 ixekizumab-treated patients had clinically meaningful improvementsa in genital itch at Week 12
♦ Percentage of patients achieving clinically meaningful improvement in genital itch was significantly greater for ixekizumab as early as Week 2
60†
8
† †
†
Resp
on
se (
%)
Week

♦ Proportion of patients achieving overall sPGA (0,1)
♦ Proportion of patients achieving a ≥3-point improvement in genital itch numeric rating scale (gen-itch NRS)
• Among patients with a baseline score of ≥3
♦ Proportion of patients whose frequency of sexual activity was never or rarely limited by genital psoriasis (SFQ Item 2 score 0 or 1)
• Among patients with a baseline score ≥2
SFQ Item 2 In the past week, how often
did your genital psoriasis
limit the frequency of your
sexual activity?
Never 0
Rarely 1
Sometimes 2
Often 3
Always 4
gen-itch NRS=genital itch numeric rating scale; SFQ=Sexual Frequency Questionnaire; sPGA=static Physician’s Global Assessment
Impact on frequency of sex! SFQ= Sexual Frequency Questionnaire

0
20
40
60
80
100
0 2 4 6 8 10 12
PBO (N=42) IXE Q2W (N=37)
SFQ Item 2 Score (0,1) Response Rate NRI, Blinded Treatment Period, ITT Population With Baseline SFQ Item 2 Score ≥2
♦ Approximately 8 out of 10 ixekizumab-treated patients were no longer or rarely limited by the impact of genital psoriasis on frequency of sexual activity at Week 12
♦ Percentage of patients who were no longer or rarely limited by the impact of genital psoriasis on frequency of sexual activity was significantly greater for ixekizumab as early as Week 1
‡ p<.05 vs. PBO; * p<.01 vs. PBO; † p<.001 vs. PBO ITT=Intent-to-Treat; IXE Q2W=80 mg ixekizumab every 2 weeks; NRI=non-responder imputation; PBO=placebo; SFQ=Sexual Frequency Questionnaire
78†
21
†
*
‡
Resp
on
se (
%)
Week

0
10
20
30
40
50
60
70
80
90
100
Patients
(%
)
Bissonnette R, et al. EADV 2017, P2223 Sponsored by Novartis Pharma AG
SCULPTURE: Long-term skin improvement responses with secukinumab 300 mg fixed interval (q4w) through 5 years
As observed (AO)
Multiple imputation (MI, n=168 at each time point)
LOCF (n=168 at each time point)
Year 1
(n=162)
Year 2
(n=152)
Year 3
(n=139)
Year 4
(n=132)
Year 5
(n=122)
PASI 75
PASI 90
PASI 100
Δ=~8%
Δ=~7%
Δ=~5%
PASI 75 (%) PASI 90 (%) PASI 100 (%)
AO MI LOCF AO MI LOCF AO MI LOCF
Year 1 88.9 – – 68.5 – – 43.8 – –
Year 5 88.5 80.1 79.2 66.4 58.6 59.5 41.0 35.6 37.5
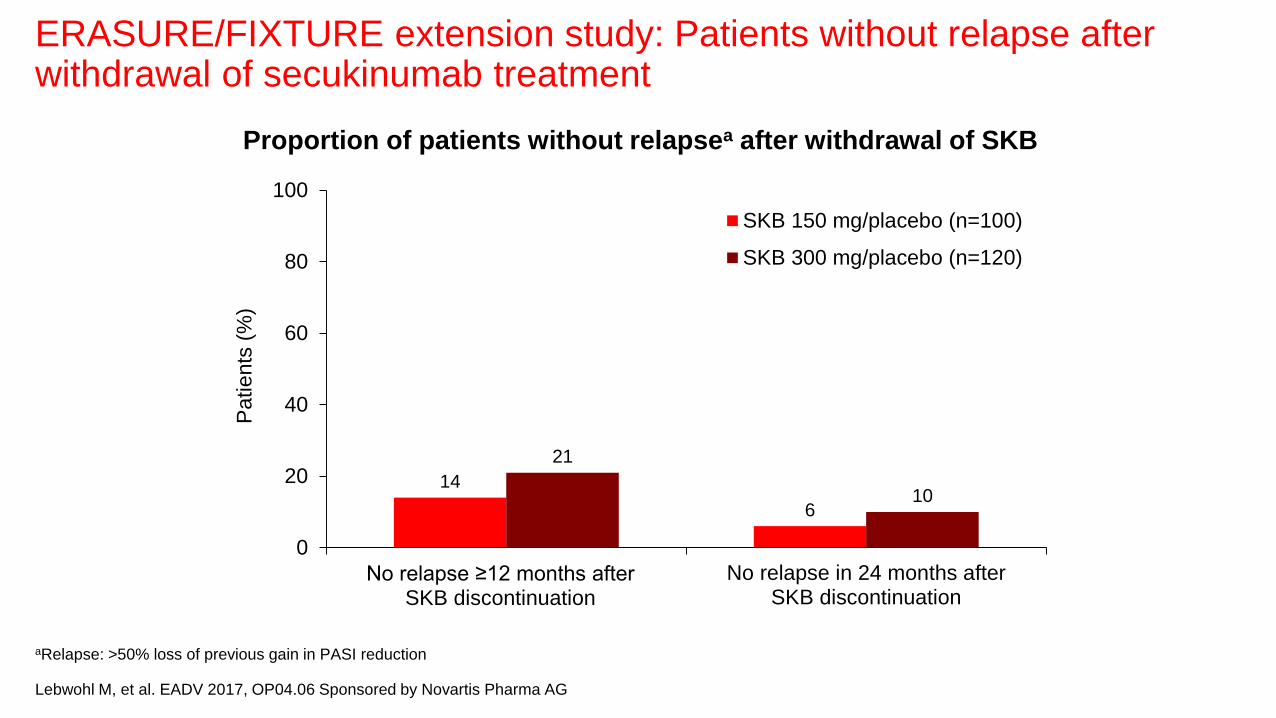
aRelapse: >50% loss of previous gain in PASI reduction
Lebwohl M, et al. EADV 2017, OP04.06 Sponsored by Novartis Pharma AG
ERASURE/FIXTURE extension study: Patients without relapse after withdrawal of secukinumab treatment
14
6
21
10
0
20
40
60
80
100
No relapse ≥12 months after SKB discontinuation
No relapse in 24 months afterSKB discontinuation
Patients
(%
) SKB 150 mg/placebo (n=100)
SKB 300 mg/placebo (n=120)
Proportion of patients without relapsea after withdrawal of SKB
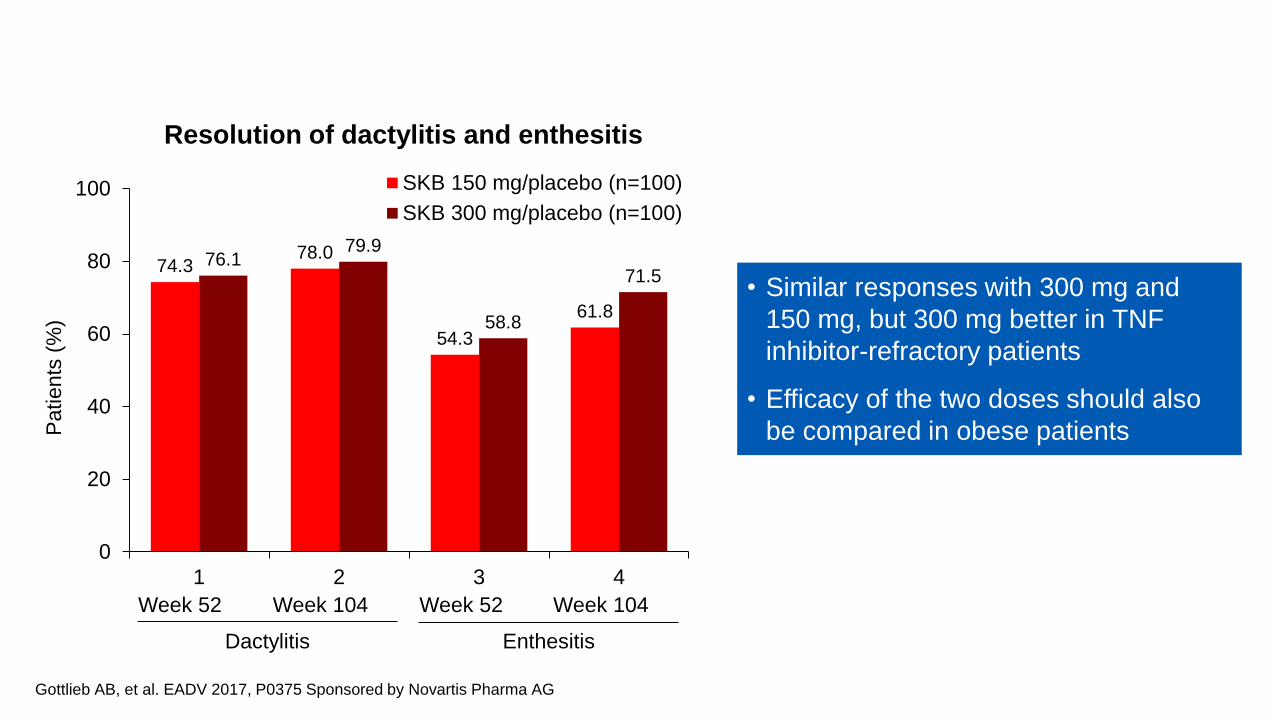
Gottlieb AB, et al. EADV 2017, P0375 Sponsored by Novartis Pharma AG
FUTURE 2: Resolution of dactylitis and enthesitis through 2 years
• Similar responses with 300 mg and
150 mg, but 300 mg better in TNF
inhibitor-refractory patients
• Efficacy of the two doses should also
be compared in obese patients
74.3 78.0
54.3
61.8
76.1 79.9
58.8
71.5
0
20
40
60
80
100
1 2 3 4
Patients
(%
)
SKB 150 mg/placebo (n=100)
SKB 300 mg/placebo (n=100)
Week 52 Week 52 Week 104 Week 104
Dactylitis Enthesitis
Resolution of dactylitis and enthesitis

Ustekinumab in adolescent patients age
12 to 17 years with moderate-to-severe
plaque psoriasis: results of the
randomized phase 3 CADMUS study.
Landells I, et al.
J Am Acad Dermatol. 2015;73(4): 594-603.

Ustekinumab package insert
Business Use Only 25
Ustekinumab as therapy for psoriasis in a
2-year-old girl.
Min MS, et al.
J Eur Acad Dermatol Venereol.
2016;30(11):e109-10.

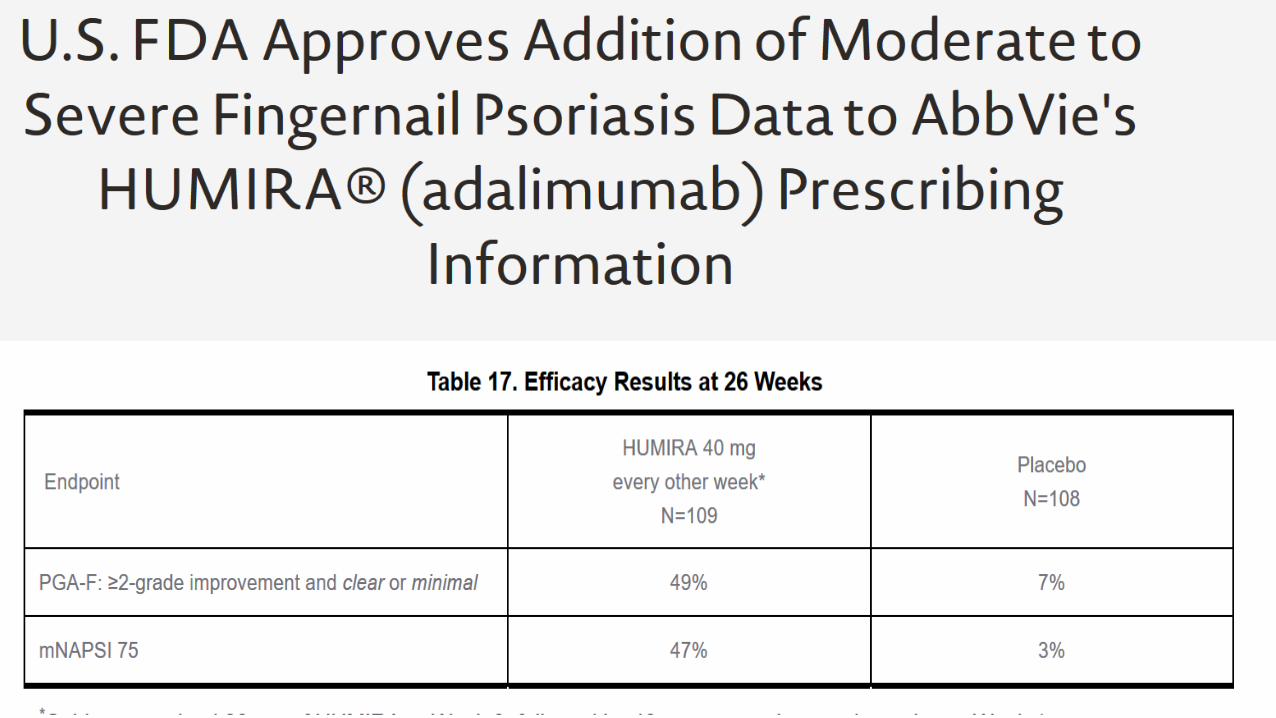
Adalimumab for nail psoriasis: Efficacy and safety
from the first 26 weeks of a phase 3, randomized,
placebo-controlled trial.
Elewski BE, Okun MM, Papp K, Baker CS,
Crowley JJ, Guillet G, Sundaram M,
Poulin Y, Gu Y, Geng Z, Williams DA, Rich PA.
J Am Acad Dermatol. 2018 Jan;78(1):90-99.
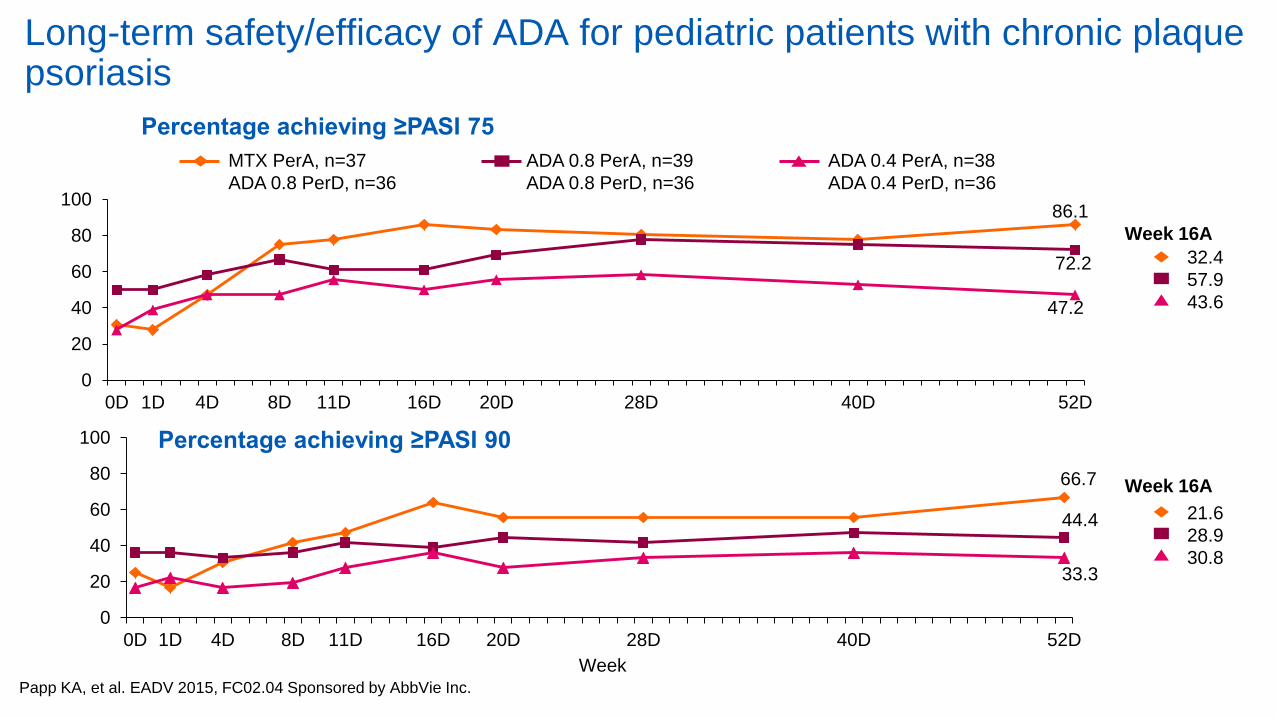
66.7
44.4
33.3
0
20
40
60
80
100
0D 1D 4D 8D 11D 16D 20D 28D 40D 52D
Long-term safety/efficacy of ADA for pediatric patients with chronic plaque psoriasis
Papp KA, et al. EADV 2015, FC02.04 Sponsored by AbbVie Inc.
86.1
72.2
47.2
0
20
40
60
80
100
0D 1D 4D 8D 11D 16D 20D 28D 40D 52D
Week
MTX PerA, n=37
ADA 0.8 PerD, n=36
ADA 0.8 PerA, n=39
ADA 0.8 PerD, n=36
ADA 0.4 PerA, n=38
ADA 0.4 PerD, n=36
32.4
57.9
43.6
Week 16A
21.6
28.9
30.8
Week 16A
Percentage achieving ≥PASI 75
Percentage achieving ≥PASI 90

Etanercept treatment for children and adolescents with plaque
psoriasis.
Paller AS, Siegfried EC, Langley RG, Gottlieb AB, Pariser D,
Landells I,Hebert AA, Eichenfield LF, Patel V, Creamer K,
Jahreis A; Etanercept PediatricPsoriasis Study Group.
N Engl J Med. 2008;358:241-51.
Long-term safety and efficacy of etanercept in children
and adolescents with plaque psoriasis.
Paller AS, Siegfried EC, Pariser DM, Rice KC, Trivedi M, Iles J,
Collier DH, Kricorian G, Langley RG
J Am Acad Dermatol. 2016;74:280-7.

5-year efficacy of ETN in children and adolescents with plaque psoriasis
Paller AS, et al. EADV 2015, FC02.05
PASI responses (as observed)
PASI 75 responses by BMI category (as observed)
• Largest and longest pediatric study with biologics in psoriasis reported to date

Strober B, et al. EADV 2017, FC02.08 Sponsored by Celgene Corporation
UNVEIL: 52-week efficacy and safety of apremilast in systemic- and biologic-naïve patients with moderate plaque psoriasis
• BSA involvement of 5% to 10%, naïve to
systemic and biologic therapy
• sPGA of 3 (moderate) based on a 0 to 5 scale
Screening Placebo-controlled
phase
0 Week 56
APR 30 mg bid (n=148)
16
Open-label treatment phase
R
1:2 Placebo (n=73)
52
Primary end point:
Mean % change in
PGA×BSA at Week 16
Safety observation
−5
APR 30 mg bid (n=64)
Placebo
(n=73)
Apremilast
(n=148)
Age (years) 51.1 ±13.7 48.6 ±15.4
Male 41 (56.2) 74 (50.0)
BMI (kg/m2) 30.8 ±6.5 30.5 ±7.4
Duration of psoriasis (years) 13.9 ±12.6 17.5 ±13.9
PGA×BSA score 21.6 ±5.9 21.8 ±5.3
% BSA 7.1 ±1.8 7.2 ±1.6
PASI score (0–72) 8.0 ±3.2 8.2 ±4.0
DLQI total score 11.1 ±6.5 11.0 ±6.5
Prior topical therapy 59 (80.8) 122 (82.4)
Data are mean ±SD or n (%)
At baseline, >80% of patients had received topical therapy before
enrollment
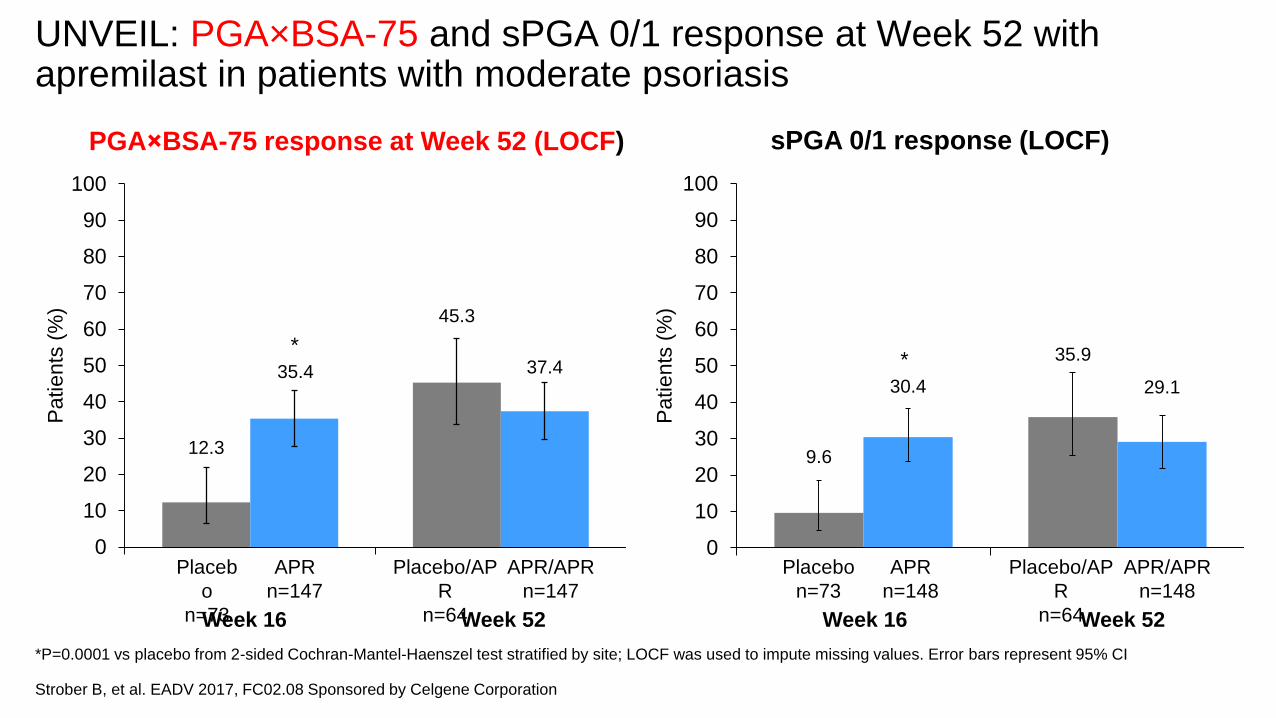
*P=0.0001 vs placebo from 2-sided Cochran-Mantel-Haenszel test stratified by site; LOCF was used to impute missing values. Error bars represent 95% CI
Strober B, et al. EADV 2017, FC02.08 Sponsored by Celgene Corporation
UNVEIL: PGA×BSA-75 and sPGA 0/1 response at Week 52 with apremilast in patients with moderate psoriasis
sPGA 0/1 response (LOCF) PGA×BSA-75 response at Week 52 (LOCF)
12.3
45.3
35.4 37.4
0
10
20
30
40
50
60
70
80
90
100
Patients
(%
)
*
Placeb
o
n=73
APR
n=147
Placebo/AP
R
n=64
APR/APR
n=147
Week 16 Week 52
9.6
35.9
30.4 29.1
0
10
20
30
40
50
60
70
80
90
100
Patients
(%
)
*
Placebo
n=73
APR
n=148
Placebo/AP
R
n=64
APR/APR
n=148
Week 16 Week 52

Jackson JM, et al. EADV 2017, P1946 Sponsored by Celgene Corporation
UNVEIL: Improvement in nails and scalp with apremilast at Week 52 in patients with moderate psoriasis
• Mild nail diseases – used target nail NAPSI – difficult to compare with other studies
• Caveat – scalp ScPGA had successes already in the baseline
• Increased attention to the moderate population is necessary as DLQI in some subsets is rather high
Characteristic Scalp psoriasisa (n=167) Nail psoriasisa (n=83)
Placebo (n=55)
APR (n=112)
Placebo (n=27)
APR (n=56)
% BSA 7.2 ±1.9 7.3 ±1.7 7.3 ±1.8 7.3 ±1.6
sPGA score=3 (moderate)b 53 (96.4) 110 (98.2) 26 (96.3) 55 (98.2)
PASI score (0–72) 8.1 ±3.2 8.2 ±4.3 8.0 ±2.8 8.1 ±2.9
DLQI total score 10.9 ±6.3 11.6 ±6.5 9.9 ±6.7 11.0 ±5.9
ScPGA score 0 (clear) 1 (minimal) 2 (mild) 3 (moderate) 4 (severe) 5 (very severe)
0 8 (14.5) 17 (30.9) 24 (43.6) 6 (10.9) 0
0 6 (5.4) 38 (33.9) 61 (54.5) 7 (6.3) 0
1 (3.7) 3 (11.1) 9 (33.3) 9 (33.3) 1 (3.7) 0
0 2 (3.6) 16 (28.6) 23 (41.1) 2 (3.6) 0
NAPSI total score 4.8 ±2.2 4.0 ±2.1 4.6 ±2.2 3.7 ±2.0
Data are mean ±SD or n (%) a65 patients had both scalp and nail psoriasis (22 placebo, 43 APR); b4 patients with sPGA=4 enrolled in error
-10.5 -28.9
-52.7 -51.9
-100
-80
-60
-40
-20
0
20
NAPSI scorec
Me
an
ch
an
ge
fro
m
ba
se
line (
%)
Week 16 Week 52
APR
(n=56)
Placebo
(n=27)
Placebo/APR
(n=23)
APR/APR
(n=48)
20.0
38.4
46.9 47.7
0
20
40
60
80
100
Pa
tie
nts
(%
)d
Week 16 Week 52
APR
(n=112)
Placebo
(n=55)
Placebo/APR
(n=49)
APR/APR
(n=88)
ScPGA 0/1 response
P=0.0178
cIncludes patients with baseline NAPSI score or ScPGA ≥1 dIncludes patients with baseline ScPGA score ≥1
Error bars represent 95% CIs

CIMPASI-1 and CIMPASI-2: Maintenance of response with certolizumab pegol during 32-week rerandomized maintenance period
*P<0.05, †P<0.0001 vs placebo, based on logistic regression model with factors for treatment, region and prior biologic exposure (yes/no). Week 16 PASI 50
nonresponders were imputed as nonresponders throughout maintenance period; all other missing data were imputed via multiple imputation (Markov chain
Monte Carlo [MCMC] method). CZP 200 mg q2w patients received loading dose of 400 mg at Weeks 0, 2 and 4
Reich K, et al. EADV 2017, P1973 Sponsored by Dermira Inc. in collaboration with UCB Pharma
PASI 75 (baseline to Week 48) PGA 0/1 (baseline to Week 48) PASI 90 (baseline to Week 48)
CIMPASI-1 CZP 200 mg q2w (n=95) CZP 400 mg q2w (n=88) Placebo (n=51)
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
60.2%
42.8%
0.4%
43.6%
†
†
* *
†
†
35.8%
Pa
tie
nts
(%
)
87.1%
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
67.2%
6.5%
75.8%
66.5%
†
† *
* * *
†
†
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
69.5%
52.7%
4.2%
†
†
†
* *
* *
*
57.9%
47.0%
CIMPASI-2
Pa
tie
nts
(%) 72.6%
66.6% 66.8%
Week
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
2.0%
† † †
*
*
†
†
71.6%
†
Week
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
78.7%
11.6%
†
†
†
†
*
81.3%
†
†
*
82.6%
81.4%
Week
20
0 48 2
40
60
100
80
12 24 16 0 28 20 4 8 32 40
62.0%
59.6%
4.5%
†
†
†
* *
*
55.4%
52.6%
CZP 200 mg q2w (n=91) CZP 400 mg q2w (n=87) Placebo (n=49)
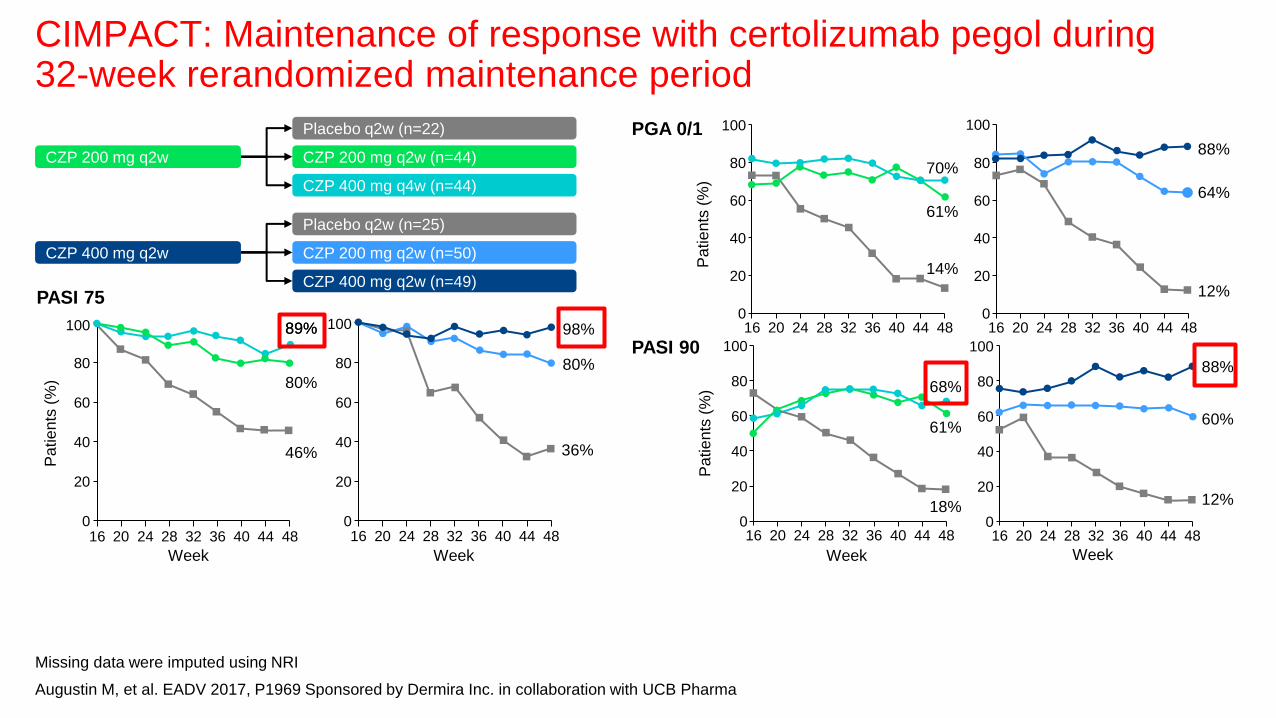
CIMPACT: Maintenance of response with certolizumab pegol during 32-week rerandomized maintenance period
Missing data were imputed using NRI
Augustin M, et al. EADV 2017, P1969 Sponsored by Dermira Inc. in collaboration with UCB Pharma
Placebo q2w (n=22)
CZP 200 mg q2w (n=44)
CZP 400 mg q4w (n=44)
CZP 200 mg q2w
Placebo q2w (n=25)
CZP 200 mg q2w (n=50)
CZP 400 mg q2w (n=49)
CZP 400 mg q2w
PASI 75
89%
PGA 0/1
PASI 90
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
70%
61%
14% Pa
tie
nts
(%
)
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
88%
64%
12%
Pa
tie
nts
(%
)
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
Week
80%
46%
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
98%
80%
36%
Week
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
68%
61%
18%
Pa
tie
nts
(%
)
Week
20
0 48 20
40
60
100
80
32 40 36 16 24 28 44
88%
60%
12%
Week
89%

a2/16 infant samples excluded from per protocol analysis set (1 missing data at birth, 1 due to implausible PK data [ie, data not consistent with pediatric CZP
PK model, based on expected range of clearance, volume of distribution, and subsequent elimination t½]); b2 samples not collected; c1 umbilical cord excluded
due to missing data; dUmbilical cords were collected within 1 h of delivery. BLQ, below limits of quantitation of the assay; LLOQ, lower limit of quantitation
Kimball A, et al. EADV 2017, FC04.03 Sponsored by UCB Pharma
CRIB: Maternal and infant plasma and umbilical cord levels of certolizumab pegol
Plasma CZP levels (n=14 mother–infant
pairsa)
CZ
P c
on
ce
ntr
atio
n (
g/m
L)
10
100
0.1
1
BLQ
Delivery
(±24 hours)
Week 4
(±7 days)b
Week 8
(±7 days)
LLOQ = 0.032 g/mL
Mothers Infants
1 infant had minimal CZP level of
0.042 μg/mL, mother’s level was
49.4 μg/mL (infant/mother ratio:
0.0009)
Plasma CZP levels in umbilical cord
(n=15c)
CZ
P c
on
ce
ntr
atio
n (
g/m
L)
10
100
0.1
1
BLQ
Delivery
(±24 hours)
Umbilical
cordsd
LLOQ = 0.032 g/mL
Mothers Infants
The infant with a CZP level at birth
of 0.042 μg/mL had a CZP level of
0.040 μg/mL in the umbilical cord
Umbilical cord

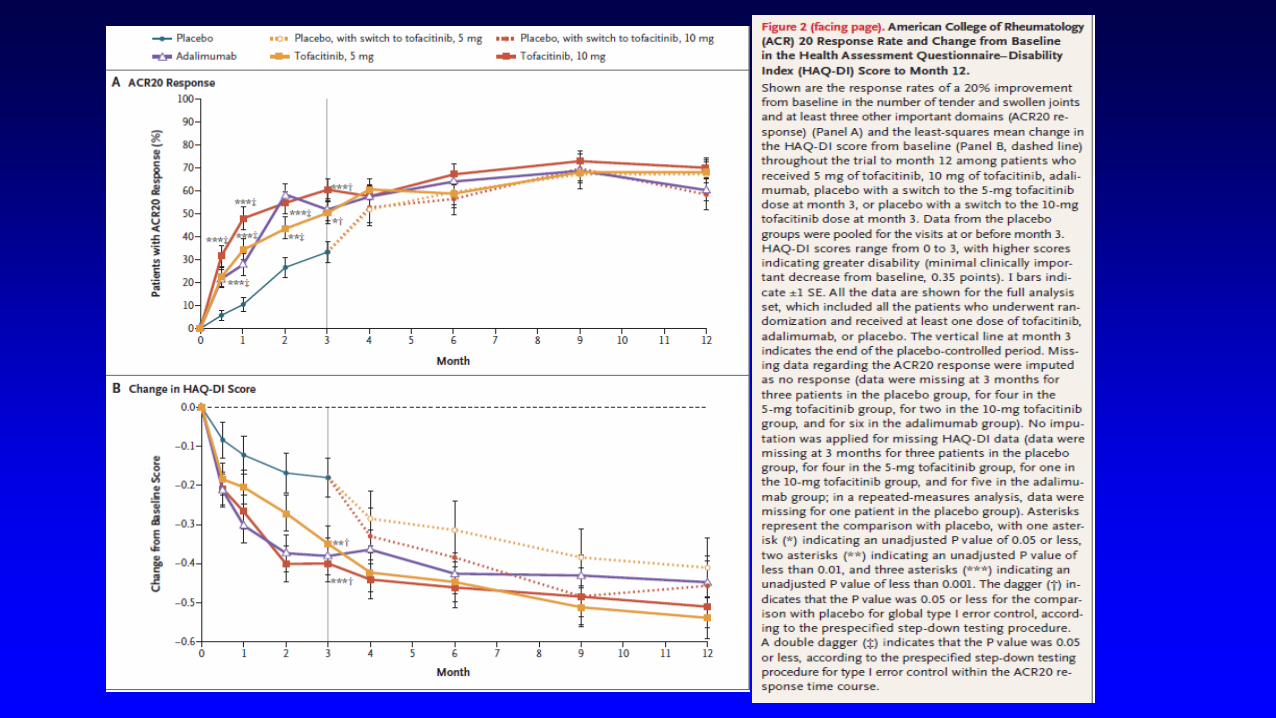
Tofacitinib or Adalimumab versus Placebo for
Psoriatic Arthritis.
Mease P, Hall S, FitzGerald O, van der Heijde D,
Merola JF, Avila-Zapata F, Cieślak D, Graham D,
Wang C, Menon S, Hendrikx T, Kanik KS.
N Engl J Med. 2017 19;377:1537-1550.

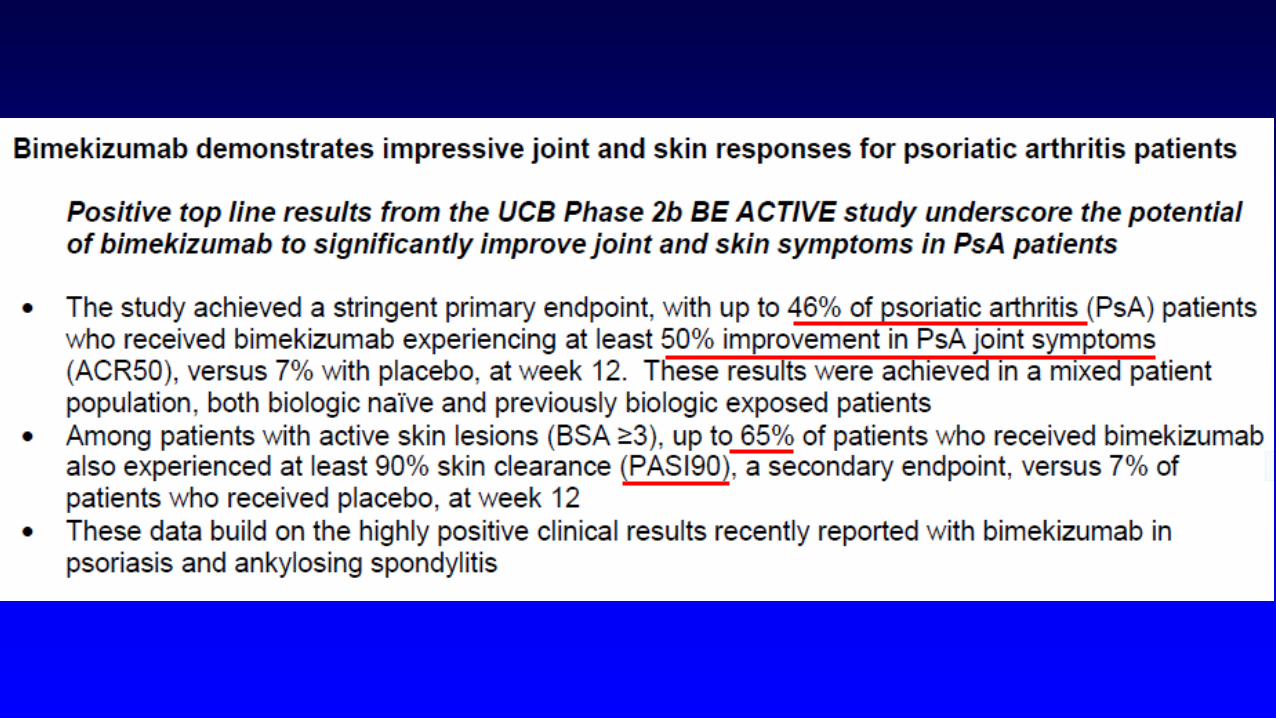
First-in-human randomized study of bimekizumab, a
humanized monoclonal antibody and selective dual
inhibitor of IL-17A and IL-17F, in mild
psoriasis. Glatt S, Helmer E, Haier B, Strimenopoulou
F, Price G, Vajjah P, Harari OA, Lambert J,
Shaw S.
Br J Clin Pharmacol. 2017;83(5):991-1001.


RISANKIZUMAB


P0456 Safety, efficacy and PK of a p19-directed IL-23 antibody (LY3074828) in patients with plaque psoriasis and healthy subjects MIRIKIZUMAB • Phase 1, placebo-controlled, 40 patients, 5 healthy volunteers, 12
weeks; 4% BSA, PASI 6.6
Tuttle J, et al. EADV 2016, P0456 Sponsored by Eli Lilly and Company 45
• Another a p19-directed IL-23 antibody effective in phase 1