whatis clinical immunology? · whatis clinical immunology? amdenman ... sent to the physicians and...
TRANSCRIPT
J Clin Pathol 1981 ;34:277-286
What is clinical immunology?AM DENMAN
From the Connective Tissue Diseases Research Group, Clinical Research Centre, Watford Road, Harrow,Middlesex HA] 3UJ, UK
SUMMARY The clinical and laboratory details of 10 patients with predominantly immunologicalproblems were circulated to selected physicians in different forms of hospital practice. In general,these physicians would prefer to select their own immunological tasks and could get these performedin their clinical pathology laboratories or regional immunology centres. Immunologists are seen
predominantly as laboratory-based advisers rather than clinicians responsible for the care of suchpatients.
Immunology pervades the activities of most clini-cians. This is scarcely surprising since so muchhuman disease results from the failure to combatinfectious agents or from allergic reactions to anti-gens in the form of drugs, chemicals, or simple floraand fauna. The importance of immunologicalmechanisms in the pathogenesis of disease is reflectedin the context of prophylactic immunisation or thetherapeutic manipulation of the immune response.These intellectual and practical considerations haveprovided the stimulus for establishing the newdiscipline of clinical immunology.
Traditionally clinical specialties have beenorganised according to the dictates of medicalpractice and, in general, physicians are classifiedaccording to their practical skills. Thus doctorswith a penchant for investigating gastrointestinalcomplaints became recognised as gastroenterolo-gists by their colleagues and learned to manipulatethe instruments which transformed this specialtyfrom one based on opinion to one based upon exactobservation. Similarly, with the growth of medicalscience, diagnostic services were provided by labora-tories with experience in the various branches ofclinical pathology. Thus a logical system was devisedwhereby the patient's symptoms provide the firstsign-post to the relevant clinical specialist and there-after essential specimens are sent to the appropriatelaboratory.Advances in clinical sciences have complicated the
operation of so simple a system. For examplehaematologists command a wide knowledge ofclinical and laboratory practice. It is widely accepted
therefore that haematologists must have access toboth beds and laboratory facilities so as to providethe best possible service for their patients. Thedilemma facing immunologists is apparently similarto that of haematologists and they must find the bestway in which increasing knowledge of immunologicalmechanisms in disease can be applied to the investi-gation and management of clinical problems. It isnecessary, however, to make a firm distinctionbetween academic immunology and immunology inclinical practice. The way in which T lymphocytesrecognise antigens is a fundamental problem whosesolution will have enormous therapeutic implications.This does not imply that a scientist investigating thisproblem should be integrated into institutions orteams dealing with clinical medicine. There may becircumstances in which the scientist investigatingsuch fundamental problems is not only clinicallyqualified but also uses clinical material as the basisfor much of his thinking and experimental work.This is not necessarily so and the situation is likelyto arise only in academic centres.
There are two principal ways in which immunologyaffects clinical practice. The first arises when clini-cians ask for immunological tests to manage a par-ticular patient. Some immunological tests have nowbecome so routine that the facilities to carry theseout have long been provided. It is obviously essentialthat physicians should be able, for example, to ordertests for detecting auto-antibodies and for measuringserum complement levels. However there are manyother tests, such as assaying blood lymphocyte sub-populations, whose practical value has not yet been
277
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from

278
firmly established. It is desirable for research pur-poses that in some centres provision be made forassessing the value of such immunological tests inadequate numbers of patients. However, hard presseddistrict general hospitals might reasonably take theline that, if only a relatively few such tests areindispensable for clinical management, these canreadily be incorporated into the work of existingdepartments of clinical pathology and other testsreferred to regional centres. Indeed the need forspecialized regional immunological laboratories andtheir functions have been persuasively argued.' 2
Secondly, immunological disturbances often pro-duce major clinical problems whose solution de-mands specialised knowledge of immunology. Somehospitals, and particularly academic institutions,have created posts for clinical immunologists usuallydefined as physicians with specialised interests in aparticular branch of clinical medicine and an activeresearch programme, eg, rheumatology and renalmedicine. Most hospitals could rightly retort thatthis is a luxury affordable only by research institu-tions and that the creation of a separate specialty ofclinical immunology is artefactual. Over the yearsspecialists in different branches of clinical medicinehave accepted the need to incorporate many facetsof basic biological sciences into their everyday prac-tice. Immunology may count as an important onebut other disciplines are at least as important andyet do not constantly lay claims to the establishmentof a separate specialty. If modern clinical specialistscan master immunology along with other basicsciences there is obviously less need for specialistimmunologists with clinical responsibility. If difficul-ties arise concerning the interpretation of a modicumof immunological tests then the clinical pathologistwith the most detailed interest in the immunologicalproblem should hasten to the bedside in the mannerof other clinical pathologists. Only in a few instanceswill the need to implement immunological techniquesso dominate their clinical practice that clinicians willfeel the need for a more formal association withimmunologists.
Immunological methods have not been introducedinto clinical practice in any systematic way. Themanner in which immunological advances have beenapplied to clinical practice has been determined bythe decisions of individual hospitals and clinicians.Thus the extent to which clinical immunology is alaboratory discipline, a clinical specialty in its ownright, or a part of existing clinical specialties hasbeen largely settled even while committees stilldebate these points. To obtain a complete picture ofthe solutions adopted throughout the United King-dom would be a formidable task. The approachadopted in this survey was to ask a small number of
Denman
physicians to reveal how they handle immunologicalproblems in their own practice. The results at leastindicate what these physicians understand by theterm clinical immunology.
Design of the study
We selected 10 immunological problems encoun-tered at this centre in the 12 months preceding thesurvey. An immunological problem was defined as adisease in which immunological mechanisms werethe most important factors in the pathogenesis ofthe disease and where the control of these processeswas the principal therapeutic problem. Detaileddescriptions of the history, clinical findings, con-ventional investigations, and specialised investiga-tions of these patients were sent to representativephysicians but details of immunological investiga-tions were mainly omitted. The recipients weregeneral physicians or physicians with a specialistinterest. Physicians practising in London and pro-vincial teaching hospitals, and in metropolitan andprovincial district hospitals, were asked to partici-pate. A note of explanation accompanied the casehistories:
'What is clinical immunology? The definition ofclinical immunology and the function of clinicalimmunologists have been extensively discussed andanalysed. At one extreme much of internal medicinehas been regarded as applied immunology. At theother extreme immunology has been considered tobe not a clinical discipline but rather one of the manybasic sciences important to clinicians practising in avariety of clinical specialties. We therefore decidedto ask knowledgeable, practising physicians to sayhow they would have handled selected clinical prob-lems with a strong immunological flavour.'
The note emphasised three problems: (1) whichimmunological tests the physicians would considerimportant in the practical management of thesepatients; (2) whether these physicians would inter-pret the results of the relevant immunological teststhemselves or would seek specialised immunologicaladvice, '3) who would have performed these tests intheir own hospital.
Case histories
The following case reports outline the informationsent to the physicians and the questions posed, inabbreviated form.
CASE 1 is a 26-year-old single, bank clerk. At theage of 20 she was investigated for secondary amenor-rhoea. Investigations revealed small, hypoplastic
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
What is clinical immunology?
ovaries. There was normal pituitary function withincreased gonadotrophin production while oestro-gen excretion never exceeded 0-02 nmol/litre ofurine. Chromosome analysis showed a normalfemale karyotype. The diagnosis was ovarian failure.
Hashimoto's thyroiditis was also diagnosed at theage of 20 but the patient was clinically euthyroid.Her protein bound iodine was raised at 829 nmol/land thyroid microsomal auto-antibodies were detec-ted but thyroid function tests were otherwise normal.Two years later she developed polyarthritis in the
hands, knees, and feet. The principal laboratoryfindings were Hb 11-7 g/dl, WBC 6-5 x 109/l with anormal differential, and ESR 72 mm/h. Latex test1:1280. Erosive changes were present radiologically.At 26 years of age she was admitted with a two
months' history of weight loss, thirst, and polyuria.Heavy glycosuria confirmed the diagnosis of acutediabetes mellitus which was rapidly controlled withsoluble insulin.
Questions(1) What additional immunological tests do you regard
as essential for this patient's management?(2) Do recent advances in basic or applied immunology
help you to understand the theoretical and practicalproblems surrounding this girl's diseases?
(3) Do you believe that a clinical immunologist couldcontribute to her management?
CASE 2, a 37-year-old housewife, gave a history ofrash on the face and exposed surfaces of the limbsmade worse by exposure to sunlight for 3 years andpainful red lumps on the legs, diffuse pain and ten-derness in the limbs, and lethargy for 1 year. Sheadmitted to dyspnoea and chest discomfort on mildexertion. There was no past history of allergies andthe patient was not currently receiving drug treat-ment.
She showed a fixed erythematous scaling eruptionin the butterfly distribution of the face with telangiec-tasia and follicular plugging. There was generalisedmuscle tenderness more marked over the proximalmuscles. Joint abnormalities, vasculitic lesions, hairloss, or lymphadenopathy were not present.
Investigations revealed Hb 11.5 g/dl withnormochromic, normocytic red cells, WBC 3-7 x109/1, of which 1924/pu were granulocytes and1517/pl lymphocytes, and ESR 40 mm. There wereno biochemical abnormalities and no urinaryabnormalities. The chest x-ray was normal. Lungfunction tests showed a reduction in TLco of13 8 ml/min/mmHg against a predicted 28-0. Duringa six-month period of observation she suffered twoattacks of severe abdominal pain and two grand malfits with a normal EEG.
Questions(1) What laboratory investigations would you need to
diagnose the nature and extent of her 'systemiclupus erythematosus'?
(2) Which ancillary tests do you use to evaluate theextent of any systemic involvement?
CASE 3 is an 18-year-old girl with severe bronchialasthma since the age of 3. She has mild sneezingbouts during the hay fever season and has noticedthat house-cleaning and exposure to dogs exacerbateher asthma. She developed eczema in infancy butthis cleared spontaneously. There is no obvioussocial stress and her attacks are not precipitated byobvious injection. There is no family history ofallergic disorders. She is a fit-looking girl with scat-tered expiratory crepitations but no other respiratoryor general abnormalities and a peak flow rate340 I/min.
Questions(1) This girl has mild bronchial asthma; would you
attempt to look for specific allergies?(2) How would you do this?(3) Who would do the relevant tests?(4) Do you think the results are of academic interest
or of practical value?
CASE 4 is a 13-year-old schoolgirl with eczema ofvarying severity since birth. It now involves theentire body including the scalp. She had a severeattack of bronchial asthma 3 years ago but has noother allergic disorders. There is no family history ofallergic disorders. She is not exposed to pets butbelieves that eggs worsen the condition. Topical andsystemic steroids have produced little improvement.Examination reveals eczema affecting the entire skinbut no systemic abnormalities. The laboratory find-ings are Hb 13-4 g/dl, WBC 7-8 x 109/l; eosinophils1326/)l, ESR 2 mm and no biochemical abnormali-ties. The urine is normal and the stools containneither ova nor parasites. However the serum IgE isconsistently over 50 000 IU/ml (normal range0-200 IU/ml).
Questions(1) Would you look for specific allergies?(2) How would you go about this task in terms of
clinical and laboratory assessment?(3) Who do you think should undertake these investi-
gations?
CASE 5 is a 32-year-old research virologist whopresented with a 12-year history of recurrent skinlesions of the lower limbs of progressive severity
279
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
Denman
diagnosed by several dermatologists as intermediatebetween mycosis fungoides and cutaneous vasculitis.Histology shows superficial changes consistent withmycosis fungoides and vasculitis in the deep dermis.The patient is occupationally exposed to severalpathogenic viruses but his illness preceded this ex-posure. He is in excellent general health. Physicalexamination is normal apart from the rash and inparticular there is no superficial lymphadenopathyand the liver and spleen are not palpable. Investiga-tions showed Hb 17 2 g/dl, WBC 10-4 x 109/l witha normal differential count, ESR 10 mm, no bio-chemical abnormalities and normal immunoglobulinconcentrations.The total body scan is reported to show unequivo-
cal, massive enlargement of the paravertebral lymphnodes. The surgeon's opinion is that a biopsy of anenlarged lymph node will involve laparotomy andhe is not convinced that the lymph nodes are involvedby neoplastic disease.
Questions(1) How would you investigate the nature and cause
of this patient's vasculitis?(2) Do you consider the lymphadenopathy clinically
relevant?(3) Do you believe that assays of 'lymphocyte markers'
or investigations of immune function would help todecide whether lymph node biopsy is unavoidable?
(4) Who would undertake the relevant investigationsin your hospital if you thought these were neces-sary?
CASE 6 is a 50-year-old lady with hypogamma-globulinaemia. At the age of 7 she is said to have haddeveloped'nephritis' of three years' duration. At theage of 23 she developed eczema followed by 'thyro-toxicosis' which was treated with thiouracil. Herfirst pregnancy at the age of 28 was marked by un-explained anaemia. At 32 years of age she sufferedan attack of severe right-sided herpes zoster ophthal-micus leading to corneal abscesses and generalisedvaricella; secondary staphylococcal skin sepsisensued. Her blood counts were Hb not less than15-0 g/dl, WBC 8-29 x 109/l, granulocyte count 3-12x 109/l, and platelet count 30-40 x 109/l.The following year she suffered repeated super-
ficial skin infections and repeated bruising. Steroidswere started at this time. At 34 years of age herspleen was removed and this was grossly enlarged.It showed hyperplasia but no evidence of lymphomaor malignant infiltration.Her platelet count improved and was maintained
at between 300 and 450 x 109/l. Steroids werewithdrawn over the next 12 months. She subse-quently developed staphylococcal pneumonia and
staphylococcal septicaemia following a perianalabscess.
In 1974, at the age of 46, hypogammaglobulinaemiawas first suspected and diagnosed. Regular treatmentwith gamma globulin injections and steroids wasstarted but the latter were discontinued after twoyears. There is no family history of immunode-ficiency.Her current admission was precipitated by 6
months' cough and sputum, watery diarrhoea, and in-creasing tiredness. She was receiving no medicationapart from y-globulin injections.On examination there were scattered small bruises
on the legs; coarse crepitations were heard at bothlung bases. Investigations revealed an Hb of 8-3 g/dlfalling to 6-8 g/dl over 2 weeks observation with amacrocytosis of 120 fi and a reticulocyte count of21-5%. The WBC was 13 2 x 109/l with a normaldifferential, and the platelet count 230 x 109/1. Thedirect Coombs test was positive with broad spectrum,anti-IgG, anti-IgM, anti-IgA, and anti-C3d reagents.The bone marrow aspirate showed increased
cellularity with erythroid hyperplasia, normal granu-lopoiesis, plentiful megakaryocytes, and no excess oflymphocytes. The serum immunoglobulin concen-trations were IgG 19 g/l, IgA 0-1 g/l, and IgM0-3 g/l. There were no other biochemical abnormali-ties and there was no evidence of malabsorption.Chest x-ray, sputum culture, MSU blood cultures,and stool cultures produced no evidence of signifi-cant infection.
Questions(1) What further investigations do you think appro-
priate for elucidating the nature of her hypogam-maglobulinaemia and haemolytic anaemia?
(2) Who do you think should manage this patient'sproblems in the short and long term assuming thatgamma globulin would be made available for who-ever undertook this responsibility?
(3) If you accepted this responsibility yourself, howwould you manage her haemolytic anaemia andher immunodeficiency?
CASE 7 is a 21-year-old woman who developedtenosynovitis 18 months ago. The arthritis spreadover the next 12 months and has been progressivelydisabling.
In the past 6 months she has suffered sore throats,recurrent mouth ulcers, intermittent fever, andworsening lethargy. She has also noted recurrentpleuritic pain and dyspnoea on exertion. She haslost 10 kg weight in the past 2 months. She has re-ceived various non-steroidal anti-inflammatorydrugs, short courses of gold, and penicillamine.
280
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
What is clinical immunology?
She was pale, underweight, and febrile (390C) withgeneralised firm lymphadenopathy. There was mini-mal symmetrical soft tissue swelling of small jointsin the hands and feet.There was no rash or vasculitic lesions. Systemic
examination was normal save that fine inspiratorycrackles were heard at both lung bases.
Investigations revealed a normochromic, normo-cytic anaemia, Hb 8-2 g/dl, WBC 4 5 x 109/l, withgranulocytes 2621/1l and lymphocytes 1428/pJ,platelets 295 x 109/l and ESR 131 mm. The bloodurea was 8-1 mmol/l, electrolytes normal, albumin25 g/l, total globulin 38 g/l, and serum iron 6 /Imol/l.No other biochemical abnormalities were noted.
Renal disease was indicated by 10 x 106 leucocytesand 160 x 106 RBC/1 urine, 5*1 g proteinuria/24 hand a reduced GFR 55 ml/min. Creatinine clear-ance was normal and the urine was sterile. Thedirect Coombs test was negative. The serum IgGconcentration was raised at 21 1 g/l but other immu-noglobulin concentrations were normal. Totalhaemolytic complement was reduced at 1 in 2, as wasthe C 3, 24 mg/100 ml and C 4, 4 mg/100 ml. Anti-nuclear antibody was detected at a titre of 1/1280;precipitating antibodies to DNA and ENA andC 1q binding material were readily detectable.The chest x-ray showed minor left lower lobe con-
solidation, and lung function tests showed severelyimpaired lung capacity, flow rate, and gas exchange.
QuestionsWe would all accept that this girl is suffering fromsystemic lupus erythematosus.(1) Who should look after her, a rheumatologist,
nephrologist, general physician, other specialist, ora combination of specialists?
(2) If there was a 'clinical immunologist' on the staffof your hospital would you rely on him or her foradvice, for total management, or would you dis-pense with their services?
(3) How would you treat this patient (given that allpossibilities were open to you including plasma-phoresis)?
(4) If you were solely responsible for her management,which laboratory tests would you regard as essen-tial for controlling her disease activity and herdrug treatment?
(5) Which department in your hospital would under-take these tests?
CA SE 8 is a 60-year-old man presenting with anephrotic syndrome. Three months beforehand hesuffered a severe attack of 'influenza' with a produc-tive cough. Thereafter he became progressively morelethargic. For the past month he has noticed swellingof the lower limbs, He has not received any medica-
281
tion in the year preceding admission and there is nohistory of allergies. There is a family history ofichthyosis.The patient was euthyroid, with congenital
ichthyosis and oedema of the lower limbs as far as themid-abdomen. There were no cardiovascular or res-piratory tract abnormalities. BP 140/80 mmHg. Therewas obvious ascites, but the liver and spleen were notpalpable and there were no abnormal masses. In-vestigations showed Hb 13 6 g/dl, WBC 6-3 x 109/l,platelets 575 x 109/l, ESR 106 mm/h, blood urea1-9 mmol/l, serum creatinine 115 mmol/l, albumin15-0 g/l, globulin 260 g/l. Liver function tests,thyroid function tests, and immunoglobulins werenormal. The IVP showed poor contrast but wasotherwise normal. Proteinuria consistently exceeded5-0 g/24 h and was non-selective. The renal biopsyshowed some mesangial thickening but no otherabnormalities by light microscopy. Chest x-ray,ECG, and lung function tests were unremarkable.There was no significant increase in anti-viral anti-body titres or anti-streptolysin 0 titre. The VDRLand WR were negative. The clinical diagnosis was'minimal change nephrotic syndrome'.
Questions(1) What contribution has 'clinical immunology' to
make to elucidating the cause and deciding themanagement of this patient's disease?
(2) If you decided that complement studies, forexample, were necessary and that the renal biopsyshould also be examined by immunofluorescenceand electron microscopy, who would undertakethese investigations and interpret the results?
CASE 9 is a 48-year-old female white physicianborn in Portugal, with Raynaud's phenomenon sinceage 42. Two years later she developed epigastricpain while working in Rio de Janeiro, and over thenext two years the symptoms worsened with pro-gressive dysphagia. For the last year of this periodshe suffered recurrent chest infections.At the age of 46 hiatus hernia repair was attemp-
ted. Forty-eight hours postoperatively she developedpulmonary embolism of both lungs. She was treatedwith anticoagulants and improved clinically. How-ever in the next four weeks the dyspnoea returned;the heart size increased radiologically with a peri-cardial effusion. Her dyspnoea continued and herPG2 did not rise above 60 mmHg while breathingroom air. Right heart catheterisation revealed pul-monary arterial hypertension but no evidence ofpericardial tamponade or constriction. On admissionone month later to Northwick Park Hospital therewas no change in her condition. The patient wasnaturally dark-skinned with areas of hyper- and
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from

282
hypo-pigmentation. Striae and maculopapularlesions suggested lichen sclerosus et atrophicus ormorphoea to the dermatologist.
There was congestive cardiac failure with pul-monary hypertension. Haematological investigationswere normal and there were no biochemical abnor-malities of note. Serum immunoglobulin concentra-tions were normal. There were no renal abnormalities.Scales from the skin lesions on the fingers grewepidermophyton floccosum. Skin biopsy showedlichen sclerosus et atrophicus. Lung function testsshowed a severe diffusion defect.
QuestionsThe two most important diagnoses considered duringthis admission were systemic sclerosis and thrombo-embolic disease with pulmonary hypertension. She hasbeen seen by general physicians, rheumatologists, anddermatologists. Do you think that a 'clinical immu-nologist' would help to clarify the problem and whatwould you expect of this person?
CASE 10 is a 70-year-old retired carpenter. Hisillness began at the age of 58 as a mixed motor andsensory neuropathy of all four limbs. There havebeen no systemic symptoms of note. There is no pastmedical or family history of significance. He hasworked exclusively in the house-building industryand has had no obvious exposure to toxins or heavymetals. He had received no regular drug treatmentbefore the start of this illness and denies taking anyunauthorised medication. He smoked heavily up to1974 (120 cigarettes daily) but has drunk alcoholsparingly.
All abnormalities were confined to the centralnervous system. There was no intellectual deteriora-tion and the cranial nerves were intact. There wassymmetrical weakness and wasting of the muscles inboth the upper and lower limbs, more markeddistally. There was sensory impairment affecting allmodalities in the same distribution as the motorchanges. The clinical diagnosis was a chronic de-myelinating polyneuropathy. Investigations showedHb 16-2 g/dl with normal red cell indices, WBC9 x 109/l, with a normal differential, ESR 27 mm andtotal serum globulin 33 g/l, IgG 7-4 g/l, IgA 1-9 g/l,IgM 7-2 g/l.Other biochemical tests, serum B12 and folate con-
centrations were normal. The WR and VDRLwere negative in the blood and CSF; no excessiveporphyrinuria was detected. Bone x-rays and scanswere normal, and a computerised body scan showedno evidence of a neoplasm. The only CSF abnor-mality was an increase of protein (Il75 g/l). AnEMG showed severely impaired conduction in the
Denman
right median and right ulnar nerves, and a suralnerve biopsy revealed severe demyelinating changeswithout inflammatory reaction or infiltration.
QuestionsThe only clue to the aetiology of this polyneuropathyis the high serum IgM concentration.(1) Is this clue worth pursuing?(2) Who should do the pursuing?(3) Are such results of practical importance?(4) Do you recognise a sub-specialty termed 'neuro-
immunology'? If you knew of a 'neuroimmunolo-gist' would you seek his/her advice?
Results
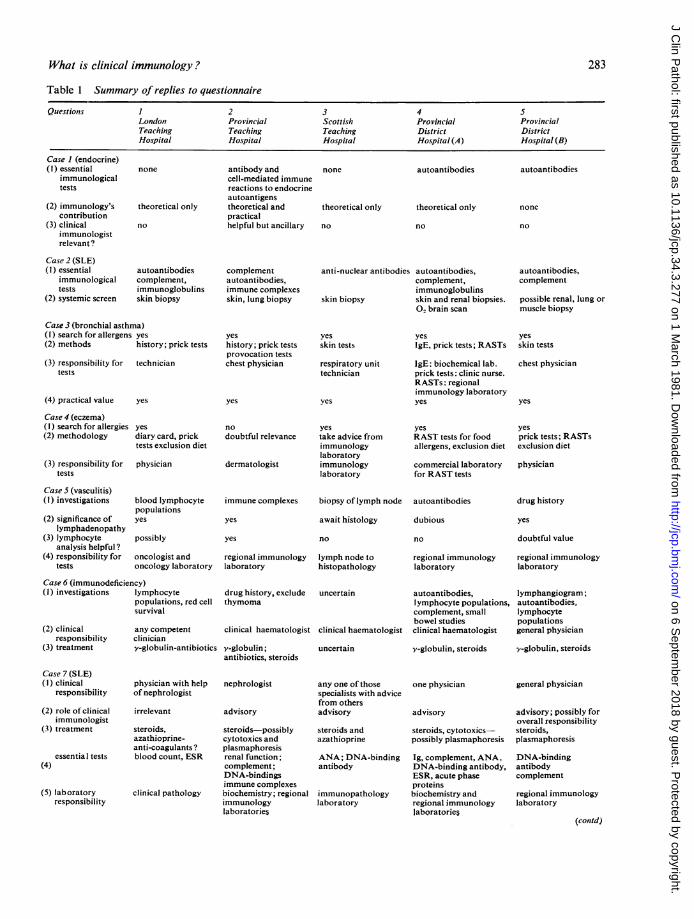
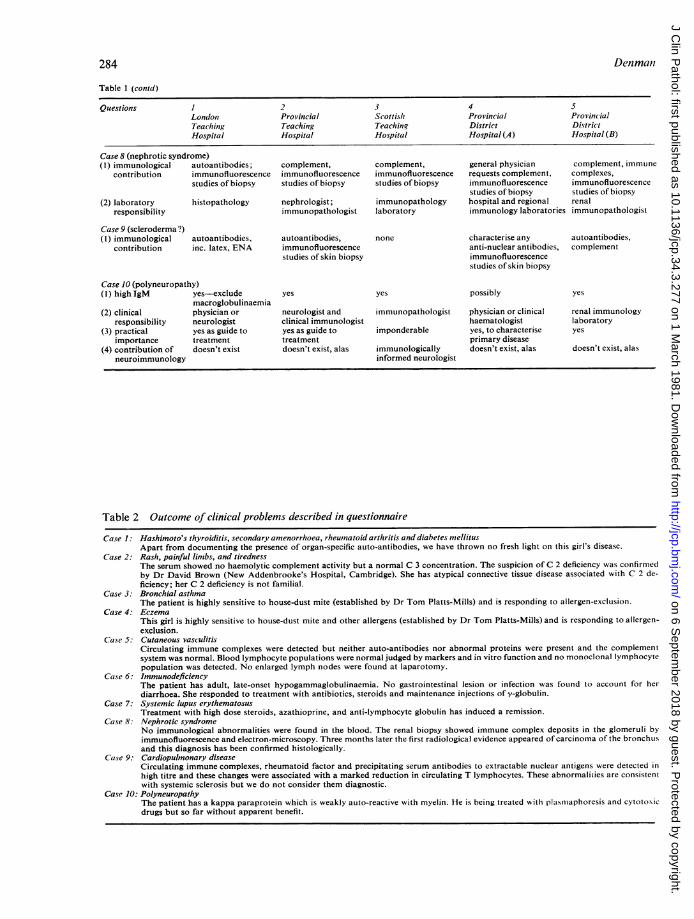
The results of enquiry are summarised in Table 1and the outcome of the clinical problems in Table 2.The results allow some provisional conclusions to bedrawn. All 5 physicians had clear ideas about whichinvestigations they thought necessary from their ownknowledge and experience. In some instances theirappraisal of current immunological practice wouldlead to firm action. Thus all 5 physicians were pre-pared to search for specific allergens in patient 3with bronchial asthma, and only one of the five wasnot prepared to embark on a similar exercise inpatient 4 with intractable eczema. All the respon-dents had personal preferences for certain tests wheninvestigating patients with inflammatory connectivetissue diseases rather than adopting the completegamut of available tests. This was reflected bydiffering predilections for complement determination,measurement of circulating immune complexes, orvarious autoantibody assays in patient 2 with sus-pected systemic lupus erythematosus. Similarlythere was no blanket request for immunologicaltests to monitor the progress of patient 7 withobvious systemic lupus erythematosus. It was alsoevident that the physicians had adopted an informedbut cautious attitude towards other tests. There waslittle enthusiasm for assaying blood lymphocytepopulations in patient 5 with a suspected lymphoma,or autoantibodies in patient 9 in whom the clinicalarguments in favour of diagnosing systemic sclerosisor thromboembolic disease were finely balanced.
Their informed attitude towards immunologicaltests was reflected in firm ideas about clinical re-sponsibility. There was a strong preference for leavingsuch responsibility in the hands of traditionallytrained specialists. Thus no one was prepared todelegate the care of patient 1 with multiple endocrineproblems to a clinical immunologist whatever thatperson's claims to understand the abstrusities ofgenetic susceptibility to these diseases. Similarly noone believed that a clinical immunologist was more
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
What is clinical immunology?
Table 1 Summary of replies to questionnaire
Questions 1 2 3 4 5London Provincial Scottish Provincial ProvincialTeaching Teaching Teaching District DistrictHospital Hospital Hospital Hospital (A) Hospital (B)
Case I (endocrine)(1) essential
immunologicaltests
(2) immunology'scontribution
(3) clinicalimmunologistrelevant ?
Case 2 (SLE)(I) essential
immunologicaltests
(2) systemic screen
none antibody andcell-mediated immunereactions to endocrineautoantigens
theoretical only theoretical andpractical
no helpful but ancillary
autoantibodiescomplement,immunoglobulinsskin biopsy
complementautoantibodies,immune complexesskin, lung biopsy
none autoantibodies
theoretical only
no
theoretical only
no
anti-nuclear antibodies autoantibodies,complement,immunoglobulins
skin biopsy skin and renal biopsies.O. brain scan
autoantibodies
none
no
autoantibodies,complement
possible renal, lung ormuscle biopsy
Case 3 (bronchial asthma)(I) search for allergens yes
(2) methods history; prick tests
(3) responsibility for techniciantests
(4) practical value yes
Case 4 (eczema)(I) search for allergies yes
(2) methodology diary card, pricktests exclusion diet
(3) responsibility for physiciantests
Case 5 (vasculitis)(I) investigations blood lymphocyte
populations(2) significance of yes
lymphadenopathy(3) lymphocyte possibly
analysis helpful ?(4) responsibility for oncologist and
tests oncology laboratory
Case 6 (immunodeficiency)(I) investigations lymphocyte
populations, red cellsurvival
(2) clinical any competentresponsibility clinician
(3) treatment v-globulin-antibiotics
Case 7 (SLE)(I) clinical physician with help
responsibility of nephrologist
(2) role of clinical irrelevantimmunologist
(3) treatment steroids,
(4)
azathioprine-anti-coagulants?
essential tests blood count, ESR
(5) laboratoryresponsibility
clinical pathology
yeshistory; prick testsprovocation testschest physician
yes
no
doubtful relevance
dermatologist
immune complexes
yes
yes
regional immunologylaboratory
drug history, excludethymoma
clinical haematologist
v-globulin;antibiotics, steroids
nephrologist
advisory
steroids-possiblycytotoxics andplasmaphoresisrenal function;complement;DNA-bindingsimmune complexesbiochemistry; regionalimmunologylaboratories
yesskin tests
respiratory unittechnician
yes
yestake advice fromimmunologylaboratoryimmunologylaboratory
biopsy of lymph node
await histology
no
lymph node tohistopathology
uncertain
clinical haematologist
uncertain
any one of thosespecialists with advicefrom othersadvisory
steroids andazathioprine
ANA; DNA-bindingantibody
immunopathologylaboratory
yesIgE, prick tests; RASTs
IgE: biochemical lab.prick tests: clinic nurse.RASTs: regionalimmunology laboratoryyes
yesRAST tests for foodallergens, exclusion diet
commercial laboratoryfor RAST tests
autoantibodies
dubious
no
regional immunologylaboratory
autoantibodies,Iymphocyte populations,complement, smallbowel studiesclinical haematologist
v-globulin, steroids
one physician
advisory
steroids, cytotoxics-possibly plasmaphoresis
Ig, complement, ANA,DNA-binding antibody,ESR, acute phaseproteinsbiochemistry andregional immunologylaboratories
yesskin tests
chest physician
yes
yesprick tests; RASTsexclusion diet
physician
drug history
yes
doubtful value
regional immunologylaboratory
lymphangiogram;autoantibodies,lymphocytepopulationsgeneral physician
y-globulin, steroids
general physician
advisory; possibly foroverall responsibilitysteroids,plasmaphoresis
DNA-bindingantibodycomplement
regional immunologylaboratory
(contd)
283
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
Denman284
Table 1 (contd)
Questions 1 2 3 4 5London Provincial Scottish Provincial ProvincialTeaching Teaching Teaching District DistrictHospital Hospital Hospital Hospital (A) Hospital (B)
Case 8 (nephrotic syndrome)(I) immunological autoantibodies; complement, complement, general physician complement, immune
contribution immunofluorescence immunofluorescence immunofluorescence requests complement, complexes,studies of biopsy studies of biopsy studies of biopsy immunofluorescence immunofluorescence
studies of biopsy studies of biopsy(2) laboratory histopathology nephrologist; immunopathology hospital and regional renal
responsibility immunopathologist laboratory immunology laboratories immunopathologist
Case 9 (scleroderma?)(I) immunological autoantibodies, autoantibodies, none characterise any autoantibodies,
contribution inc. latex, ENA immunofluorescence anti-nuclear antibodies, complementstudies of skin biopsy immunofluorescence
studies of skin biopsy
Case 10 (polyneuropathy)(1) highIgM yes-exclude yes yes possibly yes
macroglobulinaemia(2) clinical physician or neurologist and immunopathologist physician or clinical renal immunology
responsibility neurologist clinical immunologist haematologist laboratory(3) practical yes as guide to yes as guide to imponderable yes, to characterize yes
importance treatment treatment primary disease(4) contribution of doesn't exist doesn't exist, alas immunologically doesn't exist, alas doesn't exist, alas
neuroimmunology informed neurologist
Table 2 Outcome of clinical problems described in questionnaire
Case 1: Hashimoto's thyroiditis, secondary amenorrhoea, rheumatoid arthritis and diabetes nmellitusApart from documenting the presence of organ-specific auto-antibodies, we have thrown no fresh light on this girl's disease.
Case 2: Rash, painful limbs, and tirednessThe serum showed no haemolytic complement activity but a normal C 3 concentration. The suspicion of C 2 deficiency was confirmedby Dr David Brown (New Addenbrooke's Hospital, Cambridge). She has atypical connective tissue disease associated with C 2 de-ficiency; her C 2 deficiency is not familial.
Case 3: Bronchial asthmaThe patient is highly sensitive to house-dust mite (established by Dr Tom Platts-Mills) and is responding to allergen-exclusion.
Case 4: EczemaThis girl is highly sensitive to house-dust mite and other allergens (established by Dr Tom Platts-Mills) and is responding to allergen-exclusion.
Case 5: Cutaneous vasculitisCirculating immune complexes were detected but neither auto-antibodies nor abnormal proteins were present and the complementsystem was normal. Blood lymphocyte populations were normal judged by markers and in vitro function and no monoclonal lymphocytepopulation was detected. No enlarged lymph nodes were found at laparotomy.
Case 6: ImmunodeficiencyThe patient has adult, late-onset hypogammaglobulinaemia. No gastrointestinal lesion or infection was found to account for herdiarrhoea. She responded to treatment with antibiotics, steroids and maintenance injections of y-globulin.
Case 7: Systemic lupus erythematosusTreatment with high dose steroids, azathioprine, and anti-lymphocyte globulin has induced a remission.
Case 8: Nephrotic syndromeNo immunological abnormalities were found in the blood. The renal biopsy showed immune complex deposits in the glomeruli byimmunofluorescence and electron-microscopy. Three months later the first radiological evidence appeared of carcinoma of the bronchusand this diagnosis has been confirmed histologically.
Case 9: Cardiopulmonary diseaseCirculating immune complexes, rheumatoid factor and precipitating serum antibodies to extractable nuclear antigens were detected inhigh titre and these changes were associated with a marked reduction in circulating T lymphocytes. These abnormalities are consistentwith systemic sclerosis but we do not consider them diagnostic.
Case 10: PolyneuropathyThe patient has a kappa paraprotein which is weakly auto-reactive with myelin. He is being treated with plasniaphoresis and cytotoxicdrugs but so far without apparent benefit.
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from
What is clinical immunology?
qualified than a physician or a clinical haematologistto look after case 6 with immunodeficiency. Therewas a similar reluctance to accept that a clinicalimmunologist should undertake the management ofpatients with systemic lupus erythematosus, un-deniably the queen of immunological disturbances.Attitudes towards the care of case 10 with poly-neuropathy were also conservative; three of the fivephysicians felt that a competent neurologist shouldbe able to master any additional complexities im-munology might add to that already formidablyintellectual discipline.
Finally these physicians would be able to get thesetests carried out although the practical arrangementswould be different in each hospital. The majority ofthe tests considered necessary in patients 3 and 4with disorders of immediate hypersensitivity wouldbe carried out by the physicians themselves and theremainder in their clinical pathology laboratories.However in many hospitals radioallergosorbenttests (RASTs) are sent to commercial laboratories.The immunological tests in patient 5 with vasculitis,patient 7 with systemic lupus erythematosus, patient8 with the nephrotic syndrome, and patient 10 with apolyneuropathy, would be widely distributed amongexisting laboratories of clinical pathology andlaboratories more specifically devoted to immun-ology. It is noteworthy that the tests undertaken byimmunological laboratories are almost exclusivelyserological procedures involving the detection ofautoantibodies, complement measurement, and thehandling of biopsies, rather than the less well estab-lished procedures involving lymphocyte function.Indeed the one specific request that blood lympho-cyte populations should be investigated in patient5 with vasculitis is the responsibility of thedepartment of oncology in the hospital concerned.
Nevertheless all five physicians welcomed theestablishment of specialised laboratories of immu-nology and immunopathology and would seek theadvice that the consultant staff at such laboratoriescould give with more complicated problems. Recourseto this kind of assistance was reflected particularly inthose problems which are less commonly encoun-tered in recognised clinical specialties. Thus three ofthe five would use the services of their regionalimmunology laboratory in investigating the problemsof patient 5 with vasculitis. There would be a similardependence on the opinion of a specialist immuno-pathologist in interpreting the renal biopsy in patient8 with the nephrotic syndrome, and indeed immuno-fluorescence studies were considered an essentialpart of evaluating such biopsies. Although there wasless unanimity of opinion with respect to the moreunfamiliar problems of patient 6 with immuno-deficiency complicated by haemolytic anaemia, all
but one of the clinicians would seek the advice of aneuroimmunopathologist in investigating patient 10with polyneuropathy if such a specialist wereavailable.
Discussion
This study suggests that physicians accept the re-sponsibility for mastering those aspects of immun-ology which are relevant to their clinical interests.Their insight into such immunopathological mechan-isms as immediate hypersensitivity reactions andimmune complex deposition means that they do notdepend on immunologists for managing diseasessuch as chronic eczema, bronchial asthma, andsystemic lupus erythematosus. Moreover theyexpress precise preferences for immunological testsrather than simply reiterating a list of all the possibletests that have been advocated. Indeed immunolo-gists may wryly conclude that the many symposiaand textbooks devoted to teaching immunologyto clinicians have been too successful.There are few situations in which physicians see
the need for transferring clinical responsibility toimmunologists in the way that particular patientscome under the care ofrecognised medical specialists.There are complicated problems of the kind includedin this questionnaire for whose solution immunolo-gists' opinions are welcomed. Almost invariablythese relate to the choice of relevant tests, the inter-pretation of the results, and their practical applica-tion. Immunologists are seen to act in an advisorycapacity, and their specialised contribution is con-cerned primarily with directing the laboratory in-vestigations.
All the hospitals concerned have made provisionfor carrying out a limited number of essential im-munological tests. These are predominantly serologi-cal or involve the analysis of biopsy material. Therewas little indication that clinicians see the need forthose tests of lymphocyte function which loom solargely in the thoughts of academic immunologistswhen they consider clinical problems. There isobviously much local variation in the way specifictests are allocated to different laboratories: comple-ment levels, for example, are measured by the bio-chemistry laboratory in some hospitals and by theregional immunopathology centre in others. How-ever it is likely that most immunological tests areperformed in regional immunology centres.
This survey therefore leaves the strong impressionthat clinicians regard immunology as a form ofclinical practice based on the laboratory and itsconsultant staff. This is supported by the most recentanalysis3 which lists immunopathology as a recog-nised specialty: there are 35 consultants in this
285
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from

286 Denman
specialty constituting nearly 3% of the 1259 special-ists in the different branches of general and clinicalpathology. Moreover immunopathology is now arecognised subject for the membership examinationof the Royal College of Pathologists. Converselyclinical immunology is not listed as a medicalspecialty in the 1980 report, and the Royal College ofPhysicians has only this year4 announced its intentionof laying down a training programme in clinicalimmunology as part of specialist training in generalmedicine.There are obvious clinical advantages if physicians
are familiar with those immunological advanceswhich affect their own specialty. Similarly it is moreeconomical and convenient if existing departmentsof clinical pathology incorporate standard immuno-logical techniques in their working programmes. Onthe other hand our ability to analyse and controlimmunopathological events will only improve ifspecialised immunopathology laboratories arelargely responsible for immunological tests. Suchlaboratories are in a better position to test andexploit improved techniques in collaboration withresearch laboratories. The diagnosis of C2 deficiencyin patient 2 illustrates this point.As methods for immunological intervention be-
come more sophisticated it is also conceivable thattheir application to medicine will need the servicesof clinicians exclusively engaged in this task. Thiswill certainly be the case in academic centres, forexample, in the context of regulating undesirableimmune reactions with appropriate antisera to anti-gens on abnormal B lymphocyte populations or to
the idiotypes these cells express. At present howeverclinical practice is almost exclusively organised interms of diagnosing and treating patients attendingtraditional specialist clinics. Patients with allergyattributable to disorders of immediate hypersensi-tivity are perhaps the only group whose clinicalproblems can be defined almost entirely in immuno-logical terms. Unhappily allergy is a subject whichfails to appear in the list of clinical specialties recog-nised by the Department of Health and SocialSecurity.
I am extremely grateful to Dr JD Briggs, DrRC Godfrey, Professor M Lessof, Dr A Paton,and Dr AJ Swannell for their invaluable, detailed,and good-humoured response to the questionnaire.
I am grateful to Drs Geoffrey Asherson, GeraldLoewi, Tom Platts-Mills, and David Webster formany years of (discontinuous) discussion concerningthe definition of clinical immunology.
References
Simons MJ. How to use an immunology laboratory. Med JAust 1976;2:643-6.
2Bellanti JA. Diagnostic applications of immunology. In:Bellanti JA, ed. Immunology II. Philadelphia: Saunders,1978 ;758-75.
3DHSS. Medical staffing and prospects in the NHS in Eng-land and Wales 1979. Health Trends 1980;12:51-4.
4Royal College of Physicians. 3rd report on HigherMedical Training. 1980.
Requests for reprints to: Dr AM Denman, ConnectiveTissue Diseases Research Group, Clinical ResearchCentre, Watford Road, Harrow, Middlesex HAI 3UJ.
on 6 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.34.3.277 on 1 M
arch 1981. Dow
nloaded from