what’s the big deal about veins? - capanet.org · •let’s become cnizant of the fact that...
TRANSCRIPT

What’s the Big Deal
About Veins?
• Risk Factor Modification
• CAD
• Myocardial Disease
• Valvular Disease
• Conduction Abnormalites
• PAD
Disorders of the Heart
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA
Venous Disease• DVT prophylaxis or its treatment
• Pulmonary Embolus
• Hypercoagulable states
• Congenital Venous Malformations
• Anticoagulation
Coronado Vein Center, Redding CA
Chronic Venous Insufficiency and Varicose Veins

Skin UlcersSwollen Legs Skin Changes Varicose Veins
Photos courtesy of Rajabrata Sarkar, MD, PhD.
Manifestations of Venous
Insufficiency
Coronado Vein Center, Redding CA
The inability of the vein in the lower extremities to return blood back to the heart
Venous Insufficiency Defined:
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA

Pathophysiology of Venous
Insufficiency
Coronado Vein Center, Redding CA
Venous System
Coronado Vein Center, Redding CA
Three Systems:
•Deep
•Superficial
•Perforating

Venous System
Coronado Vein Center, Redding CA
• Venous Hypertension
• Leukocyte Trapping
• Release of Proteolytic Enzymes
• Destruction of CBM
• Leakage of Plasma Proteins
• Tissue Hypoxia
• Dermatitis & Lipodermatosclerosis
Coronado Vein Center, Redding CA
Magnitude of the Problem
PREVALENCE
IGNORED
MISDIAGNOSED
Coronado Vein Center, Redding CA
0 10 20 30 40
Alzheimers
Stroke
Cancer
Coronary Heart Disease
Peripheral Arterial Disease
Diabetes
Venous Reflux Disease
US Prevalence of Major Diseases-2015
(in millions)
Coronado Vein Center, Redding CA
Recognize the true suffering…
PATIENTS
ALL OF YOU
COUNTRY
Images courtesy of Paul McNeill, MD and Rajabrata Sarkar, MD
Nearly 40 million people suffer from
venous reflux disease and varicose veins
Coronado Vein Center, Redding CA
Venous Reflux disease is 5x more prevalent than PAD, 2x more
prevalent than CAD
•Only 1.7 million seek treatment annually!
•Over 36 million go untreated!
Of the estimated 38 million people with
symptomatic superficial venous reflux.
Coronado Vein Center, Redding CA
• Increase the awareness!
• Eliminate the misconception that this is just a cosmetic disorder
• Remind the patients that, in the right hands, this has a straightforward cure
• Come to the realization that disorders such as unexplained swelling, nocturnal leg cramps, and restless legs are not treated by telling patients “there is nothing we can do that really works”
• Let’s become cognizant of the fact that these patients suffer every minute of the day, not just when they are in your office complaining about the symptoms
Coronado Vein Center, Redding CA
To Improve These Statistics:
•Heredity
•Occupation
•Pregnancy
•Obesity
•Gender
•Age•Sedentary Lifestyle
Risk Factors of Venous
Insufficiency
Coronado Vein Center, Redding CA
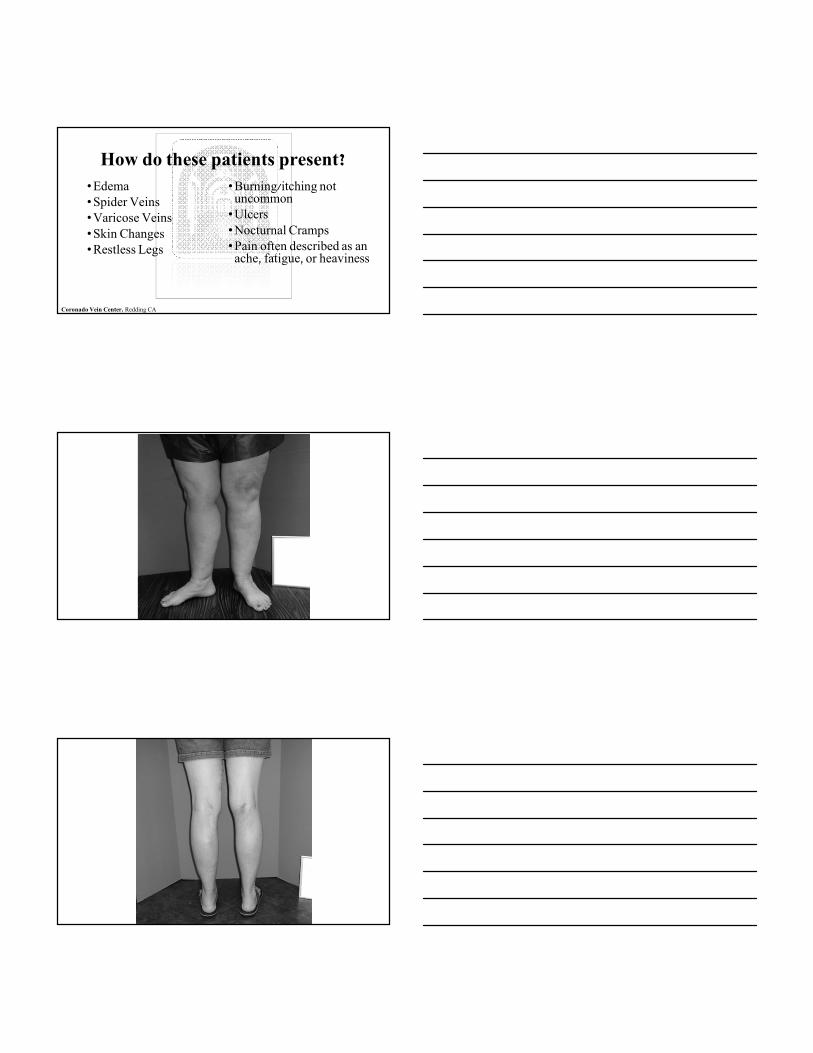
• Edema
• Spider Veins
• Varicose Veins
• Skin Changes
• Restless Legs
• Burning/itching not uncommon
• Ulcers
• Nocturnal Cramps
• Pain often described as an ache, fatigue, or heaviness
How do these patients present?
Coronado Vein Center, Redding CA
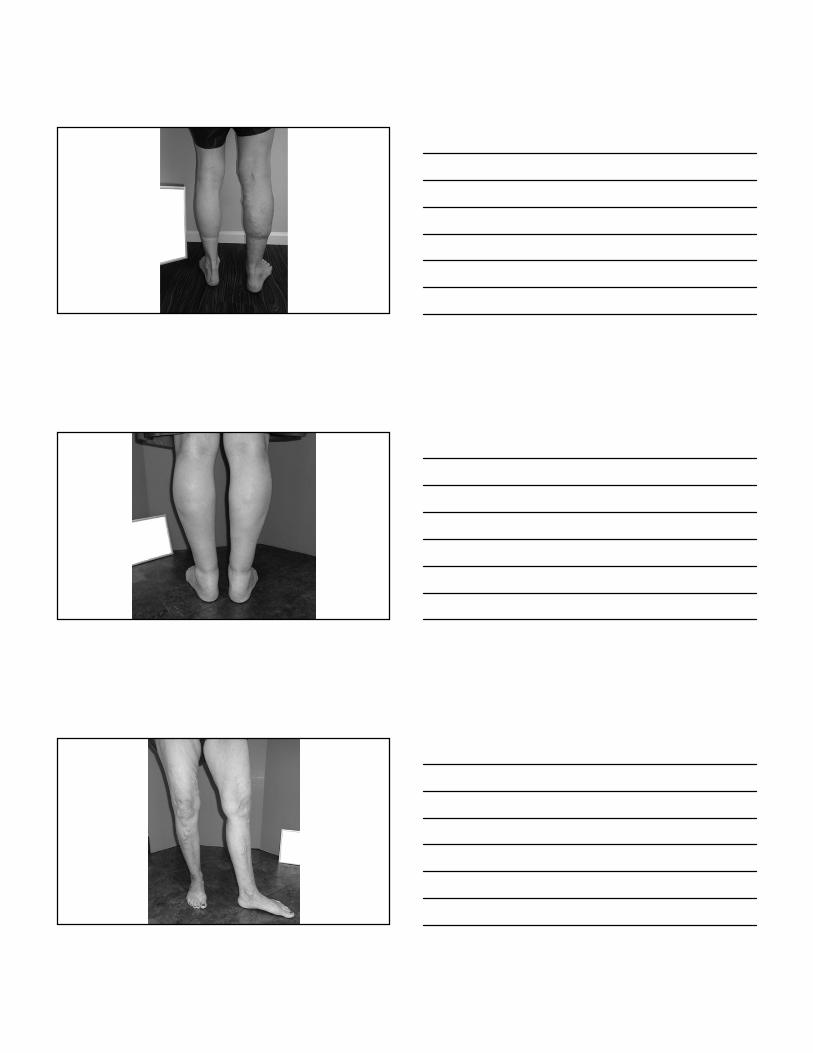
• Antegrade flow: Blood flow toward the heart
• Patency: Vessel is clear of obstruction and flow is present
• Compression: Vein wall collapses when pressure applied over vein with transducer
• Occlusion: Complete closure of a vessel with no flow present
• RETROGRADE FLOW: Blood flow away from the heart
Diagnosis
Coronado Vein Center, Redding CA
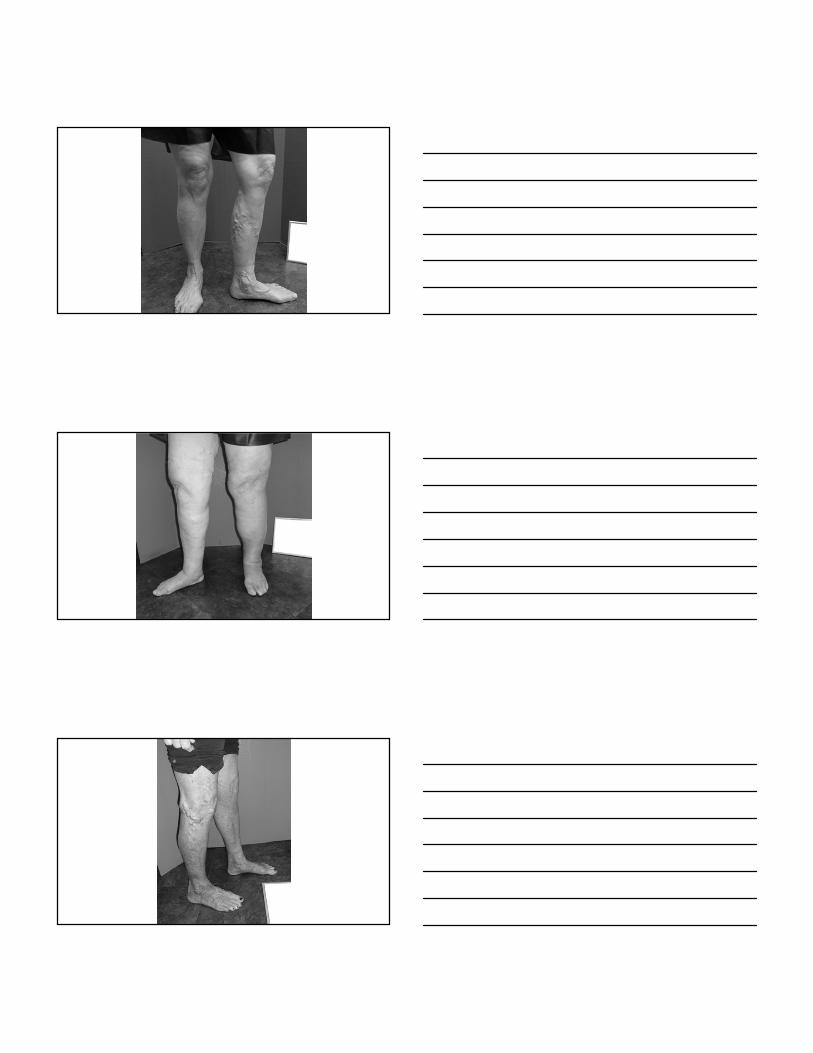
Distal Augmentation
Coronado Vein Center, Redding CA
Normal valve closure after augmentation
Abnormal valve closure after
augmentation
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA
• Detoxified by Liver• Cleared or filtered by kidneys• Oxygenated and CO2
removed by lungs• Not cleared of dying
red/white blood cells by spleen
•Thermal Ablation•Radiofrequency
•Laser
•Chemical
Endovascular Techniques
Coronado Vein Center, Redding CA
•Archaic
•Barbaric
•Obsolete
Surgical Intervention
Coronado Vein Center, Redding CA
Coronado Vein Center, Redding CA
• Detoxified by Liver• Cleared or filtered by kidneys• Oxygenated and CO2
removed by lungs• Not cleared of dying
red/white blood cells by spleen
• You can expect your patient to have complete resolution of the symptomatology related to venous insufficiency
• You can expect a decrease in the incidence of complications related to DVT, venous ulcerations, unnecessary hospitalizations and antibiotic treatments
• You can expect that patients who have restless legs or nocturnal cramps due to venous insufficiency (large portion) can come off of the medications that were unnecessary to begin with
• You can expect your venous insufficiency population to be much happier with their care
• You can expect to be happier by improving the flow of your patients
What to expect?
Coronado Vein Center, Redding CA
Case Presentations
Coronado Vein Center, Redding CA
HPI: 60y/o Female, RN who responded to DTCA Frustrated with LE edema FOR OVER 20 YEARS, puffiness, heaviness, aching at end of day. Had been treated with lasix empirically for over a decade.
PmHx: DM, HTN, sleep apnea
Medications:Metformin 500mg, bid Lipitor 40mg, qhsCaptopril 25mg, bidAspirin 81mg, qamLasix 40mg, bid
Exam 180lbs., 5’4” vitals WNL and OTW unremarkable with the exception of B 3+ pitting edema.
Case 1: Edema
Coronado Vein Center, Redding CA
“Usual Causes” of edema were nonexistent including:
• No Hx of heart failure, • No h/o renal insufficiency, • Hypoalbuminemia, • Portal or pulmonary hypertension • No TR of significance. • No calcium channel blockers, • OR ANY OTHER APARENT REASON for her edema.
Case 1: Edema
Coronado Vein Center, Redding CA

Dx workup: Included venous ultrasound which revealed severe bilateral GSV reflux.
Treatment: Radiofrequency ablation of bilateral GSV with foam sclerotherapy at 2 week intervals post RFA
Results: Since then, she has taken no Lasix in the last 3 years the iatrogenic cause of her hypokalemia! More importantly, she can sleep better and complete her standing obligation without pain and suffering! Her PMD is much happier as well not having to deal with the issue.
Case 1: Edema
Coronado Vein Center, Redding CA
HPI: 72y/o Male, businessman who responded to DTCA because of LE asymmetrical pain and discomfort described as “all night long” pinpricking and paresthesias. Unable to travel because of sx exacerbation with driving. He denied edema. “Everything would be perfect if I could just get rid of this damn pain!” He was dxed with Neuropathy despite no previous hx of DM or other known causes of neuropathy. He was experiencing severe side effects from his meds including a sensation of “being out of it” and having to hold his medications on days of meetings or presentations.
Meds: Neurontin 600 mg by mouth twice a dayCymbalta 60 mg by mouth every morningEdluar 10 mg by mouth daily at bedtimeACE – I and B-blockerASA 81 mg by mouth every morningVitamin B and D supplementsSTATINS HAD BEEN DISCONTINUED BECAUSE OF HIS LEG PAIN!
Case 2: Neuropathy
Coronado Vein Center, Redding CA
PmHx: CADHTN“Neuropathy”“Fibromyalgia”
PE: Healthy well developed gentleman. Completely unremarkable exam with the exception of tender varicosities which were asymmetrical. CV exam was unremarkable including excellent symmetrical pulses. DTRs were intact as was the remainder of his neuro exam. He had no edema
Case 2: Neuropathy
Coronado Vein Center, Redding CA

Dx : Included venous ultrasound which revealed severe right GSV and left SSV reflux
Tx: Radiofrequency ablation of right GSV and left SSV with adjunctive therapy including microphlebectomy and foam scleortherapy
F/U: Asymptomatic!, no longer takes Cymbalta or Gabapentin. No further need for B complex given for neuropathy.
TAKES STATINS!
Case 2: Neuropathy
Coronado Vein Center, Redding CA
HPI: 56y/o Male, gainfully employed who responded to DTCA because of LE pain and discomfort, discoloration and non-healing wounds of over 3 years duration. He had been evaluated and treated at a wound clinic under the care of a vascular surgeon on and off for years. He described numerous hospital admissions and countless rounds of antibiotics as well as 2 failed skin grafts.
Meds: Norco
PmHx: Negative except for the HPI
PE: Morbid obesity. B LE 2+ edema with large B 12-15 cm deep ulcerations in distal legs with pre-tibial fascia involvement and extensive areas of necrosis. Purulent exudate from the ulcer. Severe stasis dermatitis and large varicosities.
Case 3: Ulcers
Coronado Vein Center, Redding CA
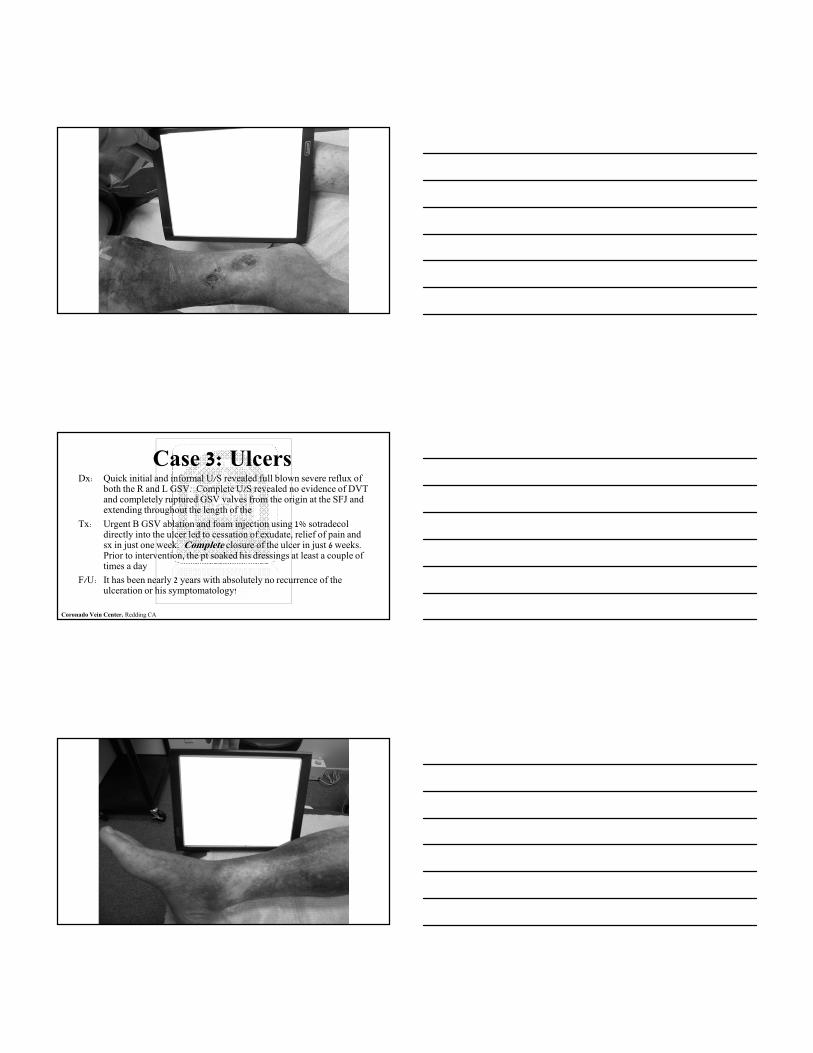
Dx: Quick initial and informal U/S revealed full blown severe reflux of both the R and L GSV. Complete U/S revealed no evidence of DVT and completely ruptured GSV valves from the origin at the SFJ and extending throughout the length of the
Tx: Urgent B GSV ablation and foam injection using 1% sotradecoldirectly into the ulcer led to cessation of exudate, relief of pain and sx in just one week. Complete closure of the ulcer in just 6 weeks. Prior to intervention, the pt soaked his dressings at least a couple of times a day
F/U: It has been nearly 2 years with absolutely no recurrence of the ulceration or his symptomatology!
Case 3: Ulcers
Coronado Vein Center, Redding CA
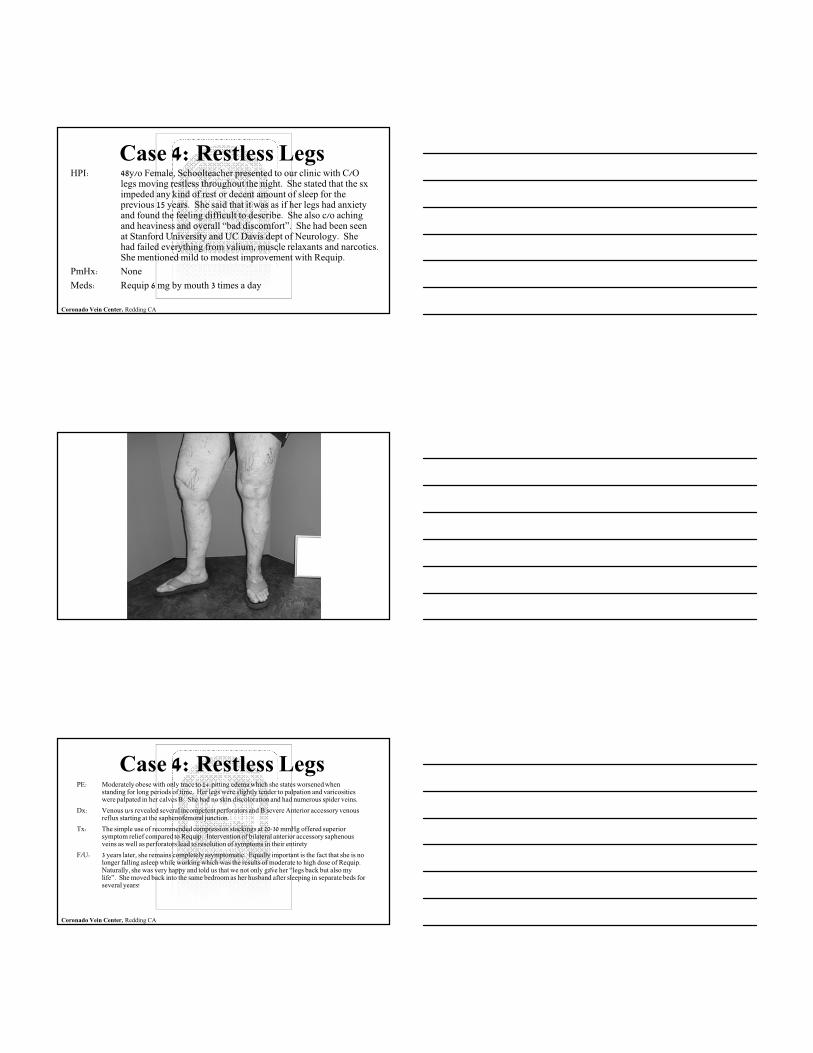
HPI: 48y/o Female, Schoolteacher presented to our clinic with C/O legs moving restless throughout the night. She stated that the sximpeded any kind of rest or decent amount of sleep for the previous 15 years. She said that it was as if her legs had anxiety and found the feeling difficult to describe. She also c/o aching and heaviness and overall “bad discomfort”. She had been seen at Stanford University and UC Davis dept of Neurology. She had failed everything from valium, muscle relaxants and narcotics. She mentioned mild to modest improvement with Requip.
PmHx: None
Meds: Requip 6 mg by mouth 3 times a day
Case 4: Restless Legs
Coronado Vein Center, Redding CA
PE: Moderately obese with only trace to 1+ pitting edema which she states worsened when standing for long periods of time. Her legs were slightly tender to palpation and varicosities were palpated in her calves B. She had no skin discoloration and had numerous spider veins.
Dx: Venous u/s revealed several incompetent perforators and B severe Anterior accessory venous reflux starting at the saphenofemoral junction.
Tx: The simple use of recommended compression stockings at 20-30 mmHg offered superior symptom relief compared to Requip. Intervention of bilateral anterior accessory saphenous veins as well as perforators lead to resolution of symptoms in their entirety
F/U: 3 years later, she remains completely asymptomatic. Equally important is the fact that she is no longer falling asleep while working which was the results of moderate to high dose of Requip. Naturally, she was very happy and told us that we not only gave her “legs back but also my life”. She moved back into the same bedroom as her husband after sleeping in separate beds for several years!
Case 4: Restless Legs
Coronado Vein Center, Redding CA
HPI: 52-year-old police officer who presented to our Vein Center because of discomfort in his lower extremities described as aching throbbing fatigue discomfort. What really bothered him most however were debilitating leg cramps. With respect to his varicose veins, he was told previously “not to worry about them”. He responded to our advertisement regarding the frequent association of leg cramps and venous insufficiency.
Meds: None
PmHx: None
PE: His physical examination revealed a muscular well-developed gentleman with normal vital signs and an unremarkable exam with the exception of obvious varicose veins, 2+ pitting edema and mild stasis dermatitis just proximal to the ankles bilaterally
Dx: Venous ultrasonography was negative with the exception of bilateral Vein of Giacomini severe reflux.
Tx: He underwent radiofrequency ablation of these veins followed by extensive foam sclerotherapy and microphlebectomy in both lower extremities with complete resolution of his nocturnal leg cramps
Note: The etiology for lower extremity muscle cramps remains poorly understood. Most treatment is empiric with inconsistencies in our approach and management. The treatment varies from empiric electrolyte “replacement” to
aggressive therapy including benzodiazepines and narcotics. There are approximately38 million Americans with venous insufficiency with a large portion of these patients complaining of muscle cramps. Treatment in many of the patients that
experience debilitating cramps leads to a significant amelioration and often complete resolution of symptoms
Cramps
Coronado Vein Center, Redding CA
• How poorly venous insufficiency is understood by the medical community and how frequent it is either misdiagnosed or ignored
• How poorly we do in the recognition of venous insufficiency contributing as an etiology to common disorders like RLS, “Neuropathy” and lower extremity muscle cramps
• The degree to which misdiagnosis leads not only to lack of appropriate treatment but also to iatrogenic results.
These cases illustrate
Coronado Vein Center, Redding CA
• Knowledge of the venous system and its true physiology is still in the diaper stage
• Understand venous physiology and disorders has, and will undoubtedly continue to provide a wealth of knowledge that we believe will unlock some of the mysteries of poorly understood disease states such as HTN, sleep apnea and sepsis to name a few
• The Coronado Vein Center has taken a leading role in investigation and research
Where are we going?
Coronado Vein Center, Redding CA

•Improves quality and quantity of life
•Lowers hypertension
•Improves performance and stamina
•Produces a favorable metabolic profile
The Coronado Vein Center is attempting to
answer the question of why and how exercise:
Coronado Vein Center, Redding CA


Thank you
Coronado Vein Center, Redding CA