what you should know practice acquisitions & post
TRANSCRIPT

WHAT YOU SHOULD KNOW –PRACTICE ACQUISITIONS & POST-TRANSACTIONCOMPENSATION: A FMV PERSPECTIVE PERSPECTIVE
Bridget Triepke, CPA & Ben Ulrich, CVA
1

2
VMG Health Service LinesSimplifying FMV Complexity
VMG HEALTH FAST FACTS
100+20 25,000+
4,153
VMG HEALTH ADVANTAGE
VMG Health helps large, complex health systems aggregate valuation and transaction advisory activities resulting in operational time efficiencies and volume pricing economies that can be reallocated to more valuable, mission‐fulfilling endeavors.
VALUATION PROFESSIONALS
YEARS OF EXPERIENCE
ENGAGEMENTS
VALUATION ENGAGEMENTS IN 2015
2
• Physician Practice Industry & Intro to FMV• Summarize the healthcare landscape from both an industry and
regulatory perspective for physician practices
• Physician Practice Acquisitions• Overview of the valuation process & components of value; How
valuation methodologies are applied with current trends
• Physician Compensation• Detail the potential service agreements, value drivers, and key
considerations in physician compensation and integration
• Best Practices – Considerations for a Transaction• Overview of key points to consider in the navigation of a transaction
Presentation Agenda
3

PHYSICIAN MARKET OVERVIEW & TRENDS
4
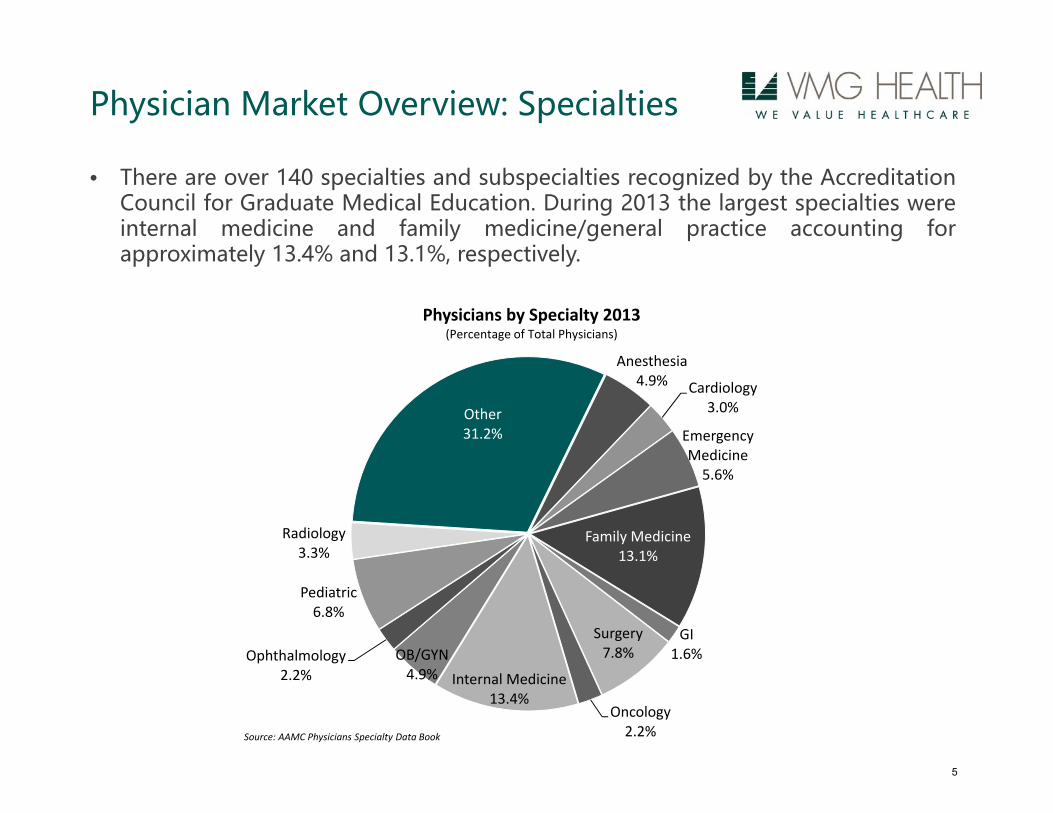
• There are over 140 specialties and subspecialties recognized by the AccreditationCouncil for Graduate Medical Education. During 2013 the largest specialties wereinternal medicine and family medicine/general practice accounting forapproximately 13.4% and 13.1%, respectively.
Physician Market Overview: Specialties
Anesthesia4.9% Cardiology
3.0%
Emergency Medicine5.6%
Family Medicine13.1%
GI1.6%
Surgery7.8%
Oncology2.2%
Internal Medicine13.4%
OB/GYN4.9%
Ophthalmology2.2%
Pediatric6.8%
Radiology3.3%
Other31.2%
Physicians by Specialty 2013(Percentage of Total Physicians)
Source: AAMC Physicians Specialty Data Book
5

• Number of Physicians has grown from approximately 400,000 in1975 to 1,000,000, in 2013; CAGR of 2.6%
Physician Market Overview: Supply
1,045,000
‐
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1975 1980 1985 1990 1995 2000 2013
Total Physicians
Source: American Medical Association Physician Characteristics and Distribution in the US, 2015 Edition
6

• 46.2 million / 14.5% over the age of 65
• 62.6 million / 19.6% over the age of 50 and will become eligible forMedicare over the next 10-15 years.
• The percentage of the population over the age of 65 is projected toincrease from 14.5% in 2014 to 16.9% by 2020 and 20.6% by 2030.
Physician Market Overview: Demand
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
Population By Age Group (2014 Census)
Source: US Census Bureau
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
22.0%
24.0%
26.0%
1980 1985 1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050 2055 2060
Age 65 and Older (% US Population)
Source: US Census Bureau
7
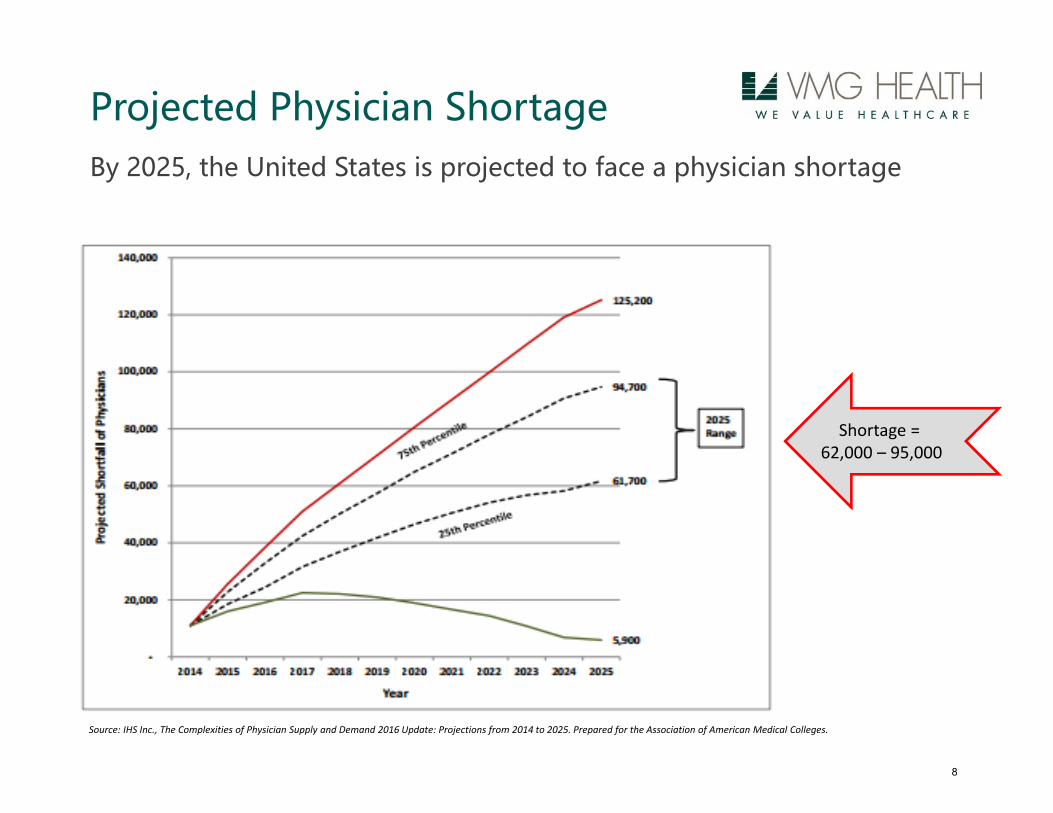
By 2025, the United States is projected to face a physician shortage
Projected Physician Shortage
Shortage =62,000 – 95,000
Source: IHS Inc., The Complexities of Physician Supply and Demand 2016 Update: Projections from 2014 to 2025. Prepared for the Association of American Medical Colleges.
8

• In most specialties, reimbursement per the Medicare Physician FeeSchedule has either been declining or below CPI
Physician Market Overview: Reimbursement Trends
CY 2014 - 2016 MPFS Final Rule ImpactSelected Specialties
Source: Federal Register
2014 2015 2016Specialty Total RVU Change Total RVU Change Total RVU Change
Total 0% ‐1% 0%Anesthesiology ‐3% 0% 0%Cardiology 1% 0% 0%Family Practice 2% 1% 0%Gastroenterology ‐2% 0% ‐4%General Surgery 0% 0% 0%Internal Medicine 1% 1% 0%Ophthalmology 0% ‐2% ‐1%Orthopedic Surgery ‐2% ‐1% 0%Radiation Oncology 1% 0% ‐2%Radiology ‐2% ‐1% 0%Urology ‐1% 0% 0%
9
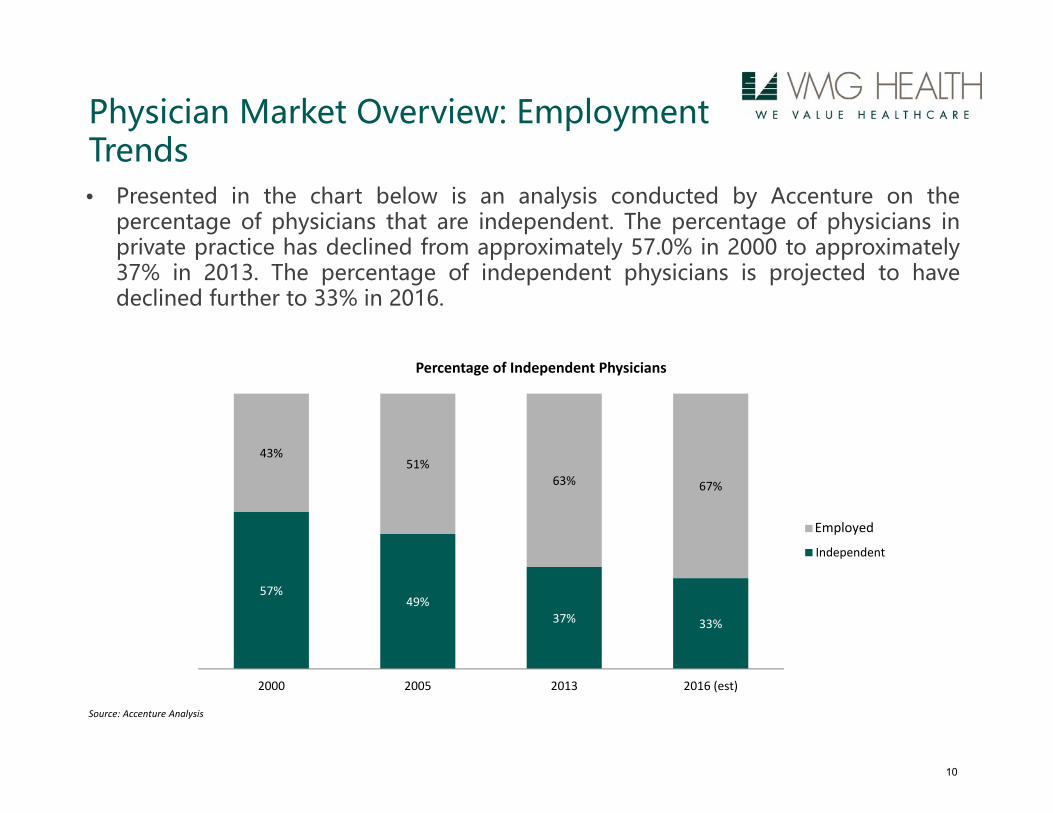
Physician Market Overview: Employment Trends• Presented in the chart below is an analysis conducted by Accenture on the
percentage of physicians that are independent. The percentage of physicians inprivate practice has declined from approximately 57.0% in 2000 to approximately37% in 2013. The percentage of independent physicians is projected to havedeclined further to 33% in 2016.
Source: Accenture Analysis
57%49%
37% 33%
43%51%
63% 67%
2000 2005 2013 2016 (est)
Percentage of Independent Physicians
Independent
Employed
10

• Driving Forces for Physicians:• Physician desire to be shielded from market forces• Reimbursement cuts – in some cases these have been drastic• Increasing costs – particularly malpractice• Increase in costly IT requirements – electronic medical records• Reaction to Healthcare Reform• Quality of life• Better Benefits• Focus on practice of Medicine and reduce administrative work
Physician Market Overview: Benefits of Alignment
11

• Driving Forces for Hospitals:• Gain and retain market share and reduce the threat of
competition• Service line development• Potentially advantageous reimbursement for ancillaries• Address physician shortages in key specialties• Call coverage needs• Healthcare Reform – Accountable Care Organizations (ACOs)• Need to improve quality of care
Physician Market Overview: Benefits of Alignment
12

WHAT IS FMV AND WHY DOES IT MATTER?
13

Amount Company Year Details of Allegations
$85m Halifax Hospital Medical Center 2013
Improperly included the value of prescription drugs and tests that oncologists ordered and Halifax billed to Medicare
Paid 3 neurosurgeons compensation in excess of Fair Market Value
$41m King’s Daughters Medical Center 2014 Cardiologist salaries in excess of Fair Market Value
$35m Columbus RegionalHealthcare System 2015
The United States alleged that between 2003 and 2013, Columbus Regional provided excessive salary and directorship payments to Dr. AndrewPippas
$21.5m Citizens Medical Center 2015
Provided compensation to several cardiologists that exceeded the fair market value of their services
Paid bonuses to emergency room physicians that improperly took into account the value of their cardiology referrals
Recent Stark/AKS Cases & Settlements
14
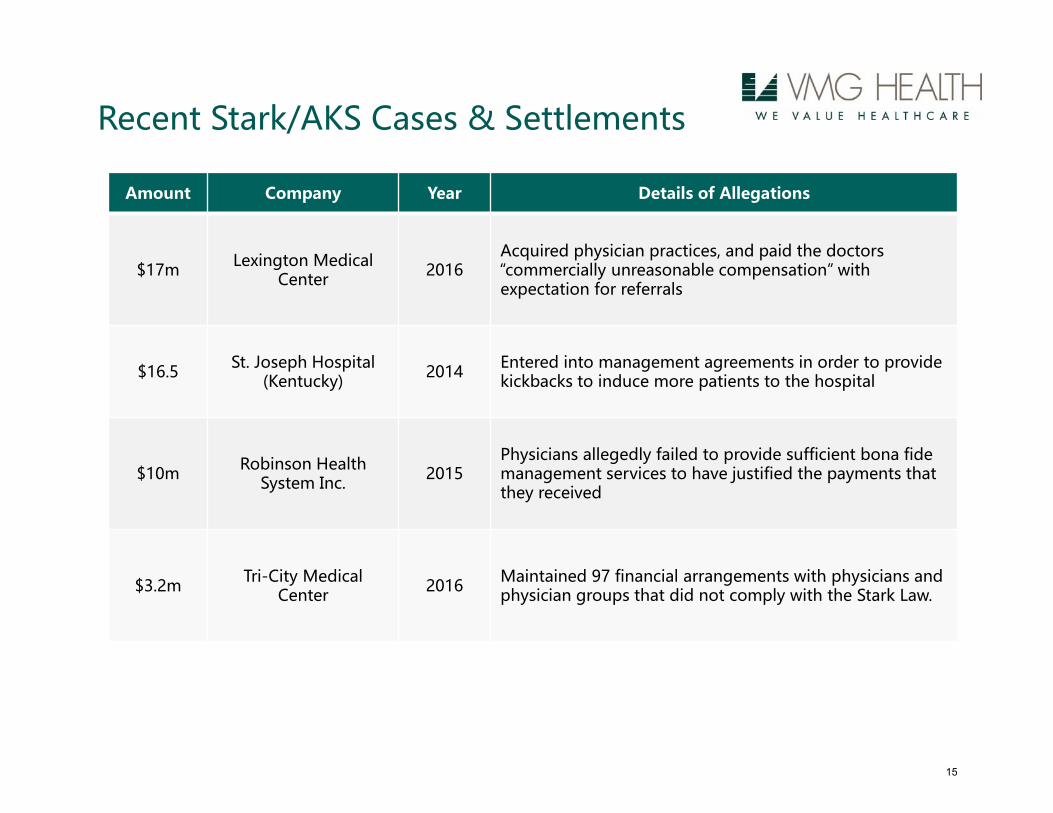
Amount Company Year Details of Allegations
$17m Lexington Medical Center 2016
Acquired physician practices, and paid the doctors“commercially unreasonable compensation” with expectation for referrals
$16.5 St. Joseph Hospital (Kentucky) 2014 Entered into management agreements in order to provide
kickbacks to induce more patients to the hospital
$10m Robinson Health System Inc. 2015
Physicians allegedly failed to provide sufficient bona fide management services to have justified the payments that they received
$3.2m Tri-City Medical Center 2016 Maintained 97 financial arrangements with physicians and
physician groups that did not comply with the Stark Law.
Recent Stark/AKS Cases & Settlements
15

• Fair Market Value (“FMV”) – the ONLY premise of value to meet theAnti-Kickback Statute and Private Inurement Regulations
• Both for-profit and not-for-profit health care providers that acceptpayments from government programs (Medicare / Medicaid) mustensure that exchanges between them and other providers are at FMV.
• Definition• IRS Revenue Ruling 59-60: The amount at which property would change
hands between a willing seller and a willing buyer when neither is actingunder compulsion and when both have reasonable knowledge of therelevant facts.”
• Stark -– similar to IRS but expanded to include General Market Value, which is the
compensation that would be included in a service agreement as the result of bonafide bargaining between well-informed parties to the agreement who are nototherwise in a position to generate business for the other party.
– Stark includes commercial reasonableness test
Regulatory Guidance
16

• Stark Law• Prohibits physicians from referring a patient to an entity with which the
physician (or an immediate family member) has a financial relationship, whenthe referral is for the furnishing of certain designated health services (DHS).
– Civil violation and restricts ownership
• Anti-Kickback Statute• Prohibits the payment or remuneration in exchange for, or in order to induce,
the referral of patients or other businesses which are reimbursed under theMedicare program.
– Criminal violation
• Federal False Claims Act• A federal statute that covers fraud involving any federally funded contract or
program (including Medicare and Medicaid). The statute contains explicitprovisions which provide a financial incentive for “whistleblowers” to makeallegations of fraud on behalf of the Government
• Private Inurement• Deals with tax-exempt entities providing excess benefits to non tax-exempt
individuals or entities
Regulatory Guidance Cont.
17

Unique Issues in JV Transactions
Fair Market Value
No buyer specific synergies
Expenses should reflect all expenses needed to operate as a freestanding
business
Revenue/reimbursement changes to reflect freestanding “market”
averages and not particular buyer
Strategic / Investment Value
Incorporates synergies to specific buyer
Unique hospital based reimbursement
Paying greater than the market could be deemed “paying for
referral”
1818

BUSINESS ENTERPRISE VALUATION APPROACHES
19

• Three Accepted Business Valuation Methods:1. Market Approach
– Guideline Public company Method and Similar Transactions Method
2. Cost Approach– Tangible and Intangible Assets
3. Income Approach– Discounted Cash Flow Method
Valuation Methods
20

• Estimates value by examining the value of similar businesses in afree and open market
• Lack of Comparable data• No publicly traded physician practices; practice transaction details are
often not disclosed
• Rarely used alone as a determinant of FMV for a physicianpractice
Market Approach
21

• Estimates the cost to replace, replicate or recreate the assetscomprising the business
• Measures value by identifying and individually valuing thebusiness’s tangible and intangible assets and liabilities
• Considered to provide a “floor” or lowest minimum value related toa business
• Typically used when the entity has projected losses or nominalprojected cash flow.
Cost Approach
22

• Typical Components…
Cost Approach
Tangible
• Working capital• Fixed assets
• limited scope• full scope
• Real estate (if applicable)
IntangibleLegally Protectable & Separately Marketable
• Trade name• Medical Records• Phone Number• Certificate of
Need• Non-Compete
23
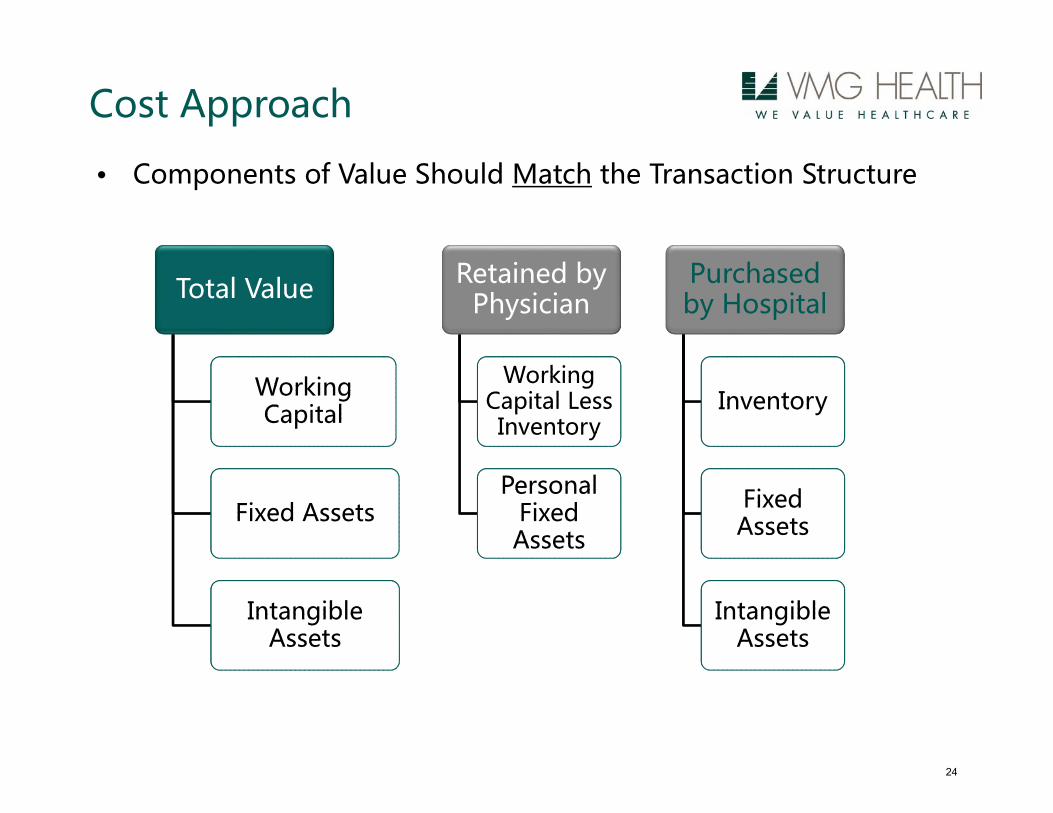
Total Value
Working Capital
Working Capital
Fixed AssetsFixed Assets
Intangible Assets
Intangible Assets
Retained by Physician
Working Capital Less
Inventory
Working Capital Less
Inventory
Personal Fixed
Assets
Personal Fixed
Assets
Purchasedby Hospital
InventoryInventory
Fixed AssetsFixed
Assets
Intangible Assets
Intangible Assets
• Components of Value Should Match the Transaction Structure
Cost Approach
24

• Projection of future revenues and expenses
• Projection of future capital expenditures and working capitalrequirements
• Discount future after tax debt free cash flows
• Single period capitalization or multi-period discounted cash flowanalysis
Income Approach
25

Considerations when Developing or Evaluating a Forecast:
Income Approach
• Planned addition of new physicians or mid-level providers
• Expected physician retirements
• Capacity constraints based on current and future work schedules
• Local competition
• Understanding of historical volume trends and fluctuations
• Expected changes in payor mix, patient population or procedure mix
• Understanding of in-office ancillary services (e.g. lab, imaging,physical therapy)
• Budgeted capital expenditures / planned replacement of equipment
• Normalizing adjustments
26
Income Approach
• Lease Rates – Is the real estate owned by a related-party?
• Staffing levels
• Employee benefits
• Excess expenses• Personal Automobile• Travel
• New contract rates for maintenance agreements or other serviceproviders
• One-time, non-recurring expenses
Common Normalizing Adjustments
27

Income Approach Illustration
Post-transaction provider compensation directly impacts forecastedcash flows and FMV of the Practice
PROFESSIONAL EARNINGS ONLY
Year 1 Year 2 Year 3 Year 4 Year 5Revenues:
Gross Fee‐for‐Service (Professional ONLY) 3,352,000 3,452,560 3,556,137 3,662,821 3,772,706 Adjustments & Refunds (1,856,000) (1,911,680) (1,969,030) (2,028,101) (2,088,944)
Total Net Operating Revenues 1,496,000 1,540,880 1,587,106 1,634,720 1,683,761
Operating Expenses:Total Operating Expenses 1,006,000 1,037,000 1,070,000 1,103,000 1,138,000
Operating Margin 490,000 503,880 517,106 531,720 545,761
Pre‐Compensation Earnings 490,000 503,880 517,106 531,720 545,761
Provider Compensation 459,734 472,734 485,092 498,775 511,895 Provider Compensation 392,000 403,000 414,000 425,000 437,000 Provider Benefits 67,000 69,000 71,000 73,000 75,000
Total Provider Compensation 459,000 472,000 485,000 498,000 512,000
Distributable Cash Flow Available to Buyer 31,000 31,880 32,106 33,720 33,761
Projection Period
28
Income Approach
– Upfront purchase price is highly dependent on go-forward compensationstructure
– All else equal, less compensation equals higher purchase price– Earnings that are paid for up front for any ancillary services should not be
considered in the post-transaction compensation – no double dipping
Physician Compensation
29

PHYSICIAN COMPENSATION ARRANGEMENTS
30

Compensation Arrangement Types & Trends
*P4P component – newest challenges for determining FMV^Non-physicians providing services through a physician owned entityVarying internal processes for setting compensation across country
Administrative Services*^ Call Coverage*
Co-management(fixed +
variable)*^
Subsidy/Hospital Coverage*^
P4P, Bundled, & ACO Payment
models*
PSA Model($/WRVU + expenses)*
Professional/ technical splits Clinical Services*
Billing and Collection
ManagementDevelopment^
Medical Director*
Telemedicine^ Hub to spoke
Hub to providerSystem to Vendor
AMCsTier 1,2,3(Sunshine Provision)
FMV and commercially reasonable continues to gain importance in recent settlements
31

An arrangement will be considered “commercially reasonable” in the absence of referrals if the arrangement would make commercial sense if entered into by a reasonable entity of similar type and size and a reasonable physician (or family member or group practice) of similar scope and specialty, even if there were no potential DHS (designated health services) referrals. (69 Federal Register (March 26, 2004), Page 16093)
• Pre‐cursor to determining FMV• Arrangement must make business sense absent considering referrals• Hospital leadership must understand this standard since they will
primarily be the individuals who assess CR. Sample considerations:• Operational assessment – does the community need this service/number of specialists?
• Physician requirements – are the number of hours required?• Financial options – can you lease equipment from a third party vendor at a better rate than from a physician group?
• Counsels role – did hospital leadership walk through the business considerations?
• Valuation firm role – is the compensation at FMV?
Compliance Basics - Commercially Reasonable
32

33
Step #1 to FMV - Commercially Reasonable Guidelines
Economic/Financial Reasonableness
1. Consider if the subject arrangement is essential to the operations of the Organization and identify and define the specific purpose of the subject arrangement.
2. Consider if the subject arrangement represents a sensible and prudent business arrangement, excluding the consideration of referrals.
3. Understand how current economic conditions have been considered in relation to the subject arrangement.
4. Ensure that the subject arrangement furthers the strategic and financial goals of the Organization.
5. Determine why alternative models have not been chosen, if applicable, that may result in similar services being offered to the Organization by a provider with similar qualifications at lower costs.
Operational Reasonableness
Physician/Clinical Requirements
1. Consider the Organization’s size, patient population, and patient demand when assessing the need for the services (patient acuity and need warrants services).
2. Consider how the subject arrangement furthers patient care, patient satisfaction, and overall public benefit.
3. Ensure there are safeguards to reduce and eliminate the possibility of fraud, prohibited referrals, waste, or abuse in relation to the subject arrangement.
4. Establish a written agreement containing the material terms of the arrangement.
1. Ensure a physician is required to perform the services.
2. Ensure a physician of a particular specialty is required to perform the services if relying upon an indication of value which represents a specialty specific opinion.
3. Ensure the physician possesses the specialized training, qualifications, and experience required to provide the services.
4. Determine that the duties of the physician under the subject arrangement will not be duplicative of any other duties performed by the Organization’s personnel once the arrangement commences.
33

• Agreements should carefully be constructed• Compensation should not be tied to expected or actual referrals. This is important when establishing compensation or when setting mechanism to drive compensation.
• Carefully construct alternative payment models (gainshare, MSSP, ACO, bundled payments) since often tied to other (non‐physician) income streams.
• Do not determine FMV based on• What the hospital next door is paying.• Non‐comparable services and associated fees (i.e.: management vs. co‐management).
• Solely on opportunity cost of the physician performing a different service, or their “going rate” (surgery vs administrative work).
Compliance Basics - Fair Market Value
34

• Medical Directorships ‐ Document services and track time, pay hourly• Call coverage – understand the burden of call per OIG opinions, caution on
surveys• Clinical services and employed compensation
Benchmark productivity – average productivity warrants average compensation
Losses in a practice ‐ understand reason (safety net hospital, restricted coverage, coordinated care costs)
Stacking – total dollars and hours make sense?• Best Practice ‐ internal policies for compliance:
1. A consistent process to determine FMV, including written agreements2. Internal thresholds with triggers when a 3rd party appraisal may be needed3. Monitor to ensure that services were performed 4. Review agreement to verify the need for services still exist5. Understand and verify the assumptions underlying any valuation
Practical Compliance Tips – Traditional Arrangements
35

Quality Payments– Metrics outlined– Primarily outcomes metrics (versus process or reporting)– Be careful with low hanging fruit metrics– Benchmark performance against medical credible evidence– Ensure physician(s) will have demonstrable impact on quality– Check for overlap of payments from co‐management, bundled payments,
etc…
Shared Savings – No cherry picking or lemon dropping– Identify separate identifiable cost savings opportunities in advance– Ensure physician(s) will have demonstrable impact on cost savings– Consider cap methodology applied in CMS models
Understand the risk and responsibility of parties prior to determining split of quality or savings payments
Practical Compliance Tips – P4P Arrangements
36
1. Outline what ‘commercially reasonable’ services will be provided and how parties will be compensated
2. Valuation should match the agreement - may require several valuations for one agreement (clinical, administrative, on-call, P4P)
3. Thorough valuation process to establish compensation should be tied to each of the services provided
4. Establish and monitor a compliant and consistent process for establishing FMV
Understand recent settlements – beware of documentation regarding referrals or no documentation regarding services
Reference to multiple, objective, independently published salary surveys remains a prudent practice for evaluating Fair Market Value
Valuation method and benchmarking is important
Consider regulatory guidance and OIG opinions (shared savings, on-call beeper rate)
Methods that won’t hold up
• Compensation models built on referrals
• What hospital next door is paying
5. New challenge – transition to compensate physicians on quality and cost-saving outcomes rather than being reimbursed solely for services and procedures. There is a lack of survey data and guidance here.
FMV Take-Aways for Physician Compensation
37

• Most commonly provided under:• Direct employment agreements• Physician leasing agreements
• What is physician leasing?• “Synthetic” employment agreement• Physicians retain ownership of the practice• Asset acquisition or lease of assets may occur (ancillary services)• Independent contractor arrangement with a hospital• Hospital bills / collects for physician services and retains revenues• Hospital pays compensation on a productivity basis (typically per work
RVU) • Practice decides how to distribute compensation internally• Practice operating expenses may be assumed by the hospital or the
practice – be careful adding fixed expenses to $/WRVU!
Clinical Services - Overview
38

• Cost and Market Approaches• Cost to employ/contract with a physician based on market data• Most commonly utilized method among valuators• Simple to understand• Benchmarking analysis that aligns compensation and productivity
• Compensation and productivity data are obtained from independent, published surveys (is MGMA median OK?)
• MGMA Physician Compensation and Production Survey• AMGA Medical Group Compensation and Financial Survey• SCA Physician Compensation and Productivity Survey
• Common productivity metrics include:• Work RVUs• Total RVUs• Professional collections• Gross Charges• Patient encounters
Clinical Services - Valuation
39

• Benchmarking example (using MGMA survey):• Solo practitioner specialized in general orthopedic surgery• 2011 annual work RVU volume of 13,687
Clinical Services - Valuation
25th Median 75th 90th
Orthopedic Surgery: General 6,239 8,250 11,021 13,867
Subject Physician's Annual Work RVUs 13,867
Conclusion: Physician productivity falls at the 90th percentile
25th Median 75th 90th
Orthopedic Surgery: General $372,437 $497,088 $658,842 $825,044
Selected Compensation (based on work RVUs) $825,044
MGMA Physician Compensation and Production Survey
Physician Work RVUs
Physician Compensation
Takeaway: Valuators commonly benchmark multiple productivity metrics to multiple surveys.
40
• Common benchmarking mistakes include:• Including mid‐level provider productivity• Benchmarking total RVUs to reported work RVUs• Benchmarking total collections to reported professional collections• Miscalculation of patient encounters (read the data definition of each survey!)
• Common mistakes in using the reported compensation per work RVU:• Per MGMA, an inverse relationship exists between work RVU volume and compensation per work RVU
• Paying a highly productive physician the 75th to 90th percentile compensation per work RVU may result in compensation outside of FMV
• See illustration on the following page.
Clinical Services – Valuation
41
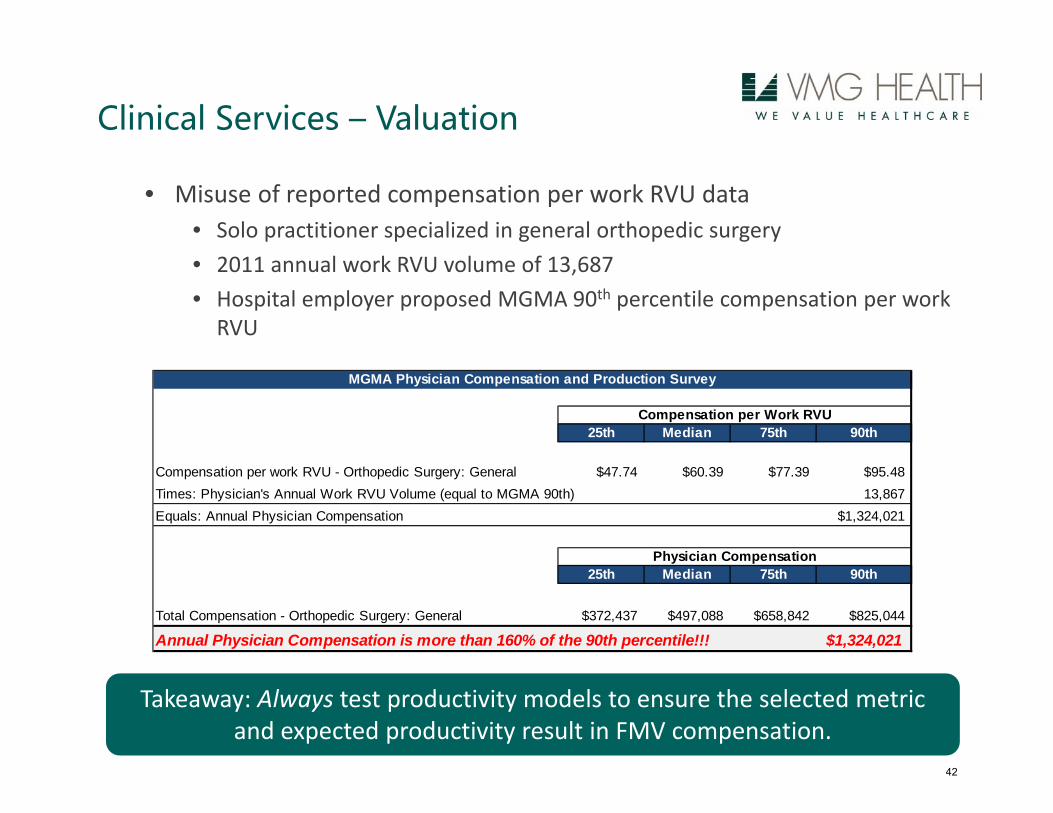
• Misuse of reported compensation per work RVU data• Solo practitioner specialized in general orthopedic surgery• 2011 annual work RVU volume of 13,687• Hospital employer proposed MGMA 90th percentile compensation per work RVU
Clinical Services – Valuation
25th Median 75th 90th
Compensation per work RVU - Orthopedic Surgery: General $47.74 $60.39 $77.39 $95.48Times: Physician's Annual Work RVU Volume (equal to MGMA 90th) 13,867 Equals: Annual Physician Compensation $1,324,021
25th Median 75th 90th
Total Compensation - Orthopedic Surgery: General $372,437 $497,088 $658,842 $825,044
Annual Physician Compensation is more than 160% of the 90th percentile!!! $1,324,021
Physician Compensation
MGMA Physician Compensation and Production Survey
Compensation per Work RVU
Takeaway: Always test productivity models to ensure the selected metric and expected productivity result in FMV compensation.
42

• Income Approach:• Another standard valuation approach• Considers normalized historical compensation• Considers normalized physician practice revenues less expenses and a reasonable rate of return to the employer.
• Considers specific economic factors of a physician’s practice such as:– Local reimbursement– Payor mix– Procedure mix– Practice expense profile
Clinical Services - Valuation
Takeaway: The Income Approach often serves as a reasonableness check to the results of the Cost and Market Approaches.
43

• Historically, physicians provided call coverage to Hospital emergency departments on an uncompensated basis
• Sometimes a condition of medical staff membership• Sometimes granting/renewal of clinical privileges
• Not anymore… Why not?• Increasing number of uninsured patients• Aging active physician staff• Increasing cost of malpractice insurance and declining reimbursement
• Perceived increase in risk of lawsuits
Call Coverage Services – Overview
44

• According to the Sullivan, Cotter and Associates Call Coverage Survey:• 63% of survey respondents had difficulty finding physicians to provide call coverage
• 7% had shut down one or more services due to lack of call coverage• 58% employ physicians specifically to provide call coverage• Most common payment structure is an hourly rate or a stipend
• First question to ask prior to valuation: Are call coverage services generally needed for the subject specialty?
• What is the burden of call for the subject specialty?
Call Coverage Services - Overview
45

• As noted previously, no published standards exist for valuing call coverage services
• Regulatory guidance – OIG Advisory Opinion no 07‐10• Issued September 20, 2007• OIG agreed not to prosecute a hospital for paying for call coverage services• OIG found the arrangement to be at low risk for fraud and abuse, and noted the
following:– Independent analysis was conducted to ensure compensation was FMV– The per diem rate was designed to compensate based on the burden of call– On‐call physicians were obligated to provide care to ED patients regardless of the
patient’s ability to pay– Physicians in each specialty received the same per diem rate– The medical center had a legitimate need for the coverage services
Call Coverage Services – Valuation
Takeaway: The development of a reasonable and FMV rate for call coverage services must consider the specific burden of call.
46

• Cost Approach – Beeper Rate Method• Determines call compensation as a percentage of base compensation• Base compensation rates are based on multiple, published surveys:
– MGMA Physician Compensation and Production Survey– AMGA Medical Group Compensation and Financial Survey– SCA Physician Compensation and Productivity Survey
• Percentage of base ranges (or beeper rates) are based on market observations and call coverage pay rates of non‐referring physicians
• Base rate may need to be adjusted for independent contractor relationship
• Factors to consider in determining a Beeper Rate:• Volume of call
– Phone calls– In‐person
• Response time requirements• Ability to bill/collect• Payor mix of patients served• Restricted versus unrestricted coverage
Call Coverage Services - Valuation
47

• Market Approach:• Considers available market survey data for call coverage services• Currently two prevalent market surveys:
– MGMA Medical Directorship and On‐Call Compensation Survey– SCA Physician On‐Call Pay Survey
• Compensation data within the surveys is reported as an hourly rate of daily stipend
• Limitations of survey data• Based on referral relationships (physician‐hospital)• Limited number of respondents• Can be large variance in the fees reported• Important factors such as call volume payor mix are unknown• Details such as whether the physician bills/collects are unknown
Directorship Services Overview
Takeaway: The shortfalls of the Market Approach often limit its use to a reasonableness check to the results of the Cost Approach.
48

• As with call coverage, historically it was not unusual for physicians to volunteer their time to hospitals for medical director duties
• Due to the increase in duties and demand for services, physicians require reasonable payment for their time and services
• According to Integrated Healthcare Strategies Medical Director Survey, medical directors commonly provide the following services:
• Act as a liaison between the medical staff and hospital management• Participate in the JCAHO accreditation process• Physician credentialing and peer review• Utilization review and quality improvement• Establish and implement clinical pathways• New program development and implementation
Medical Director Services - Overview
49

• Preliminary questions to ask prior to valuation:• Are the services needed (i.e., how many hours? How many other directors?)• Do the services require a physician? A specific specialty?
• Cost Approach• Considers the cost of the physician’s time based on clinical compensation• Considers multiple, published compensation surveys:
– MGMA Physician Compensation and Production Survey– AMGA Medical Group Compensation and Financial Survey– SCA Physician Compensation and Productivity Survey
• Careful with “opportunity cost”
• Limitations of the Cost Approach• Compensation does not match the services provided• Stark indicates that clinical compensation may not be FMV for administrative services
Medical Director Services - Valuation
Takeaway: Limited reliance is usually placed on the Cost Approach. 50

• Market Approach• Considers compensation data for similar services• Considers multiple, published medical director compensation surveys
– IHS Medical Director Survey– MGMA Medical Directorship and On‐Call Compensation Survey– SCA Physician Compensation and Productivity
• Annual hours set at 2,000 based on Stark guidance
• Limitations of the Market Approach• Limited number of respondents• Some conservative parties argue the data is “tainted” with referral relationships
• Other Considerations• Productivity data is not applicable to medical director survey data• Percentiles above the median are often selected based on qualitative factors
Medical Director Services - Valuation
Takeaway: The Market Approach matches compensation and services and is generally relied upon to determine FMV medical director compensation.
51

BEST PRACTICES IN VALUATIONS / TRANSACTIONPROCESS
52
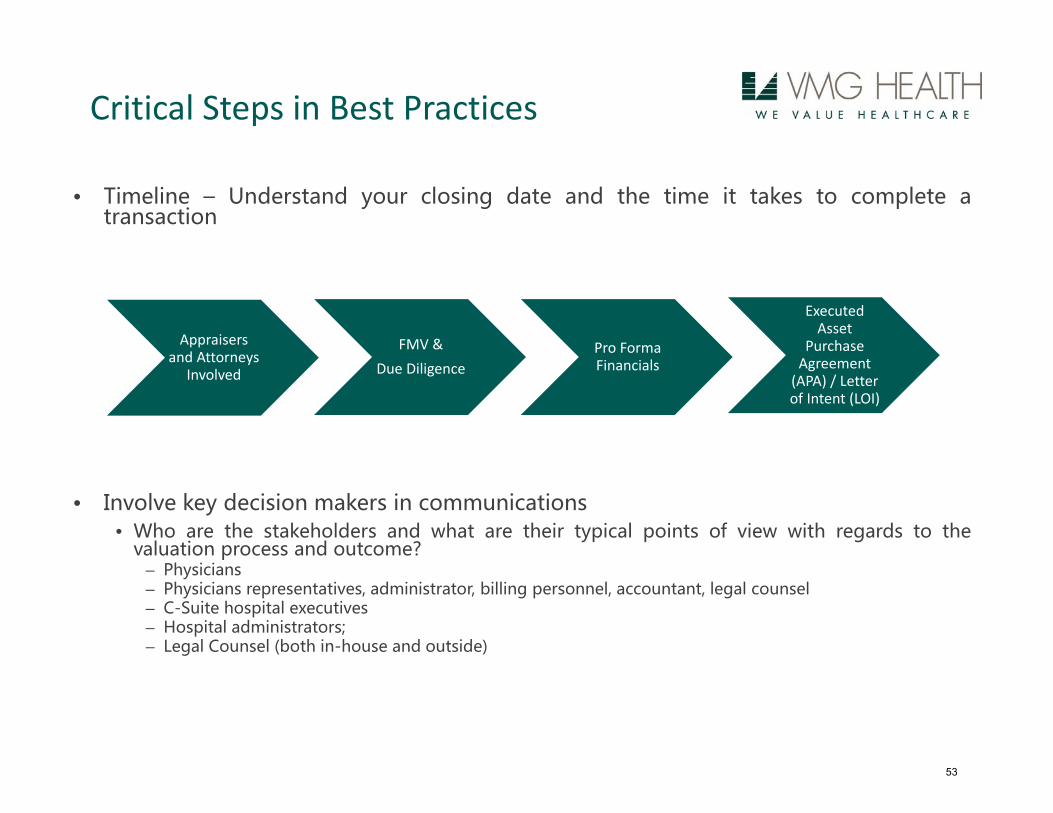
Critical Steps in Best Practices
• Timeline – Understand your closing date and the time it takes to complete atransaction
• Involve key decision makers in communications• Who are the stakeholders and what are their typical points of view with regards to the
valuation process and outcome?– Physicians– Physicians representatives, administrator, billing personnel, accountant, legal counsel– C-Suite hospital executives– Hospital administrators;– Legal Counsel (both in-house and outside)
Executed Asset
Purchase Agreement (APA) / Letter of Intent (LOI)
FMV & Due Diligence
Pro Forma Financials
Appraisers and Attorneys
Involved
53
• Were there any qualifying assumptions or scope restrictions based on dataavailability or timing that should be discussed further? Do these qualifications andlimitations impact the ability of the appraisal to withstand regulatory scrutiny?
• Is the FMV indication consistent with the transaction structure?• Net Working Capital• Non-Operating Assets
• Related-party real estate – was consideration given to performing a fair marketrental rate analysis?
• Does post-transaction compensation align with the assumptions utilized to derivethe FMV of the Practice?
• No Double Counting – The physician cannot be compensated for the revenue twice, boththrough the up front purchase and the ongoing compensation.
Best Practices – Practice Acquisition Checklist
54

• Confirm that the arrangement (transaction or compensation agreement) hasdocumentation supporting that it is commercially reasonable absent the consideration ofreferrals.
• Ensure the transaction or compensation terms are clearly outlined, set in advance andagreed upon in writing.
• If an appraiser was engaged to provide the analysis, do they have the appropriatecredentials?
• Did the appropriate party representatives to the arrangement review, understand andverify the assumptions and value drivers relied upon in the analysis?
• If there are multiple services provided, does each have a defensible valuationmethodology outlined?
• Have multiple, objective market surveys been considered as part of the analysis (whenavailable)? If only one survey is utilized, it is important that the valuation provide sufficientreasoning to explain the departure from use of multiple surveys.
• Has the potential for retaining professional collections and the employment/contractorstatus of the physician been considered?
• Are the physicians required to document time and services prior to receiving payment forthe services?
• Do the services being provided overlap with other potential financial arrangements?
Best Practices – Physician Compensation Checklist
55

56
Questions?Contact Info Below:
Bridget Triepke, CPADirector
Contact InformationPhone: 972‐616‐[email protected]
Office AddressChateau Plaza2515 McKinney Ave., Ste. 1500Dallas, Texas 75201United States
Ben Ulrich, CVADirector
Contact InformationPhone: 972‐616‐[email protected]
Office AddressChateau Plaza2515 McKinney Ave., Ste. 1500Dallas, Texas 75201United States
56